Embed Size (px)
Citation preview
12/9/2014
1
Slide 1JSOMTC, SWMG(A)
Field Treatment of the Biological CasualtyPFN: SOMEML13
Slide 2JSOMTC, SWMG(A)
Terminal Learning Objective
Action: Communicate knowledge of field treatment of the biological casualty
Condition: Given a lecture in a classroom environment
Standard: Received a minimum score of 75% on the written exam IAW course standards
Slide 3JSOMTC, SWMG(A)
Reason
12/9/2014
2
Slide 4JSOMTC, SWMG(A)
Agenda
Identify the historical aspects of biological agents used in warfare
Identify the availability, advantages, disadvantages and delivery modes of biological agents
Identify the characteristics, clinical presentation, and treatment of bacterial biological agents
Slide 5JSOMTC, SWMG(A)
Agenda
Identify the characteristics, clinical presentation, and treatment of viral biological agents
Identify the characteristics, clinical presentation, and treatment of toxin producing biological agents
Identify the characteristics and types of biological agent vaccines
Slide 6JSOMTC, SWMG(A)
Agenda
Identify the characteristics and types of biological agent protective equipment
Identify evacuation concerns for biological agent casualties
12/9/2014
3
Slide 7JSOMTC, SWMG(A)
Historical Aspects of Biological Agents Used in Warfare
Slide 8JSOMTC, SWMG(A)
Biological Warfare
Definition
The intentional use of microorganisms or toxins derived from living organisms to produce death or disease in humans, animals or plants
Types of agents
Bacteria
Viruses
Toxins
Slide 9JSOMTC, SWMG(A)
Biological Warfare
What makes an agent effective?
Pathogenicity and virulence
Infectious dose
Pathogen stability
• Aerosol
• Environment
Susceptibility of target object
12/9/2014
4
Slide 10JSOMTC, SWMG(A)
Biological Warfare History
184 BC
Hannibal
14th Century
Plague at Kaffa
18th Century
European conquest of the Americas
1937 to 1945
China
Slide 11JSOMTC, SWMG(A)
Biological Warfare History
1943
USA BIO program established
1953
USA Defensive program established
1969
USA Offensive program disestablished
1979
The Sverdlovsk Incident
Slide 12JSOMTC, SWMG(A)
Chemical versus Biological Agents
Chemical agents are typically man made through the use of industrial chemical processes
Biological agents are either replicating agents (bacteria or virus) or nonreplicating materials (toxin) that can be produced by living organisms
Almost none of the biological agents are dermally active and none are volatile
12/9/2014
5
Slide 13JSOMTC, SWMG(A)
Availability, Advantages, Disadvantages and Delivery Modes
of Biological Agents
Slide 14JSOMTC, SWMG(A)
Availability of Biological Agents
International Biological Warfare Agreements
1925 Geneva Protocol prohibits use, but not research
1969 President Nixon renounces U.S. program
Slide 15JSOMTC, SWMG(A)
Availability of Biological Agents
1972 Biological Weapons Convention
103 nations agree to never to develop, produce stockpile, acquire or retain any biological agent for other than peaceful purposes
Facilitate the exchange of equipment materials and information on use of biological agents for peaceful purposes
12/9/2014
6
Slide 16JSOMTC, SWMG(A)
Availability of Biological Agents
U.S. Biological Weapons Policy
No use under any circumstances
Research limited to defense measures
We possess no weaponized biologicals
Previous weapons stocks were destroyed
Slide 17JSOMTC, SWMG(A)
Advantages of Biological Weapons
Agents easy to produce
Inexpensive to produce
Can disseminate at great distances
Agent’s cloud invisible
Detection quite difficult
First sign is illness
Overwhelms medical capabilities
Perpetrators escape before effects
Simple threats create panic
Slide 18JSOMTC, SWMG(A)
Disadvantages of Biological Weapons
Most agents are poor tactical weapons on the modern battlefield
Agents have incubation times of several days to weeks
Countered by a rapid developing battlefield
Delayed‐onset may be the intent
• Fixed positions
12/9/2014
7
Slide 19JSOMTC, SWMG(A)
Modes of Delivery
Biological warfare agents are unconventional weapons and can be delivered by unconventional means
Conventional explosive munitions are inefficient delivery systems for agents
Heat generated
Unpredictable size of particulate matter
Approximately 1% to 2% delivered
Slide 20JSOMTC, SWMG(A)
Modes of Delivery
Slide 21JSOMTC, SWMG(A)
Modes of Delivery
Agents are most effectively delivered as an aerosol
Particles of 1 to 5 microns in diameter are most effective
Larger particles get trapped in the upper airways (filtered out)
Biological warfare agents may be used to
contaminate food or water systems/supplies
Cooking decreases contamination
Standard chlorination and filtration inactivate most pathogens
12/9/2014
8
Slide 22JSOMTC, SWMG(A)
Modes of Delivery
Agents are most effectively delivered as an aerosol
Particles of 1 to 5 microns in diameter are most effective
Larger particles get trapped in the upper airways (filtered out
Agents may also be used in food or water supplies
Limited populace affected
Slide 23JSOMTC, SWMG(A)
Modes of Delivery
Slide 24JSOMTC, SWMG(A)
Characteristics, Clinical Presentation, and Treatment of
Bacterial Biological Agents
12/9/2014
9
Slide 25JSOMTC, SWMG(A)
Bacterial Biological Agents
Anthrax
Brucellosis
Plague
Many others!
