Embed Size (px)
Citation preview

1
AbataceptAbataceptBrian Daniels, M.D.Brian Daniels, M.D.Senior Vice-PresidentSenior Vice-President
Global Clinical DevelopmentGlobal Clinical DevelopmentBristol-Myers SquibbBristol-Myers Squibb

2
Abatacept:Abatacept:IntroductionIntroduction
Anthony Waclawski, Ph.D.Anthony Waclawski, Ph.D.Executive DirectorExecutive Director
Global Regulatory SciencesGlobal Regulatory Sciences Bristol-Myers SquibbBristol-Myers Squibb
3
AbataceptAbatacept

4
Proposed IndicationProposed Indication
ORENCIA is indicated for: ORENCIA is indicated for:
Reducing signs and symptoms, inducing major Reducing signs and symptoms, inducing major clinical responseclinical response
Inhibiting the progression of structural damage, andInhibiting the progression of structural damage, and
Improving physical function Improving physical function
Adult patients with moderately to severely active Adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate rheumatoid arthritis who have had an inadequate response to one or more DMARDs, such as response to one or more DMARDs, such as methotrexate, or TNF blocking agents methotrexate, or TNF blocking agents
May be used in combination with methotrexate or May be used in combination with methotrexate or other non-biologic DMARD therapyother non-biologic DMARD therapy

5
Regulatory BackgroundRegulatory Background
IND for Rheumatoid ArthritisIND for Rheumatoid Arthritis …………………… October 2000October 2000
Special Protocol AssessmentSpecial Protocol Assessment ............ ............ November November
20022002
Fast Track Program Fast Track Program .......................................................... August 2003August 2003
Pre-BLA meetingPre-BLA meeting .................................. .................................. October 2004October 2004
Continuous Marketing Application Continuous Marketing Application ........ March 2005March 2005

