Embed Size (px)
Citation preview

10
Nutrition and ulcerative colitis
ANN BURKE MB, BCh, BAO Fellow in Gastroenterology Department of Medicine, Division of Gastroenterolog)
GARY R. LICHTENSTEIN MD
Assistant Professor of Medicine, Director of IBD Program Department of Medicine, Divisiun of Gastroenterology
JOHN L. ROMBEAU” MD Professor of Surgery Department qf Surgery
Director Harrison Surgical Nutrition Research Laboratoq
Hospital of the Universiv of Pennsylvania, 3400 Spruce Street, Philadelphia, PA 19104, USA
The role of diet in the aetiology and pathogenesis of ulcerative colitis (UC) remains uncertain. Impaired utilization by colonocytes of butyrate, a product of bacterial fermen- tation of dietary carbohydrates escaping digestion, ma9 be important. Sulphur-fermenting bacteria may be involved in this impaired utilization. Oxidative stress probably mediates tissue injury but is probably not of causative importance. Patients with UC are prone to malnutrition and its detrimental effects. However, there is no role for total parenteral nutrition and bowel rest as primary therapy for UC. The maintenance of adequate nutrition is very important, particularly in the peri-operative patient. In the absence of massive bleeding, perforation, toxic megacolon or obstruction, enteral rather than parenteral nutrition should be the mode of choice. Nutrients may be beneficial as adjuvant therapy. Butyrate enemas have improved patients with otherwise recalcitrant distal colitis in small studies. Non-cellulose fibre supplements are of benefit in rats with experimental colitis. Eicosapentaenoic acid in fish oil has a steroid-sparing effect which, although modest, is important, particularly in terms of reducing the risk of osteoporosis, but it seems to have no role in the patient with inactive disease. y-Linolenic acid and anti-oxidants also are showing promise. Nutrients may also modify the increased risk of colorectal carcinoma. Oxidative stress can damage tissue DNA but there are no data published at present on possible protection from oral anti-oxidants. Butyrate protects against experimental carcinogenesis in rats with experimental colitis. Folate supplementation is weakly associated with decreased incidence of cancer in UC patients when assessed retro- spectively. Vigilance should be maintained for increased micronutrient requirements and
* Corresponding author
BaiWre k Clinical Gastroenterolopy- 153 -. Vol. 11, No. 1, March 1997
ISBN O-702&23 10-8 0950-3528/97/010153+22 $12.00/00
Copyright 0 1997, by Baillkre Tindall All rights of reproduction in any form reserved

154 A. BURKE ET AL
supplements given as appropriate. Calcium and low-dose vitamin D should be given to patients on long-term steroids and folate to those on sulphasalazine.
Key words: ulcerative colitis; butyrate; fish oil; anti-oxidants.
The aim of this review is to analyse critically the role of nutrition in ulcerative colitis (UC). The roles for diet in the aetiology of UC and in its treatment and in the maintenance of nutrition in the patient, as well as the possibility of using nutrition as a therapy, will be addressed. The roles of nutrition in colorectal cancer, micronutrients and interaction of drugs and nutrition as they pertain to UC will also be discussed.
ROLE OF NUTRITION IN THE PATHOGENESIS OF UC
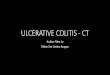
The aetiology of idiopathic inflammatory bowel disease by definition remains unknown. Because it is an enteric condition it is logical to consider diet as a possible aetiological factor. Several studies on the relationship of diet and inflammatory bowel disease have been undertaken but have not been particularly conclusive. The relevant diet may have occurred years prior to the onset of disease, and information from recalled dietary intake is unreliable. Whether dietary factors are aetiological, consequential or coincidental to inflammatory bowel disease is unknown (Sandler, 1993) Anumber of possible effects of diet on the pathogenesis of UC will be explored (Figure 1).
Butyrate
One of the many theories is that of the ‘starving colonocyte’ as proposed by Roediger (1990). Butyrate is the main fuel of the colonocyte (Roediger, 1980b) just as glutamine is the main oxidizable substrate of the enterocyte. Unlike other organs, the intestine receives its nutrients from both luminal as well as vascular sources. Indeed, 70% of the fuel requirements of the colonic mucosa are derived from butyrate and other short-chain fatty acids (SCFAs) which are the products of fermentation of dietary fibre and undigested starch by the anaerobic intestinal flora (Roediger, 1990). Concentrations of butyrate in the serum are negligible (Cummings et al, 1987) suggesting the colonocytes must obtain butyrate primarily from the lumen. The distal colon is less able than the proximal colon to utilize other fuels, a finding in keep- ing with the distribution of UC affecting distal bowel first and extending proximally. In isolated human colonocytes cultured in the presence of adequate butyrate, the percentage of oxygen consumption attributable to the utilization of n-butyrate was 73% for ascending colon and 75% for descend- ing colon (Roediger, 1980b). In the absence of butyrate but in the presence of glucose, the percentage oxygen consumption attributable to the utilization of glucose was 80% for ascending colon colonocytes and 30% for descend- ing colon colonocytes. In the presence of adequate glucose and 10mM butyrate, these decreased to 41% and 16%, respectively.
Diversion colitis, which occurs in some patients in the colonic segments

NUTRITION AND ULCERATIVE COLITIS 155
Normal colonocyte Plentiful fibre is fermented by colonic microflora to yield adequate amounts of butyrate. N-3 fatty acids modulate the potency of inflammatory cytakines. Less chemotaxis leads to less neutrophll activity. Antiwdants limit damage from free radicals.
Diseased colonocyte Scant flbre yields smaller amounts of butyrate. Its utilization is impaired by the effects of sulphate reducing bacteria. N-6 fany acids are convertad into potent cytokines. Activated neutrophils release free radicals which are not neutralized due to the lack of free radical scavengers.
Figure 1. Possible nutrient mediated mechanism in the pathogenesis of ulcerative colitis.
diverted from the faecal stream by surgery, when extensive, has an endo- scopic appearance indistinguishable from UC. Other than the absence of crypt abscesses its histological appearance is also quite similar (Komorowski, 1990). SCFA enemas instilled twice daily into the colon over a 6-week period, in open-label studies, improved diversion colitis in four patients (Harig et al, 1989). However, a 2-week trial in a double-blind study did not demonstrate efficacy (Guillemot et al, 1991), perhaps because the duration of the treatment was too short (Roediger, 1992). Colonocytes cultured from patients with quiescent UC demonstrate impaired utilization of butyrate. By measuring the rate of CO, production, Chapman et al (1994) demonstrated butyrate utilization in normal specimens to be almost double that in UC specimens obtained at endoscopy from normal-appearing colon in asympto- matic patients with quiescent colitis. The rates of utilization of glutamine and glucose were the same in normal and patient specimens and were much lower than that of butyrate. This confirmed the earlier work of Roediger (1980a), which had been called into question because of doubt about the viability of the cell suspensions. However, another study of a similar design failed to show differences in butyrate utilization in UC (Florin et al, 1991).

156 A. BURKE ET AL
Sulphides
Removal of oxygen to achieve an anaerobic environment within the colonic lumen is facilitated by the presence of reducing agents most of which contain sulphur, mercaptides, such as hydrogen sulphide (H,S), methanethiol and mercaptoacetate. Sulphur for fermentation in the colon is derived from transmural extraction mainly as sulphated mucopoly- saccharides, or from dietary sources including amino acids and crnciferous vegetables (Roediger et al, 1993a).
Limited attention has been given to the injurious nature of H,S to colonocytes. The colon contains levels of H,S that would be highly toxic to lung or brain (Roediger et al, 1993b). Colonocytes contain the highest activity of S-methyltransferase of all bodily tissues (Weiseger et al, 1990). This enzyme acts on S-adenosyl-L-methionine (SAM) to methylate sulphide to methanethiol, which is six times less toxic than sulphide to colonocytes (Roediger et al, 1993b). Exogenous methionine strongly increases SAM levels (Eloranta, 1977). Mercaptides inhibit butyrate but not glucose oxidation by colonocytes at concentrations of 5 mmol/l, which is a level found in the colonic lumen. This effect was more marked in colonocytes taken from the distal colon than from the proximal colon (Roediger et al, 1993a). It confirmed studies done earlier in animals (Roediger and Nance, 1990). The mechanism whereby sulphides impair butyrate utilization is unclear but may be via the interaction with co- enzyme-A to form a coenzyme-A-persulphite complex, which inhibits SCFA dehydrogenases and impairs ketogenesis from butyrate. Cell membranes of colonocytes in UC show structural abnormalities which are specific to the disease and which suggest impaired lipogenesis in colono- cytes. Lipogenesis from butyrate, by cultured colonocytes, is stimulated by the presence of glucose, an effect which is reversed by mercaptoacetate. This in turn was reversed by 5-amino salicylic acid (5-ASA). The mech- anism by which this is achieved is unclear. Altered cell membranes may lead to altered barrier function, a feature of UC (Roediger et al, 1992).
Luminal levels of sulphides are significantly higher in patients with UC compared with controls (Florin et al, 1990; Gibson et al, 1991). The increasing sensitivity of more distal than proximal mucosa to the effects of mercaptides and the impaired utilization of butyrate caused by mercaptides, an effect which is reversible, are all compatible with the clinical observations of UC and suggest that mercaptides may play a role in the pathogenesis of UC (Roediger et al, 1993a). Sulphate-reducing bacteria were detected in the faeces from 96% of UC patients studied compared to 75% of controls (P= 0.02) (Velazquez et al, 1996a). Dietary intake and intestinal absorption are the main factors which affect the amount of sulphate entering the colon (Florin et al, 199 1). There are no published data on manipulating dietary intake of sulphates in UC.
Oxidant injury
Various studies have showed evidence of oxidative stress in the colon in UC