Slide 26JSOMTC, SWMG(A)
Anthrax
Slide 27JSOMTC, SWMG(A)
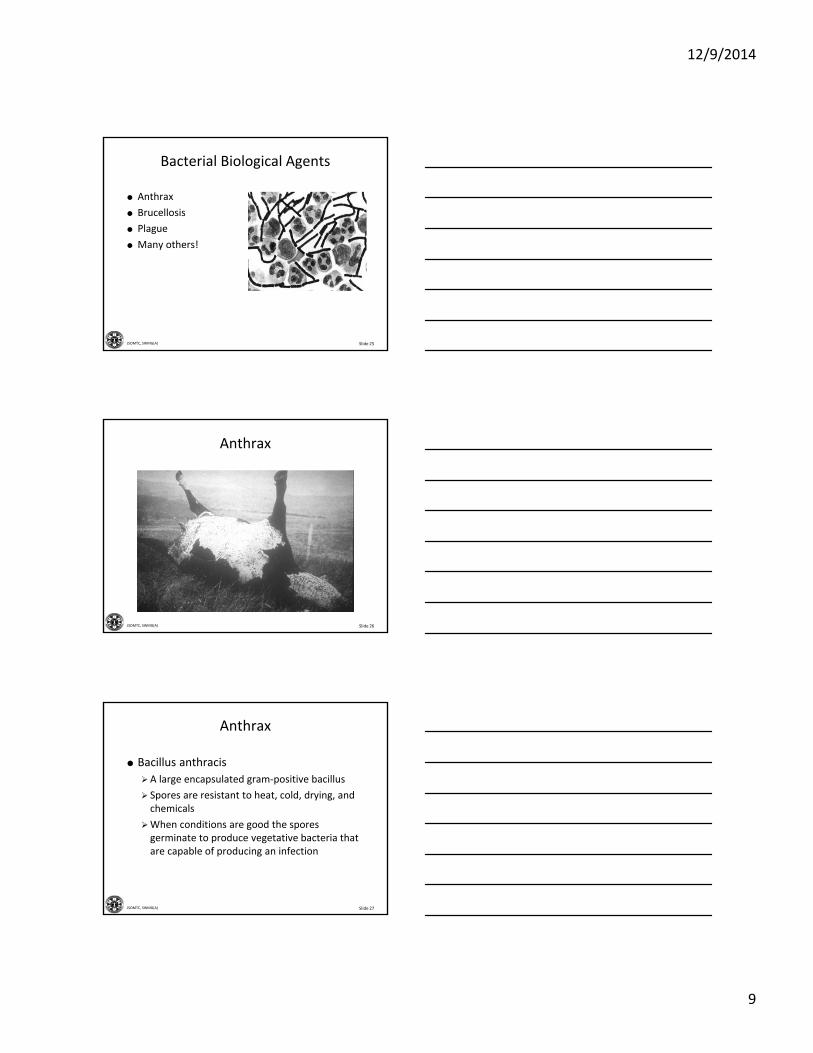
Anthrax
Bacillus anthracis
A large encapsulated gram‐positive bacillus
Spores are resistant to heat, cold, drying, and chemicals
When conditions are good the spores germinate to produce vegetative bacteria that are capable of producing an infection
12/9/2014
10
Slide 28JSOMTC, SWMG(A)
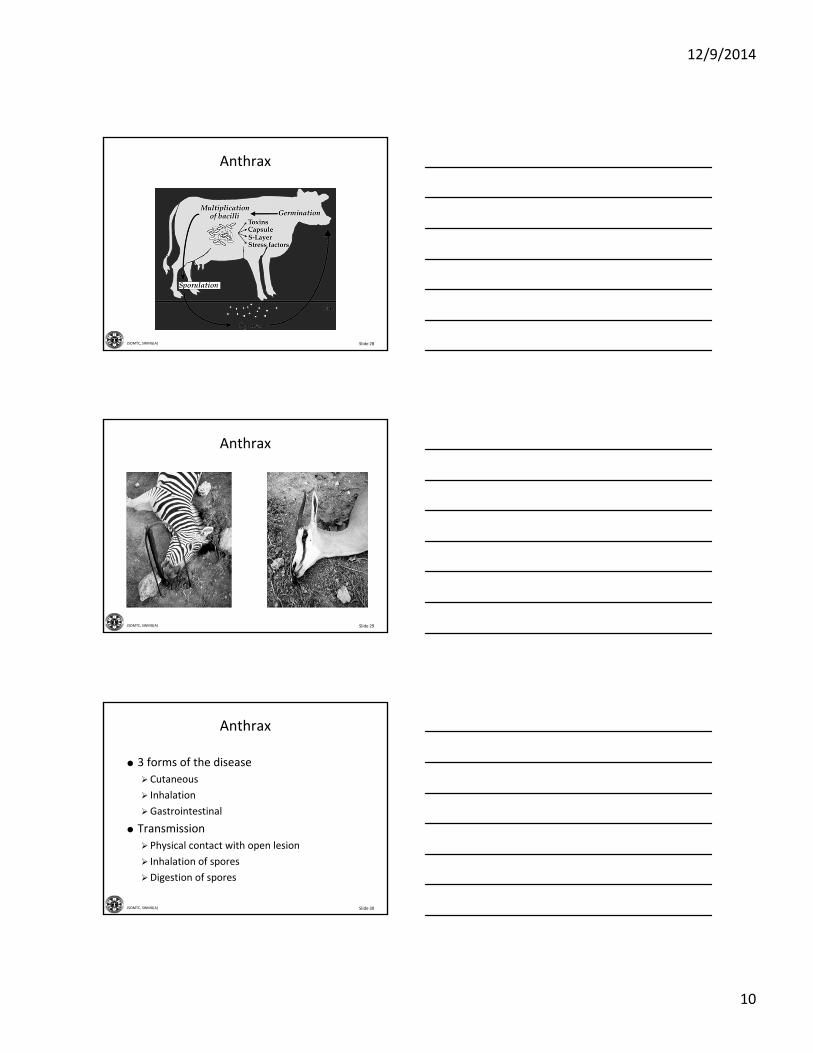
Anthrax
Slide 29JSOMTC, SWMG(A)
Anthrax
Slide 30JSOMTC, SWMG(A)
Anthrax
3 forms of the disease
Cutaneous
Inhalation
Gastrointestinal
Transmission
Physical contact with open lesion
Inhalation of spores
Digestion of spores
12/9/2014
11
Slide 31JSOMTC, SWMG(A)
Cutaneous Anthrax
95% of all anthrax infections
Occupational exposure to animals
Onset
1 to 7 days
Affects
Head, neck, and extremities
Slide 32JSOMTC, SWMG(A)
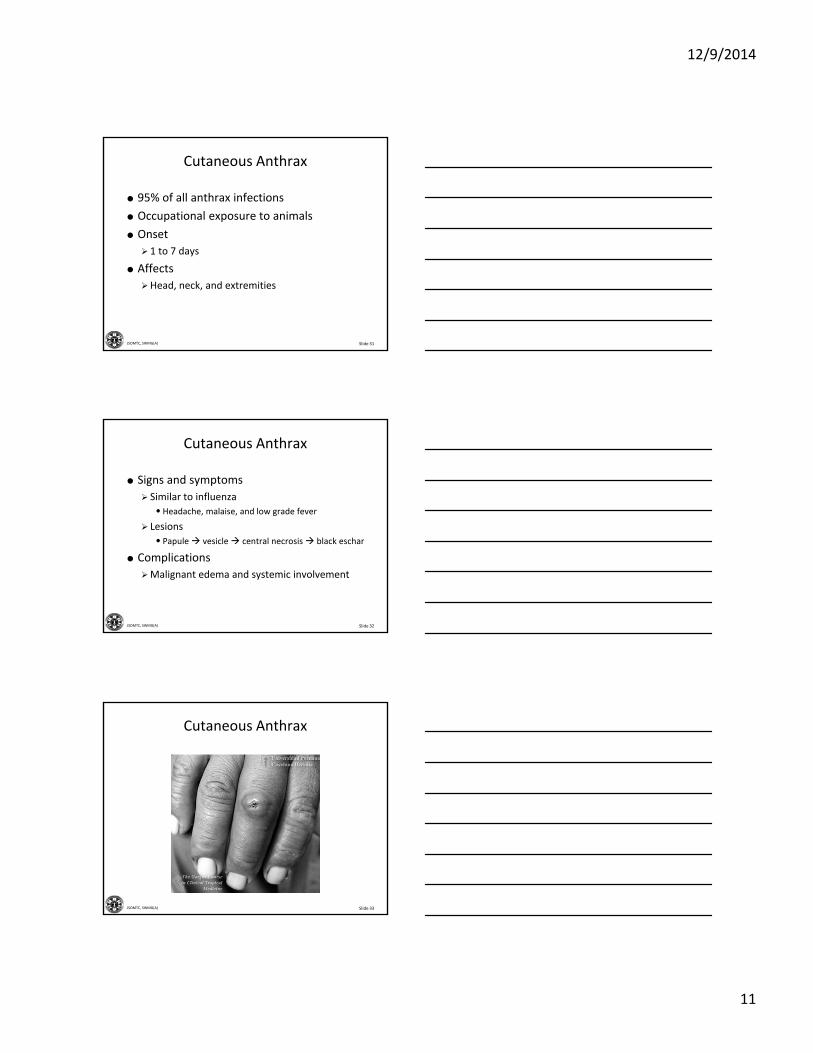
Cutaneous Anthrax
Signs and symptoms
Similar to influenza
• Headache, malaise, and low grade fever
Lesions
• Papule vesicle central necrosis black eschar
Complications
