Embed Size (px)
Citation preview

Mr Bala
http://tinyurl.com/
clinicalcases3

AKI & CKD
NigelFong

Practical approach to AKI
1. Is this AKI (vs CKD)?2. What is (are) the causes?3. What are the complications?4. Is dialysis emergent?

Scenario – Q1
Mr Bala is a 67-year old Indian gentleman. One month ago, he was diagnosed with type 2 diabetes, hypertension, and hyperlipidemia, after presenting to the polyclinic with osmotic symptoms. On diagnosis his HbA1c was 9.2%, and he was found to have retinopathy and peripheral neuropathy. He was started on losartan, atorvastatin, metformin, and glipizide. Two weeks ago he complained of muscle aches and saw a GP, who prescribed etoricoxib (arcoxia) with good relief.
He presents to the A&E with non-specific complaints of lethargy and malaise for the past week. In the past 2 days he has also become more breathless. You look through the bloods done in A&E and notice that the creatinine is 340 (eGFR 15) …

Scenario - Q1
Q1. Regarding Mr Bala’s Acute Kidney Injury (AKI), all of the following are correct EXCEPT (Choose 2 of 7)• Mr Bala may not have AKI.• Oliguria conveys a worse prognosis for renal recovery.• Mr Bala’s diabetes does not predispose him to AKI.• A rise in creatinine is expected after initiation of candesartan
and may not constitute AKI.• Unlike COX-1 (traditional) NSAIDs, COX-2 NSAIDs are less
likely to cause AKI.• In identifying the etiology of AKI, an abdominal examination
is critical.• A urine formed element microscopy (UFEME) may reveal
muddy brown granular casts

Scenario - Q1
Q1. Regarding Mr Bala’s Acute Kidney Injury (AKI), all of the following are correct EXCEPT (Choose 2 of 7)• Mr Bala may not have AKI.• Oliguria conveys a worse prognosis for renal recovery.• Mr Bala’s diabetes does not predisposes him to AKI.• A rise in creatinine is expected after initiation of candesartan
and may not constitute AKI.• Unlike COX-1 (traditional) NSAIDs, COX-2 NSAIDs are less
likely to cause AKI.• In identifying the etiology of AKI, an abdominal examination
is critical.• A urine formed element microscopy (UFEME) may reveal
muddy brown granular casts

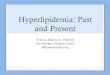
Staging of AKI

Scenario - Q1
Q1. Regarding Mr Bala’s Acute Kidney Injury (AKI), all of the following are correct EXCEPT (Choose 2 of 7)• Mr Bala may not have AKI.• Oliguria conveys a worse prognosis for renal recovery.• Mr Bala’s diabetes does not predisposes him to AKI.• A rise in creatinine is expected after initiation of candesartan
and may not constitute AKI.• Unlike COX-1 (traditional) NSAIDs, COX-2 NSAIDs are less
likely to cause AKI.• In identifying the etiology of AKI, an abdominal examination
is critical.• A urine formed element microscopy (UFEME) may reveal
muddy brown granular casts

Etiology

EtiologyAKI CKD
Prerenal HypotensionIntravascular hypovolemia(includingthirdspacing)
Renalarterystenosis
Thirdspacing– e.g.CCF(cardiorenal),cirrhosis(hepatorenal)
Renal Acutetubularnecrosis>Ischaemia,drugs,toxinsGlomerulonephritisMicroangiopathiese,g,TTP/HUSAcuteinterstitialnephritisOthers
DMHTNGlomerulonephritisVasculitisPolycystickidneyOtherinterstitial
Postrenal
Urinaryobstruction,acute Urinaryobstruction,chronic
CKDpredisposestoAKI;AKIacceleratesCKDprogression

Practical approach to AKI
1. Is this AKI (vs CKD)?2. What is (are) the causes?
• Look at the vitals chart and clinical hx• Look at the medication list• Examine hydration status• Palpating for bladder / inserting IDC• Looking at the urea / creatinine ratio• UFEME +/- phase contrast microscopy• US kidneys• Urinary protein excretion• Renal biopsy
3. What are the complications?4. Is dialysis emergent?