6
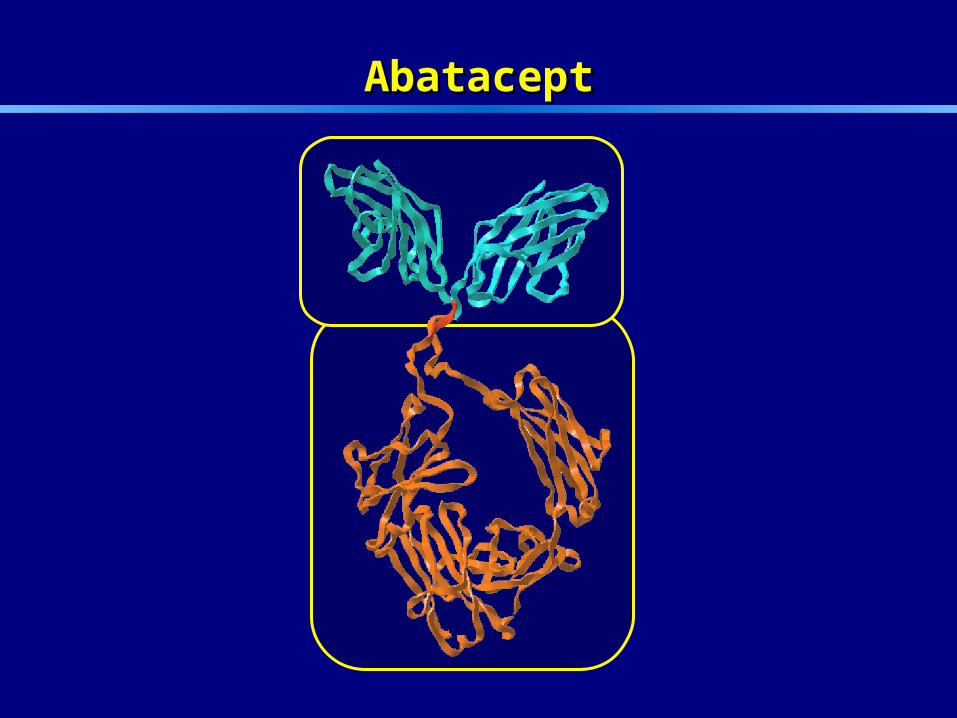
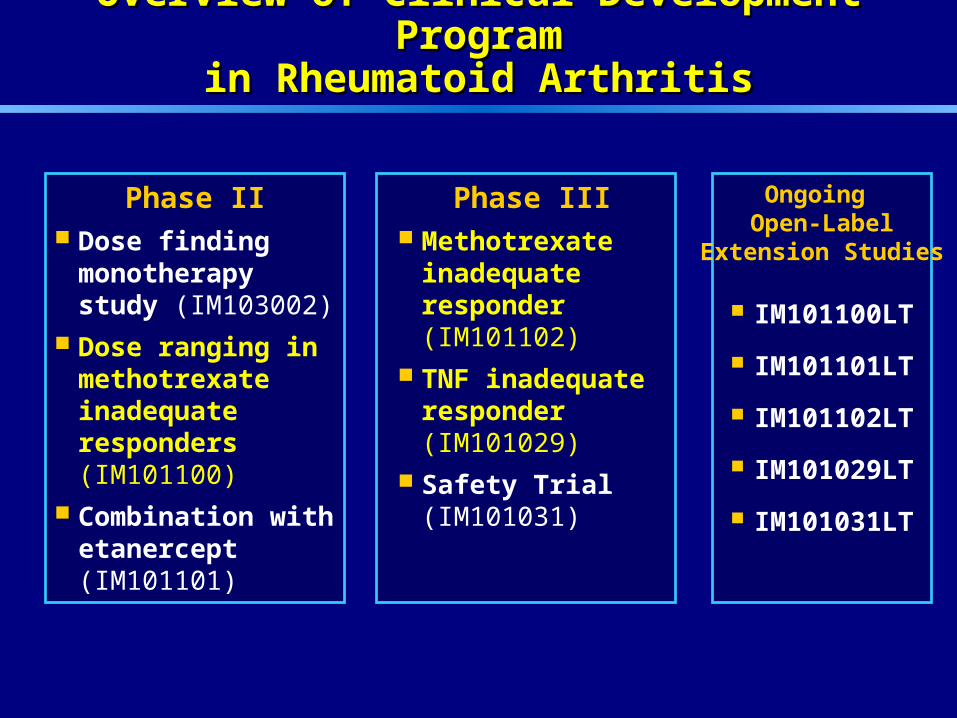
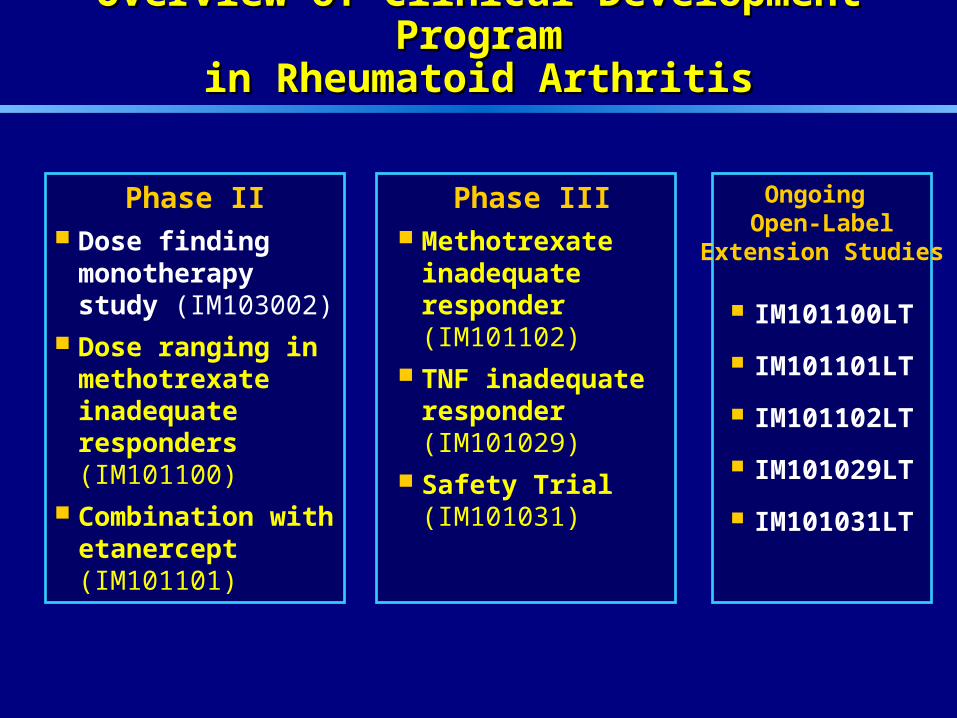
Overview of Clinical Development ProgramOverview of Clinical Development Programin Rheumatoid Arthritisin Rheumatoid Arthritis
Phase II Dose finding
monotherapy study (IM103002)
Dose ranging in methotrexate inadequate responders (IM101100)
Combination with etanercept (IM101101)
Phase III Methotrexate
inadequate responder (IM101102)
TNF inadequate responder (IM101029)
Safety Trial (IM101031)
IM101100LT
IM101101LT
IM101102LT
IM101029LT
IM101031LT
Ongoing Open-Label
Extension Studies
7
Overview of Clinical Development ProgramOverview of Clinical Development Programin Rheumatoid Arthritisin Rheumatoid Arthritis
Phase II Dose finding
monotherapy study (IM103002)
Dose ranging in methotrexate inadequate responders (IM101100)
Combination with etanercept (IM101101)
Phase III Methotrexate
inadequate responder (IM101102)
TNF inadequate responder (IM101029)
Safety Trial (IM101031)
IM101100LT
IM101101LT
IM101102LT
IM101029LT
IM101031LT
Ongoing Open-Label
Extension Studies
8
Overview of Clinical Development ProgramOverview of Clinical Development Programin Rheumatoid Arthritisin Rheumatoid Arthritis
Phase II Dose finding
monotherapy study (IM103002)
Dose ranging in methotrexate inadequate responders (IM101100)
Combination with etanercept (IM101101)
Phase III Methotrexate
inadequate responder (IM101102)
TNF inadequate responder (IM101029)
Safety Trial (IM101031)
IM101100LT
IM101101LT
IM101102LT
IM101029LT
IM101031LT
Ongoing Open-Label
Extension Studies

9
Abatacept: Safety DatabaseAbatacept: Safety Database
Placebo-controlled studiesPlacebo-controlled studies
– 1,955 patients representing 1,688 person-years1,955 patients representing 1,688 person-yearsof exposureof exposure
– 1,330 for 1 year or more1,330 for 1 year or more
Open-label uncontrolled experience: 2,339 patients Open-label uncontrolled experience: 2,339 patients
Combined double-blind and open-label: 2,688 patients Combined double-blind and open-label: 2,688 patients representing 3,827 person-years of exposurerepresenting 3,827 person-years of exposure
Pharmacovigilance Plan Pharmacovigilance Plan

10
Presentation OutlinePresentation Outline
EfficacyEfficacy .................................. George Vratsanos, M.D.George Vratsanos, M.D.
SafetySafety ........................................ Dan MacNeil, M.D.Dan MacNeil, M.D.
SummarySummary …............…............ Brian Daniels, M.D.Brian Daniels, M.D.

