Embed Size (px)
Citation preview

1
Anxiety in practice
Diagnosis and management

2
What is ‘anxiety’?
A normal feeling: transient, disagreeable emotional state, may be adaptive, signals anticipated threat, initiates action.
A symptom: seen in wide variety of disorders,
A disorder: in which anxiety symptoms form a dominant element.

3
How do the patients describe their feelings of anxiety?As an intense negative emotion, patients will use
words as –tense, panicky, terrified, jittery, nervous, wound-up, apprehensive, worried etc.
Different symptoms of anxiety:
Somatic – subjective like twitching, tremors, hot and cold flashes, sweating, palpitations, chest tightness, difficulty swallowing, nausea, diarrhoea, dry mouth, decreased libido etc.
Cognitive- hyper vigilance, poor concentration, subjective confusion, fears of loosing control, or going crazy, catastrophic thinking etc.

4
Behavioural symptoms-fearful expressions, withdrawal, irritability, immobility, hyperventilation etc.
Perceptual disturbance- depersonalization, derealisation, hyperesthesia especially hyperacusis.
5
A few terms:
Trait anxiety: lifelong pattern of anxiety as a feature of temperament.
Free floating anxiety: persistently anxious mood in which cause is unknown, and in which large number of diverse thoughts and events trigger and compound the anxiety.
Situational anxiety: only in relation to specific occasions or external stimuli as in phobias.
Existential:being aware of its possible non-being
Ontic(fate and death),moral(guilt and condemnation) and spiritual(emptiness and meaninglessness)

6
Physical conditions presenting as anxiety stateMedical diseases: brain tumours in temporal lobe
or 3rd ventricle region, stroke, migraine, encephalitis, MS, epilepsy, Alzheimer's, Parkinson's, Huntington's and Wilsons’ disease
Hypoxia, hypoglycemia, hyperthyroidism, cushing’s syndrome, mitral valve prolapse.
Medications/drugs- cocaine, sympathomimetics eg. Amphetamines, caffeine, lidocaine, alcohol & sedative withdrawal.

7
Primary vs Secondary anxiety
Secondary anxiety as a response to an underlying condition- a psychotic disorder, depressions, substance related disorders.
Anxiety and depression: coexistence is substantial,
Anxiety symptoms such as anxious mood and irritability seen in majority of depressed patients,
2/3 rd patients with Panic disorders will become depressed in their life time.
8
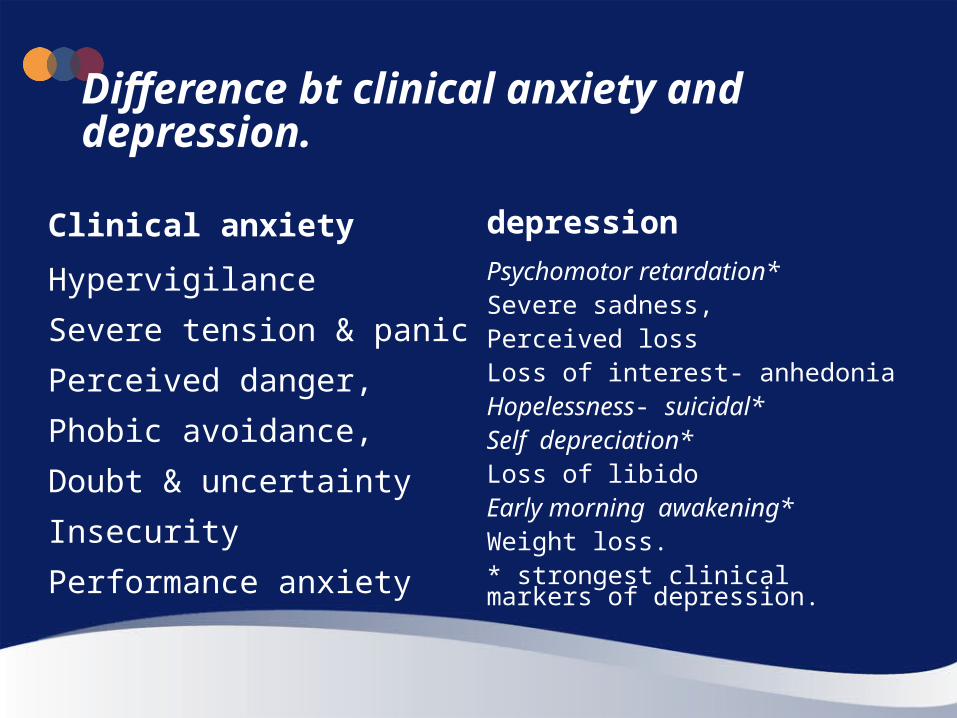
Difference bt clinical anxiety and depression.
Clinical anxiety depression
Hypervigilance
Severe tension & panic
Perceived danger,
Phobic avoidance,
Doubt & uncertainty
Insecurity
Performance anxiety
Psychomotor retardation*Severe sadness,Perceived lossLoss of interest- anhedoniaHopelessness- suicidal*Self depreciation* Loss of libidoEarly morning awakening*Weight loss.* strongest clinical markers of depression.

9
Neurobiological mechanism of anxiety Amygdala: ‘fear reaction’ in animal models,
nerve projections from amygdala activates central autonomic nervous system of brain– behavioural and physiological manifestation of acute anxiety.
Hypothalamus-pituitary- adrenal axis: following early separation distress.
‘GAD: abnormal GABA in central BDZ receptors.

10
‘Panicogens’: genetically predisposed and traumatised by early separation distress people respond with acute panic attack with sod. Lactate infusion, co2, doxapram.
Hippocampus: neuronal degeneration Glucocoticoid effects- explains memory problems in PTSD.

11
Different anxiety disorders:
PANIC DISORDER AND AGORAPHOBIA: recurrent panic attacks.
The panic attack : an episode of abrupt intense fear that is accompanied by autonomic or cognitive symptoms: palpitations, sweating, trembling or shaking, sensations of shortness of breath or smothering, feeling of choking, chest pain or discomfort, nausea or abdominal distress, feeling dizzy, unsteady, lightheaded, or faint, derealization (feelings of unreality) or depersonalization (being detached from oneself), fear of losing control or going crazy,fear of dying, paresthesias (numbness or tingling sensations), chills or hot flushes

12
Phobic Anxiety Disorders
Agoraphobia
A. There is marked and consistently manifest fear in, or avoidance of, at least two of the following situations:
(1) crowds;
(2) public places;
(3) traveling alone;
(4) traveling away from home.