Scenario - Q1
Q1. Regarding Mr Bala’s Acute Kidney Injury (AKI), all of the following are correct EXCEPT (Choose 2 of 7)• Mr Bala may not have AKI.• Oliguria conveys a worse prognosis for renal recovery.• Mr Bala’s diabetes does not predisposes him to AKI.• A rise in creatinine is expected after initiation of candesartan
and may not constitute AKI.• Unlike COX-1 (traditional) NSAIDs, COX-2 NSAIDs are less
likely to cause AKI.• In identifying the etiology of AKI, an abdominal examination
is critical.• A urine formed element microscopy (UFEME) may reveal
muddy brown granular casts

Scenario – Q2
Q2. Which of the following, if present, BEST suggests a diagnosis of acute kidney injury over chronic kidney disease? (Choose 2 of 7)• Patient with fatigue and pruritus for the past 3 months• Well patient incidentally discovers elevated creatinine during
health screening• Blood tests: Hb 9.7, MCV 85.6, Fe sat 19%, Ferritin 287• Blood tests: Hb 9.7, low platelets, low haptoglobin, LDH, and
bilirubin.• Blood tests: Hb 9.7, calcium 3.5, and new vertebral fracture.• Ultrasound scan showing a normal kidney• Bland urinary sediment

Practical approach to AKI
1. Is this AKI (vs CKD)?• Baseline creatinine• Renal ultrasound: size, parenchymal echogenicity• Long-term complications of CKD
> Anaemia> Mineral bone disease
• Symptom duration or overt precipitant for AKI
2. What is (are) the causes?3. What are the complications?4. Is dialysis emergent?

Scenario – Q2
Q2. Which of the following, if present, BEST suggests a diagnosis of acute kidney injury over chronic kidney disease? (Choose 2 of 7)• Patient with fatigue and pruritus for the past 3 months• Well patient incidentally discovers elevated creatinine during
health screening• Blood tests: Hb 9.7, MCV 85.6, Fe sat 19%, Ferritin 287• Blood tests: Hb 9.7, low platelets, low haptoglobin, LDH, and
bilirubin.• Blood tests: Hb 9.7, calcium 3.5, and new vertebral fracture.• Ultrasound scan showing a normal kidney• Bland urinary sediment

Scenario – Q3
You look through Mr Bala’s records and discover that at last month’s polyclinic visit, his creatinine was 163 (eGFR 37). On examination, he is breathless, requiring oxygen (2L nasal prongs), with bilateral pitting edema and basal lung crackles.
Available investigations are:• Hb 8.7 , TW 12, Plt 320• Urea 23, Cr 340, Na 136, K 6.2, HCO3 14, Cl 105, Glucose
7.0

Scenario – Q3
Q3. All of the following will be helpful for Mr Bala EXCEPT (Choose 2 of 7):• Serial cardiac enzymes• IV calcium gluconate• IV hydration• IV furosemide• SC actrapid 10 units• Suspend losartan• Renal ultrasound scan

Scenario – Q3
Q3. All of the following will be helpful for Mr Bala EXCEPT (Choose 2 of 7):• Serial cardiac enzymes• IV calcium gluconate• IV hydration• IV furosemide• SC actrapid 10 units• Suspend losartan• Renal ultrasound scan

Scenario – Q4
Mr Bala is diuresed and his hyperkalaemia is corrected. He remains afebrile and blood pressure is stable, but he fails to pass any urine despite a total of 160mg furosemide boluses. The next morning, he becomes confused and increasingly breathless. His oxygen requirement has gone up to 8L via face mask.
Repeat investigations reveal:- Troponin 85 – 97 – 79- pH 7.13, pO2 103, pCO2 32- Urea 30, Cr 400, Na 132, K 5.6, HCO3 7, Cl 100- Calcium / Phosphate / Magnesium unremarkable.