NUTRITION AND ULCERATIVE COLITIS 157
(Ahnfelt-Ronne et al, 1990; Yamada and Grisham, 1993; Grisham, 1994) as well as an impaired ability to counteract this oxidative injury (Bhaskar et al, 1995; Buffington and Doe, 1995). Yet the evidence for a direct causative role of oxidative stress in inflammatory bowel disease remains circumstantial. Other than one anecdotal report of remission with high doses of vitamin E in conjunction with iron (Bennet, 1986) and relapse on discontinuing it, there are no published data on the effects of dietary pro- or antioxidants on UC. In this case report, it was proposed that the iron complexed with the vitamin E to produce a-tocopherylquinone (a-TQ) and it is likely that the a-TQ was functioning as an anti-oxidant (Guthy, 1986). Whereas it is possible that oxida- tive stress is involved in mediating the injury of UC (and will be discussed later in this regard) it is less likely that it is of direct aetiological importance.
Pantothenic acid
In pigs, pantothenic acid deficiency produces a colitis resembling human UC. With supplementation, symptoms resolve rapidly, although histo- logical changes are slower to improve (Wintrobe et al, 1943). The colitis is associated with low tissue levels of coenzyme-A. This is the active form of pantothenic acid (Nelson, 1968) and is involved in ketogenesis from butyrate by the colonocyte. Low tissue levels of coenzyme A have been found in the mucosa of UC patients despite normal serum and tissue levels of pantothenic acid (Ellestad-Sayed et al, 1976).
NUTRITION AS PRIMARY THERAPY FOR UC
The development of total parenteral nutrition (TPN) has permitted provision of long-term nutrients to a patient with a non-functioning bowel or to bypass the bowel to allow it to rest. Two early studies showed a potential benefit from TPN as primary therapy in ulcerative colitis but they had only five patients each and were retrospective, uncontrolled studies (Dean et al, 1976; Fazio et al, 1976). Subsequent, larger retrospective studies were less promising, with over half of the patients requiring surgery during the initial hospitalization and many of the others relapsing after discharge (Fischer et al, 1973; Reilly et al, 1976; Harford and Fazio, 1978; Mullen et al, 1978; Hanauer et al, 1984). (Table 1). These have been reviewed and summarized many times (Afonso and Rombeau, 1990; Bartels et al, 1995; Gassull et al, 1995). The randomized prospective studies by Dickson (Dickson et al, 1980) and McIntyre (McIntyre et al, 1986) finally laid to rest any question of TPN and bowel rest as primary therapy for UC. They showed no significant differences in remission or surgery rates in 36 and 27 acute UC patients respectively, compared to controls. They concluded that TPN is not indicated as primary therapy for UC. Dickson’s study (Dickson et al, 1980) did indicate that TPN provided a nutritional benefit to the study patients. This occurred at a cost of significant complications in three of 20 patients receiving TPN (one haemothorax, one pneumothorax and one catheter-related sepsis).

Table
1.
Total
pa
rente
ral
nutri
tion
for
ulcer
ative
co
litis.
Refer
ence
St
udy
type
UC
Total
no
. of
patie
nts
Contr
ols
Mean
fo
llow
Comp
licati
ons
of G
IBD
patie
nts
with
TP
N for
TPN
St
eroid
s up
per
iod
Outco
me
TPN
(all
patie
nts)*
Go
Dean
et a
l (19
76)
Mulle
n et
al (1
978)
Re
trosp
ectiv
e
Reilly
et
al (1
976)
Re
trosp
ectiv
e
Fisch
er et
al (1
973)
Re
trosp
ectiv
e
Hana
uer
et al
(198
4)
Retro
spec
tive
Fazio
et
al (1
976)
; se
e Ha
rford
an
d Fa
zlo
( 197
8)
Retro
spec
tive
Harfo
rd
and
Fazio
(1
978)
Fo
llow-
up
of fiv
e su
cces
ses
in ab
ove
study
Elso
n et
al (1
980)
Pr
ospe
ctive
no
n-ra
ndom
Dick
son
et al
(I 98
0)
Pros
pecti
ve
rand
omize
d
Retro
spec
tive
McInt
yre
et al
(198
6)
Pros
pecti
ve
rand
omize
d
16
5 NO
llfZ
74
24
34
II
13
4
38
38
71
s
5 s
30
IO
36
13
47
IS
None
None
None
None
None
None
NOlIe
14
I2
‘As
Indica
ted’
Hosp
ital
stay
‘Ofte
n’
‘Mos
t’ ?A
ll
All
N/A
N/A
N/A
All
All
All
6-12
0 mo
nths
Hosp
ital
stay
>6 m
onths
27 m
onths
Hosp
ital
stay
741
month
s
I surg
ery
I che
st tub
e
IS s
urgery
5
relap
ses
IO s
urgery
3 su
rgery
I9 su
rgery
4 re
lapse
d+su
rger
y
I surg
ery
(add
itiona
l pa
tient
on
adju
vant
TPN
impr
oved
en
ough
to
avoid
op
)
2 su
rgery
3 re
lapse
s no
surg
ery
Up t
o 43
mon
ths
6 su
rgery
3 re
lapse
s (I
surge
ry)
I.311
ye
ars
TPN
7 su
rgery
5 re
lapse
(2
surge
ry)
Contr
ol 6
surge
ry (I
died)
; 3
relap
se
(2 su
rgery)
43
TPN
9 su
rgery
(I die
d)
4 re
lapse
Co
ntrol
5 su
rgery
(2 die
d)
4 re
lapse
?
I pne
umoth
orax
I c
andid
a se
psisA
ied
3 pn
eumo
thora
x 3
line
infec
tion
2 pn
eumo
thora
x 6
line
infec
tion-
l die
d I s
uhcla
vian
vein
thr.
I pne
umoth
orax
2
line
infec
tion
N/A
2 pn
eumo
thora
x I e
xtrav
asati
on
1 sub
clavia
n ve
in thr
. 1 d
eath
(C
NS
embo
lus)
none
4 lin
e inf
ectio
n I a
ir em
bolus
I
PE
I pne
umoth
orax
I h
aemo
thora
x I l
ine s
epsis
> I p
neum
othor
ax
z i m N/
A No
t av
ailab
le.
* No
t inc
luding
me
taboh
c co
mplic
ation
s. t
Four
of eig
ht
requ
ired
surge
ry.
4 k r

NUTRITION AND ULCERATIVE COLITIS 159
NUTRITION AS ADJUVANT THERAPY FOR UC
Indications for total parenteral or enteral nutrition in UC
Malnutrition is common in UC even though it may not be as severe or as frequent as with Crohn’s disease (Seidman, 1989). Weight loss occurs in 18-62% of adults. Ten per cent of children with UC experience growth failure and 20% pubertal delay. UC patients tend to present relatively acutely while still in a state of adequate nutrition which deteriorates if nutrition, sufficient to meet the increased needs of the patient, is not pro- vided (Gassull et al, 1996). Nutrient .intake is often decreased in UC patients because they restrict food to avoid diarrhoea or are required to fast for various investigative studies. Every day of fasting produces a negative nitrogen balance for which 3-5 days of optimal nutrition are needed to repair (ASPEN Board of Directors, 1986). Acute attacks are associated with increased protein loss from the gastrointestinal tract (Stuart Welch et al, 1937; Powell-Tuck, 1986) while at the same time the increased circulating levels of inflammatory mediators interfere with appetite and protein intake (Powell-Tuck, 1986). It is because of this that enteral supplements can be effective where oral nutrition fails (Gassull et al, 1996).
Most previously healthy adults can tolerate weight loss of 5-10% with little functional consequence (Burress Welbom and Moldawer, 1997). Losses of body weight in excess of 25-30% are associated with significant morbidity. Nutrition-associated complications include death, sepsis, abscess formation and other infections, poor wound healing and respiratory failure. The risk of complications increases with the degree of malnutrition (Detsky et al, 1994). Energy expenditure is increased in active UC (Klein et al, 1988) at a time when intake tends to be reduced. A Subjective Global Assessment using nutrition has been devised by Detsky et al (1987). It is reproducible and correlates well with indicators of hospital morbidity (Baker et al, 1982; Jeejeebhoy et al, 1990). Using a subjective scale comparing multiple indices, a grading of well-nourished, moderate or severe malnutrition can be applied to each individual (Table 2). Patients who are moderately or severely malnourished should receive nutritional support. The assistance of a dietitian is invaluable in formulating appro- priate nutritional support. Patients who present with acute severe colitis have a high rate of early surgery. Recognition of malnutrition-related complications and the reduced morbidity associated with the delivery of parenteral nutrition has led to extensive use of nutritional support in the peri-operative period. Despite this, no definite conclusions can be ascertained from the existing data on peri-operative nutrition (Poret and Kudsk, 1990). The American Society for Parenteral and Enteral Nutrition has published guidelines (ASPEN Board of Directors, 1986) which suggest that nutritional support be given if 7-10 days of post-operative starvation is expected in a previously healthy patient, or 5-7 days in a previously mal- nourished patient, which includes many patients with active UC (Poret and Kudsk, 1990). Patients with severe acute colitis undergoing or likely to undergo colectomy have a high metabolic stress. This occurs in the face of

