Embed Size (px)
Citation preview
1

2
CARE MANAGEMENT: Bending in the winds of
reformPatient-Centered Outcome-Driven
Dana Deravin Carr, Dr. PH, MPH, MS, RN-BC, CCMSenior Care Manager/ Transitions Coordinator

3
Common Themes
• Accountability• Sustainability• Efficiency – Care and System• Effectiveness – Cost, Care and System• Communication• Coordination• Collaboration• Leadership, Followership and Mentorship
4
What do we want to accomplish today?
Gain knowledge and understanding of: Trends associated with health care reform and identify
changes reflecting the new health care system including patient-centered deliverables
The concept of bending the cost curve The concept of DSRIP and the goals of the Triple AIM The difference between the Medical Care model vs PCMH
model The patient role in facilitating self-directed care See Motivational Interviewing as an important CM function in
promoting patient self empowerment and self advocacy

5
The Stormy Seas of Health Care

6
A CHANGING HEALTHCARE INDUSTRY
• Changes in Reimbursement practices– Fee For Service– Prospective Payment System– Managed Care
• Escalating Healthcare Cost– aging patient population– increases in chronic illness– Poorly managed behavioral health component– medical technological advances
complex, high tech and minimally invasive surgerylife-prolonging treatments
• Increased Patient Acuity • Shortened Hospital LOS
7
Pre-Reform Financial Trends• The cost crisis of our economy is due in most part to the
health care crisis– Of the two trillion dollars spent on US health care patients
with chronic diseases account for 75% of health care cost
•Of every dollar spent…75 cents went towards treating patients with one or more chronic illness AND
•In public programs, treatment of chronic diseases constitute an even higher portion of spending:

8
The great escape to no where…

9
• Silos - Compartmental• Provider Centered• Uncoordinated• Limited Health
Information sharing• Little meaningful
accountability for results (lack of transparency)
• Underinvestment in primary and preventative care
• System fails the most in need the most often
• Health care infrastructure that doesn’t match community need

10
US ranked last among the wealthiest nations:
1. United Kingdom2. Switzerland3. Sweden4. Australia5. Germany & Netherlands (tied)7. New Zealand & Norway (tied)9. France10. Canada11. United States

11
What we know…
• US healthcare is unsustainably expensive• As a nation we have terrible healthcare for
populations• Best healthcare in the world for few of the
very sick

12
The Call for Health Reform:
13
Health reform is largely built around the changing role of primary care
• If primary care is to be the hub of the health care wheel, instead of a feeder for the hospital and specialty system, it has to be enhanced.
How?• By changing and integrating systems• Developing models that support patient
centered care: PCMH and ACO’s• Innovation, technology and transparency
14
Moving towards VALUE
• By focusing on the “Health” in Health Reform Legislation we can show that:
• Better Health + Better Health Care = Greater Value (Higher Quality/Lower Cost
BH + BHC = GV (HQ/LC)
15
Providing Health Care NOT Sick Care
• Results oriented• Payments based on
delivering value to patients
• Continuum based collaborative care
• Rebalanced Health Care structure that meets the community’s need
• Integrated • Patient Centered• Coordinated• Accountable

