Embed Size (px)
Citation preview
1
Rare Diseases and Orphan Medicinal Products
Máster en diagnóstico y terapia de las enfermedades raras
Josep Torrent-FarnellUniversitat Autònoma de Barcelona
Hospital de la Santa Creu i Sant PauComité de Medicamentos Huérfanos, EMEA, Londres
22 marzo 2010Universidad Internacional de Andalucía
2
Why a regulation for Orphan Medicines is needed?
• Some conditions occur so infrequently that the cost
of developing a medicinal product would not be
recovered by the expected revenues. Therefore the
pharmaceutical industry is unwilling to develop
these medicines under normal market conditions.
Patients suffering from rare conditions should be entitled to the same quality of treatment as other patients
(EC Regulation No 141/2000)
3
Some facts on rare diseases (I)
• More than 6,000 rare conditions have been identified (WHO)
• People affected by Orphan diseases(*)
• USA: 20 million
• EU: 25-30 million
• Spain: 3,5 million
(*)Estimate figures
4
Some facts on rare diseases (II)
• More than 4,000 rare conditions are genetic in origin and affect paediatric population
• People affected by inborn rare diseases
• 1/3 will die during the first year of life
• 1/3 will be handicapped for the span of life
• 1/3 will receive the most suitable treatment and have an acceptable quality of life
5
• A major public health burden recognized as a health priority by the EU (DG SANCO and DG Research)
• Causing severe deficits*: » Motor (44 % of all RD)» Chronic pain (22 %)» Intellectual (6.5 %)
• Long-term permanent disabilities*:» Undermining QoL/autonomy» Partial limitations (37 %)» Restricted autonomy (30 %)» Reduced activity (23 %)» Lack of autonomy (6 %)
* Data from Orphaned database
Some facts on rare diseases (III)
6
• An heterogeneous group of different clinical conditions affecting potentially all organs and systems of the body and all ages.
• They are life-threatening, serious and/or chronically debilitating, impairing QoL and causing long-lasting disabilities and dependences.
• They are “invisible” by the society and often “unknown” by health professionals.
• Requires a multidisciplinary approach for its overall management (genetic screening, pharmacologicals, surgery,nutraceuticals, rehabilitation, specific educational strategies, and social support).
Some facts on rare diseases (IV)
7
Orphan conditions (RD) vs neglected diseases
• Neglected diseases are medical conditions (severe, life-threatening and chronically debilitating) that have a high prevalence in developing regions (“poor countries”) but they display a low prevalence in developed regions (“rich countries”)
• Some examples are: Tuberculosis, Malaria, HIV/SIDA, Chagas disease, Leihmaniasis Buruli ulcer, sleep sickness, etc.
8
Some examples of Rare Diseases*
• Hodgking and non-Hodgking Lymphomas
• All types of Leukemias
• More than 400 solid cancers conditions
• Multiple Mieloma
• Sarcoidosis
• Graft-versus-Host Diseases
• Duchene Muscular Distrophy
• Friedreich Ataxia
• Leber Hereditary Optic Neurophaty (LHON)
• Laron Syndrome
* NORD, EURORDIS, ORPHANET, databases
• ELA
• Pompe Disease
• Nieman-Pick-Disease
• Gaucher Disease
• Fabry Disease
• Polyarteritis Nodosa
• Mucopolysaccharidosis
• Thalasemias
• Ewing Sarcoma
• Churg-Strauss Syndrome
9
Some examples of “Ultra Rare Diseases” > 1000 cases*
• Cohen Syndrome
• Larsen Syndrome
• Seckel Syndrome
• Gunther Disease
• Kimura Disease
• Ondine Syndrome
• Möbius Syndrome
• Coffin-Siris Syndrome
• CHILD Syndrome
• Li-Fraumeni Syndrome
* NORD, EURORDIS, ORPHANET, databases
10
Unmet medical needs for patients affected by rare disorders require global and international joint efforts
11
Orphan Medicinal Products: International Overview
• United States ‘Orphan Drug Act’ 1983
• Japan ‘Orphan Drug Legislation’ 1993
• Singapore ‘Orphan Legislation’ 1997
• Australia ‘Orphan Legislation’ 1998
• Europe ‘Orphan Regulation’ 2000
12
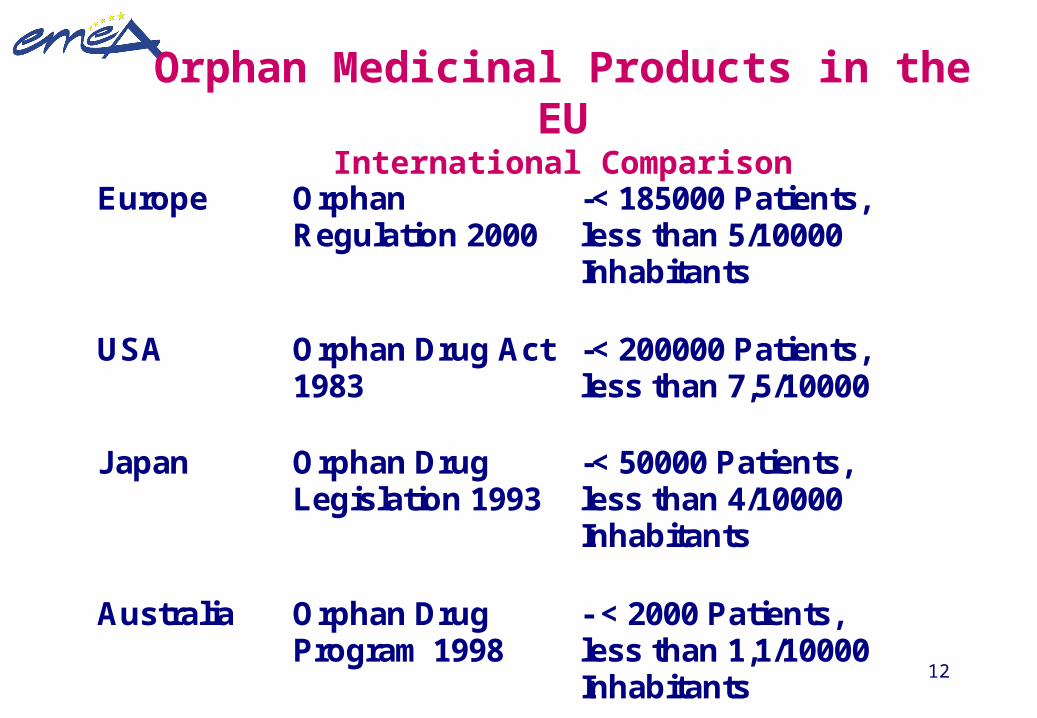
Orphan Medicinal Products in the EUInternational Comparison
Europe Orphan Regulation 2000
-< 185000 Patients, less than 5/10000 Inhabitants
USA Orphan Drug Act 1983
-< 200000 Patients, less than 7,5/10000
Japan Orphan Drug Legislation 1993
-< 50000 Patients, less than 4/10000 Inhabitants
Australia Orphan Drug Program 1998
- < 2000 Patients, less than 1,1/10000 Inhabitants
13
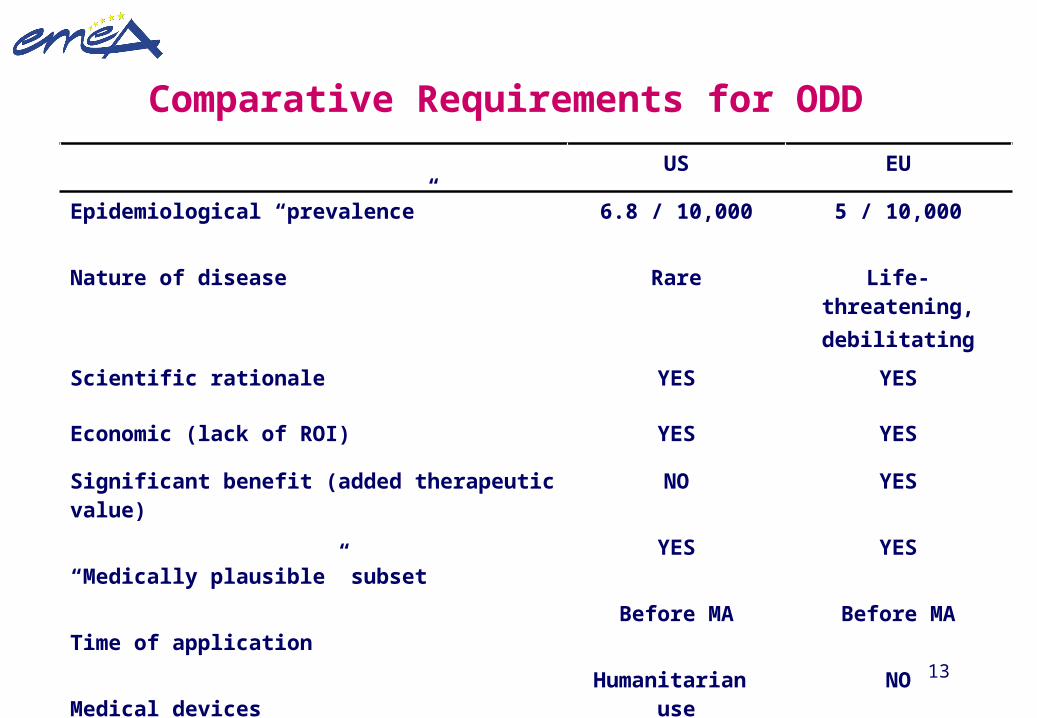
Comparative Requirements for ODD
US EU
Epidemiological “prevalence”
Nature of disease
6.8 / 10,000
Rare
5 / 10,000
Life-threatening,debilitating
Scientific rationale YES YES
Economic (lack of ROI) YES YES
Significant benefit (added therapeutic value)
“Medically plausible” subset
Time of application
Medical devices
NO
YES
Before MA
Humanitarian use
YES
YES
Before MA
NO
14
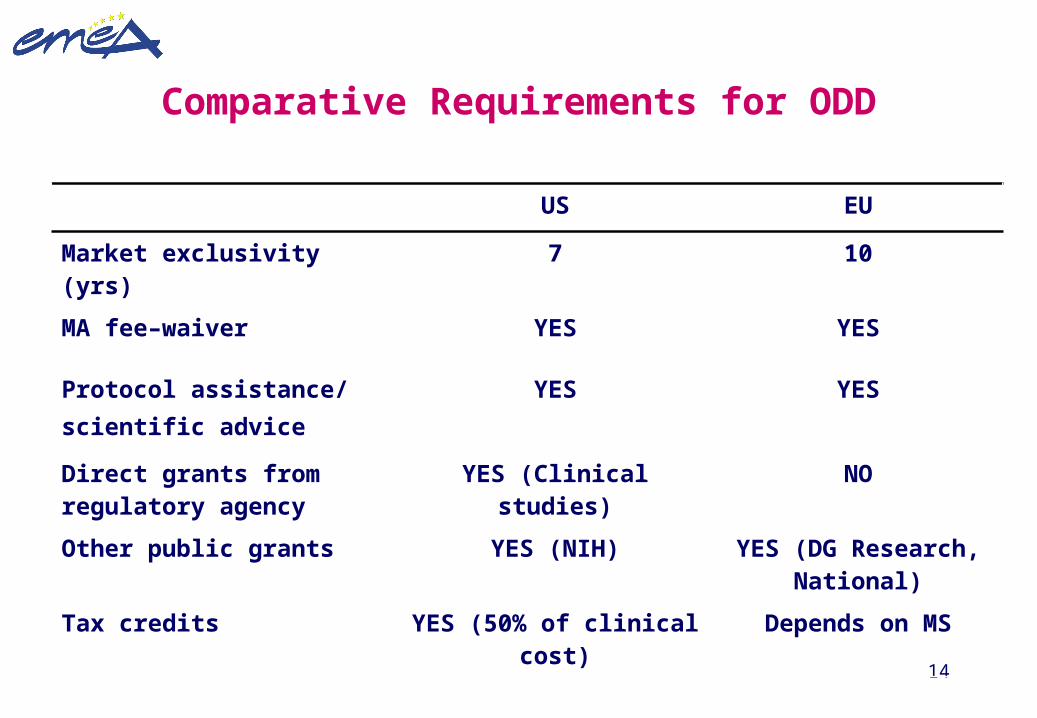
Comparative Requirements for ODD
US EU
Market exclusivity (yrs) 7 10
MA fee–waiver YES YES
Protocol assistance/scientific advice
YES YES
Direct grants from regulatory agency
YES (Clinical studies) NO
Other public grants YES (NIH) YES (DG Research, National)
Tax credits YES (50% of clinical cost) Depends on MS

15
Orphan Medicinal Products: Legal Basis
• Legal Basis Medicinal Products– Council Regulation (EEC) 2309/93– Council Directive 2001/83/EG– European Pharmacopoeia
• Legal Basis Orphan Products– EUROPEAN PARLIAMENT and COUNCIL REGULATION
(EC) No 141/2000– COMMISSION REGULATION (Ec) No 847/2000
16
Orphan Medicinal Products: Designation vs. Authorization (I)
• Authorization– ensuring that only medicinal products that
are effective, safe and of good quality are marketed.
