-
7/27/2019 1_5 farmacocinetics
1/8
1.5: Pharmacokinetics, Pharmacodynamics,and Pharmacogenetics
1.1.1
Introduction
The ultimate eect a medication has on the body is the
complex
summation o how it enters, aects, and leaves the body, and
these can all vary substantially rom one person to another
de-
pending on a wide variety o actors. This body-drug
interaction
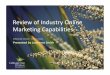
can be broken down or better understanding into pharmacoki-
netics (drug processing) and pharmacodynamics (drug eects),
as illustrated in Figure 1, and each o these broad areas can
in
turn be aected by an individuals genetic makeup leading to
pharmacogenetics (Figure 2). In this module, the authors at-
tempt to breakdown and simpliy each ocus or better under-
standing and then reunite them as is best or practical
applica-
tion, using a case example.
Pharmacokinetics
The term pharmacokinetics reers to the action the body
takes on a medication. When a medication is ingested or
admin-
istered, the medication is absorbed, distributed,
metabolized,
and eliminated. Key pharmacokinetic parameters exist or all
our o these actions. Knowledge o general pharmacokinetic
principles can be helpul in understanding the likelihood o
adverse eects o a medication, avoiding drug interactions,
pre-
dicting likely onset or duration o action, or understanding
the
inuence o organ dysunction on the use o a medication.
AbsorptionA medication can be absorbed rom the gastrointestinal
(GI) tract,
through the oral mucosa (e.g., sublingual nitroglycerin),
through
the skin (e.g., transdermal clonidine), or subcutaneously
(e.g.,
enoxaparin). Absorption is not relevant in the setting o
intrave-
nous (IV) administration because the drug is administered
directly
into the bloodstream. Medications that are available as
immedi-
ate-release dosage orms begin to be absorbed upon ingestion.
Some medications are available in ormulations that allow
or slower release o the medication (i.e., extended-release,
Chapter 1: General Principles
1.5: Pharmacokinetics, Pharmacodynamics,and
PharmacogeneticsDavid E. Lanfear, MD, MS, FACC
Research Grants: Medtronic, Cardioxyl, Amgen, Sanof-Aventis,
Johnson & Johnson; Consulting Fees/Honoraria:
Otsuka, Thoratec.
James Kalus, PharmD
This author has nothing to disclose.
Learner Objectives
Upon completion o this module, the reader will be able to:
1. Demonstrate understanding and knowledge o pharmacokinetic
drug interactions or common cardiovascular drugs.
2. Describe how principles o pharmacokinetics and
pharmacodynamics can inuence rational drug prescribing.
3. Defne pharmacokinetics and pharmacodynamics as
characteristics o medical therapeutics.
4. State principles o pharmacogenetics in cardiovascular drug
therapy and cite relevant examples.
sustained-release, delayed-release). Ater ingestion, these
drugs
are slowly made available or absorption, which allows or
less
requent dosing. For example, niedipine is available both as
anextended-release and as an immediate-release ormulation, with
sharp clinical dierences between them. The extended-release
ormulation can be given once daily, whereas the immediate-
release ormulation must be administered three times daily
and
can cause rapid hemodynamic changes, which may contribute
to adverse cardiac events.
Absorption o a drug may also be aected by a variety o actors
including the presence or absence o ood, co-administration
with other medications (e.g., antacids) that may bind with
the
Figure 1Schematic of a Drug Pathway Depicting
Transport,Targeting, and Metabolism
Schematic of a Drug Pathway Depicting Transport,Targeting, and
Metabolism
Cell MembraneDrug Absorption
Transport
Inactivation
(Activation)
Metabolite
DownstreamSignalling
Cellular Target
X
X
Y
X-1
Pharmacologic Effects
-
7/27/2019 1_5 farmacocinetics
2/8
1.1.2 Chapter 1: General Principles
medication, or GI tract abnormalities. When a transdermal
patch is used, absorption can be altered i the patch has
been
cut, or by changes in cutaneous blood ow (e.g., a high dose
o
vasopressors causing reduced cutaneous perusion).1
The amount o drug available ater absorption by a non-IV
route, divided by the amount o drug available ater IV admin-
istration is reerred to as bioavailability. All medications
have
an inherent bioavailability related to efciency o absorption
and
other actors. For example, the bioavailability o oral
amioda-
rone is approximately 50% because one-hal as much drug is
available ater oral administration, as compared to IV
adminis-
tration.
