Embed Size (px)
Citation preview

Metodiche interventistiche nelle patologie cardiache congenite
Gianfranco Butera Policlinico San Donato IRCCS
What is fetal interven.on?
• Fetal interven7on is reaching inside the uterus to help a fetus who has a problem.
• All fetal interven7on is really maternal-‐fetal interven7on
Focus is on defects which can be accurately identified antenatally and
which cause progressive and permanent damage to the fetus if
not corrected.

Michael Tynan and Lindsey Allan
256
Balloon dilatation of the aortic valve in the fetus:
a report of two cases
Darryl Maxwell, Lindsey Allan, Michael J Tynan
AbstractBecause they had irreversible damage to
the left ventricular myocardium none of
12 patients with critical aortic stenosis
diagnosed prenatally survived after
postnatal treatment. This experience
prompted three attempts at intrauterine
balloon dilatation of the aortic valve in
two fetuses with this condition. On each
attempt the balloon catheter was
successfully delivered to the left ventri-
cle. In the first fetus the aortic valve was
not crossed and the fetus died the next
day. In the second fetus the balloon was
correctly positioned across the aortic
valve and inflated in the valve ring. After
delivery, a further balloon angioplasty
was performed; this relieved the stenosis
but the patient died five weeks later from
persisting left ventricular dysfunction
related to endocardial fibroelastosis.
Balloon angioplasty is feasible in fetal
life but the prognosis depends on the
ability of the relief of stenosis to limit,
prevent, or allow regression of left
ventricular damage before delivery.
Department ofFetal Medicine,Guy's Hospital,LondonD MaxwellDepartment ofPerinatal Cardiology,Guy's Hospital,LondonL AllanDepartment ofPaediatric Cardiology,Guy's Hospital,LondonM J TynanCorrespondence to
Dr Lindsey Allan,Department of Perinatal
Cardiology, 15th Floor,Guy's Hospital, St Thomas's
Street, London SEI 9RT.
Accepted for publication22 January 1991
The mildest forms of congenital aortic
stenosis may become haemodynamically
important only in late adult life when calcifica-
tion becomes a prominent feature whereas the
most severe forms are life threatening in
infancy. In the neonate mortality is high and
left ventricular dysfunction with endocardial
fibroelastosis is common. Even when the
obstruction to the left ventricular outflow tract
is relieved the left ventricle often fails to
maintain cardiac output.
Recently, it has become possible to detect
both aortic stenosis and the severer forms of
endocardial fibroelastosis in fetal life. In our
unit, 28 fetuses were identified as having aortic
stenosis alone (two cases) or aortic stenosis
with endocardial fibroelastosis (26 cases). In
two of the 12 mothers who elected to continue
the pregnancy there was an intrauterine death.
None of the 10 livebirths survived; only four
survived long enough for treatment by balloon
dilatation of the aortic valve. In addition, we
saw another prenatal feature that influenced
the outcome. In four of the 28 fetuses, the left
ventricle failed to grow normally as gestation
advanced and the left ventricle became hypo-
plastic which made the neonate unsuitable for
relief of aortic valve obstruction.'
Balloon dilatation is a well established
technique for the relief of pulmonary or aortic
Br Heart J 1991;65:256-8
stenosis in children.23 Its efficacy in the new-
born is being compared with that of surgical
valvotomy.4 We attempted balloon dilatation
in the fetus in an attempt to improve the
dismal prognosis for this condition by
relieving obstruction to the aortic valve before
irreversible left ventricular damage had
developed and to try to prevent the growth
failure that we had seen. We report our
experience in two fetuses in whom balloon
dilatation of the aortic valve was attempted.
Patients and methodsBoth patients were referred to the Department
of Perinatal Cardiology after a four chamber
view of the heart in the local hospital indicated
an abnormality. They were examined by an
Advanced Technical Laboratories Mark 4
sector scanner and a Hewlett Packard 77020A
phased array scanner with 5 MHz transducers.
Both machines can be used for Doppler
evaluation of intracardiac velocities and the
Hewlett Packard 77020A can be used for colour
flow mapping.The parents were extensively counselled
about the experimental nature of the
procedures to be attempted. The therapeutic
procedures were performed in the Fetal
Medicine Unit at Guy's Hospital with an
Acuson 128 ultrasound system for visualisation
of the needle course and manipulation of the
guide wires and balloon catheters. Eighteen
gauge transabdominal chorionic villus sam-
pling needles were used (Rockett, London).
For needle puncture of the umbilical cord and
cardiac chambers we used a freehand ultra-
sound guided method adapted from the tech-
nique first described by Daffos et al.' The
maternal skin was infiltrated by local anaes-
thetic before each needle insertion. Intra-
uterine and intracardiac pressures were
measured by a sterile system of fluid-filled
tubing connected from the hub ofthe needle via
a solid state transducer to a Siemans Mingograf
by a previously described method.6 In the first
procedure we used a USCI coronary balloon
catheter, diameter 2-5 mmwhen inflated. In the
second case a 3-5 mm diameter balloon was
custom made by NuMed.
CASE 1This 23 year old woman (para 2) was initially
referred at 22 weeks' gestation. The left
ventricle was of normal size for the gestation
but was contracting poorly. There was little
discernible forward flow into the left ventricle
or aorta. The left ventricular wall showed
• 12 fetuses, 27-33 weeks, 8 isolated AS, 2 AA, 2 PS+AS • 7/8 Pts with isolated AS – technically successful • 4 died within 24 hours of fetal intervention • 6 died after postnatal therapy • 2 survivors
• One had procedure at 33 weeks (dilated LV - would not have developed HLHS?)
• One survivor – procedure was technically unsuccessful
Aim of Fetal Cardiac Interven.ons
1) Promote ventricular growth and func7on • Univentricular Biventricular circula7on
• Aor7c stenosis with evolving HLHS • Pulmonary stenosis or atresia and evolving HRHS
2) Improve survival • HLHS with intact atrial septum • Salvage procedures (e.g. hydrops)
• Fetal pacing for complete heart block?
