Embed Size (px)
Citation preview
11/09
NUR240Urinary Tract Stressors:
UTICystitis
UrolithiasisBladder Ca
PKDARF/CRF
Joy Borrero, RN, MSN
Kidney Physiology
Primary role of kidney is regulation of fluid and electrolyte balance, additional life preserving functions include:
• Excretion of metabolic wastes-micturition• Water and salt regulation• Maintenance of acid – base balance.
http://www.kidney.org/• Regulation of BP• Stimulation of RBC production• Regulation of calcium – phosphate metabolism.
Urinary Tract
• Upper urinary tract:• Kidneys – 2 bean shaped organs,
composed of nephrons. A complex vascular system. Each weighs about 8oz.
• Ureters – extensions of the renal pelvis and empty into the bladder.
• Lower urinary tract:• Bladder, urethra and prostate gland
(males).
Renal and Urinary Terms
Azotem ia Uremia Dysuria Frequency
Hesitency Micturation Nocturia Oliguria
Polyuria Uremia Urgency Anuria
Serum creatinine
Blood urea nitrogen
BUN/Creatinine Ratio
Glomerular FiltrationRate
Assessment of Renal and Urinary Tract Systems
• History of disease or trauma• Urinary patterns• Relevant meds• Allergies• Fluid status-edema• Pruritis• BP• LOC, level of alertness• Pain assessment• Numbness and tingling of extremities• GI symptoms- anorexia, N&V, diarrhea
Urinary Tract Pain
• Kidney- dull ache in costovertebral angle and radiates to umbilicus
• Ureteral – pain in back that radiates to abdomen, upper thigh, testes and labia
• Bladder- low abdominal or over suprapubic area
• Renal Colic- flank pain radiating to lower abdomen or epigastric area, N&V
Diagnostic Tests
• IVP• CAT Scans• Renal angiography• Ultrasounds• Cystoscopy- Dx and
Tx• Renal Bx-
Open/Closed
• UA, urine electrolytes, osmolality
• C&S• Serum creatinine and
BUN• Hgb and Hct• Creatinine clearance- 24h
collection• KUB
Cystoscopy
Pre procedure: bowel prep, NPO if general anesthesia, IVF for adequate urine flow
Post procedure: BR for short period Pink tinged urine is comon, retention may
occur Pain in back, bladder spasms and a feeling
of fullnessEncourage large amts of fluids
Urinary tract infections-described by location in the tract
• UTI – dysuria, frequency, urgency• Assessment – flank pain, cloudy urine, possible
fever. WBC’s in urine.• Treatment with antibiotics:
Fluoroquinolones(Cipro), nitrofurantoin(Macrobid), Sulfonamides (Septra, Bactrim)• Prevention: void before and after sex.• Wipe front to back, showers better than baths.• No perfumes to perineal area.• Avoid sitting in wet bathing suits• Avoid pantyhose with slacks or tight clothing
UTI-Lower and Upper
• Risk Factors:• Aging • Increased incidence with DM• Increased risk of urinary stasis• Impaired immune response• Females: short urethra, cystocele, rectocele• Males: BPH• Obstructions: tumor, calculi, strictures
EBP- UTI Bundles
• Assess daily for need for catheter
• Foley bag below level of bladder
• Closed system
• Secure cath to prevent movement, tugging
• Use of smallest size catheter possible
Cystitis
• Most common UTI (superficial, bladder mucosa)
• Manifestations:dysuria, frequency, urgency, nocturia, foul odor urine, hematuria
• Older patients:nocturia, incontinence, confusion, behavioral changes, lethargy, anorexia, fever or hypothermia
