Embed Size (px)
Citation preview

1
Trends in the Disability Market
Chris JeromeVice President, Group Underwriting Operations
March 21, 2006

2
Trends in Disability Market
• Disability Costs
• Cyclical and Non-Cyclical Cost Drivers
• Workforce Implications of Non-Cyclical Factors
• Implications for Our Market
• Key Questions to Consider

3
Overview of the Current Disability Industry
Many external factors have been working against the health of the disability industry…
DisabilityAging
Interest Rates
Economic Factors
Other Risk Factors
All providers impacted by above trends…..

4
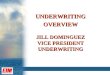
• Between 1990 and 2000, the median age of the US “working age” population increased from 40 to 42 and it will continue to rise
Changes in Risk Dynamic - Aging
Source: US Census Bureau. Statistical Abstract of the US: 2006, Section I, Table 12
Distribution of "Working Age" US Population
0%
20%
40%
60%
80%
100%
1980 1990 2000 2005 2010
25-34
35-44
45-54
55-64
• The largest proportional increase came from the 45-54 age bracket, as the “baby boomers” continue aging

5
Changes in Risk Dynamic
Source: UnumProvident Rate Basis
Mo
nth
ly L
TD
cla
im
cost
/in
sure
d l
ife
32 35 38 41 44 47 50 53 56age
Monthly LTD claim cost per age
• The population and workforce are aging
• Impact of aging along the disability curve can be steep – cost increases of 4 – 8% per age year are common.
Source: UnumProvident LTD Block
• UnumProvident block and new sales have been aging by 4-6 months each year

6
Interest Rates
• Declining rates impact new money invested, and therefore Net Investment Income as well as reserves
Source: Federal Reserve Board: H15
• Interest has a direct and significant impact on cost (100bp shift requires approximately 4% shift in rates)
• Interest rates affect all players and all sizes and segments of cases
Yield on 10 Year Constant Maturity Treasuries
3.03.54.04.55.05.56.06.57.0
Dec-99
Jun-00
Dec-00
Jun-01
Dec-01
Jun-02
Dec-02
Jun-03
Dec-03
Jun-04
Dec-04
Jun-05
Dec-05

7
Disability Incidence and Economic Recessions
• Submitted incidence increased more steeply, initially, in the most recent recession. Now 4 years later, it continues to exhibit a similar pattern as observed in 1990-91 recession.
• Submitted incidence continued to climb long after the recessions officially ended. In 1990–1991 recession, ending in March 1991, incidence reached its peak 19 quarters later.
Source: UnumProvident LTD Block Qtr End of Recession
The horizontal axis above is quarters since the recession
with 0 being the end of the
recession.
Submitted IncidenceDuring Last Two US Recessions
(indexed to the end of each recession)
0.8
0.9
1.0
1.1
1.2
-8 -6 -4 -2 0 2 4 6 8 10 12 14 16 18 20 22 24
1990-91 2001

8
Other Risk Factor Trends
0
5
10
15
20
25
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001
OBESITY - Nationwide % overweight, measured by BMI
• Prevalence of obesity has increased over the last several years
• Over past decade there has been a tenfold increase in the incidence of STD claims attributed to obesity
• Growing body of scientific evidence demonstrating significant associations between obesity and other chronic diseases (e.g. diabetes, stroke, hypertension, etc.)

9
Change in Disability Deaths
While aging is currently a secular trend impacting disability costs for US private insurers, due to the demographic profile of US employees, other secular costs such as disability death rates also affect disability cost.
The actual rates of disability death in recent years have been relatively stable;however, in the early 1990’s the disability death rates were declining.
Source: UnumProvident LTD Block
Disabled death rates by year
-
1
2
3
4
5
6
7
8
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
pe
r 1
,00
0 E
xp
os
ed

10
Disability Costs Summary
• Costs Are rising
– Interest rates
– Economy
– Obesity
– Aging
– Even mortality
• Which are cyclical?
• What are workforce implications of non-cyclical?
All contributing to higher disability costs

11
Work Force Dynamics

Source: Employment Policy Foundation analysis and projections of Census/BLS and BEA data.
Millions of People
Expected Labor Force and Labor Force Demand Palpable by the End of This Decade
0
50
100
150
200
250
2002
2004
2006
2008
2010
2012
2014
2016
2018
2020
2022
2024
2026
2028
2030
Labor Needed
Labor Available
A Growing Shortage of Workers in the US:
12

13
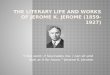
Age of Workers
Percent Growth in U.S. Population by Age: 2000-2010
Dramatically Different Patterns of Growth by Age
1. Declining number of mid-career workers
2. Few younger workers entering the work force
3. Rapid growth in the over-55 workforce
Source: US Census Bureau International Data Base
5% 5%
-9%
18%
48%
15%
-20%
0%
20%
40%
60%
80%
16-24 25-34 35-44 45-54 55-64 65+

14
. . . Continuing for Our Working Lives!
Age of Workers
Percent Growth in U.S. Workforce by Age: 2000-2020
7% 8% 7%
-10%
3%
73%
54%
-20%
0%
20%
40%
60%
80%
under 14 15-24 25-34 35-44 45-55 55-64 65+
Source: US Census Bureau International Data Base

15
Why? Dramatic Increase in Life Expectancy
1900 1950 1970 1980 1990 20001910 1920 1930 1940 1960
75
70
65
60
55
50
45
40
80
Source: U.S. Social Security Administration
Average Life Expectancy at Birth in the U.S.

16
Aging, Disability and Healthcare Costs
Patterns & Trends

17
Median age of employed population by selected industry
Source: 2003 Current Population Survey, U.S. Department of Labor

18
Distribution of short (STD) and long (LTD) term disability by age
Source: UnumProvident Disability Database, 2002-2004.

19
Risk dynamics-STD duration of lost time by age group
Source: UnumProvident Disability Database, 2002-2004.

20
Risk dynamics-STD by major impairment category
Source: UnumProvident Disability Database, 2002-2004.

21
Risk Dynamics-STD lost days by selected impairments
Source: UnumProvident Disability Database, 2002-2004.

22
AmbiguousImpairmentsAmbiguousImpairments
High ScoresHigh Scores
Prevalence =% of ee’sreporting condition
Prevalence =% of ee’sreporting condition
Medical Conditions & Productivity Connections

23
Healthcare costs by age x risk
Source: Musich, McDonald, Hirschland, Edington, Disease Managements & Health Outcomes 2002; 10(4): 251-258; University of Michigan Health Management Research Center.
Used with permission. Dee Edington, Ph.D. University of Michigan, Ann Arbor, Michigan

24
Implications for Benefits Design
• Productivity Increasing need for Disease/”Condition” Management
• Aging Increasing incidence, duration cost pressures
• Cost pressures Increasing Medical costs Ancillary Benefits??
• Decision Pressure Shift from Employer to Employee funding
+ ?

25
• What base level of ancillary benefits will employers fund?
• What design will “stabilize” employer costs?
• What gaps will remain for employees?
• How will employees choose what to add?
• What will employees consider understandable?
• What will employees consider affordable?
Things to Consider

26
Critical Illness
LTC
Medical
Dental
STDIIP
LTD
• Generally Er Funded
• Choices made by Er
Old Choices New Approach?
ConsumerChoice
DiseaseMgmt.
Medical
VisionDental
LTD
IIP
• Greater Employee Responsibility
• Reduced Employer Funding
• Longer EPs for disability
• Higher co-pays if “unmanaged
• Greater Need for support service
• Greater Need for asset consideration
HSAHRA
Co-pay
STD