Embed Size (px)
Citation preview

Overestimation of Serum �Free Light Chain Concentrationby Immunonephelometry
To the Editor:
Measurement of serum free lightchains (sFLCs)1 has become an es-tablished method in the diagnosisand monitoring of monoclonalgammopathies (1, 2). Accurate quan-tification of sFLCs is important be-cause it is one of the prognostic in-dicators at disease presentation.Moreover, the International My-eloma Working Group has recentlyincorporated concentrations ofsFLCs in the response criteria ofmultiple myeloma and relatedmonoclonal gammopathies (1 ).
sFLC quantification with neph-elometric and turbidimetric immu-noassays is subject to substantialover- or underestimation (3 ). Astrong nephelometric overrating ofsFLC concentrations was reportedin a patient with a � light chainM-protein concentration of 23 g/Ldetermined by serum protein elec-trophoresis (SPE). The �-sFLCconcentration quantified by neph-elometry was 344 g/L and was over-estimated more than 10-fold ow-ing to the reaction of trimolecularaggregates of the monoclonal�-sFLCs with the antibody (4 ). Inour institute, a similar phenome-non was observed in a patient witha � light chain M-protein concen-tration of 3.1 g/L by SPE and 32.2g/L by nephelometry. To furtherstudy this discordance in �-sFLCconcentrations, we compared 2methods, nephelometry and ELISA.When possible, �-sFLC concentra-tions were also quantified by SPE.
We carried out the nephelo-metric technique on a BNII ana-lyzer (Siemens) using Freelite®reagents (The Binding Site) ac-
cording to the manufacturer’s in-structions. For the ELISA tech-nique, we modified a reportedassay (5 ). Briefly, we added cali-brator (pooled urine samples con-taining polyclonal FLCs) and di-luted serum samples to microtiterplates coated with polyclonal free �antibody (A0100, Dako). Boundfree � was detected using poly-clonal peroxidase-labeled total �antibody (P0129, Dako). The doseresponse of the calibrator reactedin parallel to that of the serumspecimen. For this �-sFLC assay-comparison study, we includedsamples of 49 individual patients,both at diagnosis or during follow-up, with monoclonal intact and/orfree � gammopathies.
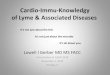
�/�-sFLC ratios measuredwith nephelometry ranged from0.8 to 77 250. An increased sFLCratio was found in 45 of 49 patients.A large difference was observed forthe �-sFLC concentrations mea-sured by the 2 methodologies, witha median �-sFLC concentrationmeasured by nephelometry of 0.41g/L vs 0.051 g/L measured withELISA. The method comparison of�-sFLC concentrations measuredby nephelometry and ELISA (Fig.1) showed an exponential correla-tion: [ELISA] � 0.63[nephelome-try]0.76 (R2 � 0.94).
Because of this exponentialdiscordance, the discrepancy be-tween the 2 assays most strongly af-fects samples with high �-sFLCconcentrations. Overall, we ob-served a qualitative disagreementbetween the 2 methods in 5 of 49samples (Fig. 1, triangles). All 5samples had a borderline increasein �-sFLC concentrations whenmeasured with nephelometry butwere considered normal by ELISA.One of these 5 had a normal sFLCratio, and 4 had increased sFLC ra-tios of 3.5, 7.8, 6.8, and 15.5,respectively.
In our cohort, 10 of 13 pa-tients with nephelometric �-sFLCconcentrations �1 g/L were ex-
pected to be quantifiable by SPEbecause the FLCs formed mono-clonal bands that migrated in the �region. However, only 4 of these 10samples (Fig. 1, circles) had aquantifiable monoclonal band bySPE, of 2.3, 2.9, 3.1, and 3.3 g/L.The �-sFLC concentrations inthese samples by nephelometrywere 22.4, 20.4, 32.2, and 34.1 g/L,and with the ELISA, 1.5, 1.9, 3.1,and 2.6 g/L. The other 6 samples(Fig. 1, squares) were below thequantifiable detection limit of SPE(�1 g/L), although the nephelo-metric �-sFLC concentrationswere quantified between 1.7 and7.9 g/L. The ELISA method didquantify the �-sFLC concentra-tions in these 6 samples as �1 g/L.These 10 samples demonstrate thatsera with high �-sFLC concentra-tions cannot be accurately quan-tified using nephelometry. Incontrast, �-sFLC concentrationsmeasured by ELISA do correspondwith the concentrations quantifiedby the monoclonal band in SPE.
Overestimation of nephelo-metric measured intact monoclo-nal immunoglobulins could beexplained by monoclonal immu-noglobulin polymerization and bythe differences in the immunoreac-tivity of monoclonal vs polyclonalimmunoglobulins. To date, 1 re-port has described an overestima-tion of a sample with a high �-sFLCconcentration caused by �-sFLCaggregates in the nephelometric as-say (4 ). We speculate that the in-trinsic capacity of monoclonal�-sFLCs to polymerize directly in-fluences nephelometric quantifica-tion. On the other hand, strong po-lymerization of FLCs could hideepitopes, which could theoreticallylead to some underreading of theFLC concentrations in both theELISA and the nephelometric as-says. Future research is warrantedto investigate the exact mechanismsthat cause the consistent overestima-tion of �-sFLC concentrations usingnephelometry.
1 Nonstandard abbreviations: sFLC, serum free lightchain; SPE, serum protein electrophoresis.
Clinical Chemistry 56:71188–1200 (2010) Letters to the Editor
1188

Our data demonstrate that�-sFLC concentrations can be mea-sured more accurately by ELISAthan by nephelometry. Our data fur-ther suggest that the �-sFLC concen-trations measured by nephelometryare constitutively and exponentiallyoverestimated, explaining the large
error in patients with high serum�-sFLC concentrations.
Author Contributions: All authors con-firmed they have contributed to the intellec-tual content of this paper and have met thefollowing 3 requirements: (a) significant con-
tributions to the conception and design, ac-quisition of data, or analysis and interpreta-tion of data; (b) drafting or revising the articlefor intellectual content; and (c) final approvalof the published article.
Authors’ Disclosures of Potential Con-flicts of Interest: No authors declared anypotential conflicts of interest.
Fig. 1. Method comparison of �-sFLC concentrations measured by nephelometry vs ELISA.
Dotted lines, upper reference values; thick solid line, the regression line of samples measured with both ELISA and nephelometry([ELISA] � 0.63[nephelometry]0.76, R2 � 0.94). For 2 patients, serum protein electrophoresis and corresponding densitometrydata are depicted. See text for definition of symbols.
Letters to the Editor
Clinical Chemistry 56:7 (2010) 1189

Role of Sponsor: The funding organiza-tions played no role in the design of study,choice of enrolled patients, review and in-terpretation of data, or preparation or ap-proval of manuscript.
References
1. Dispenzieri A, Kyle R, Merlini G, Miguel JS, Lud-wig H, Hajek R, et al. International MyelomaWorking Group guidelines for serum-free lightchain analysis in multiple myeloma and relateddisorders. Leukemia 2009;23:215–24.
2. Durie BGM, Harousseau J-L, Miguel JS, Blade J,Barlogie B, Anderson K, et al. International uni-form response criteria for multiple myeloma.Leukemia 2006;20:1467–73.