P-glycoprotein (P-gp) also oten plays a role in determining
bio-
availability. P-gp is an adenosine triphosphate
(ATP)-dependent
drug transporter that can eux certain drugs back into the GI
tract or kidney ater absorption, thereby decreasing
absorption.
Co-administration o a medication with an inhibitor o P-gp
may thus increase bioavailability o the medication. Since
P-gp
aects or is eected by many medications, it is important to
note which drugs are P-gp inhibitors and substrates in order
to
anticipate these interactions. For example, a clinically
relevant
P-gp interaction occurs when digoxin and amiodarone are co-
administered. P-gp eux o digoxin into the GI tract is
inhibited
by amiodarone, leading to a doubling o the digoxin
concentra-tion. Thereore, digoxin dose should be decreased by
one-hal
when initiating amiodarone.
Other important inhibitors o P-gp are quinidine, verapamil,
cyclosporine, tacrolimus, and many o the protease
inhibitors.2
It should also be noted that P-gp induction can also occur,
although less commonly. One example o a drug interaction
that occurs due to P-gp induction is the clinically
signifcant
interaction between riampin (a P-gp inducer) and the new
oral
anticoagulant, dabigatran, whose bioavailability may be com-
promised by this.
Another actor that may impact bioavailability is whether or
not
the drug undergoes frst-pass metabolism by the liver.
First-pass
metabolism reers to rapid metabolism that occurs ater
absorp-
tion, but beore the drug has reached the systemic
circulation
where it will have its eects. A drug that undergoes
extensive
frst-pass metabolism will have relatively lower oral
bioavailability
than otherwise expected.
DistributionAll medications have an apparent volume o
distribution (Vd), a
calculated value that relates dose o drug (e.g., millograms)
to
the concentration achieved in the blood (e.g., millograms
per
deciliter). Typically, Vd is expressed as a volume (liter) or
volume/
body weight (liter per kilogram). For medications where
specifc
drug levels are targeted, knowledge o the typical volume o
distribution o a drug can be useul in estimating the
concentra-
tion that will be achieved with a given dose o the drug.
Vd can also assist the clinician in understanding the extent
o
distribution. For example, amiodarone has one o the largest
volumes o distribution o any cardiovascular agent (approxi-
mately 50 L/kg). This is notable because amiodarone is well
known to cause extracardiac adverse eects and appears to
distribute to a variety o tissues. A newer agent,
dronedarone,
has pharmacologic properties similar to those o amiodarone,
yet has ewer extracardiac toxicities and a much smaller
volume
o distribution (approximately 15 L/kg).
In an individual patient, Vd can dier rom population
estimates
due to numerous actors including age, body habitus, disease
states, nutritional status, pregnancy, and critical illness.
For
example, selection o the appropriate bolus dose o lidocaine
is based on Vd and can be aected by these actors. Typical
loading doses are 1-1.5 mg/kg. The 1 mg/kg dose is oten used
in the elderly or in patients with heart ailure because these
pa-
tients have a lower volume o distribution than younger
patients
or those with normal ventricular unction. Thereore, a lower
dose will be required to achieve an appropriate lidocaine
level.
Protein binding may also inuence Vd, because an increase
or decrease in binding o drug to blood proteins can lead to
a
corresponding alteration in calculated Vd. For example,
digoxin
loading doses should generally be reduced in patients with
severe renal dysunction (creatinine clearance
-
7/27/2019 1_5 farmacocinetics
3/8
1.5: Pharmacokinetics, Pharmacodynamics,and Pharmacogenetics
1.1.3
The most common CYP enzyme involved with drug interactions
is CYP 3A4. Numerous cardiac medications are either
inhibitors
or substrates o CYP 3A4, including amiodarone, simvastatin,
and several calcium channel blockers. When co-administered,
these medications can reduce the inactivation o the other
and,
thus, increase medication exposure, resulting in toxicities.
Table 1 summarizes important CYP 450 enzyme system sub-
strates and inhibitors. As mentioned previously, CYP enzymesalso
play an important role in activating certain medications,
reerred to as prodrugs. For example, CYP 2C19 is a key
enzyme
in the conversion o clopidogrel (which is an inactive prodrug
in
its native state) into its active metabolite, which actually
causes
platelet inhibition.
