Embed Size (px)
Citation preview

1
Kelly Kasteel
Tylenol Toxicity

2
OBJECTIVES
• Tylenol toxicity :a) Epidemiologyb) Dosingc) Metabolismd) Diagnosise) Treatmentf) Prognosis

3

4
Epidemiology
Tylenol- A name by many others Acephen™ [OTC]; Apra Children's [OTC]; Aspirin Free Anacin® Maximum Strength [OTC]; Cetafen Extra® [OTC]; Cetafen® [OTC]; Comtrex® Sore Throat Maximum Strength [OTC]; FeverALL® [OTC]; Genapap™ Children [OTC]; Genapap™ Extra Strength [OTC]; Genapap™ Infant [OTC]; Genapap™ [OTC]; Genebs Extra Strength [OTC]; Genebs [OTC]; Infantaire [OTC]; Mapap Children's [OTC]; Mapap Extra Strength [OTC]; Mapap Infants [OTC]; Mapap [OTC]; Nortemp Children's [OTC]; Pain Eze [OTC]; Silapap® Children's [OTC]; Silapap® Infants [OTC]; Tycolene Maximum Strength [OTC]; Tycolene [OTC]; Tylenol® 8 Hour [OTC]; Tylenol® Arthritis Pain [OTC]; Tylenol® Children's with Flavor Creator [OTC]; Tylenol® Children's [OTC]; Tylenol® Extra Strength [OTC]; Tylenol® Infants [OTC]; Tylenol® Junior [OTC]; Tylenol® [OTC]; Valorin Extra [OTC]; Valorin [OTC] .
Most popular OTC analgesic in North America
Lay people commonly underestimate its toxicity

5
Epidemiology
intentional (suicidal)=unintentional (chronic) poisonings
Tylenol is often thought to be benign, or is a “hidden ingredient” in other remedies.
Accounts for more overdoses and overdose deaths each year in North America than any other pharmaceutical agent In 2000, it accounted for 5% of overdoses and
23% of reported fatalities.5
6
Dosing “Plain Tylenol”:
1. Regular-strength:325mg
2. Extra-strength:500mg
Pediatric syrup 1. 160 mg/5 mL –Childrens 2. 80 mg/0.8 mL -Infants
Other Tylenol formats include:a) tabletsb) chew-tabsc) dissolvabled) capsulese) suppositories

7
Tylenol is also available as a co-ingredient in several combination medications:
Dosing
1. Tylenol #3 (Tylenol 300 and Codeine 30mg)
2. Percocet (Tylenol 300mg and Oxycodone 2.5/5/7.5mg)

8
Dosing
Recommended Tylenol dosing is as follows: Adult: 325-650 mg every 4-6 hours or 1000 mg
3-4 times/day; do not exceed 4 g/day. 2.5mg in liver failure ( defined as
Peds: 10-15 mg/kg/dose every 4-6 hours as needed; do not exceed 5 doses (80mg/kg) in 24 hours

9
The minimum toxic dose for an acute ingestion of Tylenol (ie. occurring within a time frame of four hours) is:
a) Adults: 7.5gb) Peds: 150mg/kg
It may be prudent to also use these levels as the minimum acute toxic dose per 24 hours.
Ingestions occurring over a period of more than four hours are arbitrarily termed chronic ingestions.
Acute Toxic Dosing

10
The minimum toxic dose for chronic ingestions of Tylenol is less well defined.
Rosen’s suggests:4
a) Adults: > 4g/d if risk factors **
> 7.5g/d if no risk factorsb) Peds: > 75 mg/kg/d if risk factors
> 150mg/kg/d if no risk factors
** - Risk factors will be discussed later
Chronic Toxic Dosing

11
Metabolism
Immediate-release Tylenol is rapidly absorbed in the gut, with peak serum levels typically achieved in 30m – 2hr
Peak serum levels can be delayed…1. With sustained-release formulations.2. With combination formulations.3. In overdoses.
a) peak levels not being achieved for up to 4hrs following overdoses of immediate-release Tylenol.
b) peaks even >4hrs following OD’s of extended-release Tylenol.2

12
Metabolism
Okay… time to make learning fun. Who hasn’t memorized and forgotten the
pathways of Tylenol metabolism at least five times? Well… here’s number six.
Under normal circumstances, Tylenol is metabolized in the following manner:

