Embed Size (px)
Citation preview

Adrenal Insufficiency
23/02/07
Naree Panamonta, MD.

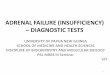
Adrenal steroids and Pathways Cholesterol
Pregnenolone
Progesterone
Aldosterone
Mineralocorticoid
17-hydroxypregnenolone
17-hydroxyprogesterone
Cortisol
Glucocorticoid
Dehydroepi
androsterone
Androstenedione
Androgens
21-hydroxylase
21-hydroxylase
Glomerulosa Fasciculata Reticularis

Physiologic actions of adrenal steroids Steroid Effect Cortisol - BP control - Glucose control - Stress response - Lymphocyte inhibition - Movement of neutrophils from
vascular wall to bloodstream - Thymus regression - Osteoclast stimulation
Aldosterone - Salt retention - K excretion - Acid secretion
DHEA/ - Muscle maintenanceAndrostenedione - Bone anabolism - Mental drive - Sexual function

Causes
Primary adrenal insufficiency Secondary adrenal insufficiency

Primary adrenal insufficiency
Causes Anatomic destruction of gland Metabolic failure in hormone production ACTH-blocking antibodies Mutation in ACTH receptor gene Adrenal hypoplasia congenita

Secondary adrenal insufficiency
Hypopituitarism due to hypothalamic-pituitary disease
Suppression of H-P axis
- By exogenous steroid
- By endogenous steroid from tumor

Primary adrenal insufficiency
(Addison’s disease)
- Involve > 90% of the glands

Pathophysiology
Gradual adrenocortical destruction- Initial phase: Decreased adrenal reserve
Basal steroid secretion- NormalNot increase in stress response
- Further loss of cortical tissueImpair basal secretion of glucocorticoid and
mineralocorticoid Plasma ACTH elevation- Earliest and most
sensitive indication

Anatomic destruction of gland1. Idiopathic atrophy: Autoimmune,
adrenoleukodystrophy
2. Surgical removal
3. Infection: TB, Fungus, Virus esp. in AIDS
4. Hemorrhage
5. Invasion: Metastasis eg. CA thyroid, breast, kidney, lymphoma

Idiopathic atrophy
Most common cause 70-80% Autoantibody: adrenal cortex Ab, 21-hydroxylase
Ab Isolated or associated with polyglandular
autoimmune syndrome PGA syndrome 2 types
1).PGA type1- more common2).PGA type2

PGA syndrome PGA type1 (Autoimmune Polyendocrinopathy- Candidiasis-
Ectodermal Dysplasia)- Autosomal recessive (no HLA association)- Childhood onset- 2/3 of these clinicals
:Chronic mucocutaneous candidiasis:Chronic hypoparathyroid:Autoimmune adrenal insufficiency
- Other: Hypogonadotropic hypogonadism, DM type1, Autoimmune thyroid disease, Lymphocytic hypophysitis, Pernicious anemia, Chronic active hepatitis, Vitiligo, Alopecia


PGA syndrome
PGA type2
- Polygenic, asso. with HLA DR3,DR4
- Adult onset
- Primary adrenal insufficiency, Grave’s disease, Autoimmune thyroiditis, DM type1, Primary hypogonadism, celiac disease

Infection- Granulomatous diseases eg.TB, MAC,
Histoplasmosis, Cryptococcosis, blastomycosis, CMV necrotizing adrenalitis
- AIDS: AIDS associated adrenal insufficiency
( necrotizing adrenalitis): Opportunistic infection- CMV,TB, MAC: Kaposi’s sarcoma

Histoplasmosis:Large bilateral adrenal masses (arrows) patchy& peripheral enhancement, central hypodensities, septations.

