Embed Size (px)
Citation preview
8/8/2019 103 Can Adrenal Insufficiency Be Diagnosed on Clinical and ...
http://slidepdf.com/reader/full/103-can-adrenal-insufficiency-be-diagnosed-on-clinical-and- 1/6
Proc. West. Pharmacol. Soc. 46: 103-108 (2003)
103
Can Adrenal Insufficiency Be Diagnosed On Clinical and Laboratory Data Basis in Patients with AIDS?
Luis Casanova-Cardiel1*, Norma Palacios-Jiménez1, Gabriela Miralrío-Gómez1, Jesús Gaytán-Martínez1,Gerardo Reyes-García1, Eduardo Mateos-García1 and José L. Fuentes-Allen1
1Department of Infectious Diseases of Adults, Infectology Hospital. National Medical Center “La Raza”. Instituto Mexicano del Seguro
Social, Mexico City. Vallejo y Jacarandas s/n, Col. La Raza, Del. Azcapotzalco, Mexico City. c.p. 02990 *email: [email protected]
INTRODUCTION: The adrenal glands are theendocrine organ most affected in HIV infection,mainly by opportunistic infections such as CMV, and
neoplasms [1-3]. The frequency of adrenal gland
pathology ranges from forty to fifty percent [4-6],and is not related to the frequency of impaired
cortisol response, which varies from 0% to 22% [7-
12], when a short corticotropin stimulation test isperformed. Differences in cortisol responses couldbe explained because adrenal function is preserved
even with significant organ damage, it being necessarythat more than 90% of tissue be affected for a classica
Addisonian symptomatology to develop [2] or show ablunted response to corticotropin test. Despite the lowfrequency of adrenal insufficiency demonstrated byCortrosyn test, it is likely than the hypothalamic-pituitary-adrenal (HPA) axis is affected in a greateproportion of patients with AIDS, when an ovine CRH
stimulation test is performed (50% and 63%)[13, 14].
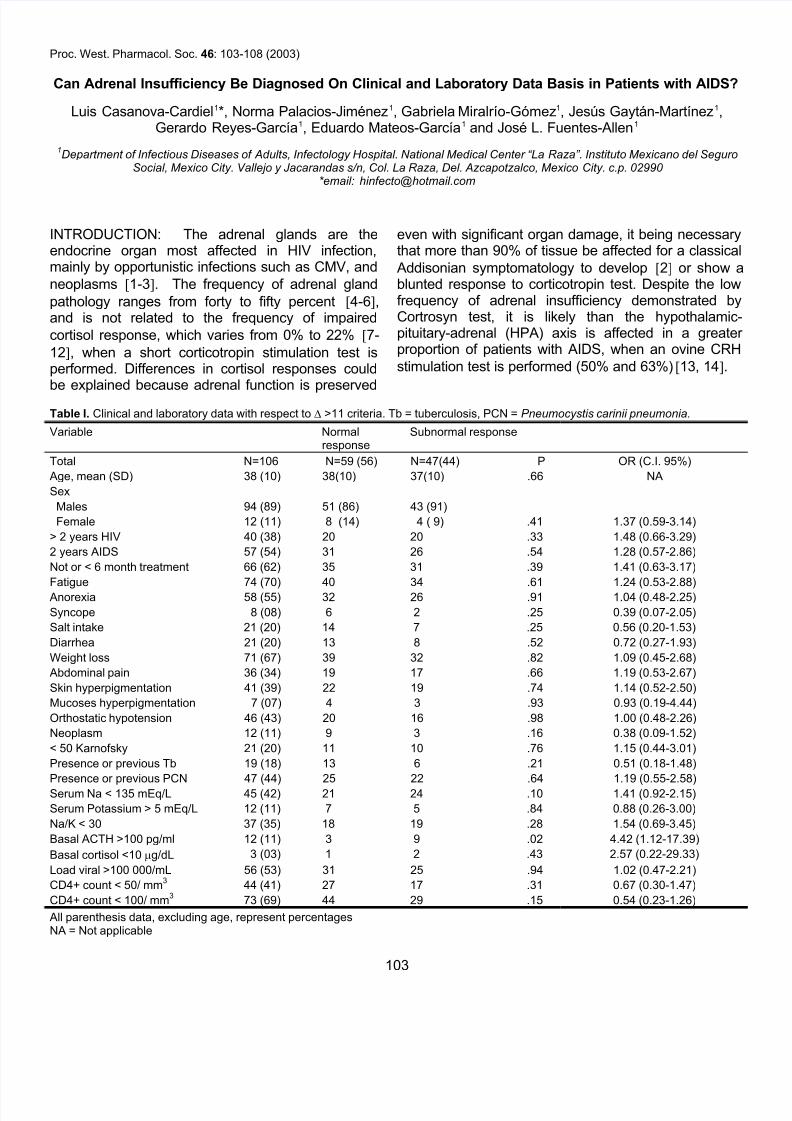
Table I. Clinical and laboratory data with respect to ∆ >11 criteria. Tb = tuberculosis, PCN = Pneumocystis carinii pneumonia.