The most common fetal cardiac interven7on procedure is AORTIC VALVULOPLASTY
The primary indica7on for fetal aor7c valvuloplasty is to alter the in utero natural
history of midgesta7on fetal aor7c stenosis with evolving HLHS
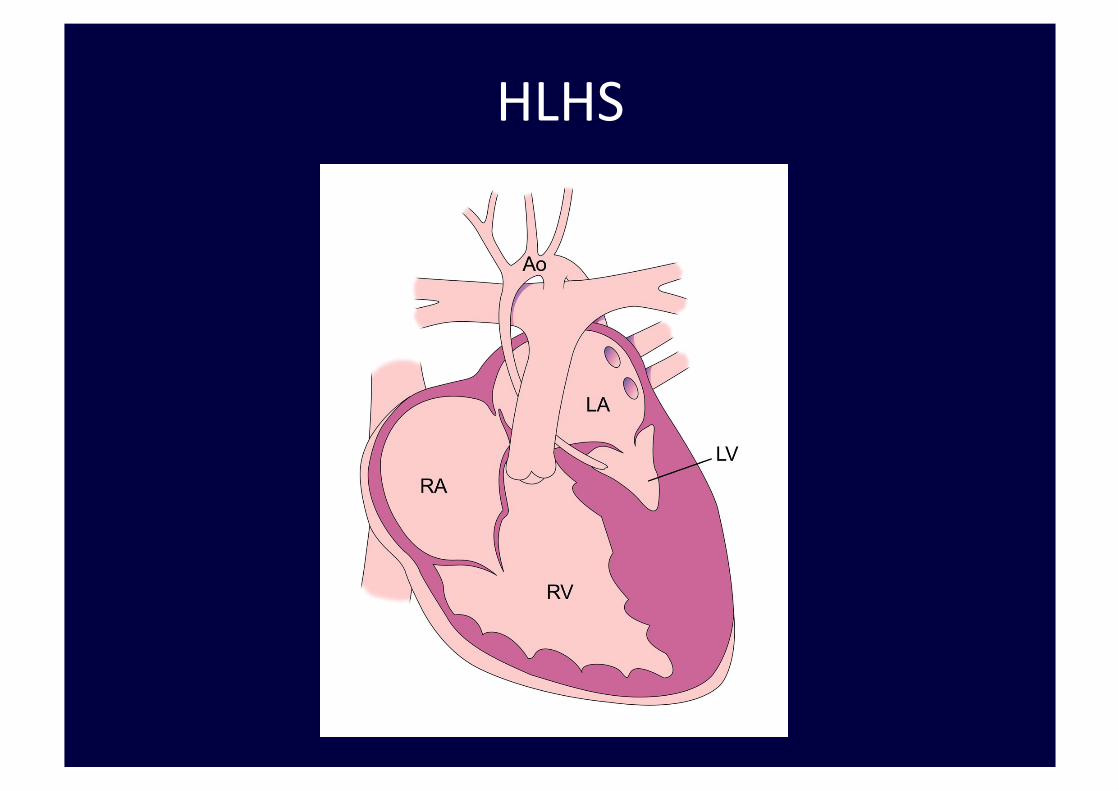
HLHS
Selec.on Guidelines for Fetal Aor.c Valvuloplasty
3 POINTS
1. The dominant cardiac anatomic anomaly is valvar aor7c stenosis
2. Evolving HLHS 3. There is poten7al for a technically successful
procedure and biventricular outcome postnatally.
1. The dominant cardiac anatomic anomaly is valvar aor.c stenosis
with ALL of the following: – Decreased mobility of valve leaflets – Antegrade Doppler color flow jet across aor7c valve smaller than the valve annulus diameter
– No or minimal subvalvar LV ouWlow obstruc7on
Selec.on Guidelines for Fetal Aor.c Valvuloplasty
2. Evolving HLHS
– LV func7on qualita7vely depressed AND
– EITHER retrograde or bidirec7onal flow in the transverse aor7c arch (between the first 2 brachiocephalic vessels) at any 7me during the cardiac cycle
– OR two of the following: • Monophasic MV inflow (Doppler profile of MV inflow without discrete E and A waves),
• Le\-‐to-‐right flow across atrial septum or intact atrial septum (bulging le\ to right),
• Bidirec7onal flow in pulmonary veins
Selec.on Guidelines for Fetal Aor.c Valvuloplasty
3. There is poten.al for a technically successful procedure and biventricular outcome postnatally
1 point for each of the following: • LV long axis Z-‐score > 0 • LV short axis Z-‐score > 0 • Aor7c anulus Z-‐score > -‐3.5 • Mitral valve anulus Z-‐score > -‐2 • Mitral valve or aor7c stenosis maximum gradient ≥ 20 mmHg
A score ≥4 had 100% sensi7vity, 53% specificity, 38% posi7ve predic7ve value, and 100% nega7ve predic7ve value.
Selec.on Guidelines for Fetal Aor.c Valvuloplasty
Fetal angioplasty
• Maternal conscious seda7on and regional spinal blockade conducted by an anesthesiologist.
• An appropriate fetal lie is achieved by external version. • Maternal posi7oning is kept with le\ uterine displacement. • To promote uterine relaxa7on mothers are given nifedipine
20 mg TID for 48-‐72 hours, star7ng 12-‐24 hours before the procedure.
• If ideal fetal posi7oning cannot be agained by external manipula7on, the procedure should be abandoned.
• A\er op7mal fetal posi7on is achieved, the fetus is anesthe7zed using a mixture of fentanil (5-‐10 micrograms/kg), pancuronium (10-‐20 micrograms/Kg) and atropine (20 micrograms/kg) given intramuscularly or in the umbilical chord using a 21-‐22G Chiba needle.
• Cardiac access is agained through direct needle puncture of the fetal heart via the uterus and the fetal chest wall.
• Under con7nuous two-‐dimensional ultrasound guidance a 15-‐cm-‐long 17-‐to-‐18-‐gauge Chiba needle (with a stylet) is advanced to the target
• The imaging plane is carefully adjusted to yield a picture in which both the en7re needle length and the target cardiac chamber are included in the field of view
Fetal angioplasty
• The Ventricle is entered at the apex, with the needle course parallel to the ouWlow track directed at the steno7c/atre7c semilunar valves.
• In this way the valves can be crossed almost blindly, with minimal wire and catheter manipula7on.
• A\er stylet removal, the catheter system is introduced and advanced un7l the sha\ mark reaches the proximal hub of the needle.
• Balloon posi7oning for infla7on is based on the external aforemen7oned measurements and ultrasound imaging, with emphasis given to the visualiza7on of the guide wire
Fetal angioplasty
• Balloons are inflated with pressure gauges to allow precise es7mates of infla7on diameters.