• Designation– providing incentives for the development
of medicinal products for the benefit of patients suffering from rare conditions
17
Orphan Medicinal Products: Designation vs. Authorization (II)
Level of proof:
• Authorization– scientifically proven fact (beyond reasonable
doubts)
• Designation– reasonable scientific assumptions (hypothesis
based on solid scientific facts)
18
• Given by COMP is the “ENTRY GATE” and gives access to several incentives and to centralised system
• Epidemiological criteria (“one in two thousand”)
• Does not lower the requirements when submitting and application for M.A.
• Are mainly intended to mobilise partnering and funding for investigation in rare diseases
• Several different (or “sameness”) active substances can be designated for one specific orphan condition
Some basic considerations (I):
Designation
19
• Are given by the CHMP assessment on the quality, safety
and efficacy data submitted for centralised applications
• Orphan-market-exclusivity rights are linked to the
approved therapeutic indication by the CPMP
• Prevents “me-too” drugs entering to the EU market
Some basic considerations (II):
Marketing authorizations
20
Orphan Medicinal Products
• Orphan Condition
– Any deviation from the normal structure and function of the body, as manifested by a characteristic set of symptoms, typically a disease or syndrome.
– Benefit from incentives
• Therapeutic Indication
– It will be the result of the assessment of the quality, safety and efficacy data submitted with the marketing application
– It may be more restrictive than the orphan condition
– Benefit from market exclusivity rights
21
COMP Composition
• The regulation establishes the Committee for Orphan Medicinal Products (COMP), within the EMEA, which is responsible for examining all applications for orphan medicinal product designation submitted to it in accordance with the Regulation.
• 33 Members:– One member nominated by each of the Member States (27)– Three members nominated by the Commission to represent
patients’ organisations (3)– Three members nominated by the Commission on the basis of a
recommendation from the Agency (3)
22
Task of the Committee
• Scientific evaluation:
– Orphan drug designation– Protocol assistance (through SAWP)– Significant benefit at the time of granting MA– 5 years review (economic evaluation upon request
from MS)
• Public health activities:
– Advice Commission to establishment develop OMP policy
– Liaising internationally and liaising with patient groups
– Assist Commission in preparing guidelines– EU Experts Network/ Increase visibility
Designation means investigational orphan products
23
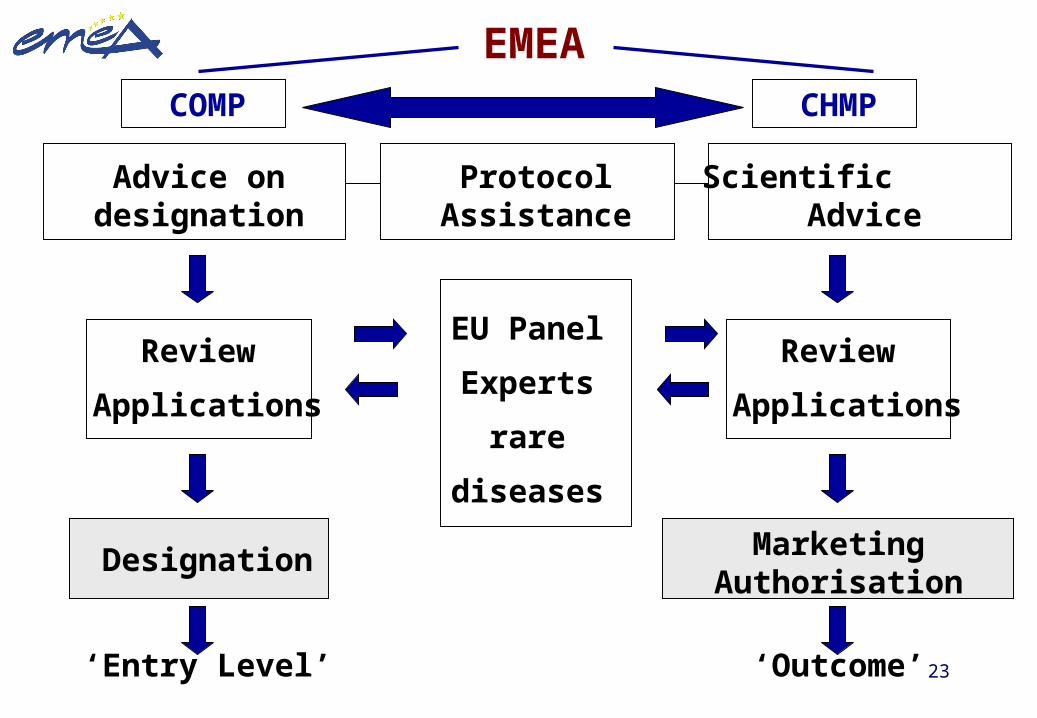
EMEACOMP
EU Panel
Experts
rare
diseases
CHMP
Marketing Authorisation
‘Entry Level’ ‘Outcome’
Review
Applications
Designation
Advice on designation Protocol Assistance Scientific Advice
Review
Applications
24
• Identifies ‘orphan’ products eligible for incentives
• Application from sponsor should demonstrate:
life-threatening or debilitating nature of condition
medical plausibility
prevalence < 5 in 10,000 or unlikely to generate sufficient return on investment no satisfactory methods exist or medicinal product will be of significant benefit
• COMP Opinions EC Designations
Orphan Designation Criteria
25
Comparative US/EU Criterion for Orphan Drug Designation
• Common• Epidemiological (prevalence)
(7/10.000 US; 5/10000 EU)• Economic (unlikely to generate sufficient return on
investment)• Medical plausibility of the condition• Biological/pharmacological rationale• Sub-setting (salami-slicing strategy):exceptional
• EU only• Assumption of significant benefit• Existing methods are not satisfactory
26
Orphan Medicinal Products in the EU
The Incentives (non exhaustive):
• Market exclusivity• Protocol assistance during the development, with
involvement of the CPMP• Access to the Centralized System (independent of List A/B)• Fee reduction for centralised applications (and marketing
authorisation maintenance activities)• Priority access to EU research programs• National incentives (grants, tax reductions)• SME’s Office (EMEA)
27
Comparative US/EU Incentive for Orphan Designated Products
• Common• Market exclusivity rights• Scientific Advice / Protocol Assistance/ SME’s• Fee-waivers
• Specific for US• Tax credit• FDA grants
• Specific for EU• Direct access to centralised procedure• Priority access to EU research programs• National incentives and measures
28
Orphan Medicinal Products in the EU
• Period of ten years exclusivity from the date of marketing
• Conditionsorphan designationAND marketing authorisation throughout EU
• Scope of exclusivity no market authorisation for similar medicinal products
in the same indication(s)
29
From: REGULATION (EC) No 141/2000Article 8, Market exclusivity
Where a marketing authorisation in respect of an orphan
medicinal product is granted pursuant to Regulation
(EEC) No 230993.. <cut>.. The Community and the
Member States shall not, for a period of 10 years, accept
another application for a marketing authorisation, or grant
a marketing authorisation or accept an application to
extend an existing marketing authorisation, for the same
therapeutic indication, in respect of a similar medicinal
product.
30
Significant benefit
• Normally in terms of improved efficacy and/or safety and/or contribution to patient care
• Exceptionally, potential availability can be taken into account, e.g. A product authorised in all Member States as opposed to a product authorised only in one or very few Member States
31
Defining a condition (I)
Exceptionally subsets as valid conditions:
A subset of a (frequent) disease could be considered a valid condition if patients in that subset present distinct evaluable characteristic(s) with a plausible link to the condition and if
– such characteristics are essential for the medicinal product to carry out its action
– the absence of these characteristics will render the product ineffective in the rest of the population
32
Defining a condition (II)
Generally invalid subset:
• Different degrees of severity or stages or localization of a disease
• A subset of patients within a condition in whom the product is expected to show a favorable benefit/risk
33
The “salami-slicing” and “evergreening” approaches are aimed to:
• Fragment the population into “artificial” subsets within a
disease/condition
• To meet the prevalence criteria by creating a “non-true” population
subgroup
• To benefit from market-exclusivity rights
• To attempt to lowering usual requirements for the submission of an
application for M.A.
• To gain additional exclusivity rights by adding subsequent new-non-
well justified target populations (“the evergreening tactic”)
34
Subsetting a medical condition:“salami-slicing strategy”
Total >5/10.000 “Subset” <5/10.000
Prevalence criteria
No Yes
35
Medically Plausible Subsets (I)
• The true disease process.
• The seriousness of the condition
• The inherent characteristics of the drug
• The mechanism of action of the drug
• Unique characteristics of the patient population
36
Medically Plausible Subsets (II)
• Is the subset a “real” sub-population?
• Eg., not a stage of the general disease category?
• Why should the drug be limited to this subset?
• Are there characteristics of the larger patient population
which exclude them from this treatment?
• Will the drug be useful in the larger population?
• Is the selection criteria in clinical trials acceptable ?
Questions to address:
37
ORPHAN DESIGNATION - How to Apply
• Sponsors to notify EMEA of intent to submit at least 2
months prior to filing
• Sponsors are encouraged to request a pre-submission
meeting with EMEA prior to filing
• Co-ordinators (1 COMP, 1 EMEA) and expert(s) will be
appointed
• Applications to be prepared in accordance with Guideline
on Format and Content of Applications for Designation
38
Orphan Medicinal Products in the EU
The procedure
A sponsor submits the application to the EMEA *
the EMEA validates the application (day 1)
the EMEA prepares a summary report
the EMEA COMP adopts an Opinion (by day 90)
the EU Commission adopts a Decision (30 days)
*Pre-submission meetings with EMEA highly encouraged
39
Protocol assistance
• 3 Representatives of the COMP are members of the Scientific Advice Review Group since January 2002.