11
Abatacept:Abatacept:Summary of EfficacySummary of Efficacy
George Vratsanos, M.D.George Vratsanos, M.D.Medical DirectorMedical Director
ImmunologyImmunologyBristol-Myers SquibbBristol-Myers Squibb

12
Outline of PresentationOutline of Presentation
Mechanism of ActionMechanism of Action
Dose selection from Phase II TrialsDose selection from Phase II Trials
Results from Pivotal Phase III Efficacy Trials in: Results from Pivotal Phase III Efficacy Trials in:
– Methotrexate Inadequate RespondersMethotrexate Inadequate Responders
– Anti-TNF Inadequate RespondersAnti-TNF Inadequate Responders
13
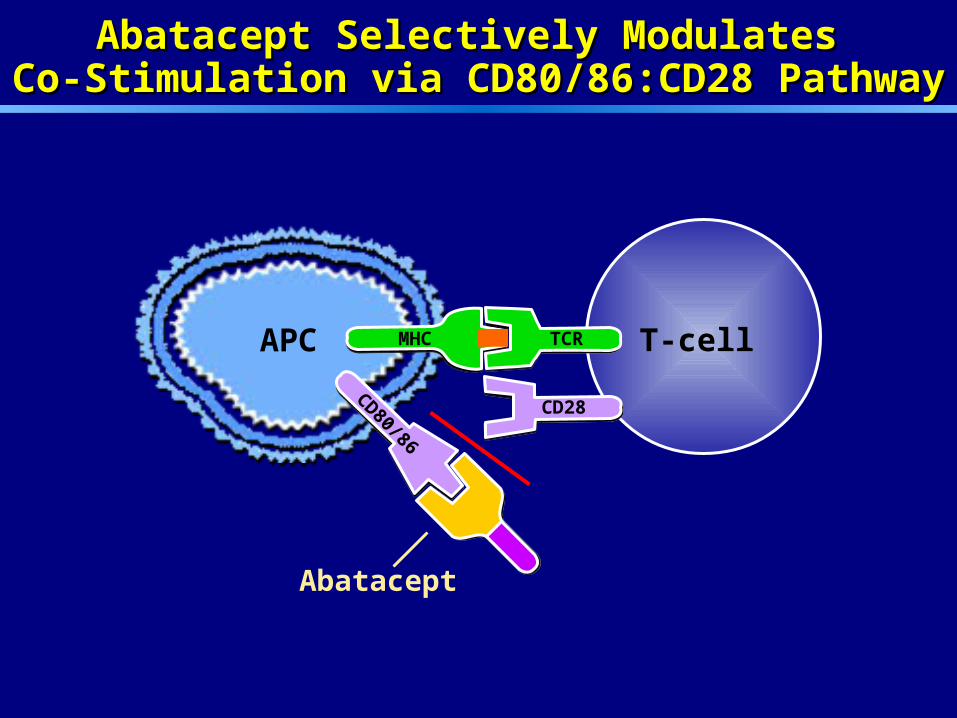
Abatacept Selectively Modulates Abatacept Selectively Modulates Co-Stimulation via CD80/86:CD28 PathwayCo-Stimulation via CD80/86:CD28 Pathway
APC
Abatacept
MHC TCR
CD80/86
CD28
T-cell
14
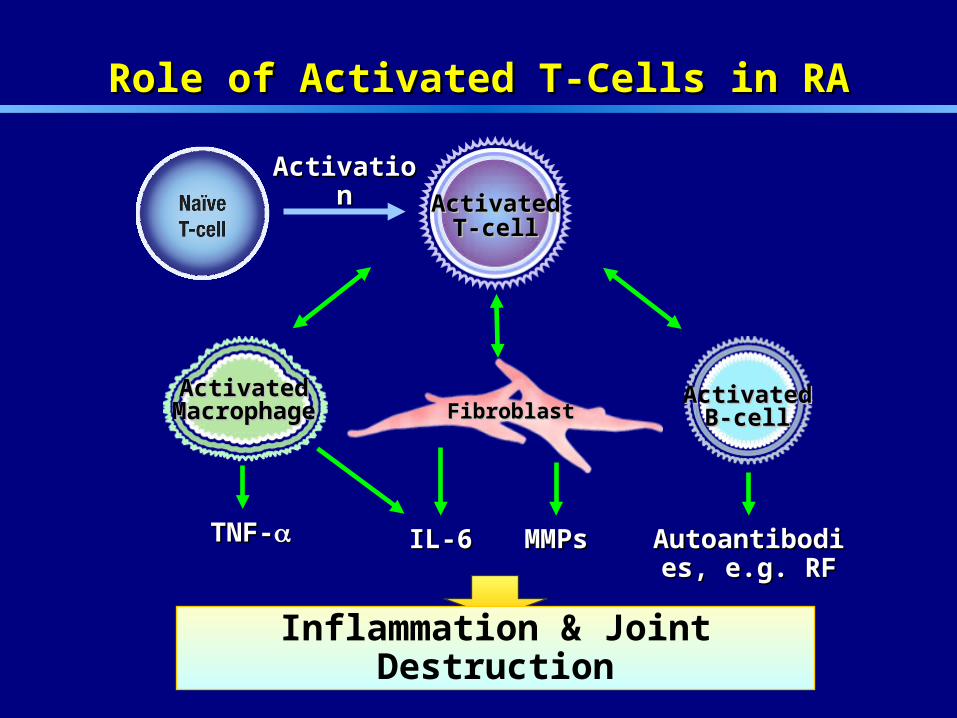
FibroblastFibroblast
Role of Activated T-Cells in RARole of Activated T-Cells in RA
ActivatedActivatedMacrophageMacrophage
ActivatedActivatedB-cellB-cell
IL-6IL-6TNF-TNF- MMPsMMPs Autoantibodies, Autoantibodies, e.g. RFe.g. RF
ActivatedActivatedT-cellT-cell
Inflammation & Joint Destruction
ActivationActivation

