-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
1/119
ESOPHAGUS AND STOMACH
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
2/119
Review Polyp: Any bump on the gut that sticks up above the inner
surface into the lumen.
Hernia: Presence of a portion of an organ in a body space where
it doesn't belong. Incarcerated hernia: One that can't be reduced,
i.e., put back in its proper place.
Strangulated hernia: Where venous drainage is compromised and
infarction is
imminent / present.
Erosion: A portion of the epithelium mucosa has been lost due to
necrosis, butthere has been no lossofthe underlying connective
tissue. In the stomach, as theterm is generally used, there may be
loss of some connective tissue but sparing themuscularis
mucosae.
Ulcer: A portion of the epithelium andsome ofthe underlying
connective tissuehas been lost due to necrosis. In the stomach, an
"ulcer" is typically diagnosed onlyif the muscularis mucosae is
lost.
Diverticulum: An outpouching ofall the layersof the wall of a
hollow organ.
Pseudo-diverticulum: Outpouching ofmucosa through a defect in
the muscularispropria.
Paracrine / endocrine cells ("enterochromaffin, formerly "APUD"
cells) are foundindividually all along the gut, and various ones
produce various peptide hormonesof known and unknown
significance.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
3/119
Strangulated umbilical hernia
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
4/119
Review Reflux leads to fibrosis (scarring, shortening, perhaps
narrowing) of
the esophagus, difficulty on swallowing ("dysphagia"), pain
inswallowing ("odynophagia"), retrosternal pain ("heartburn")
and/orslow GI bleeding leading to iron-deficiency. In severe cases,
massiveGI bleeding (hematemesis, melena) can occur.
Other noteworthy causes of esophagitis include candida, CMV,
herpes, radiation, generalized diseases of stratified
squamousepithelium or keeping a stomach tube down for more than a
fewminutes. All the above can give some nasty ulcers.
You also remember the esophageal changes ("rubber hose")
inscleroderma.
Drinking lye or some other caustic substance leads to
corrosiveesophagitis, strictures, etc., etc.
The common cancers of the GI tract are carcinomas. Often the
firstphysical finding is Virchow's sentinel lymph node, where the
thoracicduct joins the left internal jugular vein.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
5/119
Norma
gastroesophageal
junction
This is a normal esophagus with the usual white to tan
smooth mucosa seen at the left. The gastroesophageal
junction (not an anatomic sphincter) is at the center,and the
stomach is at the right. The upper GI
endoscopic view of the transition from tan squamous
mucosa to pink columnar mucosa is seen to the right.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
6/119
normal esophageal squamous mucosa
This is normal esophageal squamous mucosa at the left, with
underlying submucosa containing mucus glands and a duct
surrounded by lymphoid tissue. The muscularis is at the
right.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
7/119
Candida Esophagitis
Left: In this necrotic debris, non-branching pseudohyphae and
blastocysts arepresent.
Right: Multiple yellow plaques in the midesophagus are shown. In
some areas, theplaque material becomes confluent. The surrounding
uninvolved mucosa is normalwith a normal vascular pattern.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
8/119
Candida esophagitis
*Scrapes off,
unlike glycogen
acanthosis*
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
9/119
Candida esophagitis
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
10/119
Herpetic Esophagus
Left: Multiple well-circumscribed ulcers in the midesophagus are
shown. Some
of the ulcers have become confluent, resulting in serpiginous
shallowulcerations. The intervening mucosa is normal.
Right: The squamous epithelial cells exhibit multinucleation and
prominentintranuclear inclusions. The inclusions have a mauve
'ground glass' appearance.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
11/119
Herpes of the esophagus
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
12/119
herpes simplex
The lower esophagus here shows
sharply demarcated ulcerations that
have a brown-red base, contrasted
with the normal pale white
esophageal mucosa at the far left.Such "punched out" ulcers
are
suggestive of herpes simplex
infection.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
13/119
Cytomegalovirus Infection
of Esophagus
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
14/119
ESOPHAGUS
The "gullet" begins at the cricophagyngeus (the short "upper
esophagealsphincter" starts here) and ends at the diaphragmatic
hiatus orthereabouts ("lower esophageal sphincter").
Solid food may hang up at either site, or where the esophagus
passesbehind the left main-stem bronchus or between enlarged hilar
nodes.N
either sphincter is fool-proof (or even anatomic). Considerable
coordination is required for a proper swallow (the big word
for "swallowing" is "deglutition"). Most of the time, the
esophagusperforms its simple but important task well.
You remember that the upper esophagus (i.e., the first inch or
so) hasmostly skeletal muscle (and is thus subject to diseases of
nerve andskeletal muscle), the middle esophagus (i.e., maybe
another inch) has bothskeletal and smooth muscle, and the distal
esophagus (i.e., most of theesophagus) has mostly smooth
muscle.
Unlike most of the rest of the gut, the esophagus has noserosa
to helplimit the spreadofripsor cancers.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
15/119
Esophagus Birth Defects
Agenesis of some or all of the esophagus isuncommon.
Atresia of the esophagus, as elsewhere, is
failure of a normally-hollow organ to developits lumen. An
atretic esophagus is represented, over part or
all of its length, by a fibromuscular cord without alumen. Less
severely, portions of the esophagusmay be congenitally stenotic
(i.e., too narrow).
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
16/119
Atresia
The diagnosis of esophageal atresia is
suspected when, in the presence of
polyhydramnios (usually after 25 weeks),
repeated ultrasonographic examinations fail to
demonstrate the fetal stomach.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
17/119
Esophagus Birth Defects
Tracheo-esophageal fistulas of severalvarieties are common
neonatal surgicalproblems.