Recently, much attention has been given to a potential drug
interaction between omeprazole and clopidogrel. The
mechanism
o this drug interaction is inhibition o CYP 2C19 by
omeprazole,
which results in reduced conversion o clopidogrel to its
active
metabolite, thus reducing clopidogrel eectiveness; however,
the
clinical signifcance o this interaction continues to be
debated.5
Medications can also be CYP 450 enzyme inducers. Important
CYP enzyme inducers are riampin (2C9, 3A4), carbamazepine
(3A4), tobacco (1A2), phenytoin (3A4), and phenobarbital
(3A4). When a CYP 450 enzyme substrate is administered with
an inducer o the same enzyme system, there is potential or
in-
creased metabolism o the target drug and, thereore,
potential
reduction in drug concentrations.
EliminationElimination reers to how the medication actually
exits the body.
A ew important pharmacokinetic parameters are relevant to
drug elimination. The frst is hal-lie, which is the amount o
time required or the concentration o drug to be reduced by
one-hal. When discontinuing a medication, it generally takes
4
to 5 hal-lives or the drug to be completely removed rom the
body. Conversely, when initiating a drug, 4 to 5 hal-lives
will
also be required to achieve steady state concentrations.
Table 1Selected Substrates and Inhibitors of the CYP 450
System
*Produces active orm o agent rom prodrug.
CYP = cytochrome; HMG-CoA = hydroxy-methyl-glutaryl coenzyme
A.
Reproduced with permission rom R, DR G, ML R, PH V. Digoxin. In:
Evans WE, Schentag JJ, Jusko WJ, eds. Applied Pharmacokinetics:
Principles o
Therapeutic Drug Monitoring. Vancouver, WA: Applied
Therapeutics, Inc.; 1992.
Selected Substrates and Inhibitors of the CYP 450 System
Group/Class Medication (s) Cytochrome P450 System
HMG-CoA reductase inhibitors Atorvastatin, lovastatin,
simvastatin 3A4
Fluvastatin 2C9
Beta-blockers Metoprolol 2D6
Calcium channel blockers All except amlodipine 3A4
Angiotensin-receptor blockers Losartan 2C9
Antithrombotics Warfarin 2C9
Clopidogrel* 2C19
Antiarrhythmics Amiodarone 2C9, 3A4
Mexilitine 1A2
Propafenone 2D6
Immunesuppressives Cyclosporine,tacrolimus 3A4
Calcium channel blockers Diltiazem 3A4
Verapamil 3A4
Gembrozil 2C8
Proton pump inhibitors Omeprazole, lansoprazole 2C19
Antibiotics Clarithromycin, erythromycin 3A4
Fluconazole 2C9, 3A4
Ketoconazole, itraconole 3A4
Selective serotonin reuptake Fluoxetine, Paroxetine
2D6inhibitors
Substrates
Inhibitors
-
7/27/2019 1_5 farmacocinetics
4/8
1.1.4 Chapter 1: General Principles
Steady state is the point at which drug administration is
equal
to drug elimination.3 All medications are either eliminated
rom
the body unchanged, or i acted upon by drug metabolizing
enzymes (as described earlier), they are converted to active
or
inactive metabolites and subsequently eliminated.
The majority o medication/metabolite elimination occurs
through renal mechanisms. Patients with renal dysunction
have
reduced renal clearance o drugs and are oten at greater risk
o toxicity o agents that depend on this route. For
example,digoxin is eliminated via renal mechanisms, and the
requency
o dosing decreases rom daily to every other day in severe
renal
dysunction. Most oten renal elimination occurs via fltration
at
the glomerulus, although some medications are secreted into
the renal tubules. Both mechanisms can mediate alterations o
drug clearance and drug interactions. For example, doetilide
is secreted in renal tubules and, thus, may interact with
agents
that block tubular secretion (e.g., cimetidine, trimethoprim,
and
ketoconazole), resulting in higher doetilide levels.
Pharmacodynamics
The term pharmacodynamics reers to the action the drug
takes on the body or the biologic response that is elicited
by
the drug. Medications are generally thought to interact with
a particular target in the body, and this interaction alters
the
unction o the target, thus producing the medications eects.
The drug target can be a wide variety o macromolecules in
the
body, such as neurohormonal signaling receptors (e.g.,
adren-
ergic receptors), enzymes (e.g., HMG-CoA reductase, vitamin
K
2,3-epoxide reductase), ion channels (e.g., calcium
channels),
and many others in which the medication directly or
indirectly
alters the unction o a biologically active substance.
The pharmacodynamic eects o a drug could reer to both
the desired therapeutic eects as well as the toxic eects.
The
term therapeutic index reers to the dierence between the
minimal therapeutic threshold and the minimal toxic
threshold.