16
17
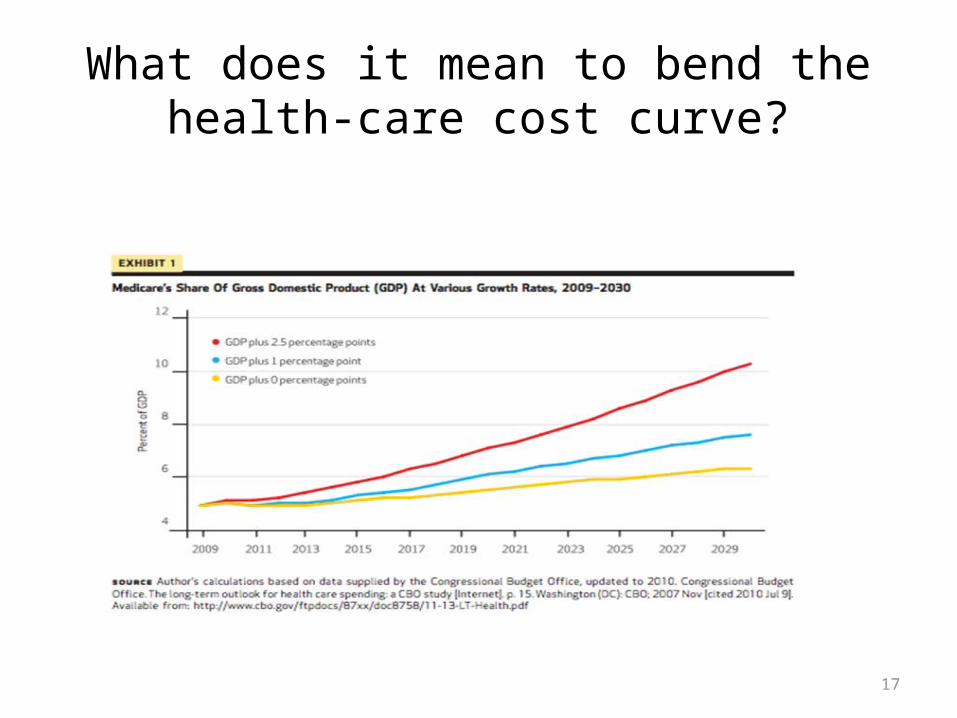
What does it mean to bend the health-care cost curve?
18
19
Evolving MEGA Trends in healthcare
Consumers take chargeThe insured consumer leads to increased
engagement and increased consumer responsibility
More with less – From Volume to ValueHealthcare everywhere – CVS. WalmartMega Health Systems – ConsolidationStates are key players – Medicaid transformed
through DSRIP
20
Trends in healthcare con’t
Integration of medical care, behavioral care, public health
Movement of high cost/high risk consumers into Managed Care
Value through data (clinical trials)Predict prevent and personalize (expanding the role
of life science)The New “AGED” will increase demand for caregiversGlobal Healthcare – medical tourism
21
10 Health Care Reform issues transforming case management
• Chronic disease management • Care transitions• Quality reporting requirements• ACO’s - embedded case management• Large DATA Expansion of health insurance• Primary care provider shortage – solutions--
condensed GME/ more physician extenders• State Action – DSRIP• Implementation Challenges
22
The Role of Case Managers in Emerging Care Delivery Models
• The changing landscape for care managers in Medical Homes and ACO’s
• Case Managers gaining increased recognition as facilitators of patient centered care
• Employ an empowering and supportive role with patients and caregivers
• Professional case management is a critical component of improving care coordination
• Embedding Case Managers into primary care

23
AND EVOLVE!
24
The 21st Century Care Manager
• Promotes collaborative partnerships with the entire health care team that includes the patient and their identified support system
• Continuously collaborates and communicates with Healthcare Team and the patient.
• Creates and implements a synchronized care plan that crosses the boundaries, promotes continuity and builds continuum based relationships
• Coordinates care and contemplates the patient holistically – including the social and psychological aspects
• Promotes Client self determination• Watches the fiscal bottom line regarding care and works with
the entire team to implement the best options

25
What skills and knowledge do you need to be even more successful as a 21st Century Care Manager?
• Step out of your comfort zone• Develop and build relationships• Find/Be a mentor• Understand the numbers• Value your work• Develop yourself professionally• Realign your goals to fit the new paradigm,
AND Develop a patient centered mentality

26
“More” does not mean “better”

27

28
Patient Centered Care
29
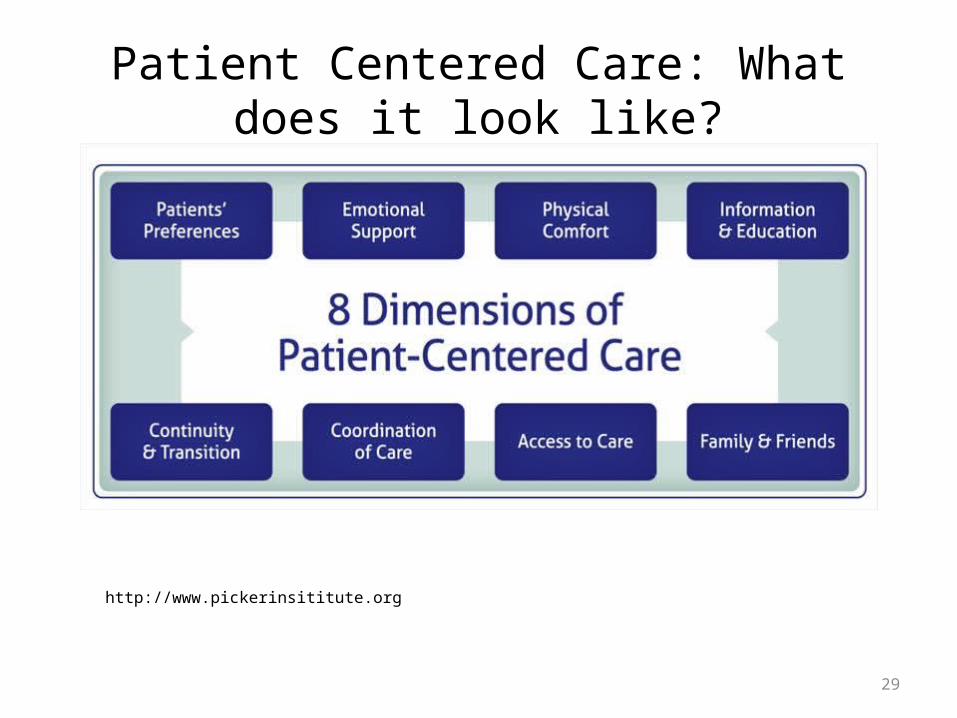
Patient Centered Care: What does it look like?
http://www.pickerinsititute.org