Variable Normalresponse
Subnormal response
Total N=106 N=59 (56) N=47(44) P OR (C.I. 95%)
Age, mean (SD) 38 (10) 38(10) 37(10) .66 NA
Sex
Males 94 (89) 51 (86) 43 (91)
Female 12 (11) 8 (14) 4 ( 9) .41 1.37 (0.59-3.14)
> 2 years HIV 40 (38) 20 20 .33 1.48 (0.66-3.29)
2 years AIDS 57 (54) 31 26 .54 1.28 (0.57-2.86)
Not or < 6 month treatment 66 (62) 35 31 .39 1.41 (0.63-3.17)
Fatigue 74 (70) 40 34 .61 1.24 (0.53-2.88)
Anorexia 58 (55) 32 26 .91 1.04 (0.48-2.25)
Syncope 8 (08) 6 2 .25 0.39 (0.07-2.05)
Salt intake 21 (20) 14 7 .25 0.56 (0.20-1.53)
Diarrhea 21 (20) 13 8 .52 0.72 (0.27-1.93)
Weight loss 71 (67) 39 32 .82 1.09 (0.45-2.68)
Abdominal pain 36 (34) 19 17 .66 1.19 (0.53-2.67)
Skin hyperpigmentation 41 (39) 22 19 .74 1.14 (0.52-2.50)
Mucoses hyperpigmentation 7 (07) 4 3 .93 0.93 (0.19-4.44)
Orthostatic hypotension 46 (43) 20 16 .98 1.00 (0.48-2.26)
Neoplasm 12 (11) 9 3 .16 0.38 (0.09-1.52)
< 50 Karnofsky 21 (20) 11 10 .76 1.15 (0.44-3.01)
Presence or previous Tb 19 (18) 13 6 .21 0.51 (0.18-1.48)
Presence or previous PCN 47 (44) 25 22 .64 1.19 (0.55-2.58)
Serum Na < 135 mEq/L 45 (42) 21 24 .10 1.41 (0.92-2.15)
Serum Potassium > 5 mEq/L 12 (11) 7 5 .84 0.88 (0.26-3.00)
Na/K < 30 37 (35) 18 19 .28 1.54 (0.69-3.45)
Basal ACTH >100 pg/ml 12 (11) 3 9 .02 4.42 (1.12-17.39)
Basal cortisol <10 µg/dL 3 (03) 1 2 .43 2.57 (0.22-29.33)
Load viral >100 000/mL 56 (53) 31 25 .94 1.02 (0.47-2.21)
CD4+ count < 50/ mm3
44 (41) 27 17 .31 0.67 (0.30-1.47)
CD4+ count < 100/ mm3
73 (69) 44 29 .15 0.54 (0.23-1.26)
All parenthesis data, excluding age, represent percentagesNA = Not applicable
8/8/2019 103 Can Adrenal Insufficiency Be Diagnosed on Clinical and ...
http://slidepdf.com/reader/full/103-can-adrenal-insufficiency-be-diagnosed-on-clinical-and- 2/6
104
When adrenal insufficiency data for a presumptivediagnosis are evident, Cortrosyn test is usuallyconfirmatory [15]; in a non-classical clinical picture,several signs, symptoms and laboratory findings havebeen described [1-3, 12, 15]. In patients with AIDSunder stress from infections or surgery, there isinsufficient clinical data to elucidate whom amongthem would benefit from steroids. In developingcountries this decision is made solely on a clinicalbasis. It is mandatory therefore to estimate the
predictive value of clinical versus laboratory data.This prospective study evaluated the utility of clinicaland laboratory data for adrenal insufficiency diagnosisin Mexican patients with AIDS, using a low-dose (10µg) short corticotropin stimulation test as goldstandard [16-20].
PATIENTS AND METHODS: From January to August 2000, weprospectively studied 106 adult (94 men, 12 women; mean age37.7 years; range 20-65) patients with HIV-infection and CD4counts less than 200/mm
3. Inclusion criteria; one or more clinical
or laboratory determination suggesting adrenal insufficiencytiredness, weakness, wasting syndrome, weight loss, anorexiahyperpigmentation, dizziness, nausea, vomiting, diarrheahypotension, hyponatremia, and/or hyperkalemia. Patients undesteroidal, ketoconazol or megestrol therapies were excluded. The
low dose (10µg I.V. bolus dose of synthetic ACTH-CortrosynOrganon Inc., West Orange. NJ, USA) short ACTH test wasperformed between 08.00 and 09.00 hours; basal ACTH, cortisoand aldosterone and 60 min cortisol and aldosterone, weredetermined by RIA (all kits from CIS bio international).
A questionnaire was designed to ask for several symptoms and
signs; and sensitivity, specificity and predictive values of thesedata were obtained, comparing these data with the result of theACTH test. We considered abnormal response when cortiso
peak response at 60 min was less than 11 µg (∆ 11) with respecto basal; we also analyze the data with three different criteria todefine subnormal response to ACTH-stimulation test: these were1) twofold value of basal cortisol; 2) any cortisol value above 18
µg/dL; and, 3) any cortisol value above 20 µg/dL.