• They are responsible for the evaluation of Questions related to significant benefit. In these cases the significant benefit responses are discussed and adopted by the COMP and the scientific advice letter is co-signed by the two Chairpersons
40
Dealing with the three possible scenarios for orphan designation
• Non authorised products are available in the EU• Evidence-based rationale needed
• Existing treatments are available in the EU
• “Assumption of significant benefit” or “Existing methods are not satisfactory”
• When a designated products holds a community authorisation
• A “similar” should demonstrate “clinical superiority” to the existing one
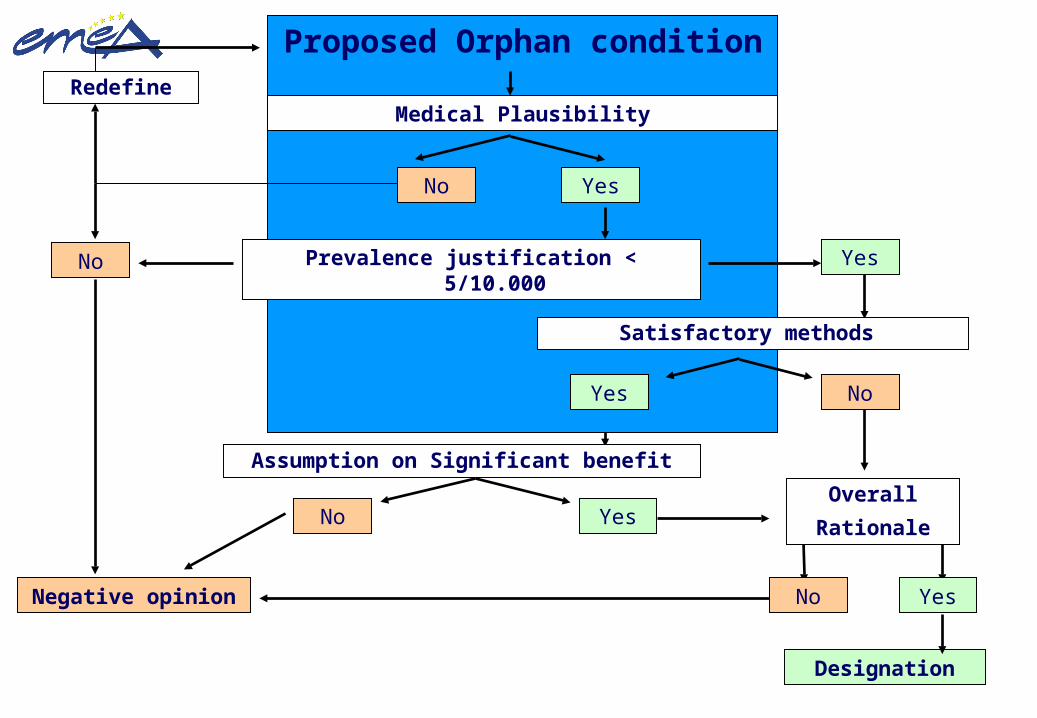
41
Proposed Orphan condition
Prevalence justification < 5/10.000No Yes
Satisfactory methods
Yes No
Negative opinion
Overall
Rationale
Designation
Assumption on Significant benefit
No Yes
No Yes
Medical Plausibility
YesNo
Redefine
42
SUMMARY OF ORPHAN DRUGS
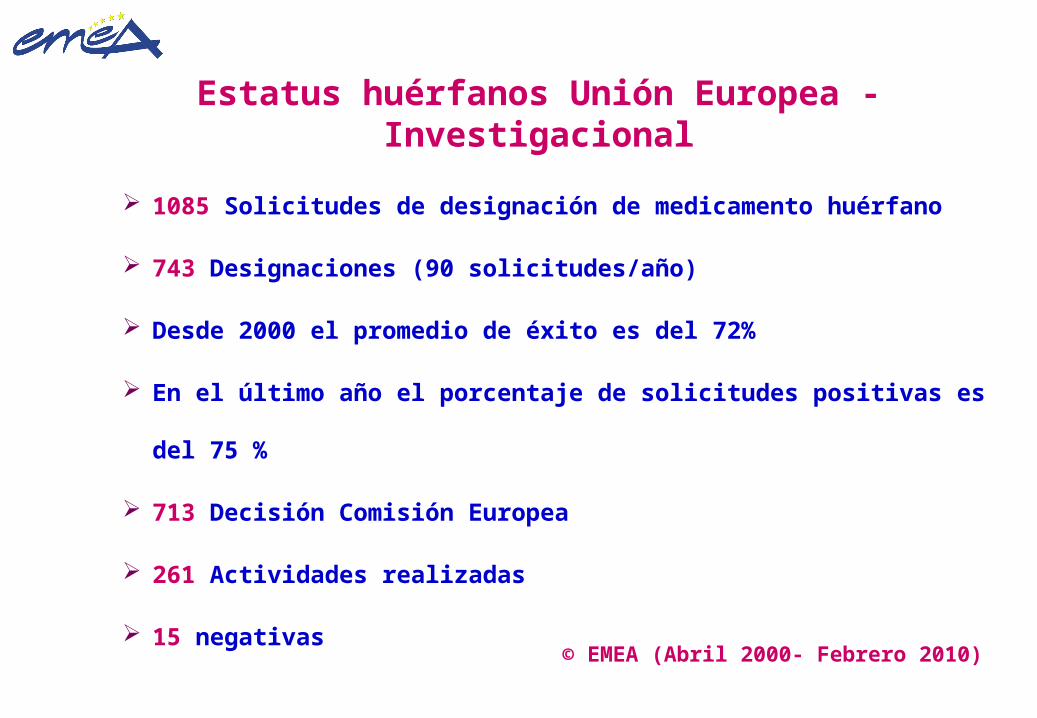
Estatus huérfanos Unión Europea - Investigacional
1085 Solicitudes de designación de medicamento huérfano
743 Designaciones (90 solicitudes/año)
Desde 2000 el promedio de éxito es del 72%
En el último año el porcentaje de solicitudes positivas es del 75 %
713 Decisión Comisión Europea
261 Actividades realizadas
15 negativas
© EMEA (Abril 2000- Febrero 2010)
Update 22 February 2010 ©European Medicines Agency
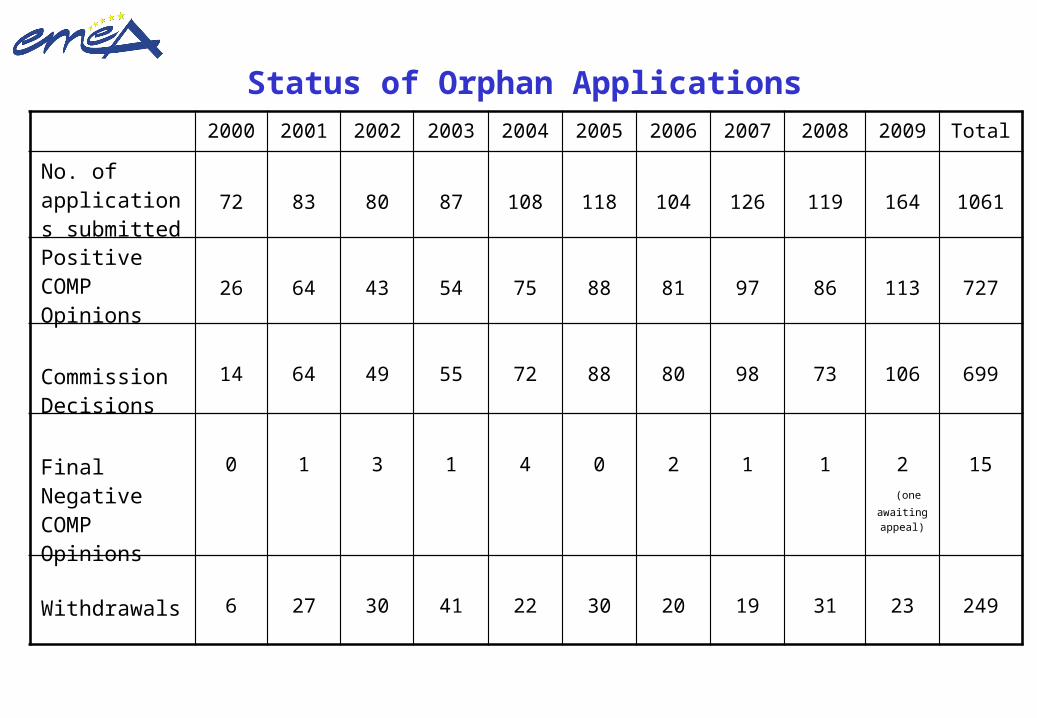
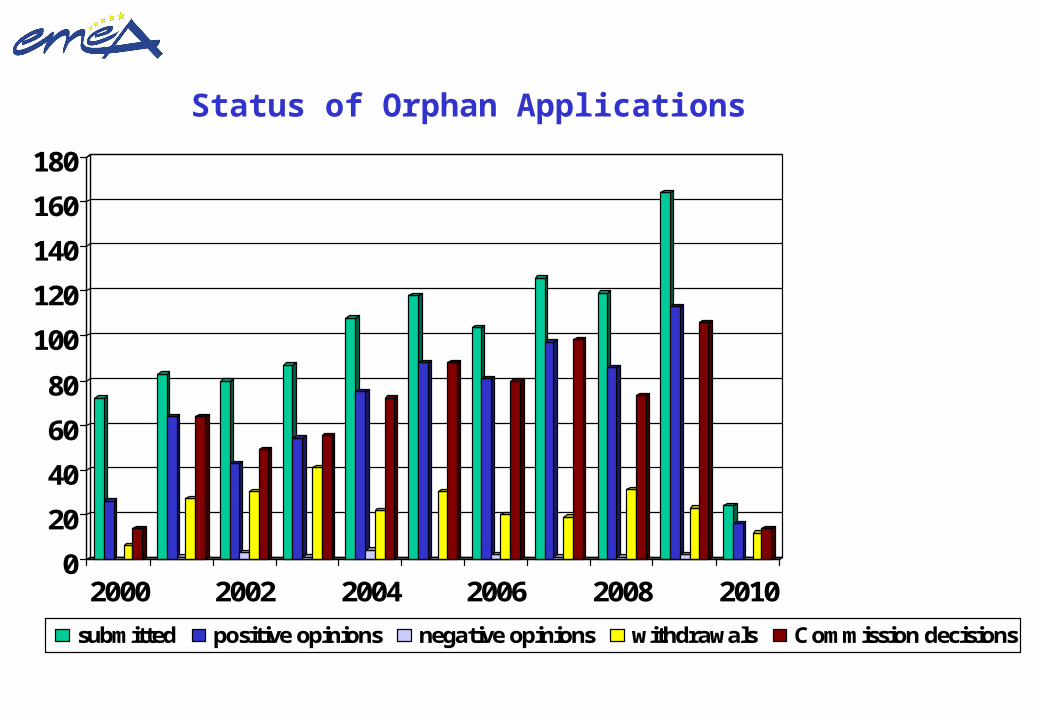
Status of Orphan Applications 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 Total
No. of applications submitted
72 83 80 87 108 118 104 126 119 164 1061
Positive COMP Opinions
26 64 43 54 75 88 81 97 86 113 727
Commission Decisions
14 64 49 55 72 88 80 98 73 106 699
Final Negative COMP Opinions
0 1 3 1 4 0 2 1 1 2 (one
awaiting appeal)
15
Withdrawals 6 27 30 41 22 30 20 19 31 23 249
Update 22 February 2010 ©European Medicines Agency
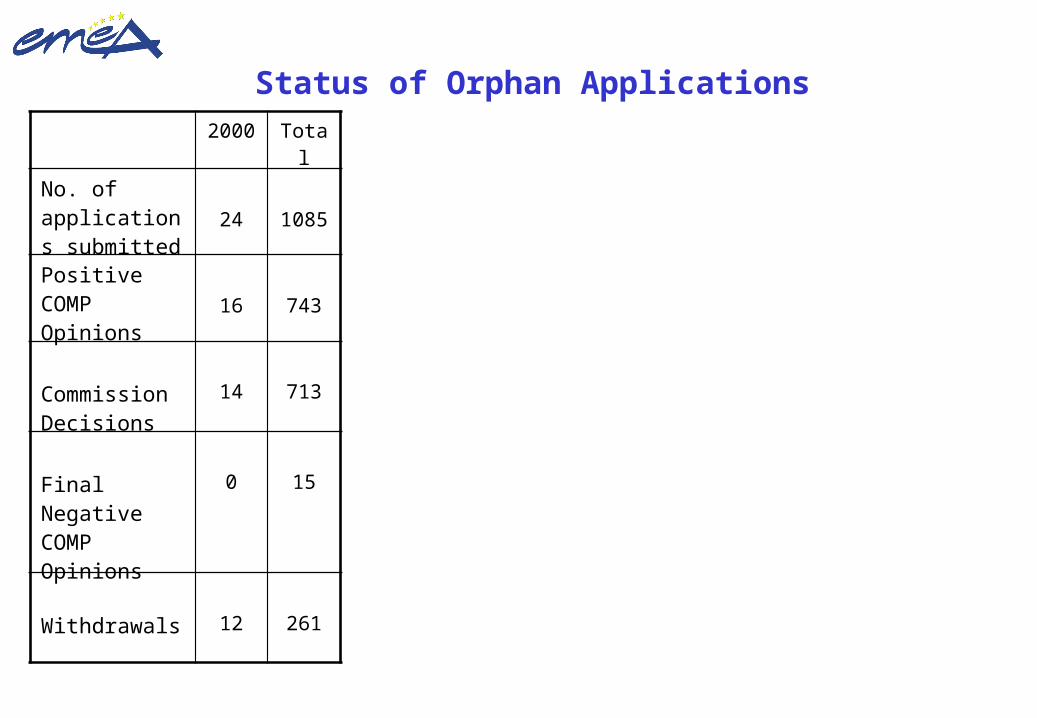
Status of Orphan Applications 2000 Total
No. of applications submitted
24 1085
Positive COMP Opinions
16 743
Commission Decisions
14 713
Final Negative COMP Opinions
0 15
Withdrawals 12 261
Update 22 February 2010 ©European Medicines Agency
0
20
40
60
80
100
120
140
160
180
2000 2002 2004 2006 2008 2010
submitted positive opinions negative opinions withdrawals Commission decisions
Status of Orphan Applications
Update 22 February 2010 ©European Medicines Agency
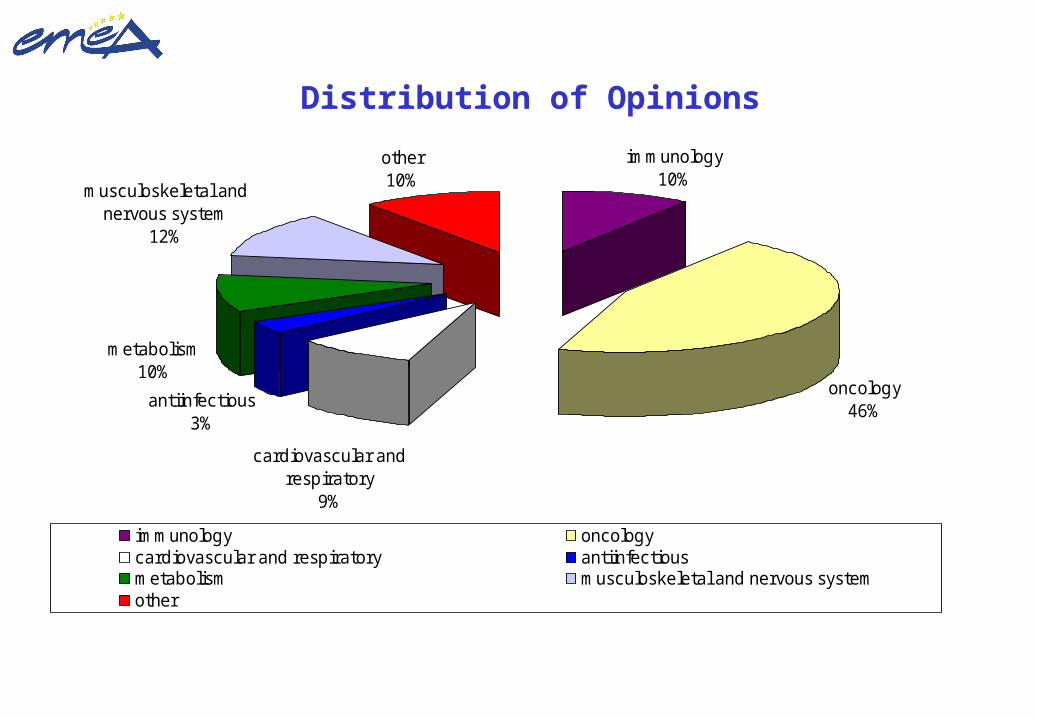
Distribution of Opinions
immunology10%
oncology46%antiinfectious
3%
musculoskeletal and nervous system
12%
other10%
metabolism10%
cardiovascular and respiratory
9%
immunology oncologycardiovascular and respiratory antiinfectiousmetabolism musculoskeletal and nervous systemother

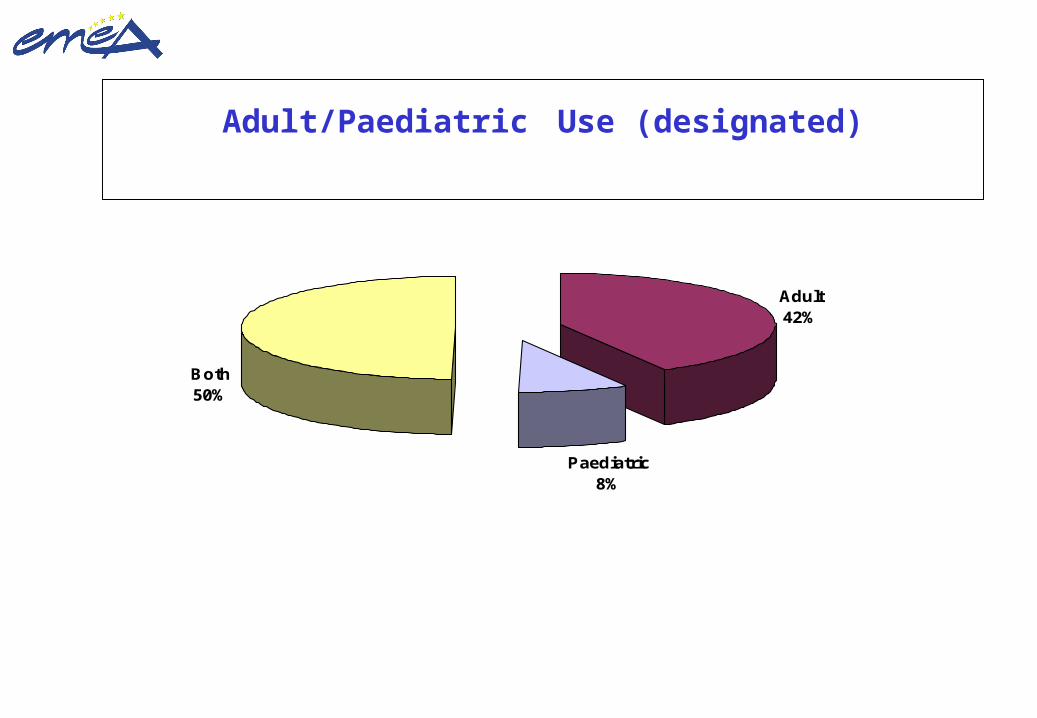
8% 50% 42% Medicamentos Huérfanos designados distribuidos por tipo de población (total: 743)
Medicamentos Huérfanos designados en la UE (II) Abril 2000 – Febrero 2010
COMP/EMEA
Update 22 February 2010 ©European Medicines Agency
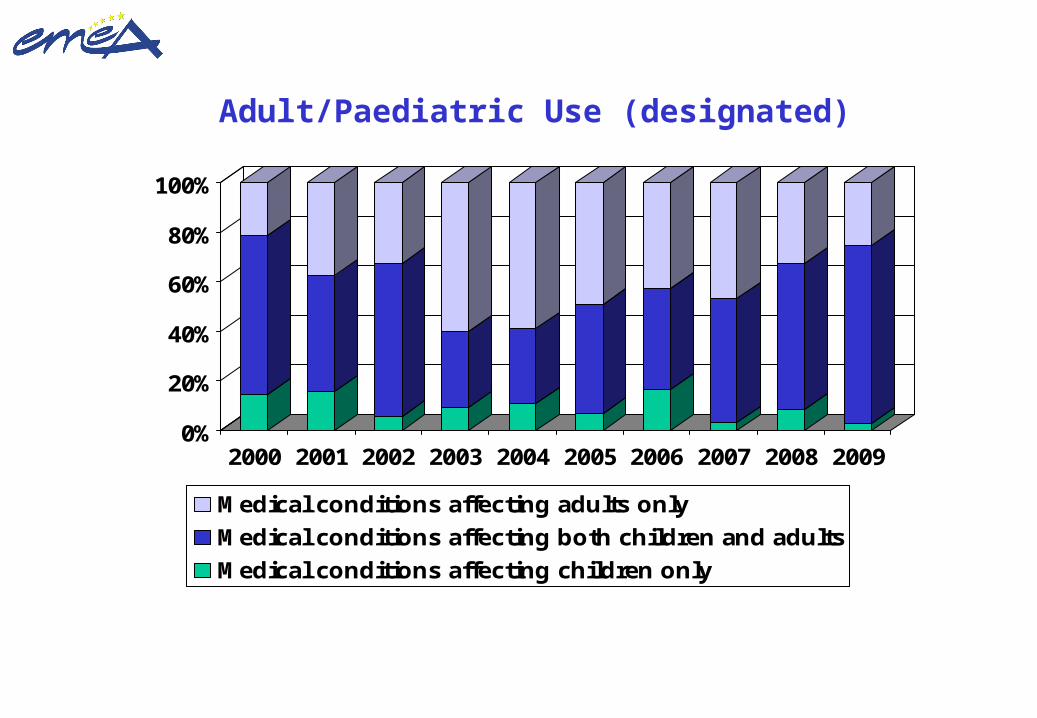
Adult/Paediatric Use (designated)
Adult42%
Paediatric8%
Both50%
Update 22 February 2010 ©European Medicines Agency
0%
20%
40%
60%
80%
100%
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Medical conditions affecting adults only
Medical conditions affecting both children and adults
Medical conditions affecting children only
Adult/Paediatric Use (designated)
Update 22 February 2010 ©European Medicines Agency
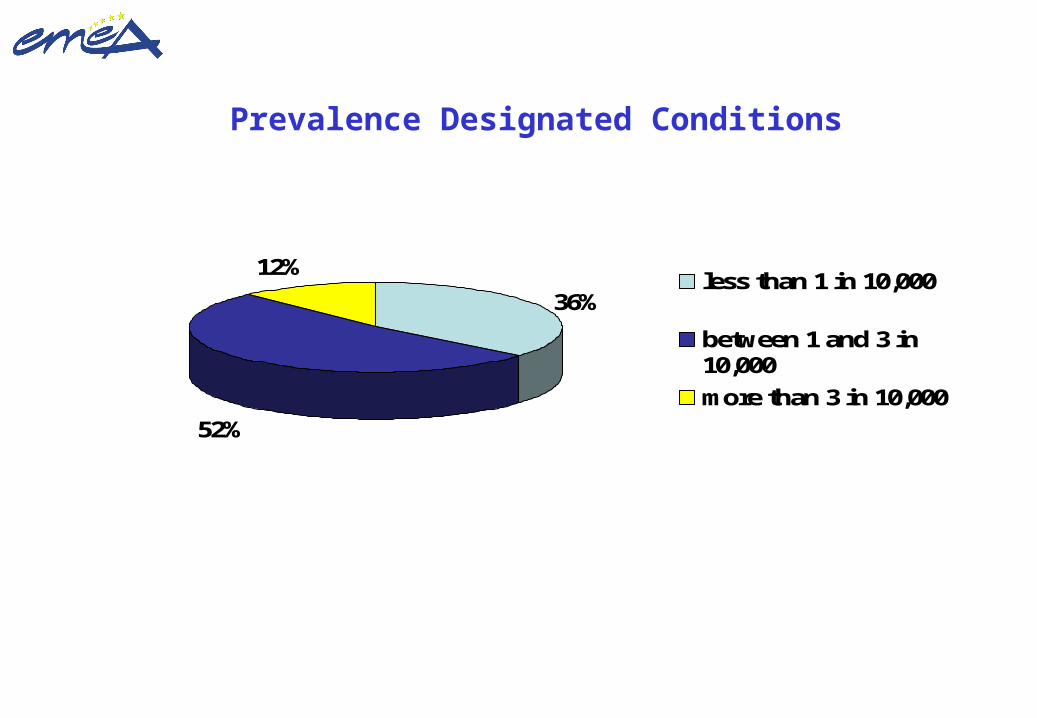
Prevalence Designated Conditions
36%
52%
12%less than 1 in 10,000
between 1 and 3 in10,000
more than 3 in 10,000
Update 22 February 2010 ©European Medicines Agency
