Embed Size (px)
Citation preview

1
Understanding and Managing Addiction as a Chronic Condition
Michael L. Dennis, Ph.D. Chestnut Health Systems
Normal, IL
Presentation at the Pacific Asia Judges Science and Technology Seminar,
November 10-12, 2010, Hyatt Regency Hotel, Tumon, Guam. This presentation was supported by funds from and data from NIDA grants no. R01 DA15523, R37-DA11323, R01 DA021174, and CSAT contract no. 270-07-0191. It is available electronically at www.chestnut.org/li/posters . The
opinions are those of the author do not reflect official positions of the government. Please address comments or questions to the author at Chestnut
Health Systems, 448 Wylie Drive, Normal, IL 61761 [email protected] or 309-451-7801.

2
The Goals of this Presentation are to:
1. Illustrate the chronic nature of substance use disorders
2. Examine the likelihood and nature of sustained recovery
3. Demonstrate the feasibility of using simple protocols like recovery checkups to improve long-term outcomes

3
1-2 M in 3-4 5-6
6-7 7-8 8-9
9-10 10-20 20-30
1-2 M in 3-4 5-6
6-7 7-8 8-9
9-10 10-20 20-30
Brain Activity on PET Scan After Brain Activity on PET Scan After Using CocaineUsing Cocaine
Photo courtesy of Nora Volkow, Ph.D. Mapping cocaine binding sites in human and baboon brain in vivo. Fowler JS, Volkow ND, Wolf AP, Dewey SL, Schlyer DJ, Macgregor RIR, Hitzemann R, Logan J, Bendreim B, Gatley ST. et al. Synapse 1989;4(4):371-377.
Rapid rise in brain activity after taking
cocaine
Actually ends up lower than they
started

4
Normal
10 days of abstinence
100 days of abstinence
Source: Volkow ND, Hitzemann R, Wang C-I, Fowler IS, Wolf AP, Dewey SL. Long-term frontal brain metabolic changes in cocaine abusers. Synapse 11:184-190, 1992; Volkow ND, Fowler JS, Wang G-J, Hitzemann R, Logan J, Schlyer D, Dewey 5, Wolf AP. Decreased dopamine D2 receptor availability is associated with reduced frontal metabolism in cocaine abusers. Synapse 14:169-177, 1993.
Prolonged Substance Use Injures The Brain:Prolonged Substance Use Injures The Brain:Healing Takes Time Healing Takes Time
Normal levels of brain activity in PET
scans show up in yellow to red
After 100 days of abstinence, we can
see brain activity “starting” to recover
Reduced brain activity after regular
use can be seen even after 10 days
of abstinence

5
Photo courtesy of the NIDA Web site. From A Slide Teaching Packet: The Brain and the Actions of Cocaine, Opiates, and Marijuana.
pain
Adolescent Brain Development Occurs from the
Inside to Out and from Back to Front

6
Alcohol and Other Drug Abuse, Dependence and Problem Use Peaks at Age 20
Source: 2002 NSDUH and Dennis & Scott, 2007, Neumark et al., 2000
0
10
20
30
40
50
60
70
80
90
100
12-13
14-15
16-17
18-20
21-29
30-34
35-49
50-64
65+Other drug or heavy alcohol use in the past year
Alcohol or Drug Use (AOD) Abuse or Dependence in the past year
Age
Severity Category
Over 90% of use and
problems start between the ages of
12-20
It takes decades before most recover or die
Per
cent
age
People with drug dependence die an
average of 22.5 years sooner than those
without a diagnosis

7
Yet Recovery is likely and better than averagecompared with other Mental Health Diagnoses
Source: Dennis, Coleman, Scott & Funk forthcoming; National Co morbidity Study Replication
15% 13%8%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%A
ny A
OD
Alc
ohol
Dru
g
Any
Ext
erna
lizi
ng
Con
duct
Opp
osit
iona
lD
efia
nt
Inte
rmit
tent
Exp
losi
ve
Att
enti
on D
efic
it
Any
Int
erna
lizi
ng
Anx
iety
:
Moo
d :
Pos
ttra
umat
icS
tres
s
Lifetime Diagnosis
10% 10% 7%
Past Year Recovery (no past year symptoms)
66%
77%
83%
Recovery Rate (% Recovery / % Dependent)
25%
10% 10% 8% 8%
46%
31%
7%
20%
15% 8% 9%4%
18%12% 11%
3%4%
58%
89% 89%
45%50%
39%
56%48%40%
SUD Remission Rates are BETTER than many other DSM Diagnoses
Median of 8 to 9 years in recovery