Statistical analysis, included demographic percentages and 2X2tables to determine sensitivity, specificity, negative predictivevalues, and positive predictive values. These same tables were
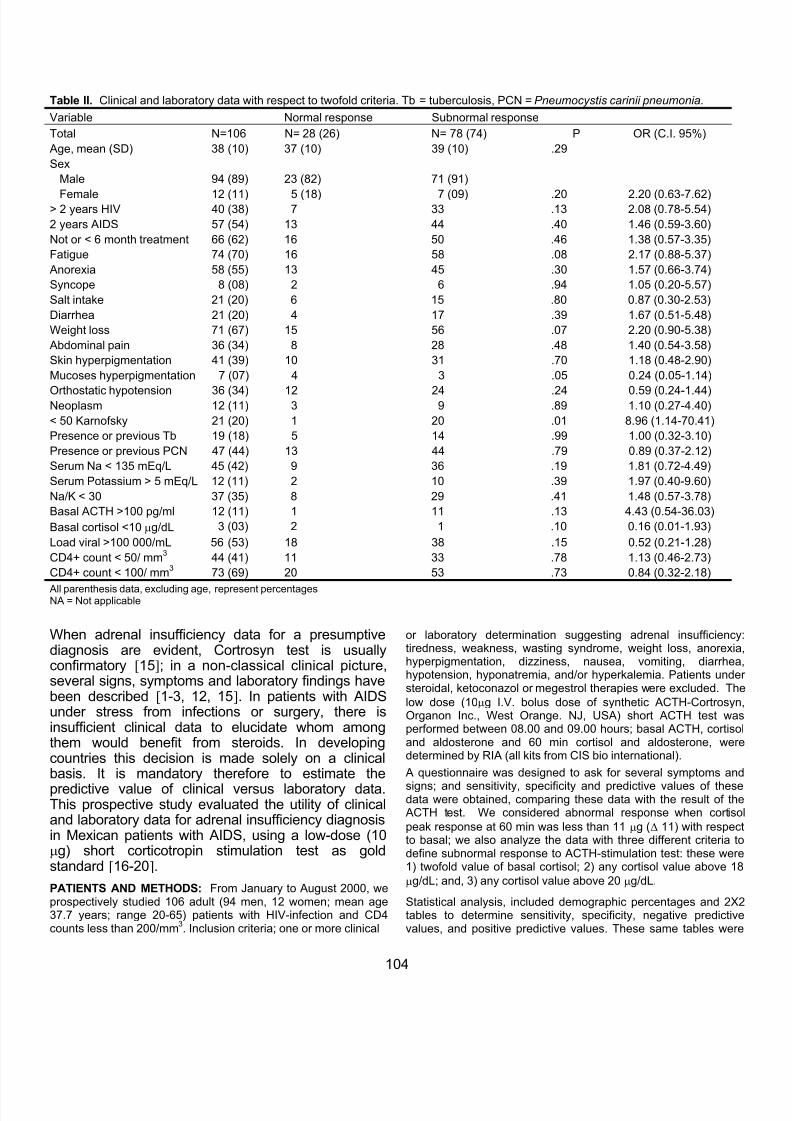
Table II. Clinical and laboratory data with respect to twofold criteria. Tb = tuberculosis, PCN = Pneumocystis carinii pneumonia.
Variable Normal response Subnormal response
Total N=106 N= 28 (26) N= 78 (74) P OR (C.I. 95%)
Age, mean (SD) 38 (10) 37 (10) 39 (10) .29
Sex
Male 94 (89) 23 (82) 71 (91)
Female 12 (11) 5 (18) 7 (09) .20 2.20 (0.63-7.62)> 2 years HIV 40 (38) 7 33 .13 2.08 (0.78-5.54)
2 years AIDS 57 (54) 13 44 .40 1.46 (0.59-3.60)
Not or < 6 month treatment 66 (62) 16 50 .46 1.38 (0.57-3.35)
Fatigue 74 (70) 16 58 .08 2.17 (0.88-5.37)
Anorexia 58 (55) 13 45 .30 1.57 (0.66-3.74)
Syncope 8 (08) 2 6 .94 1.05 (0.20-5.57)
Salt intake 21 (20) 6 15 .80 0.87 (0.30-2.53)
Diarrhea 21 (20) 4 17 .39 1.67 (0.51-5.48)
Weight loss 71 (67) 15 56 .07 2.20 (0.90-5.38)
Abdominal pain 36 (34) 8 28 .48 1.40 (0.54-3.58)
Skin hyperpigmentation 41 (39) 10 31 .70 1.18 (0.48-2.90)
Mucoses hyperpigmentation 7 (07) 4 3 .05 0.24 (0.05-1.14)
Orthostatic hypotension 36 (34) 12 24 .24 0.59 (0.24-1.44)Neoplasm 12 (11) 3 9 .89 1.10 (0.27-4.40)
< 50 Karnofsky 21 (20) 1 20 .01 8.96 (1.14-70.41)
Presence or previous Tb 19 (18) 5 14 .99 1.00 (0.32-3.10)
Presence or previous PCN 47 (44) 13 44 .79 0.89 (0.37-2.12)
Serum Na < 135 mEq/L 45 (42) 9 36 .19 1.81 (0.72-4.49)
Serum Potassium > 5 mEq/L 12 (11) 2 10 .39 1.97 (0.40-9.60)
Na/K < 30 37 (35) 8 29 .41 1.48 (0.57-3.78)
Basal ACTH >100 pg/ml 12 (11) 1 11 .13 4.43 (0.54-36.03)
Basal cortisol <10 µg/dL 3 (03) 2 1 .10 0.16 (0.01-1.93)
Load viral >100 000/mL 56 (53) 18 38 .15 0.52 (0.21-1.28)
CD4+ count < 50/ mm3
44 (41) 11 33 .78 1.13 (0.46-2.73)
CD4+ count < 100/ mm3
73 (69) 20 53 .73 0.84 (0.32-2.18)
All parenthesis data, excluding age, represent percentagesNA = Not applicable
8/8/2019 103 Can Adrenal Insufficiency Be Diagnosed on Clinical and ...
