Embed Size (px)
Citation preview

14th Chief Risk Officer AssemblyHealth Focus
Conference Report 2018

2 Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus
Editorial
The curse of plenty – Increasing longevity, rising chronic disease and our health outlook
Our ancestors would be jealous. Most countries in the world have plenty of food; infectious diseases are well understood and policed; we better comprehend the causes of inherited illness; and ultimately we are living longer. However, an abundance of food is leading to poor dietary choices; there is the danger of complacency with infectious disease; our understanding of genetics poses as many new questions as answers; and living longer brings with it greater incidents of chronic disease, requiring increased support from the active population.
These are the curses of plenty. They are causing shifts in our risk landscape around which we must adapt and seek new solutions. These factors were discussed by a range of leading experts in the field of life and health over the two days of the 14th Chief Risk Officer Assembly. As a key player in most health care delivery systems, and with a universal interest in providing life products, insurance is at the forefront of how we manage new health challenges. It is in the interest not only of insurers, but of our wider society, that we find effective and lasting solutions to the unintended consequences of having plenty.
Patrick RaaflaubGroup Chief Risk OfficerSwiss Re

Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus 3
Table of contents
Who are the ageing and who pays for them? 4
The intergenerational inequity paradox 6
Better care at lower cost: A disruptive model of care at home 7
Quantifying and mitigating the risk of infectious disease 10
Has an obsession with lowering cholesterol been responsible for the obesity epidemic? 11
Health and wealth: The impact of Type 2 diabetes remission 12
Trend spotting and portfolio management – a different approach to managing risk 13
Antibiotic resistance: Potential risks across lines of business 14
Opioids epidemic – Casualty implications 15
Genetics: What are the promises and challenges of genetic modification? 16
Bio-ethics and regulatory paradigm shift 17
Genetic testing and anti-selection risk and implications for insurers 18
Genomic medicine and the insurance industry 19

4 Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus
Health Focus
Who are the ageing and who pays for them?
Ageing is an opportunity for insurers, driven by significant demographic shifts. There are currently around 600 million over-65 year olds in the world; that figure is estimated to grow to 1.5 billion by 2050. The distribution is not even, with the percentage in Europe anticipated to rise from 17 to 27% by 2050. Far East Asia is assessed as having the next largest percentage, followed by North America. At the same time, the age band for prime insurance consumers (30 to 49) will likely significantly decline by 2050 in most countries.
Growing elderly populations will require funding, and that funding will increasingly be self-sourced. However, in terms of the provision of products for retirement and old age, insurers currently only account for around a 5% market share. The basic needs of the over-65s require on average, in the developed world and China, USD41,000 per annum to live longer, live better and bequeath to the next generations. Insurers have the potential to increase their market share of ageing products; and this can be driven by a better, in-depth understanding of current and future customers.
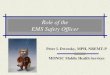
In this spirit, Swiss Re commissioned a study, ‘Who are the ageing’1, interviewing over 9,000 middle income earners from nine countries in Europe, Asia and North America, in the 35-75 age bracket. The study found that respondents’ views on ageing were conflicting and varied: individuals find themselves on two axes. One is between stability and dynamism. This measures retirees’ appetite for new adventures and hobbies against financial security and maintaining their current lifestyle. The other axis is between control and spontaneity. Some retirees favour control over timelines and finances, others make fewer plans and provisions.
Francis Blumberg, Head L&H Products Solution, Swiss Re
My vision for ageing is ...
retreat inthe nest
a time tospread wings
My
appr
oach
to p
rovi
sion
is...
prepare the nest egg
head in the sand, no plan
The Planner
The Recipient
The Entrepreneur
The Explorer

Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus 5
Our research unearthed four types of consumers: 1) the eagle, an entrepreneur, smart and independent, plans proactively and looks forward to adventures; 2) the owl, a planner, disciplined and competent, loves to plan everything and seeks stability; 3) the toucan, an explorer, idealistic and carefree, avoids any planning and just enjoys the day; 4) the ostrich, the recipient, passive and ineffective, often reactive with planning, yet hopes for stability. It became apparent from the study that those countries where state and family offer a lower proportion of financial support, a larger number of people act as planners and entrepreneurs, who are willing to plan ahead for later life.
Insurance should see itself as part of a wider ecosystem, which can enable successful ageing. The ecosystem not only includes the 3 sources of funding – society (family and state); private savings; and insurance – but also charities, technology providers and others. It is important for insurers to be relevant, including the effective use of segmentation techniques. Failure to do so will see insurers bypassed in what will be a key future market for protection.
1 www.swissre.com/library/archive/who_are_the_ageing.html