Some medications have a narrow therapeutic index, meaning
there is little dierence between doses that produce efcacy
and doses that produce toxicity in a given patient. However,
most drugs have a broader therapeutic index, where doses
much higher than usual therapeutic doses must be given to
cause toxicity. Oten, drug levels o medications with a
narrow
therapeutic index can be monitored in order to avoid
toxicity
(e.g., digoxin, procainamide, lidocaine).
When a medication elicits a response by interacting with thedrug
target, there is oten a dose-response pattern that can take
dierent orms. Most medications exhibit a linear
dose-response
relationship through their therapeutic range, where the
pharma-
cologic eect increases proportionately with
number/proportion
o occupied targets. Nonlinear dose-response relationships
occur
as well but are less common at typical doses o most
medications.
Medications that stimulate a signaling receptor, such as the
beta-adrenergic receptor, are called agonists (e.g.,
epineph-
rine), whereas medications that block the action o a
receptor
are called antagonists (e.g., metoprolol). Antagonists can
be
either competitive or noncompetitive. Competitive
antagonists
take the place o a naturally occurring ligand to block
activ-
ity, whereas noncompetitive antagonists bind elsewhere and,
thus, are less aected by the concentration o the usual
ligand.
Agents that aect the adrenergic system or those that
interact
with neurotransmitters (e.g., opioids) are good examples o
this
type o mechanism.
Many cardiovascular drugs produce their pharmacodynamic
eect by inhibiting the action o cardiac ion channels.
Calcium
channel blockers inhibit the inux o calcium into the cardiac
pacemaker cells, which can limit the inotropic and
chronotropic
activity o the heart. Vaughan Williams class I
antiarrhythmic
drugs typically inhibit inux o sodium through sodium chan-
nels, whereas class III antiarrhythmics inhibit eux o
potassium
through potassium channels. A notable pharmacodynamic
eect o the class III antiarrhythmic drugs is prolongation o
the
QT interval. Concomitant use o more than one medication that
prolongs the QT interval could result in a pharmacodynamic
drug interaction, increasing the patients risk or developing
torsade de pointes.
Enzyme inhibition is another important target o many medica-
tions. The hydroxy-methyl-glutaryl coenzyme A (HMG-CoA)
reductase inhibitors are an important example o a
cardiovascu-
lar medication class that produces a pharmacodynamic
response
through enzyme inhibition. HMG-CoA reductase inhibitors
block
the enzyme responsible or the fnal step o cholesterol orma-
tion, leading to reductions in intracellular cholesterol levels
in
the liver, which then cause enhanced reuptake o low-density
lipoprotein (LDL) particles rom plasma to liver, thus
lowering
plasma LDL levels.
Another example is vitamin K 2,3-epoxide reductase (VKORC1),
which is the target o wararin. Wararin inhibits VKORC1 rom
reducing vitamin K and, thus, impairs production o vitamin
K-
dependent clotting actors.
Drugs may also bind to other types o proteins and enhance or
impair their physiologic processes. Heparin is a good example
o
this. Antithrombin is a protein that can inactivate activated
throm-
bin, serving a counter-regulatory unction in the coagulation
cascade. Heparin enhances antithrombins action, producing an
antithrombotic eect due to greater inactivation o thrombin.
On
the other hand, bivalirudin is a direct thrombin inhibitor; it
binds
to thrombin and prevents thrombin rom converting fbrinogen
to
fbrin, resulting in the antithrombotic eect.
An understanding o pharmacodynamics can be important in
drug selection. When selecting a positive inotropic therapy
or
the treatment o end-stage systolic heart ailure, two
available
options are milrinone or dobutamine. Milrinone and dobuta-
mine both produce increases in intracellular calcium
concentra-
tions, increased heart rate, and increased contractility;
however,
the mechanism by which they achieve this eect is quite dier-
ent. Dobutamine acts as an agonist or the beta-1 receptors
on
the myocardium, increasing cyclic adenosine monophosphate
-
7/27/2019 1_5 farmacocinetics
5/8
1.5: Pharmacokinetics, Pharmacodynamics,and Pharmacogenetics
1.1.5
(cAMP) intracellularly and subsequently increasing calcium
in-
ux. Milrinone achieves this action by inhibiting the
breakdown
o cAMP, bypassing the beta-receptors, yet still increasing
cAMP
and calcium concentrations.
Considering this, in patients requiring inotropic support
who
have recently taken or are planned or uture beta-adrenergic
blocking agents, milrinone may be a more sensible choice.
