Embed Size (px)
Citation preview

1
Depression, Co-morbidities, and Access To Treatment in Hispanic Populations
Pedro L. Delgado, MDDielmann Distinguished Professor and Chairman,
Department of Psychiatry,
Associate Dean for Faculty Development and Professionalism
The University of Texas Health Science Center, San Antonio

2
Disclosures
• Advisory Board: Wyeth, Eli Lilly, Neuronetics
• Grant Support: CNS Response, NIH

3
U.S. Department of Health and Human Services, 2001
Sanchez-Lacay JA, et al. 2001
Blanco C, presented 2001
Data on file, Forest Laboratories
Treatment of Depression in Hispanics
• Paucity of data from clinical trials• Results from clinical trials of largely Caucasian patients
assumed to be applicable to Hispanics• Depressed Hispanic patients may report increased
rates of somatization/physical symptoms• More recent data suggest that compared with
Caucasians, Hispanics:– Require equal optimal antidepressant doses– Have similar rates of response to treatment– Tolerate medicines equally well– May be more likely to discontinue treatment

4
Mexican58%
South American
4%
All Other Hispanic
17%
Cuban4%
Central American
5%
Puerto Rican10%
Dominican2%
Spaniard0%
U.S. Census Bureau 2000
Distribution of the Hispanic Population
5Smedley BD, et al. 2002
Summary of Findings: Unequal Treatment, a 2001 Report by the
Institute of Medicine • Racial and ethnic disparities in health care exist
– Poorer outcomes make change imperative
• These disparities occur in the context of: – Broader historic and contemporary social and
economic inequality, and
– Evidence of persistent racial and ethnic discrimination in many sectors of American life
• Among the contributing sources are health systems, health care providers, patients, and utilization managers

6Ramirez RR, de la Cruz CG 2003
Kaiser Family Foundation 2004
Vega WA, Alegria M 2001
Access for Hispanics
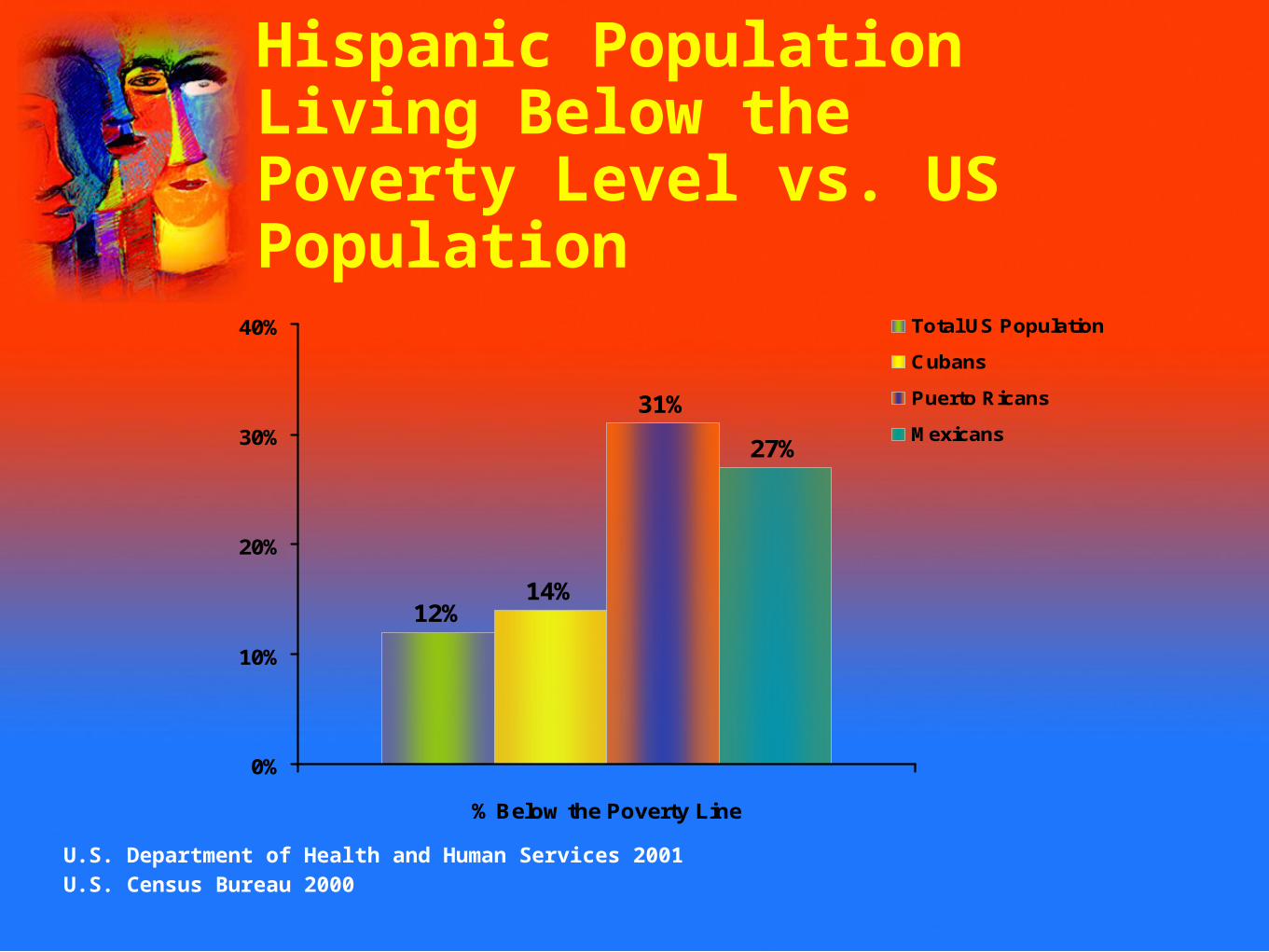
• More than 1 in 5 Hispanics live below the poverty level• Insurance status is associated with lower use of health care
services• 35% of Hispanics are uninsured
– 63% of these report being employed• For Hispanics, access to insurance is unevenly distributed:
– Within families– By geographic region according to state– Between Hispanic ethnic subgroups by country of origin
7
12%14%
31%
27%
0%
10%
20%
30%
40%
% Below the Poverty Line
Total US Population
Cubans
Puerto Ricans
Mexicans
U.S. Department of Health and Human Services 2001U.S. Census Bureau 2000
Hispanic Population Living Below the Poverty Level vs. US Population