15
Proposed Mechanism of Action of AbataceptProposed Mechanism of Action of Abatacept
Decrease T-cell activation and proliferationDecrease T-cell activation and proliferation
Decrease pro-inflammatory cytokine secretion Decrease pro-inflammatory cytokine secretion from activated synovial macrophagesfrom activated synovial macrophages
Decrease autoantibody production (e.g. RF)Decrease autoantibody production (e.g. RF)
No depletion of T-cells or other leukocytesNo depletion of T-cells or other leukocytes

16
Dose SelectionDose Selection

17
Dose Finding StudyDose Finding Study
IM103-002IM103-002
Patient PopulationPatient Population DMARD DMARD Inadequate RespondersInadequate Responders
Background Background MedicationMedication
NoneNone(Monotherapy)(Monotherapy)
Abatacept Doses Abatacept Doses 10 mg/kg10 mg/kg2 mg/kg2 mg/kg
0.5 mg/kg0.5 mg/kg
Primary EndpointPrimary Endpoint (ACR 20)(ACR 20)
3 months3 months
Dose Finding StudyDose Finding Study
IM103-002IM103-002Dose Ranging StudyDose Ranging Study
IM101-100IM101-100
Patient PopulationPatient Population DMARD DMARD Inadequate RespondersInadequate Responders
Methotrexate Methotrexate InadequateInadequate RespondersResponders
Background Background MedicationMedication
NoneNone(Monotherapy)(Monotherapy)
MethotrexateMethotrexate
Abatacept Doses Abatacept Doses 10 mg/kg10 mg/kg2 mg/kg2 mg/kg
0.5 mg/kg0.5 mg/kg
10 mg/kg10 mg/kg2 mg/kg2 mg/kg
Primary EndpointPrimary Endpoint (ACR 20)(ACR 20)
3 months3 months 6 months6 months
Phase II Dose Response StudiesPhase II Dose Response StudiesDouble-Blind, Randomized, Placebo ControlledDouble-Blind, Randomized, Placebo Controlled
18
0
10
20
30
40
50
60
70
80
0 30 60 90 120 150 180 210 240 270 300 330 360
Visit Days
% R
es
po
nd
ers
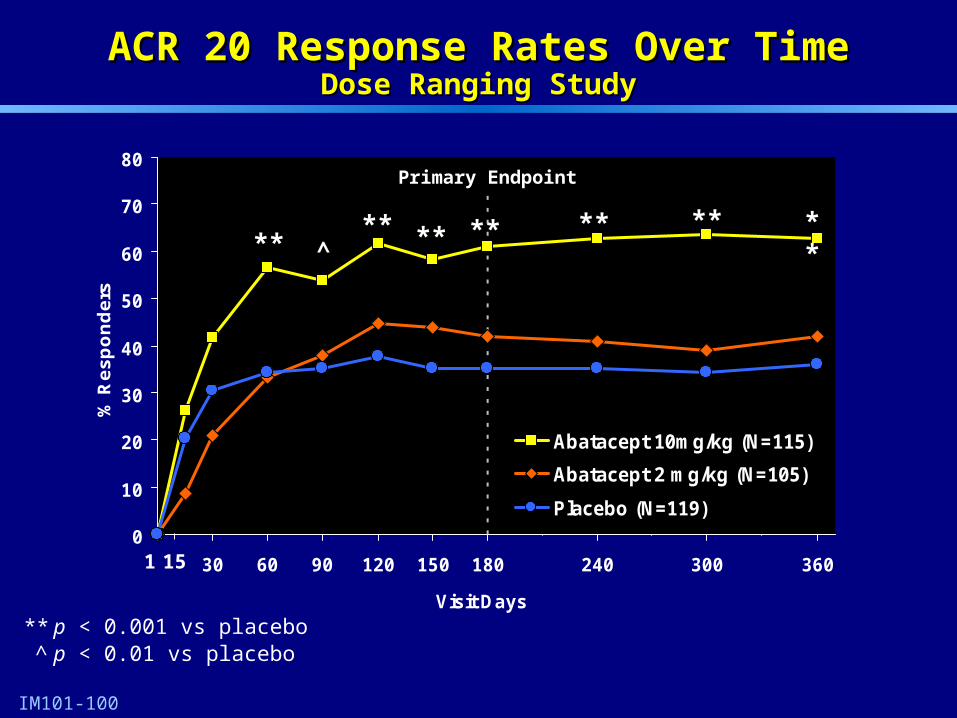
Abatacept 10mg/kg (N=115)
Abatacept 2 mg/kg (N=105)
Placebo (N=119)
15 1
** p < 0.001 vs placebo^ p < 0.01 vs placebo
IM101-100
ACR 20 Response Rates Over TimeACR 20 Response Rates Over TimeDose Ranging StudyDose Ranging Study
^** ** ** ** ** **
**
Primary Endpoint