Simi-
larly, one might expect milrinone and dobutamine to have
syner-
gistic eects (and toxicities) when co-administered because
theyare both enhancing the same pathway but at dierent steps.
An understanding o the interplay between pharmacokinetics
with pharmacodynamics is also important in practice. Aspirin
ir-
reversibly inhibits the action o cyclooxygenase (COX) enzyme
in
the platelets, leading to prevention o platelet activation.
While
the pharmacodynamic eect o most drugs will not be present
4 to 5 hal-lives ater discontinuation, the pharmacodynamic
eect o aspirin persists long ater 4 to 5 hal-lives have
passed
(approximately 12 to 24 hours or aspirin). This is because
the
irreversible inhibition o the COX enzyme in platelets
renders
those platelets permanently inactive. Thereore, the
antiplatelet
eect o aspirin does not resolve until new unctional
platelets
have been generated, which generally takes approximately one
week.
Pharmacogenetics
Pharmacogenetics is the area o research and medicine that
is concerned with understanding how genetic variation im-
pacts drug response. While still largely a research feld, it
now
has burgeoning clinical applications. Important
relationships
between genetic variation and drug eect have been observed
or a growing number o commonly used drugs,6 and ongoing
studies should continue to increase the relevance o pharma-
cogenetics to clinical practice. There are commercially
available
pharmacogenetic diagnostic tests and a handul o examples
with published guidelines or genetically-guided therapy,
some
o which are relevant to the cardiovascular system (e.g.,
wara-
rin). Thus, it is worthwhile to understand this topic
conceptually
as well as in practical terms.
While the average population response or most approved
medications is avorable, it is clear that signifcant
interindividual
variation exists in the response to most therapeutics.
Genetic
variants exist throughout the genome, and many such variants
reside in genes related to medication response (e.g., drug
recep-
tors, drug metabolizing enzymes) and have known
unctionalconsequences.
Inherited dierences in medication response were recognized
as early as the 1950s, then ocused mainly on drug metabo-
lism.8,9 Since then, as our understanding o pharmacokinetics
and dynamics has deepened, many points o genetic inuence
throughout a drug pathway have come into better ocus
(Figure 1). This includes variants that impact absorption,
dis-
tribution, excretion, binding to drug targets, and even
down-
stream eect mediators.6
The genetic sequence variants o potential interest come in
many orms with single nucleotide polymorphisms (SNP) being
the most common. There are likely at least 30 million SNPs
in
the human genome, each o which represents a change o one
base-pair to another at a given location in the DNA
sequence.
This may or may not result in a change in unction or amount
o the resulting transcript, and thus protein, depending on
the
nucleotide change and location.
SNPs in protein-coding regions can either be
synonymous(resulting in no amino acid change) or nonsynonymous,
which
results in an amino acid alteration, and may impact protein
unction directly. They can also occur in regulatory
sequences
such as promoter regions, which despite being noncoding, can
impact gene expression. Even more oten, SNPs are located in
other areas with less certain unctional impacts, such as
introns
or intergenic regions, though unctional impact cannot be
ruled
out based on location alone.
Other types o sequence variants that are less common also
occur. These include repeats (short or long sequences that
occur
a variable number o times), and insertion/deletion polymor-
phisms (one or more base pairs, which are either present or
absent). Similar principles regarding location and impact
apply
to these variants as well (e.g., variants are more likely to
have
a unctional impact i they are within a gene vs. intergenic
region). More recently, larger-scale genetic variation has
been
recognized, which can also impact gene unction, or example,
copy number variants (i.e., entire gene or larger segments
that
are duplicated).
As science has learned more about the interplay o drugs
and genes, genetic sequence variants have helped to explain
more o the variation in response between patients; in
specifc
examples, this has ranged widely and as high as 95%. The
ulti-
mate goal o pharmacogenetics (both in terms o research and
as a clinical tool) is to leverage this knowledge to help
physicians
provide more rational, efcient, and targeted treatments to
their
patients (Figure 2).7
On the other hand, due to the act that one may not always
have a perect understanding o a drug pathwayand with
the emergence o high-throughput genotyping technology,
genome-wide approaches are now also being used in research,
giving birth to pharmacogenomics. As discussed in the
previous sections on pharmacokinetics and dynamics, many
nongenetic actors (e.g., age, organ unction, drug
interactions)
inuence medication response; thus, it is important to view
pharmacogenetic actors within this larger ramework, supple-
menting (not supplanting) other more conventional
predictors.