Dx for cystitis
• UA
• Urine for Gram Stain
• Urine for C & S
• Evaluation of urinary tract
Interventions
Uncomplicated:1. Single dose regimen2. AntispasmodicsRecurrent or chronic1. Sulfonamides2. Antiseptics3. Analgesics4. Surgical Management
Management of Cystitis
• Increase fluid intake
• Acidify urine
• Ascorbic acid
• Avoid bladder irritants
• Antibiotics based on C&S
• Patient teaching
Upper Urinary Tract Infections
• Pyelonephritis: inflammation of kidney caused by bacterial infection following a bladder infection
• Infection begins in lower urinary tract with organisms ascending into renal pelvis
• E coli causes most cases of pyelonephritis
• Affects filtration,reabsorption and secretion = decrease in renal function
Risk Factors
• Women over age 65• Older men with prostate problems• Chronic urinary stone disorder• Spinal cord injury• Pregnancy• Congenital malformations• Bladder tumors• Chronic illness: HTN, DM, chronic cystitis• Recurrence is common
Physical Assessment
• Patient presents with acute distress
• Hx of dysuria, frequency, urgency and other signs of cystitis
• Costovertebral tenderness
• Fever, chills, nausea and flank pain
• N & V, malaise, fatigue
• Cloudy urine or hematuria
Diagnostic Assessment
• UA and C&S
• WBC with diff
• Blood Cultures
• Serum creatinine and BUN
• CRP-C-reactive protein
• ESR
• KUB, IVP
Nursing Interventions
• Pain management
• Antibiotic therapy
• Increase fluid intake
• Monitor temperature
• Provide emotional support
• Assist with personal hygiene
• Follow-up urine cultures
Assess for Complications
• Septic shock
• Renal Failure
• Hypertension
Urolithiasis
• Etiology- presence of calculi (stones) in the urinary tract, by an unknown cause
• Recurrence is increased 35-50% in pt with + family hx or if first stone occurs <25 yrs of age
• Increased incidence in males• Majority of stones (75%) are composed of Ca
oxalate or Ca phosphate• Hi doses of Vitamin C• Conditions causing urinary stasis, dehydration,
urinary retention
Physical Assessment
• Pain, obstruction, tissue trauma with secondary hemorrhage and infection
• Sharp, severe pain (renal colic) with sudden onset deep in lumbar region around to side
• N & V• Urinary frequency or dysuria• Pallor, diaphoresis• VS:• Oliguria, anuria, hematuria
Diagnostic Assessment
• UA- RBCs, WBCs, bacteria, turbidity,odor
• Serum Ca, PO4, Uric Acid levels
• Elevated serum WBC if infection is present
• KUB, IVP, Xrays, Ultrasound
Non-surgical Management
• Pain management- MSO4, NSAIDS• Antispasmotics-Ditropan, Pro-Banthine• Antiemetics- Zofran• Strain all urine- send stones for analysis• Increase fluid intake to 3000mL/day• Client education re: meds/diet
Methods of Stone Removal
• Stenting
• ESWL- Extracorporeal Shock Wave Lithotripsy
• Retrograde ureteroscopy/cystoscopy
• Percutaneous or open ureterolithotomy/pyelolithotomy/nephrolithotomy
Urinary Drainage Tubes
Ureteral Stents
• Maintain ureteral flow in pts with ureteral obstruction
• Divert urine
• Promote healing of ureter
• Maintain patency of ureter after sugery
• Temporary or permanent-inserted via nephrostomy tube, cystoscopy or open sx.