8
People Entering Publicly Funded Treatment Generally Use For Decades
Per
cen
t st
ill u
sin
g
Years from first use to 1+ years of abstinence302520151050
Source: Dennis et al., 2005
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
It takes 27 years before half reach 1 or more years of abstinence or die

9
Per
cen
t st
ill u
sin
g
Years from first use to 1+ years of abstinence
under 15*
21+
15-20
Age of First Use
302520151050
Source: Dennis et al., 2005
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
60% longer
The Younger They Start, The Longer They Use
* p<.05

10
Per
cen
t st
ill u
sin
g
Years from first use to 1+ years of abstinence
Years to first
Treatment Admission*
302520151050
Source: Dennis et al., 2005
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
20 or more years
0 to 9 years
10 to 19 years
57% quicker
The Sooner They Get To Treatment, The Quicker They Get To Abstinence
* p<.05

11
After Initial Treatment…
• Relapse is common, particularly for those who: – Are Younger– Have already been to treatment multiple times – Have more mental health issues or pain
• It takes an average of 3 to 4 treatment admissions over 9 years before half reach a year of abstinence
• Yet over 2/3rds do eventually abstain• Treatment predicts who starts abstinence• Self help engagement predicts who stays abstinent
Source: Dennis et al., 2005, Scott et al 2005

12* p<.05
The Likelihood of Sustaining Abstinence Another Year Grows Over Time
36%
66%
86%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1 to 12 months 1 to 3 years 4 to 7 years
Duration of Abstinence*
% S
usta
inin
g A
bsti
nenc
eA
noth
er Y
ear
.
After 1 to 3 years of abstinence, 2/3rds will make it another year
After 4 years of abstinence, about 86% will make it
another year
Source: Dennis, Foss & Scott (2007)
Only a third of people with
1 to 12 months of abstinence will
sustain it another year
But even after 7 years of abstinence, about
14% relapse each year

13
Source: Dennis, Foss & Scott (2007)
What does recovery look like on average?
Duration of Abstinence1-12 Months 1-3 Years 4-7 Years
• More social and spiritual support• Better mental health • Housing and living situations continue to improve • Dramatic rise in employment and income • Dramatic drop in people living below the poverty line
• Virtual elimination of illegal activity and illegal income • Better housing and living situations • Increasing employment and income
• More clean and sober friends• Less illegal activity and incarceration • Less homelessness, violence and victimization • Less use by others at home, work, and by social peers

14
Sustained Abstinence Also ReducesThe Risk of Death*
Source: Scott, Dennis, Laudet, Funk & Simeone (in press)
-
Users/Early Abstainers more likely
to die in the next 12
months
The Risk of Death goes down with
years of sustained abstinence
It takes 4 or more years of abstinence for
risk to get down to
community levels
(Matched on Gender, Race & Age)
Dea
ths
in t
he
nex
t 12
mon
ths
* p<.05

15
Other factors related to death rates
• Death is more likely for those who – Are older– Are engaged in illegal activity– Have chronic health conditions– Spend a lot of time in and out of hospitals– Spend a lot of time in and out of substance abuse
treatment
• Death is less common for those who – Have a greater percent of time abstinent– Have longer periods of continuous abstinence– Get back to treatment sooner after relapse
Source: Scott, Dennis, Laudet, Funk & Simeone (in press)

16
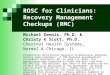
The Cyclical Course of Relapse, Incarceration, Treatment and Recovery (Pathway Adults)
In the Community
Using (53% stable)
In Treatment (21% stable)
In Recovery (58% stable)
Incarcerated(37% stable)
6%
28%
13%
30%
8%
25%
31%
4%
44%7%
29%
7%
Treatment is the most likely path
to recovery
P not the same in both directions
Over half change status annually
Source: Scott, Dennis, & Foss (2005)

17
Source: Scott, Dennis, & Foss (2005)
Predictors of Change Also Vary by Direction
In the Community
Using (53% stable)
In Recovery (58% stable)
28%
29%
Probability of Sustaining Abstinence - times in treatment (0.83) + Female (1.72)- homelessness (0.61) + ASI legal composite (1.19)- number of arrests (0.89) + # of sober friend (1.22)
+ per 77 self help sessions (1.82)
Probability of Transitioning from Using to Abstinence - mental distress (0.88) + older at first use (1.12) -ASI legal composite (0.84) + homelessness (1.27)
+ # of sober friend (1.23)+ per 8 weeks in treatment (1.14)