• Balloon diameters 10-‐30% larger than the aor7c or pulmonary valve annulus are selected for valve dila7on.
• Two to four infla7ons are performed depending on the fetal clinical status.
• A\er dilata7on, the whole system (needle + balloon + wire) is withdrawn as a unit through the fetal cardiac wall and out of the fetal and maternal bodies to avoid shearing off the balloon from the catheter sha\.
Fetal angioplasty
• A pre-‐marked system (a rapid exchange 10 mm long coronary balloon pre mounted over a cut-‐off 0.014” floppy 7p guide wire) is advanced to the desired loca7on.
• The needle, guide wire, and balloon sha\s are premeasured and marked so that posi7oning within the fetal heart is known from external measurements rather than the ultrasound imaging alone.
• The balloon sha\ is marked with sterile tapes so that no more than the full length of the balloon is extruded out of the Chiba needle 7p when fully advanced.
• The wire is also fixed with sterile tapes so that no more than 3-‐4 cm of the distal flexible wire straight 7p extruded out from the balloon 7p.
Fetal angioplasty

Fetal angioplasty
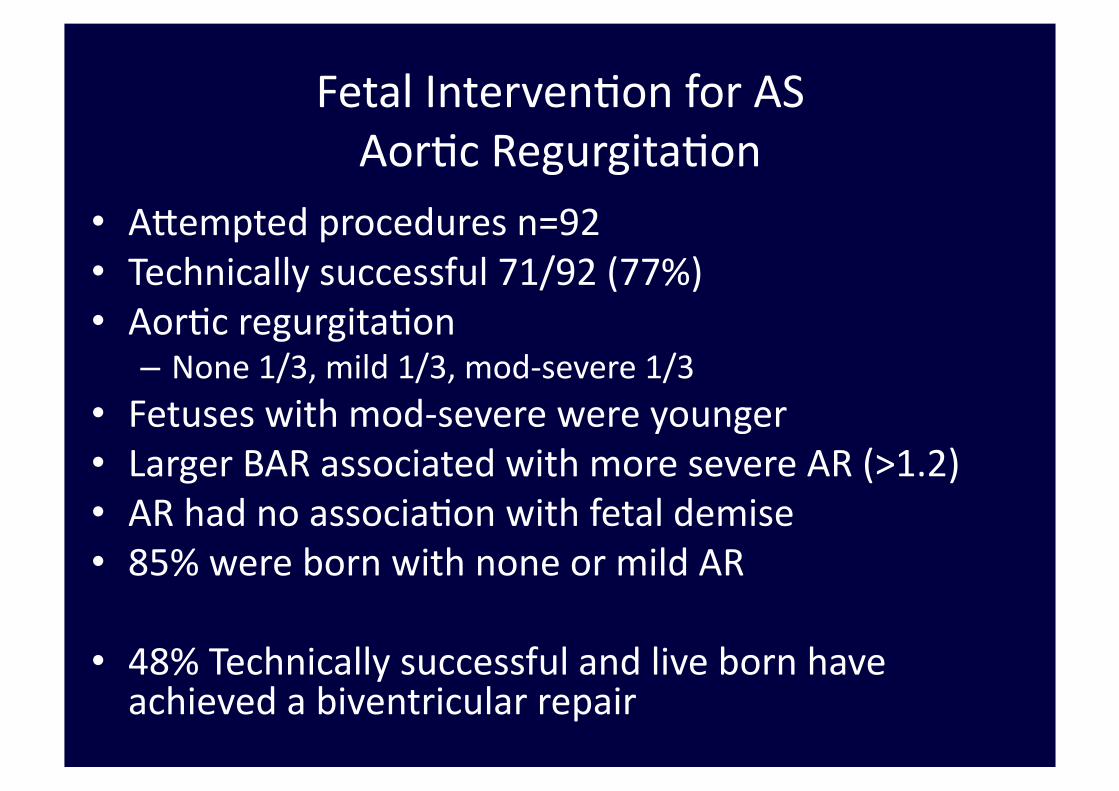
Fetal Interven7on for AS Aor7c Regurgita7on
• Agempted procedures n=92 • Technically successful 71/92 (77%) • Aor7c regurgita7on
– None 1/3, mild 1/3, mod-‐severe 1/3 • Fetuses with mod-‐severe were younger • Larger BAR associated with more severe AR (>1.2) • AR had no associa7on with fetal demise • 85% were born with none or mild AR