In this way, pharmacogenetic knowledge will oten supplement
and interact with ones knowledge about pharmacokinetics and
dynamics.
Initial applications o pharmacogenetics were limited to
medica-
tions with very narrow therapeutic indices. A classic example
o
pharmacogenetics being used clinically is azathioprine and
the
gene thiopurine methyl transerase (TPMT). Azathioprine is
used
as an immunosuppressive agent in heart transplantation, as
well
-
7/27/2019 1_5 farmacocinetics
6/8
1.1.6 Chapter 1: General Principles
as a treatment in some types o cancer. TPMT is responsible
or
inactivation o azathioprine (actually metabolizing the
active
metabolite 6-mercaptopurine into an inactive product).
Sequence variants in TPMT can disable this enzyme, thus
exposing the patient to higher than anticipated levels o the
active metabolites and causing toxicity, typically bone
marrow
suppression. This example also illustrates how a
pharmacoge-netic interaction operates via alteration o
pharmacodynamic or
pharmacokinetic actors. The pharmacogenetic impact o TPMT
variants would be difcult to appreciate without
understanding
the pharmacokinetics o azathioprine; urthermore, it suggests
the solution-reduced doses o azathioprine in subjects with
the
alternative alleles.
Advances in pharmacogenetics are now showing promise or a
broader range o medications, including cardiovascular
medica-
tions. A well-developed example o pharmacogenetics relevant
to cardiovascular disease is wararin. Wararin acts by
binding
to the vitamin K 2,3-epoxide reductase complex (VKORC1), the
enzyme responsible reducing vitamin K into its active orm,
and
genetic variants in this drug target cause resistance to
wararin
eects, requiring higher dosing. Wararin is primarily metabo-
lized by CYP 2C9 (CYP2C9), and genetic variants in this
enzyme
result in reduced enzyme unction and, thus, greater wararin
exposure. Genetic polymorphisms in VKORC1 and CYP2C9 ac-count or
roughly 40% o variation in wararin dose.
Many other cardiovascular drugs have been studied and have
signifcant pharmacogenetic interactions but have yet to
become clinically applicable. Examples include
beta-adrenergic
antagonists and adrenergic-receptor gene variants, HMG-CoA
reductase inhibitors and the risk o myopathy, and
clopidogrel
eectiveness with CYP2C19 polymorphisms. These and other
examples are summarized in Table 2.
Table 2Summary of Key Cardiovascular Pharmacogenetic
Interactions
ADRB1 = beta 1 adrenergic receptor gene; LVEF = let ventricular
ejection raction; I/D = insertion/deletion;
ADRA2C = adrenergic receptor, alpha 2c; ACE =
angiotensin-converting enzyme gene;
GRK5 = G-protein coupled receptor kinase 5 gene; AA = Arican
American; HF = heart ailure; INR = international normalized
ratio;
LVH= let ventricular hypertrophy; BP = blood pressure; CYP2C9 =
cytochrome P450, amily 2, subamily C, polypeptide 9;EF = ejection
raction; EDV = end-diastolic volume; ESV = end-systolic volume.
Summary of Key Cardiovascular Pharmacogenetic Interactions
D allele homozygotes with HF had lowerevent-free survival on
low-dose ACE-I therapy
Among HF patients, only carriers of the Iallele showed
improvements in EF, EDV, andESV with spironolactone treatment
Increased survival and LVEF recovery withArg389Arg
Glu27 allele associated with better responseto
carvedilolIncreased risk of death or transplantationArg16/Gln27
double homozygotes
Enhanced benet of bucindolol in WT-homozygotes for mortality or
transplantation
Leu allele leads to increased survival in AApatients in the
absence of beta-blockers
Lower warfarin dose requirements for similarlevel of
anticoagulation
Greater warfarin dose requirements for INR
Increased risk of myopathy or rhabdomyolysis
Greater residual platelet activity, worseoutcomes after
stenting
Increased ACE levelassociated with D alleleIncreased ACE
levelassociated with D allele
Arg389 shows greateradenylate cyclase activityGlu27 allele has
decreased
receptor down-regulationGly16 allele has greaterreceptor
down-regulationD-allele results in loss ofauto-inhibition
Leu allele enhances beta-receptor desensitizationDecreased
enzymatic activity
Transporter; variant pheno-type not well established
Reduced enzymatic activity,reduced conversion to activedrug
rs4646994
rs4646994
rs1801253
rs1042714
rs1042713
rs61767072
rs17098707
Intron 16 I/D
Intron 16 I/D
Arg389Gly
Glu27Gln
Gly16Arg
Exon 1 I/D
Gln41Leu
*2, *3
*2, *3
ACE