Nephrostomy Tubes
• Catheter is placed into renal pelvis for urine drainage (placed in flank area)
• Relieve obstruction, route for insertion of ureteral stent
• Drainage for when ureter doesn’t drain• Administer meds, biopsy• Never clamp a nephrostomy tube-can lead to
pyelonephritis• Never irrigate without specific order• Monitor urine output
Nursing Interventions in client education
• Restrictions based on stone analysis• Ca Phosphate- Limit foods high in animal
protein, limit Na and Ca intake• HCTZ- to increase Ca reabsorption• Ca Oxalate- Limit oxalate sources: spinach,
black tea, cocoa, beets, pecans, limit Na intake• Uric Acid: Limit foods high in purines: organ
meats, poultry, fish, gravies, red wine and sardines. Allopurinol (Zyloprim)
Assess for Complications
• Hydronephrosis
• Infection
• Ureteral obstruction
Bladder Cancer
• Etiology: about 54,000 new cases yearly, more common in >age 60
• Industrial exposure
• Long term use of Cyclophosphamide (Cytoxan) and Aziothioprine (Imuran)
• Tobacco use
• Secondary to mets
Diagnostic Assessment
• Urinalysis-presence of gross or microscopic hematuria
• Cystoscopy-Bladder-wash specimens and bladder biopsy
• CT scans and MRI –to assess for mets
Physical Assessment
• Painless hematuria- major sign
• Assess general health, exposure to cigarette smoke, harmful environmental agents
• Changes is urinary habits
Nonsurgical Interventions
• Intravesical immunotherapy- instillation into the bladder
Bacille Calmette-Guerin (BCG)
• Intravesical chemotherapy-mitomycin (Mutamycin), Doxorubicin (Adriamycin)
• Complications: bladder irritation, frequency, dysuria, contact dermatitis
• Systemic chemotherapy
Surgical Interventions
• Radiation used to reduce tumor size preop
• Cystoscopic tumor resection by excision, fulguration, laser photocoagulation
• TURBT- Transuretheral Resection of Bladder Tumor
• Simple or radical cystectomy-urinary diversion necessary (ileal conduit)
Methods of Urinary Diversion After Cystectomy
Urinary Diversion- divert urine away from kidney and leaves body via another route
1.Continent urinary diversion- ureters implanted into portion( pouch) of ileum (reservoir) for urine, stoma to abdomen
2.Incontinent diversions: ileal conduit
3.Uretersigmoidostomy
4. Bladder reconstruction, neobladder
Post-op Care
• Routine post op care including pain management
• Disturbed body image• Risk for impaired skin integrity• Assess urinary drainage• Sexual dysfunction• Pt and family education re: meds, fluids, care of
urinary diversion system• Referral to www.acs.org and local support
groups
PKDPolycystic Kidney Disease
• Congenital disorder-grapelike clusters of cysts in the nephrons, progressive
• Affects 250,00-500,000 people in the US• Men=Women• S&S: abdominal or flank pain, HTN,
nocturia, Increased abdominal girth, constipation, bloody or cloudy urine, kidney stones
• Renal insufficiency and CRF by age 50-60
Diagnostic Assessment
• UA-proteinuria, hematuria
• Urine C&S
• Rising BUN and Creatinine levels
• Decreased creatinine clearance
• Renal sonograms,CT and MRI
Interventions
• Mainly supportive- prevent renal damage from HTN, UTI, obstruction
• Pain management-caution with NSAIDS and ASA
• Antibiotic tx for UTIs• Constipation prevention• HTN control- ACE inhibitors• Diet management- Low NA, protein• Emotional support
Acute and Chronic Renal Failure
Acute renal failure (ARF)
Three causes of ARF:
• 1. Prerenal
• 2. Intrarenal (intrinsic)
• 3. Postrenal
1.Prerenal- conditions that cause decreased cardiac output: shock, CHF, pulmonary embolism, sepsis, anaphylaxis,hypotension
ARF
2. Intrarenal - caused by damage to renal tissue.
• Causes – glomeruonephritis,infection,drugs pyelonephritis, vasculitis, acute tubular necrosis (ATN), tumors
3. Postrenal- obstructions of outflow of urine: calculi, tumors, atony of bladder, urethral stricture, trauma
4 Phases of ARF
• Onset
• Oliguric
• Diuretic
• Recovery
1.Onset
ARF
Oliguric phase – urinary output decreased. Renal insult,gradual accumulation of
nitrogenous wastes (BUN and creatinine), can last hrs to 3 weeks.
• Increasing BUN, hyperkalemia, metabolic acidosis, hypocalcemia, hypermagnesemia, hyperphosphatemia.
• As plasma levels of nitrogenous wastes increase changes in:
• Oxygenation, metabolism, immune response, perception and coordination result.
ARF
3.Diuretic phase – high output phase, up to 10L/day. This phases lasts 1 – 2 weeks.
4.Recovery phase – begins when BUN stabilizes at normal, client begins to return to normal activities.