19
Rationale for Phase III DesignRationale for Phase III Design
20
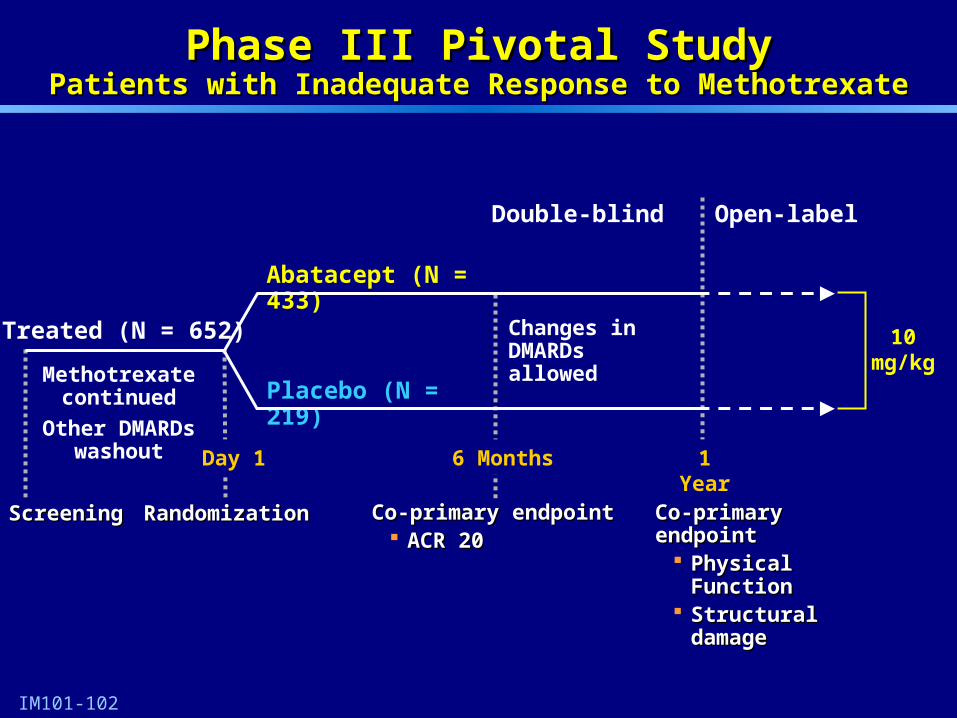
Phase III Pivotal StudyPhase III Pivotal StudyPatients with Inadequate Response to MethotrexatePatients with Inadequate Response to Methotrexate
Methotrexate continued
Other DMARDs washout
ScreeningScreening
6 Months
Co-primary eCo-primary endpointndpoint ACR 20ACR 20
Placebo (N = 219)
Abatacept (N = 433)
RandomizationRandomization
1 Year
IM101-102
Day 1
Co-primaryCo-primary endpointendpoint Physical FunctionPhysical Function Structural damageStructural damage
Double-blind Open-label
Treated (N = 652) 10mg/kg
Changes in DMARDs allowed