Fabrazyme for Fabry disease Replagal for Fabry disease Glivec for chronic myeloid leukaemia, ALL, GIST, DFSP, MDS/MPD and HES/CEL Tracleer for pulmonary arterial hypertension, systemic sclerosis Trisenox for acute promyelocytic leukaemia Somavert for acromegaly Zavesca for Gaucher disease and Niemann-Pick type C disease Carbaglu for N-acetylglutamate synthetase deficiency
•2 withdrawn from the register of orphan drugs
59 authorisations granted to date*
cont’d
Status of Orphan Marketing Authorisation Applications
Update 22 February 2010 ©European Medicines Agency
Aldurazyme for Mucopolysaccharidosis type I Busilvex for haematopoietic progenitor cell transplantation Ventavis for pulmonary arterial hypertension Onsenal for Familial Adenomatous Polyposis Litak for indolent non-Hodgkin’s lymphoma Lysodren for adrenal cortical carcinoma Pedea for Patent Ductus Arteriosus Photobarr for Barret’s oesophagus Wilzin for Wilson's disease Xagrid for Thrombocythaemia
59 authorisations granted to date
cont’d
Status of Orphan Marketing Authorisation Applications
Update 22 February 2010 ©European Medicines Agency
Orfadin for tyrosinemia type 1 Prialt for chronic pain requiring intraspinal analgesia Xyrem for narcolepsy - withdrawn from the register of orphan drugs
Revatio for pulmonary arterial hypertension Naglazyme for Mucopolysaccharidosis VI or Maroteaux-Lamy
syndrome Myozyme for Glycogen Storage Disease type II (Pompe’s
disease) Evoltra for acute lymphoblastic leukaemia Nexavar for renal cell carcinoma and hepatocellular carcinona
Status of Orphan Marketing Authorisation Applications 59 authorisations granted to date
cont’d
Update 22 February 2010 ©European Medicines Agency
Sutent for gastrointestinal stromal tumour and renall cell carcinoma - withdrawn from the register of orphan drugs
Savene for anthracycline extravasation Thelin pulmonary arterial hypertension Exjade for chronic iron overload requiring chelation
theraphy Sprycel for chronic myeloid leukaemia and acute
lymphoblastic leukaemia Inovelon for epilepsy Cystadane for homocystinuria Elaprase for mucopolysaccharidosis
Status of Orphan Marketing Authorisation Applications 59 authorisations granted to date
cont’d
Update 22 February 2010 ©European Medicines Agency
Diacomit for myoclonic epilepsy in infancy Revlimid for multiple myeloma Soliris for paroxysmal nocturnal haemoglobinuria Siklos for sickle cell syndrome Atriance for acute lymphoblastic leukaemia Increlex for growth failure Gliolan for glioma Yondelis for soft tissue sarcoma, ovarian cancer Tasigna for chronic myelogenous leukaemia Torisel for renal cell carcinoma, mantle cell lymphoma Thalidomide Pharmion 50 mg Hard Capsules for
myeloma
Status of Orphan Marketing Authorisation Applications 59 authorisations granted to date
cont’d
Update 22 February 2010 ©European Medicines Agency
Volibris for pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension
Firazyr for angioedema Ceplene for acute myeloid leukaemia Kuvan for hyperphenylalaninemia Vidaza for myelodysplastic syndromes, chronic
myelomonocytic leukemia and acute myeloid leukemia Nplate for thrombocytopenia Mepact for osteosarcoma Nymusa for apnoea Afinitor for renal cell carcinoma
Status of Orphan Marketing Authorisation Applications 59 authorisations granted to date
cont’d
Update 22 February 2010 ©European Medicines Agency
Mozobil for stem cell transplantation Cayston for cystic fibrosis Arcalyst for cryopirin-associated periodic syndromes Ilaris for cryopirin-associated periodic syndromes Firdapse for Lambert-Eaton myasthenic syndrome
59 authorisations granted to dateStatus of Orphan Marketing Authorisation Applications
Update 22 February 2010 ©European Medicines Agency
59 authorisations granted to date by THERAPEUTIC FIELD * ONCOLOGY
Acute lymphoblastic leukaemia (ALL)Evoltra, Glivec, Sprycel, Atriance
Acute myeloid leukaemiaTrisenox, Ceplene, Vidaza