8
0
5
10
15
20
25
30
35
40
45
50
Mexican Puerto Rican Cuban CenteralAmerican
SouthAmerican
Kaiser Family Foundation 2004
Uninsured Hispanics by Country of Origin

9Ruiz P 1997
0%
10%
20%
30%
40%
50%
60%
1977 1987 1997
Private Health Insurance Medicaid or Medicare Uninsured
Proportion of Hispanics Lacking Insurance on the Rise

10
Moscicki EK, et al. 1989
Depressive Symptomatology in Mexican Americans: Hispanic Health and Nutrition Examination Survey
• High levels of depressive symptoms found in 13.3% of Mexican Americans
• Higher risk of depression associated with– Female sex
– Low educational achievement
– US birth
– Anglo-oriented acculturation

11
Norms of Expressing Disorder
• Ethnic minority groups may present symptoms that are not part of established nosology – For example, “ataque de nervios” is an idiom of distress
prominent among some ethnic subgroups of Hispanics• Ignoring cultural context can lead to over- and under-
pathologization of individuals• Stigma of mental illness, denial of mental health problems
and values of self-reliance may influence Hispanics’ decisions to seek care
Lewis-Fernandez R 1996; Kleinman A 1988;
Karno M, Jenkins JH 1993; Alegria M, McGuire T 2003;Alarcon RD 1983; Fabrega H Jr. 1990;
Ortega AN, Alegria M 2002; Ortega AN, Alegria M In press;
Gonzalez J, et al. unpublished

12
Expectations(Placebo response)
Clinician Patient
Adherence
CULTURE
TherapeuticAlliance
Health belief
Personal Experiences
Lin KM, Smith MW 2000

13
Depression Includes Both Emotional and Physical Symptoms
Simon et al. NEJM. 1999;341:1329-35.A
No
. of
Ps
yc
ho
log
ica
l S
ym
pto
ms
0.0
0.5
1.0
1.5
2.0
1.51.00.50.0
GroningenParis Ankara
AthensMainz
Manchester
Rio de Janeiro
Santiago
BerlinBangalore
NagasakiShanghai
SeattleIbadan
Verona
No. of Physical Symptoms

14
Major Depression Includes Physical, Emotional and Cognitive Symptoms
Physical Emotional CognitiveWeight change Depressed mood Impaired
concentration
Fatigue, loss of energy
Guilt/worthlessness
Suicidal ideation
Insomnia/hypersomnia
Diminished pleasure/interest
Psychomotor retardation or
agitation
Pain/Somatic complaints
Anxiety
American Psychiatric Association. DSM-IV-TR. Washington, DC: American Psychiatric Association; 2000.

15
Chronic Painful Physical Symptoms Are Common in People with Depression
Ohayon & Schatzberg Arch Gen Psychiatry. 2003;60:39-47.
*
0
5
10
15
20
25
30
35
40
>1 Depressive Symptoms
Major DepressiveDisorder
(%)
CP
PS
43.4%
17.1%
GeneralPopulation
27.6%
18,980 subjects from 5 European countries by telephone interviews16.5% at least 1 depressive symptom; 4.0% full diagnosis of major depression

16
Common Physical Symptoms
• Fatigue• Leaden feelings in
arms or legs
• Insomnia• Hypersomnia• Decreased appetite• Weight loss• Increased appetite• Weight gain
• Reduced libido• Erectile dysfunction• Delayed orgasm• Headaches• Muscle tension• Gastrointestinal upset• Heart palpitations• Burning or tingling
sensations
Cassano P, Fava M. J Psychosom Res. 2002;33:849-57.