Hemorrhage and infarction - Anticoagulant - Hypercoagulable states eg. Antiphospholipid syndrome - Meningococcemia, pseudomonas infection (Waterhouse-Friderichsen syndrome)
Infiltration: - Metastasis: breast, lung, kidney, pancrease, melanoma, stomach
- Lymphoma - Other infiltrative diseases: amyloidosis, sarcoidosis, scleroderma


Metabolic failure in hormone production
Congenital adrenal hyperplasia: Inborn error of cortisol synthesis: 5 types ( classified by type of enz. deficiency)
- Most common :21-hydroxylase deficiency- 2nd most common: 11-hydroxylase
deficiency Drugs
- Enzyme inhibitors: Metyrapone, phenytoin , barbiturate, ketoconazole, aminoglutethimide- Cytotoxic agent: Mitotane

Secondary adrenal insufficiency
1.Suppression of H-P axis
- By exogenous steroid
- By endogenous steroid from tumor

Steroid induced adrenal insufficiency
Long-term glucocorticoid therapy (suppression of CRH production).
15 mg qd prednisone (or equivalent) for 3+ weeks---- HPA axis can be suppressed for ~ 8-12 months.
Divided daily dosing more suppressive than once daily dosing. Giving steroid every other day avoids axis suppression QOD dosing helps with all side effects except the cumulative
ones: osteoporosis, cataract. Clue to adrenal HPA axis suppression is small joint aches
(hands, feet) when glucocorticoid is withdrawn. Large doses of progesterone or megace also suppress
adrenal axis.

Secondary adrenal insufficiency2. Hypopituitarism due to hypothalamic-pituitary disease
- Sheehan’s syndrome- most common (not include exogenous steroid)
- Pituitary tumor, metastasis
- Craniopharyngioma
- Infection: TB
- Pituitary surgery or radiation
- Others: lymphocytic hypophysitis, sarcoidosis, histiocytosisX

Relative adrenal insufficiency Critical care and Resuscitation: Journal of the
Australasian Critical Care Medicine,2006 Dec;8(4):371-5- In septic shock- Increment of < 250 nmol/L in total serum cortisol
level after administration of 250 microg corticotropin- RAI associated with increased risk of death - There is strong, but not overwhelming, evidence
that administration of low doses of hydrocortisone to patients with septic shock, especially those with RAI, improves survival.

American Journal of Respiratory and Critical Care Medicine, 2006 Dec 15
In sepsis, adrenal insufficiency is likely when - Baseline cortisol levels <10 microg/dl
or - Delta cortisol <9 microg/dl
Unlikely when - Cosyntropin-stimulated cortisol level > 44
microg/dl or - Delta cortisol > 16.8 microg/dl

Diagnosis

Clinical manifestations Chronic Primary adrenal insufficiency
- Weakness, fatigue, anorexia, Wt. loss: cardinal symptom- Hyperpigmentation: Sun-exposed area, pressured area, skin creases, mucous membrane- Arterial hypotension, dehydration- Abnormality of GI function: N/V, diarrhea- Lab abnormalities: Anemia (NCNC/pernicious anemia), Lymphocytosis, Eosinophilia, hypoglycemia, hyponatremia, hyperkalemia, hyperchloremic metabolic acidosis


Clinical manifestations
Acute adrenal crisis- Hypovolemic shock (unexplained vascular collaspe)- Abdominal pain- Weakness, apathy, and confusion- Precipitated by stress- Acute adrenal hemorrhage: abdominal, flank, or back pain with rigidity/ rebound tenderness

Clinical manifestations Secondary adrenal insufficiency
- Clinically same as 1ry Adrenal insufficiency
- No hyperpigmentation, severe hyponatremia, severe dehydration, or hyperkalemia
- Multiple hormone deficiency: total pituitary insufficiency
- Cushinoid appearance: prolonged excess glucocorticoid

Clinical manifestations
1. Persistent shock despite adequate volume repletion
2. Abnormal Lab
3. History of prolonged steroid use+precipitating factors/ Cushinoid appearance