The proximal esophagus may enter the trachea orbronchus,
producing coughing upon feeding.
The proximal esophagus may end blindly and thedistal esophagus
arise from a large airway,preventing feeding and causing the
stomach to fill
with air (the most common version). Or there may simply be a
window between the
two organs.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
18/119
Tracheo-esophageal
fistulas Left: The probe enters the
larynx and trachea andpasses through the fistula tothe
esophagus.
Right: Barium of fistula
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
19/119
Globus hystericus ("globus syndrome",
"globus pharyngeus")
A "lump in the throat", is spasm of the back of thethroat and
perhaps the upper esophagus.
It creates the feeling of a mass in the hypopharynx.Sometimes
the cause is organic (i.e., a reflex fromsomething wrong nearby,
perhaps reflux from theesophagus spilling into the larynx); often
it'spsychosomatic.
Psychiatrists attribute it to "swallowed tears", and
the cure is to cry. (D
espite its banal nature, thesensation of a mass may frighten a
patient.Spontaneous cures of non-biopsy-proven throatcancer" sound
like globus.)
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
20/119
Zenker's "pulsion" diverticulum
Adjacent to the cricophagyngeus muscle. A
hiding-place for last week's spaghetti and last
month's pills (so that's why they didn't work....)
The smell alone may create a serious social
problem.
A Zenker's can be a true or pseudodiverticulum
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
21/119
Zenker's "pulsion"
diverticulum
Left: The diverticulum is on theright and the true
esophageallumen is on the left. They areseparated by a "bridge"
oftissue.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
22/119
Zenkers pulsion diverticulum
*Adjacent to the cricophagyngeus muscle;
can be a true or pseudodiverticulum.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
23/119
Achalasia
Means "failure of a sphincter to relax when it should".U
sually, this meansthe lower esophageal sphincter.
In the U.S., the problem is usually idiopathic failure of the
lower sphincterto relax. The cause is usually inflammation of the
myenteric plexus, witheventual nerve damage, but nobody knows why
this happens. In othercases, the ganglion cells are simply lost
instead.
The esophagus remains filled with food. The patient (typically a
youngadult) will notice regurgitation and bad breath. The situation
may becomereally nasty as more and more food accumulates in a
mega-esophagus.Fortunately, most patients are cured by a single
endoscopic dilatation ofthe sphincter; there's also "botox", or
laparoscopic myotomy and partialfundoplication for the hard
cases
Untreated, achalasia is a life-threatening problem (carcinoma,
aspiration
pneumonia). You remember that Chagas' disease (T. cruzi) is an
important cause of
mega-esophagus worldwide.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
24/119
Esophageal Achalasia Failure of a sphincter to relax when it
should, usually the lower
Usually caused by inflammation of the Myenteric plexus
Can be treated with botox
Birds beak sign on barium swallow
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
25/119
Achalasia
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
26/119
Glycogen plaques
These are acanthotic (i.e., thick spiny layer)
epithelium with extra glycogen.
The most common lesion of the esophagus, byfar, and exactly as
serious as freckles.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
27/119
Webs
These are contracted, localized fibrous scars thatform little
shelves ("ledges") that may obstruct thelumen.
They are most common in the upper esophagus, andmost common in
women. Their etiology is usually
obscure; some are congenital, some result fromreflux,
graft-vs-host disease, and pemphigus.
No one knows quite what to make of a supposedassociation between
upper esophageal webs, irondeficiency anemia, and a risk for
squamous cellcarcinoma in the proximal esophagus. Whether ornot
this really exists, it's called "Plummer-Vinson
syndrome Shown Right.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
28/119
Schatzki's ring
This is a washer-shaped partially-obstructing fibrous ring atthe
squamo-columnar junctionjust above thegastroesophageal junction. It
is a radiologist's delight and maybe seen in any adult; long a
mystery, cases that occur in the
absence of reflux may be due to pill enlodgement. A-ring is the
same, at the gastro-esophageal junction.
A big chunk of solid food (i.e., poorly-chewed beef) may hangup
on a web or ring. In bad cases, softer food may havetrouble
negotiating the obstruction.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
29/119
Schatzkis ring
A washer-shaped partially-obstructing fibrous ring at
thesquamo-columnar junction just above the
gastroesophagealjunction
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
30/119
Schatzki's ring
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
31/119
Hiatus hernia
This is said to be present whenever a portion
of the stomach pooches up through the
diaphragmatic hiatus.
Present in up to 10% of adults (typically the
overweight), they are most often sub-clinical.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
32/119
Hiatus hernia The stomach herniates
upwards into theoesophagus
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
33/119
Sliding hiatus hernia
A sliding hiatus hernia (the usual kind) is presentwhen a short
esophagus (congenital, fibrous scarringfrom years of reflux,
diaphragm pulled low byobesity) pulls the proximal stomach into the
chest.
As the esophagus contracts during swallowing,radiologists watch
the stomach slide further upthrough the diaphragm.
As with "reflux esophagitis", the distal esophagus is
likely to become inflamed and damaged as a result ofexposure to
pepsin and acid.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
34/119
Para-esophageal ("rolling") hiatus hernia
Para-esophageal ("rolling") hiatus hernia (the lesscommon kind)
is present when a portion of thestomach rolls up through the
diaphragm alongside anesophagusofnormal length.
This is typically a non-problem, but the herniatedportion of
stomach may become strangulated.
Future pathologists: Don't expect to see either type
of hernia (or, for that matter, a Schatzki's ring, or
anintestinal hernia) after death, when the muscles ofthe body relax
/ go into rigor mortis.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
35/119
Para-esophageal
("rolling") hiatushernia
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
36/119
Traction diverticula
These probably result from scar contraction in
the mediastinum (i.e., TB).