160 A. BURKE ET AL
protein and blood loss from an inflamed gastrointestinal tract and decreased intake from the anorexia associated with significant inflammation. They are in a group who should receive TPN within l-3 days of fasting. Minimal stress in a well-nourished patient where gastrointestinal function is expected to return within 10 days, such as in a patient with a mild to moderate flare of brief duration, is not an indication for TPN (ASPEN Board of Directors, 1986).
Table 2. Subjective global assessment of nutritional status
Well Moderate Severe Criterion nourished malnutrition malnutrition
Weight loss measured as a percentage of body <5% 5-10% >lO% weight; recent stabilization of weight or recovery of weight lost is also important
Dietary intake is assessed as a percentage of nutritional requirements
100% 70-90% < 70%
GI symptoms
Functional capacity
Loss of subcutaneous fat, assessed at triceps and costal margin in mid-axillary line
None Intermittent Daily, > 2 weeks
At baseline Some limitations Bedridden
None Slight Marked
Loss of muscle bulk, at quadriceps and deltoids None Slight Marked
Peripheral oedema None Slight Marked
Ascites None Slight Marked
Finally, based on the above information but without using any formal scoring system, the patient is assigned a nutritional state of well nourished, moderately malnourished or severely malnourished- the subjective global assessment
Reproduced from Rombeau and Afonso (1992, Inflammatory Bowel Disease, MacDermott RP & Stenson W (eds), pp 525-553, New York: Elsevier) with permission.
Total enteral nutrition or total parenteral nutrition?
Despite studies indicating its lack of efficacy, the temptation remains to use the parenteral rather than the enteral route for alimentation in the UC patient. There is a concern that total enteral nutrition (TEN) will only exacerbate the patient’s diarrhoea and inflammation even though it has already been shown that oral diet is as well tolerated as TPN in acute colitis patients (Dickson et al, 1980; McIntyre et al, 1986). Rats with experimental colitis gained a protective effect when pectin was added to their enteral feed compared to fibre-free enteral nutrition or the same diet given parenterally (Rolandelli et al, 1988). Non-cellulosic fibres are completely fermented in the colon providing short-chain fatty acids without adding bulk. Rao et al (1987) showed that active UC patients have normal fat and xylose absorption and that the diarrhoea is secretory. The introduction of total enteral nutrition (TEN) after 24 hours of fasting was associated with a slight but insignificant increase in diarrhoea and was very well tolerated. The diarrhoea settled as the corticosteroids took effect. They achieved improved nutritional status comparable to that of Dickson’s study. Gonzalez-Huix et

NUTRITION AND ULCERATIVE COLITIS 161
al (1993) also demonstrated equal nutritional improvement with TPN and TEN in inflammatory bowel disease patients with fewer complications in the TEN group. TEN is also considerably less expensive than TPN. Currently, most commercially available enteral supplements contain little or no fibre. Absolute contra-indications to TEN in inflammatory bowel disease are massive haemorrhage, bowel perforation, toxic megacolon and intestinal obstruction (Gassull et al, 1996).
Oral nutrition
Not to be forgotten is the well-balanced healthy diet for the patient with mild to moderate disease who is being managed as an outpatient. It is important to avoid unnecessary dietary restrictions. Many patients put themselves on very restrictive diets to avoid diarrhoea. Lactose intolerance occurs at the same rate in UC patients as in the general population and so lactose need not be restricted routinely. Its prevalence is dependent on race: Northern Europeans 5-15%, African-Americans 45-80%, Asians 90- 100% (Lloyd and Olsen, 1995). There have been no studies demonstrating advantage of soluble or insoluble fibre in UC. In quiescent or mild UC there is probably no reason to avoid fibre and possibly several beneficial effects to support its use. These include the trophic (Fleming and Arce, 1986; Chapman et al, 1994) and anti-inflammatory (Rolandelli et al, 1988) effects that fibre has been shown to have on the colon in rats. In addition, butyrate was demonstrated to inhibit the development of colon cancer in rats (D’Argenio et al, 1996) and to promote the differentiation of several human colon and other cancer cell lines in vitro (Kim et al, 1982; Dexter et al, 1984; Kruh et al, 1991; Young, 1991; Hague et al, 1993). In a double-blind placebo-controlled cross-over study, patients with ulcerative colitis in remission reported improved gastrointestinal symptoms on ispaghula husk compared to controls (Hallert et al, 1991). At the very least, over the 2-month study period no adverse effects were noted. However, more in vivo studies are needed in this area.
SPECIFIC NUTRIENTS AS ADJUVANT THERAPY FOR ULCERATIVE COLITIS
Butyrate
Following its success in the treatment of diversion colitis, several small trials have been performed to assess the impact on UC of butyrate given by enema. The mixed results are reviewed in Chapter 7. Larger prospective trials need to be done to assess its true efficacy. In a rat model, the administration of an enteral diet supplemented with indigestible oligo- saccharide (a putative butyrate precursor) was associated with anti-inflam- matory activity that was similar in efficacy to sulphasalazine (Grisham et al, 1996).

162 A. BURKE ET AL
Eicosapentaenoic acid and gamma linolenic acid
A primer in lipids and injlammation
Fatty acids are identified by the number of carbons (C20) followed by the number of double bonds, (C20:4), followed by the identification of the position of the first double bond, (C20:4 n-6).
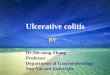
The two essential fatty acids are linoleic acid (C 18:2 n-6) and a-linolenic acid (C18:3 n-3) of which the daily requirements are approximately 2.5-5 g of linoleic and 2-3 g of a-linolenic acid per day. By a series of desaturation and elongation steps, linoleic acid is converted to y-linolenic acid (GLA) to dihomo-y-linolenic acid (DHLA) to arachidonic acid (C20:4 n-6), and a- linolenic acid is converted to stearidonic and to eicosapentanoic acid (EPA) (C20:5 n-3) via a C20:4 n-6 intermediary (Rolandelli and Ullrich, 1997) (Figure 2).
Evening Primrose Oil I Fish 011
Li lolipase
pG~~~~ PGI,‘antl-inflammatory PGI,‘anti-inflammatory ver;potent LTBS
TXA, prwnflammatory TXA, pro-Mammatory chemoattractant weak chemo- attractant
Figure 2. Modification of eicosanoids in ulcerative colitis. Phospholipase releases arachidonic acid from the cell membrane. It is converted to prostaglandins of the 2 series by cycle-oxygenase and to leukotrienes of the 4 series by S’lipoxygenase. Supplementing the diet with evening primrose or fish oils enriches the membrane lipid content of GLA and EPA respectively which, in turn, are converted to 1 and 3 series prostaglandins and the EPA is converted to 5 series leukotrienes. PGEI can inhibit the action of phospholipase, so decreasing the release of arachidonic acid, the rate limiting step in PG synthesis. AA = arachidonic acid, DHLA = dihomo-gamma linolenic acid, EPA = eicosapentaenoic acid; GLA = gamma hnolenic acid; LT = leukotriene; PG = prostaglandin; TX = thromboxane.
Arachidonic acid, an o-6 fatty acid, is the substrate of the cyclo- oxygenase 1 and 2 enzymes which synthesize prostaglandins (PG) of the 2 series e.g. PGE,, PGF,, PGI, and the 5’-lipoxygenase enzymes which synthesize leukotrienes (LT) of the 4 series e.g. LTB, the main neutrophil chemo-attractant in UC (Lobos et al, 1987). These derivatives of arachidonic acid are collectively known as eicosanoids and are important mediators of inflammation. The release of arachidonic acid from membrane phospholipids by phospholipase A, is the rate-limiting step in eicosanoid synthesis. Glucocorticoids generate a membrane-bound protein called