6 Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus
Health Focus
The intergenerational inequity paradoxThe demographic shift has effects across the population pyramid. Those aged 25-45 are variously described as the ‘jilted generation’ or the ‘squeezed middle’. They may well be looking after children on the one side and elderly relations on the other. They are middle or working class, cannot afford their own housing, and frequently have debt from education. They are in jobs with stagnating wages, low security, or may be working in the gig economy. These generations have little in the way of savings and are aware that public provision for pensions and social support are minimal. Their disposable income is restricted and milestones – first car, for example – are frequently delayed. These individuals can be angry, feel disenfranchised and may be prone to mental illness2.
Insurers are busy thinking how they can help retirees – can they also provide risk management solutions for these generations, a mix of late Generation X, Generation Y and the Millennials? This was a question one of the big five consultancy firms approached Swiss Re Australia with. They had noted the time lost in the work place for 25-45 year olds as a result of care and related stresses were caused by dependent children or an ageing relative.
The result was a concept called Family Care Credit. This product is structured around two pillars. The first is making services available to help employees manage their dependents – such as extra childcare help at a moment of need. The second is financial support to provide funding for care of dependent relatives without sacrificing work time; and a one-off payment to cope with a trauma occurring to dependent children.
There are other means of supporting generational resilience, potentially through insurance products. These include providing certainty around rent payments; compensating lack of wage growth through flexible solutions for gig-economy workers, improved education access; insurance solutions around retirement, including custodianship of savings; and further solutions to help manage dependencies.
Generational equity is no longer just about care of the young and the elderly – it is also about ensuring those in the middle can enjoy health, wealth and security.
2 ANZ Through Retirement consumer research completed in 2017
Bronwyn Kirwan, Head L&H Solutions Group, Swiss Re ANZ

Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus 7
Health Focus
Better care at lower cost: A disruptive model of care at homeThe market for elderly care is an expanding one; but even if it is, it still requires exceptional performance to increase from an organisation of 4 nurses, as Buurtzorg was in 2007, to 10,000 nurses a decade later. Buurtzorg has achieved this on the back of a disruptive and radical new model of elderly care.
Buurtzorg empowers local, small scale provision, caring for neighbourhoods of 5-10,000 with self-managing teams of up to 12 nurses. This provides the nurses with autonomy over all processes, which is fundamental to their job satisfaction. Neighbourhood coverage ensures low travel times and patient familiarity, as well as allowing nurses to work flexibly. For patients, the at-home care helps encourage independence and tailored solutions. On top of this service provision, Buurtzorg has built very lean management structures together with smart IT systems. Buurtzorg represents cost effective community care in close collaboration with GPs, family care givers and other support.
Key to the success of Buurtzorg is the recognition that informal structures and nursing autonomy are far more important than formal structure layers and prescribed practices. The lack of hierarchy – there are 50 support staff, 21 coaches and only two managers – encourages trust within the organisation. Smart IT systems allow the administrative load to be inputted over simplified iPad functionalities.
The result has been an alignment of stakeholders – contented nurses, contented clients and payees happy at the reduction of per patient costs. This positive combination has resulted in a number of other ‘Buurt’ or neighbourhood organisations being established. It has also allowed Buurtzorg to expand internationally, into all six continents. This requires necessary adaptation to local countries, for example, a culture of hierarchy and deference in China. The focus in Asia has been on integrated care centres in the neighbourhoods rather than stand-alone home nursing/care support.
Buurtzorg is highly relevant to all payees within the system, whether they are public sector, or, like insurers, in the private sector. It provides both an improved cost base, particularly by keeping clients in their own houses, together with better patient outcomes. Wherever Buurtzorg establishes its branches, one element remains constant: first coffee, then care. It reflects care as a tailored, human product, rather than something reduced to a commodity.
Stephan Dyckerhoff, President, Buurtzorg Neighbourhood Care Asia Ltd, Hong Kong



