Embed Size (px)
Citation preview

C O M N O V. 2 0 0 8 C A S E 2
POSTERIOR FOSSA TUMOR IN A 2 YEAR-OLD GIRL
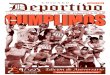
CLINICAL HISTORYA 2-year-old girl was admitted to the department of neurosciences,King Faisal Specialist Hospital and Research Center, Riyadh,Saudi Arabia, with three weeks history of deterioration of walking,then became unable to walk and later she developed a projectilevomiting mostly in early morning. There was no history of seizuresor loss of consciousness. At admission her neurological examina-tion revealed bilateral papilledema, nystagmus and truncal ataxiawith intention tremor. Magnetic Resonance Images (MRI) of thebrain showed a 3 ¥ 4 cm posterior fossa enhancing mass extendingfrom the base of the cerebellum to the roof of the fourth ventriclewithout calcification (fig. 1, sagittal T-1 weighted with contrast)and (figure 2: axial T2-weighted with contrast). Then, the patientunderwent midline suboccipital craniotomy with a near total resec-tion of the tumor.
PATHOLOGIC FINDINGSGross examination of the tumor showed white-tan soft friabletissue. Microscopically, the tumor consisted of highly cellular clus-ters of small to medium-sized cells with hyperchromatic round
to oval nuclei and indistinct cell borders (figure 3) admixed withareas showing fine fibrillary, paucicellular, neuropil-like matrix(figure 4). Also noted were areas containing true rosettes (ependy-moblastomatous type) with well-formed central lumina (figure 5).These rosettes consisted of multilayered cells with hyperchromaticnuclei, numerous mitotic figures and apoptotic bodies (figure 6).The lumina of some rosettes contained granular eosinophilic mate-rial. Periodic Acid Schiff (PAS) special stain was positive along theluminal border of the true rosettes and highlighted some of thegranular material within the lumina (figure 7). Immunohistochemi-cal studies were characterized by positivity for synaptophysin(figure 8) and CD56 (figure 9) in the neuroblastic tumor cells andneuropil-like areas. Glial fibrillary acidic protein (GFAP) was onlypositive in scattered cells in these areas (figure 10 & 11). Neu-rofilament protein was negative. The true ependymoblastomatousrosettes were negative for CD56, GFAP and synaptophysin butthey strongly expressed vimentin (figure 12). The Ki-67 was muchhigher in the ependymoblastomatous rosettes (over 90%) than inthe neuroblastic areas (approximately 15%), as seen in (figure 13).The patient was then treated with chemotherapy which includedcourses of cyclophosphamide and vincristine, cisplatin and etopo-side (VP16). Unfortunately, the patient developed recurrent disease6 months after resection and chemotherapy.
Figure 1. Figure 2.
doi:10.1111/j.1750-3639.2009.00279.x
343Brain Pathology 19 (2009) 343–346
© 2009 The Authors; Journal Compilation © 2009 International Society of Neuropathology

Figure 4. Figure 5.
Figure 3.
Correspondence
344 Brain Pathology 19 (2009) 343–346
© 2009 The Authors; Journal Compilation © 2009 International Society of Neuropathology

Figure 6. Figure 7.
Figure 8. Figure 9.
Figure 10. Figure 11.
Figure 12. Figure 13.
Correspondence
345Brain Pathology 19 (2009) 343–346
© 2009 The Authors; Journal Compilation © 2009 International Society of Neuropathology