http://slidepdf.com/reader/full/103-can-adrenal-insufficiency-be-diagnosed-on-clinical-and- 3/6
105
used to determine if there was any difference in the univariateanalysis and to determine the odds ratio for selected studyvariables.
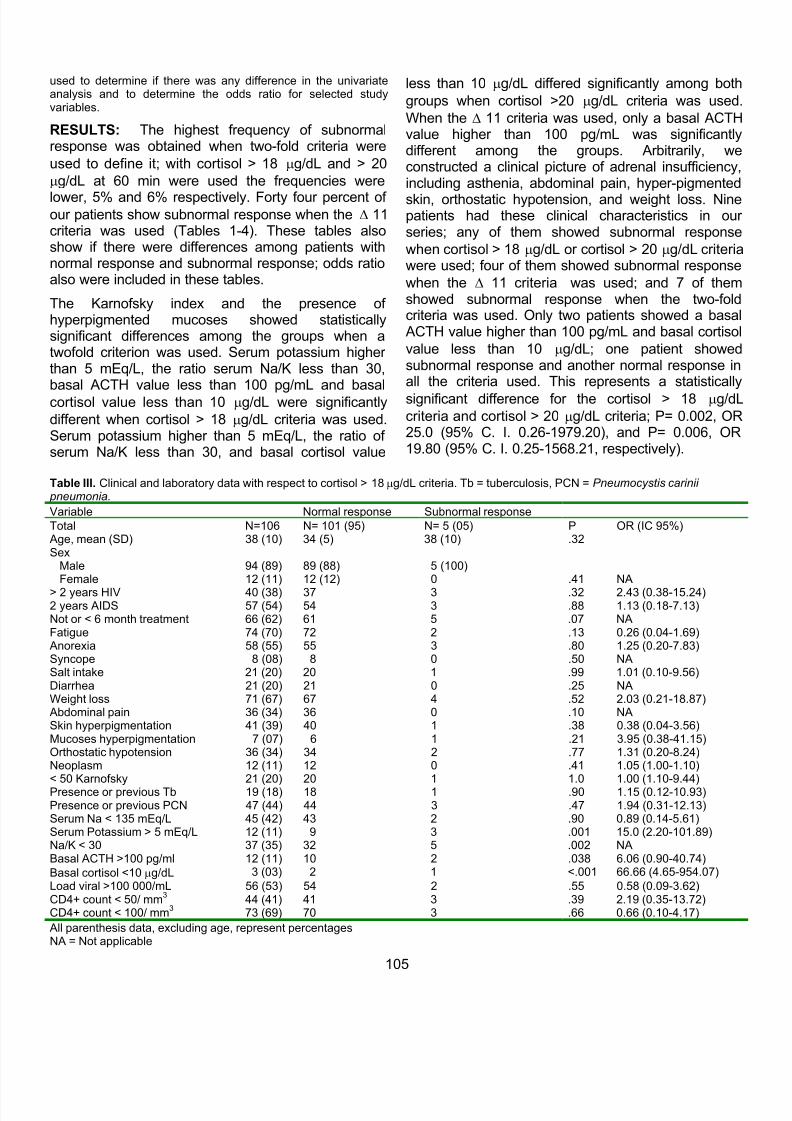
RESULTS: The highest frequency of subnormalresponse was obtained when two-fold criteria were
used to define it; with cortisol > 18 µg/dL and > 20
µg/dL at 60 min were used the frequencies were
lower, 5% and 6% respectively. Forty four percent of our patients show subnormal response when the ∆ 11criteria was used (Tables 1-4). These tables alsoshow if there were differences among patients withnormal response and subnormal response; odds ratioalso were included in these tables.