They are uncommon.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
37/119
Traction diverticula
Arrows point to the small, wide mouth pouch
located at the tracheal bifurcation
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
38/119
Gastroesophageal reflux (GERD, formerly,
"peptic esophagitis") Common esophagal problem; result of an
incompetent lower esophageal sphincter.
Everyone has probably experienced sudden, unexpected
reappearance of a little bitof lunch in the back of the mouth. But
sustained or frequent reflux starts a viciouscycle that becomes a
major threat to the health of the esophagus and lungs.
The sphincter is inflamed, scars, and becomes further damaged.
The epitheliumkeeps getting digested and regrowing, with much more
opportunity to select formutated cells.
The correlation between clinical symptoms and endoscopy is
remarkably poor. Onlyabout half of the patients with severe "GERD"
on endoscopy even have heartburn.
The cause of common "reflux" remains obscure. Mechanical
problems (includingoverweight and sliding hiatus hernia) must
contribute, and the problem is moresevere if there's "excess
stomach acid / pepsin / bile" or the gastric contents staysfor some
reason within the esophagus. Other things that irritate the
esophagus(swallowing spicy food, alcohol, very hot beverages,
and/or tobacco juice) will nothelp either. Pregnancy,
benzodiazepines, intubation, and tobacco use are allimplicated as
well. Lying flat makes matters worse (tip: try propping the head of
thebed up on cinder blocks).
The diagnosis of GERD is made clinically on endoscopy, but
pathology may beobtained for confirmation.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
39/119
GERD
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
40/119
GERD
Pathologists diagnose reflux based on the following criteria:
More than 20% of the thickness of the epithelium is taken up by
basal cells (i.e., cuboidal ones with scanty cytoplasm, i.e.,
nuclei atleast half the diameter of the cells. Why the thickness of
the basal cell layer? In reflux, the surface cells get
digested and the basal cells are multiplying overtime to replace
them.
papillae with visible cores more than 2/3 of the way up
theepithelium;
eosinophils in the epithelium (we used to teach that this is
moresensitive and specific than it really is, but it's still a
fairly goodmarker:
polys in the epithelium (this just means there's an ulcer, which
iswhat you'd expect if reflux is severe)
balloon cells (hydropic change in injured cells)
Future pathologists: Be sure you've got that specimenproperly
oriented, and consider asking the clinician to send
it up on cardboard
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
41/119
GERD
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
42/119
Gastroesophageal reflux
THE common esophageal problem, the
result of an incompetent lower
esophageal sphincter.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
43/119
Reflux
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
44/119
esophageal acute ulcer
An esophageal acute ulcer is shown here in which the
squamous
mucosa has been lost. In the ulcer base are inflammatory
cells
and fibrin.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
45/119
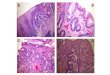
Barrett's
Esophagus If replacement of the normal squamous epithelium by a
columnar epithelium has
occurred, you may have a Barrett's esophagus.
Today's definitions of Barrett's usually require goblet cells,
and for the truly hardcore,the non-goblet cells are both absorptive
and secretory. Older definitions of Barrett'sallowed any columnar
epithelium type.
Ignore hamartomas of gastric-type mucosa; cancer probably only
occurs if there ismetaplasia w/goblet cells, so perhaps one day
Barrett's will be redefined to this.
There are at least 2 million "Barrett's" patients in the U.S. In
Sweden, 1.6% of thepopulation is affected, with alcohol and tobacco
being risk factors.
As you'd expect ("Nowell's law triumphant"), finding a Barrett's
esophagus meansthere's been some hits on the genome, and the
genetically damaged cells have had achance to overgrow the area
because of repeated healing from reflux. This is a fertilebreeding
ground for adenocarcinoma of the esophagus.
You'll look at dysplasias from Barrett's biopsies frequently,
and there are likely to befurther refinements that will help you
let the surgeons know when to operate (laser,scrape, etc). All
Barrett's have some hyperchromasia of the nuclei in the lower
portionsof the glands. Low-grade dysplasia features loss of mucus
production, stratified nuclei inthe crypts, and elongated nuclei in
parallel. High-grade dysplasia features stratificationon the
surface, branching glands, and/or cribriform stuff in the crypts.
Be careful aboutcalling "severe dysplasia" if there is
inflammation; it might be better to treat the refluxand repeat the
biopsy. One major criterion that says "operate" is loss of the
basalorientation of the nuclei, i.e., this is more than just the
kind of atypia that one finds in
an adenomatous polyp.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
46/119
Barrett's
Esophagus
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
47/119
Barretts esophagus
Pre-cancer A: normal, stratified squamous epithelium
B: Intestinal metaplasia of epithelium with
chronic inflammation
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
48/119
Barrett's
esophagus
Another cause for inflammation is a so-called
"Barrett's esophagus" in which there is gastric-
type mucosa above the gastroesophageal
junction.Note the columnar epithelium to the
left and the squamous epithelium at the right.
This is "typical" Barrett's mucosa, because
there is intestinal metaplasia as well (note the
goblet cells in the columnar mucosa).
Metaplasia of the normal
esophageal squamous mucosa
has occurred here, with the
appearance of gastric typecolumnar mucosa.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
49/119
Barrett's esophagus
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
50/119
Perforated esophagus
Perforated esophagus can result from
swallowing the wrong thing. Chicken bones
are infamous these can pierce the heart or
cause other dreadful problems.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
51/119
Perforated esophagus
Left: (1)Perforated esophagus with (2) intraluminalhematoma
Right: Histopathology reveals transmural acute and
chronicinflammation with extensive ulceration and necrosis of
theesophagus.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
52/119
Lacerated esophagus
Lacerated esophagus usually results from heavy-dutyvomiting
during which the esophagus fails to relax(alcohol abuse, pregnancy,
post-anesthesia;"Mallory-Weisssyndrome").