Malignant edema and systemic involvement
Slide 33JSOMTC, SWMG(A)
Cutaneous Anthrax
12/9/2014
12
Slide 34JSOMTC, SWMG(A)
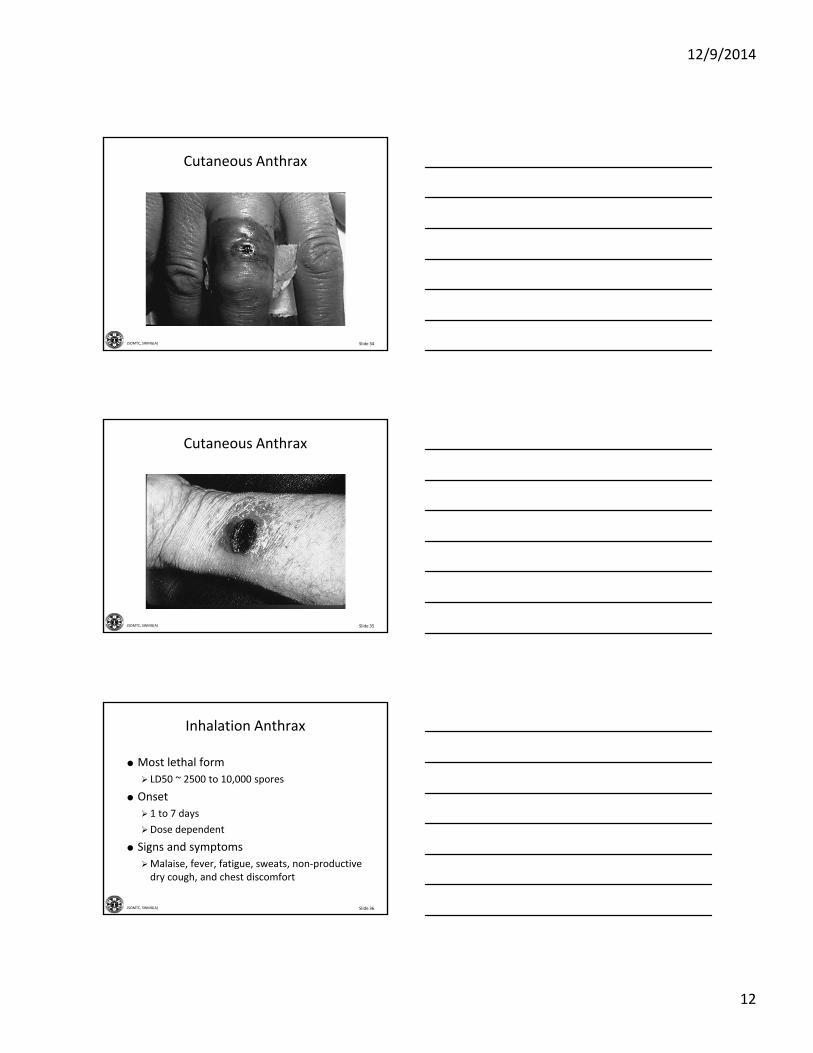
Cutaneous Anthrax
Slide 35JSOMTC, SWMG(A)
Cutaneous Anthrax
Slide 36JSOMTC, SWMG(A)
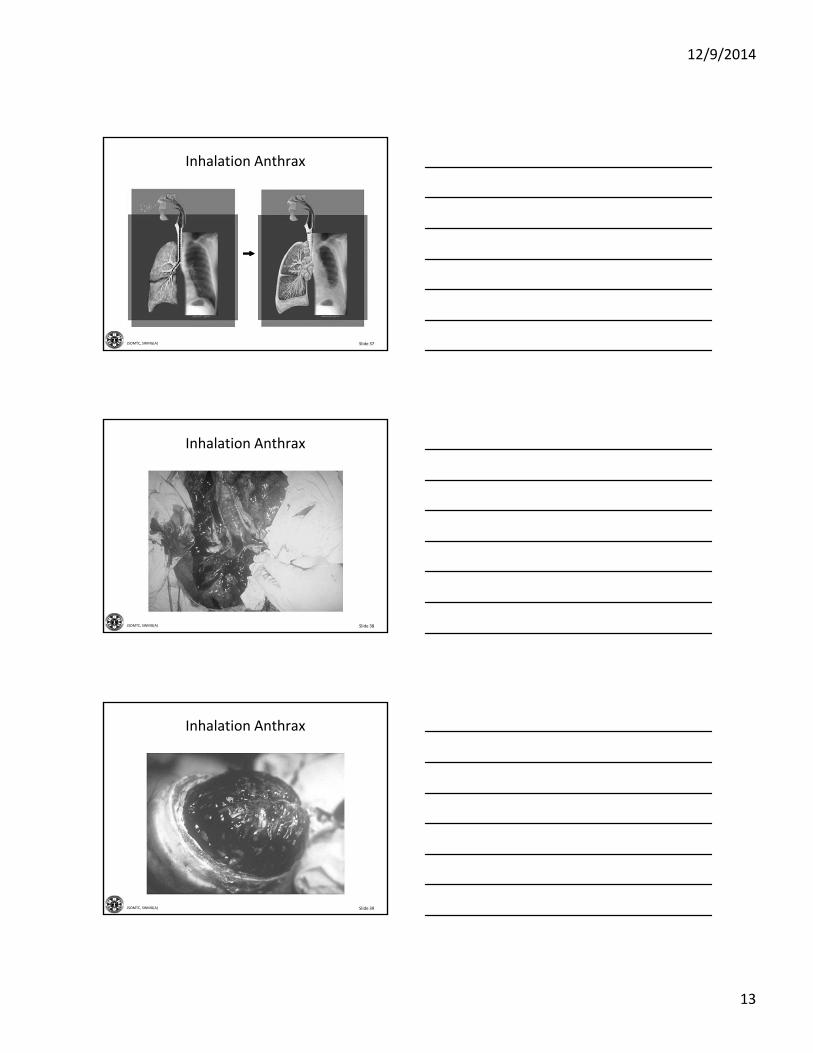
Inhalation Anthrax
Most lethal form
LD50 ~ 2500 to 10,000 spores
Onset
1 to 7 days
Dose dependent
Signs and symptoms
Malaise, fever, fatigue, sweats, non‐productive dry cough, and chest discomfort
12/9/2014
13
Slide 37JSOMTC, SWMG(A)
Inhalation Anthrax
Slide 38JSOMTC, SWMG(A)
Inhalation Anthrax
Slide 39JSOMTC, SWMG(A)
Inhalation Anthrax
12/9/2014
14
Slide 40JSOMTC, SWMG(A)
Brucellosis
Brucella abortus(cattle), B.suis (pigs), B. canis(dogs)
Gram negative coccobacilli
Aerobic, non‐motile
Slow growing pathogen
Slide 41JSOMTC, SWMG(A)
Brucellosis
Primarily found in sheep, goats, cattle, swine, and camels
Also infects bison, elk, caribou, and some species of deer
Produced in the laboratory for biological warfare purposes using a single cell or a small amount of the organism from natural sources