Somatic Symptoms and Psychiatric Disorders
0
10
20
30
40
50
60
70
80
90
Any Disorder Mood Anxiety
0 Symptoms
3-5 Symptoms
6+ Symptoms
Kroenke K, et al. 1994

18
Phases of Treatment
Adapted from: Kupfer, et al. J Clin Psychiatry. 1991;52:28-34.
MaintenanceContinuationAcute
Full Recovery
Seve
rity
Time
Response
RelapseRecurrence
Treatment Phases
Symptoms
Remission
Syndrome
Relapse
Progression
to disorder
No Depression

19
Candidates for Maintenance Treatment
• Three episodes, or• Two episodes and a risk factor
– Family history of bipolar disorder or recurrent major depression
– Psychotic or severe prior episodes
– Closely spaced episodes
– Incomplete interepisode recovery
• Patient preference

20
Depression: Response vs. Remission
HAM-D17 Scores
15
7
Response: 50% reduction in baseline HAM-D score or HAM-D 15
Remission: HAM-D Score 7
“Virtually Complete Symptom Resolution”
Depression
HAM-D17 Scores (total possible score = 56)

21
Antidepressants are Generally Helpful in Reducing Chronic Pain
McQuay et al BMJ. 1997;314:763-4.
Meta-analysis: L'Abbe plot for trials of antidepressants in diabetic neuropathy and postherpetic neuralgia, showing percentage of patients achieving at least 50% pain relief when taking antidepressants versus placebo
Pe
rce
nta
ge
Wit
h P
ain
Re
lief
on
Ta
kin
g T
rea
tme
nt
Percentage With Pain Relief on Taking Placebo
50
25
75
100
00 25 50 75 100
Diabetic neuropathyPostherpetic neuralgia
unlabeled or investigational uses

22
Treatment of Neuropathic Pain Conditions with Antidepressants
Number Needed to Treat
TCA (mainly amitriptyline) 2–3
SNRI (mainly venlafaxine) 4–5
SSRI (fluoxetine, citalopram) 7 or more
NRI (reboxetine) insufficientNaSSA (mirtazapine) reliable data
Sindrup SH, et al. Basic Clin Pharmacol Toxicol. 2005;96:399-409.
unlabeled or investigational uses

23
Efficacy for the Treatment of MDD: Venlafaxine vs SSRI vs Placebo
1 2 3 4 6 80
50
40
30
20
10
Week of treatment
Rem
issio
n r
ate
(%
) Venlafaxine
SSRI
Placebo
*
* †‡
* †
* †
‡
¶ ║
§
Remission rates (score ≤7 on 17-item HAM-D) for pooled studies.*P≤.05 venlafaxine vs SSRI; †P≤.05 venlafaxine vs placebo; ‡P≤.05 SSRI vs placebo;§P<.001 SSRI vs placebo; ¶P<.001 venlafaxine vs SSRI; ║P<.001 venlafaxine vs placebo.HAM-D=Hamilton Depression Rating Scale; MDD=major depressive disorder.
Thase ME et al. Br J Psychiatry. 2001;178:234-241.

24
Duloxetine 80 mg/day Duloxetine 60 mg/day Duloxetine 40 mg/day Duloxetine 20 mg/day Placebo
Duloxetine Versus Placebo in MDD With Painful Physical Symptoms
Goldstein DJ, et al. Psychosomatics. 2004;45:17-28.
-12
-10
-8
-6
-4
-2
0
2
0 1 2 3 4 5 6 7 8 9
b
bb
b
ca
aa
a
0 1 2 3 4 5 6 7 8 9 0 1 2 3 4 5 6 7 8 9
Treatment (Weeks)
Le
ast
Sq
ua
res
Mea
n C
han
ge
a Significant difference, compared with placebo, P ≤0.05.b Significant difference, compared with placebo, P ≤0.001.c Significant difference, compared with placebo, P ≤0.01.
Study 1 Study 2 Study 3
• Change from baseline in overall pain severity scores of patients with major depressive disorder in three studies evaluating the effects of duloxetine on painful physical symptoms

25
Summary• Hispanics face similar depression risks as Caucasians
– Although presentation may vary
– Gender and socioeconomic status contribute more to risk than ethnicity
• Culture, sociodemographic factors impact patient interaction with, adherence to treatment programs
• Few trials have identified Hispanics as a distinct treatment population– CBT focus on environmental factors is valuable
– Response to antidepressants is comparable
– More research is needed
• Much still to be known

26
Conclusion• Despite improved recognition in treatment advances,
depression remains a significant health care burden• Goal of treating depression should be complete symptom
resolution• Antidepressants that effect both 5-HT and NE may have
advantages over more selective antidepressants• Goal to achieve remission• Unmet need exists for patients with depression with
physical symptoms• Serotonin and norepinephrine are shared biochemical
mediators in modulating depression, including physical symptoms of depression