18
Source: French et al., 2008; Chandler et al., 2009; Capriccioso, 2004
Cost of Substance Abuse Treatment Episode
$407
$1,249$1,132$1,384$2,486$2,907
$4,277$14,818
$0
$1
0,0
00
$2
0,0
00
$3
0,0
00
$4
0,0
00
$5
0,0
00
$6
0,0
00
$7
0,0
00
Screening & Brief Inter.(1-2 days)In-prison Therap. Com. (28 weeks)
Outpatient (18 weeks)
Intensive Outpatient (12 weeks)Treatment Drug Court (46 weeks)
Residential (13 weeks)Methadone Maintenance (87 weeks)Therapeutic Community (33 weeks)
$22,000 / year to incarcerate
an adult
$30,000/ child-year in foster care
$70,000/year to keep a child in
detention
• $750 per night in Detox• $1,115 per night in hospital • $13,000 per week in intensive care for premature baby• $27,000 per robbery• $67,000 per assault

19
Investing in Treatment has a Positive Annual Return on Investment (ROI)2
• Substance abuse treatment has been shown to have a ROI of between $1.28 to $7.26 per dollar invested
• Even the long term and more intensive Treatment Drug Courts programs have an average ROI of $2.14 to $2.71 per dollar invested
Source: Bhati et al., (2008); Ettner et al., (2006)
This also means that for every dollar treatment is cut, we lose more money than we saved.

20
Early Re-Intervention (ERI) Experiment and Hypotheses
Source: Dennis et al 2003, 2007; Scott et al 2005, in press
Monitoring and
Early Re-Intervention
Reduce Time to Re-admission
Relative to Control, RMC will reduce the time from relapse to readmission
Less Successive Quarters
Using
The quicker the return to treatment, the less successive quarters using in the community
Less Risk Behaviors, MH and Crime
The less quarters using in the community, the less HIV Risk Behaviors, Mental Health and Crime Problems

21
Recovery Management Checkups (RMC)
• Quarterly monitoring after treatment• Linkage meeting/motivational interviewing to:
– provide personalized feedback to participants about their substance use and related problems,
– help the participant recognize the problem and consider returning to treatment,
– address existing barriers to treatment, and – schedule an assessment.
• Linkage assistance– reminder calls and rescheduling– Transportation and being escorted as needed
• Treatment Engagement Specialist

22
ERI-2 Time to Treatment Re-Entry at Year 4
Percent Readmitted 1+ Times
Wilcoxon-Gehen statistic (df=1) = 28.60, p<.001
OR=3.1, p<.05
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45
Months from 1st Follow-up In Need for Treatment,
Time from relapse to readmission reduce by
78% (45-13 = -32 months; d=-.41)
74% ERI-2 RMC* (n=198)
48% ERI-2 OM (n=195)
RMC increases the odds of re-entering treatment over 4 years by 3.1
Source: Scott & Dennis (2009); Dennis & Scott (under review)
The size of the effect grew every quarter

23
Positive Consequences of Early Readmission
• Checkups and Early Readmission to Treatment were associated with: – Less substance use and problems– Longer periods of abstinence– More attendance and engagement in self help
activities• Above were associated with:
– Fewer HIV risk behaviours– Less illegal activity, arrests, and time
incarcerated– Fewer mental health problems– Less utilization and costs to society
Source: Scott & Dennis (2009); Dennis & Scott (under review)

24
In the Community
Using (71% stable)
In Treatment (35% stable)
In Recovery (76% stable)
Incarcerated(60% stable)
3%
18%
8%
15%
9%
16%
27%
4%
33%5%
17%
2%
32% Changed Status in an
Average Quarter
Again the Probability of
Entering Recovery is Higher from
Treatment
Source: Scott et al 2005, Dennis & Scott, 2007
ERI 1: Impact on Primary Quarterly Pathways to Recovery over 2 years

25
In the Community
Using (71% stable)
Transition to Tx vs.
Continued Use- Freq. of Use (0.7)+ Prob. Orient. (1.4)+ Desire for Help (1.6)+ RMC (3.22)
8%
In Treatment(35% stable)
18%
Transition to Recovery vs Continued Use - Freq. of Use (0.7) + Prob. Orient. (1.3)
- Dep/Abs Prob (0.7) + Self Efficacy (1.2) - Recovery Env. (0.8) + Self Help Hist (1.2)
- Access Barriers (0.8) + per 10 wks Tx (1.2)
In Recovery(76% stable)
Source: Scott et al 2005, Dennis & Scott, 2007
ERI 1: Impact on Primary Quarterly Pathways to Recovery over 2 years

26
Adolescents: Also Have Complex Pathways to Recovery
In the Community
Using (60% stable)
In Treatment (45% stable)
In Recovery (61% stable)
Incarcerated(41% stable)
Source: 2009 CSAT AT data set; unique n = 11,710
Avg of 48% change status each quarter
18%
16%
22%17%
27%
14%
17%
24%
21%9 %
4%4%
Treatment is the most likely path
to recovery
What predicts who enters and maintains recovery?