13
Tylenol
Sulfation
Glucuronidation
5%
20-45%
40-65%
Remaining 5-15%
NAPQI
Cyt P450
Tylenol –mercaptate compound
NORMAL TYLENOL METABOLISM
Oxidation
Glutathione

14
Tylenol
Sulfation
Glucuronidation
5%
20-45%
40-65%
Remaining 5-15%
NAPQI
Cyt P450
Tylenol –mercaptate compound
NORMAL TYLENOL METABOLISM
Oxidation
Glutathione

15
Tylenol
Sulfation
Glucuronidation
5%
20-45%
40-65%
NAPQI
Cyt P450
Glutathione
TYLENOL METABOLISM IN OVERDOSE
Oxidation
SATURATED
SATURATED
SATURATED
Tylenol -mercaptatecompound
Remaining 5-15%
>>> 5- 15%
Tylenol
Glutathione
NAPQI
Oxidation
Cyt P450

16
Risk Factors for Tylenol Toxicity An obvious corollary of the previous slide is
that anything which potentiates the action of Cyt P450 will accelerate the production of NAPQI.
(And vice-versa.)

17
Risk Factors
1. Chronic alcohol consumption2. Anticonvulsants:
Tegretol Dilantin Phenobarb
3. Anti-tuberculosis medications: Rifampin INH
4. Dexamethasone5. St. John’s Wort
Cyt P450 Potentiators ( NAPQI):
18
(Not) Risk Factors
1. Acute alcohol consumption2. Macrolides
• Erythromycin, Biaxin, Zithromax
3. Antifungals4. Amiodarone5. HIV protease-inhibitors6. Cyclosporine7. Grapefruit juice
Cyt P450 Inhibitors ( NAPQI):

19
Quick note on the sauce… As you can see, if you are going to overdose
on Tylenol, at least have the good sense to wash it down with some Scotch.
Chronic EtOH use, on the other hand, will (at least, theoretically) increase the risk of sequelae in Tylenol OD:
1. Cyt P450 is potentiated.2. Alcoholics tend to have low pre-existing levels
of glutathione.

20
Quick note on the sauce… In practice, alcoholics tend not to be at
increased risk for hepatotoxicity following an acute overdose of Tylenol.
Practice matches theory more closely, however, in alcoholics with chronic Tylenol overdoses.
Even so, these pts are still unlikely to develop toxicity if they restrict their Tylenol use to <4g/d.

21
More Risk Factors Anything that slows down or interferes with
sulfation and/or glucouronidation will leave more Tylenol available for Cyt P450 processing (and NAPQI production).
1. Septra and AZT are metabolized via glucouronidation (and may slow this pathway down for Tylenol).
2. Patients with Gilbert’s disease may have decreased glucouronidation.
3. Elderly patients may have decreased rates of sulfation and/or glucouronidation.

22
More Risk Factors Anything that decreases the amount of
glutathione in the body leaves less of it available to bind to NAPQI.
1. Chronically malnourished or acutely fasting patients may have decreased glutathione stores.
Febrile pediatric patients are especially susceptible to falling into the latter group.
2. Elderly patients can have chronically decreased glutathione stores.
23
Summary of Risk Factors 1. Induced Cyt-P4502. Chronic alcoholism3. Acute fasting (may include febrile peds)
4. Chronic malnutrition5. Septra or AZT use6. Gilbert’s disease7. Elderly patients

24
1. Elderly patient.
6. Gilbert’s disease.
5. Septra is making her vomit…
4. On Septra for bladder infection.
2. Fallen off wagon.
3. On INH for TB.
Pictorial Summary of Risk Factors
so she’s not eating.

25
Treatment (For reasons that I hope will later become
obvious), I will now break with tradition and discuss treatment before diagnosis.

26
Clinical Stages• In untreated patients, there are four
clinical stages of Tylenol toxicity:
1. Stage One (0-24hrs)• minimal clinical findings.• may be completely asymptomatic.• may have minor non-specific
findings such as N/V, pallor, malaise.
• liver panel unremarkable.
27
2. Stage Two (Day 2-3)• clinical signs of hepatotoxicity.• RUQ pain, hepatomegaly,
AST/ALT/bili/PT/lipase elevation.
Clinical Stages
• In untreated patients, there are four clinical stages of Tylenol toxicity:
Most sensitive
• patients may also develop early signs of renal failure or pancreatitis during this stage.