Endoscopists and pathologists see little longitudinaltears,
usually in the distal esophagus. They are aproblem only if bleeding
is massive, or if theesophagus actually ruptures
("Boerhaave'ssyndrome"; at these sites of rupture, the
muscularis
mucosae is apparently absent:
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
53/119
Lacerated esophagus
A large bird with laceration Only good gross pic. Its
Nasty!
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
54/119
Mallory-Weiss syndrome
Lacerated esophagus usually results from heavy-duty
vomiting during which the esophagus fails to relax.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
55/119
Esophageal varices
Esophageal varices are dilatations of the esophago-gastric
venous plexus. These result from portal veinhypertension from any
cause, as the blood from thestomach and intestines seeks the
low-pressurepathway back to the heart.
You won't know varices are there until they bleed.And they bleed
massively when their attenuatedoverlying mucosa is rubbed away, or
they just pop
from pressure. This is the fast way out of life formany problem
drinkers.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
56/119
Esophageal varices
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
57/119
Esophageal VaricesDilations of the esophago-
gastric venous plexus as a
result of portal vein
hypertension.
* Prone to rupture*
Blue arrows: gastroesophageal junction
Black arrows: varices
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
58/119
Portal hypertension
Portal hypertension patients will also
commonly exhibit hemorrhoids and dilated
veins around the umbilicus ("caput medusae")
Remember that portal hypertension will
greatly accelerate GI bleeding from non-
variceal causes (gastritis, peptic esophagitis,
ulcer, Mallory-Weiss) as well.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
59/119
The causes of portal hypertension....
Pre-hepatic Thrombosis of the portal vein
Hypercoagulability
Polycythemia vera, sickle cell, others
Invasion by tumor (usually hepatocellular carcinoma)
Tumor compressing the portal vein
Intra-hepatic Cirrhosis from any cause
Other obstructive disease Bad alcoholic liver disease without
cirrhosis
Schistosomiasis without cirrhosis
Central hyaline sclerosis in alcoholism
Various birth defects Post-hepatic
Budd-Chiari (thrombosis of hepatic veins) Causes as for
thrombosis of portal vein
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
60/119
Tumors of the Esophagus
Benign tumors of the esophagus: Banal, and
relatively uncommon. For example,
fibrovascular hamartomas.
Carcinoma of the esophagus strikes around
8000 people each years and kills most of
them.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
61/119
Squamous cell carcinoma
Squamous cell carcinoma has historically been the most common
esophagealcancer in the United States, but is becoming less
common.
Most patients are males (more than 4:1), black men are at higher
risk thanothers, and in the U.S., the large majority are both
smokers (cigarets, cigars)anddrinkers.
Old lye strictures are also frequent sites for esophageal
cancer, as is the Chagas-disease ridden mega-esophagus.
The epidemic of highly-aggressive squamous cell carcinoma in
Mainland Chinahas been attributed to aspergillus fungus
contamination, nitrosamines, vitamindeficiency, zinc deficiency,
molybdenum deficiency, ethnic teas, and ethnicdelicacies that are
pickled (i.e., rendered rich in certain fungi).
Any portion of the esophagus can be involved; the middle third
is slightly more
common than the others. Like most squamous cell carcinomas,
esophageal cancer arises in squamous
dysplasia, is often multifocal, grows as a fungating lesion
(less often, just anulcer), and produces symptoms (dysphagia, food
"sticking") only late. Becauseof its location, the later stages of
this disease are particularly cruel.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
62/119
Squamous cell
carcinoma
The whorled structuresrepresent keratin pearls andindicate that
this tumor isdifferentiating into structuresrecognizable as being
of
squamous origin
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
63/119
Squamous Cell Carcinoma of Esopohagus
Most patients are males who
smoke and drink
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
64/119
SCC of
esophagus
At the upper left is a remnant of
squamous esophageal mucosa
that has been undermined by an
infiltrating squamous cell
carcinoma of the mid-esophagus.
Solid nests of neoplastic cells are
infiltrating down through the
submucosa at the right.
Esophageal cancers often spread
to surrounding structures, making
surgical removal difficult.
At high power, these infiltrating nests
of neoplastic cells have abundant pink
cytoplasm and distinct cell borders
typical for squamous cell carcinoma.
Esophageal carcinomas are not usually
detected early and, therefore, have a
very poor prognosis.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
65/119
Adenocarcinoma
Adenocarcinoma is now almost as common as squamous
cellcarcinoma, and is probably increasing in frequency. It arises
mostoften arising in a Barrett's esophagus. Again, the
malepredominance is marked (more than 6:1) and as you'd
expect,symptomatic reflux is a strong risk factor.
Tobacco and obesity are risk factors, alcohol consumption is
not. It'sbasically the same lesion as cancer of the gastric
cardia.
The longer the Barrett's region, the higher the risk, and
smoking alsoincreases risk.
Most of the current work on esophageal carcinoma focuses on
early,
accurate diagnosis and surgical treatment. This will be of
specialinterest to those of you who do primary care in rural areas;
you arelikely to do your own endoscopy.
