Embed Size (px)
Citation preview
ABSTRACT: Endodontically treated grossly destructed teeth when left untreated for a long
period of time may cause supraeruption, drifting, tipping, and rotation of adjacent and opposing
teeth. This may be challenging to the restorative dentist, when fabricating a crown because of
inadequate interocclusal space. This case report describes a simple technique to restore an
endodontically treated mandibular second premolar with the loss of coronal tooth structure and
lack of interocclusal space. The mandibular second premolar had a single root canal and was
endodontically treated. The opposing upper premolar had supraerupted results in reducing the
interocclusal space. A minimally invasive and esthetic technique was used to restore the tooth
with limited interocclusal clearance. In such cases additional retention and support of the
restoration are difficult to achieve. Richmond crown (post-core & crown as a single unit) give
this additional amount of retention & support and proves to be very promising in long term. In this
article we have discussed a case report showing successful restoration of functionally &
structurally compromised endodontically treated posterior tooth with Richmond crown.
1 2 3Rajashekar Sangur, Achyut Sinha, Neha Sonali Massey1 2,3Professor & Head, Post Graduate Student Department of Prosthodontics, Rama Dental College Hospital & Research Centre , Kanpur
INTRODUCTION : Root canal therapy cannot be
summarized by saying, “fill it, shut it, forget it”. The final
restoration over an endodontically treated tooth is as
important or probably even more important than the actual
root canal therapy itself. The main aim of endodontics and
restorative dentistry is to retain the natural teeth with maximal
function and pleasing esthetics.
Endodontically treated teeth are more prone to fractures than
the vital teeth. Fracture occurrence is more in posterior teeth
than anterior teeth as the masticatory forces are higher and
teeth are weaker.[1] The endodontically treated tooth has got
an impaired neurosensory feed- back mechanism because of
the lack of pulpal tissue i.e. the protective property of
'proprioception' is lost. This renders the tooth more vulnerable
to fracture under normal masticatory forces. So, a person can
un-intentionally bite too hard on the RC treated tooth
compared to a vital tooth, which can lead to its fracture and
failure. An accountable percentage of structural integrity is
lost because of the root canal therapy itself due to access
cavity preparation and canal instrumentation leading to
increased flexing of the tooth and ultimately its fracture.
Some authors quote an alteration in the composition of the
dentin such as a change in the collagen cross linking,
dehydration etc. weakening the tooth structure which can also
lead to increase chances of fracture of an endodontically
treated tooth.
Endodontically treated teeth with the loss of coronal tooth
structure when left untreated for a long period may cause
supraeruption, drifting, tipping, rotation of neighboring and
opposing teeth. This may be challenging to the clinician,
when fabricating a restoration because of lack of interocclusal
space. Many methods have been advocated for treatment of
localized loss of space such as minor tooth movement,
reducing the opposing teeth, elective root canal treatment and
restoration with post retained restorations or combination of
two or more of the above.[2] All these methods of gaining
TREATING AN ENDODONTICALLY TREATED PREMOLAR WITH LIMITED INTEROCCLUSAL CLEARANCE USING RICHMOND CROWN : A CASE REPORT
Keywords:
Limited interocclusal
clearance, Richmond
crown, endodontic treated
tooth, cast post.
Source of support: Nil
Conflict of interest: Nil
Journal of Dental Sciences
University
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 62
University J Dent Scie 2017; No. 3, Vol. 1
CaseReport
space require removal of healthy tooth structure and are time
consuming.
Wherever remaining crown structure is insufficient to retain
full coverage crown then post and core is necessary means to
increase retention and resistance form of tooth.[3,4]
However, post and core procedure can give rise to
complications such as dislodgement of assembly, fracture of
post/root, loss of restorative seal and periodontal injury.[5-8]
Such situations further get complicated when there is limited
interocclusal clearance in posterior teeth; as occlusal forces
are maximum and core reduction should be adequate to
provide indicated thickness for metal ceramic crown to
achieve desirable esthetics. Richmond crown is best indicated
solution in such conditions.