3. Tate JR, Gill D, Cobcroft R, Hickman PE. Practicalconsiderations for the measurement of free lightchains in serum. Clin Chem 2003;49:1252–7.
4. Abraham RS, Charlesworth MC, Owen BAL, Ben-son LM, Katzmann JA, Reeder CB, et al. Trimo-lecular complexes of � light chain dimers inserum of a patient with multiple myeloma. ClinChem 2002;48:1805–11.
5. Lamers KJ, Jongen PJ, Kock-Jansen MJ, TeunesenMA, Prudon-Rosmulder EM. Cerebrospinal fluidfree kappa light chains versus IgG findings in neu-rological disorders: qualitative and quantitativemeasurements. J Neuroimmunol 1995;62:19–25.
Corrie M. de Kat Angelino2
Reinier Raymakers3
Maria A. Teunesen2
Joannes F.M. Jacobs2,4,5
Ina S. Klasen2*
2 Department of Laboratory Medicine
Laboratory of Medical Immunology4 Department of Tumor Immunology
and 5 Department of Medical Oncology
Radboud University
Nijmegen Medical Centre
Nijmegen, the Netherlands3 Department of Hematology
University Medical Centre Utrecht
Utrecht, the Netherlands
*Address correspondence to this author at:
Radboud University Nijmegen Medical Centre
Department of Medical Immunology (469)
Geert Grooteplein 10
6525 GA Nijmegen
The Netherlands
Fax 31-24-3619415
E-mail [email protected]
Previously published online atDOI: 10.1373/clinchem.2010.143529
Circadian Secretion Pattern ofCopeptin, the C-TerminalVasopressin PrecursorFragment
To the Editor:
Copeptin, the C-terminal peptideof provasopressin, is stoichiomet-rically released with arginine vaso-pressin (AVP). In contrast to AVP,it is stable ex vivo (1 ) and reflectsthe AVP system, as shown in diabe-tes insipidus or the syndrome of in-appropriate antidiuretic hormonesecretion (2 ). Copeptin is a reliablemarker of severe stress, with in-creased concentrations found incases of critical illness, sepsis, hem-orrhagic shock, and stroke (2 ). Theserum copeptin concentration isprofoundly and immediately stim-ulated after myocardial infarction(3 ). The absence of such stimula-tion within the first hours after theonset of symptoms has recently beenproposed as an important negativepredictor for excluding the likeli-hood of infarction in patients withunspecific chest pain (3).
Any further use of the peptideas a marker critically depends onclear cutoffs between health anddisease. To better characterize thediagnostic accuracy of copeptin,we studied its physiological pulsa-tile and circadian variation in
healthy individuals and comparedcopeptin rhythms with those ofcortisol in these patients.
Blood for copeptin analysiswas sampled every 20 min for 24 h(0900 to 0900) in 7 healthy individ-uals (1 female, 6 males; age range,18–37 years; mean body mass index,22.6 kg/m2). Sera were separated andimmediately frozen at �80 °C. Thestudy was approved by the local re-search ethics committee.
Serum copeptin was measuredwith a chemiluminescence sand-wich immunoassay [lower detec-tion limit, 0.4 pmol/L; functionalassay sensitivity at �20% interas-say CV, �1 pmol/L; see (1 )]. Cor-tisol was measured immunometri-cally (Bayer Immuno 1™ System,Bayer Corp.) according to manu-facturer’s instructions. The maxi-mal inter- and intraassay CVs were6.5% at a copeptin concentrationof 4.1 pmol/L and 7.9% at a cortisolconcentration of 88 nmol/L (4 ).
We used a clustering algo-rithm to analyze attributes of thecopeptin concentration profiles(fixed CV of 10%; t statistic for anupstroke/downstroke � 1; clustersize for test peak/nadir � 1) pro-vided optimal peak detection(�90% sensitivity and positivepredictive accuracy) (5 ).
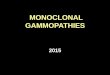
Copeptin concentrations showedno consistent circadian rhythm.
Fig. 1. Individual 24-h copeptin rhythms for 7 healthy individuals.
Letters to the Editor
1190 Clinical Chemistry 56:7 (2010)

Peaks and troughs of the individualrhythms varied widely over the24-h period with no evidence ofsynchronization among individu-als or a clear relationship withthe light– dark cycle [mean (SD)copeptin concentration, 4.3 (1.5)pmol/L; 11.4 (3.6) pulses/24-h pe-riod; mean pulse height, 5.1 (1.8)pmol/L] (Fig. 1). Interestingly, theexpected large increase in cortisolduring the second half of thenight in these individuals [see(4 )] is not related to copeptin.Because AVP is known to acutelystimulate cortisol via cortico-tropin release in stress situations,our present findings argueagainst both a role of AVP in thecircadian release of cortisol andan important physiological roleof AVP in the generation of cor-tisol pulses under nonstressconditions.
The highest copeptin con-centration measured was 13.1pmol/L; the mean maximumconcentration for all individualswas 7.8 (2.9) pmol/L. Therefore,the variation in circadian copep-tin concentration in healthy indi-viduals remained well within thedescribed reference interval (1 ).The timing of blood sampling didnot appear as critical as for theinterpretation of cortisol results.Our data will help to better definereference values for the use ofcopeptin measurements in pre-dicting stress conditions. Refer-ence values may be particularlyimportant when a low copeptinconcentration is used as a veryearly negative predictor in stresssituations such as myocardial in-farction (3 ), in which the physio-logical variation in copeptin haslittle influence on the interpreta-tion of the results.
Author Contributions: All authors con-firmed they have contributed to the intellec-tual content of this paper and have met thefollowing 3 requirements: (a) significant con-
tributions to the conception and design, ac-quisition of data, or analysis and interpreta-tion of data; (b) drafting or revising the articlefor intellectual content; and (c) final approvalof the published article.
Authors’ Disclosures of Potential Con-flicts of Interest: Upon manuscript submis-sion, all authors completed the Disclosures ofPotential Conflict of Interest form. Potentialconflicts of interest:
Employment or Leadership: N.G. Mor-genthaler, Global Medical Affairs,BRAHMS AG.Consultant or Advisory Role: Nonedeclared.Stock Ownership: None declared.Honoraria: None declared.Research Funding: None declared.Expert Testimony: None declared.
Role of Sponsor: The funding organiza-tions played a direct role in the preparationof the manuscript.
References
1. Morgenthaler NG, Struck J, Alonso C, BergmannA. Assay for the measurement of copeptin, astable peptide derived from the precursor ofvasopressin. Clin Chem 2006;52:112–9.
2. Morgenthaler NG, Struck J, Jochberger S, DunserMW. Copeptin: clinical use of a new biomarker.Trends Endocrinol Metab 2008;19:43–9.
3. Reichlin T, Hochholzer W, Stelzig C, Laule K,Freidank H, Morgenthaler NG, et al. Incrementalvalue of copeptin for rapid rule out of acutemyocardial infarction. J Am Coll Cardiol 2009;54:60–8.
4. Darzy KH, Shalet SM. Absence of adrenocortico-tropin (ACTH) neurosecretory dysfunction butincreased cortisol concentrations and productionrates in ACTH-replete adult cancer survivors af-ter cranial irradiation for nonpituitary brain tu-mors. J Clin Endocrinol Metab 2005;90:5217–25.