• The mortality rate for ARF- greater than 50% and for those requiring dialysis, between 60 -90%
• Prerenal is the most common cause and is usually reversible with prompt interventions
ARF
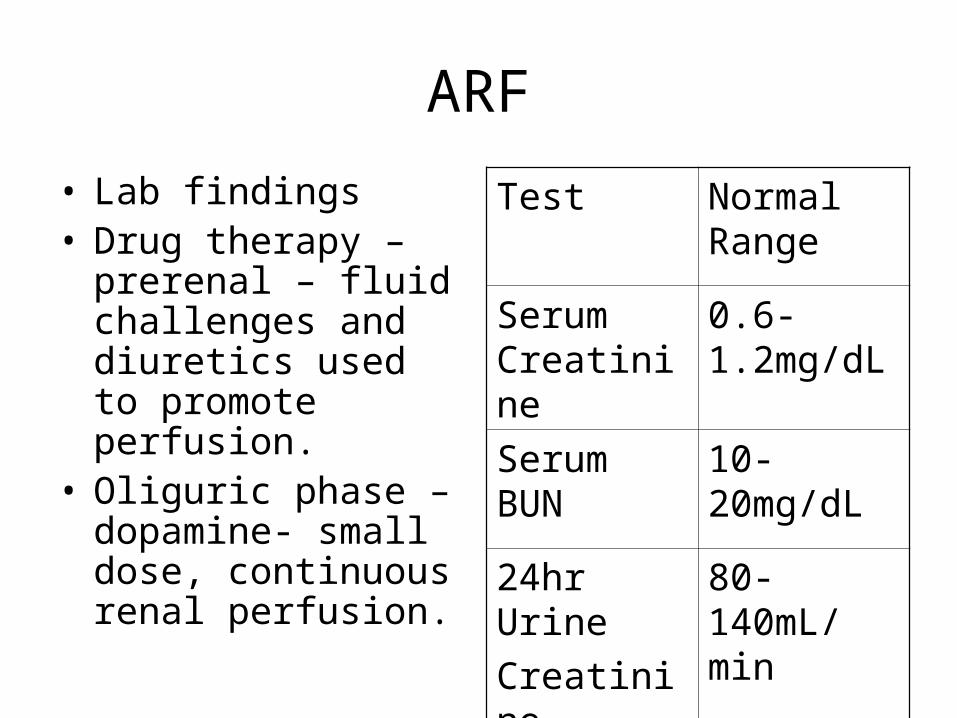
• Lab findings• Drug therapy –
prerenal – fluid challenges and diuretics used to promote perfusion.
• Oliguric phase – dopamine- small dose, continuous renal perfusion.
Test Normal Range
Serum Creatinine
0.6-1.2mg/dL
Serum BUN
10-20mg/dL
24hr Urine
Creatinine
Clearance
80-140mL/min
ARF
• Diet – high calorie diet needed for catabolic state, if client cannot eat enough, then TPN is considered.
• During the oliguric phase of ARF, the following diagnoses may apply :
• High risk for fluid volume excess
• High risk for injury
• High risk for altered nutrition.
ARF- Physical Assessment
1.Prerenal – hypotension, tachycardia, decreased cardiac output and CVP, decreased urine output and lethargy.
2. Intrarenal and postrenal-:
• Renal – oliguria or anuria
• Cardiac- hypertension, tachycardia, JVD, increased CVP, peripheral edema, efffusions,
ARF- Assessment
• Respiratory – SOB, orthopnea, crackles, pulmonary edema.
• GI – anorexia, nausea, vomiting, flank pain,metallic taste, gastritis
• Neuro- lethargy, headache, tremors, confusion, insomnia, seizures
• Hematology-anemia, bruising• Weight gain. 1kg=approx 1L fluid retained
Management and Prognosis of ARF
• Tx precipitating cause• Fluid restriction (500-600mL) plus fluid
loss• Nutritional management• Measures to lower serum K• Phosphate binding agents• TPN or enteral nutrition• Initiation of dialysis is necessary
Nursing Management & Interventions
1. Fluid volume deficit r/t…2. Fluid volume excess r/t…3. Nutrition: Less than body requirements r/t4, Impaired gas exchange r/t…5. PC: Hyperkalemia r/t….6. PC Metabolic acidosis r/t…7. PC Decreased Calcium r/t…
• The patient is a 64-year-old man. He visits the primary care provider because of mild lower abdominal pain, decreased urine output, and increased shortness of breath. He is 5 feet, 8 inches tall and weighs 246 pounds. The only drugs he takes include a daily multivitamin, a beta blocker, and occasionally acetaminophen for headache. His past medical history includes kidney stones 1 year ago and mild hypertension over the past 5 years. Physical assessment reveals bilateral crackles in the lung bases. Vital signs are T, 98.8 F; P, 96/min, R, 28/min, and BP, 148/92.