13
Phobic Anxiety DisordersAgoraphobiaThere is marked and consistently manifest fear in, or avoidance of, at least two of the following situations:(1) crowds;(2) public places;3) traveling alone;(4) traveling away from home.B. At least two symptoms of anxiety in the feared situation Autonomic arousal symptoms(1) palpitations or pounding heart, or accelerated heart rate;(2) sweating; (3) trembling or shaking;(4) dry mouth (not due to medication or dehydration);
Symptoms involving chest and abdomen(5) difficulty in breathing;(6) feeling of choking;(7) chest pain or discomfort;(8) nausea or abdominal distress (e.g., churning in stomach);
Symptoms involving mental state(9) feeling dizzy, unsteady, faint, or light-headed;(10) feelings that objects are unreal (derealization), or that the self is distant or "not really here" (depersonalization);(11) fear of losing control, "going crazy," or passing out;(12) fear of dying;General symptoms(13) hot flushes or cold chills;(14) numbness or tingling sensations.
14
SPECIFIC AND SOCIAL PHOBIAS:"phobia" refers to an excessive fear of a specific object, circumstance, or situation.
Both require the development of intense anxiety, to the point of even situationally bound panic, upon exposure to the feared object or situation.
Also require that fear either interferes with functioning or causes marked distress.
Finally, both conditions require that an individual recognizes the fear as excessive or irrational and that the feared object or situation is either avoided or endured with great difficulty.

15
Obsessive-Compulsive Disorder:
Obsessions as defined by recurrent and persistent thoughts, impulses, or images that are experienced, at some time during the disturbance, as intrusive and inappropriate and that cause marked anxiety or distress,
Compulsions as defined by repetitive behaviors (e.g., hand washing, ordering, checking) or mental acts (e.g., praying, counting, repeating words silently) that the person feels driven to perform in response to an obsession, or according to rules that must be applied rigidly.

16
PTSD

17
SUBSTANCE-INDUCED ANXIETY AND ANXIETY DUE TO A GENERAL MEDICAL CONDITION
prominent anxiety that arises as the direct result of some underlying physiological perturbation.
clinically significant symptoms of panic, worry, phobia, or obsessions emerge in the context of prescribed or illicit substance use.
For example, panic attacks have been tied to various medical conditions, including endocrinologic, cardiac, and respiratory illnesses.

18
Anxiety Disorder Not Otherwise Specified
This category includes disorders with prominent anxiety or phobic avoidance that do not meet criteria for any specific anxiety, disorder, adjustment disorder with anxiety, or adjustment disorder with mixed anxiety and depressed mood.
Examples include
1. Mixed anxiety-depressive disorder:
2. Clinically significant social phobic symptoms that are related to the social impact of having a general medical condition or mental disorder (e.g., Parkinson's disease, dermatological conditions, stuttering, anorexia nervosa, body dysmorphic disorder).
3. Situations in which the clinician has concluded that an anxiety disorder is present but is unable to determine whether it is primary, due to a general medical condition, or substance induced.

19
GENERALIZED ANXIETY DISORDER: a pattern of frequent, persistent worry and anxiety that is out of proportion to the impact of the event or circumstance that is the focus of the worry .
For example, while college students often worry about examinations, a student who persistently worries about failure despite consistently outstanding grades displays the pattern of worry typical of generalized anxiety disorder.
Patients with generalized anxiety disorder may not acknowledge the excessive nature of their worry, but they must be bothered by their degree of worry.
This pattern must occur "more days than not" for at least 6 months.

20
Case studies: 1
Ms. S. was a 25-year-old student who was referred for a psychiatric evaluation from the medical emergency room at a larger university-based medical center.
Ms. S. had been evaluated three times over the preceding 3 weeks in this emergency room.
Her first visit was prompted by a paroxysm of extreme dyspnea and terror that occurred while she was working on a term paper. The dyspnea was accompanied by palpitations, choking sensations, sweating, shakiness, and a strong urge to flee. Ms. S. thought that she was having a heart attack, and she immediately went to the emergency room.
She received a full medical evaluation, including an electrocardiogram (ECG) and routine blood work, which revealed no sign of cardiovascular, pulmonary, or other illness.
Although Ms. S. was given the number of a local psychiatrist, she did not make a follow-up appointment, since she did not think that her episode would recur.
She developed two other similar episodes, one while she was on her way to visit a friend and a second that woke her up from sleep. She immediately went to the emergency room after experiencing both paroxysms, receiving full medical workups that showed no sign of illness.-

21
Diagnosis:
Panic disorder:
22
Case study: 2
Mr. A. was a successful businessman who presented for treatment following a change in his business schedule. While he had formerly worked largely from an office near his home, a promotion led to a schedule of frequent out-of-town meetings, requiring weekly flights.
Mr. A. reported being "deathly afraid" of flying. Even the thought of getting on an airplane led to thoughts of impending doom as he envisioned his airplane crashing to the ground.
These thoughts were associated with intense fear, palpitations, sweating, clammy feelings, and stomach upset. While the thought of flying was terrifying enough, Mr. A. became nearly incapacitated when he went to the airport. Immediately before boarding, Mr. A. often had to turn back from the plane and run to the bathroom to vomit.

23
Diagnosis:
Specific phobia.

24
Case study:3Ms. B. presented for psychiatric admission after being transferred from a medical
floor where she had been treated for malnutrition.
Ms. B. had been found unconscious in her apartment by a neighbor. When brought to the emergency room by ambulance, she was found to be hypotensive and hypokalemic.
At psychiatric admission, Ms. B. described a long history of excessive cleanliness, particularly related to food items.
She reported that it was difficult for her to eat any food unless it had been washed by her three to four times, since she often thought that a food item was dirty. She reported that washing her food decreased the anxiety she felt about the dirtiness of food.
While Ms. B. reported that she occasionally tried to eat food that she did not wash (e.g., in a restaurant), she became so worried about contracting an illness from eating such food that she could no longer dine in restaurants. Ms. B. reported that her obsessions about the cleanliness of food had become so extreme over the past 3 months that she could eat very few foods, even if she washed them excessively.
She recognized the irrational nature of these obsessive concerns, but either could not bring herself to eat or became extremely nervous and nauseous after eating.
25
Diagnosis
OCD:
26
Case study:4
Mr. F. sought treatment for symptoms that he developed in the wake of an automobile accident that had occurred about 6 weeks prior to his psychiatric evaluation.
While driving to work on a mid-January morning, Mr. F. lost control of his car on an icy road. His car swerved out of control into oncoming traffic in another lane, collided with another car, and then hit a nearby pedestrian. Mr. F. was trapped in his car for 3 hours while rescue workers cut the door of his car.
Upon referral, Mr. F. reported frequent intrusive thoughts about the accident, including nightmares of the event and recurrent intrusive visions of his car slamming into the pedestrian.
He reported that he had altered his driving route to work to avoid the scene of the accident, and he found himself switching the television channel whenever a commercial for snow tires appeared. Mr. F. described frequent difficulty falling asleep, poor concentration, and an increased focus on his environment, particularly when he was driving.
27
Diagnosis:
PTSD

28
Case study: 5Ms. X. was a successful, married, 30-year-old attorney who
presented for a psychiatric evaluation to treat growing symptoms of worry and anxiety.
For the preceding 8 months, Ms. X. had noted increased worry about her job performance. For example, while she had always been a superb litigator, she increasingly found herself worrying about her ability to win each new case she was presented. Similarly, while she had always been in outstanding physical condition, she increasingly worried that her health had begun to deteriorate.
Ms. X. noted frequent somatic symptoms that accompanied her worries. For example, she often felt restless while she worked and while she commuted to her office, thinking about the upcoming challenges of the day.
She reported feeling increasingly fatigued, irritable, and tense.
She noted that she had increasing difficulty falling asleep at night as she worried about her job performance and impending trials.-