ACE
ADRB1
ADRB2
ADRA2C
GRK5
CYP2C9
VKORC1
SLCOB1
CYP2C19
ACE
Inhibitors
Aldosterone
Antagonists
Beta-
Blockers
Warfarin
Simvastatin
Clopidogrel
Drug Gene Variant rs Number Molecular Phenotype Clinical
Phenotype
-
7/27/2019 1_5 farmacocinetics
7/8
1.5: Pharmacokinetics, Pharmacodynamics,and Pharmacogenetics
1.1.7
Principles Applied in a Case Discussion
Pharmacokinetics, pharmacodynamics, and pharmacogenetics can
impact medication eects, explain drug interactions, or
suggest
modifcations o dosing. These principles do not act in
isolation,
but rather clinical application o each is critically dependent
on
appreciating the others as well. Thus, understanding the
interplay
o principles is important to optimizing clinical care. The
ollowing
case discussion is presented to provide an illustrative example
o
applying these principles together in a case-based setting:
Case StudyA 50-year-old man with a history o hypertension,
systolic heart
ailure, and hyperlipidemia presents to the emergency depart-
ment with palpitations and shortness o breath, which started
today, and he is ound to be in atrial fbrillation. Home
medica-
tions include hydroclorothiazide 25 mg daily, metoprolol XL
100
mg daily, aspirin 81 mg daily, digoxin 0.25 mg daily (last
digoxin
level = 1.5),and simvastatin 40 mg daily. He is admitted,
cardio-
verted, and wararin is initiated.
DiscussionWararin is a good example o pharmacogenetic
interactions
operating via both pharmacodynamic and pharmacokinetic
aspects o the drug. Recommended algorithms or determining
initial wararin dosing based on genotype have been
published;
commercial testing is available or genotype; pharmacogenetic
dosing is routinely used at some institutions; and it has
been
associated in multiple studies with more rapidly and more
oten
achieving therapeutic international normalized ratio (INR).
CYP2C9 variant alleles (so-called *2 or *3) are associated
with
reduced enzyme activity, resulting in delayed clearance o
wararin and, thus, lower dose requirements (i.e., a genetic-
pharmacokinetic eect). On the other hand, VKORC1 variants
are associated with increased activity or resistance to
wararins
eects, thus requiring greater wararin dose to achieve a
similar
eect as compared to a patient with wild type VKORC1 (i.e., a
genetic-pharmacodynamic interaction).
Testing or genotype can help generate a more accurate
initial
estimate o stable wararin dosing. Routine testing or this or
other variants to help determine initial wararin dosing is
used
at some centers but remains controversial and is the subject
o an ongoing National Institutes o Healthmulticenter trial.
Pharmacogenetic wararin dosing is most oten currently
utilized
in patients who are planned in advance or impending wara-
rin initiation (e.g., joint replacement patients) because o
thecurrent turnaround time in genotype testing (several days).
In
the near uture, more rapid testing will be available, which
will
allow pharmacogenetic dosing to be utilized in a wider
variety
o patients and indications.
Case Study (continued)The man is subsequently discharged in
sinus rhythm on the
same medicines. He is asymptomatic at rest. Three weeks
later, he presents again to the emergency department in
atrial
fbrillation with rapid ventricular response. He is admitted
and
undergoes repeat cardioversion and initiation o amiodarone
to
attempt maintenance o sinus rhythm.
Discussion (continued)Several pharmacokinetic drug interactions
should be considered
when adding amiodarone in this situation. Amiodarone
inhibits
metabolism o wararin by CYP2C9. This patient is currently on
a stable dose o wararin, and addition o amiodarone would
likely increase the INR unless the wararin dose is reduced.
Typically, wararin dose is reduced by 30to 50% when
initiating
amiodarone.
Another concern is the use o simvastatin with amiodarone.
Simvastatin doses >10 mg are contraindicated in combina-
tion with amiodarone due to increased risk o myopathy rom
simvastatin.10 In this case, the interaction is due to
amiodarone
inhibition o CYP 450 3A4 metabolism o simvastatin, leading
to increased simvastatin concentrations. Interestingly, there
are
also genetic variants that appear to predispose to
statin-induced
myopathy. In the case o simvastatin, airly strong evidence
points to a polymorphism in the gene SLCOB1, which is
associ-
ated with 20% lietime risk o myopathy in patients treated
with
simvastatin.