Slide 42JSOMTC, SWMG(A)
Brucellosis
Transmission
Inhalation of aerosols or dust that contain organisms
Ingestion of unpasteurized dairy products and contaminated meat
Inoculation of abraded skin or mucosal surfaces
12/9/2014
15
Slide 43JSOMTC, SWMG(A)
Brucellosis
Onset
May be sudden or insidious
5 to 60 days
Signs and symptoms
Fluctuating fevers, sweating, weakness, anemia, headache, and muscular pain
Incapacitating and disabling disease in humans
Slide 44JSOMTC, SWMG(A)
Plague
Yersina pestis
Gram negative bacillus
Slide 45JSOMTC, SWMG(A)
Plague
3 forms
Bubonic
Pneumonic
Septicemic
Transmission
Man to man is through coughing (droplets)
Respiratory transmission is enhanced by humid climates
Primary reservoir is rodents, domestic cats, and wild carnivores
12/9/2014
16
Slide 46JSOMTC, SWMG(A)
Plague
Slide 47JSOMTC, SWMG(A)
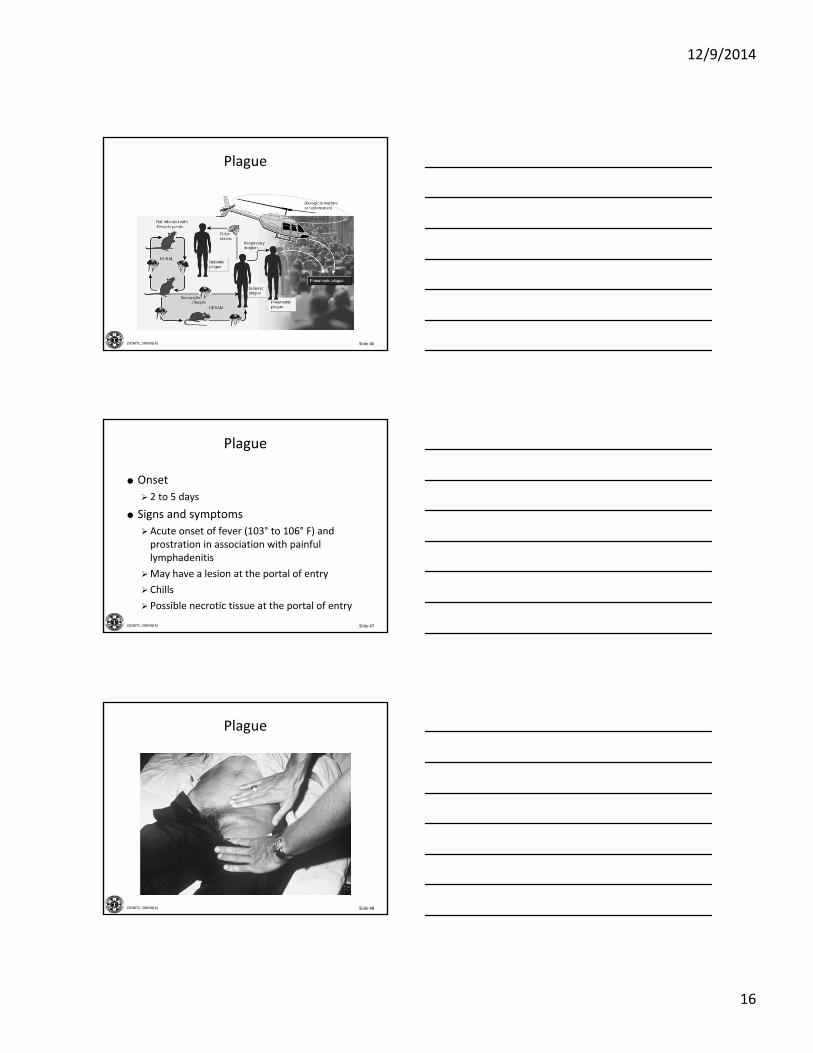
Plague
Onset
2 to 5 days
Signs and symptoms
Acute onset of fever (103° to 106° F) and prostration in association with painful lymphadenitis