• 48% Technically successful and live born have achieved a biventricular repair
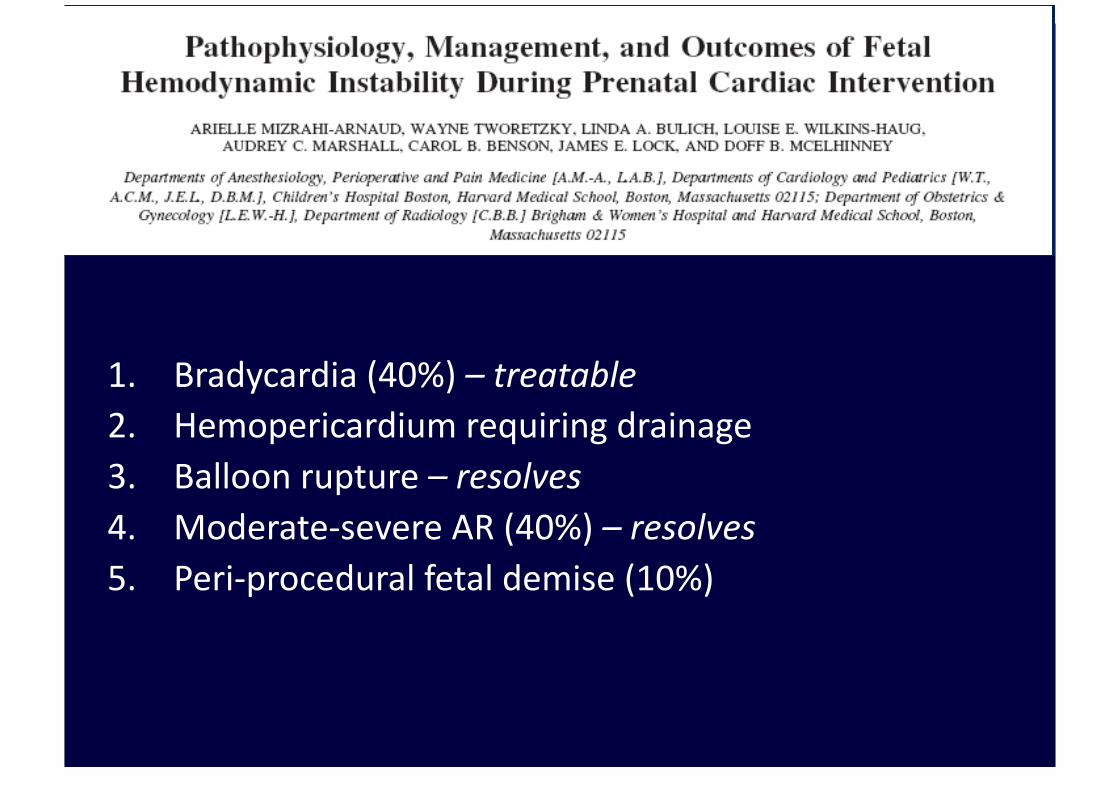
1. Bradycardia (40%) – treatable 2. Hemopericardium requiring drainage 3. Balloon rupture – resolves 4. Moderate-‐severe AR (40%) – resolves 5. Peri-‐procedural fetal demise (10%)
Complications
Mizrahi-Arnaud A - Pediatric Research 2007
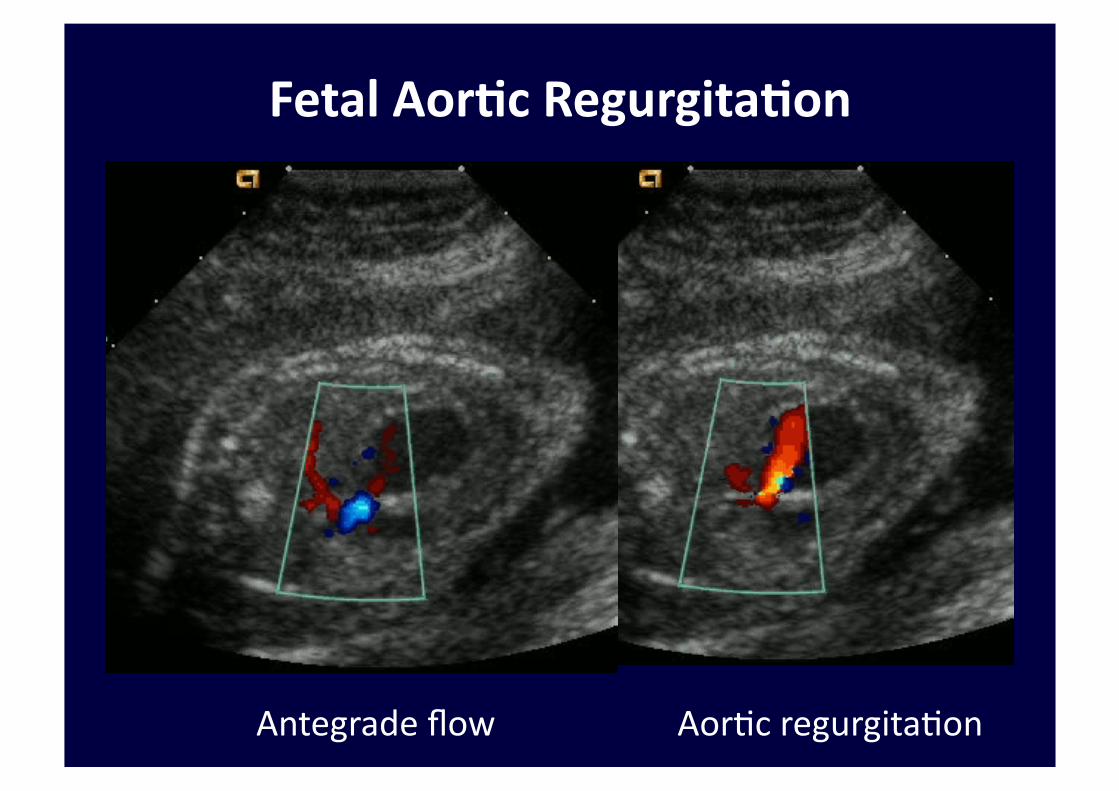
Fetal Aor.c Regurgita.on
Antegrade flow Aor7c regurgita7on
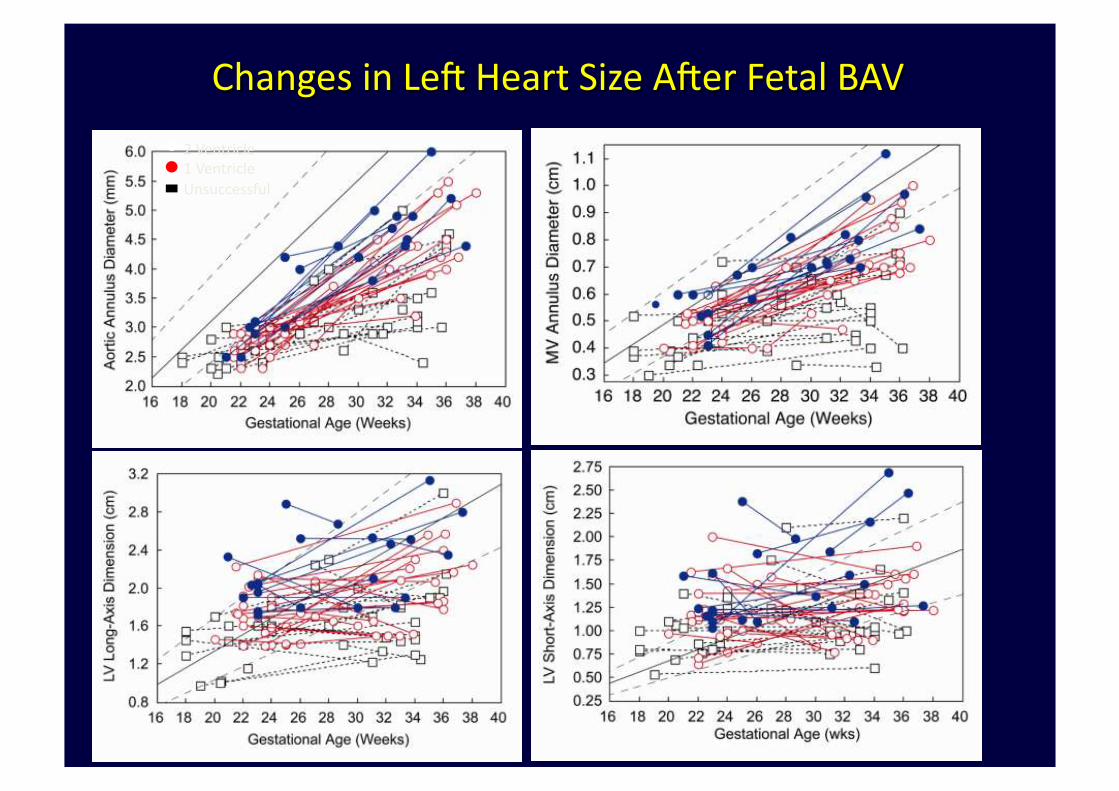
Results 2 Ventricle 1 Ventricle Unsuccessful
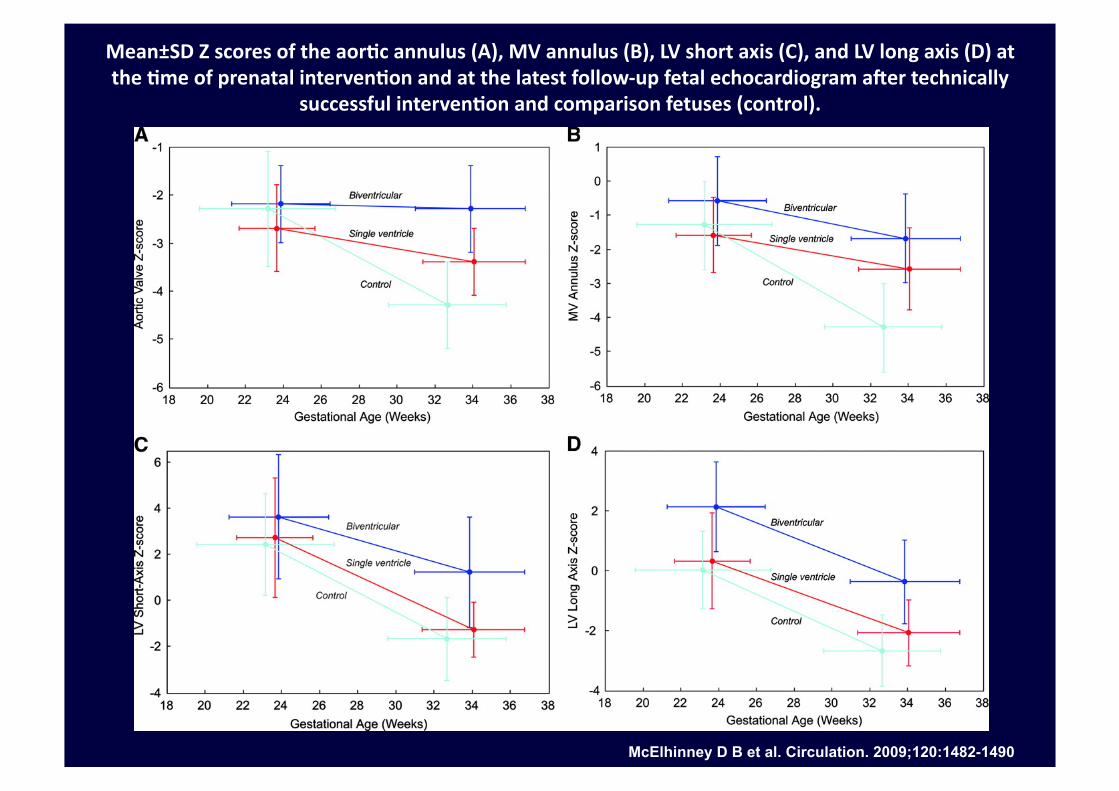
Mean±SD Z scores of the aor.c annulus (A), MV annulus (B), LV short axis (C), and LV long axis (D) at the .me of prenatal interven.on and at the latest follow-‐up fetal echocardiogram aXer technically
successful interven.on and comparison fetuses (control).
McElhinney D B et al. Circulation. 2009;120:1482-1490
Summary In utero balloon aor.c valvuloplasty
• AR occurred in 63% of our fetuses after BAV (44/69 technically successful)
• AR resolved completely in 73% who had AR (28/38 live-born)
• AR grade improved among the remaining 7/10 patients who had any residual AR at birth
• 2 patients had moderate or severe AR at birth and one had mild AR
Fetal AR
1. Why does fetal AR appear to be well tolerated? 1. Low systemic resistance – placenta