Scenario – Q4
Q4. The BEST management for Mr Bala is (Choose 1 of 5):• Add IV albumin to IV furosemide• Change IV furosemide to an infusion, titrated to maintain
SBP >90 mmHg• IV sodium bicarbonate infusion• Insertion of femoral vascular catheter and hemodialysis• Intubation and ventilation

Scenario – Q4
Q4. The BEST management for Mr Bala is (Choose 1 of 5):• Add IV albumin to IV furosemide• Change IV furosemide to an infusion, titrated to maintain
SBP >90 mmHg• IV sodium bicarbonate infusion• Insertion of femoral vascular catheter and hemodialysis• Intubation and ventilation

Indications for urgent dialysis• A Severe acidosis• E Electrolytes: hyperK refractory to medical Rx• I Intoxication with dialysable toxin• O Overload: refractory pulmonary edema• U Uremia: uremic encephalopathy, pericarditis

Scenario – Q5
Mr Bala undergoes one session of slow low efficiency dialysis in high dependency and is thereafter able to wean off oxygen. His subsequent renal panels are:• 4h post dialysis: Cr 262, Na 139, K 3.6, HCO3 15, Cl 96• Next morning: Cr 250, Na 142, K 3.9, HCO3 14, Cl 97• Following am: Cr 241, Na 138, K 4.0, HCO3 17, Cl 97
He is transferred out of high dependency.

Scenario – Q5
Q5. Regarding Mr Bala’s subsequent progress and management, which of the following statements is FALSE? (Choose 1 in 5)• Creatinine may never return to baseline• Over the next few days, Mr Bala may develop hypernatremia• Over the next few days, Mr Bala may develop hypokalaemia• Candesartan should not be restarted, regardless of
creatinine level• The temporary dialysis catheter should be removed.

Scenario – Q5
Q5. Regarding Mr Bala’s subsequent progress and management, which of the following statements is FALSE? (Choose 1 in 5)• Creatinine may never return to baseline• Over the next few days, Mr Bala may develop hypernatremia• Over the next few days, Mr Bala may develop hypokalaemia• Candesartan should not be restarted, regardless of
creatinine level• The temporary dialysis catheter should be removed.

Management of AKI
Oliguric phase • Remove inciting agent (sepsis, toxin, etc)• Supportive management especially that for complications
Polyuric phase• Balance I/O• Correct electrolyte losses
Recovery phase• But creatinine may never return to baseline

Practical approach to CKD
1. How bad is the CKD?2. Why does this patient have CKD?3. How can I retard disease progression?4. What complications do I have to manage?5. Is it time to start renal replacement therapy?6. If on RRT, what are the issues with RRT?7. What are the comorbids?

Practical approach to CKD


Practical approach to CKD
1. How bad is the CKD?2. Why does this patient have CKD?

Practical approach to CKD
1. How bad is the CKD?2. Why does this patient have CKD?3. How can I retard disease progression?
• Treat the cause• Inhibit proteinuria• Avoid further insults
4. What complications do I have to manage?5. Is it time to start renal replacement therapy?6. If on RRT, what are the issues with RRT?7. What are the comorbids?

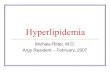
ThecrucialroleofACEinhibition

Scenario – Q6
Over the new few days, Mr Bala receives IV hydration and electrolyte corrections. His vascular catheter is removed and he is discharged.
At his follow up visit 2-weeks after discharge, he is well and back to his usual daily activities with good effort tolerance. BP is 160/93, HR 79, SpO2 97% on room air. He has slight pedal edema. Laboratory results are:

Scenario – Q6
BP is 160/93, HR 79, SpO2 97% on room air. He has slight pedal edema. Laboratory results are:• Hb 8.3, Ferritin 200 ng/ml, transferrin saturation 18%• Cr 201 (GFR 28), Urea 16, Na 134, K 4.5, Cl 105, HCO3 14• cCa 2.1 (2.1-2.4), PO4 1.80 (0.9-1.5), vit D 23 ng/nmol, iPTH
29.5 (1-6)• Urine protein/creatinine ratio 1.7 g/g (= proteinuric)• US: shrunken kidney, loss of norm parenchymal echogenicity• HbA1c 8.5%
Meds: PO losartan 50mg OM, PO atorvastatin 40mg ON, PO metformin 500mg BD, PO glipizide 5mg BD