Adrenal cortical carcinomaLysodren
Chronic eosinophilic leukaemia (CEL) and the hypereosinophilic syndrome (HES)
Glivec
Chronic myeloid leukaemia (CML)Glivec, Sprycel, Tasigna * 2 withdrawn from the register of orphan drugs
Status of Orphan Marketing Authorisation Applications by Therapeutic Field
cont’d
Update 22 February 2010 ©European Medicines Agency
59 authorisations granted to date by THERAPEUTIC FIELD
ONCOLOGY cont’d
Dermafibrosarcoma protuberans (DFSP)Glivec
Dysplasia in Barrett's EsophagusPhotobarr
Familial Adenomatous PolyposisOnsenal
Gastrointestinal stromal tumours (GIST)Glivec, Sutent withdrawn from the register of orphan drugs
GliomaGliolan
Status of Orphan Marketing Authorisation Applications by Therapeutic Field
cont’d
Update 22 February 2010 ©European Medicines Agency
59 authorisations granted to date by THERAPEUTIC FIELD
ONCOLOGY cont’d
Hairy cell leukaemiaLitak
Hepatocellular carcinomaNexavar
Mantle cell LymphomaTorisel
OsteosarcomaMepact
Ovarian cancerYondelis
Status of Orphan Marketing Authorisation Applications by Therapeutic Field
cont’d
Update 22 February 2010 ©European Medicines Agency
59 authorisations granted to date by THERAPEUTIC FIELD
ONCOLOGY cont’d
Renal cell carcinomaNexavar, Sutent withdrawn from the register of orphan drugs, Torisel, Afinitor
Soft tissue sarcoma (STS)Yondelis
Status of Orphan Marketing Authorisation Applications by Therapeutic Field
Update 22 February 2010 ©European Medicines Agency
Status of Orphan Marketing Authorisation Applications by Therapeutic Field
59 authorisations granted to date by THERAPEUTIC FIELD
ENDOCRINO/METABOLISM
AcromegalySomavert
Fabry diseaseFabrazyme, Replagal
Gaucher diseaseZavesca
Glycogen Storage DiseaseMyozyme
Growth factor-1 deficiencyIncrelex cont’d
Update 22 February 2010 ©European Medicines Agency
Status of Orphan Marketing Authorisation Applications by Therapeutic Field - cont’d
59 authorisations granted to date by THERAPEUTIC FIELD
ENDOCRINO/METABOLISM cont’d
HomocystinuriaCystadane
HyperphenylalaninemiaKuvan
MucopolysaccharidosisAldurazyme, Elaprase, Naglazyme
N-acetylglutamate synthetase deficiencyCarbaglu
Niemann-Pick type C disease
Zavesca cont’d
Update 22 February 2010 ©European Medicines Agency
Status of Orphan Marketing Authorisation Applications by Therapeutic Field
59 authorisations granted to date by THERAPEUTIC FIELD ENDOCRINO/METABOLISM cont’d
TyrosinaemiaOrfadin
Wilson's diseaseWilzin
HAEMATOLOGY
Essential thrombocythaemiaXagrid
Haematopoietic cell transplantationBusilvex
Haemoglobinuria Soliris cont’d
Update 22 February 2010 ©European Medicines Agency
Status of Orphan Marketing Authorisation Applications by Therapeutic Field
59 authorisations granted to date by THERAPEUTIC FIELD HAEMATOLOGY cont’d
Iron overload Exjade
Multiple myeloma (MM)Revlimid, Thalidomide Pharmion 50 mg Hard Capsules
Myelodysplastic/myeloproliferative diseases (MDS/MPD)Glivec, Vidaza
Sickle cell syndromeSiklos
ThrombocytopeniaNplate
Stem cell transplantationMozobil cont’d
Update 22 February 2010 ©European Medicines Agency
59 authorisations granted to date by THERAPEUTIC FIELD
CARDIOVASCULAR AND RESPIRATORY
Patent ductus arteriosusPedea
Pulmonary arterial hypertension (PAH)Tracleer, Ventavis, Revatio, Thelin
Pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension
VolibrisApnoea
Nymusa
Cystic fibrosisCayston
Status of Orphan Marketing Authorisation Applications by Therapeutic Field
cont’d
Update 22 February 2010 ©European Medicines Agency
59 authorisations granted to date by THERAPEUTIC FIELD
NERVOUS SYSTEM
EpilepsyDiacomit, Inovelon
NarcolepsyXyrem withdrawn from the register of orphan drugs
PainPrialt
Lambert-Eaton myasthenic syndromeFirdapse
Status of Orphan Marketing Authorisation Applications by Therapeutic Field
cont’d
Update 22 February 2010 ©European Medicines Agency