28
2. Stage Two continued…• From Stage 2, patients progress
either to Stage 4 (with subsequent full recovery) or to Stage 3 (with subsequent probable death).
Clinical Stages
• In untreated patients, there are four clinical stages of Tylenol toxicity:

29
Clinical Stages
3. Stage Three (Day 3-4)• Fulminant hepatic failure +/- death• Associated lactic acidosis, coag-
ulopathy, encephalopathy; possible pancreatitis, hypoglycemia, ARF.
• Marked elevation of liver enzymes (with AST typically >3,000),
• Elevation of NH3, coags, lactate.
• In untreated patients, there are four clinical stages of Tylenol toxicity:
30
Clinical Stages
3. Stage Three continued…
• In untreated patients, there are four clinical stages of Tylenol toxicity:
• Stage 3 will progress to:(a)death.(b)if lucky, a liver transplant.(c) if even luckier, Stage 4 and a full
recovery.

31
Clinical Stages
4. Stage Four (Day 4 - 10)• If you do not die in Stage 3, you
arrive at Stage 4 with rapid and complete hepatic recovery.
• Clinical recovery usually begins by Day 4 and is complete by Day 7-10.
• Histological recovery may take up to 3 months.
• In untreated patients, there are four clinical stages of Tylenol toxicity:
32
Clinical Stages
• Summary of stages: Days:1. Minimal symptoms 12. Moderate symptoms 2-33. Severe symptoms +/- death 3-4 4. Complete recovery 4-10
• In untreated patients, there are four clinical stages of Tylenol toxicity:
33
Treatment The treatment for Tylenol toxicity is N-
acetylcysteine, or NAC. Early on in Tylenol toxicity, NAC:
1. Acts as a glutathione precursor, increasing glutathione stores.
2. Binds NAPQI directly.3. Enhances the sulfation pathway.

34
Treatment Later on in Tylenol toxicity…
(when Tylenol levels are absent, but hepatotoxicity has begun)…NAC continues to offer benefit:
1. It has strong antiinflammatory effects.2. It has strong antioxidant effects.3. It scavenges free radicals.4. It modifies cytokine production.5. It increases inotropy and vasodilation, thereby
improving microcirculation.

35
Treatment So how well does NAC work? Pretty bloody well. If NAC is initiated within 8 hours of (even a
massive) acute Tylenol overdose, the patient:
1. Is very unlikely to suffer (even transient) serious hepatotoxicity.
2. Essentially never dies from the overdose Beyond the 8-hour point, NAC’s protective
abilities steadily diminish.

36
Treatment But NAC continues to provide significant
benefit even if initiated quite late in Tylenol toxicity:
In a 1991 trial in the BMJ, 50 patients presenting with Tylenol-induced fulminant liver failure were randomized to either: (a) NAC (b) Supportive care
NAC patients had significantly less:1. mortality (20% vs. 48%)2. cerebral edema (40% vs. 68%)3. need for inotropes (48% vs. 80%)

37
Diagnosis

38
Diagnosis• The diagnosis of a disease (as any
medical student will tell you) begins with history.
• Sadly, with Tylenol toxicity, history can sometimes be a bit of a problem.

39
Diagnosis Patients coming to
the ED with a Tylenol overdose dose are not, strictly speaking, the most reliable of historians.
• So you really have to rely on something else.

40
Diagnosis As such, the diagnosis of Tylenol toxicity
rests on:1. Tylenol levels2. AST/ALT (and other bloodwork) levels3. The Rumack-Matthew nomogram.
The “other bloodwork” to consider drawing in Tylenol toxicity includes:
1. PT, BUN/Cr, glucose, lipase, CK2. Medication levels (eg. ASA, EtOH, etc.)

41
Cost of Diagnosis In a 1989 study in the Annals of Emergency
Medicine, 1 in 500 patients who presented to the ED with an overdose—but denied Tylenol ingestion—was found to have a potentially toxic level.5
Tintinalli estimates that the cost of drawing 500 negative Tylenol levels is less than the cost of missing one case of Tylenol-induced hepatic failure.5