27
Risk and Protective Factors Associated with Transitioning to/Remaining in Recovery
• Risk Factors– Older – Male– Caucasian– Substance Problems
Substance Frequency– Repeated Treatment– Emotional Problems– Illegal Activity– Employment
• Protective Factors– Younger– Female– Racial Minority – Recent Treatment – Number of drug screens– Attend 12 Step Meetings– Positive Social Peers– Positive Recovery
Environment– School Attendance/
ConductSource: 2009 CSAT AT data set; unique n = 11,710

28
Cumulative Recovery Pattern 30 Months After Intake
Source: Godley et al 2004
37% Sustained Problems
5% Sustained Recovery
19% Intermittent, currently in
recovery
39% Intermittent, currently not in
recovery
The Majority of Adolescents Cycle in and out of Recovery
(n=600 adolescents)

29
Recovery* by Level of Care
* Recovery defined as no past month use, abuse, or dependence symptoms while living in the community. Percentages in parentheses are the treatment outcome (intake to 12 month change) and the stability of the outcomes (3months to 12 month change) Source: CSAT Adolescent Treatment Outcome Data Set (n-9,276)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pre-Intake Mon 1-3 Mon 4-6 Mon 7-9 Mon 10-12
Per
cent
in P
ast
Mon
th R
ecov
ery* Outpatient (+79%, -1%)
Residential(+143%, +17%)
Post Corr/Res (+220%, +18%)
OP & Resid
Similar
CC better

30
Time to Enter Continuing Care and Relapse after Residential Treatment (Age 12-17)
Source: Godley et al., 2004 for relapse and 2000 Statewide Illinois DARTS data for CC admissions
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 10 20 30 40 50 60 70 80 90
Days after Residential (capped at 90)
Per
cen
t of
Clie
nts
Cont.CareAdmis.
Relapse

31
Source: Godley et al 2002, 2007
Assertive Continuing Care (ACC) Experiment (n=183) and Hypotheses
Assertive Continuin
g Care
General Continuin
g Care Adherence
Relative to UCC, ACC will increase General Continuing Care Adherence (GCCA)
Early Abstinence
GCCA (whether due to UCC or ACC) will be associated with higher rates of early abstinence
Sustained Abstinence
Early abstinence will be associated with higher rates of long term abstinence.

32
Assertive Continuing Care (ACC) Enhancements
• Continue to participate in UCC • Home Visits• Sessions for adolescent, parents, and together• Sessions based on Adolescent Community
Reinforcement Approach (A-CRA) manual (Godley, Meyers et al., 2001)
• Case Management based on ACC manual (Godley et al, 2001) to assist with other issues (e.g., job finding, medication evaluation)
Source: Godley et al 2002, 2007

33
General Continuing Care Adherence (GCCA)
Source: Godley et al 2002, 2007
0% 10%
20%
30%
40%
50%
60%
70%
80%
Weekly Tx Weekly 12 step meetings
Regular urine tests
Contact w/probation/school
Follow up on referrals*
ACC * p<.05
90%
100%
Relapse prevention*
Communication skills training*
Problem solving component*
Meet with parents 1-2x month*
Weekly telephone contact*
Referrals to other services*
Discuss probation/school compliance*
Adherence: Meets 7/12 criteria*
UCC

34
Adherence Improved Early (0-3 mon.) Abstinence
Source: Godley et al 2002, 2007
24%
36% 38%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Any AOD (OR=2.16*) Alcohol (OR=1.94*) Marijuana (OR=1.98*)
Low (0-6/12) GCCA
43%
55% 55%
High (7-12/12) GCCA * p<.05

35
Opportunities to Better Support Recovery
Evidenced Based Recovery Services forAdolescents (1-2 Clinical Trials)• Telephone Counseling • Assertive Continuing Care • Contingency Managements • Recovery Coaches or Mentors
Other Promising Recovery Services• Alcohol/Drug Test Monitoring• Self Help Participation• Community Reinforcement Approach Family Training (CRAFT)• Recovery School • Recovery oriented support via technology (ie text, email, social
networking, skype)

36
Summary Points
• Addiction can be a chronic condition with high costs to the individual and society
• Getting people to sustained recovery earlier requires getting people to treatment sooner after initial use and after relapse
• Simple protocols like recovery checkups can help achieve abstinence sooner and improve a wide range of outcomes