2. High LVEDP in fetus with AS – mi7gates the degree of AR
3. RV is providing circulatory support
2. Why does AR improve post-‐BAV? 1. Unique hemodynamics result in less mechanical stress
on the valve
2. Fetal valves are dynamic, contain prolifera7ng cells with an immature phenotype
3. Underlying pathologic stenosing process
Personal experience
• 2 cases
• 24 Weeks GA
• Detec7on at 22 WGA

• Pa7ents should have a prenatal echocardiographic diagnosis of PA/IVS or cri7cal pulmonary stenosis with the following features:
• membranous pulmonary atresia, with iden7fiable pulmonary valve (PV) leaflets or membrane,
• no or minimal systolic opening, • and no or minimal color Doppler ultrasound flow across the pulmonary valve (PV);
• an intact ventricular septum; • le\-‐to-‐right shun7ng across a patent ductus arteriosus (PDA);
Pulmonary atresia/IVS and evolving hypoplas.c right heart syndrome
• Pa7ents should have a prenatal echocardiographic diagnosis of PA/IVS with the following features:
• right heart hypoplasia, with a tricuspid valve (TV) annulus Z score below < 2 and an iden7fiable but qualita7vely small right ventricle (RV)
• with no evidence of RV growth a\er 2-‐4 weeks of serial echocardiographic evalua7on.
• Cases with fetal diagnosis of major coronary-‐to-‐RV fistulas should be excluded. Pulmonary valvuloplasty is performed between 24 and 30 weeks’ gesta7on.