Status of Orphan Marketing Authorisation Applications by Therapeutic Field
59 authorisations granted to date by THERAPEUTIC FIELD
OTHER
Systemic sclerosis (scleroderma)Tracleer
Anthracycline extravasationsSavene
Angioedema Firazyr
Cryopirin-associated periodic syndromesArcalyst, Ilaris
Update 22 February 2010 ©European Medicines Agency
Adopted positive opinion Tepadina for haematopoietic progenitor cell
transplantation Revolade for idiopathic thrombocytopenic purpura Arzerra for chronic lymphocytic leukaemia
Ongoing applications in review process 12 centralised applications in review process
Variations / Line Extensions in review process Negative outcomes for orphan MAA
34 applications for MA withdrawn 6 negative decisions/refusals
Status of Orphan Marketing Authorisation Applications
Update 22 February 2010 ©European Medicines Agency
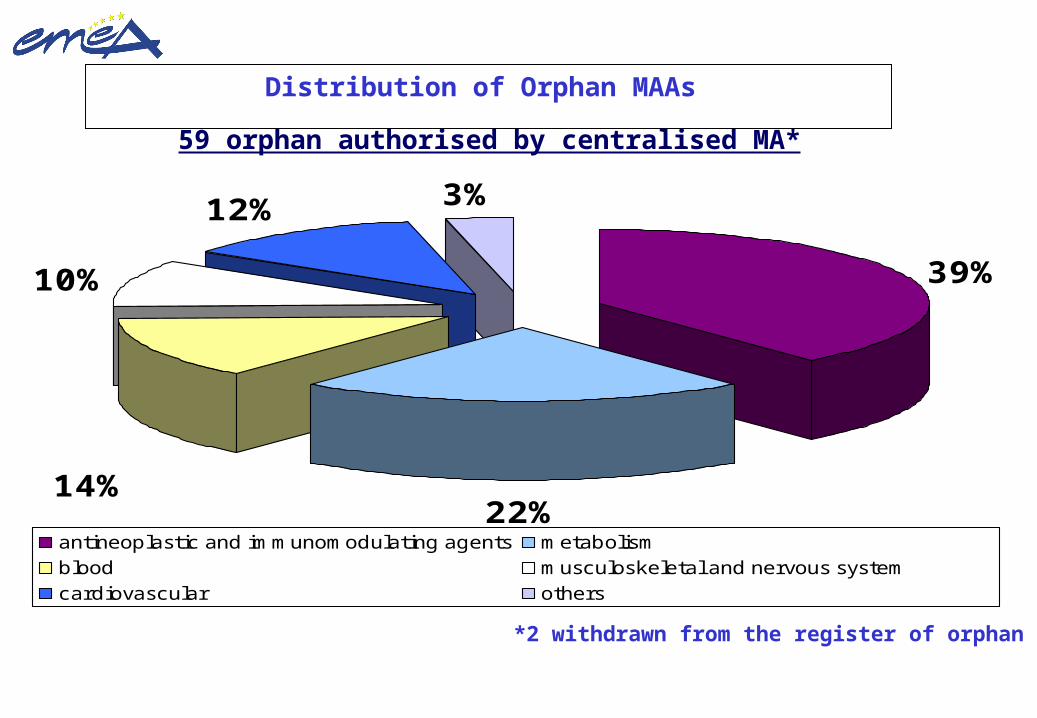
Distribution of Orphan MAAs
39%
22%
10%
12% 3%
14%
antineoplastic and immunomodulating agents metabolismblood musculoskeletal and nervous systemcardiovascular others
59 orphan authorised by centralised MA*
*2 withdrawn from the register of orphan drugs
Update 22 February 2010 ©European Medicines Agency
©European Medicines Agency 2010. Reproduction and/or distribution of this document is possible for non-commercial purposes provided that EMEA is always acknowledged as the source in each copy. Citations may be made, provided the source is always acknowledged. See: http://www.emea.europa.eu/htms/technical/dmp/copyritel.htm
73
Common deficiencies for ODD refusal
1) Scientific rational (Proof of Concept) weak, inconsistent or poorly
justified (40%)
2) Prevalence figures based on inappropriate epidemiological data (59%)
3) Lack of medically plausible target population (artificial subsetting) (41%)
4) Inaccurate search of existing authorised methods for the orphan
condition
5) Assumptions on significant benefit not credible or not well-substantiated
(42%)
A “dream” is not enough for designation
74
APPROVAL UNDER: EXCEPTIONAL CIRCUMSTANCES or CONDITIONAL APPROVAL
Limited clinical data available because:
rare disease (“orphan disease”) current scientific knowledge does not allow a
comprehensive assessment ethical constraints in performing conventional RCT
“Specific Obligations” (i.e. Clinical studies) should be carried out within an agreed timeframe
Annual re-assessment of the benefit/risk ratio by the CHMP
The SPC should contain this information
75
Some hurdles on Orphan Medicines Clinical Research (I)
• Lack of public awareness (“Invisible diseases”)• Scarcity of Clinical Experts and Reference Centres• Delays on Diagnosis (Genetic Testing / Neonatal screening)• Small size population• Geographic dispersion• Life-threatening /chronic debilitating conditions• Heterogeneous conditions• Difficult to stratify by stage/severity• Limited available treatments
76
• Lack of validated biomarkers and surrogate endpoints• Lack of predictive/validated preclinical models• Ethical concerns on the use of placebo (e.g. Emerging
therapies) and vulnerable population• Off-label use (medicines for children)• Participative role of patients to be increased• Poorly motivated health professionals/investigators• Lack of information to “care-givers”• Excessive bureaucratic/administrative barriers
Some hurdles on Orphan Medicines Clinical Research (II)
77
Challenges on Orphan Drug Clinical Development (“Feasibility Concept”)
• Conventional methodological designs need to be adjusted and applied in a flexible manner
• Alternative methodological approaches and patient-saving designs should be encouraged
• Compassionate and expanded access programs should not undermined the conduct of well-designed studies
• Investigation phase goes beyond the MA: conditional / under exceptional circumstances approval, thus early PhV planning and risk-management strategies becomes crucial