Both types of cancers often arise multifocally. Since
normalesophageal epithelium contains glycogen, you can help
demarcate
dysplastic squamous epithelium using Lugol's iodine
solution.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
66/119
Adenocarcinoma Risk Factors:
Male Barretts Esophagus
Tobacco
Obesity
Reflux
Alcohol is not a risk factor
Esophagus
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
67/119
Stomach Review Healthy mucosa:
Surface, pits ("crypts" / "foveolae") in all areas... Tall
surface mucous cells (make "neutral mucus") Deep in pits, all
areas... Neck cells (reserve cells for both above and below; "the
proliferative zone")
Cardiac glands... More neck-type cells
Gastric glands... Parietal cells (eosinophilic, packed with
mitochondria; make acid and intrinsicfactor); Chief cells
(pale,granular)
Pyloric glands...Neck-type cells; G-cells (gastrin
producers)
Dieulafoy's malformation is an extra-large artery running along
the mucosa of the lesser curvature. It
can cause severe bleeding, even into the chest. Intestinal
metaplasia: A common finding. Most often it's caused by
helicobacter; you might see it in
autoimmune atrophic gastritis with achlorhydria (perhaps due to
the associated bacterial colonization);bile reflux and previous
radiation.
An experienced endoscopistcan spot areas of intestinal
metaplasia by their slightly morewhitish color.
Intestinal metaplasia is clearly the precursor lesion for
"intestinal type" stomach cancer.
Any kind of stomach cancer can harbor any kind of mucin. In case
somebody (not me) asks: Sulfomucin... Very acid... Intestine; if in
stomach, the epithelium is atrophic-metaplastic and is likely
to turn nasty
Carboxymucin... Acid... Intestine (also called "acid
sialomucin")
Neutral mucin,,, Neutral... Stomach (also called "neutral
sialomucin").
Future pathologists: Use alcian blue to stain the acid
mucins!
l
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
68/119
Normal
Stomach
This is the normal appearance of thestomach, which has been
opened along
the greater curvature. The esophagus is
at the left. In the fundus can be seen the
lesser curvature. Just beyond the antrum
is the pylorus emptying into the first
portion of duodenum is at the lower right.The normal appearance
of the gastric
fundus on upper GI endoscopy is shown
below at the left, with the normal
duodenal appearance at the right.
This is the normal appearance of
the gastric antrum extending to
the pylorus at the right of center.
The first portion of the duodenum(duodenal bulb) is at the far
right.
Di h iIn this case, the diaphragmatic dome is missing
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
69/119
Diaphragmatic
hernias
result from failure of the
diaphragm to form properly.
Portions of stomach,
intestines, and other organs
end up in the chest.
on the left, allowing herniation of the abdominal
contents into the chest cavity. The metal probe in
the photograph is behind the left lung, which has
been displaced by the stomach. Below the
stomach is a dark spleen (at the white arrow).The white arrow
overlies the left lobe of liver
which is extending upward.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
70/119
Stomach Birth Defects
Congenital pyloric stenosis isprobably a hereditary defect
ofvariable penetrance in which thepylorus of the stomach
ishypertrophic, and the gastric outletmay become fully
obstructed,
typically at the endofthe firstmonth oflife.
The infant experiences projectilevomiting, and the surgeon feels
amass in the upper abdomen. Surgicalsplitting of the pylorus
effects acure.
It is more common in boys, andTurner's XO is also a risk.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
71/119
Pyloric Stenosis
More common inmales and TurnersXO
Infant experiencesprojectile vomiting
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
72/119
pyloric stenosis
This is pyloric stenosis. Note the prominent hypertrophied
muscle with elongation and
narrowing of the pylorus at the gastric outlet on the left.
Pyloric stenosis is uncommon,
but is a cause for "projectile" vomiting in an infant about 3 to
6 weeks of age. Males areaffected more than females. The overall
incidence is approximately 3 per 1000 livebirths.
The "pacemaker" interstitial cells of Cajal (ICC) regulate
motility, and contain the enzyme
heme oxygenase-2 which generates carbon monoxide (CO) as a
neurotransmitter to
cause relaxation in adjacent smooth muscle cells. The lack of
ICCs in pyloric stenosis
results in deficient CO production leading to motility
dysfunction.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
73/119
Dilated stomach
Often impressive.
Causes include beer chug-a-lugging, bowel obstruction,
misplacedendotracheal tubes, gastroparesis (think of diabetic
autonomicneuropathy), and (in the dead) inept CPR attempts.
(Amateursfirst blow air into the stomach, then rupture it by
pressing in the
wrong place.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
74/119
Bezoars
These are swallowed goodies that remainpermanently in the
stomach.
Hairballs (trichobezoars) are seen in people whoenjoy nibbling
their long hair ("Rapunzel
syndrome"). Or ask a pet cat.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
75/119
Phytobezoars
May be chunks of ill-chewed vegetable matter, or (worst)
persimmonremnants. The latter contain a substance that, complexed
with acid, turnsinto cementand may require surgery.
Treating a gastric phytobezoar with meat tenderizer.
Things that interfere with gastric emptying (diabetes, other
dysautonomias,post-vagotomy, anti-cholinergic medicines) enhance
one's ability topersonally experience a bezoar.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
76/119
gastroparesis
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
77/119
Acute gastritis
Acute damage to the gastric mucosa from any cause.
Pathologists define this to be neutrophils in the
epitheliumabove the basement membrane.
If there is necrosis of any epithelial cells, it is
"erosivegastritis" -- you remember that an erosion is
inflammationplus necrosis of an epithelium without necrosis of
theunderlying connective tissue (at least not yet).
Pathogenetic mechanisms include: compromise of the mucosal
defenses
killing of epithelial cells
increased acid production / decreased bicarbonate production
ischemic injury
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
78/119
Acute Gastritis Important causes:
alcohol consumption
aspirin use (remember this one; even the "minidose aspirin" that
is supposed to be sogood for you gives about half of users gastric
erosions
caffeine use
chemotherapy for cancer
food allergy (it's for real, and endoscopy is much more accurate
than skin-tests or RAST.Probably causes at least some of the cases
of the mysterious "eosinophilicgastroenteritis".