• 1. For which type(s) of acute renal failure is he at risk? Why?• 2. Do any of his usual drugs increase his risk for ARF? Which one(s) and
why?• 3. Is there any specific assessment data you could obtain without a
prescription to evaluate his risk for acute renal failure? If so, which ones and why?
• • The physician prescribes these interventions:• IV placement with a 20-gauge cannula, NS at 20 mL/hr• Accurate intake and output• Ibuprofen 600 mg orally• Furosemide 40 mg IV
Chronic renal failure (CRF)
• CRF is a chronic,progressive, irreversible disease, leading to end stage renal disease
• Five stages:• Stage 1- diminished renal reserve, increased
BP, increased pressure on glomerular apparatus, decreased ability to concentrate urine- nocturia and polyuria.
• Stage 2 – Renal Insufficiency- metabolic wastes begin to accumulate
CRF
• Stage 3- End stage renal disease, excessive amounts urea and creatinine in blood.
• Treatment by dialysis is necessary.• Sodium: • Early in CRF – hyponatremia, polyuria
causes sodium depletion. • Later, ESRD – sodium retention – but
dilutional hyponatremia (masked by fluid volume excess).
CRF
• Potassium – hyperkalemia – 7 -8 meq/L, ECG changes and fatal dysrhythmias.
• Acid – base balance: Acid excretion (H ions)- restricted results in metabolic acidosis. Kussmaul respirations.
• Calcium and phosphate – demineralization.
• Uremic pruritis- toxic accumulation of nitrogenous wastes.
CRF- Affects all body systems
• Cardiac Alterations• Hypertension • CHF and LV hypertrophy• Uremic Pericarditis• Hematologic Alterations• GI alterations• MS• Neuro• Dermatological• Endocrine
Goals of Therapy
• Retain kidney function and maintain homeostasis as long as possible
• Improve nutrition• Monitor electrolytes• Manage anemia• Control HTN• Maintain glycemic control• Emotional support
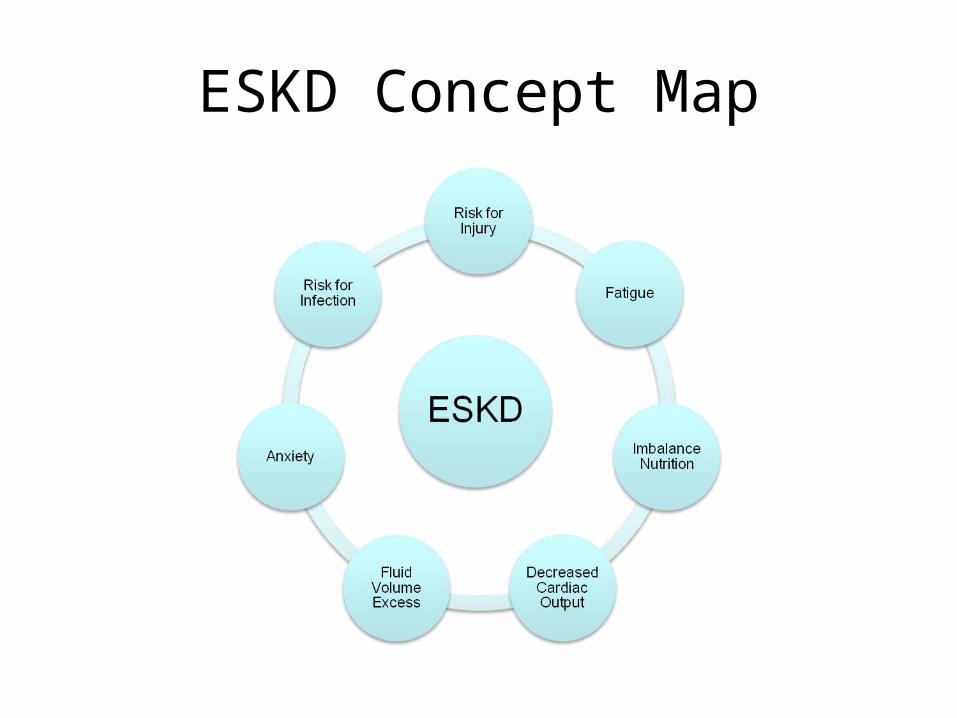
ESKD Concept Map
CRF
• Common Nursing diagnoses:
• 1. Altered nutrition less than body requirements r/t nausea, vomiting, decreased appetite, effects of catabolic state, decreased LOC, altered taste, or dietary restrictions.