30
Medical Model vs. Patient Centered Model
31
By adopting a transition outlook that targets:
Medication Adherence Care Transitions Management Reducing Readmissions Case Management Patient-Centered Medical Home – Embedded Case
ManagementUnderstanding and Advancing Health LiteracyCoaching strategies that incorporate Motivational
Interviewing techniques
32
Empowering the patient’s voice
33
Nothing about Me without ME
• A patient is an individual to be cared for not a medical condition to be treated
• Treatment and care should take into account patient’s individual needs, preferences and ability to process and understand health information
• Good communication is essential supported by evidence based information to allow patients to reach informed decisions about their care.

34
Transforming the Conversation through Motivational Interviewing
• Encouraging patients to set and achieve goals for health maintenance and disease management
• Engaging patients in active (non-pharmacological) management of chronic pain
• Addressing issues of problematic alcohol, opiate, and other drug use
• Improving patient's medication adherence• Promoting engagement in other evidence based
behavior changes approaches, such as Cognitive-Behavioral Therapy
35
Principles of MI
• Expressing empathy• Supporting self efficacy• Rolling with resistance• Developing discrepancy

36
Strategies of MI
• Open ended questions• Affirmations• Reflective Listening• Summary Statements
37
A Patient’s Voice
“I would tell them that they need to write it – not in cursive, in print, and to use small words so I can read it.
You see, I can hardly understand those real big words. You have to break down the syllables to understand the big
words.”
If you had any advice to people that work in the clinic to make information they give you easier to understand, what
would you tell them to do?
*Used with permission

38
39

40
Delivery System Reform Incentive Payment (DSRIP)• States establish a framework for projects and objectives that
Center for Medicare and Medicaid Services (CMS) approves.
• Entities eligible for DSRIP funds select targets and approaches from this framework, and shape a tailored plan on how their entity will meet those goals. This plan must receive state and federal approval.
• A reporting structure is assembled, activities conducted, and data driven progress reports are is provided to the state.
• Some DSRIPs require hospitals to partner with other providers to be eligible for funds. This establishes a common financial interest and alignment across providers to affect change.
41
Core Strategies
1. Care Management for all2. Global Spending Cap3. Health Homes4. High Quality Primary Care for All5. Address the Social Determinants of Health6. Promote Health Literacy across the
continuum

42
What is happening in NYS?
43
Delivery System Reform Incentive Payment (DSRIP)
• Started as Medicaid Redesign Team Waiver Amendment 2011
• Now restructured to DSRIP—incorporates Behavioral Health, Long term care workforce, and Home health development.– Criteria for participation – hospitals must be public , critical
access or sole community hospital– Minimum threshold of Medicaid, uninsured and dual eligible
patient volume – 30% inpatient and 35% outpatient OR – Hospital serving more than 30% of MA, dual eligible or
uninsured in a county or multiple county region– Must be a safety-net provider

44
What is the Current State of NYC HHC
• Complicated delivery system - . The NYC public health hospital corporation comprises 11 public hospitals, six SNF’s one home health agencies spans five boroughs and serves over 250 languages.
• Complex system leads to failure to deliver appropriate level of care, over utilization and ED services and repeated readmissions
• DSRIP Provides and opportunity to provide transformational change