5. Veldhuis JD, Johnson ML. Cluster analysis: asimple, versatile, and robust algorithm for endo-crine pulse detection. Am J Physiol 1986;250:E486–93.
Ken H. DarzyKashinath C. DixitStephen M. Shalet
Nils G. MorgenthalerGeorg Brabant*
Department of Endocrinology
Christie Hospital NHSFT
Manchester, UK
* Address correspondence to this author at:
Department of Endocrinology
Christie Hospital NHSFT
Wilmslow Rd
Manchester M20 4BX, UK
Previously published online atDOI: 10.1373/clinchem.2009.141689
Evaluation of the Quo-TestHemoglobin A1c Point-of-CareInstrument: Second Chance
To the Editor:
We previously reported the evalu-ation of 8 different hemoglobin A1c
(Hb A1c)1 point-of-care instruments
(1). Two of 8 manufacturers with-drew from that study after initial un-promising results. One of the 2 in-struments withdrawn was the Quo-Test A1c (Quotient Diagnostics),which was withdrawn because of atechnical problem. The manufac-turer claimed to have resolved theproblem and asked us to reevaluatethe instrument.
The Quo-Test method isbased on affinity separation andthe use of fluorescence quenchingand gives results in 3 min. The in-strument was certified by the Na-tional Gycohemoglobin Standard-ization Program (NGSP) as ofSeptember 2009 (2 ).
We used the same approachfor evaluation as in the initialstudy, following the CLSI EP-5protocol for imprecision and theCLSI EP-9 protocol for methodcomparison. Because the Ameri-can Diabetes Association has rec-ommended Hb A1c as the preferredtest for the diagnosis of diabetes(3 ), we added an additional sampleof approximately 6.5% Hb A1c inthe EP-5 protocol. The EP-9 proto-col was performed twice with 2 dif-ferent lot numbers and compared
1 Nonstandard abbreviations: Hb A1c, hemoglobinA1c; NGSP, National Glycohemoglobin Standard-ization Program; SRM, secondary reference mea-surement procedure.
Letters to the Editor
Clinical Chemistry 56:7 (2010) 1191

with 3 IFCC and NGSP secondaryreference measurement procedures(SRM): the Roche Tina-quant He-moglobin A1c Gen.2 on Cobas In-tegra 800, immunoassay, IFCC andNGSP SRM (Roche Diagnostics);the Primus Ultra2, affinity chroma-tography HPLC, IFCC, and NGSPSRM (Primus Diagnostics, a TrinityBiotech Company); and the TosohG8, cation-exchange HPLC, IFCCSRM (Tosoh Bioscience N.V./S.A.).
To check overall calibrationand bias, we compared the EP-9protocol results to the mean of the3 SRM results and also used theEP-9 protocol results to calculatethe NGSP certification criterionwith 2 reagent lot numbers.
In monitoring therapy, the re-producibility of Hb A1c assays is
critical. The total CV should be�3% (realistic goal) and for opti-mal clinical use �2% (desirablegoal) (1 ). The total CVs in the EP-5protocol for the Quo-Test at HbA1c values of 5.0%, 6.2%, and10.2% were 5.9%, 4.5%, and 2.9%,respectively.
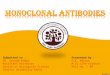
Comparisons between theQuo-Test with 2 reagent lot num-bers and the mean of the 3 SRM areshown in Fig. 1 with the individualEP-9 results and the NGSP certifi-cation calculations. The 95% CI ofthe differences between the SRMand test methods should fall within�0.75% Hb A1c (total error) topass the current NGSP criteria (4 ).The Quo-Test NGSP certificationwas granted in September 2009 (2 )before the tightening of the NGSP
criteria from �0.85% Hb A1c to�0.75% Hb A1c. To evaluate thismethod in the same way as theother methods in our previousstudy (1 ), we used the old criteria.The calibration of the first lotnumber appeared adequate, butwith the EP-5 protocol we ob-served high variability reflected bya high total CV, and a high SE ofestimates was still a matter of con-cern. The discrepancy with the sec-ond lot number may have been at-tributable to problems associatedwith upscaling of the production ofcartridges.
The Quo-Test passed theNGSP criteria compared with 1SRM (Tosoh G8) with 1 lot num-ber but failed the NGSP criteria forall the other comparisons (Fig. 1).
Fig. 1. Hb A1c results for 2 different lot numbers from the Quo-Test point-of-care instrument compared to the meanHb A1c results from 3 SRM procedures (individual EP-9 regression lines and NGSP certification criteria are shownbelow the graph).
The P value of the regression lines between the 2 lot numbers was �0.001, which confirmed the statistically significantdifference between the 2 regression lines.
Letters to the Editor
1192 Clinical Chemistry 56:7 (2010)

Tests performed by using Chow-statistics for the overall differencesin slope and intercept per methodfor lot numbers 1 and 2 showedsignificant differences in analyticalperformance between the 2 lotnumbers (P� 0.001).
The manufacturer provided 2controls with wide ranges: low con-trol 4.2% to 7.5% and high control10.5% to 15.3%. The manufacturershould narrow these ranges as wasdescribed recently (1).
Results of analysis of the ana-lytical performance of the Quo-Test showed a high total CV, largebias with 1 lot number, failedNGSP criteria, and significant dif-ferences between lot numbers. TheQuo-Test is officially NGSP certi-fied and passed the NGSP criteriawith only 1 lot number as tested atthe manufacturer’s site (2 ). The re-sults we report here demonstratethe large lot-to-lot variability inquality of the Quo-Test Hb A1c
point-of-care test.Health care professionals
should be aware of the clinical im-plications for an Hb A1c valuethat is determined by usinga point-of-care instrument (5 ).Moreover, to properly interpretthe result, health care profession-als must know the analytical per-formance of the Hb A1c methodused. This study and the previousstudy (1 ) prove that an NGSPcertification does not guaranteethe quality of results produced inthe field and confirms the recom-mendation of the American Dia-betes Association not to use HbA1c point-of-care assays for diag-nostic purposes at this time (3 ).Validation of a new method is al-ways necessary and cannot be ex-pected to be carried out by healthcare professionals. For this rea-son we think that point-of-caredevices should be guided by andfall under the responsibility of acentral laboratory.
Author Contributions: All authors con-firmed they have contributed to the intellec-tual content of this paper and have met thefollowing 3 requirements: (a) significant con-tributions to the conception and design, ac-quisition of data, or analysis and interpreta-tion of data; (b) drafting or revising the articlefor intellectual content; and (c) final approvalof the published article.
Authors’ Disclosures of Potential Con-flicts of Interest: No authors declared anypotential conflicts of interest.
Role of Sponsor: The funding organiza-tions played no role in the design of study,choice of enrolled patients, review and in-terpretation of data, or preparation or ap-proval of manuscript.
References
1. Lenters-Westra E, Slingerland RJ. Six of eighthemoglobin A1c point-of-care instruments donot meet the general accepted analytical perfor-mance criteria. Clin Chem 2010;56:44–52.
2. NGSP. List of NGSP certified methods. [Updated12/09, listed by date certified]. http://www.ngsp.org/prog/methods.pdf (Accessed March 2010).