NUTRITION AND ULCERATIVE COLITIS 163
lipocortin which reduces arachidonic acid release and thus reduces the production of all eicosanoids (Schumert et al, 1988). Fish oil is high in the w-3 fatty acids, eicosapentaenoic acid (EPA) and docosahexaenoic (DHA) (C22:5 n-3) acid. EPA can act as an alternative substrate for these enzymes to yield LTB,, which is 30 times less potent than LTB, in stimulating neutrophil chemotaxis (Terano et al, 1984; Lee et al, 1985). Moreover, PGI, is synthesized in favour of PGI,. They have approximately the same anti- inflammatory activity, and thromboxane A, (TXA,) is synthesized in preference to the more pro-inflammatory TXA, (Greenfield et al, 1993).
Evening primrose oil and borage oil are high in GLA (C18:3 n-6). GLA is rapidly converted to DHLA (C20:3 n-6) and competes with arachidonic acid for the cycle-oxygenase enzymes yielding prostaglandin PGE, in preference to PGE,. PGE, raises intracellular CAMP which inhibits phospholipase and the release of arachidonic acid from cell membranes (Greenfield et al, 1993). DHLA is converted to its 15-lipoxygenase product which is also anti-inflammatory in that it inhibits the actions of 5-lipoxy- genase which is responsible for the synthesis of LTB,.
Fish oil
With improved understanding of the role of eicosanoids in the pathogenesis of inflammation has come an interest in trying to alter this inflammatory response by modifying tissue fatty acid and phospholipid content. A low incidence of UC is noted in Japan where fish consumption is high (Sandler, 1993), but no studies assessing fish consumption in UC have been published. UC is associated with a marked neutrophilic infiltrate in the diseased colon. LTB, is a potent neutrophil chemotactic agent and is the main neutrophil chemo-attractant in UC (Lobos et al, 1987). In patients with UC, concentrations of LTB, and PGE, in rectal dialysates are increased, and the levels correlate with disease activity (Lauritsen et al, 1986). Fish oil increases the concentration of the less potent pro-inflam- matory agent LTB, in lieu of LTB, (Terano et al, 1984; Lee et al, 1985). Modulating plasma lipids alters their physical properties. It is possible that EPA could have a beneficial effect independent of leukotrienes. Marotta et al (1995) showed a protective effect of EPA on experimental colitis induced by dextran sulphate in rats. In their study dextran sulphate altered membrane lipids when compared to controls but this alteration did not occur when EPA was given at the same time. Eicosanoid levels were not assessed in this study.
Several studies have been performed to investigate the effects of fish oil supplementation on membrane lipid composition, inflammatory mediators and UC. A case report using intravenous fish oil supplements demonstrated marked increase in tissue EPA and DHA until they exceeded the levels of arachidonic acid. This was associated with LTB, levels greater than LTB, levels, and TXB, levels greater than TXB, levels. This enrichment was maintained only to a minor extent with oral supplements. Colitis activity was decreased during periods of parenteral but not enteral supplementation (Grimminger et al, 1993). Several studies have investigated oral EPA

164 A.BURKE ETAL
supplements, in the form of fish oil capsules, for the treatment of UC (McCall et al, 1989; Salomon et al, 1990; Aslan and Triadafilopoulos, 1992; Hawthorne et al, 1992; Stenson et al, 1992; Greenfield et al, 1993) (Table 3). The results of early open label studies were very promising (McCall et al, 1989; Salomon et al, 1990). Larger, more controlled trials have shown more modest but consistent results. It would seem that in active disease, fish oil supplements have a steroid-sparing effect (Aslan and Triadafilopoulos, 1992; Hawthorne et al, 1992; Stenson et al, 1992), but have no prophylactic effect on quiescent disease to maintain remission (Hawthorne et al, 1992; Greenfield et al, 1993).
Gamma linolenic acid
GLA is present in large quantities in evening primrose oil and borage oil. It has become popular as a ‘health food supplement’ and has been used in small studies in rheumatoid arthritis (Leventhal et al, 1994; DeLuca et al, 199.5). By promoting PGE, in favour of PGE, production, it inhibits arachidonic acid release and eicosanoid synthesis. In 19 patients with mild or quiescent colitis, compared to eight controls, GLA administration led to increased tissue levels of DHLA and improvement in stool consistency in eight patients (Greenfield et al, 1993). This effect was maintained 3 months after discontinuation of GLA. GLA has not been studied in more active disease. GLA improves P-oxidation of fatty acids in the liver in rats (Takada et al, 1994); however, whether it enhances colonocyte P-oxidation of butyrate and other fatty acids is unknown. The possibility also exists that prolonged administration could eventually lead to increased tissue arachidonic acid counteracting its original inhibitory effect (Phinney, 1994). At present, there is no clear evidence to advocate the use of GLA supplementation in UC.
Anti-oxidants
A primer in oxidative stress
A free radical is any chemical species capable of independent existence and containing one or more unpaired electrons (Gutteridge, 1995). Reactive oxygen species are free radicals which contain oxygen, e.g. superoxide anion O,‘-, which is produced during the respiratory burst in the activated neutrophil, and hydroxyl radical *OH, which is many times more potent than the superoxide anion. Reactive oxygen species mediate the injury of inflammation. They are produced enzymatically by activated neutrophils and macrophages and non-enzymatically by the Fenton or Haber-Weiss reaction (Grisham and Granger, 1988; Schumert et al, 1988):
Together
O,‘- + Fe3+ -+ 0, + Fe*+ H,O, + Fe2+ + *OH + OH- + Fe3+
O;- + H,O, + *OH + OH- + 0,

Refer
ence
Ty
pe
of stu
dy
Table
3.
Fish
oil
and
even
ing
prim
rose
oi
l for
ulc
erati
ve
coliti
s.
Numb
er
Wee
ks
of Do
se
of EP
A +
of pa
tients
Pa
tients
on
PO
Dise
ase
study
/trea
tmen
t DH
A (g/
day)
(stud
y/con
trol)
stero
ids/S
-ASA
ac
tivity
Ou
tcome
McCa
ll et
al (1
989)
Op
en
label
12/1
2
Salom
on
et al
(199
0)
Open
lab
el 8/8
Aslan
an
d Do
uble
blind
48
/12
Triad
afilop
oulos
Cr
oss-o
ver
(199
2)
*
Sten
son
et al
(I 99
2)
Doub
le bli
nd
36/l
6 Cr
oss-o
ver
Hawt
horn
e et
al (1
992)
Do
uble
blind
52
/.52
Rand
omize
d Co
ntro
lled
Gree
nfield
et
al (1
993)
Ra
ndom
ized
4314
3 Co
ntro
lled
3-4
+ N/
A
2.7+
1.8
2.7+
I.8
Plac
ebo’1
3.24+
1.2
6 Pl
aceb
oi
4.8 +
I .2
Pl
aceb
o6
l.13+
1.2
2 GL
A 0.2
4 Pl
aceb
o’j
6/6+
I o/o
I l/C
ross-o
ver
24iC
ross-o
ver
46lS
O
1618
I9
on e
venin
g pr
imro
se
oil
04
O/3
Activ
e
S/8
Activ
e
2/l
I Mi
ld-mo
dera
te
6112
Ac
tive
EPA
N/A/
38
Activ
e 56
pla
cebo
N/
A 30
Re
miss
ion
40
media
n pr
ed.
IO m
g in
both
grou
ps
EPA
l/l 1
Mode
rate
1 GL
A l/1
7 Mi
ld 29
co
ntrol
O/4
Remi
ssion
I3
6/6
symp
tomati
c im
prov
e-
ment
at
4 we
eks;
616
in re
miss
ion
at 12
wee
ks
71 IO
sym
ptoma
tic
and
endo
- sc
opic
impr
ovem
ent;
4/5
decre
ased
ste
roid
dose
Daily
ac
tivity
ind
ex
decre
ased
56
%
in EP
A ve
rsus
4%
in co
ntrols
; 8/
l I
decre
ased
or
elimi
- na
ted
other
me
dicati
ons
Impr
oved
his
tolog
y an
d re
ctal
LTB4
co
mpar
ed
to pla
cebo
; 53
%
decre
ase
in ste
roid
requ
ireme
nts
on
EPA
(P =
NS)
Activ
e dis
ease
; me
dian
pred
nison
e do
se
at 2
month
s 0
mg (
EPA)
5
mg
(contr
ol)
(P =
0.01
) re
miss
ion:
no e
ffect
EPA
no e
ffect
GLA
impr
oved
sto
ol co
nsist
ency
* Co
ntrols
we
re
healt
hy
volun
teers
given
EP
A.
i- Pl
aceb
o ole
ic ac
id IO
.3 g,
palm
itic
acid
2. I
g, lin
oleic
acid
I .8
g da
ily.
$ Pl
aceb
o (ve
getab
le oil
) ole
ic ac
id 12
.36
g, pa
lmitic
ac
id 2.5
2 g,
linole
ic ac
id 2.
I6 g
daily
. 8
Plac
ebo
(oliv
e oil
) ole
ic ac
id 72
%,
palm
itic
acid
l2%,
linole
ic ac
id I I
%.
¶ Fis
h oi
l (E
PA
2.25
g/day
+
DHA
I .4S
g/da
y for
I
mont
h,
then
EPA
I. I3
g/day
+
DHA
I .22
g/da
y for
5
month
s).
Even
ing
prim
rose
oi
l (G
LA
0.47
g/day
for
I
mont
h the
n 0.2
4 g/d
ay
for
S mo
nths).
Ol
ive
oil
(plac
ebo)
(o
leic
acid
8.28
g/day
, pa
lmitic
ac
id I .
64 g
/day,
linole
ic ac
id I .
45 g
/day
for
I mo
nth,
the
n 4.1
4, I.3
2 an
d I .
22 g
/day
resp
ectiv
ely,
for
5 mo
nths).