The Richmond crown was introduced in 1878 and
incorporated a threaded tube in the canal with a screw retained
crown. It was later modified to eliminate the threaded tube
and was redesigned as a one piece dowel and crown.[9] It is
easier to make cast metal restorations with the aid of posts for
retention and lasting service for limited interocclusal
clearance cases. However, whenever possible, the metal can
be camouflaged by veneering with tooth-colored restorations.
The aim of this case report is to describe a simple and
minimally invasive technique to restore an endodontically
treated tooth with limited interocclusal space.
CASE REPORT : A female patient aged 46 years reported
to the Department of Prosthodontics, with the chief complaint
of dislodgement of crown in lower left back tooth region.
On intra-oral examination, it was observed that the tooth 35
was root canal treated with very little crown structure
remaining to hold the crown. Tooth 36 was also root canal
treated. (PHOTOGRAPH 1)
Inter arch space was not enough for the conventional post and
core and thus it was planned to prepare RICHMOND
CROWN for tooth 35 and a conventional porcelain fused to
metal crown for the tooth 36 .
PHOTOGRAPH 1: PRE OPERATIVE
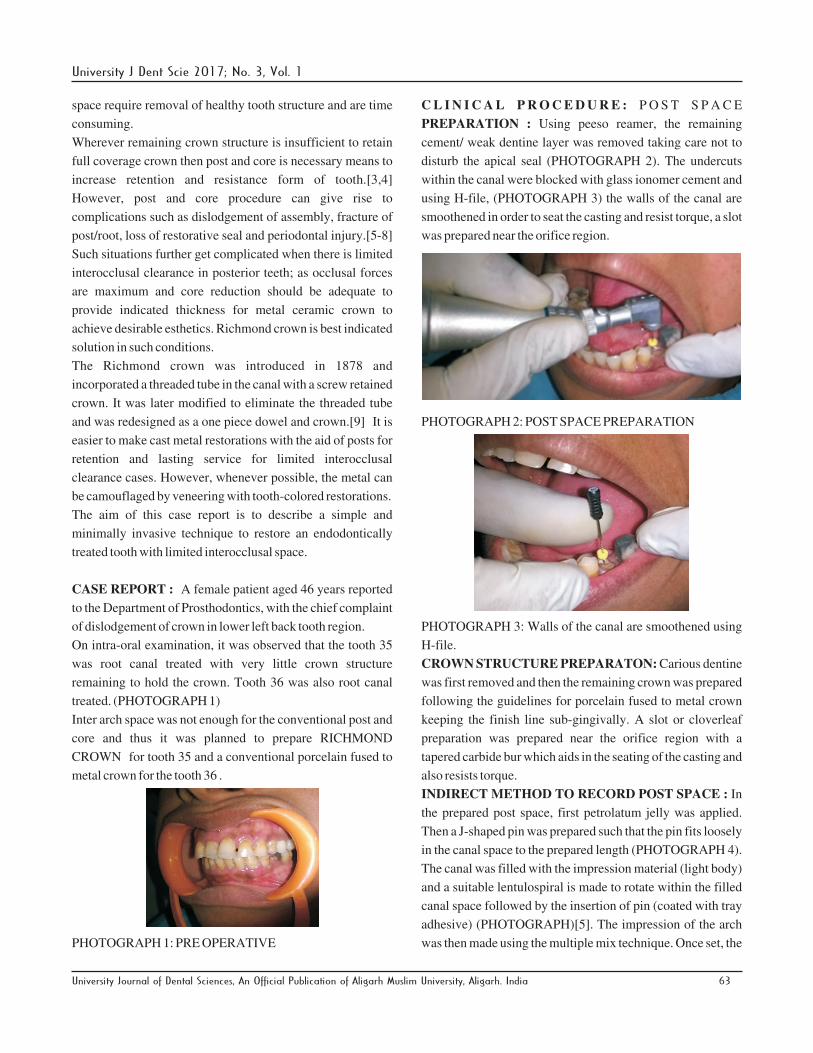
C L I N I C A L P R O C E D U R E : P O S T S P A C E
PREPARATION : Using peeso reamer, the remaining
cement/ weak dentine layer was removed taking care not to
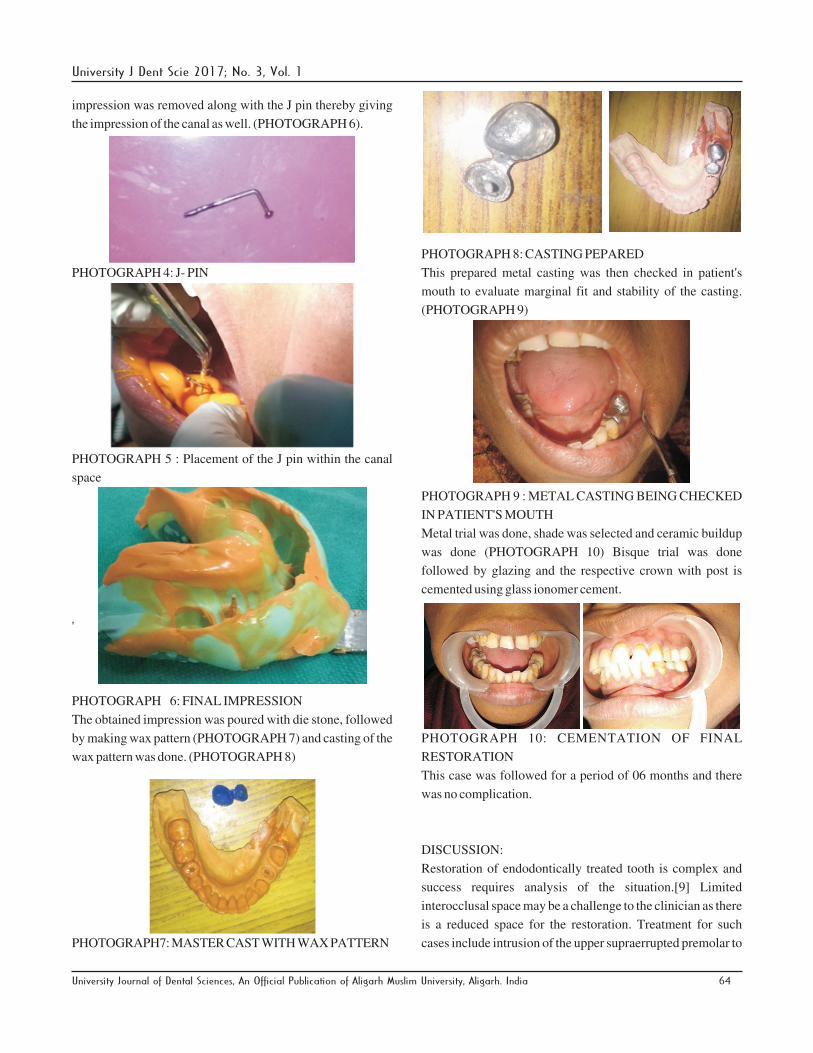