Finally, there is an interaction between amiodarone and
digoxin.
Amiodarone is an inhibitor o P-gp, and digoxin is a substrate
o
P-gp. Thereore, addition o amiodarone to digoxin without ad-
justment would likely lead to a doubling o the patients
digoxin
level, with signifcant risk o toxic symptoms.
Case Study (continued)The patient improves and is discharged on
amiodarone. He
ollows up six months later, reports no urther episodes o
pal-
pations, and is in sinus rhythm. However, he has developed
skin
discoloration and photosensitivity, and you discontinue
amioda-
rone. You consult the electrophysiology service, who
consider
doetilide as an alternative rhythm control strategy.
Case DiscussionThe most important issue regarding the initiation
o doetilide
in this patient is the current use o hydroclorothiazide.
Hydro-
chlorothiazide is contraindicated or use with doetilide due
to
the potential or hydrochlorothiazide to increase doetilide
levels
through reduced renal secretion, as well as the potential or
hydroclorothiazide to reduce potassium levels predisposing
to
proarrhythmia. Thereore, hydrochlorothiazide would need to
be
discontinued prior to initiation o doetilide.
Key Points
Pharmacokinetics reers to all aspects o drug absorption,
transport, and metabolism, which can greatly impact
optimal dosing and drug interactions.
CYP P450 enzymes in the liver metabolize a large
proportion o medications and are a very common reason
or cardiovascular drug interactions.
-
7/27/2019 1_5 farmacocinetics
8/8
1.1.8 Chapter 1: General Principles
The actions o a medication in the body are known as
pharmacodynamic eects, and knowledge o these can aid
in avoiding toxicities and anticipating pharmacodynamic
drug interactions.
Pharmacogenetics seeks to use knowledge o genetic
variation and how it aects drug response to better target
medications.
Current clinically relevant examples o pharmacogeneticimpacts on
cardiovascular medication use include
wararin, while emerging applications include simvastatin,
clopidogrel, and beta-blockers.
References
1. Dorer-Melly J, de Jonge E, Pont AC, et al. Bioavailability o
subcu-
taneous low-molecular-weight heparin to patients on
vasopressors.Lancet 2002;359:849-50.
2. Food and Drug Administration. Drug Development and Drug
Interactions: Table o Substrates, Inhibitors and Inducers.
2009.
Available at:
http://www.da.gov/drugs/developmentapprovalpro-cess/developmentresources/druginteractionslabeling/ucm093664.
htm. Accessed 12/12/2011.
3. RH R, DR G, ML R, PH V. Digoxin. In: Evans WE, Schentag JJ,
JuskoWJ, eds. Applied Pharmacokinetics: Principles o Therapeutic
Drug
Monitoring. Vancouver, WA: Applied Therapeutics, Inc.; 1992.
4. Wilkinson GR. Drug metabolism and variability among patients
in
drug response. N Engl J Med 2005;352:2211-21.
5. Depta JP, Bhatt DL. Omeprazole and clopidogrel: Should
clinicians
be worried? Cleve Clin J Med 2010;77:113-6.
6. Evans WE, McLeod HL. Pharmacogenomicsdrug disposition,
drug
targets, and side eects. N Engl J Med 2003;348:538-49.
7. Lanear DE, McLeod HL. Pharmacogenetics: using DNA to
optimize
drug therapy. Am Fam Physician 2007;76:1179-82.
8. Weinshilboum R. Inheritance and drug response. N Engl J
Med
2003;348:529-37.
9. Lehmann H, Ryan E. The amilial incidence o low
pseudocholines-
terase level. Lancet 1956;271:124.
10. Food and Drug Administration. FDA Drug Saety Communica-tion:
Ongoing saety review o high-dose Zocor (simvastatin) and
increased risk o muscle injury. 2010. Available at:
http://www.da.
gov/Drugs/DrugSaety/PostmarketDrugSaetyInormationorPatient-sandProviders/ucm204882.htm.
Accessed 12/12/2011.
11. Shuldiner AR, OConnell JR, Bliden KP, et al. Association o
cyto-
chrome P450 2C19 genotype with the antiplatelet eect and
clini-
cal efcacy o clopidogrel therapy. JAMA 2009;302:849-57.
12. Lillvis JH, Lanear DE. Progress toward genetic tailoring o
heart
ailure therapy. Curr Opin Mol Ther 2010;12:294-304.