29
Diagnosis:
GAD:

30
Generalized Anxiety Disorder

31
GAD: Content Overview• GAD Background
— Epidemiology— Burden of illness— Treatment— Diagnosis
• Pregabalin Pharmacokinetics
• Pregabalin in GAD— Overview of clinical program— Efficacy— Tolerability and safety
32
GAD Epidemiology
General Population, Primary Care Setting, and Comorbidities

33
GAD Symptoms: Prevalence Estimates in the General Population
Prevalence (n=9282)
Duration of anxiety symptoms (minimum) Point (current) 1-year Lifetime
1 month* 2.6% 5.5% 12.7%
3 months* 2.1% 3.9% 8.0%
6 months (DSM-IV GAD)
1.8% 2.9% 6.1%
12 months(DSM-IV GAD)
1.6% 2.2% 4.2%
*Anxiety symptoms fulfilling DSM-IV criteria for GAD, except for durationData from NCS-R (DSM-IV criteria), USA Kessler et al. Psychological Med. 2005;35:1073-1082.
34
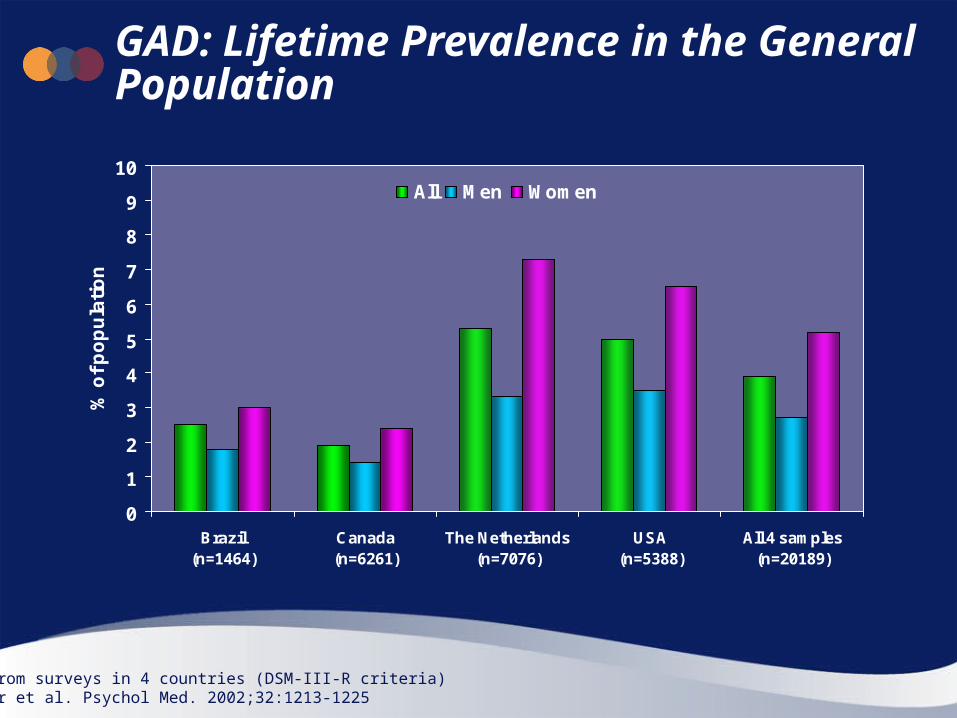
GAD: Lifetime Prevalence in the General Population
0
1
2
3
4
5
6
7
8
9
10
Brazil (n=1464)
Canada (n=6261)
The Netherlands(n=7076)
USA (n=5388)
All 4 samples(n=20189)
% o
f p
op
ula
tio
n
All Men Women
Data from surveys in 4 countries (DSM-III-R criteria)Kessler et al. Psychol Med. 2002;32:1213-1225

35
Lifetime Prevalence of GAD in the General Population by Age and Gender
0
5
10
15
15–24 25–34 35–44 > 45
Age (years)
Lif
eti
me
pre
va
len
ce
(%
)
Women
All
Men
Data from NCS (DSM-III-R criteria), USAWittchen et al. Arch Gen Psychiatry 1994;51:355-364

36
Anxiety Disorders in Primary Care: Point Prevalence Estimates
3.7
1.52.6
2
8.5
3.1
7
11.8
0
5
10
15
20
GAD Panic disorder Social anxietydisorder
PTSD
Po
int
pre
va
len
ce
(%
)
Lowest estimate Highest estimate
Stein. J Clin Psychiatry. 2003;64(suppl 15):35-39

37
Prevalence of GAD Symptoms in the Primary Care Setting
0
5
10
15
20
25
30
35
40
% o
f p
ati
en
ts
All (n=17,739) Men (n=7,274) Women (n=10,465)
GAD symptoms 1-4 weeks
GAD symptoms >6 months
(DSM-IV GAD)
Anxiety symptoms fulfilling DSM-IV for GAD criteriaWittchen et al. J Clin Psychiatry. 2002;63(suppl 8):24-34

38
GAD Symptoms Present Across the Age Spectrum in Primary Care Setting
20.3 21.123.3 23.2 23.3
19.8 19.3 19.5
5.66.6
6.8 7 6.6
2.7 2.4 3.1
0
5
10
15
20
25
30
35
40
16-19 20-29 30-39 40-49 50-59 60-69 70-79 80+
Age (years)
% o
f p
ati
en
ts
GAD DSM-IV diagnosis
*Anxiety symptoms
*Anxiety symptoms fulfilling DSM-IV GAD criteria, except for duration Based on sample of n=17,739Wittchen et al. J Clin Psychiatry. 2002;63(suppl 8):24-34
39
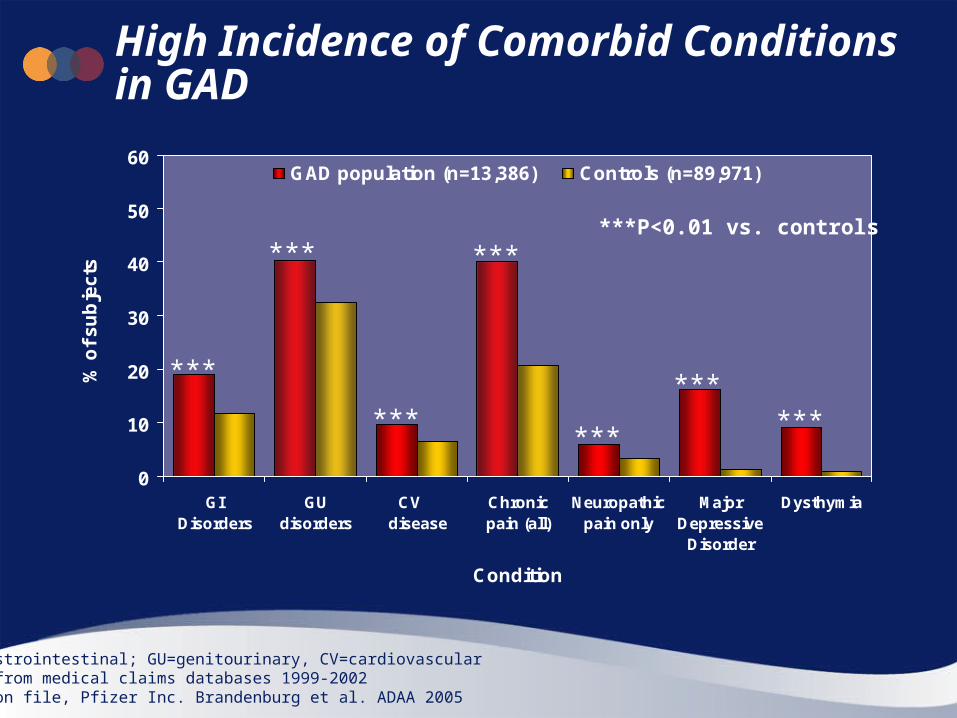
High Incidence of Comorbid Conditions in GAD
0
10
20
30
40
50
60
GI Disorders
GUdisorders
CV disease
Chronicpain (all)
Neuropathicpain only
MajorDepressive
Disorder
Dysthymia
Condition
% o
f s
ub
jec
ts
GAD population (n=13,386) Controls (n=89,971)
GI=gastrointestinal; GU=genitourinary, CV=cardiovascularData from medical claims databases 1999-2002 Data on file, Pfizer Inc. Brandenburg et al. ADAA 2005
***
***
***
***
***
******
***P<0.01 vs. controls