« Nice to know v.s. Need to know »
78
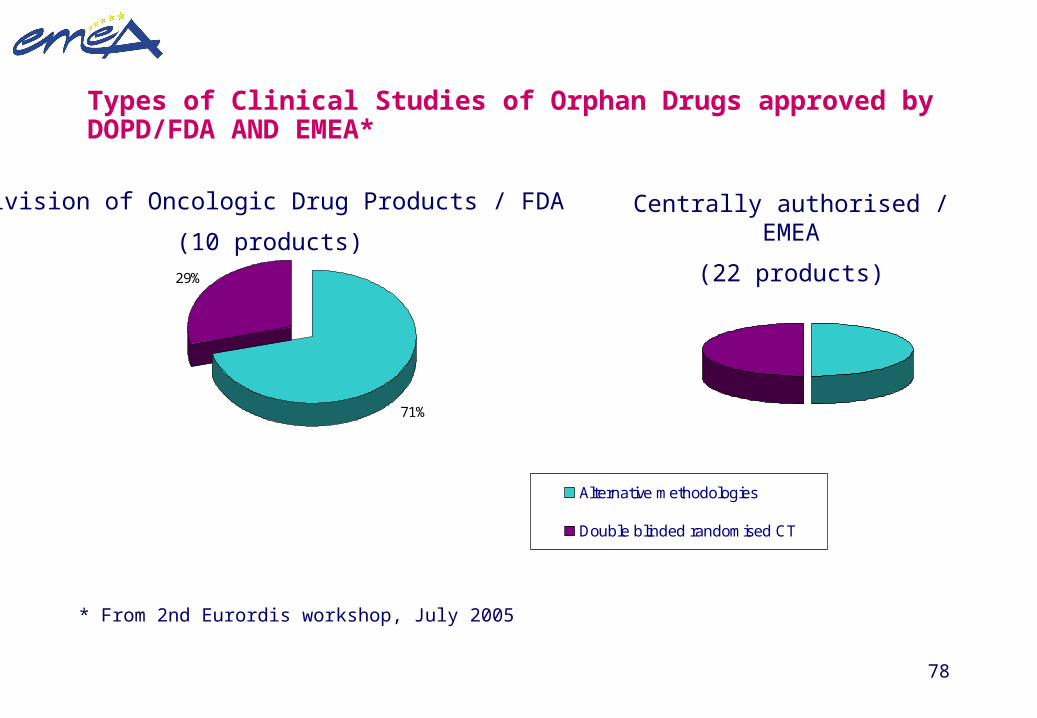
Types of Clinical Studies of Orphan Drugs approved by DOPD/FDA AND EMEA*
71%
29%
Division of Oncologic Drug Products / FDA
(10 products)
Alternative methodologies
Double blinded randomised CT
Centrally authorised / EMEA
(22 products)
* From 2nd Eurordis workshop, July 2005

79
List of Drugs Approved by DODP
Drug (Year of Approval)
Indication Number of
“Pivotal” Studies
Patients
Clofarabine (’04) Relapsed or refractory ALL 2 66
Tositumomab (’01) CD20+ follicular NHL 5 230
Alitretinoin (’99) Kaposi sarcoma 2 350
Bortezomid (’03) Progressive multiple myeloma 2 256
Imatinib (’02) CD117+ unresectable GIST 1 147
Pemetrexed (’04) Metastatic malignant mesotheliona 1 448
Doxorubicin (’99) Refractory metastatic ovarian cancer 4 650
Gemtuzumab ozogamicin (’00)
CD33+ acute myelocytic leukemia 3 277
Carmustine (’96) Recurrent glioblastoma multiforme 1 222
Alemtuzumab (’01) Chronic lymphocytic leukemia 3 149
80
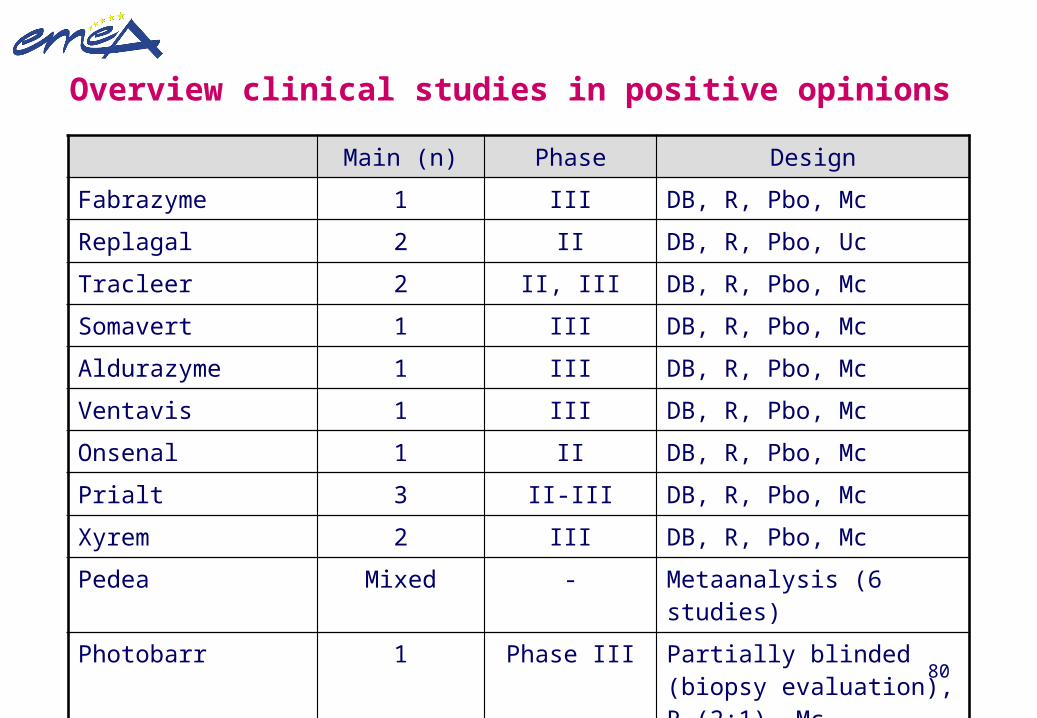
Overview clinical studies in positive opinions
Main (n) Phase Design
Fabrazyme 1 III DB, R, Pbo, Mc
Replagal 2 II DB, R, Pbo, Uc
Tracleer 2 II, III DB, R, Pbo, Mc
Somavert 1 III DB, R, Pbo, Mc
Aldurazyme 1 III DB, R, Pbo, Mc
Ventavis 1 III DB, R, Pbo, Mc
Onsenal 1 II DB, R, Pbo, Mc
Prialt 3 II-III DB, R, Pbo, Mc
Xyrem 2 III DB, R, Pbo, Mc
Pedea Mixed - Metaanalysis (6 studies)
Photobarr 1 Phase III Partially blinded (biopsy evaluation), R (2:1), Mc
81
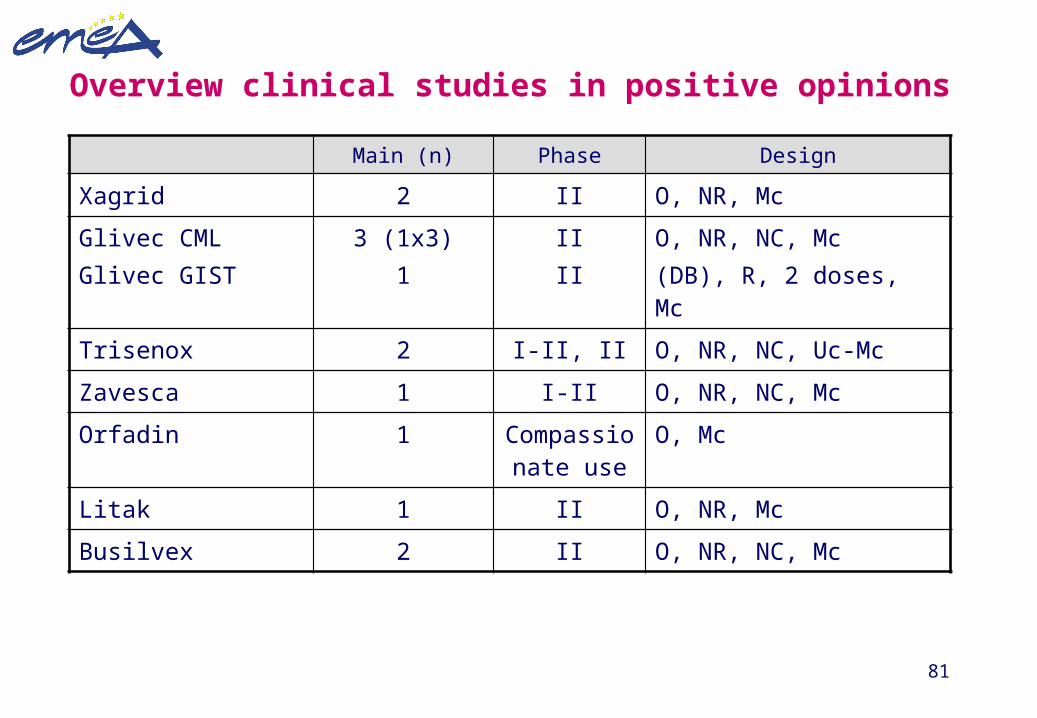
Main (n) Phase Design
Xagrid 2 II O, NR, Mc
Glivec CMLGlivec GIST
3 (1x3)1
IIII
O, NR, NC, Mc (DB), R, 2 doses, Mc
Trisenox 2 I-II, II O, NR, NC, Uc-Mc
Zavesca 1 I-II O, NR, NC, Mc
Orfadin 1 Compassionate use
O, Mc
Litak 1 II O, NR, Mc
Busilvex 2 II O, NR, NC, Mc
Overview clinical studies in positive opinions
82
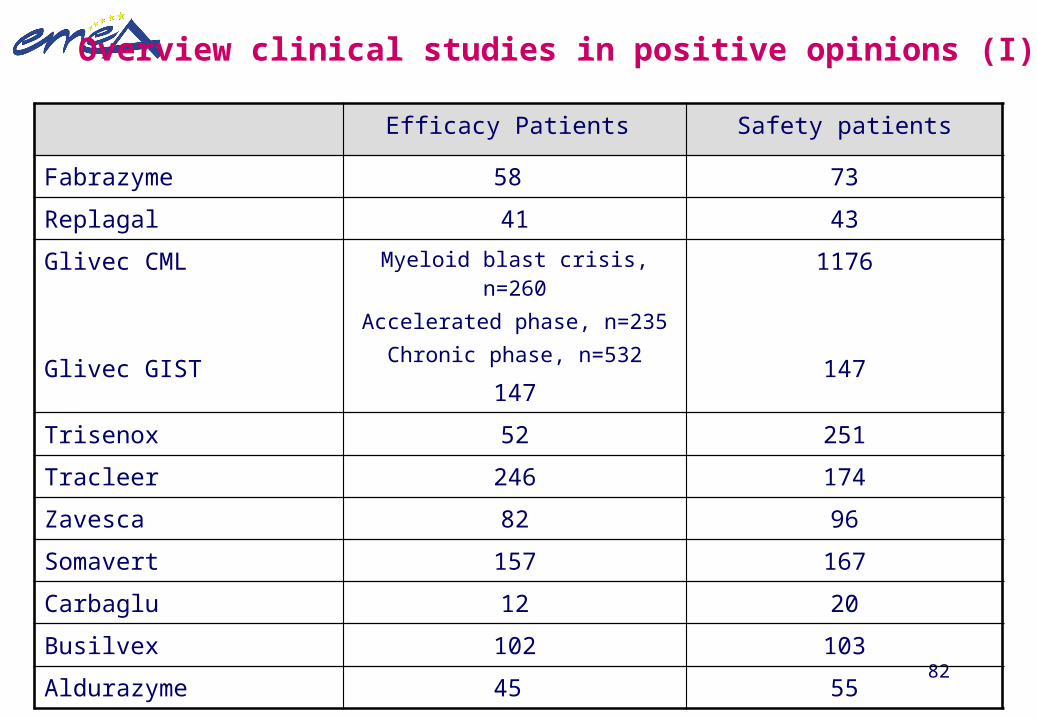
Overview clinical studies in positive opinions (I)
Efficacy Patients Safety patients
Fabrazyme 58 73
Replagal 41 43
Glivec CML
Glivec GIST
Myeloid blast crisis, n=260Accelerated phase, n=235
Chronic phase, n=532
147
1176
147
Trisenox 52 251
Tracleer 246 174
Zavesca 82 96
Somavert 157 167
Carbaglu 12 20
Busilvex 102 103
Aldurazyme 45 55

83
Efficacy Patients Safety patients
Ventavis 203 279
Xagrid* 316 (+ 242 compassionate)
>4600
Onsenal 83 83
Litak 63 523
Photobarr 208 324
Lysodren 1064, bibliographic >2000
Pedea 429 metaanalysis 986
Wilzin 191 bibliographic 255
Overview clinical studies in positive opinions (II)
84
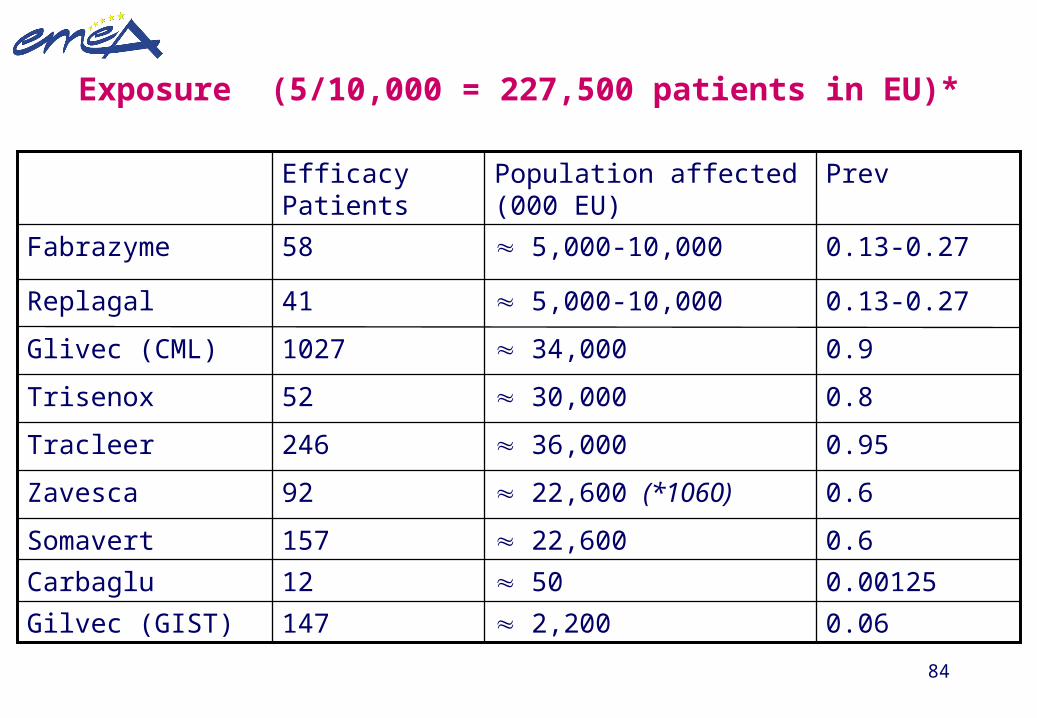
Exposure (5/10,000 = 227,500 patients in EU)*
0.00125 5012Carbaglu
0.6 22,600157Somavert
0.06 2,200147Gilvec (GIST)
0.6 22,600 (*1060)92Zavesca
0.95 36,000246Tracleer
0.8 30,00052Trisenox
0.9 34,0001027Glivec (CML)
0.13-0.27 5,000-10,00041Replagal
0.13-0.27 5,000-10,00058Fabrazyme
PrevPopulation affected (000 EU)
Efficacy Patients
85
BE AWARE OF...
... the evidence indicates that the benefit/risk profile is driving the orphan drug approval when there are difficulties to perform conventional prospective randomised trials
Randomised clinical trials are the gold standard for investigating and confirming clinical safety and efficacy of new medicinal products ...
but
(Some) rare conditions may need alternative methodological and statistical considerations without compromising efficacy and/or undermining safety
EMEA guideline for the conduct of clinical investigations insmall sized populations (adopted, February 2006)
86
Patients
The patient’s perspective:Why collaborate in clinical trials?
Clinical trials
Disease Treatments
Experts Actors Users
Research Market
Sponsors
87
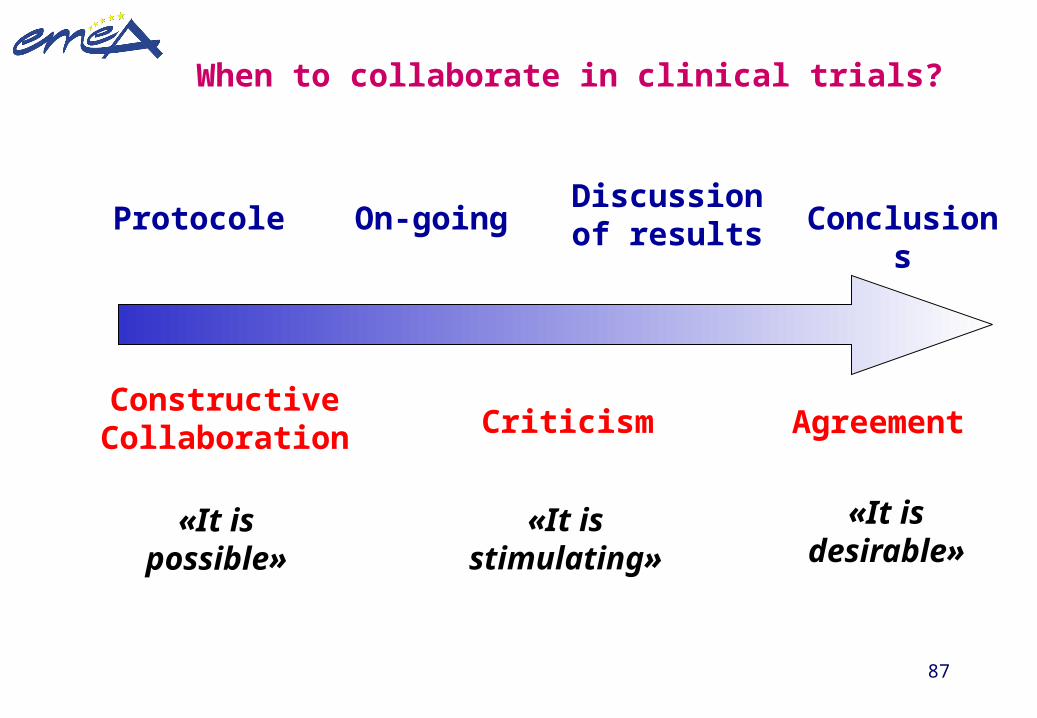
When to collaborate in clinical trials?