The Karnofsky index and the presence of hyperpigmented mucoses showed statisticallysignificant differences among the groups when atwofold criterion was used. Serum potassium higher than 5 mEq/L, the ratio serum Na/K less than 30,basal ACTH value less than 100 pg/mL and basal
cortisol value less than 10 µg/dL were significantly
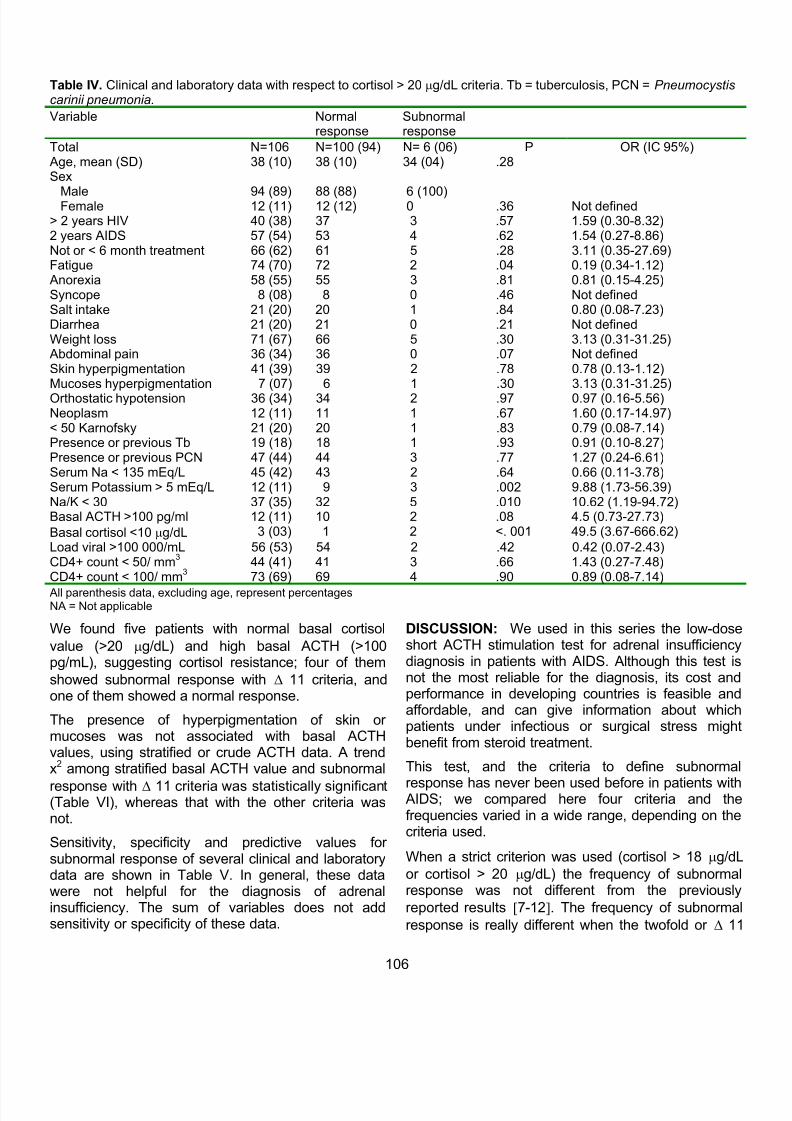
different when cortisol > 18 µg/dL criteria was used.Serum potassium higher than 5 mEq/L, the ratio of serum Na/K less than 30, and basal cortisol value
less than 10 µg/dL differed significantly among both
groups when cortisol >20 µg/dL criteria was used
When the ∆ 11 criteria was used, only a basal ACTHvalue higher than 100 pg/mL was significantlydifferent among the groups. Arbitrarily, weconstructed a clinical picture of adrenal insufficiencyincluding asthenia, abdominal pain, hyper-pigmented
skin, orthostatic hypotension, and weight loss. Ninepatients had these clinical characteristics in ourseries; any of them showed subnormal response
when cortisol > 18 µg/dL or cortisol > 20 µg/dL criteriawere used; four of them showed subnormal response
when the ∆ 11 criteria was used; and 7 of themshowed subnormal response when the two-foldcriteria was used. Only two patients showed a basaACTH value higher than 100 pg/mL and basal cortiso
value less than 10 µg/dL; one patient showedsubnormal response and another normal response inall the criteria used. This represents a statistically
significant difference for the cortisol > 18 µg/dL
criteria and cortisol > 20 µg/dL criteria; P= 0.002, OR25.0 (95% C. I. 0.26-1979.20), and P= 0.006, OR19.80 (95% C. I. 0.25-1568.21, respectively).
Table III. Clinical and laboratory data with respect to cortisol > 18 µg/dL criteria. Tb = tuberculosis, PCN = Pneumocystis carinii pneumonia.