Scenario – Q6Q6. All of the following medication changes should be made at THIS visit EXCEPT (Choose 3 in 10): • Increase metformin to 850mg BD• Increase PO glipizide to 10mg BD• Add PO furosemide 40mg OM • Add PO calcium acetate 667mg TDS• Add PO alphacalcidol (“one alpha”) 0.25mcg 3 times a week• Add PO cholecalciferol 1000 unit OM• Add PO sodium bicarbonate 500mg TDS• Add PO nifedipine LA 30mg OM• Add PO ferrous fumarate 400mg BD• Add SC recormon (recombinant erythropoietin) 4000 units
alternate weeks

Practical approach to CKD
1. How bad is the CKD?2. Why does this patient have CKD?3. How can I retard disease progression?4. What complications do I have to manage?
• A: Anaemia• B: Blood pressure• C: Calcium / Phosphate• D: Vitamin D / PTH / Bone disease• E: Electrolytes - Hyperkalaemia
- Acidosis • F: Fluid overload
5. Is it time to start renal replacement therapy?6. If on RRT, what are the issues with RRT?7. What are the comorbids?

Anaemia in CKD
• Anemia in CKD should be investigated before concluding that it is due to renal disease alone.
• Target Hb: 10-11.5 (avoid <9 or >13)
Management1. Ensure adequate iron stores – PO or IV
(Aim ferritin >500, transferrin saturation >30%)2. Prescribe erythropoietin stimulating agent
Beware risks: HTN, risk of thrombolic event

Blood pressure in CKD
• Most guidelines: aim <140/90 (KDIGO guideline: <130/80 for proteinuric CKD)
Management1. Use an ACE/ARB 2. Adjust dry weight3. Add antihypertensives as needed to meet target

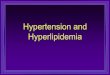
Ca/PO4 / Bone disease in CKD
• Pathophysiology

Ca/PO4 / Bone disease in CKD
• Importance: phosphate is a modifiable risk factor in vasculopathy and cardiovascular death.
Management: stepwise1. Bring down the phosphate
- Diet: phosphate restriction- Phosphate binder
> Calcium-based initially> Non-calcium based if hypercalcemia
2. When phosphate controlled, supplement vitamin D

Ca/PO4 / Bone disease in CKD
Management: stepwise1. Bring down the phosphate2. When phosphate controlled, supplement vitamin D
• Need an activated form of vitamin D.• Note the difference between
> Ergocalciferol / cholecalciferol> One alpha calcidol --- the one for CKD> Calcitriol

Ca/PO4 / Bone disease in CKD
Management: stepwise1. Bring down the phosphate2. When phosphate controlled, supplement vitamin D3. If becomes hypercalcaemic, patient may have developed
tertiary hyperparathyroidism. Options:- Cinacalcet- Parathyroidectomy.

Electrolytes & Fluid in CKD
Hyperkalaemia• Diet• Resonium
Acidosis: • Usually NAGMA initially, then NAGMA + HAGMA• Associated with mortality• Give sodium bicarbonate tab to keep bicarb in normal range
Fluid status:• Fluid restrict• Furosemide

Other tasks in CKD
• Look through all medications: doses often need to be changed
• Treat comorbids• Psychosocial support

Scenario – Q6
BP is 160/93, HR 79, SpO2 97% on room air. He has slight pedal edema. Laboratory results are:• Hb 8.3, Ferritin 200 ng/ml, transferrin saturation 18%• Cr 201 (GFR 28), Urea 16, Na 134, K 4.5, Cl 105, HCO3 14• cCa 2.1 (2.1-2.4), PO4 1.80 (0.9-1.5), vit D 23 ng/nmol, iPTH
29.5 (1-6)• Urine protein/creatinine ratio 1.7 g/g (= proteinuric)• US: shrunken kidney, loss of norm parenchymal echogenicity• HbA1c 8.5%
Meds: PO losartan 50mg OM, PO atorvastatin 40mg ON, PO metformin 500mg BD, PO glipizide 5mg BD