42
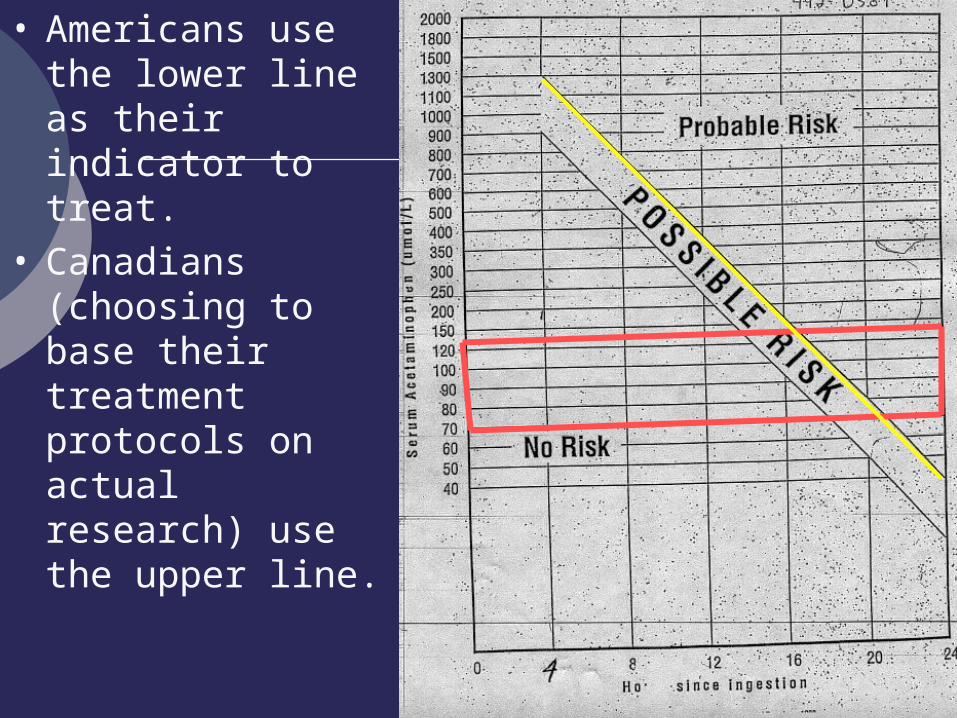
• This is the Cdn units (umol/L) version of the Rumack-Matthew nomogram.
• Therapeutic Tylenol levels are 70-130 umol/L.
Rumack-Matthew
Nomogram
• Note that the y-axis is logarithmic.

43
• “Tylenol levels” on the y-axis range from 0 – 2000.
• “Time since ingestion” on the x-axis ranges from 0 – 24 hours.
• Toxicity cannot be predicted before 4hrs or after 24hrs using this nomogram.

44
• The nomogram is based on a study of a large number of patients who following an acute OD of immediate-release Tylenol were not treated with antidote.2
• Note that there are two diagonal lines indicating potential toxicity.

45
• The original nomogram used just one line – the upper line.
• Following an acute ingestion of immediate-release Tylenol, no patients with a Tylenol level below the upper line…
• developed severe hepatotoxicity or died.

46
• The U.S. FDA later developed a second line—the lower line—to offer an increased safety margin.
• Presumably to cover those patients with risk factors for Tylenol toxicity.
47
• Americans use the lower line as their indicator to treat.
• Canadians (choosing to base their treatment protocols on actual research) use the upper line.

48
• To use the nomogram…
• Wait until at least four hours after ingestion of an acute OD of immediate-release Tylenol
• (This 4hr waiting period ensures that serum levels have peaked.)
• Then simply draw and plot the Tylenol level.

49
• N.B. It is safe to wait for 4hrs before drawing the first Tylenol level.
• This is because the risk of Tylenol toxicity (following an acute OD) is essentially zero as long as NAC is initiated within 8hrs of ingestion.

50
• Plot points below the upper-line represent:• negligible risk
of significant hepatotoxicity
• essentially no risk of long-term morbidity or mortality.
• And, thus, no need for treatment.

51
• Plot points above the upper-line represent…
1. 60% chance of AST > 1000
2. 1% chance of renal failure
3. 5% chance of mortality
• And, thus, the need for treatment.

52
• So… draw your level, plot your point, start your NAC.
• Piece of cake right?
• Well… mayhab, mayhab no.

53
Diagnosis
1. What about chronic or multiple ingestions?2. What if the time of acute ingestion is not firmly
established?3. What if the pt is lying to you?
5. What about sustained-release Tylenol?
#
4. What if the acute ingestion was <4 or >24 hours ago?
There are some potential problems with the Rumack-Matthew nomogram.