166 A. BURKE ET AL
The identity and availability of in vivo compounds that catalyse the Fenton reaction remain unknown (Grisham and Granger, 1988). However, haem proteins can release chelatable iron that can participate in Fenton chemistry (Gutteridge, 1995). The hydroxyl radical produced by the Fenton reaction is probably the chemical entity which initiates lipid (LH) peroxidation (Gutteridge, 1995):
LH + *OH + L* + H,O
This lipid radical can, in turn, react with molecular oxygen to form a hydroperoxide radical which can attack the next lipid (L’H) and a chain reaction has been set up (Kappus, 1985):
L* + o2 * LOO* LOO* + L’ + L’. + LOOH
Anti-oxidants such as vitamin E (TH), break the chain by forming stable intermediaries which can be further metabolized enzymatically to less harmful products (Kappus, 1985):
L’* + TH -+ LOOH + T*
or by enzymatically removing free radicals (Grisham and Granger, 1988; Kehrer and Lund, 1994):
2 o;- + 2H’
2H20, catalase ) O1 + H,O 2~s~ + H,O, glutathione peroxidz GSSG + 0 ‘7)
2
GSSG + NADPH + II+ glutathione reducta; 2GSH + NADP
Oxidative stress and UC
A direct role for oxidative stress as a pathogenic factor in chronic gut inflammation remains to be defined (Grisham, 1994) but indirect evidence abounds. In UC, activated neutrophils come in contact with chelate iron in stool, ideal for the Fenton reaction (Babbs, 1992). Several studies suggest a role for oxidative stress in UC. Ahnfelt-Ronne, in an elegant paper, demonstrated increased concentration of lipid peroxides in pre-treatment biopsies and normalization with treatment with 5-ASA in 15 patients with UC or Crohn’s colitis (the numbers with each diagnosis were not given) in conjunction with clinical improvement in disease activity (Ahnfelt-Ronne et al, 1990). He also showed that metabolites of 5-ASA formed in vitro by exposure to oxygen free radicals could be demonstrated in the faeces of patients with ulcerative or Crohn’s colitis treated with 5-ASA but not in rheumatoid arthritis patients with normal bowel function. The concen- trations of 5-ASA found in normal colonic mucosa (0.1-0.2 mmoV1) are much lower than that required to inhibit cycle-oxygenase and S’lipoxy- genase (I-10 mmol/l). Diseased mucosa from patients with UC can achieve levels five-fold normal, which is within the range required to scavenge free

NUTRITION AND ULCERATIVE COLITIS 167
radicals (0.01-0.4 mmol/l). Hydroxyl radicals require higher concen- trations of .5-ASA but are largely derived from superoxide radicals which are readily scavenged at 0.01-0.02 mmol/l (Grisham, 1994). Increased lipid peroxidation has also been demonstrated by Sedghi et al (1994). Bhaskar et al (1995) failed to show a significant increase in lipid peroxidation even though the patient levels were twice that of controls, but they used an assay less sensitive than that of Sedghi. Depletion of different colonic anti- oxidant defences in UC patients has been demonstrated in various studies (Mulder et al, 1991; Fields et al, 1994; Buffington and Doe, 1995). Salim used allopurinol, which is a potent scavenger of hydroxyl radicals and inhibits xanthine oxidase which forms superoxide radicals, and dimethyl sulphoxide (DMSO), which also scavenges hydroxyl radicals in a double- blind randomized controlled study (Salim, 1992). Patients received sulpha- salazine alone (51), sulphasalazine and allopurinol (50) or sulphasalazine, a,llopurinol and DMSO for 1 year. The treated groups, compared with controls, had improved remission (84% versus 5 1%) and relapse rates (5% versus 25%). Few studies have been done assessing the role of dietary anti- oxidants in UC. The use of high-dose a-tocopherylquinone (a-TQ), a likely product of vitamin E and iron interaction in vivo, is reported as a personal experience (Bennet, 1986). The author notes marked improvement with a-TQ and relapse within 2-3 days of stopping it. The mechanism of action is unclear but a-TQ does have potent anti-oxidant properties (Guthy, 1986). A study using vitamin C as a single agent in six patients with inactive to moderately active disease showed no effect on clinical parameters or neutrophil chemotaxis over a 6-month period (Hermanowicz et al, 1985). The role of other dietary anti-oxidant manipulations remains to be seen.
UC AND MALIGNANCY
The increased risk of colonic neoplasm with long-standing UC is well known. To date, there is no dietary intervention to alter this risk but a number of interesting possibilities warrant further exploration.
Butyrate
It is over 20 years since Burkitt suggested an association between colorectal cancer and a diet low in fibre (Burkitt, 1973). Some of this effect is possibly mediated by butyrate. Butyrate, although trophic to normal colonic mucosa, has an inhibitory effect on the replication of colon cancer cells in vitro, promoting apoptosis or differentiation (Kim et al, 1982; Dexter et al, 1984; Fleming and Arce, 1986; Kruh et al, 199 1; Young, 199 1; Hague et al, 1993). In an experimental model where colon cancer was induced in colitic rats, butyrate restored depressed transglutaminase levels and decreased the number and surface area of tumours compared with controls (D’Argenio et al, 1996). Transglutaminase is involved in apoptosis and reactions between extracellular matrix proteins. Butyrate alters the gene expression for several proteins, including those inducing transglutamine activity. In another study,

168 A. BURKE ET AL
butyrate decreased the amount of crypt surface proliferation, which, in comparison to crypt base proliferation, is a biomarker of colon cancer risk and increased c-&n expression (Velazquez et al, 1996b). c-&n is the key component of the AP-1 complex which mediates terminal differentiation- a state which, in turn, is associated with growth arrest. Intravenous infusion of butyrate reduced seeding and growth of malignant colorectal cells in vivo in mice (Velazquez et al, 1996a). No studies of sufficient duration have been done to assess possible similar protective effects in humans.
Anti-oxidants
Free radicals are known to mediate carcinogenesis. Indeed, the malignant effect of radiation is via free radical production. No studies have been published assessing a possible anticarcinogenic effect of anti-oxidants in UC.
Folate
In a retrospective study, folate supplementation was associated with a lower incidence of neoplasia in patients with UC (Lashner et al, 1989). A more recent cohort study of 98 patients, although failing to reach statistical significance, supports this, with a relative risk of 0.72 for neoplasia in UC patients taking folate supplements (Lashner et al, 1997). To date, no pros- pective, published data exist. However, because sulphasalazine impairs folate absorption by > 30%, it is probably wise to provide folate supple- ments routinely.
Fish oils
It is interesting to note increased levels of cycle-oxygenase-2 (the inducible form) in rat colonic tumours compared to areas of normal tissue in the same animals (DuBois et al, 1996). NSAIDs seem to exert a protective effect in colorectal cancer. The mechanism of this effect is unknown but it would seem not to be due to cycle-oxygenase inhibition (Alberts et al, 1995). That EPA or GLA might exert a similar effect is purely speculative.
MICRONUTRIENTS
The status of various micronutrients in UC is difficult to assess. There are relatively few studies examining this and most do not separate Crohn’s disease, with its small-bowel involvement, from UC. Malnutrition is common in UC, and iron deficiency occurs in two-thirds of patients (Seidman, 1989). Overt manifestations of micronutrient deficiency, other than iron, are rare in UC. Malitolli et al (1988) report a patient with severe UC who, despite several days of peri-operative TPN, including thiamine 3.2 mg/day, developed Wemicke’s encephalopathy. Deficiencies are more likely to occur during periods of increased disease activity when demands and losses are increased and intake decreased. Serum copper levels tend to