3. American Diabetes Association. Diagnosis andclassification of diabetes mellitus. Diabetes Care2010;33:S62–9.
4. NGSP. NGSP protocol: C. standardization andcertification of methods by manufacturers.http://www.ngsp.org/prog/protocol/prot.html(Accessed December 2009).
5. Bruns DE, Boyd JC. Few point-of-care hemoglo-bin A1c assay methods meet clinical needs. ClinChem 2010;56:4–6.
Erna Lenters-Westra2,3*
Robbert J. Slingerland2,3
2 Department of Clinical Chemistry, Isala
KliniekenZwolle, the Netherlands
3 European Reference Laboratory for
GlycohemoglobinZwolle, the Netherlands
* Address correspondence to this author at:
Isala Klinieken, Department of Clinical
Chemistry
Groot Wezenland 20
8011 JW Zwolle
the Netherlands
Fax �31-38-4242-676
E-mail [email protected]
Previously published online atDOI: 10.1373/clinchem.2010.143149
Could Susceptibility to LowHematocrit Interference HaveCompromised the Results ofthe NICE-SUGAR Trial?
To the Editor:
The recently published findings ofthe Normoglycemia in IntensiveCare Evaluation and Survival UsingGlucose Algorithm Regulation(NICE-SUGAR)1 trial have dramat-ically changed clinician attitudes to-ward the achievement of euglycemiain intensive care unit (ICU) patients(1). In defending the proof-of-concept studies that validated the ef-ficacy of normalizing blood glucosein the ICU, Van den Berghe et al.pointed out numerous variances be-tween their original studies andthose of the NICE-SUGAR trial (2).They included differences in bloodglucose targets, insulin administra-tion, blood sampling, nutritionalstrategies, clinician expertise, and therelative accuracy of the glucose mea-surement devices. Recently, ClinicalChemistry presented a very interest-ing Q&A on the use of blood glucosemeters to achieve tight glucose con-trol in patients in the ICU (3). Be-cause one of our ICUs participatedin the NICE-SUGAR trial, we reporthere some interesting and relevantdata that shed more light on theNICE-SUGAR trial, data that yieldmore questions than answers.
In our 30-bed general systemsICU at the University of AlbertaHospital, point-of-care glucose con-centrations can be measured in 2 dif-ferent ways: respiratory therapistsmeasure arterial blood gases, hemo-globin, electrolytes, and glucose val-ues with the Radiometer 800 bloodgas system (BGA) and nurses mea-sure arterial blood and capillary
1 Nonstandard abbreviations: NICE-SUGAR, Normo-glycemia in Intensive Care Evaluation and SurvivalUsing Glucose Algorithm Regulation; ICU, inten-sive care unit; BGA, blood gas system; BGM, bloodglucose meter.
Letters to the Editor
Clinical Chemistry 56:7 (2010) 1193

blood glucose with the LifeScan Sur-eStep Flexx blood glucose meter(BGM). Both the BGA and BGMglucose results are stored in a centrallaboratory data repository, and weretrieved Radiometer BGA andLifescan BGM glucose results thatwere run within 15 min of each otherfor individual patients. The numericdifferences between these paired val-ues graphed against the date of col-lection (represented by the pointdata) are shown in Fig. 1. The BGMresults were usually higher than theBGA results for the first 3 strip lots,with the difference averaging 0.83mmol/L or 13.6%. For the next 3strip lots, this BGM/BGA glucosebias was almost zero (0.03 mmol/L;1.4%). Neither of the manufactur-ers, Radiometer or Lifescan, could
offer any reason for these differencetrends.
Because many BGM systemsprovide artifactually high glucoseconcentrations in patients with lowhematocrits (4), we graphed theBGM/BGA differences against he-moglobin that was proportional tohematocrit and measured by usingthe Radiometer analyzer. [The mean(SD) hemoglobin concentrationswere very similar over the 2 periods,92.7 (16.9) vs 92.8 (18.1) g/L]. Thefirst 3 glucose reagent-strip lots weremore sensitive to the effects of he-moglobin compared to the next3 lots [glucose difference ��0.0195 � hemoglobin (mg/L) �2.41; r2 � 0.108; P � 0.0001 (first 3strip lots); glucose difference ��0.0103 � hemoglobin (mg/L)
�1.09; r2 � 0.0926; P � 0.0021 (last3 strip lots)]. It appears that many ofthe samples measured with the first 3lots of strips would have artifactuallyincreased glucose concentrations.Our hospital general systems ICUparticipated in the NICE-SUGARstudy, and the time of the data collec-tion for NICE-SUGAR coincidedwith the period during which wewere using lots 1, 2, and 3. Of theglucose values reported by our ICUfor the NICE-SUGAR patients, theLifeScan BGMs were the source ofthe most of the glucose values. In ac-cordance with the NICE-SUGARprotocol, high glucose values wouldbe treated. During the NICE-SUGAR study, our LifeScan BGMswere providing increased glucoseconcentration results on most of our
Fig. 1. Glucose differences (BGM � BGA) vs time in any patient who had arterial blood glucose measured on theRadiometer BGA and arterial or capillary blood measured on the LifeScan BGM within 15 minutes.
Six different strip lots were primarily used. The 15-point moving average of these numeric differences and the moving average of therelative differences are shown (relative difference data not presented). The numeric differences are represented by 6 different symbols,with each representing a different reagent strip lot. The lines represent lot-specific moving averages of the 237 differences (the darkline represents the moving average of the numeric differences; light line, the moving average of the relative [%] differences).
Letters to the Editor
1194 Clinical Chemistry 56:7 (2010)

ICU patients because the majorityhad low hemoglobin concentra-tions. Treatment of artifactual hy-perglycemia can cause hypoglycemia(5), which should be verified by themain laboratory or a point-of-careblood gas glucose measurement.BGM manufacturers produce multi-ple strip lots that should exhibit min-imum variation. It is possible thatother NICE-SUGAR study sites thatused LifeScan meters would be treat-ing such artifactual hyperglycemiaand thus provoking hypoglycemia. Itis important to know what propor-tion of participating institutionsused LifeScan meters. It is also im-portant to know the relative fre-quency of blood glucose measure-ments that were obtained by usingthe LifeScan BGM system in NICE-SUGAR study patients compared tomore accurate methods such as BGAglucoses. Finally, we should alsoknow the frequency of occasions inwhich there was subsequent corrob-oration of hyperglycemia by themain laboratory or by BGA glucoseanalysis. If a large proportion ofstudy participants used LifeScan sys-tems and relatively few of the hyper-glycemic episodes were verified byalternate methods, then perhaps theNICE-SUGAR study should be re-peated with more attention paidto the accuracy of the glucose-measuring device (6).
Author Contributions: All authors con-firmed they have contributed to the intellectualcontent of this paper and have met the following3 requirements: (a) significant contributions tothe conception and design, acquisition of data,or analysis and interpretation of data; (b) draft-ing or revising the article for intellectual content;and (c) final approval of the published article.
Authors’ Disclosures of Potential Con-flicts of Interest: Upon manuscript submis-sion, all authors completed the Disclosures ofPotential Conflict of Interest form. Potentialconflicts of interest:
Employment or Leadership: None declared.Consultant or Advisory Role: None declared.