1ry and 2ry adrenal insuff.
1ry adrenal insuff. and associated disorder
2ry adrenal insuff. and associated disorders
-Tiredness, weakness, mental depression, headache
-Anorexia, wt. loss
-Dizziness, orthostatic hypotension
-Abdominal cramps, N/V, diarrhea
-Hyponatremia
-Hypoglycemia
-Mild normocytic anemia, lymphocytosis, eosinophilia
-Hypercalcemia(rare)
-Loss of body hair in women
-Hyperpigmentation
-Hyperkalemia
-Vitiligo
-Autoimmune thyroid disease
-CNS symptoms in adrenomyeloneuro
pathy
-Salt craving
-Acidosis (type IV RTA)
-Increased taste sensitivity (to salt)
-Hyperacusis
-Thorn’s sign: auricular calcification (male only)
-Pale skin with out marked anemia
-Amenorrhea, decraesed libido, and potency
-Scanty axillary and pubic hair
-Small testicles
-Secondary hypothyroidism
-Prepubertal growth deficit, delayed puberty
-Headache, visual symptoms
-Diabetes insipidus

suspected adrenal insufficiency
Rapid ACTH stimulation test
Abnormal NormalDecreased ACTH reserve not excluded
Metyrapone or insulin hypoglycemia testing
Adrenocortical insufficiency
Plasma ACTH
Elevated Normal or low
1ry Adrenal insufficiency
2ry Adrenal insufficiency
Abnormal Normal
Exclude 2ry Adrenal insufficiency
Exclude 1ry Adrenal insufficiency

Morning plasma cortisol: <5 ug/dL--- Suspected adrenal insufficiency>20 ug/dL--- Exclude adrenal insufficiency
Rapid ACTH stimulation test- Serum cortisol at 8.00 am- Cosyntropin 250 ug iv. or IM- Plasma cortisol at 30 and 60 min after injection
: Normal cortisol > 20 ug/dL or >7 ug/dL from baseline Adrenal insufficiency < 20 ug/dL

Plasma ACTH level- Primary adrenal insufficiency >52 pg/ml ( usually>200 pg/ml)- Secondary adrenal insufficiency –normal or<10 pg/ml
Aldosterone increment- Aldosterone response 60 min after
cosyntropin 250 mg IV or IM- Secondary adrenal insufficiency: Normal
increment > 5 ng/dL- Primary adrenal insufficiency: No
increment

Tests to confirm 2ry adrenal insufficiency Prolong ACTH stimulation
- Baseline plasma cortisol
- Cosyntropin 250 ug iv q 8 hr for 48 hr.
: Primary adrenal insufficiency- plasma cortisol no change
: Secondary adrenal insufficiency- progressive increase in plasma cortisol, and level >20 ug/dL

Tests to confirm 2ry adrenal insufficiency
Insulin induced hypoglycemia- Suspected hypothalamic or pituitary disease- NPO after midnight, 0.9% NSS iv- Short acting insulin 0.05-0.1 u/kg at morning- Blood for plasma glucose and cortisol at 30, 60, 90, and 120 minNormal response- if BS <40 mg/dl---cortisol> 20 ug/dl( Avoid when hypoglycemia is contraindicated, 1ry adrenal insufficiency, stroke, epilepsy)

Tests to confirm 2ry adrenal insufficiency Short metyrapone test
- Metyrapone 30 mg/kg orally at 24.00 PM- Blood for cortisol and 11-deoxycortisol at 8.00 AMNormal- cortisol < 8 ug/dl
deoxycortisol > 7ug/dl(Metyrapone not available in Thailand)

Treatment :Acute Adrenal crisisGlucocorticoid replacement
1.Hydrocortisone 100 mg iv every 6 hr. for 24 hr.2. Hydrocortisone 50 mg every 6 hr. when stable3. Maintenance therapy (10 mg 3 times/days) by day 4
or 5 4. Increase dose to 200-400 mg/day if complication
occursGeneral and supportive measures
1. Correct volume depletion, dehydration, hypoglycemia with iv saline and glucose
2. Correct infection and other precipitating causes