NUTRITION AND ULCERATIVE COLITIS 169
be increased in UC patients (Femandez-Banares et al, 1990; Ringstad et al, 1993). Serum levels of zinc have been reported to be decreased with an associated decreased vitamin A level (Femandez-Banares et al, 1990; Mulder et al, 1994), normal (Ainley et al, 1988) with normal absorption (Valberg et al, 1986), or increased (Ringstad et al, 1993). It is of interest that Mulder et al noted decreased copper and zinc metallothionein, which are free radical scavengers, in patients with UC compared to controls, and in inflamed mucosa compared to non-inflamed mucosa in UC patients. Tissue zinc is one of the many factors regulating metallothionein synthesis (Mulder et al, 1991). It is probably wise to measure Zn and Mg levels in the plasma in acutely ill patients and those with very long-term disease and supplement as needed. Likewise, low plasma levels of fat-soluble vitamins with low vitamin B, and elevated vitamin B, have also been reported in a study involving 12 UC and three Crohn’s colitis patients (Femandez- Banares et al, 1989). The significance of these findings in such a small group of patients is difficult to ascertain but, again, water and fat-soluble vitamins should be supplemented on an ‘as needed’ basis. Iron should be monitored in the ‘well’ patient also and supplemented as needed.
NUTRITIONAL IMPLICATION OF DRUG THERAPY
The two main drugs in the treatment of UC are glucocorticoids and 5-ASA compounds. Glucocorticoids, when given in pharmacological doses for extended durations, are associated with the development of osteoporosis. Part of this is due to steroid-mediated impaired intestinal absorption and renal resorbtion of calcium leading to secondary hyperparathyroidism and bone resorption (Nesbitt, 1995). Oral calcium supplementation decreases bone resorption (Reid and Ibbertson, 1986). Glucocorticoids also influence osteoblast function and bone turnover, so calcium supplementation alone will not prevent bone loss (Adler and Rosen, 1994). Vitamin D supple- mentation in unselected patients with glucocorticoid-induced osteoporosis simply led to hypercalcaemia. In patients on long-term or frequent steroids, calcium supplementation of l-l.5 g/day with the vitamin D supplemen- tation available in fortified dairy products or a simple multivitamin pill is probably worthwhile. Higher doses of vitamin D are warranted only in patients with proven vitamin D deficiency. As mentioned previously, patients taking sulphasalazine should also take folate supplements.
THE FUTURE
The low incidence of UC in Japan has been attributed in part to dietary factors. The Japanese diet, compared to the Western diet, is very high in soy bean products. Soy beans are known to contain protease inhibitors. One of these protease inhibitors which has received much attention is the Bowman-Birk inhibitor (BBI). It is possible that these protease inhibitors have an anti-inflammatory effect. Indeed, BBI prevents the production of

170 A. BURKE ET AL
the superoxide radical by stimulated neutrophils (Frenkel et al, 1987). Trials assessing its use in UC are in progress.
Due to its rapid absorption, butyrate is currently used only as an enema for the treatment of distal colitis. The development of butyrate precursors, e.g. fructo-oligosaccharides and xylo-oligosaccharides (Grisham et al, 1996), and formulations whereby the oral butyrate reaches the colon will allow the assessment of this treatment modality in more extensive colitis.
Finally, the definitive role for butyrate, fish oil, evening primrose oil and anti-oxidants remains to be clarified. Further studies will need to be done in this area.
REFERENCES
Adler RA & Rosen CJ (1994) Glucocorticoids and osteoporosis. Endocrinology und Metabolism Clinics of North America 23: 641-654.
’ Afonso JJ & Rombeau JL (1990) Parenteral nutrition for patients with inRammatory bowel disease. In Rombeau JL (ed.) Clinicul Nutrition: Purenteral Nutrition, pp 427-441. Philadelphia: W.B. Saunders.
Ahnfelt-Ronne I, Nielsen OH, Christensen A et al (1990) Clinical evidence supporting the radical scavenging mechanism of 5-aminosalicyclic acid. Gastroenterology 98: 1162-l 169.
Ainley CC, Cason J, Carlsson LK et al (1988) Zinc status in inflammatory bowel disease. Clinical Science IS: 271-283.
Alberts, DS, Hixson L, Ahnen D et al (1995) Do NSAIDs exert their colon cancer chemoprotective activities through the inhibition of mucosal prostaglandin synthetase? Journal of Cellular Biochemistry supplement 22: 18-23.
Aslan A & Triadafilopoulos G (1992) Fish oil fatty acid supplementation in active ulcerative colitis: a double-blind, placebo-controlled cross-over study. Arnericnn J<~ournal ofGa.~rroenterolofiy 87: 432-437.
‘ASPEN Board of Directors (1986) Guidelines for the use of total parenteral nutrition in the hospitalised adult patient. Jownaf offurenteral and Enteral Nutrition 10: 441-445.
Babbs CF (1992) Oxygen radicals in ulcerative colitis. Free Radical Biology und Medicme 13: 169-181.
Baker JP. Detsky AS, Wesson DE et al (1982) Nutritional assessment. A comparison of clinical judge- ment and objective measurements. New England Journal ofMedicine 306: 969-972.
Banels M, Nagel E & Pichlmayr R (1995) Welche Rolle spielt die Ernaehrung bie der Colitis Ulcerosa? Ein Beitmg zum heutigen Stellenwert der diaetetischen Therapie in der Behandlung entzuendlicher Darmerkrankungen. Lungenbecks Archive der Chirurgie 380: 4-l 1.
Bennet JD (1986) Use of a-tocopherylquinone in the treatment of ulcerative colitis. Personal experience. Gut 27: 695-697.
Bhaskar L, Ramakrishna BS & Balasubramanian KA (1995) Colonic mucosal antioxidant enzymes and lipid peroxide levels in normal subjects and patients with ulcerative colitis. Journul of Gustroenterology and Hepatology 10: 140-143.
Buffington G & Doe WF (1995) Depleted mucosal antioxidant defences in inflammatory bowel disease. Free Rudical Biology and Medicine 19: 91 I-918.
Burkitt DP (1973) Some diseases characteristic of modem western civilization. British Medical Jonmu 1: 274-278.
Burress Welbom M & Moldawer LL (1997) Glucose metabolism. In Rombeau JL & Rolandelli RH (eds) Clinical Nutrition: Enterctl md Tube Feediq, 3rd edn, pp 61-80. Philadelphia: W.B. Saunders.
Chapman MAS, Grahn MF, Boyle MA et al (1994) Butyrate oxidatia . LJ a+,,ired in the colonic mucosa of sufferers of quiescient ulcerative colitis. Gut 35: 73-70.
Cummings JH. Pomare EW, Branch WJ et al (1987) Short chain fatty acids in human large intestine, portal hepatic and venous blood. Gut 28: 1221-1227.
D’Argenio G, Cosenza V, Delle Cave M et al (1996) Butyrate enemas in experimental colitis and protection against large bowel cancer in a rat model. Gnstr~~ente,olo~~ 110: 1727-1734.