40
Lifetime Prevalence of Comorbid Psychiatric Disorders in Patients with GAD
34
38
61
72
22
34
58
0 10 20 30 40 50 60 70 80 90 100
Substance abuse/dependence
Dysthymia
Major depression
Any mood disorder
Panic disorder
Social phobia
Any other anxietydisorder
% of population with GAD
Data from international surveys in 4 countries (DSM-III-R criteria)Subset of population with GADKessler et al. Psychol Med. 2002;32:1213-1225

41
GAD Often Precedes the Development of Other Psychiatric Disorders
52
25
21
29
16
22
25
0 10 20 30 40 50 60 70 80 90 100
Substance abuse/dependence
Dysthymia
Major depression
Any mood disorder
Panic disorder
Social phobia
Any other anxietydisorder
% of population with GAD
Data from international surveys in 4 countries (DSM-III R criteria)Kessler et al. Psychol Med. 2002;32:1213-1225
Subset of those with GAD + comorbid disorder: GAD occurred first

42
GAD: Comorbidity, Presentation and Course of Illness

43
GAD: A Common Comorbid Condition
— Major depression1-4
— Panic disorder1-3
— Social phobia1
— Specific phobia1
— Post-traumatic stress disorder2
— Chronic pain conditions4
— Chronic fatigue syndrome2
— Gastrointestinal disease5
— Irritable bowel syndrome2,5
— Hypertension2
— Heart disease2
• GAD is one of the most common conditions that occurs comorbidly with other disorders
— 91% of patients with GAD have ≥1 additional diagnosis1
• GAD occurs comorbidly with many medical and psychiatric conditions, including:
1. Sanderson. J Nerve Ment Dis. 1990;178:588-591 2. Stein. J Clin Psychiatry 2001;62(suppl 11):29-34; 3. Keller. J Clin Psychiatry 2002;63(suppl 8):11-16 4. Data on file Pfizer Inc; 5. Sareen et al. Depress Anxiety 2005;21:193-202

44
Physical Symptoms May Predominate in GAD• Aches, pains, soreness
• Insomnia (difficulty falling asleep)
• Symptoms of autonomic arousal— Tachycardia, palpitations, sweating, tremor
• Gastrointestinal symptoms— Nausea, diarrhea
• Other— Dizziness, light-headedness— Breathing difficulties— Numbness, tingling— Hot or cold flushes
Starcevic. Anxiety Disorder in Adults. Oxford University Press. 2005:102-140Gorman. Clin Cornerstone. 2001;3(3):37-43

45
Most Patients with GAD do NOT Present with Anxiety as the Primary Complaint
0
10
20
30
40
50
60
Anxiety Somaticillness/
complaints
Pain Sleepdisturbance
Depression
% o
f p
ati
en
ts w
ith
GA
D
Based on sample of n=17,739; 5.3% with GAD (DSM-IV)Wittchen et al. J Clin Psychiatry. 2002;63(suppl 8):24-34
Only 13% had anxiety as primary complaint
46
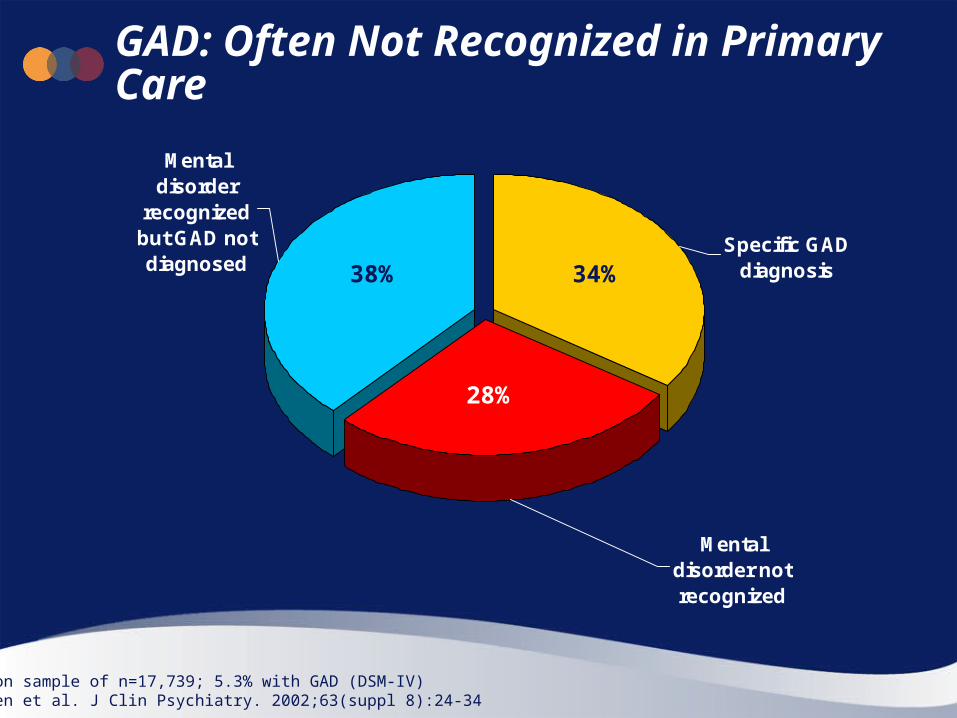
GAD: Often Not Recognized in Primary Care
Mental disorder not recognized
Specific GAD diagnosis
Mental disorder
recognized but GAD not diagnosed
34%38%
28%
Based on sample of n=17,739; 5.3% with GAD (DSM-IV)Wittchen et al. J Clin Psychiatry. 2002;63(suppl 8):24-34