Scenario – Q6Q6. All of the following medication changes should be made at THIS visit EXCEPT: • Increase metformin to 850mg BD• Increase PO glipizide to 10mg BD• Add PO furosemide 40mg OM • Add PO calcium acetate 667mg TDS• Add PO alphacalcidol (“one alpha”) 0.25mcg 3 times a week• Add PO cholecalciferol 1000 unit OM• Add PO sodium bicarbonate 500mg TDS• Add PO nifedipine LA 30mg OM• Add PO ferrous fumarate 400mg BD• Add SC recormon (recombinant erythropoietin) 4000 units
alternate weeks

Scenario – Q7
Over the next 3 years, he suffers another 2 episodes of acute kidney injury, both precipitated by infections. He also complains of a change in bowel habit, and is discovered to have T3N1M0 colon cancer for which he undergoes an open right hemicolectomy. His creatinine has increased gradually to 342 (GFR 15) and he feels generally lethargic. Despite furosemide doses of 80mg TDS, he still has bilateral pedal edema but is not dyspneic. He remains normokalaemic.
Mr Bala is counselled for dialysis initiation.

Scenario – Q7
Q7. With regards to dialysis initiation, which of the following options is BEST for Mr Bala? (Choose 1 in 5)• He should be offered peritoneal dialysis, which better
preserves residual urine output• He should be considered for renal transplant.• A tunneled catheter (permcath) should be inserted for urgent
dialysis initiation• He should be referred for early vascular access creation,
and hemodialysis initiated thereafter.• He should receive an arteriovenous graft as first-choice
vascular access.

Practical approach to CKD
1. How bad is the CKD?2. Why does this patient have CKD?3. How can I retard disease progression?4. What complications do I have to manage?5. Is it time to start renal replacement therapy?
• Hemodialysis• Peritoneal dialysis• Transplant
6. If on RRT, what are the issues with RRT?7. What are the comorbids?

Renal replacement therapy
Hemodialysis• Types: HD, SLED, CRRT• Access – permanent: AVF (RC, BC, BB)
AVG- temporary: Permcath
Vascath
Peritoneal dialysis• Types: Continuous ambulatory PD
Automated (night) PD• Access: Insertion of tenckoff catheter

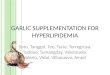
Renal replacement therapy
APD
CAPD

Renal replacement therapy

Renal replacement therapy
Complications• Adequacy of dialysis• Access issues• Infection
- Line / access sepsis- PD peritonitis
• Intra-dialysis issues: e.g. hypotension, angina, disequilibrium

Scenario – Q7
Q7. With regards to dialysis initiation, which of the following options is BEST for Mr Bala?• He should be offered peritoneal dialysis, which better
preserves residual urine output• He should be considered for renal transplant.• A tunneled catheter (permcath) should be inserted for urgent
dialysis initiation• He should be referred for early vascular access creation,
and hemodialysis initiated thereafter.• He should receive an arteriovenous graft as first-choice
vascular access.

Practical approach to AKI
1. Is this AKI (vs CKD)?2. What is (are) the causes?3. What are the complications?4. Is dialysis emergent?

Practical approach to CKD
1. How bad is the CKD?2. Why does this patient have CKD?3. How can I retard disease progression?4. What complications do I have to manage?
• A: Anaemia• B: Blood pressure• C: Calcium / Phosphate• D: Vitamin D / PTH / Bone disease• E: Electrolytes - Hyperkalaemia
- Acidosis • F: Fluid overload
5. Is it time to start renal replacement therapy?6. If on RRT, what are the issues with RRT?7. What are the comorbids?