Embed Size (px)
Citation preview
Comorbidities in acute heart failure- pulmonary disease
Frans H. Rutten, MD, PhD, general practitionerFrans H. Rutten, MD, PhD, general practitioner
Julius Center, University Medical Center Utrecht, Netherlands
No conflict of interest on this topic
40% ‘COPD’ aged 65 yrs or over: NO COPD1
78% ‘COPD’ hospitalized acute systolic HF: NO COPD 2
20.5% ‘COPD’: unrecognized HF 120.5% real COPD: unrecognized HF 1
1. Rutten FH et al. EHJ 2005;26:1887-942. Brenner S et al. Int J Card 2013;168:1910-6.
Doubt diagnosis of COPD!!
cardiologists afraid to overdiagnose HF..pulmonologist/GPs are not afraid to overdiagnose COPD..
Background heart and lungs ‘tandem’ in providing oxygen saturated blood
both share tobacco smoking as important risk factor: - lung destruction (Western world >90% COPD by smoking) - endothelial dysfunction atherosclerosis and IHD - first/second/third hand smoke plaque rupture/erosion
risk of acute MI , also in non-smokers
- cause of death in COPD patients often cardiovascular
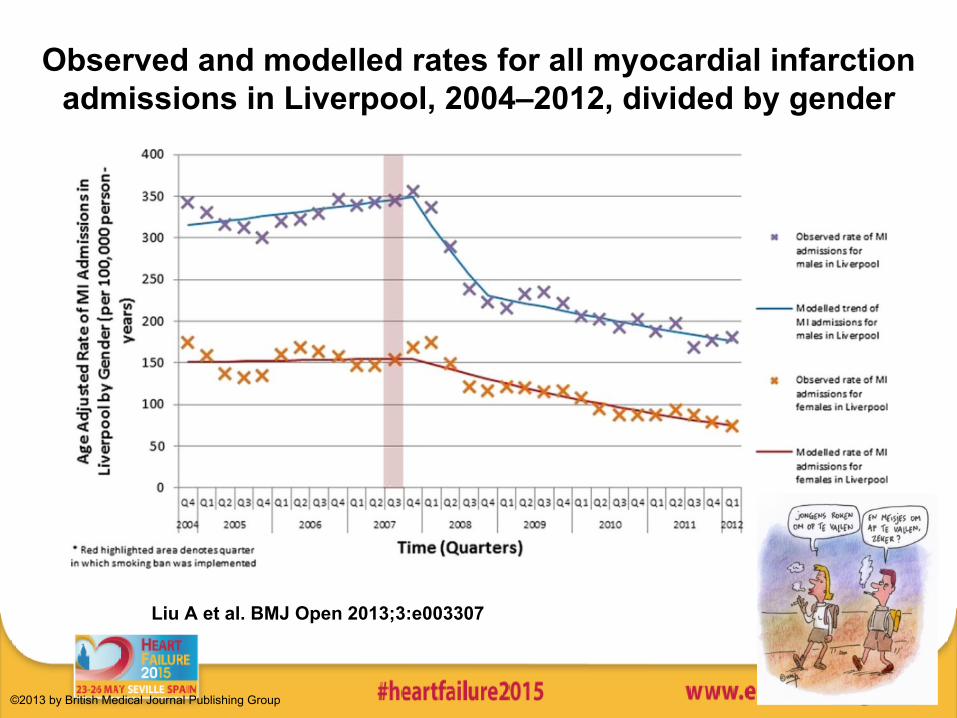