Protocole On-goingDiscussion of results
Constructive Collaboration Criticism Agreemen
t
«It is possible»
«It is stimulating
»
«It is desirable»
Conclusions
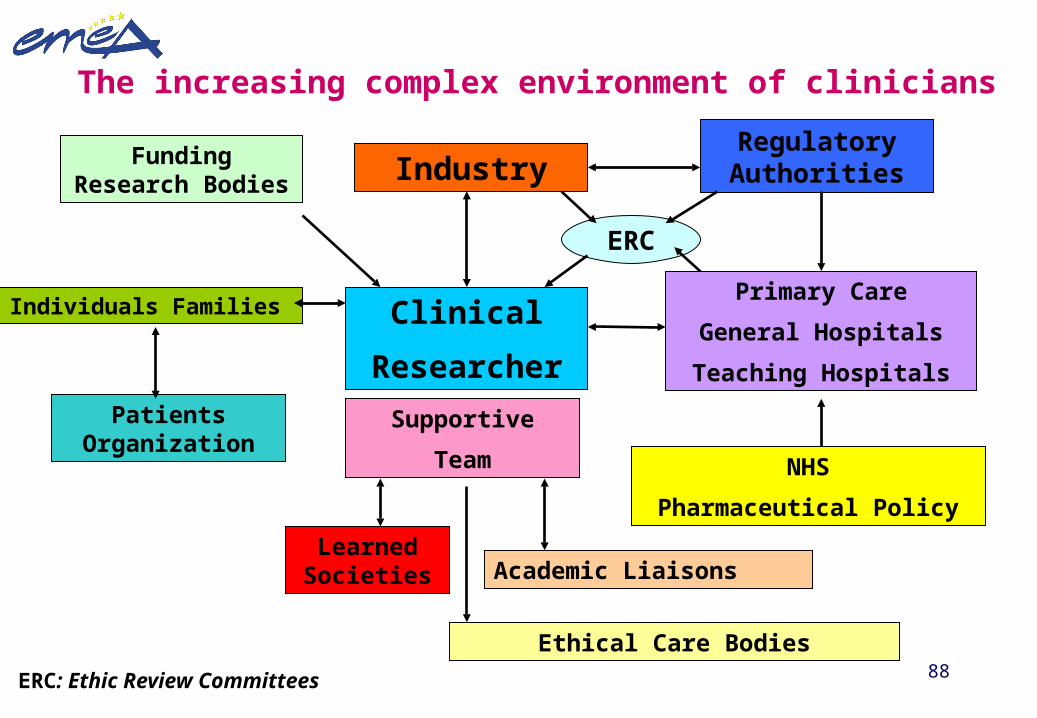
88
Clinical
Researcher
Individuals Families
Patients Organization
Learned Societies
Supportive
Team NHS
Pharmaceutical Policy
IndustryRegulatory Authorities
Primary Care
General Hospitals
Teaching Hospitals
Academic Liaisons
ERC
The increasing complex environment of clinicians
Funding Research Bodies
Ethical Care Bodies
ERC: Ethic Review Committees
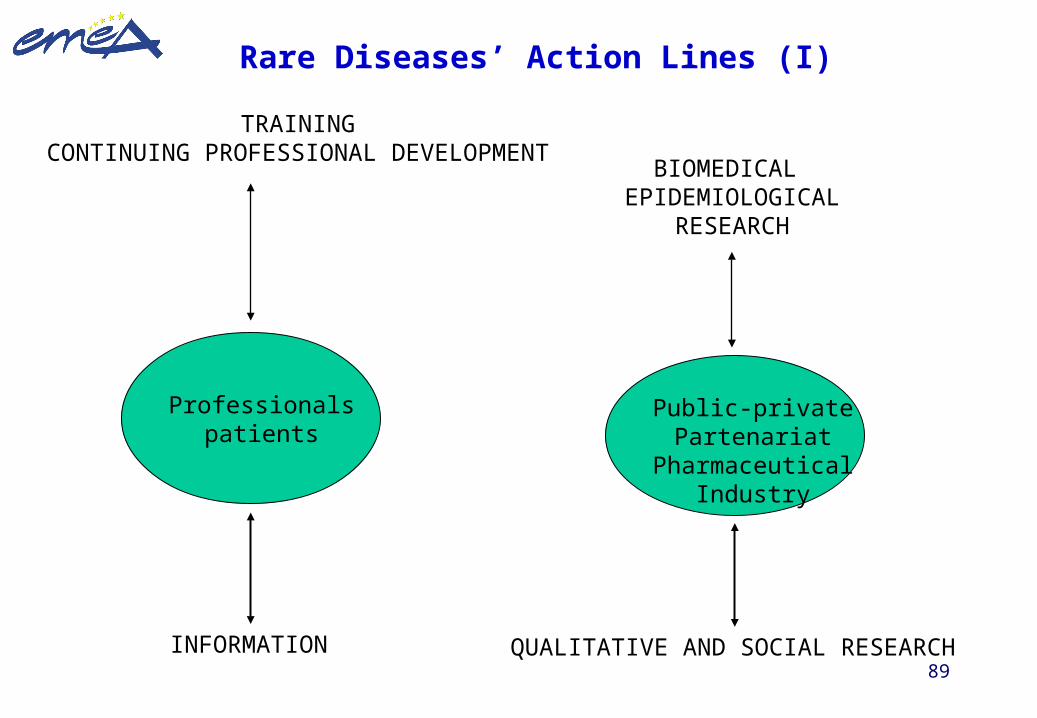
89
TRAININGCONTINUING PROFESSIONAL DEVELOPMENT
Professionalspatients
INFORMATION
BIOMEDICAL EPIDEMIOLOGICAL
RESEARCH
Public-privatePartenariat
PharmaceuticalIndustry
QUALITATIVE AND SOCIAL RESEARCH
Rare Diseases’ Action Lines (I)
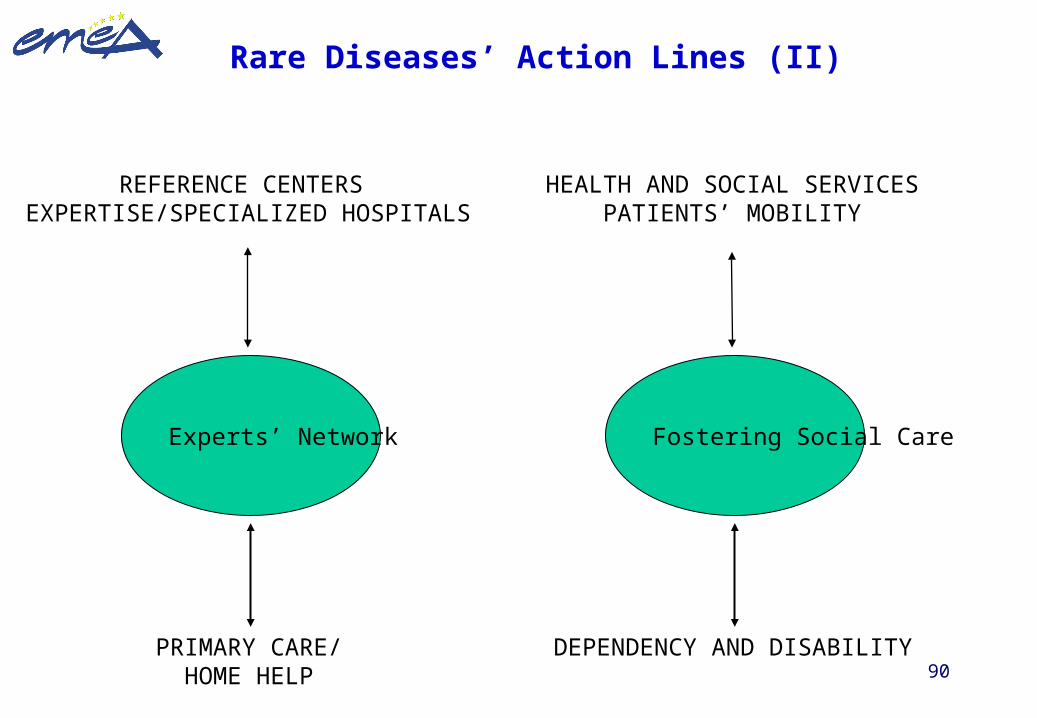
90
REFERENCE CENTERS EXPERTISE/SPECIALIZED HOSPITALS
Experts’ Network
PRIMARY CARE/HOME HELP
HEALTH AND SOCIAL SERVICESPATIENTS’ MOBILITY
Fostering Social Care
DEPENDENCY AND DISABILITY
Rare Diseases’ Action Lines (II)
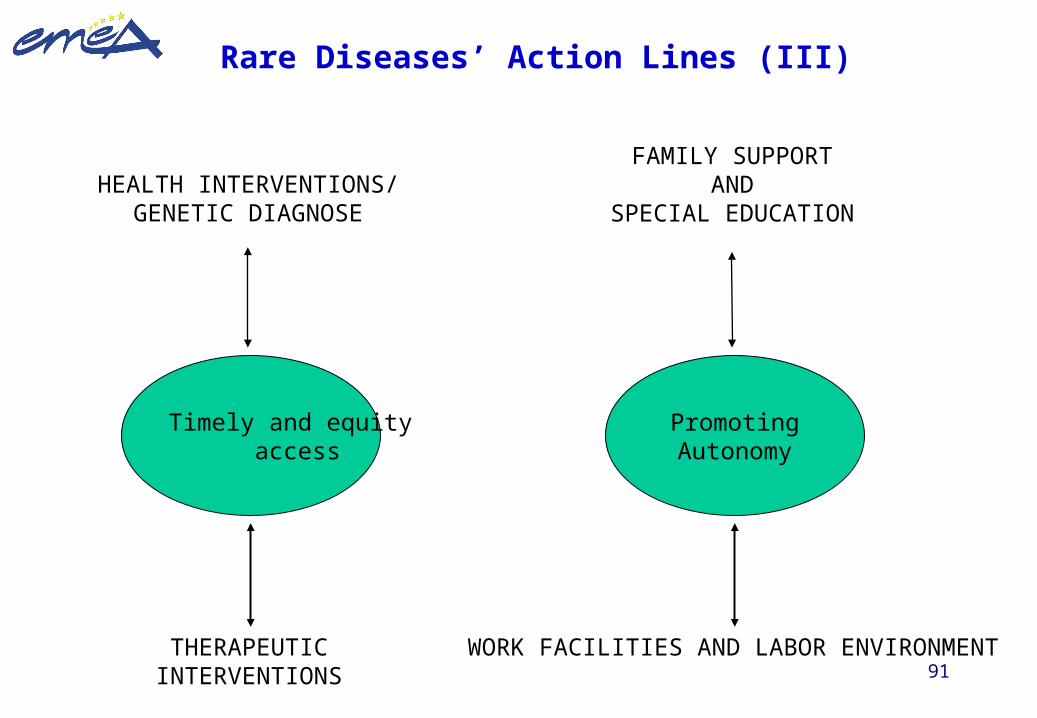
91
HEALTH INTERVENTIONS/GENETIC DIAGNOSE
Timely and equity access
THERAPEUTICINTERVENTIONS
FAMILY SUPPORTAND
SPECIAL EDUCATION
PromotingAutonomy
WORK FACILITIES AND LABOR ENVIRONMENT
Rare Diseases’ Action Lines (III)
92
EU Advisory AgencyOEER
EU/National and
Regional Co-ordination
RESEARCH, TRAINING, EXPERTS
BEST PRACTICESEU CONFERENCES
EU BUDGET
Health Indicators
NATIONAL BUDGETS
Rare Diseases’ Action Lines (IV)
93
DOCUMENTOS DE REFERENCIA
• Comunicación de la Comisión Europea (GD Sanco, 2008): Las enfermedades raras: un desafío para Europa. Comisión Europea
• Recomendación del Consejo, 2009
• Senado: Ponencia de Estudio de ER, 23 febrero 2007
• Plan Nacional de Enfermedades Raras 20 junio 2009
Plan Nacional Francés de ER 2004-2008
94
Recent Spanish contribution to foster Orphan Drug Research for Rare Diseases (I)
1. Priority for pricing and reimbursement (Dirección General de Farmacia)2. New decree for compassionate and extended use (AEMPS)3. Scientific Advice for Clinical Investigations (AEMPS)4. CIBER for Rare Diseases Research (Instituto de Salud Carlos III)5. Burgos National Center (Ministerio de Asuntos Sociales)6. Decree for establishing references centers (Ministerio de Sanidad)7. Call for funding independent clinical research (January 2007/20ME,
DGF/AEMPS)8. Report and recommendations from the Spanish Senate (February 2007)9. Priority for several Spanish-based pharmaceutical industries
(Farmaindustria / Plan Profarma, Ministerio de Industria)10. Disabilities and Social Help (Ley de Dependencia)
95
Recent Spanish contribution to foster Orphan Drug Research for Rare Diseases (II)
11. National Health Care System: Plan Nacional de Enfermedades Raras (June 2009)
12. Several actions at autonomous and regional level: Cataluña
– Propuesta de resolución sobre enfermedades raras; Parlamento de Cataluña. Tram 250/01182-08; Butlletí Oficial del Parlament de Catalunya; 31 julio 2008; Núm. 312;
– Generalitat de Catalunya; creación de la Comisión Asesora en Enfermedades Raras (CAMM) (mayo 2009)
– La Marató de TV3 año 2009 Enfermedades Raras– Generalitat de Catalunya; creación de la Comisión de Acceso a Terapias
Complejas (CATFAC) (febrero 2010)
96
Awareness activities growing
Positive impact on SME’s
Increasing innovative medicines: paving the road for the entrance of emerging therapies
Facilitating liaison of reference health/research centres
Openness of Public Clinical Trials Database
Better understanding of patient’s needs
Progressive prioritisation of RD on public health agendas
….But ……
Benefits of EU Orphan Medicines Regulation
97
…….Much still remains to be done………
Ensuring availability/access to OMP for all patients
Warranting affordability and long-term sustainability
Global approach and more inter-regional cross-collaboration
Better epidemiological knowledge of many rare conditions
Developing appropriate methodological / statistical patient-saving approaches
Strengthen early pharmacovigilance planning and risk management strategies
Increasing public funding from UE/national institutions
More and better co-ordination of National Incentives
98
So….. Rare Diseases offers…..
• An unique and challenging clinical paradigm
• Encompasses a wide range of different medical conditions
• Knowledge gather in this setting can be extrapolated in other conventional diseases
• High contribution from patients organisations
• Stimulates creativity and interest of clinicians and academics
• Big-pharma and SMEs may use this opportunity to further develop “personalised” medicines
99
Creating a true EU partnering environment with all stake-holders
Rare (low-prevalence) diseases are a pan-European challenge that need national solutions
…also…
Rare conditions are a national problem that need EU strong support and policy commitment