May have a lesion at the portal of entry
Chills
Possible necrotic tissue at the portal of entry
Slide 48JSOMTC, SWMG(A)
Plague
12/9/2014
17
Slide 49JSOMTC, SWMG(A)
Plague
Slide 50JSOMTC, SWMG(A)
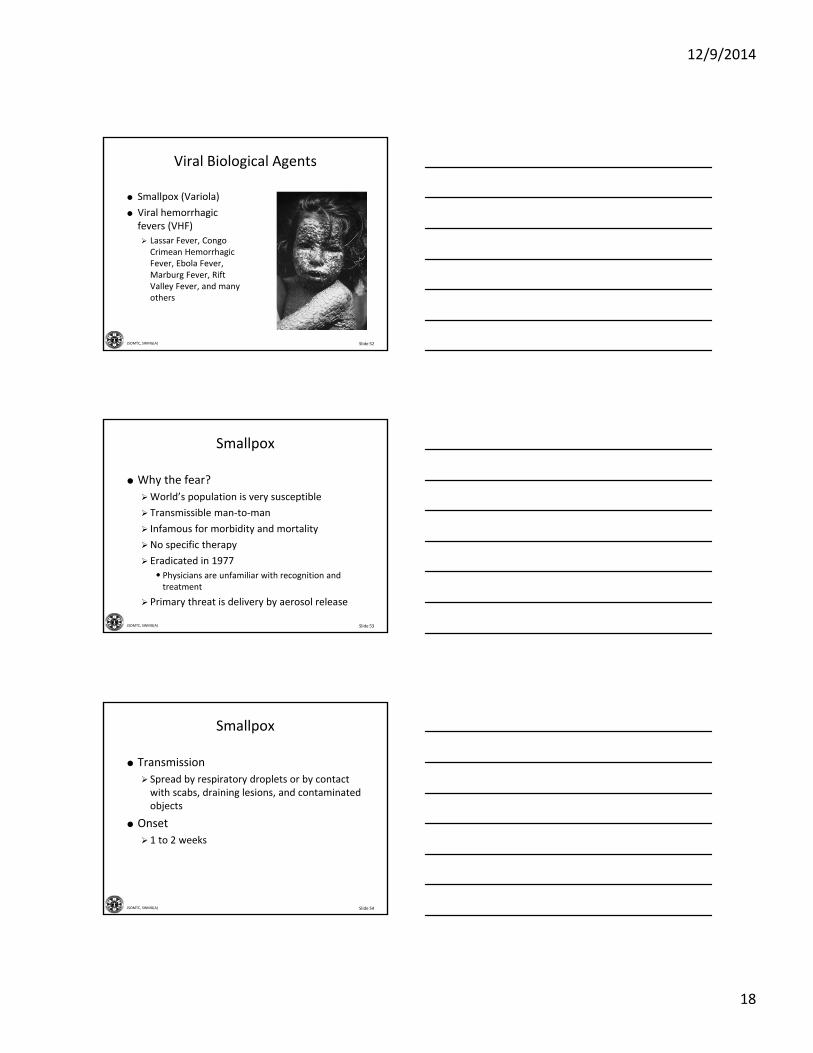
Bacterial Agent Treatment
Anthrax (Inhalation)
(Cutaneous)
1‐6 days Fever/chills, malaise, fatigue, cough,
Papule, fluid filled
vesicle black eschar
Aerosol
Direct
Cipro, Doxy, then PCN
Same as Inhalation
Brucellosis 1‐2 months Fever/chills, HA, malaise, myalgia
Aerosol Doxy + Rifam
Plague (Inhalation)
2‐3 days Fever/chills, HA, hemoptysis, toximia, Resp failure
Aerosol Cipro, Doxy (IV) then PO after improvement
Agent Onset Symptoms Mode Treatment
Slide 51JSOMTC, SWMG(A)
Characteristics, Clinical Presentation, and Treatment of Viral
Biological Agents
12/9/2014
18
Slide 52JSOMTC, SWMG(A)
Viral Biological Agents
Smallpox (Variola)
Viral hemorrhagic fevers (VHF)
Lassar Fever, Congo Crimean Hemorrhagic Fever, Ebola Fever, Marburg Fever, Rift Valley Fever, and many others
Slide 53JSOMTC, SWMG(A)
Smallpox
Why the fear?
