Embed Size (px)
Citation preview

1
Louise Maye
PodiatristPodiatry and Footcare Services
Greater Newcastle Cluster
Care of the diabetic foot
A podiatrist’s perspective

Diabetes & Feet
“Diabetic foot complications are the single most common cause of non-traumatic lower limb amputations in the industrialised world”
Armstrong D, Lavery L & Harkless L (1998) Who is at risk for diabetic foot ulceration? Clinics in Podiatric Medicine and Surgery, 15 pp
11-19
Foot problems are the most common reason for hospital admissions for people with diabetes and approximately 50% of all amputations are attributable to diabetesNational Report to Health Ministers on Diabetes 1998 p124 and ABS 1997

Diabetes & Feet
It has been suggested that as many as 75% of amputations due to diabetes could be prevented by appropriate foot care
Larsson J, Apelqvist J, Agardh C & Stenstrom A (1995) Decreasing the incidence of major amputation in diabetic patients: a
consequence of multi-disciplinary foot care team approach? Diabetic Medicine 12, 770

• Most foot problems are preventable when:
they are identified early
they are treated appropriately
people are educated to avoid these problems

Role of the Podiatrist in Diabetes
provide … wound care
biomechanical assessment
footwear / orthotic prescription
palliative care
ingrown toenail surgery
Conduct diabetes foot assessments
Provide education to clients and their families

Diabetes Foot Assessment
Should be performed every 6-12 months
Risk factors to be assessed:
peripheral vascular disease
peripheral neuropathy
dermatological conditions and skin integrity
abnormal lower limb biomechanics
inappropriate footwear
poor self care

Education: Client needs to …
Standard holistic advice regarding blood pressure, BGLs, smoking, diet and exercise
But the main points that need to get across from our behalf are to:
Be aware of potential foot problems
Check feet DAILY!
Wear appropriate footwear at all times

Aetiology of Foot Wounds
Primary Factors
Peripheral neuropathy
Peripheral vascular disease
Secondary Factors
Limited joint mobility
Bony deformity
Trauma
Immune responseAustralian National
Association of Diabetes Centres, The National Diabetes Foot Care
Project

Assessment of Foot Wounds
Aetiology
Neuropathic ulcer
Ischaemic ulcer
Neuroischaemic ulcer
Infection
Local
Cellulitis
Osteomyelitis
Investigations
X-ray
Swab
Bone scans
MRI
Referral
Endocrinologist
Vascular Consultant
Orthopaedic Consultant
Rehabilitation Consultant
Dietitian

Treatment of Foot Wounds
Debridement
Conservative sharp
Mechanical
Autolytic
Enzymatic
Surgical
Dressings
Pressure management
Surgery
Infection management
Oedema management

Off-Loading Options
total contact cast
soft cast shoes
removable cast walkers
post-op shoes / all purpose boots
orthoses
felt padding
combination of the above

Total Contact Casts
Gold standard for offloading plantar neuropathic foot wounds
Traditionally plaster of paris with fibreglass shell – minimally padded, contact with entire plantar surface and lower leg
Compression and pressure relief
Pressure transferred from forefoot to the cast walls and rear foot
Forces compliance
Armstrong, D. and Stacpoole-Shea, S. 1999. Total contact casts and removable cast walkers: mitigation of plantar heel pressure.
JAPMA, (89), pp 50-53.

Charcot Neuroarthropathy
• Is a rapid destructive arthropathy associated with peripheral neuropathy.
• Long standing diabetes is the most common cause (Approx 15%).
• The foot is the most common site.
• Other predisposing conditions include
Alcoholism Spinal Cord lesions Other Any condition that involves a
degeneration of sensory, motor and autonomic nerve function
• Aetiology is unclear.

Charcot Neuroarthropathy
Suggested aetiology:
Autonomic neuropathy increases blood flow to the extremity and bones, resulting in osteopenia amking it more prone to fractures
Motor neuropathy results in muscle imbalance
Sensory neuropathy means that patient in unaware of the osseous destruction that is taking place
Armstrong DG, Todd WF, Lavery LA, Harkless LB, Bushman TR (1997). The Natural Histroy of Acute Charcot’s Arthropathy in a Diabetic Foot Specialty
Clinic. Diabetic Medicine, 14 pp 357-363.

Charcot Neuroarthropathy
• Acute
Aim – Maintain normal foot structure
Off load
- TCC
- Air cast
- Crutches, compliance??
• Chronic
Hopefully no deformity
Orthosis
Custom made footwear
Management

Case Study Eight 75 yo male with type 2 diabetes referred to podiatry department by
GP
Seven years ago client fell off a ladder and was diagnosed simply with a foot fracture
Since this time, his foot has progressively changed shape into a rocker-bottom foot type
Until his podiatry appointment, no diagnosis of Charcot Neuroarthropathy was ever made
No medical intervention was initiated during the acute phase

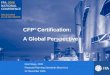
Footwear
Protects feet and skin integrity
Can be …
Off-the-shelf
Medical grade
Custom made
Orthoses / accommodative insoles are important in patients with biomechanical abnormalities to prevent ulceration

Footwear
All footwear should have the following features…
1. Fastenings
2. A firm heel counter
3. Heel height of less than 2cm
4. A firm sole
5. A wide and deep toe-box
6. One thumbs-width from the longest toe to the end of the shoe
7. Preferably a leather upper and lining