Stock Ownership: G. S. Cembrowski, John-son and Johnson (immediate family mem-ber).Honoraria: G. S. Cembrowski, Radiometer.Research Funding: None declared.Expert Testimony: None declared.
Role of Sponsor: The funding organiza-tions played no role in the design of study,choice of enrolled patients, review and in-terpretation of data, or preparation or ap-proval of manuscript.
References
1. NICE-SUGAR Study Investigators, Finfer S, Chit-tock DR, Su SY, Blair D, Foster D, et al. Intensiveversus conventional glucose control in criticallyill patients. N Engl J Med 2009;360:1283–97.
2. Van den Berghe G, Schetz M, Vlasselaers D,Hermans G, Wilmer A, Bouillon R, Mesotten D.Intensive insulin therapy in critically ill patients:NICE-SUGAR or Leuven blood glucose target?J Clin Endocrinol Metab 2009;94:3163–70.
3. Sacks DB. Tight glucose control in critically illpatients: should glucose meters be used? ClinChem 2009;55:1580–3.
4. Lyon ME, Baskin LB, Braakman S, Presti S,Dubois J, Shirey T. Interference studies with twohospital-grade and two home-grade glucosemeters. Diabetes Technol Ther 2009;11:641–7.
5. Pidcoke HF, Wade CE, Mann EA, Salinas J, Co-hee BM, Holcomb JB, Wolf SE. Anemia causeshypoglycemia in intensive care unit patients dueto error in single-channel glucometers: methodsof reducing patient risk. Crit Care Med 2010;38:471–6.
6. Scott MG, Bruns DE, Boyd JC, Sacks DB. Tightglucose control in the intensive care unit: areglucose meters up to the task? Clin Chem 2009;55:18–20.
George S. Cembrowski*David V. Tran
Linda Slater-MacLeanDat Chin
R. T. Noel GibneyMichael Jacka
University of Alberta Hospital
Edmonton, Alberta, Canada
* Address correspondence to this author at:University of Alberta Hospital Site
Lab Med/Rm 4B1.24, WCM Center8440 112th St.
Edmonton, Alberta T6G 2B7, CanadaFax 780-407-8599
Email [email protected]
Previously published online atDOI: 10.1373/clinchem.2010.146217
The Effect of Hemolysis onCurrent Troponin Assays—AConfounding PreanalyticalVariable?
To the Editor:
The universal definition of myo-cardial infarction stipulates thedetection of an increase and/ordecrease in cardiac biomarkers[preferably troponin I (TnI)1 or T(TnT)], with at least 1 value�99th percentile of the upperreference limit, together with ev-idence of myocardial ischemia(1 ). With the emergence of moresensitive troponin assays, whatconstitutes a genuine increaseand/or decrease becomes criti-cally important (2 ). For analyti-cal values to be considered differ-ent, it has been suggested thatsuch values should vary by �3SDs of the variance of the mea-surement method and that a 20%change for troponins is greaterthan what would be expectedfrom analytical variation (1 ). Atlow troponin concentrations, ei-ther definition translates intosmall absolute changes. Good an-alytical precision is therefore crit-ically important, as is carefulconsideration of preanalyticalvariables, such as sample type andparticularly hemolysis. Hemoly-sis is known to be more prevalentin the emergency department en-vironment, with rates of up to20% of samples (3 ). Hemolysis isknown to cause interference inboth TnT and TnI assays (4 ), al-though such effects become evenmore important with the emer-gence of more sensitive troponinassays and the increased relianceon interpretation of small abso-lute changes. We therefore evalu-ated the degree of analytical inter-
1 Nonstandard abbreviations: TnI, troponin I; TnT,troponin T; HI, hemolysis index.
Letters to the Editor
Clinical Chemistry 56:7 (2010) 1195

ference from hemolysis withcurrently available troponin assays.
Erythrocyte hemolysates wereprepared according to the proce-dure of Meites (5 ) and added to 4unhemolyzed pools of heparinizedplasma with TnI concentrations of0.00, 0.03, 0.5, and 5 �g/L, as mea-sured with the Architect (AbbottDiagnostics), to produce a range ofhemolyzed plasma samples. Thehemoglobin concentration wasmeasured as a hemolysis index(HI) (calibrated in milligrams perdeciliter hemoglobin) on the Ab-bott c8000 analyzer.
TnI was measured with theAbbott Troponin I (840549/R6)assay on the Abbott Architect in-strument (99th percentile, 0.028�g/L; 10% CV, 0.032 �g/L) (2 )and the Ortho Clinical DiagnosticsVitros ECi instrument (99th per-centile, 0.034 �g/L; 10% CV, 0.034�g/L) (2 ). TnT was measured withthe Roche Troponin T STAT(04660307) assay (99th percentile,�0.01 �g/L; 10% CV, 0.03 �g/L)(2 ) and the Roche Troponin T hs
(05092744/190) assay (99th per-centile, 13 ng/L; 10% CV, 12 ng/L)on the ElecSys 2010 instrument(Roche Diagnostics) (2 ). Thewithin-batch CV was �3% for allpools without added hemolysate.
In the calendar month of Au-gust 2009, we assayed 966 samples(788 patients) from our emergencydepartment for Troponin I on theAbbott Architect and measured theHI on our Abbott c8000 analyzer.Nineteen percent of these sampleswere hemolyzed, and 786 samples(81%) were not hemolyzed (HI,0 –35 mg/dL). Of the hemolyzedsamples, 111 (12%) were slightlyhemolyzed (HI, 36 –100 mg/dL),43 (4%) were hemolyzed (HI, 101–250 mg/dL), and 26 (3%) weregrossly hemolyzed (HI, �250 mg/dL). Of the 788 patients, 177 (22%)had at least 1 hemolyzed sample,and 112 (63%) of these patientshad subsequent samples that werenot hemolyzed.
Current troponin assaysshowed different susceptibilities tointerference by hemolysis (Table
1). The Roche TnT assays bothshowed negative interference (upto 50% in low pool B for TroponinT hs) with increasing degrees of he-molysis, as previously described forthe fourth-generation Roche TnTassay (4 ). The Vitros ECi TnI assayshowed positive interference (upto 576% in low pool B), as previ-ously documented for a prior gen-eration of the same assay (4 ),whereas the Abbott Architect TnIassay appeared to be more robustto interference from hemolysis(�10% in low pool B).
These considerations are criti-cally important when interpretingchanges of 20% or 30% at low tro-ponin concentrations, whichtranslate into small absolutechanges in concentration. Initialsamples taken in the emergencydepartment are more likely to behemolyzed than samples takenlater in other areas; thus, an in-crease and/or decrease in troponinconcentration may be masked byhemolysis in either sample, de-pending on the assay. From our
Table 1. Troponin concentrations in 4 pools at 6 levels of hemolysis.