Treatment: Maintenance therapy
Hydrocortisone 15-20 mg in AM and 10 mg orally at 4-5 PM
Fludrocortisone 0.05-0.1 mg orally in AM Clinical follow-up: Clinical feature, BW,
BP, Elyte Increased hydrocortisone during stress

Response to therapy
General clinical signs: appetite, sense of well-being Cushing’s syndrome: overtreatment ACTH and urine free cortisol not a reliable index Mineralocorticoid replacement:
- BP without orthostatic change
- Elyte- Na and K
- Plasma renin activity (PRA)- upright <5 ng/mL/hr

Steroid coverage for surgery
Correct Elyte, BP, hydration Hydrocortisone 100 mg IM on call Hydrocortisone 50 mg IM or IV in recovery
room and q 6 hr. for 24 hr. Reduce dose to 25 mg q 6 hr. for 24 hr. and
taper to maintenance dose over 3-5 days Increase dose to 200-400 mg/day if
complications occur

Case 1 69-year-old female presented with palpitations
and a history of tiredness and shortness of breath for several weeks.
She had a previous history of Raynaud
syndrome. Get a persistent tan since the previous summer Her only medication was nifedipine for her Ray
naud syndrome.

Progress Admitted into hospital two weeks after initial pres
entation. Increasing lethargy and tiredness, reduced appe
tite ,fainting, and weight loss. On examination, she was pigmented and thin Her pulse rate 76/min. BP 77/59 mm Hg. The rest of the examination was normal. Serum sodium 132 mmol/l, potassium 5.1 mmol/l
BUN/Cr within normal limits



SerumTSH 7.87 mU/l (0.3–4.1 mU/l); serum FT3 18 pmol/l (11–23 pmol/l)
Extractable-nuclear-antigen ribonucleic proteins - positive
Thyroid microsomal antibodies- positive (titre greater than 1/800)
ANA - negative. Cortisol at baseline 135 mmol/l Rapid ACTH test- cortisol at 30 minutes 144 mmol/l Baseline ACTH 434 pg/l (0–47 pg/l) Plasma renin activity 8.9 ng/ml/h (1.1–4.1 ng/ml/h); a
nd aldosterone <50 pmol/l (220–430 pmol/l).

Primary adrenal insufficiency: Addison’s disease

IV saline and dextrose. IV or IM hydrocortisone by multiple bolus injectio
ns or by continuous infusion 100-150 mg daily Patient’s condition improved : Hydrocortisone giv
en orally 40 mg in the morning and 20 mg in the evening
3-4 days hydrocortisone reduced to 20-30 mg daily in two or three divided doses,
Mineralocorticoid is introduced at this stage (Fluodrocortisone 50-100 mg daily)

Case 2 68-year-old woman found on the floor 28 hr PTA Cough and diarrhea. No significant medical history ,not take any regula
r medications. At presentation, her core temperature was 24.9 C,
BP 80 mm Hg systolic, PR 40, and GCS 11 Physical examination
- Consistent with right basal pneumonia.
- No abdominal tenderness, or signs of endocrine dysfunction or trauma.

Haemoglobin was 138 g/L, but fell to 97 g/L 24 h later.
Electrolytes, clotting profile, DIC screen, serum calcium, and TFT were normal.
Toxicology screen- negative. CRP 170 mg/L (normal <10 mg/L). Antiphospholipid antibody screen - negativ
e. She was rewarmed, fluid-resuscitated, giv
en adrenaline and atropine,

ECG showed sinus bradycardia and Osborn waves, which disappeared after rewarming.

Persistent, inotrope-refractory hypotension Short Synacthen (ACTH) test : Basal cortisol le
vel 57 nmol/L Failed to rise 30 and 60 min- 55 and 60 nmol/L,
respectively. ACTH was 178 pmol/L (normal<46 pmol/L) Consistent with primary adrenal insufficiency. Adrenal CT - showed bilateral adrenal haemorr
hages


Chest radiography confirmed right basal pneumonia.
She received intravenous hydrocortisone and antibiotics, and made an uneventful recovery.

Thank you
For your attention