21
Demographic and Patient CharacteristicsDemographic and Patient CharacteristicsPatients with Inadequate Response to MethotrexatePatients with Inadequate Response to Methotrexate
IM101-102
AbataceptAbataceptN = 433N = 433
PlaceboPlaceboN = 219N = 219
Age in years, meanAge in years, mean 5252 5050
Female (%)Female (%) 78 78 8282
Caucasian (%)Caucasian (%) 8888 8888
Disease duration in years, meanDisease duration in years, mean 99 99
RF+ (%)RF+ (%) 8282 7979
Steroids (%)Steroids (%) 7272 6868
Methotrexate dose, mean mg/wkMethotrexate dose, mean mg/wk 1616 1616
22
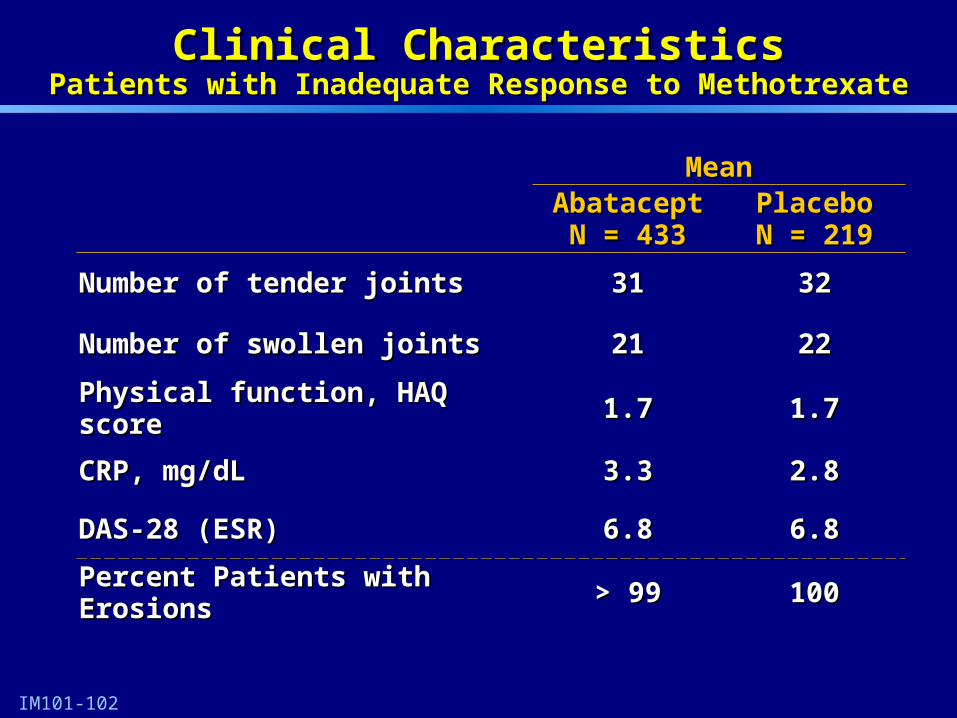
Clinical CharacteristicsClinical CharacteristicsPatients with Inadequate Response to MethotrexatePatients with Inadequate Response to Methotrexate
MeanMeanAbataceptAbatacept
N = 433N = 433PlaceboPlaceboN = 219N = 219
Number of tNumber of tender jointsender joints 3131 3232
Number of swollen jointsNumber of swollen joints 2121 2222
Physical function, HAQ scorePhysical function, HAQ score 1.71.7 1.71.7
CRP, mg/dLCRP, mg/dL 3.33.3 2.82.8
DAS-28 (ESR)DAS-28 (ESR) 6.86.8 6.86.8
Percent Patients with ErosionsPercent Patients with Erosions > 99> 99 100100
IM101-102
23IM101-102
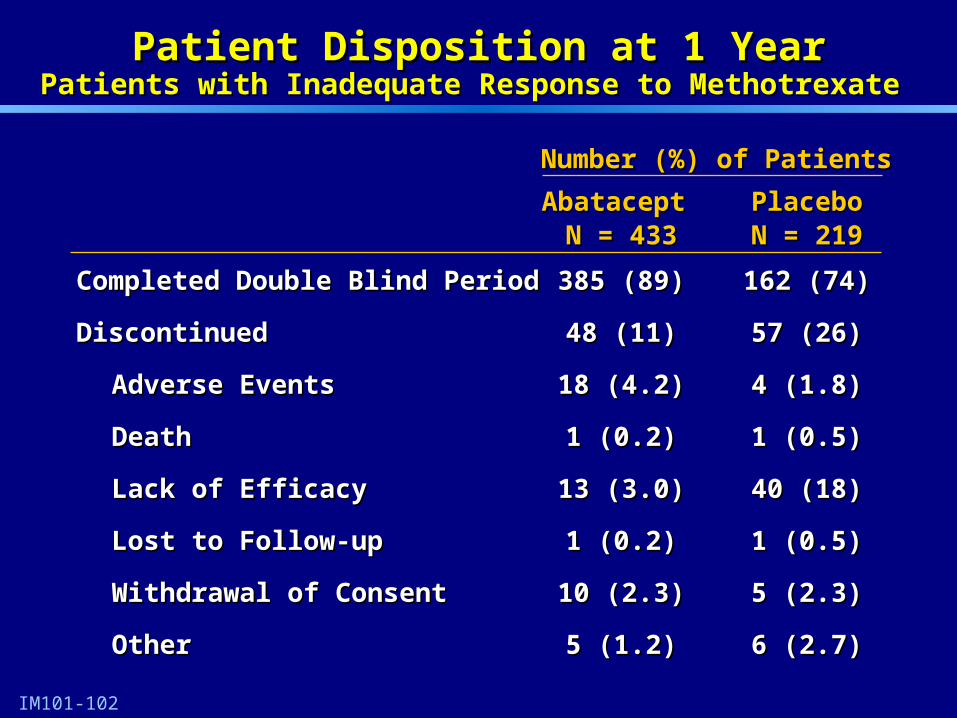
Abatacept Abatacept PlaceboPlaceboN = 433N = 433 N = 219N = 219
Completed Double Blind PeriodCompleted Double Blind Period 385 (89)385 (89) 162 (74)162 (74)
DiscontinuedDiscontinued 48 (11)48 (11) 57 (26)57 (26)
Adverse EventsAdverse Events 18 (4.2)18 (4.2) 4 (1.8)4 (1.8)
DeathDeath 1 (0.2)1 (0.2) 1 (0.5)1 (0.5)
Lack of EfficacyLack of Efficacy 13 (3.0)13 (3.0) 40 (18)40 (18)
Lost to Follow-upLost to Follow-up 1 (0.2)1 (0.2) 1 (0.5)1 (0.5)
Withdrawal of ConsentWithdrawal of Consent 10 (2.3)10 (2.3) 5 (2.3)5 (2.3)
OtherOther 5 (1.2)5 (1.2) 6 (2.7)6 (2.7)
Patient Disposition at 1 YearPatient Disposition at 1 YearPatients with Inadequate Response to MethotrexatePatients with Inadequate Response to Methotrexate
Number (%) of PatientsNumber (%) of Patients