10 Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus
Quantifying and mitigating the risk of infectious diseaseAgeing is a problem of the modern world, so conventional wisdom has it; infectious diseases are largely a problem of the old world. Yet this assertion only holds partially true. Epidemics are constantly with us.
Epidemics primarily emerge through human interaction with animals. HIV crossed from apes, yellow fever from primates, and strains of influenza can be traced from birds and domestic animals. These can be managed partially by vaccine development; but only partially, as distribution challenges of even the most effective drug will always exist, and viruses constantly mutate. The world is currently divided into regions that can be understood as spark countries – areas where viruses can mutate and cross species – and spread countries, where significant international traffic and hub status facilitate virus profusion.
There are a number of myths about epi- and pandemics, which need exploring: Pandemics are black swan events. The reference point for pandemics is typically
the 1918 Spanish flu pandemic, a truly global phenomenon. However, more localised epidemics are constantly occurring, including more recently SARS, MERS, Zika, variations of bird flu and Ebola.
The impact of epidemics is primarily health and disease. This is to miss the fact that epidemics impose significant costs on local economies. The logistics of the foot and mouth clear up in 2001 in the UK cost around USD12 billion; while the SARS outbreak in Singapore in 2003 saw hotel occupancy rates fall by around 40% over normally expected.
Epidemics are public sector problems, and will be solved with public sector solutions. Epidemics, such as the 1957 influenza pandemic, saw a spike in worker absenteeism in public and private sector alike. Ebola epidemics in more recent years have endangered cobalt mining, one of the rare earth minerals found in a number of communications devices. The costs of supply chain disruption to this rare mineral are substantial.
Epidemics cannot be quantified or insured against. Metabiota believes epidemics can be quantified. This can be done through past data – an event catalogue, which can be built into a disease spread model, and a risk engineering layer of analysis. It can also have a forward looking component, with Metabiota running a preparedness index of countries based on a number of factors from public health through to institutional effectiveness. Swiss Re has joined forces with the World Bank and other insurers to use such quantification as the basis for a Pandemic Emergency Financing Facility.
Nathan Wolfe, Founder and Chair, Metabiota
Health Focus

Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus 11
Aseem Malhotra, Honorary Consultant Cardiologist, Lister Hospital Stevenage and ROC Private Clinic, Harley Street, London
Health Focus
Has an obsession with lowering cholesterol been responsible for the obesity epidemic?It started with a seven country study by Ancel Keys in 1970, which concluded that saturated fat and cholesterol were major drivers of heart disease. As a result, dietary advice shifted away from fats to carbohydrates, which favoured industrial food and sugar producers in particular. Despite a prevalence of low fat diets in recent decades, obesity and diabetes have both rocketed.
Clinical scientists have begun to question a continued focus on cholesterol, and the robustness of the original Keys’ findings. One study found a trial group replacing butter with lower cholesterol margarine actually increased cardiovascular mortality, suggesting that some cholesterol is actually beneficial for the heart [see Malhotra, BMJ, 10/2013]. The Cambridge Medical Research Council concluded: “current evidence does not support guidelines that restrict the consumption of saturated fats and encourage consumption of polyunsaturated fats in order to prevent heart disease.”
Equally, studies on diabetes have concluded it is of little value to focus on saturated fats; and that some saturated fats have positive health benefits. The replacement of saturated fats by sugar has been particularly detrimental.
One means of controlling blood cholesterol has been the use of statins. However, a 2013 study, published in the British Medical Journal, concluded statins had no appreciable health benefits for those with low risk of heart disease; and had significant side effects in around 20% of those taking the drug. This provoked disagreement among researchers, primarily between the University of Oxford and Harvard University. However, subsequent studies have backed the 2013 report findings, indicating the use of statins in cholesterol reduction confers no population mortality benefit; and suggests that statins have been overprescribed to millions of patients.
In the meantime, the controversy over cholesterol has meant that focus has been lost on the bigger picture, which is that obesity is rife, and that Type-2 diabetes is at epidemic proportions. The most significant single cause of these conditions is poor diet. Adopting a Mediterranean diet high in fresh vegetables, oily fish and olive oil, with moderate intake of cheese and yoghurt and minimal sugar or refined carbohydrates, confers substantial health benefits.
In the words of Christiaan Barnard, the first surgeon to undertake a heart transplant: “I have saved the lives of 150 people with heart transplantations. If I had focused on preventative medicine earlier, I would have saved 150 million.”