54
Diagnosis1. What about chronic or multiple ingestions?
It is generally accepted that the nomogram is not reliable in this situation.
Tylenol levels could potentially be therapeutic (or, for that matter, undetectable) even in the face of significant hepatotoxicity.

55
Diagnosis2. What if the time of acute ingestion is not
firmly established? In this instance (since the actual time of
ingestion may well be >8hrs ago), one would be wise to draw a Tylenol level at once and initiate NAC immediately.
This is especially true for patients who have RUQ pain, are jaundiced, or look ill.
When the Tylenol (and other bloodwork) levels come back, one can decide whether or not to continue therapy.

56
Diagnosis3. What if the pt is lying to you?
If you have these, then feel free to trust all your patients and follow the nomogram.
– If you are not quite as trusting, then draw a Tylenol level at once and and initiate NAC immediately.
– At least one conscientious, young (and handsome) physician I know recommends trusting no one.

57
Diagnosis4. What if the ingestion was < 4 or >24 hours
ago? As already mentioned, the nomogram is
unreliable outside of these timeframes.a) If <4hrs from time of ingestion, Tylenol levels may
still be increasing.b) If >24hrs from time of ingestion, Tylenol levels may
be undetectable, even in the face of significant hepatotoxicity.

58
Diagnosis5. What about sustained-release Tylenol?
There is not currently sufficient evidence to validate (or invalidate) the nomogram for use with sustained-release Tylenol.2
Which is not to say we don’t do use it. In something of an “off-label” use of the
nomogram, manufacturers of sustained-release Tylenol recommend…
“draw both a 4- and 8-hour Tylenol level, and initiate NAC if either level is potentially toxic.”

59
And now… a return to Treatment

60
Treatment In the ED, the most difficult question to
answer is not which therapy to use (psst… use
NAC), but whether or not therapy is actually required.
And this question will have to be answered at least twice:
(a) Once before the bloodwork is back.(b) Once after the bloodwork is back.

61
Treatment And—both times—one will need to consider
whether there is grounds for clinical suspicion of Tylenol toxicity:
1. Hx of ingestion suggestive of toxicity.
a) acute overdose (eg. >7.5g or >150mg/kg).
b) chronic supratherapeutic use (>4g/d or
>75mg/kg).
c) chronic therapeutic use in a patient with risk factors.
d) chronic use or overuse of sustained-release or combined-ingredient Tylenol.

62
Treatment
2. Hx of ingestion that is not suggestive of toxicity, but sounds like it is:a) inconsistent.b) incomplete.c) a big fat lie.
And—both times—one will need to consider whether there is grounds for clinical suspicion of Tylenol toxicity:

63
Treatment
3. Clinical findings suspicious of Tylenol toxicity:a) RUQ pain
b) jaundicec) N/Vd) lethargy and malaisee) dehydration
And—both times—one will need to consider whether there is grounds for clinical suspicion of Tylenol toxicity:

64
Treatment In summary, be clinically suspicious of
Tylenol toxicity if:1. History sounds bad.2. History sounds like bullshit.3. Clinical findings.

65
Treatment So back to the original question:
When is therapy warranted?

66
Treatment before bloodwork Before bloodwork is back, initiate NAC if:
1. Clinical suspicion of Tylenol toxicity. Some will argue that if the bloodwork will be back
within 8 hours of the time of ingestion, that you do not need to initiate empiric therapy.
And, strictly speaking, this is true. So, by all means…

67
Treatment before bloodwork …if your patient took an acute dose of
immediate-release Tylenol at an exact and known time, has no risk factors, and is not potentially lying to you, then go ahead and wait for the bloodwork to come back.
#

68
Treatment after bloodwork After bloodwork is back, initiate and/or
continue NAC if:1. Nomogram indicates probable toxicity.2. In the setting of a unreliable nomogram you
have:a) clinical suspicion of toxicity and Tylenol levels are
even detectable.b) clinical suspicion of toxicity with undetectable
Tylenol levels, but AST or other bloodwork is abnormal.

69
Treatment after bloodwork What if you still have clinical suspicion of toxicity when all your bloodwork is back and it is all completely normal?
Chances are, you worry too much. Theoretically (although I never saw this documented
anywhere), I suppose there could be a window right around the 24-hr mark where Tylenol levels were undetect-able but the AST had not yet begun to rise.
I would have to have some overwhelming clinical suspicion of Tylenol toxicity before I investigated this scenario further.