HI, mg/dL Hb
Abbott Troponin I, �g/L Vitros ECi Troponin I, �g/L
Pool A Pool B Pool C Pool D Pool A Pool B Pool C Pool D
12 0.000 0.032 0.444 4.170 0.002 0.050 0.482 4.360
43 0.000 0.029 0.454 3.858 0.069 0.081 0.532 4.400
77 0.000 0.030 0.437 3.946 0.094 0.119 0.547 4.280
132 0.000 0.026 0.423 3.871 0.120 0.174 0.574 4.270
235 0.000 0.027 0.425 3.760 0.187 0.255 0.658 4.250
392 0.000 0.029 0.477 3.540 0.284 0.338 0.825 4.080
Roche Troponin T STAT, �g/L Roche Troponin T hs, ng/L
Pool A Pool B Pool C Pool D Pool A Pool B Pool C Pool D
12 �0.010 �0.010 0.069 0.267 �3.00 19.26 87.32 273.70
43 �0.010 �0.010 0.069 0.264 �3.00 19.19 87.77 274.90
77 �0.010 �0.010 0.065 0.258 �3.00 19.22 87.47 271.30
132 �0.010 �0.010 0.054 0.233 �3.00 16.23 73.20 233.90
235 �0.010 �0.010 0.043 0.200 �3.00 11.46 60.10 192.30
392 �0.010 �0.010 0.032 0.170 �3.00 9.66 48.10 157.30
a Hb, hemoglobin.
Letters to the Editor
1196 Clinical Chemistry 56:7 (2010)

data, the confounding effects of he-molysis on the interpretation of se-rial changes in troponins vary ac-cording to what assay is being used.Laboratories should be aware ofthe influence of hemolysis andshould offer caveats regardingpotential interference whenappropriate.
Author Contributions: All authors con-firmed they have contributed to the intellec-tual content of this paper and have met thefollowing 3 requirements: (a) significant con-tributions to the conception and design, ac-quisition of data, or analysis and interpreta-tion of data; (b) drafting or revising the articlefor intellectual content; and (c) final approvalof the published article.
Authors’ Disclosures of Potential Con-flicts of Interest: No authors declared anypotential conflicts of interest.
Role of Sponsor: The funding organiza-tions played no role in the design of study,choice of enrolled patients, review and in-terpretation of data, or preparation or ap-proval of manuscript.
References
1. Thygesen K, Alpert JS, White HD on behalf ofthe Joint ESC/ACCF/AHA/WHF Task Force forthe Redefinition of Myocardial Infarction. Uni-versal definition of myocardial infarction. EurHeart J 2007;28:2525–38.
2. Apple FS. A new season for cardiac troponinassays: It’s time to keep a scorecard. Clin Chem2009;55:1303–6.
3. Ong MEH, Chan YH, Lim CS. Observational studyto determine factors associated with blood sam-ple haemolysis in the emergency department.Ann Acad Med Singapore 2008;37:745–8.
4. Snyder JA, Rogers MW, King MS, Phillips JC,Chapman JF, Hammett-Stabler CA. The impactof hemolysis on Ortho-Clinical Diagnostic’sECi and Roche’s Elecsys immunoassay sys-tems. Clin Chim Acta 2004;348:181–7.
5. Meites S. Reproducibly simulating hemolysis,for evaluating its interference with chemicalmethods [Letter]. Clin Chem 1973;19:1319.
Chris Florkowski*John Wallace
Trevor WalmsleyPeter George
2 Clinical Biochemistry Unit
Canterbury Health Laboratories
Christchurch, New Zealand
* Address correspondence to this author at:
Clinical Biochemistry Unit
Canterbury Health Laboratories
Hagley Ave.
Christchurch, New Zealand 8002
Fax 64-3-364-1460
E-mail [email protected]
Previously published online atDOI: 10.1373/clinchem.2009.140863
High-Sensitivity CardiacTroponin: Seeing the Woodfrom the Trees
To the Editor:
The perspective provided by Jaffeand Apple (1 ) regarding the land-mark publications in The New En-gland Journal of Medicine offers aninsightful commentary regardingthe clinical utility of the so-calledhigh-sensitivity cardiac troponinassays (2, 3 ).
We fully support the notionthat many of the assays evaluatedin these papers should be consid-ered contemporary rather thanhigh-sensitivity. The scorecard cat-egorization is a valuable tool forany clinical laboratory to assess theanalytical performance of theircardiac troponin assay (4 ). Jaffeand Apple incorrectly referencedthe high-sensitivity cardiac tropo-nin T (hs-cTnT) (Roche) in thestudy of Keller and colleagues. Inreviewing the Keller et al. article(2 ) and the supplementary meth-ods (available as an online appen-dix), we observed that the authorsused the current fourth-generationcTnT assay rather than the hs-cTnT assay for comparison be-tween methodologies.
It is interesting to note that thediagnostic utility of the AbbottcTnI, the Roche standard cTnT,and developmental cTnI assays issuperior when using the 99th per-centile cutoff rather than the 10%
coefficient of variation, at the costof specificity (3 ). Diagnostically,they perform as well as the hs-cTnT, calling into question the truesensitivity of this assay. Many clin-ical laboratorians still favor the10% coefficient of variation cutoffvalue over the 99th percentile, pre-sumably as this is within a marginof safety with which they are bothfamiliar and comfortable and thatis applied to other immunoassaytests.
The drive to use the 99th per-centile is warranted, as demon-strated by the studies of Keller et al.and Reichlin et al. (2, 3 ); however,the real challenge to adequately as-sess clinical sensitivity and specific-ity will come from prospectivestudies of unselected chest pain pa-tients presenting to the emergencydepartment.
The newer hs-cTn assays indevelopment may prove to be su-perior diagnostically. Analytically,both the contemporary and high-sensitive assays challenge the per-formance of current immunoassaytechnology. The development ofother detection methods such assingle-molecule-counting technol-ogy may be the appropriate alter-native (5 ), if this technology can beadapted for large high-throughputanalyzers with reduced turn-around time without compromis-ing analytical performance.
Author Contributions: All authors con-firmed they have contributed to the intellec-tual content of this paper and have met thefollowing 3 requirements: (a) significant con-tributions to the conception and design, ac-quisition of data, or analysis and interpreta-tion of data; (b) drafting or revising the articlefor intellectual content; and (c) final approvalof the published article.
Authors’ Disclosures of Potential Con-flicts of Interest: No authors declared anypotential conflicts of interest.
Role of Sponsor: The funding organiza-tions played no role in the design of study,choice of enrolled patients, review and in
Letters to the Editor
Clinical Chemistry 56:7 (2010) 1197

terpretation of data, or preparation or ap-proval of manuscript.
References
1. Jaffe AS, Apple FS. High-sensitivity cardiactroponin: hype, help, and reality. Clin Chem2010;56:342–4.
2. Keller T, Zeller T, Peetz D, Tzikas S, Roth A, CzyzE, et al. Sensitive troponin I assay in early diag-nosis of acute myocardial infarction. N EnglJ Med 2009;361:868–77.
3. Reichlin T, Hochholzer W, Bassetti S, Steuer S,Stelzig C, Hartwiger S, et al. Early diagnosis ofmyocardial infarction with sensitive cardiac tro-ponin assays. N Engl J Med 2009;361:858–67.
4. Apple FS. A new season for cardiac troponinassays: it’s time to keep a scorecard. Clin Chem2009;55:1303–6.
5. Wu AH, Agee SJ, Lu QA, Todd J, Jaffe AS.Specificity of a high-sensitivity cardiac troponin Iassay using single-molecule-counting technol-ogy. Clin Chem 2009;55:196–8.