37
References• Bhati et al. (2008) To Treat or Not To Treat: Evidence on the Prospects of Expanding Treatment to Drug-Involved Offenders. Washington, DC: Urban Institute.• Capriccioso, R. (2004). Foster care: No cure for mental illness. Connect for Kids. Accessed on 6/3/09 from http://www.connectforkids.org/node/571• Chandler, R.K., Fletcher, B.W., Volkow, N.D. (2009). Treating drug abuse and addiction in the criminal justice system: Improving public health and safety. Journal American Medical
Association, 301(2), 183-190• Dennis, M.L., Coleman, V., Scott, C.K & Funk, R (forthcoming). The Prevalence of Remission from Major Mental Health Disorder in the US: Findings from the National Co morbidity
Study Replication.• Dennis, M.L., Foss, M.A., & Scott, C.K (2007). An eight-year perspective on the relationship between the duration of abstinence and other aspects of recovery. Evaluation Review, 31(6),
585-612• Dennis, M. L., Scott, C. K. (2007). Managing Addiction as a Chronic Condition. Addiction Science & Clinical Practice , 4(1), 45-55.• Dennis, M. L., Scott, C. K., Funk, R., & Foss, M. A. (2005). The duration and correlates of addiction and treatment careers. Journal of Substance Abuse Treatment, 28, S51-S62.• Dennis, M. L., Scott, C. K., & Funk, R. (2003). An experimental evaluation of recovery management checkups (RMC) for people with chronic substance use disorders. Evaluation and
Program Planning, 26(3), 339-352.• Ettner, S.L., Huang, D., Evans, E., Ash, D.R., Hardy, M., Jourabchi, M., & Hser, Y.I. (2006). Benefit Cost in the California Treatment Outcome Project: Does Substance Abuse Treatment
Pay for Itself?. Health Services Research, 41(1), 192-213. • French, M.T., Popovici, I., & Tapsell, L. (2008). The economic costs of substance abuse treatment: Updated estimates of cost bands for program assessment and reimbursement. Journal of
Substance Abuse Treatment, 35, 462-469• Neumark, Y.D., Van Etten, M.L., & Anthony, J.C. (2000). Drug dependence and death: Survival analysis of the Baltimore ECA sample from 1981 to 1995. Substance Use and Misuse, 35,
313-327.• Office of Applied Studies (2006). Results from the 2005 National Survey on Drug Use and Health: National Findings Rockville, MD: Substance Abuse and Mental Health Services
Administration. http://www.oas.samhsa.gov/NSDUH/2k5NSDUH/2k5results.htm#7.3.1 • Riley, B.B.,, Scott, C.K, & Dennis, M.L. (2008). The effect of recovery management checkups on transitions from substance use to substance abuse treatment and from treatment to
recovery. Poster presented at the UCLA Center for Advancing Longitudinal Drug Abuse Research Annual Conference, August 13-15, 2008, Los Angles, CA. www.caldar.org .• Rush, B., Dennis, M.L., Scott, C.K, Castel, S., & Funk, R.R. (2008). The Interaction of Co-Occurring Mental Disorders and Recovery Management Checkups on Treatment Participation and
Recovery. • Scott, C. K., & Dennis, M. L. (2009). Results from Two Randomized Clinical Trials evaluating the impact of Quarterly Recovery Management Checkups with Adult Chronic Substance
Users. Addiction.• Scott, C. K., Dennis, M. L., & Foss, M. A. (2005). Utilizing recovery management checkups to shorten the cycle of relapse, treatment re-entry, and recovery. Drug and Alcohol Dependence,
78, 325-338.• Scott, C. K., Dennis, M. L., & Funk, R.R. (2008). Predicting the relative risk of death over 9 years based on treatment completion and duration of abstinence . Poster 119 at the College of
Problems on Drug Dependence (CPDD) Annual Meeting, San Juan, PR, June 16, 2008. Available at www.chestnut.org/li/posters .• Scott, C. K., Foss, M. A., & Dennis, M. L. (2005). Pathways in the relapse, treatment, and recovery cycle over three years. Journal of Substance Abuse Treatment, 28, S61-S70.• Volkow ND, Fowler JS, Wang G-J, Hitzemann R, Logan J, Schlyer D, Dewey 5, Wolf AP. (1993). Decreased dopamine D2 receptor availability is associated with reduced frontal
metabolism in cocaine abusers. Synapse 14:169-177.• Volkow, ND, Hitzemann R, Wang C-I, Fowler IS, Wolf AP, Dewey SL. (1992). Long-term frontal brain metabolic changes in cocaine abusers. Synapse 11:184-190.