World’s population is very susceptible
Transmissible man‐to‐man
Infamous for morbidity and mortality
No specific therapy
Eradicated in 1977
• Physicians are unfamiliar with recognition and treatment
Primary threat is delivery by aerosol release
Slide 54JSOMTC, SWMG(A)
Smallpox
Transmission
Spread by respiratory droplets or by contact with scabs, draining lesions, and contaminated objects
Onset
1 to 2 weeks
12/9/2014
19
Slide 55JSOMTC, SWMG(A)
Smallpox
Signs and symptoms
Fever begins followed by a rash (exanthema)
Inflammation of respiratory mucosa
Inflammation of regional lymphatics
Minor viremia
• Spreads to liver, spleen, lung and bone marrow in approximately 7 to 14 days
Slide 56JSOMTC, SWMG(A)
Smallpox
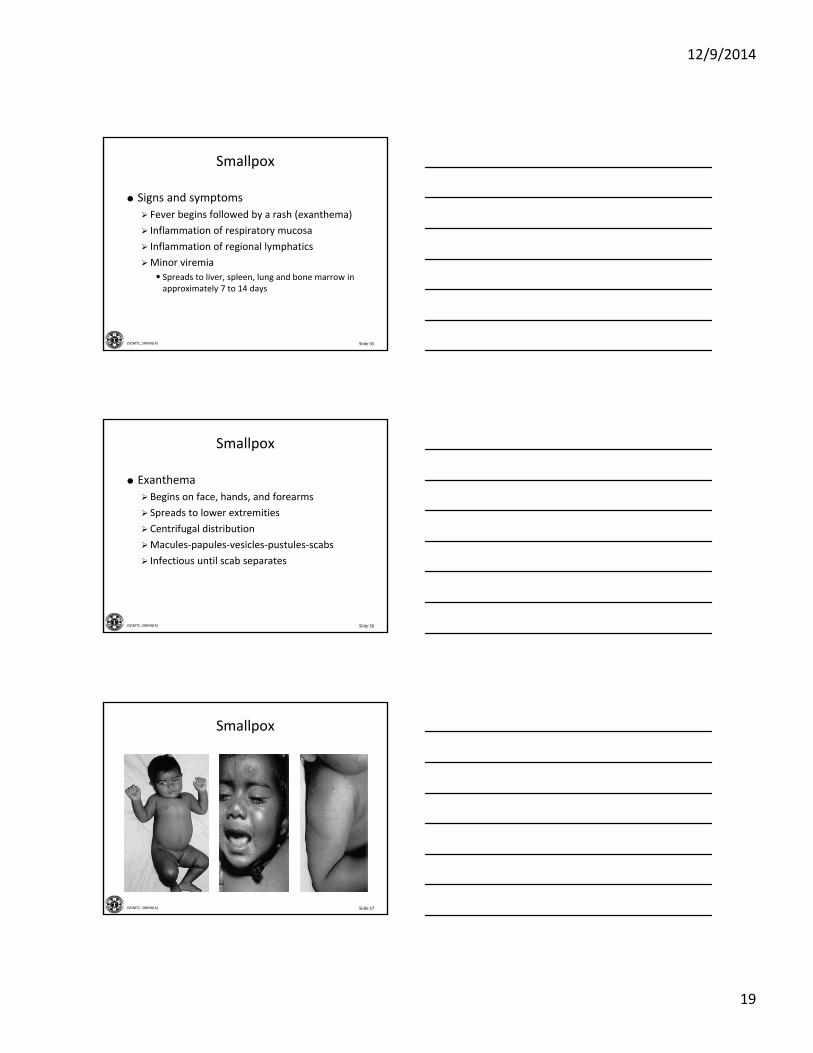
Exanthema
Begins on face, hands, and forearms
Spreads to lower extremities
Centrifugal distribution
Macules‐papules‐vesicles‐pustules‐scabs
Infectious until scab separates
Slide 57JSOMTC, SWMG(A)
Smallpox
12/9/2014
20
Slide 58JSOMTC, SWMG(A)
Smallpox
Slide 59JSOMTC, SWMG(A)
Smallpox
Slide 60JSOMTC, SWMG(A)
Smallpox
12/9/2014
21
Slide 61JSOMTC, SWMG(A)
Smallpox
Slide 62JSOMTC, SWMG(A)
Viral Hemorrhagic Fevers
VHF agents can be transmitted by aerosol in laboratory models
Stability in aerosols must be enhanced for weaponization
Considered too dangerous to use because of the lack of protective vaccines and therapeutic measures to protect the users
Slide 63JSOMTC, SWMG(A)
Viral Hemorrhagic Fevers
Transmission
Respiratory droplets or conact with body fluids depending on type of VHF
Onset
Days to weeks depending on type of VHF
12/9/2014
22
Slide 64JSOMTC, SWMG(A)
Viral Hemorrhagic Fevers
Signs and symptoms
Fever, headache, malaise, and dizziness
Myalgias
Nausea and vomiting
Petechiae
Bleeding manifestations
Hypotension
Shock and death
Slide 65JSOMTC, SWMG(A)
Viral Agent Treatment
Agent Onset Symptoms Mode Treatment
Smallpox 10 to 12 days Fever, chills, headache, malaise, backache, and lesions
Aerosol
Direct
Supportive care
Viral Hemorrhagic Fevers
4 to 21 days Early: headache, malaise, and myalgia
Late: bleeding, petechiae, and hypotension
Aerosol
Direct
Supportive care
Slide 66JSOMTC, SWMG(A)
Characteristics, Clinical Presentation, and Treatment of Toxin Producing Biological Agents
12/9/2014
23
Slide 67JSOMTC, SWMG(A)
Toxin Producing Biological Agents
Clostridium perfringens
Ricin
Staphylococcal Enterotoxin B
TrichotheceneMycotoxins
Slide 68JSOMTC, SWMG(A)
Toxin Producing Biological Agents
Toxins are poisonous by‐products of living organisms
They are very stable and produce severe illness when ingested, inhaled or introduced into the body by any other means
There effects on the human body range from minor illness to death
Slide 69JSOMTC, SWMG(A)
Botulism
Clostridium botulinum
Spore forming anaerobe
Botulinum toxin is the most potent neurotoxin known to man
Causes cranial nerve paralysis followed by descending skeletal muscle paralysis
• Inactivates the axon
12/9/2014
24
Slide 70JSOMTC, SWMG(A)
Botulism
Transmission
Ingestion
Contamination of open wounds
Inhalation through weaponized versions of toxin
Onset
12 to 72 hours after exposure
Slide 71JSOMTC, SWMG(A)
Botulism
Signs and symptoms
Muscle weakness and paralysis
• Double vision and drooping of both eye lids
• Difficulty chewing and swallowing• Dyspnea and respiratory failure
Slide 72JSOMTC, SWMG(A)
Botulism