70
Treatment Protocols For uncomplicated Tylenol overdose, there
are two types of NAC protocols:1. Oral NAC
A 72-hour course of therapy. 18 total doses (q4h dosing). Total dose = 1330mg/kg of NAC.
2. IV NAC1. A 20-hour course of therapy.2. Continuous IV infusion.3. Total dose = 300mg/kg of NAC.
#

71
Treatment Protocols For Tylenol overdose complicated by liver-
failure, IV NAC is used but the infusion is not stopped at 20 hours.
Instead, the NAC is continued until the patient:
1. Fully recovers.2. Dies.3. Receives a liver transplant.

72
– This is the U. of A. nursing protocol for IV NAC in uncomplicated Tylenol toxicity.
– (N.B. NAC concentration = 200mg/mL)

73
Comparing Treatment Protocols1. Oral NAC
– method of choice in the U.S.
2. IV NAC– method of choice in Canada.– typically better tolerated.– major limitation is rate-related IV reactions
(discussed next slide), which are typically non-serious and easily controlled.

74
Comparing Treatment Protocols
1. Reported frequency is 0.2 – 21%2. Reported rxns (in order of increasing
severity and decreasing frequency): nausea/flushing/chills/fever urticarial rash/hypotension bronchospasm/angioedema hemolysis cardiovascular collapse
• Adverse reactions with IV NAC:

75
Comparing Treatment Protocols
3. These IV-related reactions: are dose- and rate-dependent usually occur in the first hour of Rx are usually easily controlled with:
a) temporarily stopping the IV.b) treating with antihistamines.c) re-starting the IV at a (temporarily) lower-rate.
• Adverse reactions with IV NAC:

76
Comparing Treatment Protocols
4. Continuation of IV therapy is the rule in all but life-threatening scenarios.
• Adverse reactions with IV NAC:

77
Comparing Treatment Protocols Effectiveness of IV vs. oral NAC.
1. In an uncomplicated Tylenol overdose at <8hrs, IV NAC is as effective as oral.
2. In an uncomplicated Tylenol overdose at >8hrs, oral NAC may be superior to IV.
Possibly secondary to the increased amount and duration of oral NAC.
3. In Tylenol-induced fulminant liver failure, only IV protocols have ever been formally used and studied.

78
Comparing Treatment Protocols4. Tylenol toxicity in pregnancy has not been
rigorously studied, but IV NAC is typically recommended:
a) Fetal Tylenol toxicity is rare, but has been reported at all stages of pregnancy.
b) IV NAC is safe and effective in mom.c) Higher serum levels obtained with IV NAC (by
avoiding hepatic first-pass metabolism in mom) may translate into higher serum levels in the fetus.
d) Exact treatment guidelines are controversial, and require toxicological and/or obstetrical consultation.

79
Prognosis

80
Prognosis Although AST is the most sensitive marker
for Tylenol-induced liver damage, it is a poor prognosticator.
Two large studies (>500 patients each)1 established markers for prognosis in hepatic failure.
Patients with poor prognostic markers can be evaluated to see if they are eligible for liver transplantation.

81
Prognosis Following Tylenol-induced fulminant liver
failure, patients are eligible for liver transplantation if:**
1. Arterial pH < 7.30 (following fluid resuscitation)
2. They have all three of the following:a) > Grade 3 encephalopathy b) INR > 6c) Cr > 300-310
OR
** Cdn adaptation of the King’s College Hospital criteria.

82
Prognosis Patients who meet these criteria and:
a) Get a liver transplant… have a 66% one-year survival rate.
b) Do not get a liver transplant… have a 80-90% mortality rate.

83
In summary…

84
Idiot’s Guide to Tylenol Toxicity1. Patient presents with possible Tylenol
toxicity.2. Unless all of the following apply (in which
case you can wait until 4hrs post-ingestion) immediately draw and send:
a) Tylenol levelsb) AST, PTc) lytes, BUN/Cr, glucosed) urine for pregnancy testing (women only)

85
Idiot’s Guide to Tylenol Toxicity3. While the bloodwork is pending, if you are
clinically suspicious of potential toxicity, start NAC.
4. When bloodwork is back, if the nomogram can be used, plot the Tylenol level and treat as indicated.
5. When bloodwork is back, if the nomogram cannot be used, rely on combination of bloodwork and clinical suspicion to determine need for NAC.