DIAGNOSISEmbryonal Tumor with Abundant Neuropil and True Rosettes(ETANTR).
DISCUSSIONThe 2007 World Health Organization (WHO) classification ofcentral nervous system (CNS) tumors classifies the embryonaltumors into three categories: 1) Medulloblastoma, 2) Atypicalteratoid/rhabdoid tumor, and 3) CNS primitive neuroectodermaltumor (PNET). The latter category (PNET) includes five sub-categories: 1) CNS PNET; 2) CNS neuroblastoma, 3) CNS gan-glioneuroblastoma, 4) medulloepithelioma, and 5) ependymo-blastoma. (7). In the “CNS PNET” section of the 2007 WHOclassification of tumors of the CNS, there is a short paragraph,describing an extremely aggressive type of tumor called “Embryo-nal tumor with abundant neuropil and true rosettes” (ETANTR),suggesting that this tumor might eventually be considered as aseparate entity (7).
Embryonal tumors with abundant neuropil and true rosetteswere first reported as neuroblastic tumors with abundant neuropiland true rosettes in 2000 by Eberhart et al (3), who described ninecases. In 2006, three additional cases were been reported, one caseby Spina et al (6) and two cases by Fuller et al (4). Recently, in2007, an additional case was reported by Dunham et al (2). Thesecases are summarized in a table on-line (see: http://path.upmc.edu/divisions/neuropath/bpath/cases/case175/dx.html
All ETANTR cases reported so far have been in children aged 4years old or less. This tumor combines the features of a neuroblas-toma and an ependymoblastoma, by showing fine fibrillaryneuropil-like areas admixed with cellular regions andependymoblastoma-like rosettes. Nevertheless, Homer Wrightrosettes are absent or rarely identified. Eberhart et al (3) reportednine cases of tumors in children ages 1–3 years containing abun-dant neuropil and true rosettes. The tumor involved the frontopari-etal region in six cases, the frontal lobe in one case, the cerebellumin one case and the tectal plate in the last case. Two additional caseswere described in an addendum, one involved the cerebellum andthe other in the frontal lobe. These were positive for synaptophysinand neurofilament protein and only one case showed focal GFAPpositivity (3). Most of the patients died 5–14 months after presen-tation. Spina et al (6) reported a 4-year old boy who presented withan infiltrating ETANTR of the pons and midbrain. Histologically,the tumor was similar to that described by Eberhart et al (3).Thetumor cells were positive for synaptophysin and negative for GFAP.Their patient was alive 34 months after surgery with no evidence ofdisease. Fuller et al (4) reported two cases in 4-year-old children (amidpontine tumor and a large cerebral lesion). The first caseshowed polysomy of chromosomes 2, 8, 17, and 22. The secondcase showed isochromosome 17q which is molecular alterationtypical of medulloblastomas. The midpontine tumor was stable at19 months but in the other case the patient died 6 months afterinitial examination. Recently, Dunham et al (2) reported a caseoccurring in a 2-year-old boy as a large left temporoparietal mass.The tumor exhibited extensive neurocytic differentiation. Theirpatient developed recurrence approximately after one year. Similarcases have been previously described as ependymoblastoma andneuroblastoma (1, 5).
In summary ETANTR is a very rare, highly aggressive CNSneoplasm and we are reporting here an additional case to the previ-ously reported thirteen cases, which also represents the second caseoccurring in the cerebellum.
REFERENCES
1. Cenacchi G, Giangaspero F (2004) Emerging tumor entities andvariants of CNS neoplasms. J Neuropathol Exp Neurol 63(3):185–192.
2. Dunham C, Sugo E, Tobias V, Wills E, Perry A (2007) Embryonaltumor with abundant neuropil and true rosettes (ETANTR): report of acase with prominent neurocytic differentiation. Journal ofNeuro-Oncology. 84(1):91–98.
3. Eberhart CG, Brat DJ, Cohen KJ, Burger PC (2000) Pediatricneuroblastic tumors containing abundant neuropil and true rosettes.Pediatr Dev Pathol. 3:346–352.
4. Fuller C, Fouladi M, Gajjar A, Dalton J, Sanford RA, Helton KJ (2006)Chromosome 17 abnormalities in pediatric neuroblastic tumor withabundant neuropil and true rosettes. Am J Clin Pathol 126:277–283.
5. Queiroz LS, de Faria JL, Cruz JN (1975) An ependymoblastoma of thepons. J Pathol 115:207–212.
6. Spina ML, Pizzolitto S, Skrap M, Nocerino A, Russo G, Di Cataldo A,Perilongo G (2006) Embryonal tumor with abundant neuropil and truerosettes. A new entity or only variations of a parent neoplasms(PNETs)? This is the dilemma. Journal of Neuro-Oncology78:317–320.
7. WHO Classification of Tumors of the Central Nervous System (2007)4th ed. IARC Press; Lyon, France: p 8–9.
Contributors:Turki Omar Al-Hussain, MBBS, Mohammad Anas Dababo, MD
Department of Pathology and Laboratory MedicineKing Faisal Specialist Hospital and Research Center
Riyadh, 11211, Saudi Arabia
ABSTRACTWe report a case of a 2 year-old girl who presented with threeweeks history of deterioration of walking, then became unable towalk and later she developed a projectile vomiting. Neurologicalexamination revealed bilateral papilledema, nystagmus, andtruncal ataxia with intention tremor. Radiological studies showedan enhancing mass in the posterior fossa extending from the cer-ebellum to the roof of the fourth ventricle. The tumor was diag-nosed as an embryonal tumor with abundant neuropil and truerosettes (ETANTR). The tumor cells in the neuroblastic componentwere diffusely positive for synaptophysin and CD56, with scatteredpositive cells for glial fibrillary acidic protein. The true rosetteswere only positive for vimentin. Ki67 showed high index (over90%) in the true rosettes, while the neuroblastic areas were upto 15%. Our patient developed recurrent disease 6 months afterresection and chemotherapy. ETANTR is a very rare aggressiveembryonal CNS tumor that combines features of neuroblastomaand ependymoblastoma. We review the thirteen cases reported inthe literatures. This case represents the second report of anETANTR arising in the cerebellum.
Correspondence
346 Brain Pathology 19 (2009) 343–346
© 2009 The Authors; Journal Compilation © 2009 International Society of Neuropathology