Helicobacter (see below)
radiation injury
reflux of lysed lecithin ("lysolecithin") from the duodenal
bile
shock
spicy foods
staph food poisoning
"stress" (maybe)
tobacco use
viruses (Norwalk calicivirus winter "stomach 'flu", others; all
about viral gastroenteritis
You can figure out for yourself what the mechanisms might be in
each case.Anatomically, you may see anything from mild edema and a
few polys to bloodysloughing of chunks of the upper mucosa, and
symptoms can range from "upsetstomach to vomiting blood by the
pint.
Autoimmune ("fundic", "chronic active",
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
79/119
Autoimmune ( fundic , chronic active ,
"diffuse atrophic", "type A") chronic
gastritis An autoimmune process that attacks primarily the
fundic glands. You'll see loss of mucous secretion, striking
shortening of the glands,
and usually loss of the parietal cells.
Patients usually (60+%) have autoantibodies against parietal
cellH+/K+ ATPase (and usually others against intrinsic factor).
This is the usual cause of the achlorhydria (i.e., greatly
diminished orno stomach acid) and Addisonian pernicious anemia.
Around 10% of these patients go on to develop stomach
cancer.
Many of these patients have other autoimmune endocrine
diseasesas well. The three to remember are Addison'sdisease
oftheadrenals, Hashimoto'sdisease ofthe thyroid and
insulin-dependentdiabetes.
Future pathologists: Since there is no acid and no feedback, the
G-cells undergo hyperplasia in the antrum. They are a single layer
ofclear cells. This is a breeding-ground for carcinoids
supposedly.
Work on autoimmune gastritis is overshadowed nowadays
byhelicobacter, but the finding of anti-parietal cells seems
solid.
Perhaps those lacking the antibody were really
helicobacter-inducedatrophy (see below). And helicobacter itself
can supposedly triggerthe autoantibodies.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
80/119
Acute Gastritis
Neutrophils in the epithelium above the basement
membrane
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
81/119
acute gastritis
At high power, gastric mucosademonstrates infiltration by
neutrophils.
This is a more typical acute gastritis
with a diffusely hyperemic gastric
mucosa. There are many causes for
acute gastritis: alcoholism, drugs,
infections, etc.
Eosinop i ic
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
82/119
allergic
gastroenteritis
H li b t t iti
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
83/119
Helicobacter gastritis The vast majority of the old "unexplained
chronic gastritis" ("type B gastritis") cases are caused by
helicobacter.
You'll have no trouble recognizing the familiar wiggly creatures
on the surface of (often obviouslydamaged) gastric mucosa.
Giemsa, immune, or silver stains show them to advantage.
Helicobacter flourishes in the stomach because it cleaves urea
to ammonia under acid conditions.
Helicobacter's virulence factor, CagA protein, actually gets
inoculated into the stomach cells.
Nobody knows yet exactly what it does to cells after it enters,
though it deregulates at least one growthcontrol gene. The other
virulence factor, VacA (vacuolizing cytotoxin A) is even more
mysterious.
There's a chronic infiltrate with both lymphocytes and
neutrophils. Lymphoidfollicles in the mucosa
suggest "Helicobacter". Pyloric metaplasia advances from the
antral area into the fundus, perhaps decreasing acid
production,
and the fundic glands may atrophy as well. You may see
intestinal metaplasia, especially near any ulcersthat may be
present. Acid production may be increased, decreased, or
normal.
When the fundus is involved, the fundic glands become shallow
("patchy atrophic gastritis", to bedistinguished from autoimmune
atrophic gastritis), and typically exhibit intestinal metaplasia
(i.e.,enterocytes, goblet cells; it's especially pre-malignant --
type III -- when they are filled with "acidmucus/sulfomucus" as in
the real intestine) and/or antral metaplasia (neck cells, G-cells).
In advanced
autoimmune gastritis only, the parietal cells are completely
gone. In any portion, the rugae are likely to flatten and vanish.
The process begins at the surface and work
downward into the glands. Lesions of various stages are present
simultaneously in different parts of thestomach. Eventually, the
surface will come to exhibit at least some intestinal metaplasia
and probablysome degree of dysplasia.
Helicobacter gastritis involving most of the stomach is the
precursor lesion to the epidemic stomachcancers seen in much of the
world.
Removing Helicobacter cures this illnes. Most people with
significant duodenitis (i.e., polys) have
Helicobacter gastritis
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
84/119
Helicobacter
gastritis
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
85/119
Helicobacter Pylori Helicobacter gastritis involving most of
the stomach is the precursor lesion tothe epidemic stomach
cancers seen inmuch of the world
Lymphoid follicles in the mucosa suggestHelicobacter
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
86/119
Menetrier's disease ("idiopathic
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
87/119
( p
hypertrophic gastritis"; "enlarged fold
gastitis) Idiopathic hyperplasia of
the surface mucous cells,with correspondingatrophy of the
glands.Makes for some big folds,and a lot of protein loss inthe
excessive mucus.
Menetrier's is caused (at
least sometimes) byHelicobacter, and resolveswhen you clear
thebacteria.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
88/119
Menetriers disease
Idiopathic hyperplasia
of the surface mucous
cells, with
corresponding atrophyof the glands
Menetriers
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
89/119
Menetrier s
disease
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
90/119
Zollinger-Ellison syndrome
Gastrinoma (often in the pancreas) causing
hyperplasia of the gastric glands. Makes for a
very upset, ulcerated stomach.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
91/119
Stress ulcers
(the usual "acute erosions")
small (less than 1 cm) areas of loss of some (or all) the
mucosa.Note thatnobody really knows where "acute gastritis" leaves
off and "stress ulcers"begin; probably they're part and parcel of
the same reaction pattern.