24
0
10
20
30
40
50
60
70
80
1 29 57 85 113 141 169 197 225 253 281 309 337 365
Visit Days
% R
es
po
nd
ers
Abatacept (N = 424)
Placebo (N = 214)
ACR 20 Response Over TimeACR 20 Response Over TimePatients with Inadequate Response to MethotrexatePatients with Inadequate Response to Methotrexate
IM101-102
**** ** **
** ** **
*
^
**
15
** p < 0.001^ p < 0.01* p < 0.05
ITT analysis; All patients who D/C are considered non-responders
Primary Endpoint
25
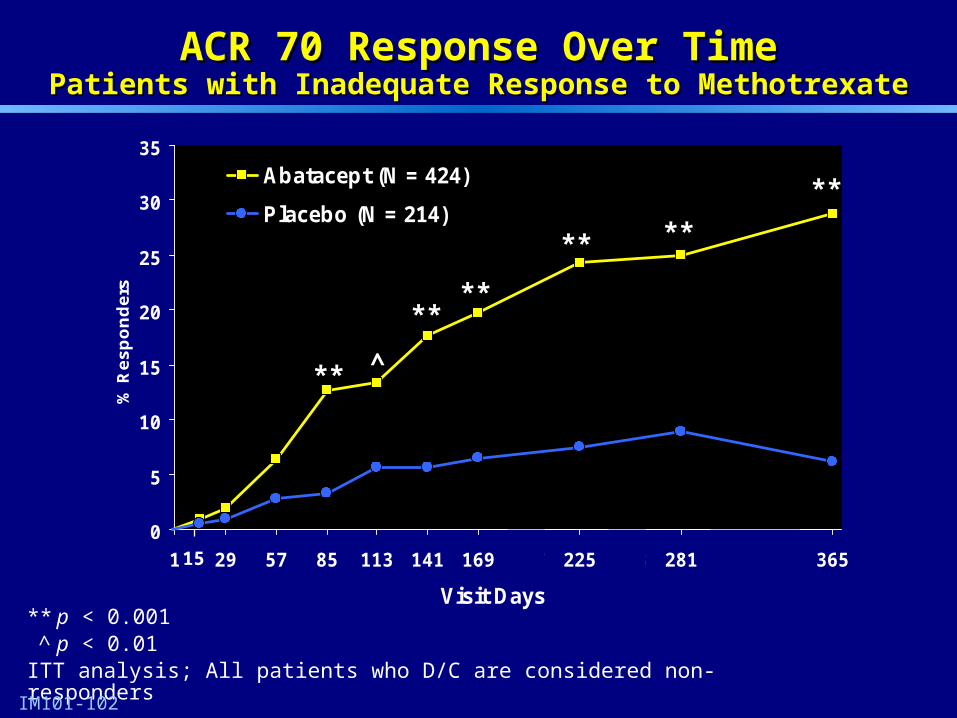
** p < 0.001^ p < 0.01
ITT analysis; All patients who D/C are considered non-responders
0
5
10
15
20
25
30
35
1 29 57 85 113 141 169 197 225 253 281 309 337 365
Visit Days
% R
es
po
nd
ers
Abatacept (N = 424)
Placebo (N = 214)
IM101-102
ACR 70 Response Over TimeACR 70 Response Over TimePatients with Inadequate Response to MethotrexatePatients with Inadequate Response to Methotrexate
** ^
****
**
**
**
15
26
14
1.90
5
10
15
20
25
% R
es
po
nd
ers
Abatacept (N = 424)
Placebo (N = 214)
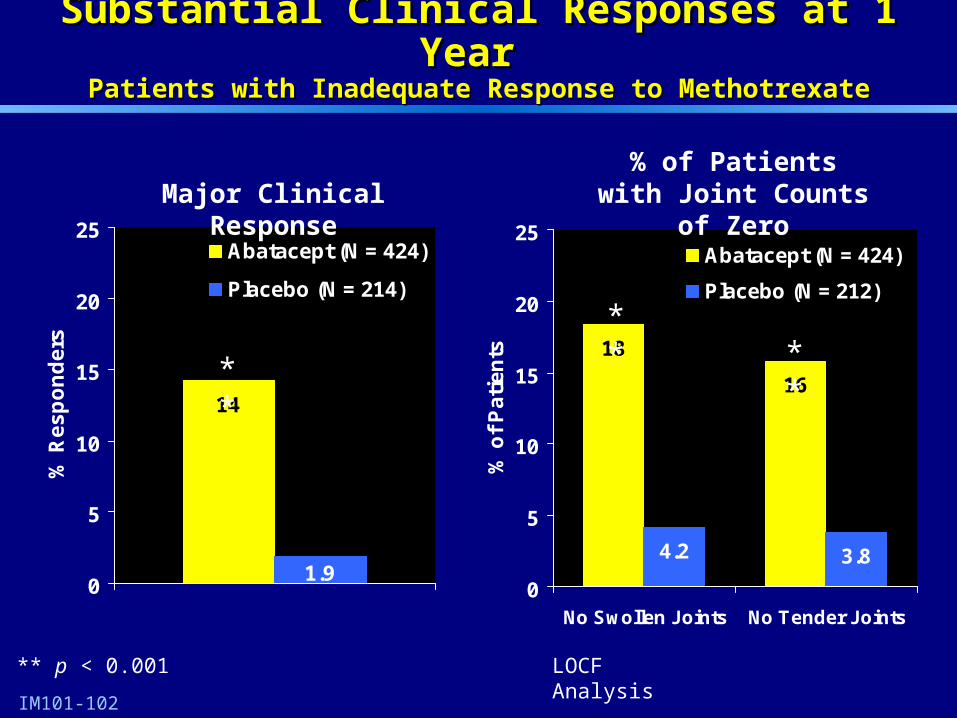
Substantial Clinical Responses at 1 Year Substantial Clinical Responses at 1 Year Patients with Inadequate Response to MethotrexatePatients with Inadequate Response to Methotrexate
**
** p < 0.001
Major Clinical Response
IM101-102
18
16
4.2 3.8
0
5
10
15
20
25
No Swollen Joints No Tender Joints
% o
f P
ati
en
ts
Abatacept (N = 424)
Placebo (N = 212)
% of Patients with Joint Counts of Zero
****
LOCF Analysis
27
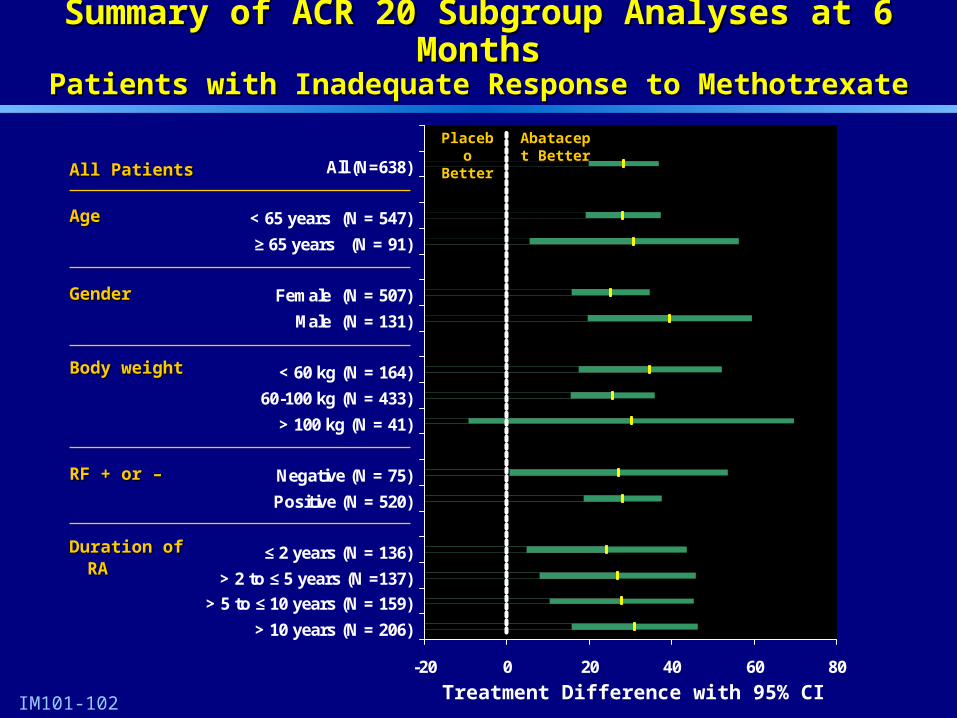
Summary of ACR 20 Subgroup Analyses at 6 MonthsSummary of ACR 20 Subgroup Analyses at 6 MonthsPatients with Inadequate Response to MethotrexatePatients with Inadequate Response to Methotrexate
All PatientsAll Patients
IM101-102
-20 0 20 40 60 80
All (N=638)
< 65 years (N = 547)
≥ 65 years (N = 91)
Female (N = 507)
Male (N = 131)
< 60 kg (N = 164)
60-100 kg (N = 433)
> 100 kg (N = 41)
Negative (N = 75)
Positive (N = 520)
≤ 2 years (N = 136)
> 2 to ≤ 5 years (N =137)
> 5 to ≤ 10 years (N = 159)
> 10 years (N = 206)
AgeAge
GenderGender
RF + or –RF + or –
Body weightBody weight
Duration of RADuration of RA
Treatment Difference with 95% CI
Abatacept Better
Placebo Better
28
Evaluation of Structural Damage ProgressionEvaluation of Structural Damage ProgressionPatients with Inadequate Response to MethotrexatePatients with Inadequate Response to Methotrexate
Assessed using Genant Modified Sharp Assessed using Genant Modified Sharp scoringscoring systemsystem
Paired radiographs obtained in over 90% of all Paired radiographs obtained in over 90% of all randomized patientsrandomized patients
Radiographs scored in blinded fashion using Radiographs scored in blinded fashion using validated methodvalidated method
Data analyzed using comparison of distribution Data analyzed using comparison of distribution of changes from baseline, mean and median of changes from baseline, mean and median changeschanges