12/9/2014
25
Slide 73JSOMTC, SWMG(A)
Botulism
Slide 74JSOMTC, SWMG(A)
Toxin Producing Agent Treatment
Agent Onset Symptoms Mode Treatment
Botulinumtoxin
12 to 72 hours Ptsosis, ~bulbar, muscular and resp. weakness
Late: resp. failure
Aerosol
Ingestion
Dermal
Antitoxin Supportive
Staphylococcal enterotoxin B
3 to 12 hours Fever/chills, headache, myalgia, productive cough
Aerosol
Ingestion
Supportive
Ricin 4 to 8 hours Fever/chills, cough, malaise, dypnea
Aerosol Supportive
TricotheceneMycotoxin
2 to 4 hours Necrosis and sloughing of affected tissues
Aerosol
Ingestion
Dermal
Supportiv
Slide 75JSOMTC, SWMG(A)
Characteristics and Types of Biological Agent Vaccines
12/9/2014
26
Slide 76JSOMTC, SWMG(A)
Biological Agent Vaccines
As of January 1999, vaccines are available for the following potential BW agent threats:
Anthrax
Botulinum toxin
Rift Valley Fever
Tularemia
Yellow fever
Argentine Hemorrhagic Fever
Plague
Smallpox
Venezuela Equine Encephalitis
Q‐Fever
Slide 77JSOMTC, SWMG(A)
Anthrax Vaccine
Slide 78JSOMTC, SWMG(A)
Anthrax Vaccine
After the Gulf war
Admission by Iraq that it had indeed produced weapons containing anthrax spores confirmed fears of use of anthrax as a biological weapon
Dec 1997
In response to this threat Secretary of Defense William Cohen announced a vaccination plan to vaccinate all U.S. service members using the licensed anthrax vaccine
12/9/2014
27
Slide 79JSOMTC, SWMG(A)
Anthrax Vaccine
Side effects
Fever, malaise, and myalgia
Less common than those observed following other vaccines
Slide 80JSOMTC, SWMG(A)
Smallpox Vaccine
Slide 81JSOMTC, SWMG(A)
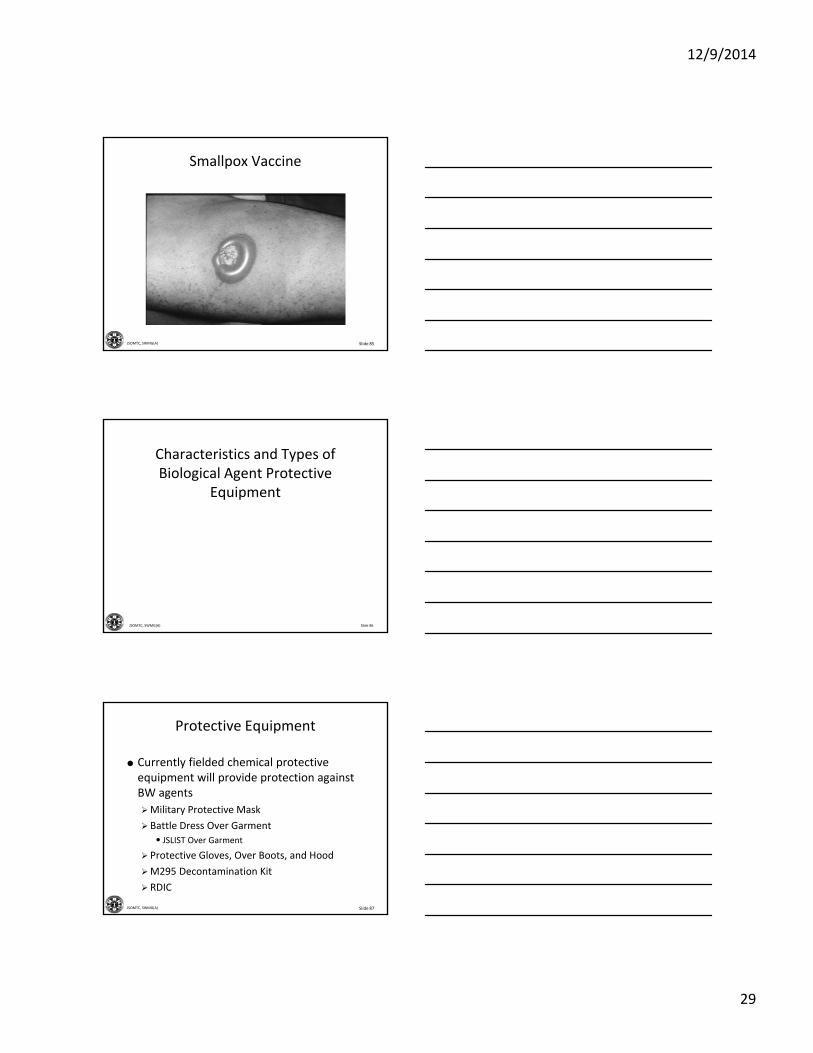
Smallpox Vaccine
There are no routine immunizations of US Forces for smallpox
When the threat indicates, senior leadership may direct vaccination
US adopted vaccinate in route protocol
Contraindications
Pregnancy, eczema, severe burns, psoriasis and other dermatoses
12/9/2014
28
Slide 82JSOMTC, SWMG(A)
Smallpox Vaccine
Slide 83JSOMTC, SWMG(A)
Smallpox Vaccine
Complications
Normal host
• Inadvertent inoculation (skin or eye)
• Generalized vaccinia• Erythema multiforme
• Encephalitis
Pregnancy
• Fetal vaccinia
Slide 84JSOMTC, SWMG(A)
Smallpox Vaccine
12/9/2014
29
Slide 85JSOMTC, SWMG(A)
Smallpox Vaccine
Slide 86JSOMTC, SWMG(A)
Characteristics and Types of Biological Agent Protective
Equipment
Slide 87JSOMTC, SWMG(A)
Protective Equipment
Currently fielded chemical protective equipment will provide protection against BW agents
Military Protective Mask
Battle Dress Over Garment
• JSLIST Over Garment
Protective Gloves, Over Boots, and Hood
M295 Decontamination Kit
RDIC
12/9/2014
30
Slide 88JSOMTC, SWMG(A)
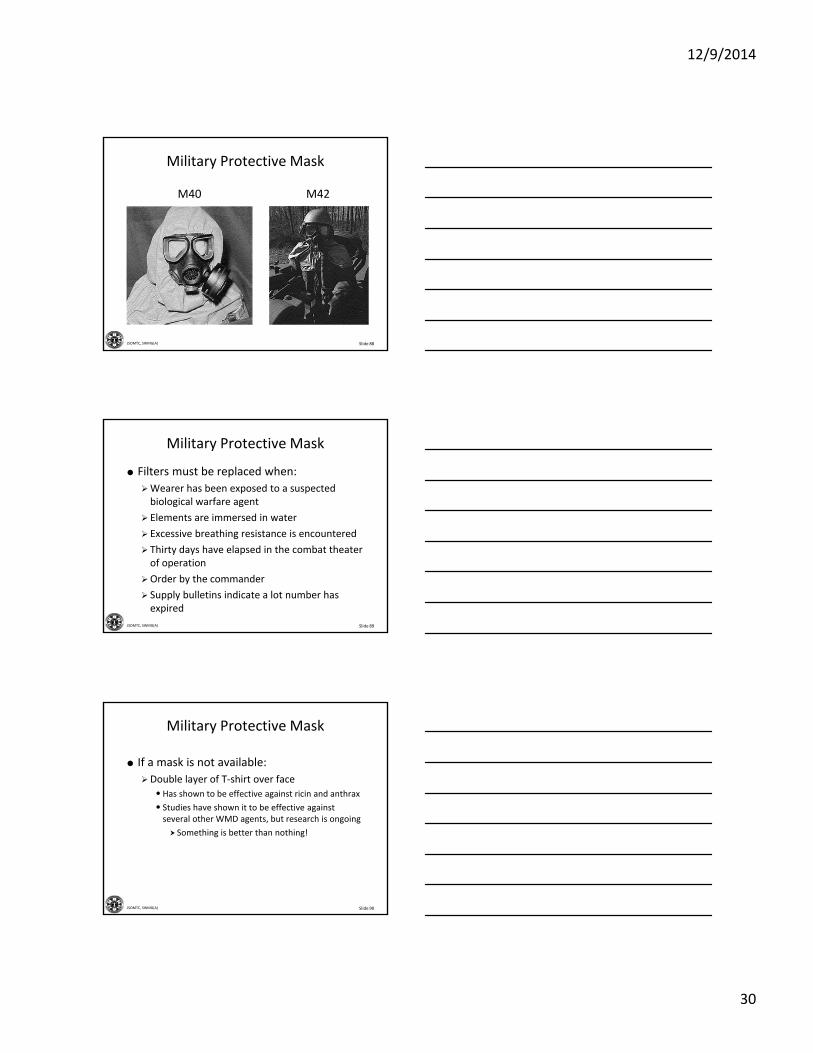
Military Protective Mask
M40 M42
Slide 89JSOMTC, SWMG(A)
Military Protective Mask
Filters must be replaced when:
Wearer has been exposed to a suspected biological warfare agent
Elements are immersed in water
Excessive breathing resistance is encountered
Thirty days have elapsed in the combat theater of operation
Order by the commander
Supply bulletins indicate a lot number has expired
Slide 90JSOMTC, SWMG(A)
Military Protective Mask
If a mask is not available:
Double layer of T‐shirt over face
• Has shown to be effective against ricin and anthrax
• Studies have shown it to be effective against several other WMD agents, but research is ongoing
Something is better than nothing!