If the patient has burns, they are "Curling's ulcers" (* think
of a hotcurling iron). If the patient has intracranial trauma, they
are "Cushing'sulcers" (attributed to vagal stimulation of gastric
acid secretion, named forfamous neurosurgeon Harvey Cushing).
Their pathogenesis constitutes a major mystery of medicine.
Except inCushing's ulcers, hyperacidity does not seem to be the
problem. Most ofthe factors that produce "acute gastritis" can also
help produce stressulcers. Some workers now favor catecholamine
effect (i.e., ischemia)
and/or some glucocorticoid effect. Pre-pyloric erosions are due
to stress
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
92/119
Stress Ulcers
Small (
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
93/119
Curling Ulcers
Peptic Ulcers
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
94/119
Peptic Ulcers Ulcers resulting from the digestive
actionofacid-pepsin ("no acid, no ulcer") on the gastric
mucosa. A common problem,somewhat more common in men, usually
subclinical, prone to
remit and relapse ("once an ulcer, always an ulcer"). "U
lcers can occur anywhere along theGI tract. Frequency: 80%
duodenum 19% stomach 1% elsewhere
The early wisdom was that almost all patients with either
gastric or duodenal ulcer patientshave Helicobacter on board, and
eliminating the creature eliminates the disease. Of coursethat was
an exaggeration; a large minority of stomach ulcer patients are
helicobacter-negative.
Other risk factors for ulcer include being under physical or
emotional stress, smoking, takingaspirin or NSAID's, boozing, a
family history, blood type O (* blood group factors, notablyLewis
B, mediate attachment of Helicobacter:; a factor BabA binds to
blood group O), havinga job that requires you to be physically
active, * non-secretor status (ask a blood banker orcriminologist,
these people keep Lewis B on board), hypercalcemia from any cause
(enhancesgastrin secretion), cirrhosis and emphysema (make life
stressful), and having a stomach tubedown.None of these are
overwhelmingly powerful. (You will get an ulcer, and
probablyseveral, if you develop a gastrinoma.)
Those with duodenal ulcers tend to secrete acid too abundantly
when stimulated, and to
empty their stomachs too readily. Gastric ulcer types tend to
have low-normal levels of acid, and tend either to have chronic
gastritis or take lots of aspirin or other substances noxious to
the stomach. People withlongstanding gastric ulcers almost all have
"chronicgastritis" in the antrum, and intestinalmetaplasia near the
ulcer.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
95/119
Peptic Ulcers
Most (almost all) patients with duodenal ulcers, and a majority
of those with gastric ulcers,now are known to have Helicobacteron
board, and the bug is thought to be an importantpart of the
pathogenesis.
In the duodenum, there appears to be a vicious cycle between
Helicobacter infection andantral metaplasia that permits the bugs
to thrive. This is not surprising, considering theabrupt appearance
and disappearance of ulcers. Antral metaplasia is a common finding
innormal duodenum, and perhaps this how duodenal ulcers begin.
The rare Helicobacter-negative duodenal ulcer patient may have
Crohn's, Zollinger-E
llison,taking steroids or NSAID's, or just be unlucky.
Peptic ulcers are usually single, and most are less then 3 cm
across. They look sharplypunched-out (as you'd expect, rolled
borders suggest malignancy). However, they maypenetrate deeply. The
base is always keep clean by digestive juice.
Gastric ulcers are usually on the lesser curvature, and the
favorite site is near or in theantrum. Duodenal ulcers are usually
in the first portion, but may be anywhere. As scarcontracts, the
mucosal folds radiate from the ulcer.
Peptic ulcers may cause pain (relieved when food or antacid
neutralizes stomach acid,recurring after a meal stimulates stomach
acid), hemorrhage, perforate (call the surgeon!)and/or cause
fibrosis leading to obstruction (notably of the pylorus).
We believe they do not undergo malignant transformation
("cancers often ulcerate, butulcers seldom/never cancerate").
Future surgeons: You may "CHOP" out the ulcer if it is chronic,
hemorrhaging uncontrollably,obstructing the gastric outlet, or
perforated.
Peptic Ulcers
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
96/119
Peptic Ulcers
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
97/119
Peptic Ulcers
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
98/119
Hyperplastic ("inflammatory") polyps
Extremely common and thought to result fromexuberant
regeneration of the mucosalepithelium.
They usually look like multiple little rice grains,but may be
larger. Microscopically, they arecomposed ofdilated glands lined
with pit-typecells.
The big ones (over 1.5 cm) can turn cancerous
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
99/119
Hyperplastic polyps of stomach Extremely common and thought
to
result from exuberant regenerationof the mucosal epithelium
Microscopically: dilated glands linedwith pit-type cells
Stomach
Adenomatous polyps
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
100/119
Adenomatous polyps
("neoplastic polyps", "adenomas")
Tend to be pedunculated, with villi and/or
crypts, and the current definitions require
some dysplasia. They are premalignant, there
is a link to syndromes and a familial tendency,and maybe half
would turn into cancer if left
alone (but who wants to do that study?)
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
101/119
Adenomatouspolyps
adenomatous
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
102/119
adenomatous
polyp
The concept of differentiation is
demonstrated by this smalladenomatous polyp (tubular
adenoma)
of the colon. Note the difference in
staining quality between the epithelial
cells of the adenoma at the top and the
normal glandular epithelium of the
colonic mucosa below.
i i bl
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
103/119
Gastric Leiomyoblastoma
This unusual smooth muscle tumor showsa velvetty red mucosa over
its surface.