Pulmonary atresia/IVS and evolving hypoplas.c right heart syndrome
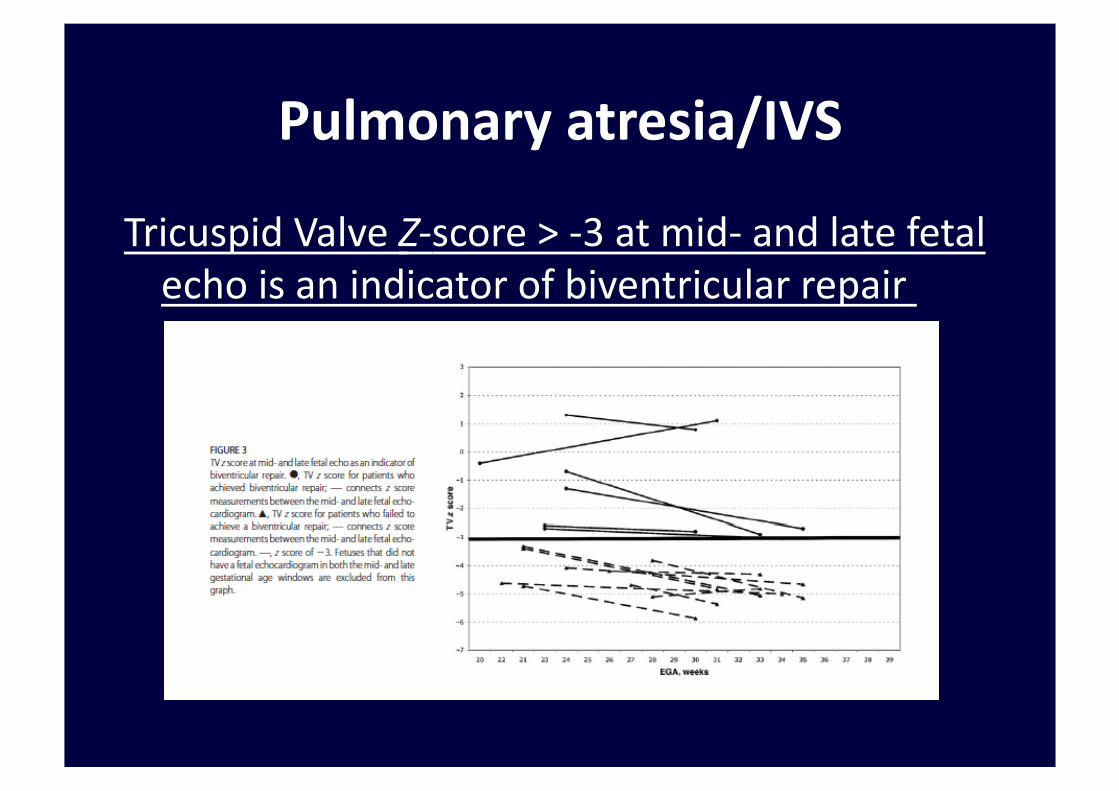
Pulmonary atresia/IVS
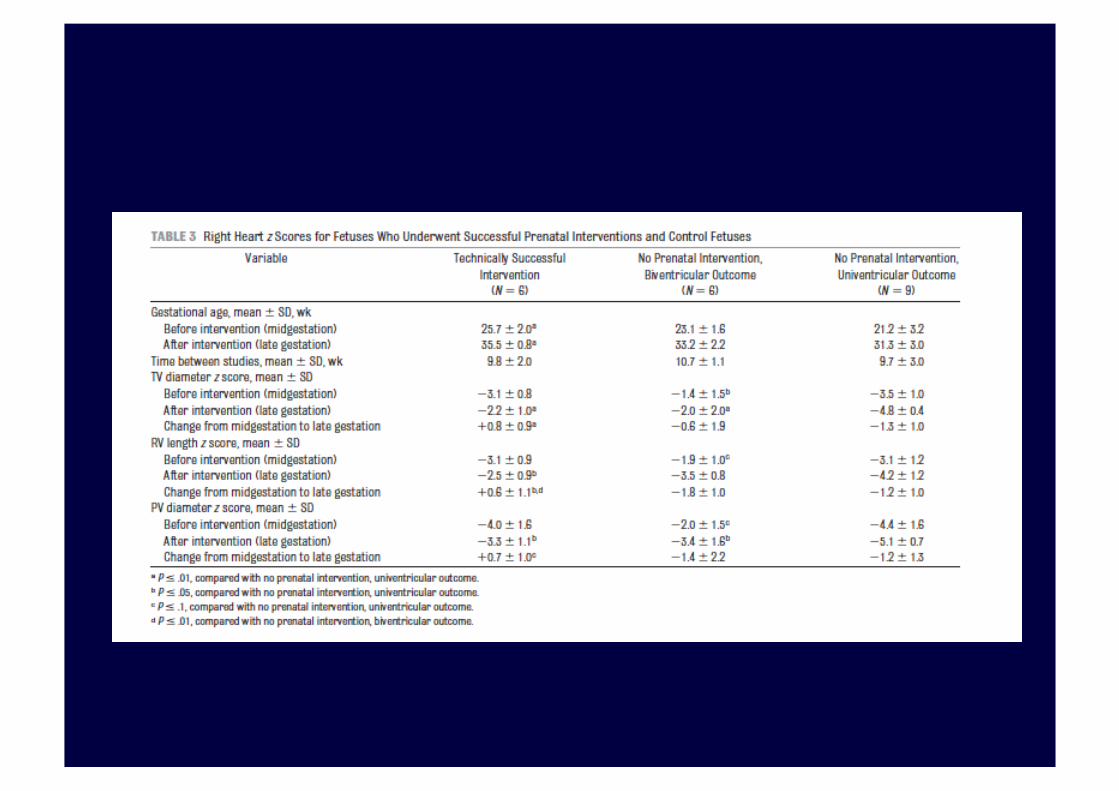
Tricuspid Valve Z-‐score > -‐3 at mid-‐ and late fetal echo is an indicator of biventricular repair
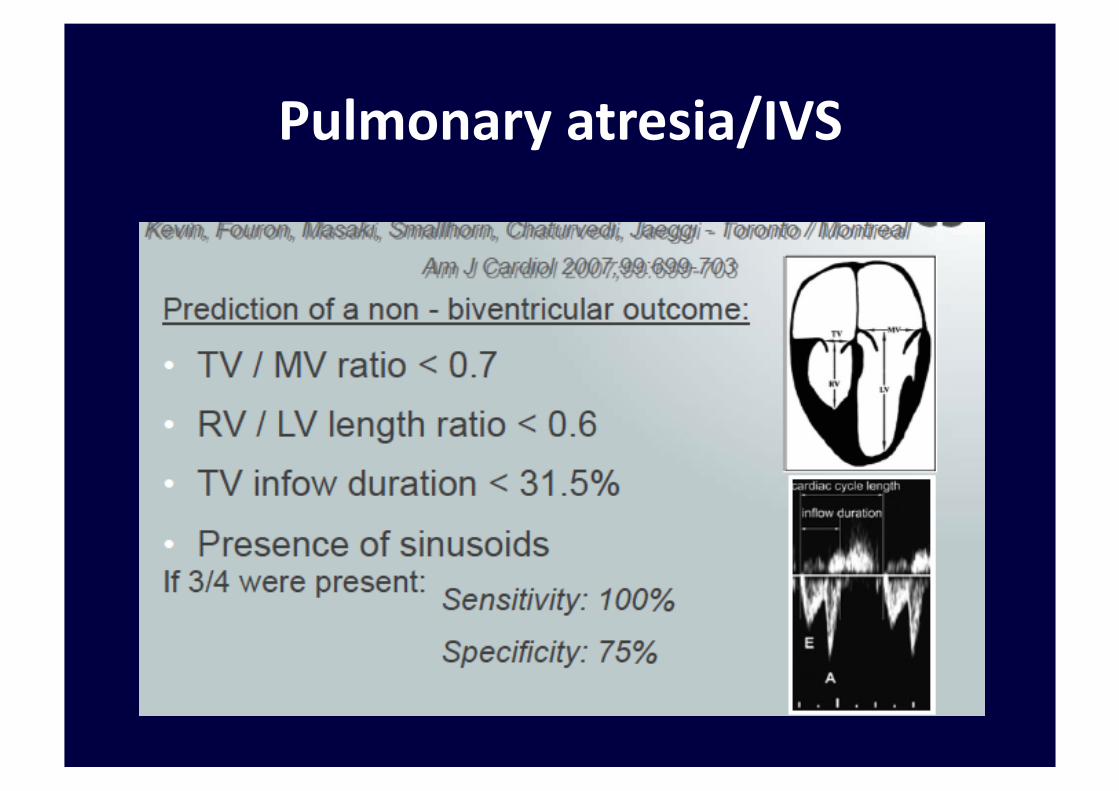
Pulmonary atresia/IVS
1. Bradycardia (40%) – treatable
2. Hemopericardium requiring drainage
3. Balloon rupture – resolves
4. Moderate-‐severe PR – resolves
5. Peri-‐procedural fetal demise (10%)
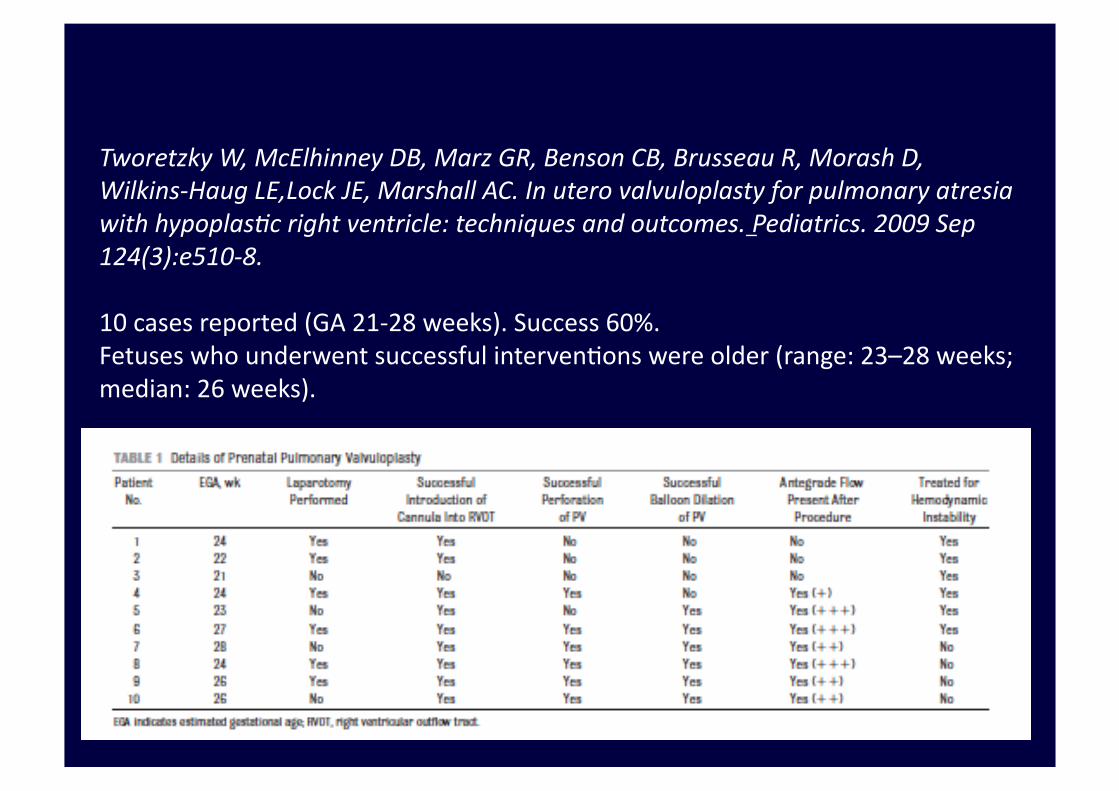
Tworetzky W, McElhinney DB, Marz GR, Benson CB, Brusseau R, Morash D, Wilkins-‐Haug LE,Lock JE, Marshall AC. In utero valvuloplasty for pulmonary atresia with hypoplasMc right ventricle: techniques and outcomes. Pediatrics. 2009 Sep 124(3):e510-‐8.
10 cases reported (GA 21-‐28 weeks). Success 60%. Fetuses who underwent successful interven7ons were older (range: 23–28 weeks; median: 26 weeks).
The procedure on the right ventricle is more challenging
due to: the more complex RV geometry, the smaller size of
the right ventricle compared to the le\, and the fact that
RVOT is behind the sternum.