disturb the apical seal (PHOTOGRAPH 2). The undercuts
within the canal were blocked with glass ionomer cement and
using H-file, (PHOTOGRAPH 3) the walls of the canal are
smoothened in order to seat the casting and resist torque, a slot
was prepared near the orifice region.
PHOTOGRAPH 2: POST SPACE PREPARATION
PHOTOGRAPH 3: Walls of the canal are smoothened using
H-file.
CROWN STRUCTURE PREPARATON: Carious dentine
was first removed and then the remaining crown was prepared
following the guidelines for porcelain fused to metal crown
keeping the finish line sub-gingivally. A slot or cloverleaf
preparation was prepared near the orifice region with a
tapered carbide bur which aids in the seating of the casting and
also resists torque.
INDIRECT METHOD TO RECORD POST SPACE : In
the prepared post space, first petrolatum jelly was applied.
Then a J-shaped pin was prepared such that the pin fits loosely
in the canal space to the prepared length (PHOTOGRAPH 4).
The canal was filled with the impression material (light body)
and a suitable lentulospiral is made to rotate within the filled
canal space followed by the insertion of pin (coated with tray
adhesive) (PHOTOGRAPH)[5]. The impression of the arch
was then made using the multiple mix technique. Once set, the
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 63
University J Dent Scie 2017; No. 3, Vol. 1
impression was removed along with the J pin thereby giving
the impression of the canal as well. (PHOTOGRAPH 6).