CRF- Interventions
• Dietary restrictions: limit protein intake• Limitation of fluid intake• Restriction of K, NA, phosphorous• Administration of Vitamins and minerals• Adequate calories to meet metabolic
demands• Collaborate with MD and dietician
CRF
• Fluid volume excess r/t inability of kidney to maintain body fluid balance.
• Interventions: Fluid restriction depends on-– Urinary output– Based on fluid wt. gain– With hemodialysis, 500 -700 ml/day plus
amount of urinary output.
Nursing Diagnoses
• Impaired skin integrity
• Risk for injury
• Activity intolerance
• Constipation
• Diarrhea
• Anticipatory Grieving
CRF- Drug Therapy
Cardiac glycosides: digoxin• Monitor for signs and symptoms of toxicity
and hypokalemiaVitamins and minerals- FeSo4 and Folic
AcidErythropoietin- Epogen, ProcritPhosphate Binders- Renagel, TumsStool Softeners- Colace
Assessment for patients with CRF
• Assess CV and respiratory systems:• VS, especially BP, heart sounds• Chest pain?, Edema?, JVD?• Dyspnea?, Crackles?• Assess nutritional status- Protein, fluid, K,
Na, P restrictions• Weight gain or loss• Anorexia, nausea, vomiting
Assessment
• Assess renal status-
• Amount, frequency and appearance urine
• Bone Pain?
• Hyperglycemia-stress need for control
• Assess hematologic status, including_
• Petichiae, purpura, ecchymosis?
• Fatigue?, SOB?
Assessment
• Assess GI status-
• Stomatitis
• Melena
• Assess neurological status-
• Change in mental status?
• Seizure activity?
• Sensory changes?, Lower ext. weakness?
Assessment
• Assess Integumentary system-
• Skin integrity
• Discoloration?
• Pruritis?
• Assess lab data, including:
• BUN, creatinine, creatinine clearance, CBC, electrolytes.
Assessment
• Assess psychosocial status, including-
• Anxiety?
• Maladaptive behavior
• Refer to a community resource group
Interventions to Manage ESRDPeritoneal Dialysis and Hemodialysis
Functions:
1. Rid the body of excess fluids and electrolytes
2. Achieve acid-base balance
3. Eliminate waste products, toxins
4. Restore internal fluid balance through osmosis, diffusion and ultrafiltration
Concepts of Dialysis
• Dialysate: solution of electrolytes,modified salt, acetate, glucose and heparin
• Dialyzer- Artificial kidney with a semipermeable membrane (Hemodialysis) or the peritoneum as a semipermeable membrane (Peritoneal Dialysis)
• Diffusion-
• Osmosis-
Peritoneal Dialysis
• May be hemodynamically unstable, can’t tolerate anticoagulation.
• Peritonitis is a major complication.• Procedure- surgically inserted tube into abdominal
cavity- infusion of dialysate.ONE EXCHANGE:Fill time: Infuse 1-2 liters by gravity over 20 min.Dwell time: Dialysate dwells in abdomen over
specified period of time.Drain Time- 10-15 min. Output usually 100-200mL.
input
PD
• Fluid then drains out by gravity.• This effluent contains dialysate, excess
water, electrolytes and nitrogenous wastes.