Variable Normal response Subnormal response
Total N=106 N= 101 (95) N= 5 (05) P OR (IC 95%)Age, mean (SD) 38 (10) 34 (5) 38 (10) .32Sex
Male 94 (89) 89 (88) 5 (100)Female 12 (11) 12 (12) 0 .41 NA
> 2 years HIV 40 (38) 37 3 .32 2.43 (0.38-15.24)2 years AIDS 57 (54) 54 3 .88 1.13 (0.18-7.13)Not or < 6 month treatment 66 (62) 61 5 .07 NAFatigue 74 (70) 72 2 .13 0.26 (0.04-1.69)Anorexia 58 (55) 55 3 .80 1.25 (0.20-7.83)Syncope 8 (08) 8 0 .50 NASalt intake 21 (20) 20 1 .99 1.01 (0.10-9.56)Diarrhea 21 (20) 21 0 .25 NAWeight loss 71 (67) 67 4 .52 2.03 (0.21-18.87)Abdominal pain 36 (34) 36 0 .10 NASkin hyperpigmentation 41 (39) 40 1 .38 0.38 (0.04-3.56)Mucoses hyperpigmentation 7 (07) 6 1 .21 3.95 (0.38-41.15)Orthostatic hypotension 36 (34) 34 2 .77 1.31 (0.20-8.24)Neoplasm 12 (11) 12 0 .41 1.05 (1.00-1.10)< 50 Karnofsky 21 (20) 20 1 1.0 1.00 (1.10-9.44)Presence or previous Tb 19 (18) 18 1 .90 1.15 (0.12-10.93)Presence or previous PCN 47 (44) 44 3 .47 1.94 (0.31-12.13)Serum Na < 135 mEq/L 45 (42) 43 2 .90 0.89 (0.14-5.61)Serum Potassium > 5 mEq/L 12 (11) 9 3 .001 15.0 (2.20-101.89)Na/K < 30 37 (35) 32 5 .002 NABasal ACTH >100 pg/ml 12 (11) 10 2 .038 6.06 (0.90-40.74)
Basal cortisol <10 µg/dL 3 (03) 2 1 <.001 66.66 (4.65-954.07)
Load viral >100 000/mL 56 (53) 54 2 .55 0.58 (0.09-3.62)CD4+ count < 50/ mm
344 (41) 41 3 .39 2.19 (0.35-13.72)
CD4+ count < 100/ mm3
73 (69) 70 3 .66 0.66 (0.10-4.17)
All parenthesis data, excluding age, represent percentagesNA = Not applicable
8/8/2019 103 Can Adrenal Insufficiency Be Diagnosed on Clinical and ...
http://slidepdf.com/reader/full/103-can-adrenal-insufficiency-be-diagnosed-on-clinical-and- 4/6
106
We found five patients with normal basal cortisol
value (>20 µg/dL) and high basal ACTH (>100pg/mL), suggesting cortisol resistance; four of them
showed subnormal response with ∆ 11 criteria, andone of them showed a normal response.
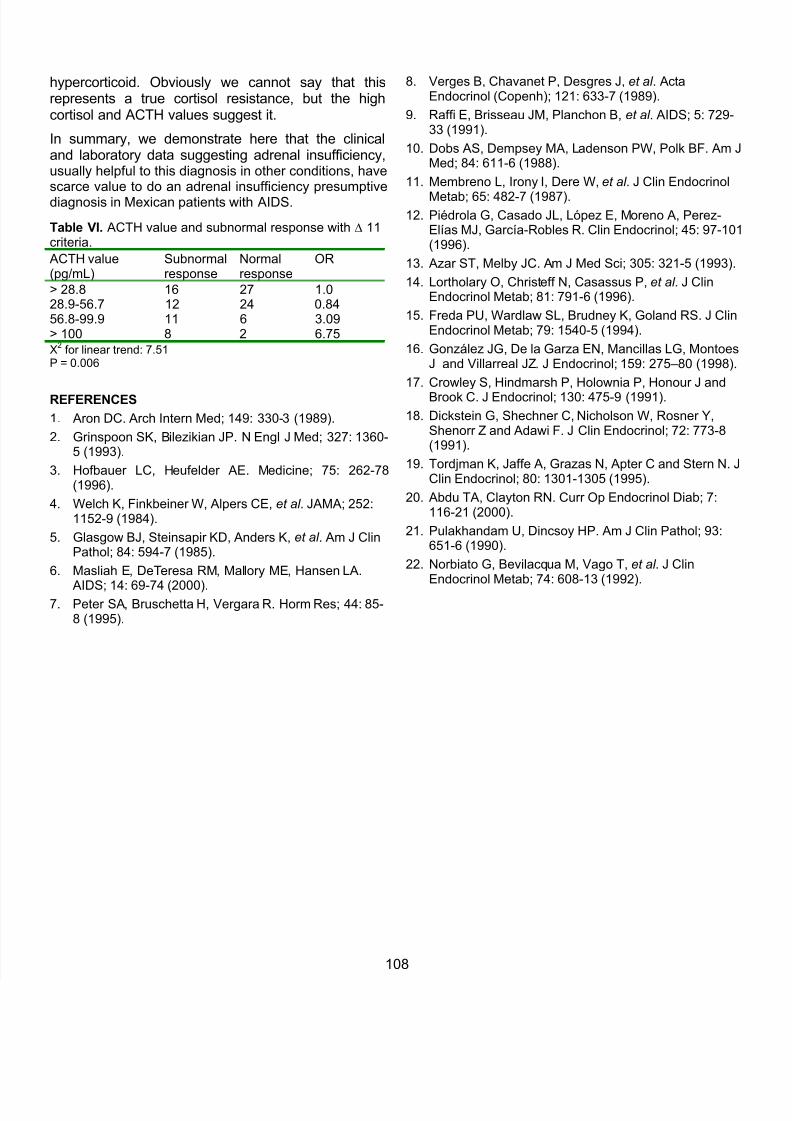
The presence of hyperpigmentation of skin or mucoses was not associated with basal ACTHvalues, using stratified or crude ACTH data. A trendx2 among stratified basal ACTH value and subnormal
response with ∆ 11 criteria was statistically significant(Table VI), whereas that with the other criteria wasnot.