PHOTOGRAPH 4: J- PIN
PHOTOGRAPH 5 : Placement of the J pin within the canal
space
'
PHOTOGRAPH 6: FINAL IMPRESSION
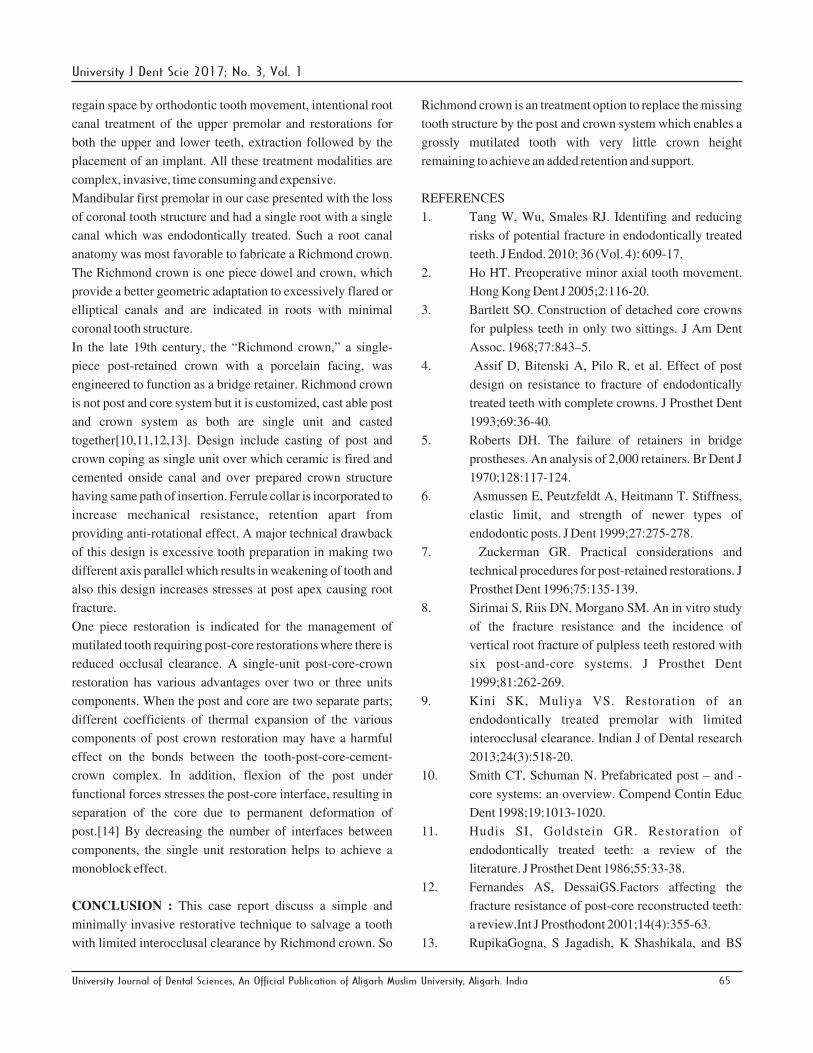
The obtained impression was poured with die stone, followed
by making wax pattern (PHOTOGRAPH 7) and casting of the
wax pattern was done. (PHOTOGRAPH 8)
PHOTOGRAPH7: MASTER CAST WITH WAX PATTERN
PHOTOGRAPH 8: CASTING PEPARED
This prepared metal casting was then checked in patient's
mouth to evaluate marginal fit and stability of the casting.