Observed and modelled rates for all myocardial infarction admissions in Liverpool, 2004–2012, divided by gender
Liu A et al. BMJ Open 2013;3:e003307
©2013 by British Medical Journal Publishing Group
smoking ban resulted in reduction in acute MI
• Flanders Belgium Heart 2014;100:1430-5before and after smoking ban in public places, work places, restaurantswomen < 60 jr - 33.8% > 60 jr - 9.0%men < 60 jr - 13.1% > 60 jr - 7.0%
• Schmucker Germany Eur J Prev Cardiol 2014;9:1180-6
+4% smokers16% reduction STEMI
-26% non smokers
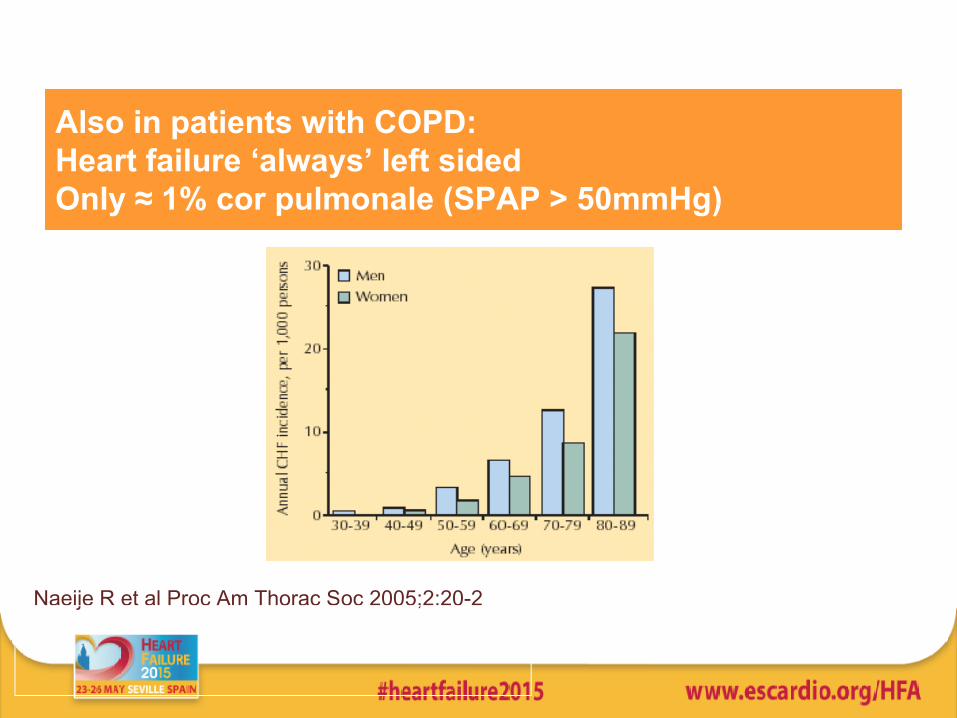
Also in patients with COPD: Heart failure ‘always’ left sidedOnly ≈ 1% cor pulmonale (SPAP > 50mmHg)
Naeije R et al Proc Am Thorac Soc 2005;2:20-2
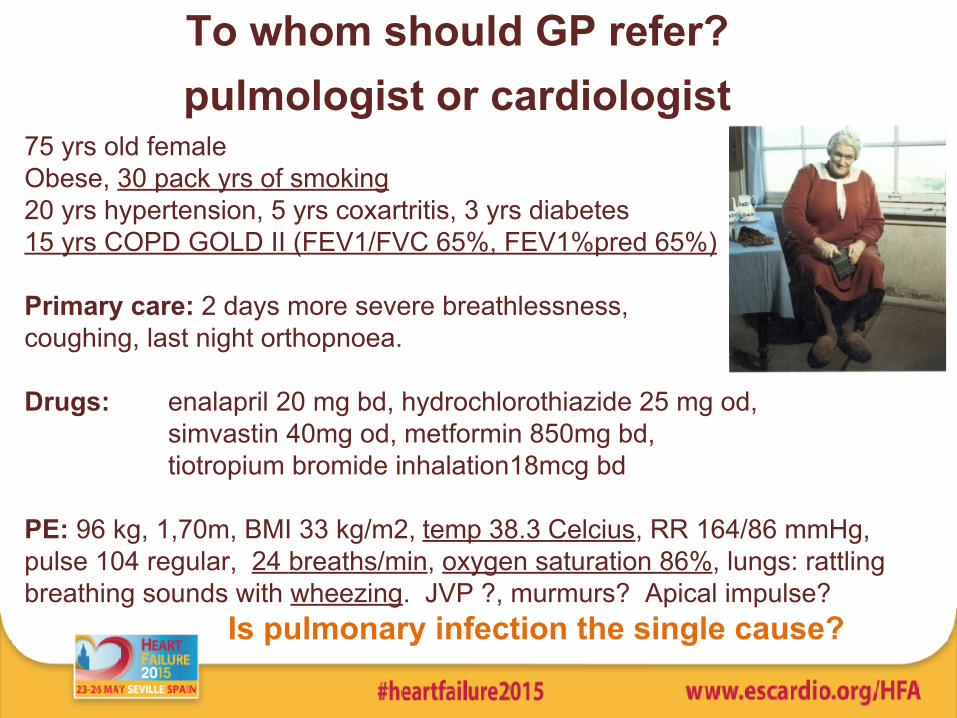
To whom should GP refer? pulmologist or cardiologist
75 yrs old femaleObese, 30 pack yrs of smoking20 yrs hypertension, 5 yrs coxartritis, 3 yrs diabetes 15 yrs COPD GOLD II (FEV1/FVC 65%, FEV1%pred 65%) Primary care: 2 days more severe breathlessness, coughing, last night orthopnoea.