• The number and frequency of exchanges depend on client’s condition and lab data.
• Types of PD – Continuous ambulatory PD (CAPD), multiple bag CAPD, automated or continuous cycle.
PD- Complications
Peritonitis, manifested by:• Cloudy outflow (effluent)• Rebound abdominal tenderness• Abdominal pain• General malaise• Nausea, vomiting• Intervention – send C and S, Tx. with
appropriate Antibiotic.
PD- Complications
• Pain – pain initially
• Exit site and tunnel infection
• Insufficient flow of dialysate
• Dialysate leakage.Dyspnea
• Formation of fibrin clots
• Altered body image
Care of the Tenckhoff Catheter
• Mask for yourself and client• Put on clean gloves. Remove the old dressing,
remove contaminated gloves.• Assess area for signs of infection, swelling,
redness, or discharge around catheter site.• Use aseptic technique:• Sterile field, 2 4x4”s, cotton swabs soaked in
providone iodine, put on sterile gloves.• Use cotton swabs to clean around catheter site,
in a circular motion. • Apply pre-cut gauze pads over catheter site.• Tape edges of gauze pads.
Care of patient during PD
• Before treatment – monitor vitals, weight, lab values.
• During dialysis – continually monitor pt., VS taken regularly, assess for pain, assess catheter site for leaking.. Monitor dwell time, and document.
• Record amount outflow, note clarity of effluent, I and O.
Hemodialysis
http://kidney.niddk.nih.gov/kudiseases/pub/• Vascular access – AV fistula,anastomosis of an
artery and a vein or AV shunt• Temporary double lumen catheter in subclavian,
IJ or femoral vein• Pre-dialysis Interventions-• Assess patency – bruit, thrill,distal pulses• Common complications of access- • Thrombosis or stenosis, infection, aneurysm
formation, ischemia, bleeding• Determime if meds should be held
Post Dialysis Nursing Care
Assess for Complications:• Hypotension• Headache• Nausea, vomiting• Malaise• Dizziness• Muscle cramps• Monitor BUN/Creat/Lytes/Hct• LOC• Bleeding
HD
• Heparinization – used for dialysis:
• All invasive procedure avoided 4-6 hrs. after dialysis.
• Nurse monitors for signs of hemorrhage during dialysis and 1 hr. after.
• Complications – Disequilibrium syndrome
• Infectious diseases – can be transmitted, hepatitis and HIV
HD
• Nursing Care- Get report.
• Weigh client before and after dialysis
• Know the client’s dry weight
• Measure vitals, observe for bleeding
• Assess LOC, HA?, nausea? Vomiting?
Renal Transplantation
• Candidates must be:• Free from medical problems• Usually age 40 – 70 years old.• Candidates excluded:
– Active infection– IV drug abuse– Malignant neoplasm– Severe obesity– Acute vascultitis– Severe psych problems– Long standing pulmonary disease– Advanced cardiac disease
Renal Transplantation
Donors- Absence of systemic disease/ infectionNo history of cancerAbsence hypertension and renal diseaseAdequate renal function – diagnostic tests.
Renal Transplantation
• Complications-
• Rejection- immunosuppressive drug therapy, corticosteroids.
• Renal artery stenosis – HTN, bruit, decreased renal function.
• Post – op care- Monitor vitals, renal function, I and O, urine output, color.
• Diuretics may be ordered.
Renal Transplantation
• Daily weights
• Carefully monitor I and O.
• Monitor for electrolyte imbalances.
• Patient teaching for discharge regarding: meds, diet, wound care,signs of infection and rejection, and follow up care with PMD.
Review of Terminology
Acute Renal Failure• Usually temporary
and may be reversed, leaving no permanent or serious damage to kidneys
• Sudden loss of the ability of the kidneys to excrete wastes, concentrate urine and conserve electrolytes
Chronic Renal Failure• Long term and
irreversible• Usually occurs over a
number of years as the internal structures of the kidney are slowly damaged