NUTRITION AND ULCERATIVE COLITIS 171
Dean RE. Campos MM & Barrett B (1976) Hyperalimentation in the management of chronic inflam- matory intestinal disease. Disease of the Colon and Rectum 19: 601-604.
DeLuca P, Rothman D & Zurier RB (1995) Marine and botanical lipids as immunomodulatory and therapeutic agents in the treatment of rheumatoid arthritis. Rheumatic Disease Clinics of North America 21: 159-711.
*Detsky AS, McLaughlin JR, Baker JPet al (1987) What is subjective global assessment of nutritional status? Journal of Parenteral and Enteral Nutrition 11: 8-13.
Detsky AS, Smalley PS & Chang J (1994) Is this patient malnourished? JAMA 271: 54-58. Dexter DL, Lev R, McKendall CR et al (1984) Sodium butyrate-induced alteration of growth
properties and glycogen levels in cultured human colon carcinoma cells. Histochemical Journal 16: 137-149.
*Dickson RJ, Ashton MC, Axon ATR et al (1980) Controlled trial of intravenous hyperalimentation and total bowel rest: as an adjunct to the routine therapy of acute colitis. Gastroenterology 79: 1199-1204.
DuBois RN, Radhika A, Reddy BS et al (1996) Increased cyclooxygenase-2 levels in carcinogen- induced rat colonic tumors. Gustroenterology 110: 1259-1262.
Ellestad-Sayed JJ, Nelson RA, Adson MA et al (1976) Pantothenic acid, coenzyme-A and human chronic ulcerative and granulomatous colitis. American Journal of Clinical Nutrition 29: 1333-1338.
Eloranta TO (1977) Tissue distribution of S-adenosylmethionine and S-adenosylhomocysteine in the rat. Biochemical Journal 166: 521-529.
Elson CO, Layden TJ, Nemchausky BA et al (1980) An evaluation of total parenteral nutrition in the management of inflammatory bowel disease. Digestive Diseases and Sciences 25: 42-48.
Fazio VW, Kodner 1, Jagelman DC et al (1976) Parenteral nutrition as primary or adjunctive treat- ment. Diseases qf the Colon and Rectum 19: 574-578.
Femandez-Banares F, Abad-Lacruz A. Xiol X et al (1989) Vitamin status in patients with inflam- matory bowel disease. American Journal of Gastroenterology 84: 744-748.
Femandez-Banares F, Mingorance MD, Esteve M et al (1990) Serum zinc, copper and selenium levels in inflammatory bowel disease: effect of total enteral nutrition on trace element status. American Journal of Gastroenterology 85: 1584-1589.
Fields JZ, Keshavarzian, A & Einzhamer D (1994) Low levels of blood and colonic glutathione in ulcerative colitis. Gastroenterology 106: A680 (abstract).
Fischer JE, Foster GS, Abel RM & et al (1973) Hyperalimentation as primary therapy for inflam- matory bowel disease. American Journal ofSurgery 125: 165-179.
Fleming SE & Arce DS (1986) Volatile fatty acids: their production, absorption, utilization, and roles in human health. Clinics in Gastroenterology 15: 787-814.
Florin THJ, Gibson CR, Neale G et al (1990) A role for sulphate reducing bacteria in ulcerative colitis, Gastroenierology 98: Al70 (abstract).
Florin T, Neale G, Gibson CR et al (1991) Metabolism of dietary sulphate: absorption and excretion in humans. Gut 32: 766-773.
Frenkel K, Chrzan K, Ryan CA et al (1987) Chymotrypsin-specific protease inhibitors decrease H,O, formation by activated polymorphonuclear leukocytes. Carcinogenesis 8: 1207-1212.
Gassull MA, Femandez-Banares F & Esteve-Comos M (1995) Nutrition in inflammatory bowel disease. In Payne-James J et al (eds) Artificial Nutrition Support in Clinicul Practice, pp 443- 458. London: Edward Arnold.
*Gassull MA, Femandez-Banares F, Cabre E et al (1996) Enteral nutrition in inflammatory bowel disease. In Rombeau JL & Rolandelli RH (eds) Clinical Nutrition: Enteral and Tube Feeding, 3rd edn, pp 403-416. Philadelphia: W.B. Saunders.
Gibson CR, Cummings JH & McFarlane CT (1991) Growth and activities of sulphate-reducing bacteria in gut contents of healthy subjects and patients with ulcerative colitis. FEMS Microbiology Ecology 86: 103- 112.
Gonzalez-Huix F, Fernandez-Banares F, Esteve-Comas M et al (1993) Enteral vs parenteral nutrition as adjunct therapy in acute ulcerative colitis. American Journal of Gastroenterology 88: 227-232.
Greenfield SM. Green AT, Teare JP et al (I 993) A randomized controlled study of evening primrose oil and fish oil in ulcerative colitis. Alimentury Pharmacology and Therapeutics 7: 159-166.
Grimminger F, Fuehrer D, Papavnssilis C et al (1993) Influence of intravenous n-3 lipid supple- mentation on fatty acid profiles and lipid mediator generation in a patient with severe ulcerative colitis. Europearr Journal of Clinical Investigution 23: 706-7 15.

172 A. BURKE ET AL
Grisham MB (1994) Oxidants and free radicals in inflammatory bowel disease. Lancer 344: 859-861. *Grisham MB & Granger ND (1988) Neutrophil-mediated mucosal injury. Role of reactive oxygen
species. Digestive Diseases and Sciences 33: 6S-15s. Grisham MB, DeMichele SJ, Garleb KA et al (1996) Sulfasalazine or enteral diets containing fish
oil or oligosaccharides attenuate chronic colitis in rats. Injlammafory Bowel Diseases 2: 178-188.
Guillemot F, Colombel JF, Neut C et al (1991) Treatment of diversion colitis by short-chain fatty acids. Prospective and double-blind study. Diseases of rhe Colon and Rectum 34: 861-864.
Guthy E (1986) Use of alpha-tocopherylquinone in ulcerative colitis. Gut 27: 1400. Gutteridge JMC (1995) Lipid peroxidation and antioxidants as biomarkers of tissue damage. Clinicul
Chemisrry 41: 1819-1828. Hague A, Manning AM, Hanlon KA et al (1993) Sodium butyrate induces apoptosis in human colonic
tumor cell lines in a p53 independent pathway: implication for the possible role of dietary fiber in the prevention of large bowel cancer. International Journal of Cancer 5.5: 498-505.
Hallert C, Kaldma M & Petersson BG (199 1) Ispaghula husk may relieve gastrointestinal symptoms in ulcerative colitis in remission. Scandinavian Journal of Castroenterology 26: 747-750.
Hanauer SB, Evans AA, Newcomb SA et al (1984) Can response of ulcerative colitis to total parenteral nutrition (TPN) be predicted? Gastroenterology 86: 1106 (abstract).
Harford FJ & Fazio VW (1978) Total parenteral nutrition as primary therapy for inflammatory disease of the bowel. Diseases of the Colon and Rectum 21: 555-557.
Harig JM & Soergel KH (1987) Treatment of diversion colitis with short-chain fatty acid irrigation. Gasfroenterology 92: 1425(abstract).
Harig JM, Soergel KH, Komorowski RA et al (1989) Treatment of diversion colitis with short-chain fatty acid irrigation. New England Journal of Medicine 320: 23-28.
Hawthorne AB, Daneshmend TK, Hawkey CJ et al (1992) Treatment of ulcerative colitis with fish oil supplementation: a prospective 12 month randomised controlled trial. Gut 33: 922-928.
Hermanowicz A, Sliwinski Z, Kaczor Ret al (1985) Effect of long-term therapy with sulphasalazine, levamisole, cotticosteroids and ascorbic acid and of disease activity on polymorphonuclear leukocyte function in patients with ulcerative colitis. Hepatology-Gastroenterology 32: 8 1-86.
Jeejeebhoy KN, Detsky AS & Baker JP (1990) Assessment of nutritional status. Journal of Parenteral and Enteral h’utrition 14: l93S-196s.
Kappus H (1985) Lipid peroxidation: mechanisms, analysis, enzymology and biological relevance. In Sies H (ed.) Oxidutive Stress, pp 273-3 10. London: Academic Press.
Kehrer JP & Lund LG (1994) Cellular reducing equivalents and oxidative stress. Free Radical Biology and Medicine 17: 65-77.
Kim YS, Tsao D, Marita T et al (1982) In Malt RA & Williamson RCN (eds) Colonic Carcinogenesis, pp 3 17-323. Lancaster: MTP.
Klein S, Meyers S, O’Sullivan Pet al (1988) The metabolic impact of active ulcerative colitis: energy expenditure and nitrogen balance. Journal of Clinical Gastroenterology 10: 34-40.
Komorowski RA (1990) Histologic spectrum of diversion colitis. American Journal of Surgical Pathology 14: 548-554.
Kruh J, Defer N & Tichonicky L (1991) Molecular and cellular effects of sodium butyrate. In Roche AF (ed.) Short-Chain Fatty Acids: Metabolism and Clinical Importance, Report of the Tenth Ross Conference on Medical Reseurch, pp 45-50. Columbus, Ohio: Ross Laboratories.
Lashner BA, Heidenreich PA, Su GL et al (1989) Effect of folate supplementation on the incidence of dysplasia and cancer in chronic ulcerative colitis. A case-controlled study. Gastroenterology 97: 255-259.
Lashner BA, Provencher KS, Seidner DL et al (1997) The effect of folic acid supplementation on the risk for cancer of dysplasia in ulcerative colitis. Gastroenterology 112: 29-32.
Lauritsen K, Laursen LS, Bukhave K et al (1986) Effects of topical 5-aminosalicylic acid and prednisolone on prostaglandin Ei and leukottiene B, levels determined by equilibrium in vivo dialysis of rectum in relapsing ulcerative colitis. Gastroenterology 91: 837-844.
Lee TH, Hoover RL, Williams JD et al (I 985) Effect of dietary enrichment with eicosapentaenoic and docosahexanoic acids of in vitro neutrophil and monocyte leukotriene generation and neutrophil function. Nerr England Journal of Medicine 312: 1217-1224.
Leventhal LJ, Boyce EG & Zurier RB (1994) Treatment of rheumatoid arthritis with blackcurrant seed oil. British Journal of Rheumatology 33: 847-852.
Lloyd ML & Olsen WA (1995) Disorders of epithelial transport in the small intestine. In Yamada T et al (eds) Textbook of Gastroenterology, 2nd edn, pp 1661-1672. Philadelphia: J.B. Lippincott Co.