12/9/2014
31
Slide 91JSOMTC, SWMG(A)
Military Protective Mask
Slide 92JSOMTC, SWMG(A)
Battle Dress Over Garment
Slide 93JSOMTC, SWMG(A)
JSLIST Over Garment
12/9/2014
32
Slide 94JSOMTC, SWMG(A)
Protective Over Boots
Slide 95JSOMTC, SWMG(A)
M295 Decontamination Kit
Slide 96JSOMTC, SWMG(A)
RDIC

12/9/2014
33
Slide 97JSOMTC, SWMG(A)
Mission Oriented Protective Posture
Initiate
When the local alarm or command is given
When entering an area known to be or suspected of being contaminated with an NBC agent
When casualties are being received by personnel at the patient receiving/decontamination area
Slide 98JSOMTC, SWMG(A)
Mission Oriented Protective Posture
Initiate (cont.)
Your position is under attack by aircraft spray
Mist or smoke of an unknown source is present
Suspicious odor, liquid or solid is present
Slide 99JSOMTC, SWMG(A)
Mission Oriented Protective Posture
Terminate
When the all clear is given
On order from the commander or the highest ranking official with a sound knowledge of the degree of contamination
Casualties unable to continue to wear the protective clothing may be protected by using wraps to protect against further chemical‐biological agent exposure
12/9/2014
34
Slide 100JSOMTC, SWMG(A)
Evacuation Concerns for Biological Agent Casualties
Slide 101JSOMTC, SWMG(A)
Evacuation Concerns
Evacuation platforms
Difficult to decontaminate
• Especially airframes
Percentage will become contaminated
•Mark contaminated vehicles
• Protect 50% of platforms from contamination
Identify routes for contaminated vehicles
Consider effect of rotor wash
Slide 102JSOMTC, SWMG(A)
Evacuation Concerns
When preparing casualties for medical evacuation, attempts should be made to identify the agent
Decontaminate externally when at all possible
USAF will not fly any patients who are contaminated
Special wraps and containers
12/9/2014
35
Slide 103JSOMTC, SWMG(A)
Evacuation Concerns
Casualties
Apply strict quarantine measures
Isolate and evacuate all smallpox patients
Cannot be evacuated across national boundaries unless approved by major command authority
Isolate all clothing of contaminated patients to include equipment
Identifying one single case of smallpox is an world emergency
Slide 104JSOMTC, SWMG(A)
Questions?
Slide 105JSOMTC, SWMG(A)
Terminal Learning Objective
Action: Communicate knowledge of field treatment of the biological casualty
Condition: Given a lecture in a classroom environment
Standard: Received a minimum score of 75% on the written exam IAW course standards
12/9/2014
36
Slide 106JSOMTC, SWMG(A)
Agenda
Identify the historical aspects of biological agents used in warfare
Identify the availability, advantages, disadvantages and delivery modes of biological agents
Identify the characteristics, clinical presentation, and treatment of bacterial biological agents
Slide 107JSOMTC, SWMG(A)
Agenda
Identify the characteristics, clinical presentation, and treatment of viral biological agents
Identify the characteristics, clinical presentation, and treatment of toxin producing biological agents
Identify the characteristics and types of biological agent vaccines
Slide 108JSOMTC, SWMG(A)
Agenda
Identify the characteristics and types of biological agent protective equipment
Identify evacuation concerns for biological agent casualties
12/9/2014
37
Slide 109JSOMTC, SWMG(A)
Reason





