47
GAD Course of Illness
• Chronic — Waxing and waning of symptoms1
— Low rates of remission over long term1,2
• Intermittent exacerbations — Exaggerated response to stress1,3
• Symptom overlap with medical and psychiatric disorders3
— Many are undiagnosed4
• Episodes may be more persistent with age5
• Poorer outcomes in patients with psychiatric comorbidities6
1. Starcevic. Anxiety Disorder in Adults. Oxford University Press. 2005:102-1402. Yonkers et al. Depress Anxiety. 2003;17:173-9; 3. Stein. J Clin Psychiatry 2003.64(suppl 15):35-39; 4. Wittchen et al. J Clin Psychiatry. 2002;63(suppl 8):24-34; 5. Wittchen et al. Arch Gen Psychiatry 1994;51:355-364; 6. Bruce et al. Am J Psychiatry. 2005;162:1179-87

48
Low Probability of Remission in GAD
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
1 (n=167) 2 (n=133) 3 (n=111) 4 (n=91) 5 (n=73)
Years since index episode
Pro
bab
ilit
yProbability of full remission
Full remission: PSR <3 for 8 weeks following index episode HARP 5-year prospective studyYonkers et al. Br J Psychiatry. 2000;176:544-549

49
Low Probability of Remission in GAD in Men and Women
0
0.2
0.4
0.6
0.8
1
0 1 2 3 4 5 6 7 8
Years since index episode
Pro
ba
bili
ty o
f re
mis
sio
n
Men (n=48)
Women (n=119)
P=0.24 test for gender difference
Full remission: PSR <3 for 8 weeks following index episodeHARP 8-year prospective studyYonkers et al. Depress Anxiety. 2003;17(3):173-179

50
GAD: Burden of Illness

51
GAD Patients in Primary Care: Difficulty with Usual Activities in Past 4 Weeks
A little difficulty26%
No difficulty16%
Much difficulty26%
Some difficulty30%
Incapacitated2%
Data from PCAP (n=142), USAMaki et al. 2003. APA Presentation
Over 50% of patients had at least some difficulty
52
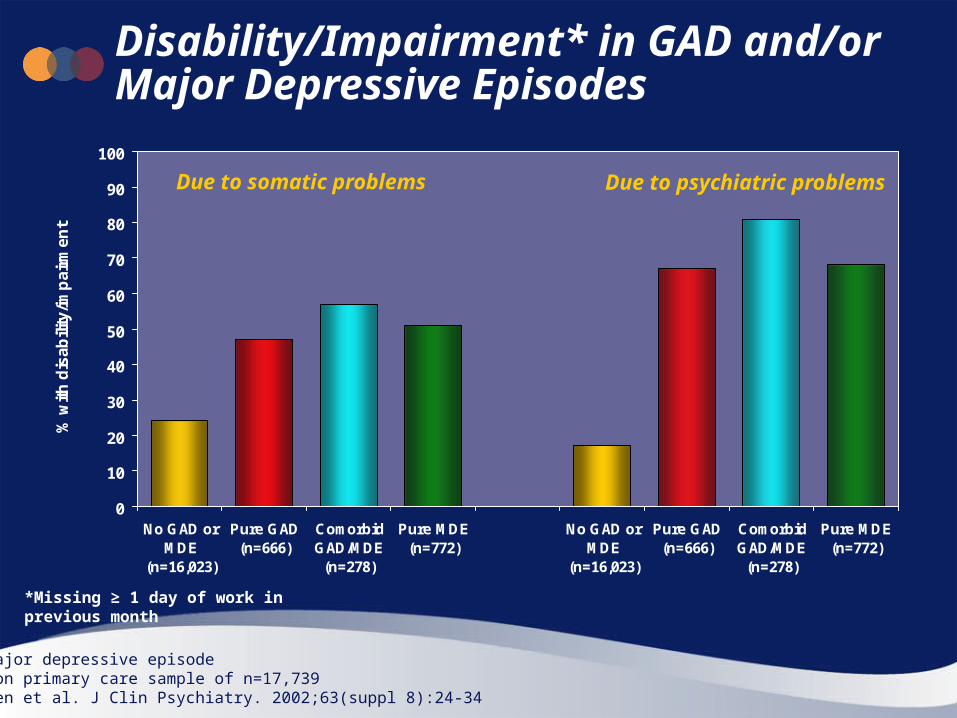
Disability/Impairment* in GAD and/or Major Depressive Episodes
0
10
20
30
40
50
60
70
80
90
100
No GAD orMDE
(n=16,023)
Pure GAD(n=666)
ComorbidGAD/MDE
(n=278)
Pure MDE(n=772)
No GAD orMDE
(n=16,023)
Pure GAD(n=666)
ComorbidGAD/MDE
(n=278)
Pure MDE(n=772)
% w
ith
dis
ab
ility
/imp
air
me
nt
MDE: major depressive episodeBased on primary care sample of n=17,739Wittchen et al. J Clin Psychiatry. 2002;63(suppl 8):24-34
Due to somatic problems Due to psychiatric problems
*Missing ≥ 1 day of work in previous month

53
Work Impairment in GAD and Other Chronic Conditions
0
2
4
6
8
10
12
14
GAD MDD Hypertension Arthritis Asthma Diabetes
Me
an
da
ys
Days work impairment in past month
Data from Midlife Development in the US survey (MIDUS)Work impairment based on work-loss days and work-cutback daysKessler et al. 2001. In: Rossi AS, editor. Chicago: University of Chicago Press. pp403-426