David C. Gaze*Paul O. Collinson
Clinical Blood Sciences
St George’s Healthcare NHS Trust
London, UK
* Address correspondence to this author at:
Clinical Blood Sciences
St George’s Healthcare NHS Trust
London, SW17 0QT UK
Fax �44-(0)20-8725-5868
E-mail [email protected]
Previously published online atDOI: 10.1373/clinchem.2010.147215
Comment on “High-SensitivityCardiac Troponin: Hype, Help,and Reality”
To the Editor:
We thank Jaffe and Apple (1 ) fortheir interest in our study. In theirperspectives article, they com-mented on details of our study andthe study by Keller et al., whichwere both published recently in theNew England Journal of Medicine(2, 3 ). Although we fully agreewith several of their statements, westrongly disagree with others. It is
detrimental to the much-neededinterdisciplinary discussion on thebest possible clinical use of sensi-tive cardiac troponin assays whenthe discussion is based on incorrectstatements. Unfortunately, theJaffe and Apple perspective con-tains 2 important errors.
First, and of most importance,Jaffe and Apple (1 ) asked, “Howdid these studies deal with theproblem of increased [cardiac tro-ponin] concentrations produced[by diseases other than acute myo-cardial infarction (AMI)1]?” andstated, “Not very well. For the mostpart, the authors . . . used a [car-diac troponin] concentrationabove the cutoff value as the solecriterion for the diagnosis of acutecoronary syndrome (ACS).” Theyalso stated, “The presence of achanging . . . pattern, which is anessential part of the criteria for thediagnosis of AMI in all the guide-lines, was used in only a subset ofpatients in the Reichlin et al. article. . . .” These statements are incor-rect in 2 respects. On the one hand,AMI was defined in our study in allpatients in full agreement with thecurrent universal definition ofAMI (4 ), which requires evidenceof myocardial necrosis with achanging pattern associated withclinical signs of myocardial isch-emia, as stated clearly in the Meth-ods section of our report (2 ). Ne-crosis was diagnosed on the basis ofa rising and/or falling pattern ofthe cardiac troponin concentra-tion, with at least 1 value above the99th percentile at a level of impre-cision of �10% (2 ). On the otherhand, noncoronary conditionsthat increased cardiac troponinconcentrations according to con-ventional cardiac troponin assayswere not called “true positives” butwere included in the diagnostic
group “cardiac symptoms fromcauses other than coronary arterydisease” (2 ). Ninety-five (13%) of718 patients were adjudicated inthis group, and 16 of these patientshad acute cardiac necrosis of an or-igin other than coronary artery dis-ease (e.g., myocarditis, tachyar-rhythmias, or acute heart failure).
Second, Jaffe and Apple (1 )argue that the incidence of ACS ismuch lower in the US than the in-cidence reported in the 2 studiespublished in the New England Jour-nal of Medicine (2, 3 ) and state thatthe incidence of ACS was 46% inour study. This statement is incor-rect. The incidence of ACS in ourstudy as reported in the Resultssection of the report was 33% (2 ).In addition, results from a recentlycompleted multicenter study thatincluded consecutive patients pre-senting to the emergency depart-ment with symptoms suggestive ofAMI showed that the difference inthe incidence of local emergencydepartment diagnosis of ACSamong centers in the US [range,4%– 40%; data on file at FAST-TRAC Data Management Center,San Diego, CA (Dr. Greg Shipp,Nanosphere, personal communi-cation, January 15, 2010)] wasgreater by far than potential differ-ences between the US and Europe.Therefore, we think that the dis-ease incidence encountered in anindividual emergency departmentis predominantly determined bythe details of the local patient flow,such as a competing high-volumecatheterization laboratory in aneighboring hospital that receivesmost high-risk and high-probability ambulance cases, orsuch as local hospital standardsthat guide chest pain patients onlyto the emergency department aslong as they are perceived as lowrisk and low probability and thattriage all high-probability patientsdirectly to a coronary care unit.
We hope that these clarifica-tions help to advance the important
1 Nonstandard abbreviations: AMI, acute myocar-dial infarction; ACS, acute coronary syndrome.
Letters to the Editor
1198 Clinical Chemistry 56:7 (2010)

discussion on the best clinical use ofsensitive cardiac troponin assays.
Author Contributions: All authors con-firmed they have contributed to the intellec-tual content of this paper and have met thefollowing 3 requirements: (a) significant con-tributions to the conception and design, ac-quisition of data, or analysis and interpreta-tion of data; (b) drafting or revising the articlefor intellectual content; and (c) final approvalof the published article.
Authors’ Disclosures of Potential Con-flicts of Interest: Upon manuscript submis-sion, all authors completed the Disclosures ofPotential Conflict of Interest form. Potentialconflicts of interest:
Employment or Leadership: None declared.Consultant or Advisory Role: C. Mueller,BRAHMS and Abbott Laboratories.Stock Ownership: None declared.Honoraria: C. Mueller, Biosite, AbbottLaboratories, BRAHMS, Siemens, andRoche.Research Funding: C. Mueller, Abbott Lab-oratories, BRAHMS, Nanosphere, Siemens,and Biosite.Expert Testimony: None declared.
Role of Sponsor: The funding organiza-tions played no role in the design of study,choice of enrolled patients, review and in-terpretation of data, or preparation or ap-proval of manuscript.
References
1. Jaffe AS, Apple FS. High-sensitivity cardiactroponin: hype, help, and reality. Clin Chem2010;56:342–4.
2. Reichlin T, Hochholzer W, Bassetti S, Steuer S,Stelzig C, Hartwiger S, et al. Early diagnosis ofmyocardial infarction with sensitive cardiac tro-ponin assays. N Engl J Med 2009;361:858–67.
3. Keller T, Zeller T, Peetz D, Tzikas S, Roth A, CzyzE, et al. Sensitive troponin I assay in early diag-nosis of acute myocardial infarction. N EnglJ Med 2009;361:868–77.
4. Thygesen K, Alpert JS, White HD. Universal def-inition of myocardial infarction. J Am Coll Car-diol 2007;50:2173–95.
Tobias Reichlin2,3
Raphael Twerenbold2
Christian Mueller2*
Departments of 2 Internal Medicine
and 3 Cardiology
University Hospital Basel
Basel, Switzerland
* Address correspondence to this author at:
Department of Internal Medicine
University Hospital Basel
Petersgraben 4
CH-4031 Basel, Switzerland
Fax �41-61-265-53-53
E-mail [email protected]
Previously published online atDOI: 10.1373/clinchem.2010.147728
In Reply
We are pleased to have the oppor-tunity to clarify some issues that,due to word count restrictions,were not as clear as would havebeen ideal.