Drugs: enalapril 20 mg bd, hydrochlorothiazide 25 mg od, simvastin 40mg od, metformin 850mg bd,
tiotropium bromide inhalation18mcg bd
PE: 96 kg, 1,70m, BMI 33 kg/m2, temp 38.3 Celcius, RR 164/86 mmHg, pulse 104 regular, 24 breaths/min, oxygen saturation 86%, lungs: rattling breathing sounds with wheezing. JVP ?, murmurs? Apical impulse?
Is pulmonary infection the single cause?
respiratory symptoms ≠ pulmonary disease Does wheezing fit with asthma or COPD?
35% of elderly with AHF wheeze at initial presentation
Risk of overdiagnosing COPD
Jorge S et al. BMC Cardiovasc Disord 2007;7:16
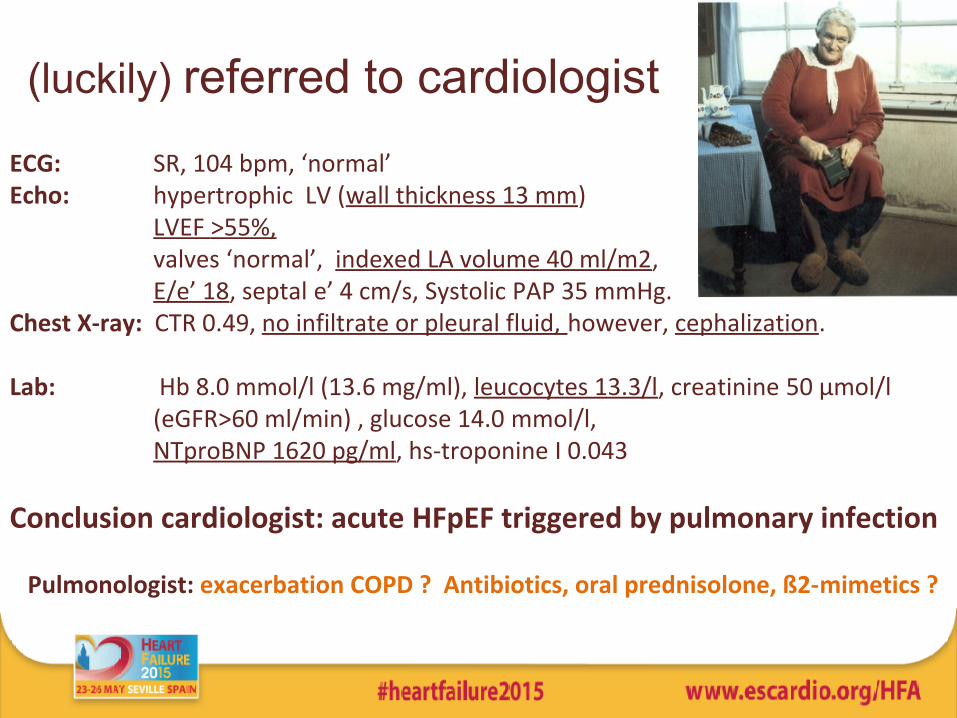
(luckily) referred to cardiologistECG: SR, 104 bpm, ‘normal’ Echo: hypertrophic LV (wall thickness 13 mm)
LVEF >55%, valves ‘normal’, indexed LA volume 40 ml/m2, E/e’ 18, septal e’ 4 cm/s, Systolic PAP 35 mmHg. Chest X-ray: CTR 0.49, no infiltrate or pleural fluid, however, cephalization.