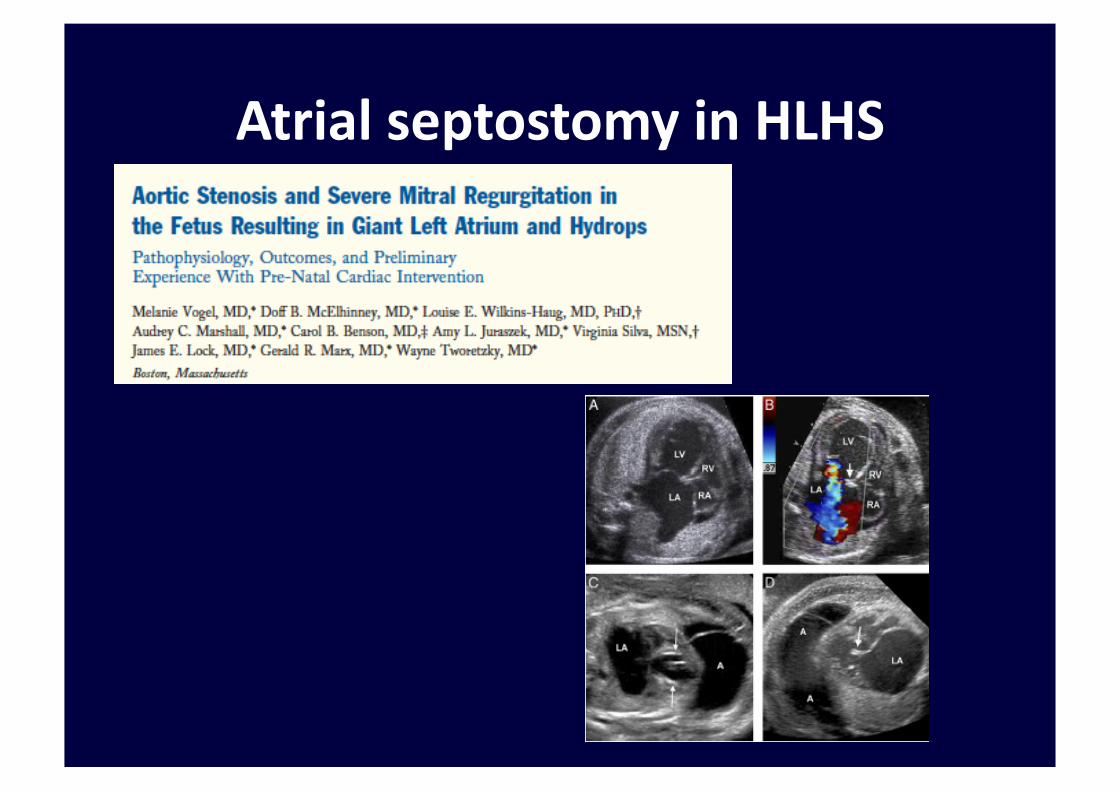
Atrial septostomy in HLHS
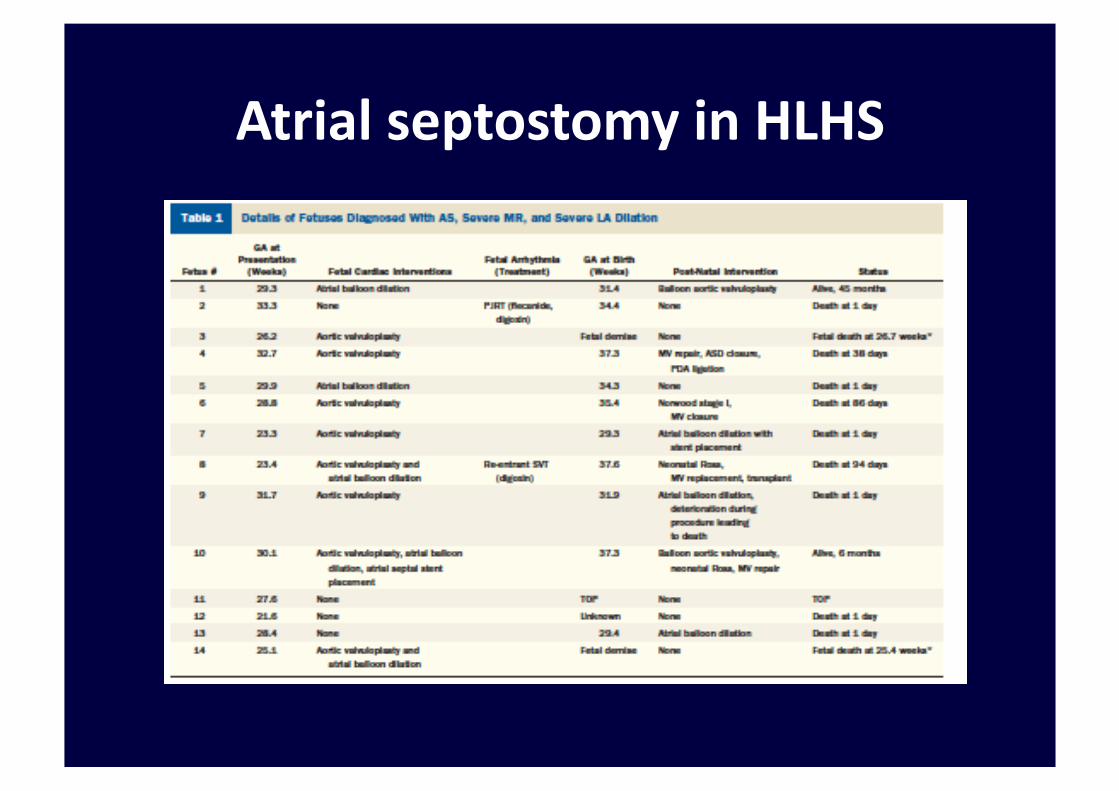
Atrial septostomy in HLHS
Limita.ons/Failures of Fetal Interven.ons
1) Technical limita7ons • Fetal posi7oning • Fetal stabiliza7on / movement
• Imaging • Equipment inadequacies
2) Biological limita7ons
• No animal model • Late referral
• Pa7ent selec7on • No uniform postnatal approach

Thank you for your agen7on








![Metodiche Estrattive Innovative [modalità compatibilità] 2013_2014... · Sono dotate di software che permettono di monitorare molteplici parametri per il controllo di ... Un altro](https://img.pdfslide.us/doc/110x75/5c66252309d3f2d12a8bd3c8/metodiche-estrattive-innovative-modalita-compatibilita-20132014-sono.jpg)