54
Patients with GAD Report Greater Work Impairment than Patients with MDD
0
10
20
30
40
50
60
70
No GAD orMDD (n=3764)
Pure GAD(n=33)
ComorbidGAD/MDD
(n=40)
Pure MDD(n=344)
% o
f re
spo
nd
ents
% with work days lost/impaired in past month
0
2
4
6
8
No GAD orMDD (n=3764)
Pure GAD(n=33)
ComorbidGAD/MDD
(n=40)
Pure MDD(n=344)
Wo
rk d
ays
lost
Average work days lost in past month
Wittchen et al. Int Clin Psychopharmacol. 2000;15:319-328
55
0
10
20
30
40
50
60
70
80
90
100
Generalhealth
Physicalfunction
Physicalrole
Bodily pain Mentalhealth
Socialfunction
Emotionalrole
Vitality
Me
an
SF
-36
sc
ore
No GAD or MDD
Pure MDD
Comorbid GAD/MDD
Pure GAD
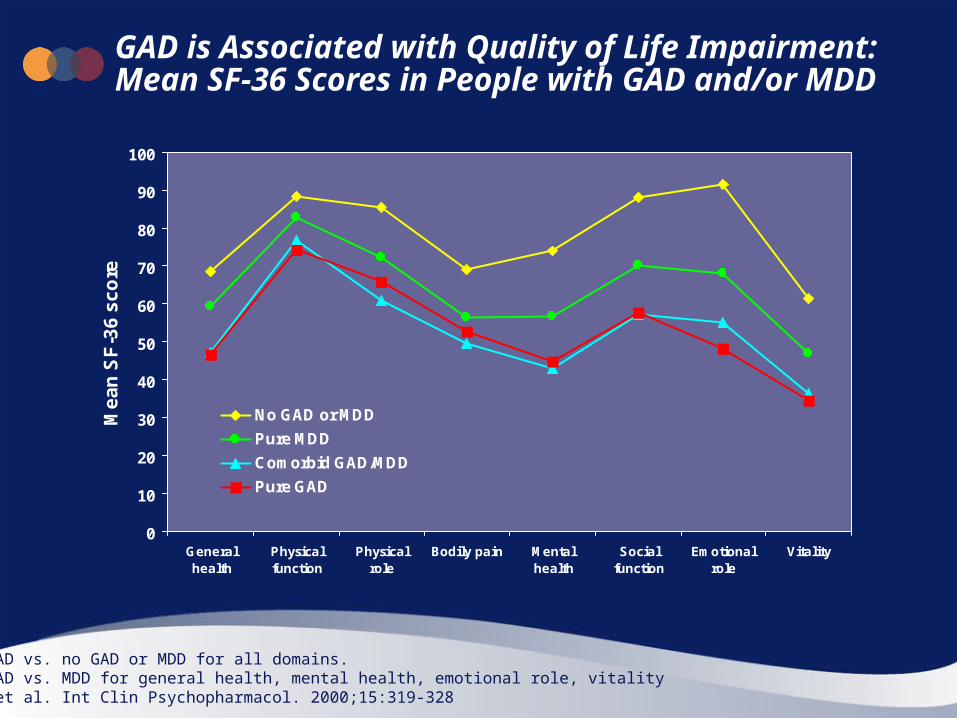
GAD is Associated with Quality of Life Impairment: Mean SF-36 Scores in People with GAD and/or MDD
P<0.05: GAD vs. no GAD or MDD for all domains.P<0.05: GAD vs. MDD for general health, mental health, emotional role, vitalityWittchen et al. Int Clin Psychopharmacol. 2000;15:319-328

56
Increased Healthcare Utilization in GAD
7
1415
23
4
0
4
8
12
16
20
24
No GAD or MDE Pure GAD GAD + MDE
Av
era
ge
nu
mb
er
of
vis
its
/ye
ar
Primary care Specialist (outpatient)
Average number of visits in past year
MDE: major depressive episodeBased on primary care sample of n=17,739Wittchen. Depress Anxiety. 2002;16(4):162-171
(n=16,023) (n=666) (n=278)

57
Patients with GAD Have as Many Doctor Visits as Patients with Depression
0
10
20
30
40
50
60
70
80
4+ to PCPs 2+ to other specialists Psychiatrist
Doctors visited in the past year
% o
f re
sp
on
de
nts
No GAD or MDE (n=16,023)
Pure GAD (N=666)
GAD + MDE (n=278)
Pure MDE (n=772)
MDE: Major Depressive EpisodeWittchen et al. J Clin Psychiatry. 2002;63(suppl 8):24-34

58
Number of Concurrent Psychiatric Disorders† in GAD Patients
34
27
23
9.7
2
1.6
1.2
0 10 20 30 40 50 60
Other anxiety and/ordepressive disorders
Depressive disorders
Other anxietydisorders
% of patients
One
Two
Three ormore
†Excluding GAD itselfN=3,340 GAD patients. Psychiatric disorder in the same yearIMS Mediplus Database German GP Analysis. Data on file, Pfizer Inc
GAD in German GP database
# of concurrent disorders24%
29%
45%

59
Direct and Indirect Costs in GAD With and Without Comorbidity
35
21
25
42
34 33
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
GAD WITH comorbidity(n=604)
GAD without comorbidity(n=395)
% o
f p
ati
en
ts Work absenteeism
Outpatient services
HospitalizationMedications
Diagnostic tests
$2050/3 months $1250/3 months
Costs calculated as $(USA) in 1994 and expressed as equivalent value in 2007 $(USA)Souêtre et al. J Psychosom Res. 1994;38:151-160

60
GP Visits and Referrals in 1 Year: GAD Patients vs. Comparison Group
0
10
20
30
40
50
60
70
80
90
100
GAD patients Comparisongroup
% o
f p
ati
en
ts
>6
5 or 6
3 or 4
2
1
0
10
20
30
40
50
60
70
80
90
100
GAD patients Comparisongroup
% o
f p
ati
en
ts
4+
3
2
167%
39%
GP visits Referrals by GP# of referrals
**
**P<0.001 GAD vs. comparison group
N=3,340 in each group. Frequency in the yearIMS Mediplus Database German GP Analysis. Data on file, Pfizer Inc
GAD in German GP database
# of visits

61
GAD: Diagnosis
"Normal" worry vs. Generalized Anxiety Disorder (GAD)
“Normal” Worry: Generalized Anxiety Disorder:
Your worrying doesn’t get in the way of your daily activities and responsibilities.
You’re able to control your worrying. Your worries, while unpleasant, don’t
cause significant distress. Your worries are limited to a specific,
small number of realistic concerns. Your bouts of worrying last for only a
short time period.
Your worrying significantly disrupts your job, activities, or social life.
Your worrying is uncontrollable. Your worries are extremely upsetting
and stressful. You worry about all sorts of things,
and tend to expect the worst. You’ve been worrying almost every
day for at least six months.

62
Another GAD- Carrie’s story:
Carrie has always been a worrier, but it never interfered with her life before. Lately, however, she’s been feeling keyed up all the time. She’s paralyzed by an omnipresent sense of dread, and worries constantly about the future. Her worries make it difficult to concentrate at work, and when she gets home she can’t relax. Carrie is also having sleep difficulties, tossing and turning for hours before she falls asleep. She also gets frequent stomach cramps and diarrhea, and has a chronic stiff neck from muscle tension. Carrie feels like she’s on the verge of a nervous breakdown.