Lab: Hb 8.0 mmol/l (13.6 mg/ml), leucocytes 13.3/l, creatinine 50 μmol/l (eGFR>60 ml/min) , glucose 14.0 mmol/l,
NTproBNP 1620 pg/ml, hs-troponine I 0.043
Conclusion cardiologist: acute HFpEF triggered by pulmonary infection
Pulmonologist: exacerbation COPD ? Antibiotics, oral prednisolone, ß2-mimetics ?
diagnostic pitfalls with spirometry in HF COPD (GOLD-criteria) = Obstruction on spirometry
= FEV1/FVC <70% (or LLN)
acute HF (fluid overload): FEV1 more reduced than FVC
elevated interstitial pulmonary fluid pressure
pulmonary obstruction with spirometry !!
better to (also) perform bodyplethysmography (RV/TLC)
Gueder G, et al. J Card Fail 2012;18:637-644
diagnostic pitfalls with spirometry in HF (2) Should be done when ‘dry’: 3 months after hospitalization
stable non-acute HF: both FEV1 and FVC reduced with 20%, but
FEV1/FVC ratio may be used
(over-rating FEV1%pred !)
619 SHF (LVEF <40%) admitted for acute HF, 23% labeled COPD
After 6 months when ‘dry’: in 9% COPD (5% known, 4% new cases)
Brenner S et al. Int J Card 2013;168:1910-6. J Card Fail 2012;18:637-644

Therapeutic challenges in our case
Pre-hospital treatment options
• measure oxygen saturation
• 5 l/min oxygen (2 l/min in COPD patients)
• when systolic >90 mmHg; nitroglycerine sublingual
• furosemide 40 mg iv
• 2.5-5 mg morphine slowly iv (severe dyspnoea/agitation)
Other options for our case?
–
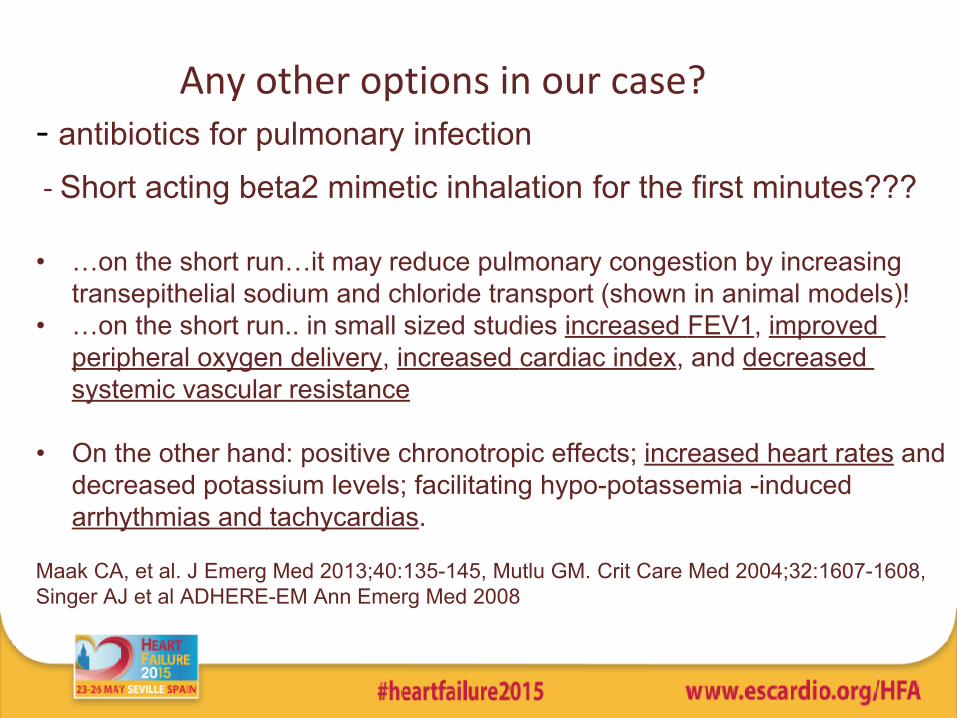
Any other options in our case? - antibiotics for pulmonary infection
- Short acting beta2 mimetic inhalation for the first minutes???