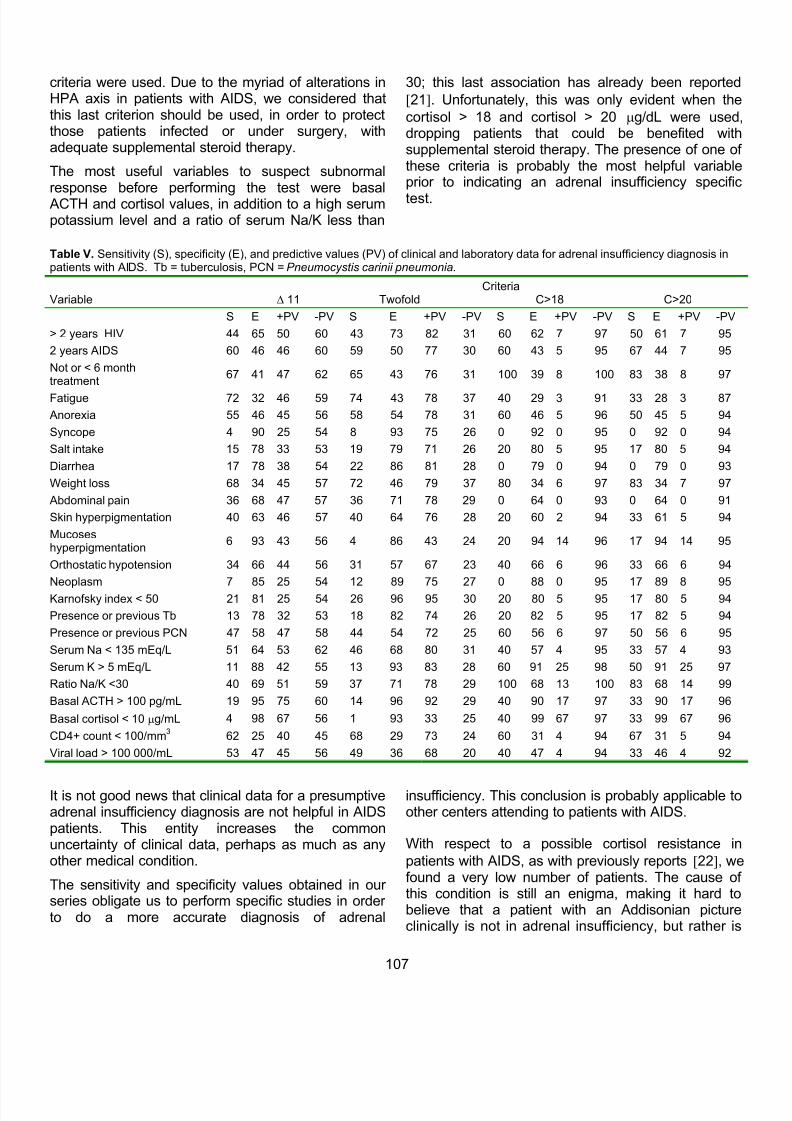
Sensitivity, specificity and predictive values for subnormal response of several clinical and laboratorydata are shown in Table V. In general, these datawere not helpful for the diagnosis of adrenalinsufficiency. The sum of variables does not addsensitivity or specificity of these data.
DISCUSSION: We used in this series the low-doseshort ACTH stimulation test for adrenal insufficiencydiagnosis in patients with AIDS. Although this test isnot the most reliable for the diagnosis, its cost andperformance in developing countries is feasible andaffordable, and can give information about whichpatients under infectious or surgical stress mightbenefit from steroid treatment.
This test, and the criteria to define subnorma
response has never been used before in patients withAIDS; we compared here four criteria and thefrequencies varied in a wide range, depending on thecriteria used.
When a strict criterion was used (cortisol > 18 µg/dL
or cortisol > 20 µg/dL) the frequency of subnormaresponse was not different from the previously
reported results [7-12]. The frequency of subnorma
response is really different when the twofold or ∆ 11
Table IV. Clinical and laboratory data with respect to cortisol > 20 µg/dL criteria. Tb = tuberculosis, PCN = Pneumocystiscarinii pneumonia.