The issue of the use of a �(changing pattern) is a good exam-ple. Deltas are important for lowercardiac troponin concentrationsbecause most chronic increases (anoccasional dialysis patient ex-cepted) are modest. At low concen-trations, the � takes into accountthe imprecision of the assay and, ifpossible, biological variation. The� for the cardiac troponin T(cTnT)1 assay used for the goldstandard diagnosis was unstated.Clinicians think of a changing pat-tern as any alteration, and that isnot the case. At the Mayo Clinic,we require a 0.03-�g/L change atlow cTnT concentrations, which is300% from 0.01 �g/L and 100%from 0.03 �g/L. At higher concen-trations, lower � values are usedbecause the imprecision is less. Nocriteria were provided for the com-parison assays or for the novelhigh-sensitivity assay (1 ). Table 3Cin the supplementary material forthe report of Reichlin et al. (1 ),where this matter is evaluated, pro-
vides no criteria. We have recentlyestablished that the conjoint bio-logical and analytical variationwith the high-sensitivity cTnT as-say is 85% in the short term (2 ).Kavsak et al. used a 20% change onthe basis of an imprecision profilewith the Beckman assay (3 ). It ap-pears that Reichlin et al. (1 ) al-lowed clinical judgment ratherthan criteria to be used, with theconsequence varying from em-bracing a change of 0.01 �g/L (a20% change at 0.05 �g/L) tosomething more reasonable. Inaddition, most cardiac troponinassay results are reported in hun-dredths, and rounding issues willthus alter percentage changes. Itis not clear that these authors un-derstand these issues, which af-fect clinical classifications andtriage decisions.
Who was or was not includedin the various diagnostic groupsand what criteria were used are alsounclear. Even now, how many pa-tients had increases in cTnT is un-clear. The authors say that 95(13%) of 718 patients were in thegroup, but only 16 had necrosis. Ifindeed 13% had increases due tononcoronary causes, it would havebeen important to comment on thespecificity of rising and/or fallingcTnT concentrations for coro-nary disease in patients with chestdiscomfort because noncoronaryincreases were nearly as prevalentas acute myocardial infarction(AMI). If only 16 patients fit andthe others had typical cTnT valuesbut alternative diagnoses, thatmight be less necessary. The crite-ria for these decisions are notstated. For example, for patientswho present late after AMI and thecardiac troponin concentration isnear its peak, a changing patternmight not be seen. Was this possi-bility taken into account? If pa-tients did not have acute lesions ac-cording to the angiography resultsbut had severe coronary artery dis-ease, were they then classified as
1 Nonstandard abbreviations: cTnT, cardiac troponinT; AMI, acute myocardial infarction; ACS, acutecoronary syndrome; STEMI, ST-elevation myocar-dial infarction; ROMICAT, Rule Out MyocardialInfarction Using Computer-Assisted Tomography.
Letters to the Editor
Clinical Chemistry 56:7 (2010) 1199

having a noncoronary etiology forchest pain, stable angina, or unsta-ble angina? If patients had classicsymptoms but did not have ob-structive disease, were they diag-nosed with acute coronary syn-drome (ACS), AMI, or noncardiacpain? Some patients, especiallywomen, present this way and likelyhave ACS (4 ). It is important toknow whether these patients wereincluded in the ROC curve analysesbecause they would influence theanalyses.
The issue of incidence andhow it affects the data are impor-tant. There are differences betweenthe US and Europe in most of thechest pain studies, likely due tohow patients are screened. In Eu-rope, there often are cardiologistsin the emergency department. Inthe US, that 46% of patients wouldhave acute cardiac disease in achest pain cohort would be un-usual. This percentage includesAMI, unstable angina, and cardiacsymptoms from other “noncardiacdiseases” [page 861 of the authors’report (1 )]. The issue is not thenumber but an important concep-tual issue. If one includes all the pa-tients with ST-elevation myocar-dial infarction (STEMI) and overtnon-STEMI, the pretest probabil-ity that an increased cardiac tropo-nin concentration will be associ-ated with ACS is higher than if oneincludes only patients for whomthe diagnosis is unclear. Such agroup, judging from ROMICAT(Rule Out Myocardial InfarctionUsing Computer-Assisted Tomog-raphy) trial data, has an incidence
of coronary artery disease of about8%. This changes the pretest prob-ability of disease and exaggeratesthe predictive accuracies of theapproach. This is the point of therecent report of Januzzi and col-leagues (5 ).
Author Contributions: All authors con-firmed they have contributed to the intellec-tual content of this paper and have met thefollowing 3 requirements: (a) significant con-tributions to the conception and design, ac-quisition of data, or analysis and interpreta-tion of data; (b) drafting or revising the articlefor intellectual content; and (c) final approvalof the published article.
Authors’ Disclosures of Potential Con-flicts of Interest: Upon manuscript submis-sion, all authors completed the Disclosures ofPotential Conflict of Interest form. Potentialconflicts of interest:
Employment or Leadership: None declared.Consultant or Advisory Role: A.S. Jaffe,Beckman Coulter, Siemens, Inverness Med-ical Innovations, Critical Diagnostics, Sin-gulex, Pfizer, GlaxoSmithKline, Merck, andTethys Bioscience; F.S. Apple, Abbott Diag-nostics, Ortho Clinical Diagnostics, Beck-man Coulter, and Biosite.Stock Ownership: None declared.Honoraria: F.S. Apple, Abbott Laborato-ries, Biosite/Inverness, Beckman Coulter,Ortho Clinical Diagnostics, and Instrumen-tation Laboratories.Research Funding: F.S. Apple, Abbott Di-agnostics, Siemens, Ortho Clinical Diagnos-tics, Roche Diagnostics, Nanosphere, Bio-RadLaboratories, Response Medical, Radiometer,BRAHMS, and Becton Dickinson.Expert Testimony: None declared.
Role of Sponsor: The funding organiza-tions played no role in the design of study,choice of enrolled patients, review and in-terpretation of data, or preparation or ap-proval of manuscript.
References
1. Reichlin T, Hochholzer W, Bassetti S, Steuer S,Stelzig C, Hartwiger S, et al. Early diagnosis ofmyocardial infarction with sensitive cardiactroponin assays. N Engl J Med 2009;361:858 –67.
2. Vasile VC, Saenger AK, Kroning JM, Jaffe AS.Biological and analytical variability of a novelhigh-sensitivity cardiac troponin T assay. ClinChem 2010;56:1086–90.
3. Kavsak PA, MacRae AR, Lustig V, Bhargava R,Vandersluis R, Palomaki GE, et al. The impact ofthe ESC/ACC redefinition of myocardial infarc-tion and new sensitive troponin assays on thefrequency of acute myocardial infarction. AmHeart J 2006;152:118–25.
4. Martinez MW, Babuin L, Syed IS, Feng DL, MillerWL, Mathew V, et al. Myocardial infarction withnormal coronary arteries: a role for MRI? ClinChem 2007;53:995–6.
5. Januzzi JL Jr, Bamberg F, Lee H, Truong QA,Nichols JH, Karakas M, et al. High-sensitivitytroponin T concentrations in acute chest painpatients evaluated with cardiac computed to-mography. Circulation 2010;121:1227–34.
Allan S. Jaffe2*
Fred S. Apple3
2 Mayo Clinic
Rochester, MN3 Hennepin County Medical Center
and University of Minnesota
Minneapolis, MN
* Address correspondence to this author at:
Mayo Clinic
Gonda Building, 5th Flr.
200 First St. S.W.
Rochester, MN 55905
Fax 507-266-0228
E-mail [email protected]
Previously published online atDOI: 10.1373/clinchem.2010.148460
Letters to the Editor
1200 Clinical Chemistry 56:7 (2010)