• …on the short run…it may reduce pulmonary congestion by increasing transepithelial sodium and chloride transport (shown in animal models)!
• …on the short run.. in small sized studies increased FEV1, improved peripheral oxygen delivery, increased cardiac index, and decreased systemic vascular resistance
• On the other hand: positive chronotropic effects; increased heart rates and decreased potassium levels; facilitating hypo-potassemia -induced arrhythmias and tachycardias.
Maak CA, et al. J Emerg Med 2013;40:135-145, Mutlu GM. Crit Care Med 2004;32:1607-1608,Singer AJ et al ADHERE-EM Ann Emerg Med 2008
When stable again; beta-blockers allowed?
practice study UK: >80% of HFrEF patients with COPD managed in HF outpatient clinic tolerated beta-blockers Shelton RJ, et al. Heart 2006;92:331-36.
But,
Beta-blockers might slightly reduce FEV1
- clinically irrelevan, but ….
another risk of overdiagnosing COPDGueder G et al EJHF 2014
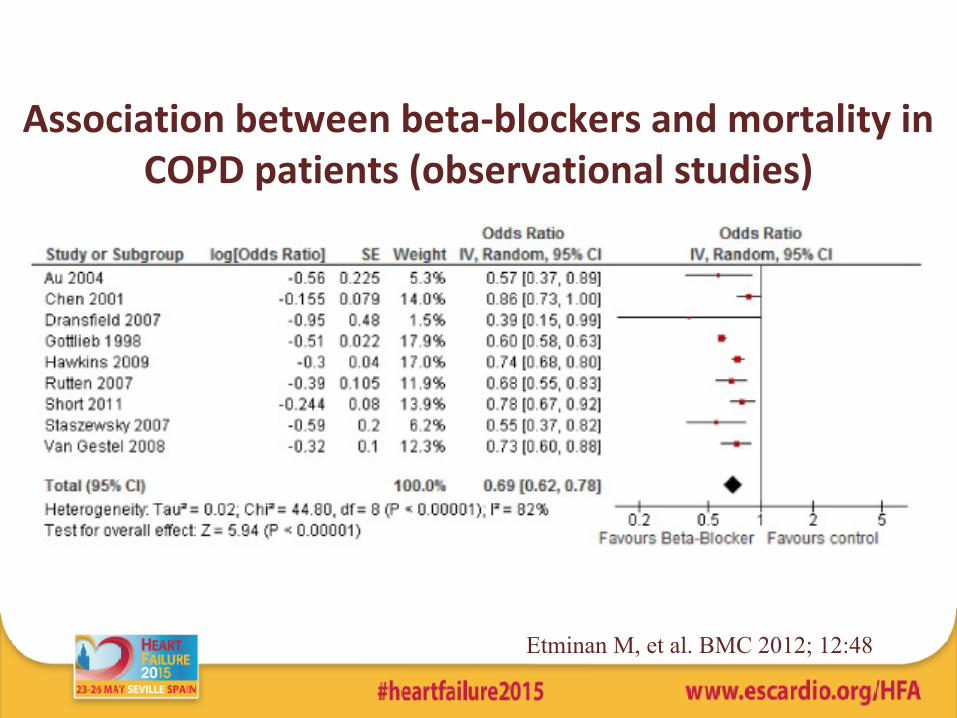
Association between beta-blockers and mortality in COPD patients (observational studies)
Etminan M, et al. BMC 2012; 12:48
Other cardiovascular drugs in COPD
Same story as for beta-blockers.
Also statins and ACEi and ARBs may reduce all-cause mortality
But, observational studies !!
Risk of (residual) confounding
1. Mancini GBJ et al. JACC 2006;47:2554-60 (ACE-i/ARBs, statins)
2. Soyeth V et al. Eur Resp J 2007;29:279-83 (statins)
Conclusions
• a label of COPD ≠ true COPD
• HF treatment on the first place before inhalers
• spirometry should be done when stable/euvolemic
• shortacting beta2-mimetics in acute HF (those wheezing)??
• near future; RCTs with CV drugs in COPD??
• when stabilised: not withhold HF patients from beta-blockers

Thank you for your attention





