12 Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus
Health and wealth: The impact of Type 2 diabetes remissionDiabetes Digital Media is a data-driven empowerment platform providing the needs of the global diabetes community with academic partners. It provides its users with structured education programmes on changing their behavioural lifestyles; on supporting patients with the use of their real time data; and precision audience engagement through real world evidence and publishing research.
Central to Diabetes Digital Media is its low carbohydrate programme. Developed by Dr David Unwin, it has been rolled out in a number of countries in multiple languages. It focuses on four areas of modifiable risk: nutrition, activity, sleep, and stress. The programmes are built on the use of multiple data sources from tracking devices, setting targets, recording exercise and monitoring an array of health markers. The programme has had considerable success, with 71% continuing after a year [Saslow et al, JMIR Diabetes, dio: 10.2196/diabetes.9333]; participants losing an average of 7.4 kilos; 61% able to reduce or remove insulin; and 1 in 4 able to put their Type 2 diabetes into remission. In the UK, the programme is estimated to save the National Health Service over GBP800 per user per year in medication and treatments.
The site similarly provides guidance and tuition for medical professionals. It offers the latest in clinical evidence and expert opinion, together with e-learning modules developed together with the Royal College of General Practitioners. These e-learning programmes are presented in augmented and in virtual reality.
There is no silver bullet or magic drug in tackling a complex disease such as diabetes. Only a multi-disciplinary approach, with practical and psychological advice for those with the illness, can help us make steps against one of the great epidemics of our age.
Arjun Pensar, co-founder, diabetes.co.uk
Health Focus

Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus 13
Health Focus
Trend spotting and portfolio management – a different approach to managing riskActive asset management is based on the belief that it is possible for well managed funds to be steered and adjusted to out-perform the market. Swiss Re believes this dynamic can also be applied to the liability side of the balance sheet. Swiss Re does this in the form of a target liability portfolio.
The process begins with trend spotting, a structured, data-driven approach to understanding trends to enhance risk assessment. This trend spotting provides independent quantitative analysis which goes beyond actuarial analysis in a hypothesis driven approach. The process is designed to provide a robust systematic approach, which resists knowledge being concentrated in one individual.
One such example of this has been US commercial auto lines, in which losses deteriorated unexpectedly as a result of crashes with increased severity post 2010. On analysis, and while correlation is not causation, potential contributory trends could be identified. The recession of 2008-9 saw a fall in the volume of road haulage; and a number of experienced truckers retiring. As the economy began to recover, road haulage became more concentrated in larger vehicles; but being driven by younger drivers. The changes were subtle, but understanding them and projecting those trends can help steer the underwriting portfolio.
Once trends have been identified, Swiss Re seeks to build a forward looking view around a framework triaged by growth, risk and profitability. This then allows Swiss Re to steer its portfolio through combining past, present and future beliefs around the attractiveness of particular business lines. The portfolio is steered through adjusting risk limits and varying the distribution of available risk to underwriters. Finally, there is a process of back testing, in which previous expectations are matched with real life experience – and if there has been divergence, to understand the lessons learned.
Ashley Hirst, Head Underwriting Strategy, Swiss Re

14 Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus
Antibiotic resistance: Potential risks across lines of businessAntibiotic resistance is one of the biggest threats to global health, food security, and development today. It affects the treatment of multiple infectious conditions such as pneumonia, tuberculosis, gonorrhoea, and salmonellosis, to name a few. Antibiotic resistance occurs naturally, but misuse of antibiotics in humans and animals is accelerating the process significantly and selective pressure does its job. With antibiotic consumption rising (in particular in high growth markets), antibiotic resistance currently contributes to around 50,000 deaths in the US, the EU and 700,000 globally. Increased costs of hospitalization and health care were estimated at USD20 billion annually in the US in 20133.
Antibiotic resistance may expose insurers over a number of lines. Medical malpractice and faulty medical equipment are two of these. For example, there have been multiple reports alleging that antibiotic resistant bacteria has spread to several hundreds of patients through improperly sterilized duodenoscopes. Several of these patients had fallen seriously ill and at least two fatalities have been reported. Following a warning letter from the US Food and Drug Administration (FDA), litigation against medical device producers was initiated, which has led to multiple million awards so far.
Within agriculture, some countries appear to be using high volumes of antibiotics, which is creating bacteria that is resistant to them. One salmonella outbreak in the US caused over 600 cases of illness4.
By 2050 some estimates suggest that the deaths attributed to AMR every year might climb to 10 million, at which point it will overtake cancer as a cause of death5. Ultimately this can only be combatted by a multidisciplinary approach, including the prudent use of existing antibiotics, high standards of food processing, particularly meat, and the effective treatment of water.
3 https://amr-review.org/4 Cianflone NFC. Salmonellosis and the GI Tract: More than Just Peanut Butter. Current gastroenterology
reports. 2008;10(4):424-431.5 https://amr-review.org/
Ramiro Dip, Senior Risk Engineer P&C Centre, Swiss Re
Urs Widmer, Senior Life Guide Medical Officer, Swiss Re
Health Focus

Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus 15
Health Focus
Opioids epidemic – Casualty implicationsThe US is facing an opioid epidemic. In 2016, there were 115 deaths a day attributable to opioid overdose [all figures: The US Opioid Epidemic6, Swiss Re 2018]. This puts it on a par with the number of fatalities at the peak of HIV/AIDS epidemic of 1995. An estimated 2.1 million in 2016 had an opioid use disorder and a total of 11.5 million are estimated to have misused medication. Street opioids, most notably fentanyl and heroin, play an important role in the increasing mortality due to opioid overdose. The economic burden of the epidemic has been substantial, and estimated 2.8% of US GDP in 2015 (USD 504 billion).
The epidemic is not without substance for the insurance industry. There is a clear health angle to the epidemic, not least the mortality rises it brings with it, which is affecting longevity in the US.
A major risk for insurers also comes on the casualty side. Such a disease epidemic, particularly in the US, does not come without those seeking litigation and ultimately compensation. Hundreds of US State Attorney Generals, counties, townships, cities and municipalities have filed federal and state civil suits against all players along the opioid supply chain, from manufacturers to distributors to retailers to prescribing physicians. A number of cases have been settled but the majority of the cases have now been consolidated in a multidistrict litigation (MDL) in the Northern District of Ohio. The MDL currently holds over 700 cases, and the judge has indicated his will to move forward swiftly and will likely promote settlements.
Several of these risks could potentially fall within an insurance portfolio, affecting multiple lines of business, such as product liability, primary general liability (non-product lines), excess casualty, medical malpractice and directors and officers (D&O). It is not just the potential for losses to fall in individual lines that insurers must judge; they must also assess the cumulative potential of any losses. Issues to be resolved are whether there is personal culpability in taking opioids; whether there are multiple occurrences if a clause has been triggered; and if insured parties undertook actions that would invalidate their insurance policy.
Insurers are bracing themselves for potential losses to come. In order to limit exposure insurers can review underwriting standards, or create opioid exclusions to policies, but the effectiveness of such measures remain to be seen. In this complex and fast evolving scenario insurers must closely monitor developments. Opioid losses are likely to be long tail and highly litigious, and will be of concern to the insurance industry for many years to come.
6 http://media.swissre.com/documents/ZRH_18_01082_P1_US_Letter_Opioid.pdf
Ramiro Dip, Senior Risk Engineer P&C Centre, Swiss Re
Patrik Kneubühler, Business Steering Specialist, Swiss Re

Health Focus
Nicholas Wood, Galton Chair of Genetics, Professor of Clinical Neurology and Neurogenetics, UCL Institute of Neurology
Genetics: What are the promises and challenges of genetic modification?Dementia is a complex illness, a non-specific syndrome, which may have many causes, and a disease to which no one is immune. Its prevalence grows with age, and accounting for significant costs in developed economies. Absolute numbers are growing rapidly as the population ages. The ability to delay the onset of dementia by five years would have a significant influence on overall prevalence of the disease.
The difficulty with Alzheimer’s disease is that the causes of the condition are multiple. Genetic factors play as much of a role as environmental, which can include trauma injuries or brain infections. Moreover, by the time a dementia has become apparent, it is too late for early stage intervention, where it might be more successful. In part as a result, drug trials for dementia treatments have a low overall success rate. The diagnosis and treatment of diseases such as cancer are well ahead of neurological conditions.
There has been some success in genetic targeting of neurological disease, most notably of Huntington’s disease. There have also been successes in the genetic treatment of spinal muscular atrophy. However, other neurological conditions are harder to genetically pinpoint, as at least half of our genes contribute to the development of the nervous system.
The main challenges in understanding and treating the genetic causes of neurological disease include:
Technical: Any genetic intervention may have knock-on effects, such as over expression or influencing protein regulation. There are questions of targeting wider populations, or more sporadic sufferers; and in finding biomarkers for disease at a sufficiently early stage.
Ethical: Some will allege genetic intervention is the equivalent of playing God, as can be seen in discussions on GM foods. There may also be fear of eugenics.
Society: This will largely come in the form of costs. Treatments are expensive, as would be widespread testing or even screening programmes.

Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus 17
Session 2: Big data and the data protection challenge
Bio-ethics and regulatory paradigm shiftOur approach to using genomic analysis has gone from being excited with the sequencing of the first genome, to being disappointed that it revealed few secrets, to becoming more productive as we take steps in understanding our complex genetic structures. Where we are now is that genetic data is cheap, good and plenty. The cost of a full genome sequencing is around USD1,000.
This opens the door to precision, personalised medicine – but the revolution has been some time in coming. This is down to the inevitably long journey through drug research and trials to final treatments; and in the fundamental principles of genetics. Within the principles of genetics, there are a handful of Mendelian conditions, including certain breast cancers, cystic fibrosis and Huntington’s disease, which are associated with specific points on the genome. Such conditions are low in the frequency, but with a high likelihood of illness where genetic mutations exist. Most genetic diseases are, however, polygenic in their nature, a complex interaction of genetic mutations frequent within the population, but less commonly resulting in illness.
The use of genetic data faces many regulatory challenges. Significantly, there is the use of consumer as opposed to physician use of genetic tests. Up until now, direct-to-consumer genetic tests have focused largely on lifestyle factors and genetic heritage. In 2015, however, the FDA first approved the use of genetic tests in determining illnesses. In 2018 the FDA approved the use of direct-to-consumer products for medical tests, including breast cancer risk. Tests have to pass the FDA’s level of clinical and analytical validity; and the customer must be cognizant of the limitations of the test. That does raise the potential of information asymmetry. This should not, however, be overplayed. The first stop after an adverse test is likely to be the physician, at which point the condition would appear on medical records.
There are further ethical issues to genetic data. The first is ownership of genetic data; and a second, can individuals be forced to share genetic data. Some states, including Canada, enforce a ban against the use of genetic data in underwriting; others have selective access; and some have no restrictions. Genetic data is different from other health data: it affects not only the individual, but family members and descendants; there is no choice around genetic inheritance; and it has a history of misuse. There are likely to be tensions around the use of genetic data for some time to come.
Larry Brody, Senior Investigator Medical Genomics and Metabolic Genetics Branch and Director, National Human Genome Research Institute at the National Institutes of Health
Health Focus

18 Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus
Health Focus
Genetic testing, anti-selection risk and implications for insurersGenetic testing looks for alterations in a person’s genes or chromosomes to identify heritable or acquired mutations related to disease and health. It can occur at a number of points, from new born screening, to predictive and diagnostic testing, nutrigenomic and pharmacogenetic testing, direct-to-consumer testing and liquid biopsies. All this has been supported by declining costs of genetic testing, so that sequencing a genome could come down to USD100 in the foreseeable future. As a result, recent years have seen a steady growth in clinical genetic testing of 20% or more annually.
The number of firms offering genetic tests to consumers has similarly expanded. One important segment is the direct-to-consumer (DTC) market, the leader of which is 23andMe. It offers a range of services, from ancestry, trait and wellness analysis through to carrier status and genetic health risk. Around 15% of US consumers are estimated to have had a genetic test, about two-thirds at the request of a physician and one-third through DTC providers, whereby the latter see massive growth rates. At least half of consumers are open to taking a genetic test in the future as prices drop; most to satisfy personal curiosity but half wants to know more about potential disease risk.
The use of genetic information in insurance underwriting varies from no regulation/self-regulation (Japan, Australia, China, India, South Africa, US (life insurance)) to a legal ban (Canada, France, Poland, Portugal, US (health insurance)). The majority of developed economies allow use of family history in underwriting; although family history questions provide limited value in fully assessing genetic risk and protecting against adverse-selection from genetic testing. As there is increasing predictive value from genetic testing, non-disclosure of risk-relevant genetic information is of concern for insurers.
This cocktail of growing genetic data, better understanding of the data, and increasingly restrictive regulatory systems has increased the danger of adverse-selection, driven by an information asymmetry between applicants and insurers. Applicants in many states do not have to disclose genetic data to their insurers, which might have a significant bearing on their future health condition. Studies suggest that individuals aware of their high risk for certain genetic conditions are more likely to purchase insurance or extend existing coverage. Actuarial studies across the globe have shown that the impact of such adverse-selection from genetic testing is substantial and can threaten the sensitive balance between the financial viability of certain insurance products and fair premium rates for consumers.
Swiss Re constantly monitors and models these developments. A full report on the risks of adverse-selection from genetic testing can be found here: http://media.swissre.com/documents/Genetics_Seeing_the_future.pdf
Florian Rechfeld, Senior Research Analyst, L&H, Swiss Re

Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus 19
Genomic medicine and the insurance industryEpigenetics is the adaptive response system of our genome to deal with environmental exposure. Whilst our genetics carry the blueprint, biology – influenced by a range of factors, from diet to exercise, stress and social interaction – will influence the expression of that blueprint. DNA methylation is one of three distinct epigenetic mechanisms; and as such, DNA methylation can be used as an indicator to monitor gene activity. Methylation can influence conditions such as the predisposition of obesity in individuals. If DNA methylation serves as a biomarker for obesity/diabetes disease progression, it begs the question: Will the insurance industry start incentivising healthy behaviour and measure outcome by epigenetic monitoring?
DNA methylation can be used as an ageing marker. Spreading of DNA methylation on the DNA corresponds to biological age, according to Horvarth (2013). There is much speculation that a variety of factors, including dietary restrictions and telomere modification, may create longevity enhancement. A number of companies are researching these, including understanding how epigenetics can be employed. Altering epigenetics may be able to extend life expectancy. Will the insurance industry start using epigenetic patterns in underwriting to determine the “real” age?
Liquid biopsy is a new cancer monitoring tool to guide personalised cancer therapy approaches. Liquid biopsy is a fast and easy blood test, which allows for the frequent monitoring of somatic mutations acquired by an evolving cancer. Used as a cancer screening tool, liquid biopsy has the potential to lead to over-diagnosis and impact cancer products. There has been evidence of this in Korea around thyroid cancer screening, which had an impact on critical illness claims. Will cancer diagnostic definitions change due to new molecular profiles and will critical illness claims definitions withstand?
Gene editing approaches are the big hope for cancer cure. The development of CRISPR technology has allowed cheap and precise gene editing techniques. Gene editing may contribute to the development of immunology, whereby T-cells are reprogrammed to recognise cancer cells as invasive and activate an immune response. However, there are potential risks in CRISPR, for example developing new diseases or even modified organisms that may have environmental impact. Indeed, there may be risk in success, in that there may be an insurance impact in mortality gains. Will the insurance industry provide a solution to costly gene therapy approaches or is it too risky?
Christoph Nabholz, Head R&D Life and Health, Swiss Re
Health Focus


Swiss Re Institute 14th Chief Risk Officer Assembly - Health Focus 21


© 2018 Swiss Re. All rights reserved.
Publisher: Swiss Re Institute
Author: Simon Woodward
Photography: David Ausserhofer
Design: Corporate Real Estate&Logistics/ Media Production, Zurich
The entire content of this publication is subject to copyright with all rights reserved. The information may be used for private or internal purposes, provided that any copyright or other proprietary notices are not removed. Electronic reuse of the data published in this publication is prohibited.
Reproduction in whole or in part or use for any public purpose is permitted only with the prior written approval of Swiss Re Institute, and if the source reference is indicated. Courtesy copies are appreciated.
This publication is for information purposes only. It does not constitute any recommendation, advice, solicitation, offer or commitment to effect any transaction or to conclude any legal act of any kind whatsoever. Any views or opinions expressed in this publication are solely those of the respective speakers and do not necessarily represent those of Swiss Re, in particular in any relation to any ongoing or future dispute. Anyone shall at its own risk interpret and employ this publication without relying on it in isolation. Although all the information used in this publication was taken from reliable sources, Swiss Re does not accept any responsibility for the accuracy or comprehensiveness of the information given or forward looking statements made. In no event will Swiss Re or one of its affiliates be liable for any loss or damages of any kind, including any direct, indirect or consequential damages, arising out of or in connection with the use of this publication and readers are cautioned not to place undue reliance on forward-looking statements. Swiss Re undertakes no obligation to publicly revise or update any forward-looking statements, whether as a result of new information, future events or otherwise.

Swiss Re Management Ltd. Swiss Re Institute Mythenquai 50/60 P.O. Box 8022 Zurich Switzerland
Telephone +41 43 285 2551 institute.swissre.com
©2018 Swiss Re. All rights reserved.
10/18, en