45
HHC Program Goals (1)
• Build Health Literacy
– 2/3rds of U.S. adults ≥ 60 yo have inadequate or marginal literacy skills
– 81% of patients ≥ 60 yo at a public hospital could not read or understand basic materials such as prescription labels
46
Appointment Reminders
Phone Follow-Up
Confirm Understanding
(Teach-Back Method)
Treatment Simplification
Shared Decision-Making
Medication Review (Brown
Bag)
Kind, Supportive
Staff
Health Literacy Best
Practices
47
HHC Program Goals (2)
• Build Care Teams that include the patient• Engage physicians and the team in the work
flow processes • Mentor and support patients• Affect population health by building self
efficacy and self esteem

48
“High Risk Transitional Care Teams”
•Identify using combination of clinical and non-clinical criteria
•In safety net – use a multi-disciplinary team
•Address full complement of medical, social, logistical needs
•Don’t over medicalize – whole person, psychosocial
49
Jacobi Medical Center

50
What keeps you up at night?
The Scream..Edward Munch, 1893

51
Dr. Dana’s Transitional Care Heart Failure Project

52
The Portrait of Heart Failure
53
Project 2.b.iv: Care Transitions Intervention Model
• 30- day supported transition period after hospitalization for patients at high risk of readmission, particularly those with cardiac, renal, DM, respiratory, and/or behavioral health dx
• Transition case manager working 1:1• Identify risks/barriers and find solutions
54
Transforming Care at the Bedside

55
Communication is fundamental
56
Continuing Patient Centered Care Post Discharge
57
Strengthen weak linkages by adopting a transition outlook that:
Supports the patient throughout the 30-day high risk period
Emphasizes patient/caregiver educationSupports Medication Adherence Builds patient centered collaborative relationships Reduces ED visits and Readmissions Empowers and encourages patient/caregivers to take
an active role in their careBuilds Health Literacy

58
Post discharge calls & care coordination
• Within 72 hours of discharge • Over a 30 day period, the Care Manager will:
– Confer with Home Care Provider after initial visit for medication reconciliation, plan of care and planned visit frequency
– Collaborate with PCP and care team to resolve problems and provide clinical updates
– Educate patient regarding disease processes and care interventions
– Promote self directed care, ensure access to care and empower patients to facilitate problem solving

59
Discharge from Care Transitions Program
• Patient will be discharged from Care Transition Program:– If Patient/caregiver request discontinuation of
Care Transition services– If Patient is admitted to an inpatient setting
• Patient no longer requires this level of intervention as evidenced by:
60
Patient no longer requires this level of intervention as evidenced by:
• Patient/caregiver ability to self-manage• Goals of care have been achieved or patient is
progressing to desired state• Patient has established community Primary
Care Provider engagement• Risk reduction interventions that address risk
factors implemented
61
Ensure a warm “hand off” to the next provider

62
This looks like a good outcome

63
This is the IDEAL State..
64
And perhaps for some of us….THE BOOMERS..to this “IDEAL” state!

65

66
References• Auslander,E. & Carneal, G. (2013). 10 healthcare reform issues
transforming case management. Case –In – Point. 11(11) p. 1.• Chernof, B. (2014) Achieving Patient Centered Care. United Hospital
Fund.• Congressional Budget Office (2010). The long-term outlook for
healthcare spending: A CB study. Retrieved from http://www.cbo.gov • NPR Blogs (2014) A hospital reboots medicaid to give better care for less
money. Retrieved http://www.npr.org/blogs/health/2014• United Hospital Fund (2014). A professional coordinators guide to
partnering with family caregivers. Retrieved from http://www.nextstepincare.org
• Altman, D. (2014) A Perilous Gap in Health Insurance Literacy. The Wall Street Journal. Retrieved from http://blogs.wsj.com/washwire/2014/09/04/a-perilous-gap-in-health-insurance-literacy/

67
PCMH ACO
• Personal physician, focus on patient-physician relationship (single practice)
• Physician-led team• Whole person model of care,
patient and family-centered• Enhanced access to care• Care coordinated, integrated• Comprehensive, continuous care• Continuous improvement• Quality and safety, guide all care
individual/population• Payment supports patient-
centered care, and is value driven
• Provider-led organization, multiple providers, practices organized
• Culture of teamwork• Complete and timely information about
patients and services provided • Resources & support for patient education
and self management• Coordinated relationships of PCP with
specialists and other providers• Population based continuum of care
management• Accountable for quality and safety• Technology and skills for population
management and coordination of care• Ability to measure and report on quality• Accountable for overall costs• Infrastructure and skills for management of
financial risk• Leaders committed to improving value of
health care services





