63
Sound Familiar?
“I can’t get my mind to stop…it’s driving me crazy!"
“He’s late - he was supposed to be here 20 minutes ago! Oh my God, he must have been in an accident!”
“I can’t sleep — I just feel such dread … and I don’t know why!”
64
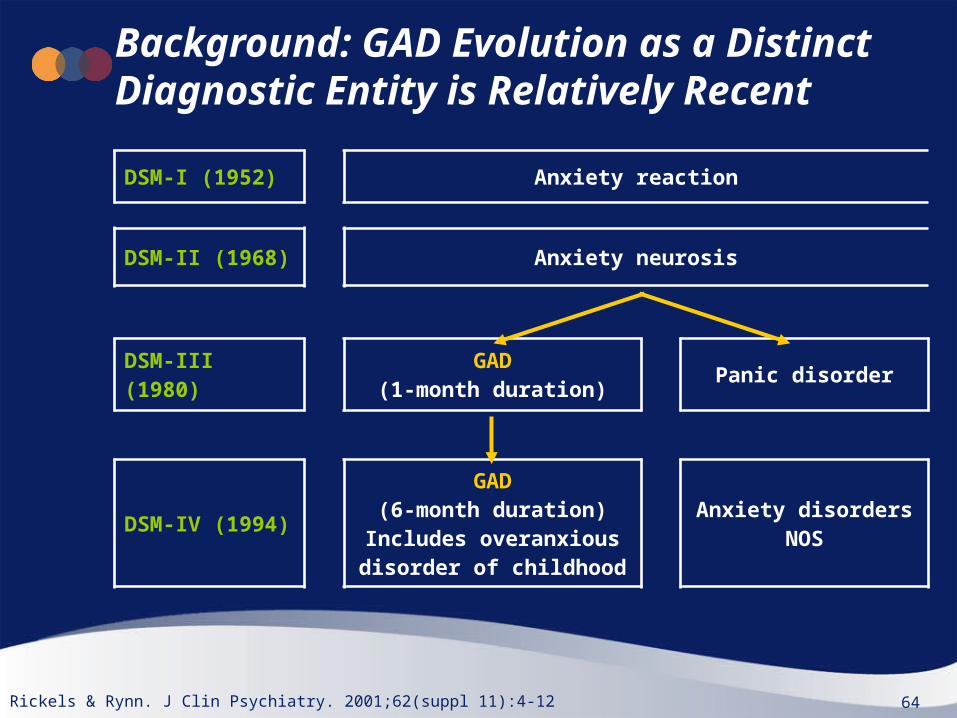
Background: GAD Evolution as a Distinct Diagnostic Entity is Relatively Recent
DSM-I (1952) Anxiety reaction
DSM-II (1968) Anxiety neurosis
DSM-III (1980) GAD(1-month duration) Panic disorder
DSM-IV (1994)
GAD(6-month duration)
Includes overanxious disorder of childhood
Anxiety disorders NOS
Rickels & Rynn. J Clin Psychiatry. 2001;62(suppl 11):4-12

65
Generalized Anxiety Disorder: DSM-IV Diagnostic Criteria
• Excessive anxiety and worry present most of the time for > 6 months• Difficult to control worry• Associated with (at least 3 items):
─ Restlessness ─ Being easily fatigued ─ Concentration difficulties─ Irritability─ Muscle tension─ Sleep disturbance
• Focus of anxiety and worry not confined to features of an Axis I disorder• Causes clincially significant distress or functional impairment• Not due to medication, illness, or substance abuse
DSM-IV-TR. APA 2000

66
Generalized Anxiety Disorder: ICD-10 Summary
• Anxiety is generalized and persistent and not associated with a particular environmental circumstance (i.e. it is free-floating)
• Anxiety present most days for at least several weeks at a time and usually for several months
• Symptoms should involve elements of:─ Apprehension
• E.g. Worry about future, feeling “on edge”, difficulty concentrating─ Motor tension
• E.g. Restlessness, fidgeting, tension headaches, trembling─ Autonomic overactivity
• E.g. Light-headedness, sweating, tachycardia, epigastric discomfort• Must not meet full criteria for depressive episode, phobic anxiety disorder,
panic disorder, or obsessive-compulsive disorder
ICD-10, WHO 1992

67
DSM-IV and ICD-10 GAD Diagnostic Criteria: Some Differences
DSM-IV ICD-10
Diagnostic classificationIndependent
categoryResidual category
Worry/anxiety symptomExcessive anxiety
and worryPersistent free-floating anxiety
Duration ≥6 months Several months
Autonomic hyper-activity and physical symptoms
Not essential Must be present
Functional impairment Must be present Not specified
Rickels & Rynn. J Clin Psychiatry. 2001;62(suppl 11):4-12Starcevic. Anxiety Disorder in Adults. Oxford University Press. 2005:102-140

68
Use of Published GAD Diagnostic Guidelines
66
49
4340
28 27
0
10
20
30
40
50
60
70
80
90
100
Germany Italy Spain UK
% u
sin
g g
uid
eln
es
Psychiatrist
PCP
Data on file, Pfizer Inc
n=44 n=43 n=40 n=40 n=30n=36
• DSM-III and IV guidelines most commonly used

69
Guidance for Exploring a Suspected Anxiety Disorder
Baldwin et al. J Psychopharmacol. 2005;19(6):567-596British Association for Psychopharmacology
Predominant symptom focus
Trauma history &
flashbacks
Obsessions
compulsions
Uncontrollable worry in several
areas
Intermittent panic/anxiety attacks and avoidance
Fear of social
scrutiny
Discrete/object
situation
Some uncued/ spontaneous
Check for PTSD
Check for OCD
Check for GAD
Check for Social
Anxiety Disorder
Check for specific phobia
Check for Panic
Disorder
Specific anxiety-related symptoms & impaired function
Also moderate/severe depression?Treat
depressionYes
No

70
GAD: Disease and Management Issues
• GAD lifetime prevalence ~5%• Comorbid disorders common
─ Common comorbidity of medical and psychiatric disorders• Usually chronic, relapsing-remitting course
─ Low probability of remission─ Long-term treatment often needed
• Sub-optimal recognition and diagnosis is common─ Often presents as somatic complaint
• Substantial quality of life and economic burden• Current treatments may have limitations

71
GAD Treatment
Cognitive therapy (CBT): probably the most effective treatment.
Counseling :
Anxiety management courses : learning how to relax, problem solving skills, coping strategies, and group support.
Self helpYou can get leaflets, books, tapes, videos, etc, on relaxation and combating stress. They teach simple deep breathing techniques and other measures to relieve stress, help you to relax.

72
Drug treatment for GAD:
73
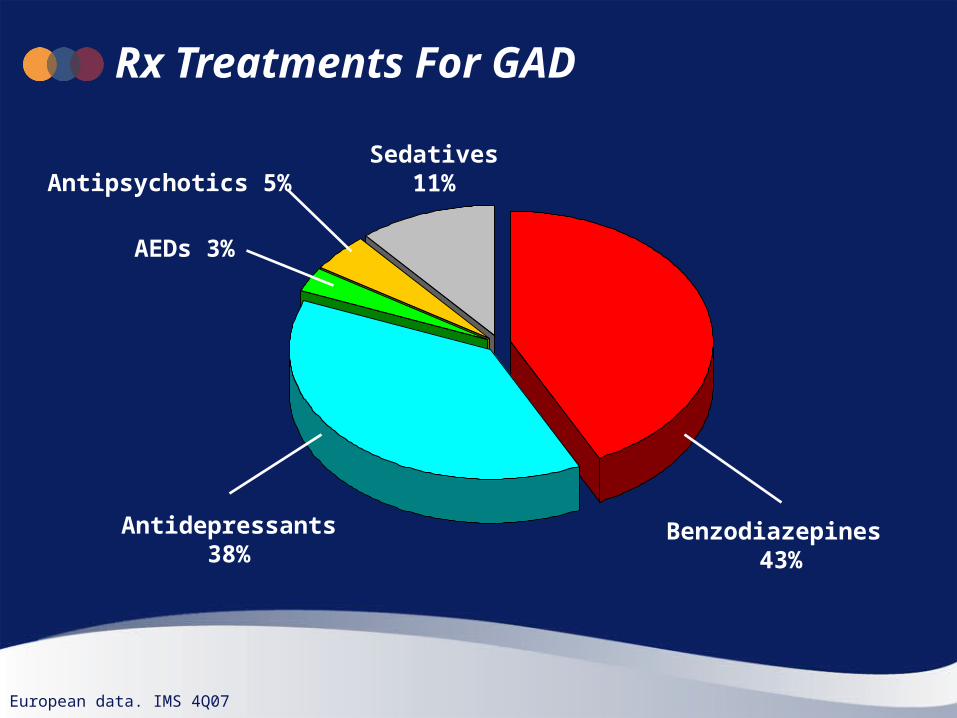
Rx Treatments For GAD
Benzodiazepines 43%
Antidepressants38%
European data. IMS 4Q07
Sedatives11%
AEDs 3%
Antipsychotics 5%