86
Idiot’s Guide to Tylenol Toxicity6. If there is yet no indication to treat, consider
the possibility that Tylenol levels may still be rising:
a) additional Tylenol may have been ingested just before arrival at ED.
b) sustained-release and/or comb-ination Tylenol may have delayed absorption kinetics in overdose.
If these apply, draw another set of Tylenol levels and bloodwork in 4hrs time, and use these to guide your therapy decisions.

87
Idiot’s Guide to Tylenol Toxicity
7. Patients requiring treatment with NAC will also require:
monitoring for hepatic or renal failure. Internal Medicine/Hepatology/ICU
consultation if hepatic failure develops Obstetrics/Toxicology consultation if patient
is pregnant. Psychiatric consultation if overdose
represented a suicide attempt.

88
Final Points to Discuss1. NAC within the first 24hrs… no one dies?
True?2. Charcoal? What do you think?

89
That’s all folks…

90
?

91
References1. Burns, Ismail, et al. UpToDate Online 12.2.
“Management of acetaminophen (paracetamol) intoxication.” April 2004.
2. Burns, Ismail, et al. UpToDate Online 12.2. “Pathophysiology and diagnosis of acetaminophen (paracetamol) intoxication.” April 2004.
3. Canadian Pharmacist’s Association. CPS. 2002. p1751-53
4. Marx, Hockberger, et al. Rosen’s Emergency Medicine. 5th Edition. p2069-74.
5. Tintinalli, Kelen, et al. Emergency Medicine. 6th Edition. p1088-93.
92
THE END
93
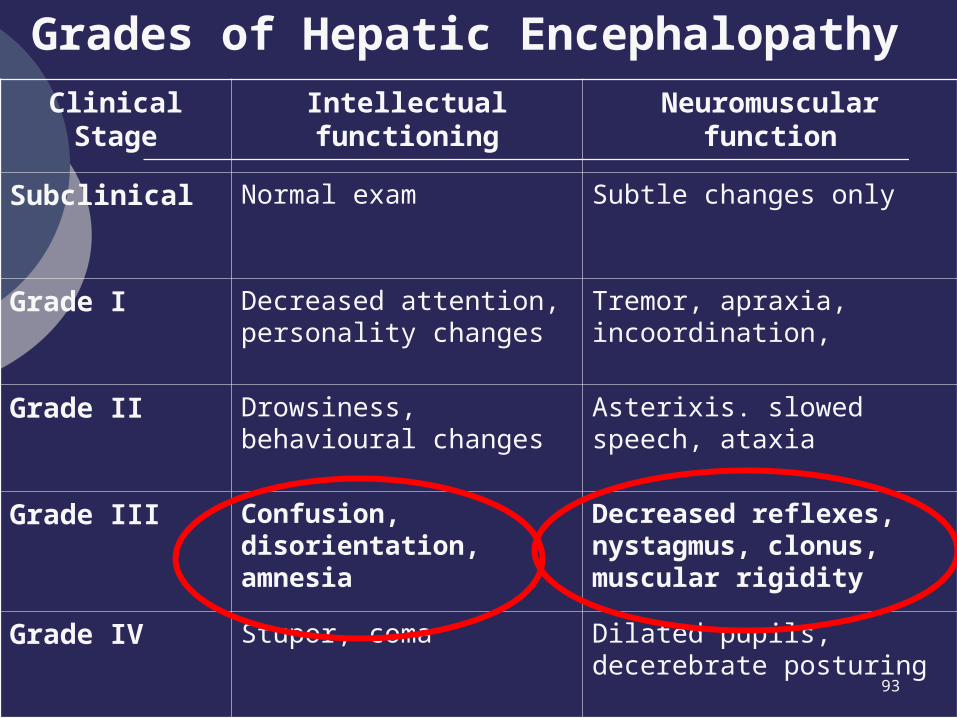
Grades of Hepatic Encephalopathy Clinical Stage
Intellectual functioning
Neuromuscular function
Subclinical Normal exam Subtle changes only
Grade I Decreased attention, personality changes
Tremor, apraxia, incoordination,
Grade II Drowsiness, behavioural changes
Asterixis. slowed speech, ataxia
Grade III Confusion, disorientation, amnesia
Decreased reflexes, nystagmus, clonus, muscular rigidity
Grade IV Stupor, coma Dilated pupils, decerebrate posturing

94