Variable Normalresponse
Subnormalresponse
Total N=106 N=100 (94) N= 6 (06) P OR (IC 95%)Age, mean (SD) 38 (10) 38 (10) 34 (04) .28Sex
Male 94 (89) 88 (88) 6 (100)Female 12 (11) 12 (12) 0 .36 Not defined> 2 years HIV 40 (38) 37 3 .57 1.59 (0.30-8.32)2 years AIDS 57 (54) 53 4 .62 1.54 (0.27-8.86)Not or < 6 month treatment 66 (62) 61 5 .28 3.11 (0.35-27.69)Fatigue 74 (70) 72 2 .04 0.19 (0.34-1.12)Anorexia 58 (55) 55 3 .81 0.81 (0.15-4.25)Syncope 8 (08) 8 0 .46 Not definedSalt intake 21 (20) 20 1 .84 0.80 (0.08-7.23)Diarrhea 21 (20) 21 0 .21 Not definedWeight loss 71 (67) 66 5 .30 3.13 (0.31-31.25)Abdominal pain 36 (34) 36 0 .07 Not definedSkin hyperpigmentation 41 (39) 39 2 .78 0.78 (0.13-1.12)Mucoses hyperpigmentation 7 (07) 6 1 .30 3.13 (0.31-31.25)Orthostatic hypotension 36 (34) 34 2 .97 0.97 (0.16-5.56)Neoplasm 12 (11) 11 1 .67 1.60 (0.17-14.97)< 50 Karnofsky 21 (20) 20 1 .83 0.79 (0.08-7.14)Presence or previous Tb 19 (18) 18 1 .93 0.91 (0.10-8.27)Presence or previous PCN 47 (44) 44 3 .77 1.27 (0.24-6.61)Serum Na < 135 mEq/L 45 (42) 43 2 .64 0.66 (0.11-3.78)Serum Potassium > 5 mEq/L 12 (11) 9 3 .002 9.88 (1.73-56.39)Na/K < 30 37 (35) 32 5 .010 10.62 (1.19-94.72)Basal ACTH >100 pg/ml 12 (11) 10 2 .08 4.5 (0.73-27.73)
Basal cortisol <10 µg/dL 3 (03) 1 2 <. 001 49.5 (3.67-666.62)
Load viral >100 000/mL 56 (53) 54 2 .42 0.42 (0.07-2.43)CD4+ count < 50/ mm
344 (41) 41 3 .66 1.43 (0.27-7.48)
CD4+ count < 100/ mm3
73 (69) 69 4 .90 0.89 (0.08-7.14)
All parenthesis data, excluding age, represent percentagesNA = Not applicable
8/8/2019 103 Can Adrenal Insufficiency Be Diagnosed on Clinical and ...
http://slidepdf.com/reader/full/103-can-adrenal-insufficiency-be-diagnosed-on-clinical-and- 5/6
8/8/2019 103 Can Adrenal Insufficiency Be Diagnosed on Clinical and ...
http://slidepdf.com/reader/full/103-can-adrenal-insufficiency-be-diagnosed-on-clinical-and- 6/6
108
hypercorticoid. Obviously we cannot say that thisrepresents a true cortisol resistance, but the highcortisol and ACTH values suggest it.
In summary, we demonstrate here that the clinicaland laboratory data suggesting adrenal insufficiency, usually helpful to this diagnosis in other conditions, havescarce value to do an adrenal insufficiency presumptivediagnosis in Mexican patients with AIDS.
REFERENCES
1. Aron DC. Arch Intern Med; 149: 330-3 (1989).
2. Grinspoon SK, Bilezikian JP. N Engl J Med; 327: 1360-5 (1993).
3. Hofbauer LC, Heufelder AE. Medicine; 75: 262-78(1996).
4. Welch K, Finkbeiner W, Alpers CE, et al . JAMA; 252:1152-9 (1984).
5. Glasgow BJ, Steinsapir KD, Anders K, et al . Am J ClinPathol; 84: 594-7 (1985).
6. Masliah E, DeTeresa RM, Mallory ME, Hansen LA.
AIDS; 14: 69-74 (2000).7. Peter SA, Bruschetta H, Vergara R. Horm Res; 44: 85-
8 (1995).
8. Verges B, Chavanet P, Desgres J, et al . ActaEndocrinol (Copenh); 121: 633-7 (1989).
9. Raffi E, Brisseau JM, Planchon B, et al . AIDS; 5: 729-33 (1991).
10. Dobs AS, Dempsey MA, Ladenson PW, Polk BF. Am JMed; 84: 611-6 (1988).
11. Membreno L, Irony I, Dere W, et al . J Clin Endocrinol
Metab; 65: 482-7 (1987).12. Piédrola G, Casado JL, López E, Moreno A, Perez-
Elías MJ, García-Robles R. Clin Endocrinol; 45: 97-101(1996).
13. Azar ST, Melby JC. Am J Med Sci; 305: 321-5 (1993).
14. Lortholary O, Christeff N, Casassus P, et al . J ClinEndocrinol Metab; 81: 791-6 (1996).
15. Freda PU, Wardlaw SL, Brudney K, Goland RS. J ClinEndocrinol Metab; 79: 1540-5 (1994).
16. González JG, De la Garza EN, Mancillas LG, MontoesJ and Villarreal JZ. J Endocrinol; 159: 275–80 (1998).
17. Crowley S, Hindmarsh P, Holownia P, Honour J and
Brook C. J Endocrinol; 130: 475-9 (1991).
18. Dickstein G, Shechner C, Nicholson W, Rosner Y,Shenorr Z and Adawi F. J Clin Endocrinol; 72: 773-8(1991).
19. Tordjman K, Jaffe A, Grazas N, Apter C and Stern N. JClin Endocrinol; 80: 1301-1305 (1995).
20. Abdu TA, Clayton RN. Curr Op Endocrinol Diab; 7:116-21 (2000).
21. Pulakhandam U, Dincsoy HP. Am J Clin Pathol; 93:651-6 (1990).
22. Norbiato G, Bevilacqua M, Vago T, et al . J ClinEndocrinol Metab; 74: 608-13 (1992).
Table VI. ACTH value and subnormal response with ∆ 11criteria.
ACTH value(pg/mL)
Subnormalresponse
Normalresponse
OR
> 28.8 16 27 1.028.9-56.7 12 24 0.8456.8-99.9 11 6 3.09> 100 8 2 6.75
X2
for linear trend: 7.51P = 0.006