(PHOTOGRAPH 9)
PHOTOGRAPH 9 : METAL CASTING BEING CHECKED
IN PATIENT'S MOUTH
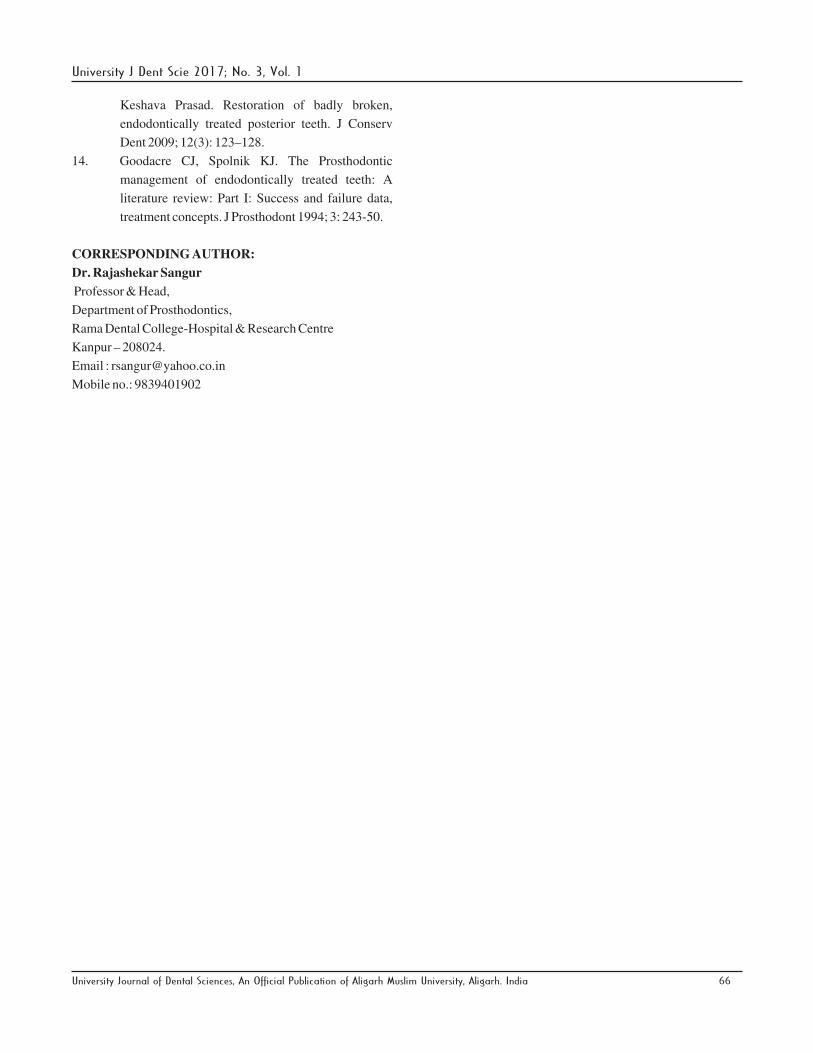
Metal trial was done, shade was selected and ceramic buildup
was done (PHOTOGRAPH 10) Bisque trial was done
followed by glazing and the respective crown with post is
cemented using glass ionomer cement.
PHOTOGRAPH 10: CEMENTATION OF FINAL
RESTORATION
This case was followed for a period of 06 months and there
was no complication.
DISCUSSION:
Restoration of endodontically treated tooth is complex and
success requires analysis of the situation.[9] Limited
interocclusal space may be a challenge to the clinician as there
is a reduced space for the restoration. Treatment for such
cases include intrusion of the upper supraerrupted premolar to
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 64
University J Dent Scie 2017; No. 3, Vol. 1
regain space by orthodontic tooth movement, intentional root
canal treatment of the upper premolar and restorations for
both the upper and lower teeth, extraction followed by the
placement of an implant. All these treatment modalities are
complex, invasive, time consuming and expensive.
Mandibular first premolar in our case presented with the loss
of coronal tooth structure and had a single root with a single
canal which was endodontically treated. Such a root canal
anatomy was most favorable to fabricate a Richmond crown.
The Richmond crown is one piece dowel and crown, which
provide a better geometric adaptation to excessively flared or
elliptical canals and are indicated in roots with minimal
coronal tooth structure.