This is stomach mucosa.
i i l l
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
104/119
Gastrointestinal stromal tumors
The common spindle-cell neoplasms of the
stomach, bearing a trademark c-kit mutation
and stainable antigen, and responding to
Gleevic(imatinib). They range from totallybenign to highly
malignant.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
105/119
Gastrointestinal
stromal tumors
G i i id
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
106/119
Gastric carcinoid
High levels of gastrin causes enterochromaffin
cell hyperplasia, and most people who get
gastric carcinoid have high gastrin levels
(atrophic gastritis or Zollinger-Ellison). Andrats actually get
such tumors after lifetime
omeprazole.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
107/119
Gastric carcinoid
G t i d i
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
108/119
Gastric adenocarcinoma
While its prevalence in the U.S. has decreased strikingly in
recent decades, thiscontinues to be an important cancer killer in
every country. Around 15,000 peopleper year die of stomach cancer
in the U.S. Rates in the rest of the world are alsodeclining.
Risk factors include: diet -- smoked food, ethnic pickled
delicacies, lack of green vegetables, liking your meat
well-done, lack of meat / animal fat, nitrates/nitrites
(obviously alot of this is junk
science) status post partial gastrectomy (the old ulcer
operation)
helicobacter
blood groups A and AB
Diet and environment are evidently much more important than
ethnicbackground. First-generation immigrants have the risk of
their home countries;second-generation immigrants the risk of their
new countries
There are two major types of gastric adenocarcinoma, with
different cells of origin: (1) Diffuse infiltrative gastric
adenocarcinoma
(2) Intestinal type gastric adenocarcinoma.
G t i d i
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
109/119
Gastric adenocarcinoma
G t i d i
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
110/119
Gastric adenocarcinoma
Gastric
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
111/119
adenocarcinoma
This is a signet ring cell pattern of
adenocarcinoma in which the cells arefilled with mucin vacuoles
that push the
nucleus to one side, as shown at the arrow.
Diff i filt ti t i d i
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
112/119
Diffuse infiltrative gastric adenocarcinoma
Arises from the neck cell.
It exhibits small glands made of polyhedralcells with round,
tame-looking nuclei, or cells
infiltrating singly. It is the most commonsubtype of signet-ring
cancers.
Helicobacter, autoimmune gastritis, andintestinal metaplasia are
not risk factors.
The frequency of this cancer is actuallyincreasing dramatically
in the US.
Diffuse infiltrative
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
113/119
Diffuse infiltrative
gastric
adenocarcinoma
I t ti l t t i d i
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
114/119
Intestinal type gastric adenocarcinoma
Typically arises in the setting oflongstanding
"atrophic gastritis" or other "chronic gastritis",
usually in the presence of helicobacter and/or
autoimmune gastritis and/or intestinal metaplasia
and/or bile reflux.
It features large glands made oftall cells with rod-
shaped nuclei (as in the more common, more
familiar primary carcinomas of the colon). This is thecommon
type of stomach cancer in the high-risk
countries
Intestinal type
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
115/119
Intestinal type
gastricadenocarcinoma
Stomach Cancers
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
116/119
Stomach Cancers The gross is the usual for a cancer (a
cauliflower, an ulcer, or diffuse invasion). The histology
is what you'd expect. In either case, you may see invasive
glands, papillae, signet-ring cells,mucus lakes, desmoplasia, and
most anything else, though when you see signet ring cellinvasion,
it is usually the "diffuse" type rather than the "intestinal" type.
Terms: linitisplastica: "leather bottle stomach from a
diffusely-infiltrating, desmoplastic cancer.Krukenberg tumor:
Drop-metastases causing enlargement of the ovaries. Sister
MaryJoseph's node: metastasis to the umbilicus (named for the Mayo
brothers' scrub nurse).Rectal shelf ("of Blumer"): Drop-metastases
to the lowest place on the peritoneum(remember the "pouch
ofDouglas"?)
Symptoms are also what you'd expect -- nausea, vomiting, early
satiety, GI bleeding. Asyou'd also expect, there are usually no
symptoms until it's too late. (If you have an extracauliflower in
you stomach, you'd never know it.)
There is so much stomach cancer in Japan that people get
endoscoped routinely in search ofit, and there are many cures
(unlike in the US). (For some reason that no one understands,the
Japanese have a tremendously high rate of atrophic gastritis,
conceivably from the localstrains of helicobacter, and this is
where most of these cancers arise. Biopsy all stomach
ulcers you see --even a cancer may shrink on a regimen of
H2-blockers and antacids. Most gastric adenocarcinomas are probably
preceded by high-grade carcinoma-in-
situ/dysplasia; dysplasia usually invades the mucosa soon, and
until it penetrates themuscularis propria, it's called "early
gastric cancer" (EGC). It can stay in the mucosa for a
longtime.
Some diffuse-infiltrating cancers may start de novo, without
dysplasia
Detected late (and it still usually is), stomach cancer has a
generally poor prognosis.
The mainstay of therapy for stomach cancer is surgery.
Lymphomas
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
117/119
Lymphomas
Stomach lymphomas (and other GI lymphomas) are
less common than carcinomas but have a better
prognosis. Since they tend to be bulky, patients
present with obstruction.
Western ("American") lymphomas are usually
familiar B-cell lymphomas. Helicobacter seems to be
the big risk factor. (no surprise, since Helicobacter
makes lymphoid follicles grow). However, manygastric lymphomas
are helicobacter-negative and
different genetically.
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
118/119
Lymphomas
Stomach Lymphoma
-
8/7/2019 1 ESOPHAGUS AND STOMACH_Learn
119/119
Stomach Lymphoma
Stomach
Less common than carcinomasb h b