74
Evidence That Treating GAD Reduces the Risk of Developing MDD
0
5
10
15
20
25
30
GAD untreated (n=99) GAD treated (n=120)
% d
evel
op
ing
dep
ress
ion
Data from NCS, USA. MDD: Major Depressive Disorder (DSM-III-R) Hazard ratio =0.52 in patients who had taken psychotropic medication ≥4 times. Goodwin et al. Am J Psychiatry. 2002; 159(11):1935-1937
48% reduction: P<0.001
75
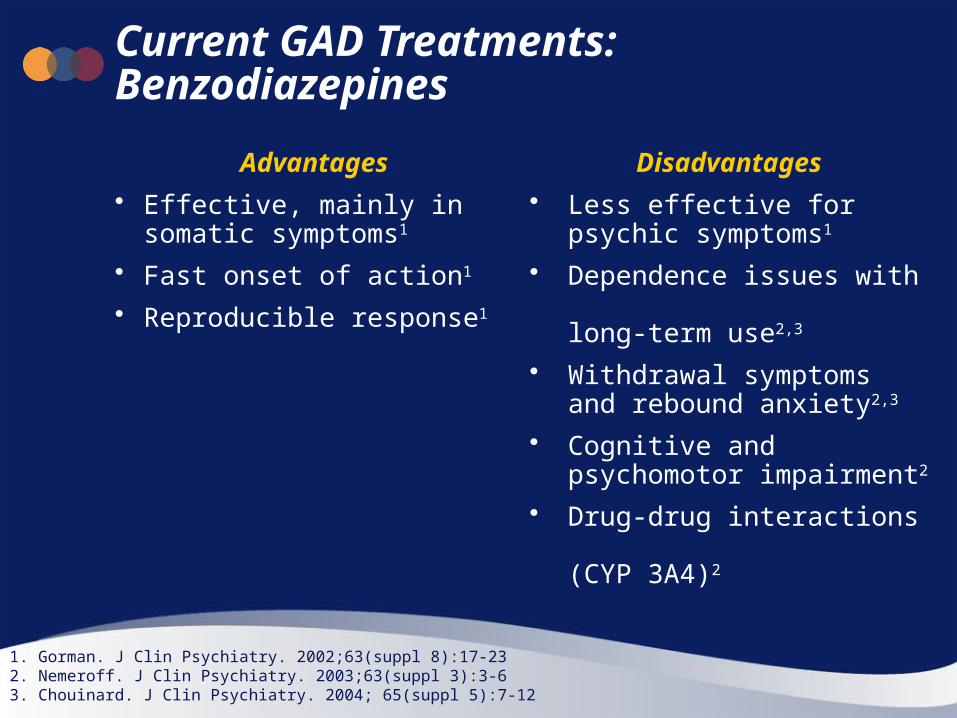
Current GAD Treatments: Benzodiazepines
Advantages
• Effective, mainly in somatic symptoms1
• Fast onset of action1
• Reproducible response1
Disadvantages
• Less effective for psychic symptoms1
• Dependence issues with long-term use2,3
• Withdrawal symptoms and rebound anxiety2,3
• Cognitive and psychomotor impairment2
• Drug-drug interactions (CYP 3A4)2
1. Gorman. J Clin Psychiatry. 2002;63(suppl 8):17-232. Nemeroff. J Clin Psychiatry. 2003;63(suppl 3):3-63. Chouinard. J Clin Psychiatry. 2004; 65(suppl 5):7-12

76
Current GAD Treatments: SSRIs/SNRIs
Advantages
• Effective, mainly in psychic symptoms1
• Reduce comorbid depressive symptoms1
• Low potential for abuse
Disadvantages
• Less effective for somatic symptoms1
• Variable patient response2
• Delayed onset of action2
• Sexual dysfunction2
• Weight gain1
• Discontinuation symptoms2
• Drug-drug interactions (CYP 2D6)1
1. Raj & Sheehan. Generalized Anxiety Disorder. Martin Dunitz Ltd. 2002:137-1522. Nemeroff. J Clin Psychiatry. 2003;63(suppl 3):3-6

77
Efficacy in Key Symptoms of GAD Across Drug Classes
Benzo TCAs SSRIs & SNRIs
Azapirones α2δ ligand
Speed of onset <7 days ~3 weeks ~3 weeks ~3 weeks <7 days
Psychic symptoms ++ +++ +++ +++ +++
Somatic symptoms +++ + + + +++
Associated insomnia +++ + + + +++
Secondary depressive symptoms
+ +++ +++ ++ ++
Benzo: benzodiazepine, SSRI: Selective serotonin re-uptake inhibitor, SNRI: Serotonin-noradrenaline re-uptake inhibitor; TCA: Tricyclic antidepressant. Not all classes approved for use in GAD in Europe. Montgomery. Expert Opin. Pharmacother. 2006;7(15):2139-54
+ Some efficacy, ++ Moderate efficacy, +++ Marked efficacy

78
Tolerability and Safety Profiles Across Drug Classes used in GAD
Benzo TCAs SSRIs & SNRIs
Azapirones α2δ ligand
Sedation/ psychomotor impairment
+++ ++ +/++ + ++
Weight gain + ++ + + ++
Sexual dysfunction 0/+ + ++ + 0/+
GI side-effects 0 + + + 0
Withdrawal syndrome +++ ++ 0/+/++ + +
Risk of drug interactions ++ ++ 0/+/++ + 0/+
Benzo: benzodiazepine, SSRI: Selective serotonin re-uptake inhibitor, SNRI: Serotonin-noradrenaline re-uptake inhibitor; TCA: Tricyclic antidepressant. Not all classes approved for use in GAD in Europe. Montgomery. Expert Opin. Pharmacother. 2006;7(15):2139-54
0: minimum-to-none; + Some, ++ Moderate, +++ Marked

79
Pregabalin: A new Approach
Advantages
Effective in somatic and psychic symptoms1
Fast onset of action2
Effective in refractory patients3
Low abuse potential
Familiar molecule through other indications
NO known PCK drug interactions – easy to use
Disadvantages
Less familiar with use in GAD
Potential rebound Anxiety on withdrawal
Dizziness and somnolence main AEs
1. Montgomery . Expert Opin. Pharmacother. 2006; 7(15):2139-2154 (6 studies combined)2. Herman et al. CINP 20083. Miceli et al. 2008

80
Thank you.