In the late 19th century, the “Richmond crown,” a single-
piece post-retained crown with a porcelain facing, was
engineered to function as a bridge retainer. Richmond crown
is not post and core system but it is customized, cast able post
and crown system as both are single unit and casted
together[10,11,12,13]. Design include casting of post and
crown coping as single unit over which ceramic is fired and
cemented onside canal and over prepared crown structure
having same path of insertion. Ferrule collar is incorporated to
increase mechanical resistance, retention apart from
providing anti-rotational effect. A major technical drawback
of this design is excessive tooth preparation in making two
different axis parallel which results in weakening of tooth and
also this design increases stresses at post apex causing root
fracture.
One piece restoration is indicated for the management of
mutilated tooth requiring post-core restorations where there is
reduced occlusal clearance. A single-unit post-core-crown
restoration has various advantages over two or three units
components. When the post and core are two separate parts;
different coefficients of thermal expansion of the various
components of post crown restoration may have a harmful
effect on the bonds between the tooth-post-core-cement-
crown complex. In addition, flexion of the post under
functional forces stresses the post-core interface, resulting in
separation of the core due to permanent deformation of
post.[14] By decreasing the number of interfaces between
components, the single unit restoration helps to achieve a
monoblock effect.
CONCLUSION : This case report discuss a simple and
minimally invasive restorative technique to salvage a tooth
with limited interocclusal clearance by Richmond crown. So
Richmond crown is an treatment option to replace the missing
tooth structure by the post and crown system which enables a
grossly mutilated tooth with very little crown height
remaining to achieve an added retention and support.
REFERENCES
1. Tang W, Wu, Smales RJ. Identifing and reducing
risks of potential fracture in endodontically treated
teeth. J Endod. 2010; 36 (Vol. 4): 609-17.
2. Ho HT. Preoperative minor axial tooth movement.
Hong Kong Dent J 2005;2:116-20.
3. Bartlett SO. Construction of detached core crowns
for pulpless teeth in only two sittings. J Am Dent
Assoc. 1968;77:843–5.
4. Assif D, Bitenski A, Pilo R, et al. Effect of post
design on resistance to fracture of endodontically
treated teeth with complete crowns. J Prosthet Dent
1993;69:36-40.
5. Roberts DH. The failure of retainers in bridge
prostheses. An analysis of 2,000 retainers. Br Dent J
1970;128:117-124.
6. Asmussen E, Peutzfeldt A, Heitmann T. Stiffness,
elastic limit, and strength of newer types of
endodontic posts. J Dent 1999;27:275-278.
7. Zuckerman GR. Practical considerations and
technical procedures for post-retained restorations. J
Prosthet Dent 1996;75:135-139.
8. Sirimai S, Riis DN, Morgano SM. An in vitro study
of the fracture resistance and the incidence of
vertical root fracture of pulpless teeth restored with
six post-and-core systems. J Prosthet Dent
1999;81:262-269.
9. Kini SK, Muliya VS. Restoration of an
endodontically treated premolar with limited
interocclusal clearance. Indian J of Dental research
2013;24(3):518-20.
10. Smith CT, Schuman N. Prefabricated post – and -
core systems: an overview. Compend Contin Educ
Dent 1998;19:1013-1020.
11. Hudis SI, Goldstein GR. Restoration of
endodontically treated teeth: a review of the
literature. J Prosthet Dent 1986;55:33-38.
12. Fernandes AS, DessaiGS.Factors affecting the
fracture resistance of post-core reconstructed teeth:
a review.Int J Prosthodont 2001;14(4):355-63.
13. RupikaGogna, S Jagadish, K Shashikala, and BS
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 65
University J Dent Scie 2017; No. 3, Vol. 1
Keshava Prasad. Restoration of badly broken,
endodontically treated posterior teeth. J Conserv
Dent 2009; 12(3): 123–128.
14. Goodacre CJ, Spolnik KJ. The Prosthodontic
management of endodontically treated teeth: A
literature review: Part I: Success and failure data,
treatment concepts. J Prosthodont 1994; 3: 243-50.
CORRESPONDING AUTHOR:
Dr. Rajashekar Sangur
Professor & Head,
Department of Prosthodontics,
Rama Dental College-Hospital & Research Centre
Kanpur – 208024.
Email : [email protected]
Mobile no.: 9839401902
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 66
University J Dent Scie 2017; No. 3, Vol. 1