NUTRITION AND ULCERATIVE COLITIS 173
Lobos EA. Sharon P & Stenson WF (1987) Chemotactic activity in inflammatory bowel disease. Digestive Diseases and Sciences 32: 1380-1388.
McCall TB, O’Leary D, Bloomfield J et al (1989) Therapeutic potential of fish oil in the treatment of ulcerative colitis. Alimentary Pharmacology and Therapeutics 3: 415-424.
McIntyre PB, Powell-Tuck J, Wood SR et al (1986) Controlled trial of bowel rest in the treatment of severe acute colitis. Gut 27: 481-485.
MarottaF. ChuiDH. Safran Pet al (1995) Shark fin enriched diet prevents mucosal lipid abnormalities in experimental acute colitis. Digestion 56: 46-5 1.
Mattioli S, Miglioli M, Montagna P et al (1988) Wemicke’s encephalopathy during total parenteral nutrition: observation in one case. Journal of Parenteral and Enteral Nutrition 12: 626-627.
Mulder TPJ, Verspaaget HW, Janssens AR et al (1991) Decreases in two intestinal Cu/Zn containing proteins with antioxidant function in inflammatory bowel disease. Gut 32: 1146-l 150.
Mulder TPJ, van der Sluys Veer A, Verspaget HW et al (1994) Effect of oral zinc supplementation on metallothionein and superoxide dismutase concentrations in patients with inflammatory bowel disease. Journal of Gastroenterology and Hepatology 9: 472-477.
Mullen JL, Clark Hargrove W, Dudrick SJ et al (1978) Ten years experience with intravenous hyper- ahmentation and inflammatory bowel disease. Annuls of Surgery 187: 523-529.
Nelson RA (1968) Intestinal transport, coenzyme-A and colitis in pathothenic acid deficiency. American Journal of Clinical Nutrition 21: 495-501.
Nesbitt LT (1995) Minimizing complications from systemic glucocorticosteroid use. Dermafologic Clinics 13: 925-939.
Phinney S (1994) Potential risk of prolonged gamma linolenic acid use (letter). Annuls of Internal Medicine 120: 692.
Poret HA & Kudsk KA (1990) In Rombean JL (ed.) Clinicnl Nutrition: Parenteral Nutrition, pp 409-426. Philadelphia: W.B. Saunders.
Powell-Tuck J (1986) Protein metabolism in inflammatory bowel disease. Gut 27: 67-71. Rao SSC, Holdsworth CD & Forrest ARW (1987) Small intestinal absorption and tolerance of enteral
nutrition in acute colitis. British Medical Journal 295: 698. Reid IR & Ibbertson HK (1986) Calcium supplements in the prevention of steroid-induced osteo-
porosis American Journul of Clinical Nutrition 44: 287-290. Reilly J, Ryan JA, Strole W et al (1976) Hyperalimentation in inflammatory bowel disease. American
Journal of Surgery 131: 192-200. Ringstad J, Kildubo S & Thomassen Y (1993) Serum selenium, copper and zinc concentrations in
Crohn’s disease and ulcerative colitis. Scandinavian Journal of Gastroenferology 28: 605-608. * Roediger WEW (1980a) The colonic epithelium in ulcerative colitis; an energy deficient disease?
Lancer ii: 712-715. Roediger WEW (1980b) Role of anaerobic bacteria in the metabolic welfare of the colonic mucosa in
man. Gut 21: 793-798. Roediger WEW (1990) The starved colon--diminished mucosal nutrition, diminished absorption and
colitis. Diseases of the Colon and Rectum 33: 858-862. Roediger WEW (1991) Cellular metabolism of short-chain fatty acids in colonic epithelial cells. In
Roche AF (ed.) Short-Chain Fatty Acids: Metabolism and Clinical Importance, Report of the Tenth Ross Conference on Medical Research, pp 67-7 1. Columbus, Ohio: Ross Laboratories.
Roediger WEW (1992) Oxidative and synthetic functions of n-butyrate in colonocytes (letter). Diseases of the Colon and Rectum 35: 5 II-5 12.
Roediger WEW & Nance S (1990) Selective reduction of fatty acid oxidation in colonocytes: correlation with ulcerative colitis. Lipids 25: 646652.
Roediger WEW, Kapaniris 0 & Millard S (I 992) Lipogenesis from n-butyrate in colonocytes: action of reducing agent and 5-aminosalicylic acid with relevance to ulcerative colitis. Molecular and Cellular Biochemistry 118: 113-I 18.
* Roediger WEW, Duncan A, Kapaniris 0 et al (1993a) Reducing sulfur compounds of the colon impair colonocyte nutrition: implications for ulcerative colitis. Gastroenterology 104: 802-809.
Roediger WEW, Duncan A, Kapaniris 0 et al (1993b) Sulphide impairment of substrate oxidation in rat colonocytes: a biochemical basis for ulcerative colitis? Chnical Science 8.5: 623-627.
Rolandelli RH, Saul SH, Gregg Settle R et al (1988) Comparison of parenteral nutrition and enteral feeding with pectin in experimental colitis in the rat. American Journal ofClinical Nutrition 47: 715-721.
Rolandelli RH & Ulhich JR (1997) Lipids and enteral nutrition. In Rombeau JL & Rolandelli RH (eds) Clinical Nutrition: Enterul and Tube Feeding, 3rd edn, pp 47-60. Philadelphia: W.B. Saunders.

174 A. BURKE ET AL
Rombeau JL & Afonso JJ (1992) Clinical and scientific basis for nutritional support of patients with inflammatory bowel disease. In MacDermott RP & Stenson W (eds) InjIammaro~ Bu& Disease, pp 525-553. New York: Elsevier.
Salim AS (1992) Role of oxygen-derived free radical scavengers in the management of recurrent attacks of ulcerative colitis: a new approach. JOUWIA~ of Laboratory and Clinical Medicine 119: 710-717.
Salomon P, Komblath AA & Janowitz HD (1990) Treatment of ulcerative colitis with fish oil n-3-o- fatty acid: an open trial. Journal of Clinical Gastroenterology 12: 157-161.
Sandler RS (1993) Epidemiology of inflammatory bowel disease. In Targan SR & Shanahan F (eds) In~ammatory Bowel Disease: from Bench to Bedside, pp 5-30. Baltimore: Williams & Wilkins.
Schumert R, Towner J & Zipser RD (1988) Role of eicosanoids in human and experimental colitis. Digestive Diseases and Sciences 33: 58S-64s.
Sedghi S, Keshavarzian A, Klamut M et al (1994) Elevated breath ethane levels in active ulcerative colitis: evidence for excessive lipid peroxidation. American Journal of Gastroenterology 89: 2217-2221.
Seidman EG (1989) Nutritional management of inflammatory bowel disease. Gastroenterology Clinics of North America 17: 129-155.
Soergel KH (1991a) The treatment of diversion colitis and pouchitis. In Roche AF (ed.) Short-Chain Fatty Acids: Metabolism and Clinical Importance, Report of the Tenth Ross Conference on Medical Research, pp 82-85. Columbus, Ohio: Ross Laboratories.
Soergel KH (1991b) The role of short-chain fatty acids in the treatment of colitis. In Goebell H & Malchow EK (eds) Inflnmmatory Bowel Diseases. Progress in Basic Research and Clinical Implications, pp 373-379. Dordrecht, Netherlands: Kluwer Academic Press.
* Stenson WF, Cort D, Rodgers J et al (1992) Dietary supplementation with fish oil in ulcerative colitis. Annals of Internal Medicine 116: 609-614.
Stuart Welch C, Adams M & Wakefield EG (1937) Metabolic studies of chronic ulcerative colitis. Journal of Clinical Investigation 16: 161-168.
Takada R, Saitoh M & Mori T (1994) Dietary gamma-linolenic acid enriched oil reduces body fat content and induces liver enzyme activities relating to fatty acid P-oxidation in rats. Journal qf Nutrition 124: 469-474.
Terano T, Salmon JA & Moncada S et al (1984) Biosynthesis and biologic activity of leukotriene B,. Prostaglandins 27: 2 17-232.
Valberg LS, Flanagan PR, Kertesz A et al (1986) Zinc absorption in inflammatory bowel disease. Digestive Diseases and Sciences 31: 724-73 1.
Velazquez OC, Jabbar A, DeMatteo RP & Rombeau JL (1996a) Butyrate inhibits seeding and growth of colorectal metastases to the liver in mice. Surgery 120: 440-448.
Velazquez OC, Zhou D, Seto RW et al (1996b) In vivo crypt surface hyperproliferation is decreased by butyrate and increased by deoxycholate in normal rat colon: associated in vivo effects of c-fos and c-jun expression. Journal of Parenteral and Enteral Nutrition 20: 243-250.
Weiseger RA, Pinkus LM & Jakoby WB (1990) Thiol S-methyltransferase: suggested role in detoxication of intestinal hydrogen sulfide. Biochemical Pharmacology 29: 2885-2887.
Wintrobe MM, Follis RH, Alcayaga R et aI (1943) Pantothenic acid deficiency in swine, with particular reference to the dietary effects of growth and on the alimentary tract. Bulletin of Johns Hopkins Hospital 73: 3 13-340.
Yamada T & Grisham MB (1993) Pathogenesis of tissue injury: role of reactive metabolites of oxygen and nitrogen. In Targan SR & Shanahan F (eds) Injammatory Bowel Disease: from Bench to Bedside, pp 133-l SO. Baltimore: Williams & Wilkins.
Young GP (1991) Butyrate and the molecular biology of the large bowel. In Roche AF (ed.) Short- Chain Fatty Acids: Metabolism and Clinical Importance, Report of the Tenth Ross Conference on Medical Research, pp 39-45. Columbus, Ohio: Ross Laboratories.