29
Genant Modified Sharp Scoring SystemGenant Modified Sharp Scoring SystemPatients with Inadequate Response to MethotrexatePatients with Inadequate Response to Methotrexate
Erosions (Maximum score: 145)Erosions (Maximum score: 145)
– 14 joints in each hand / wrist14 joints in each hand / wrist
– 6 joints in each foot6 joints in each foot
Joint Space Narrowing (Maximum score: 145)Joint Space Narrowing (Maximum score: 145)
– 13 joints in each hand / wrist13 joints in each hand / wrist
– 6 joints in each foot6 joints in each foot
30
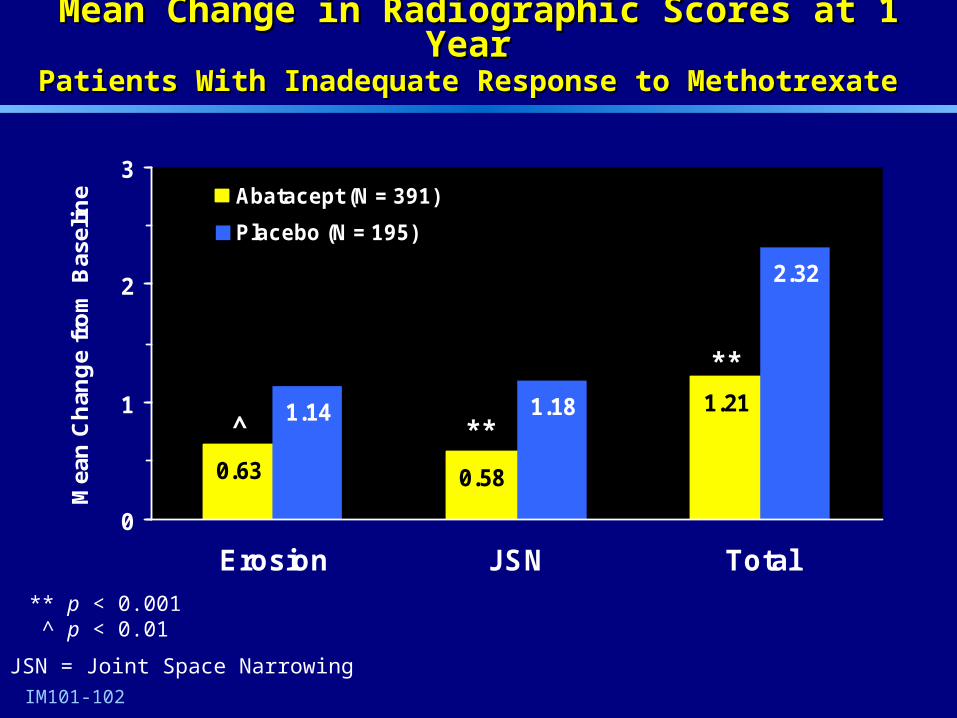
0.58
1.211.18
2.32
0.63
1.14
0
1
2
3
Erosion JSN Total
Mea
n C
han
ge
fro
m B
asel
ine Abatacept (N = 391)
Placebo (N = 195)
**^
**
IM101-102
Mean Change in Radiographic Scores at 1 Year Mean Change in Radiographic Scores at 1 Year Patients With Inadequate Response to MethotrexatePatients With Inadequate Response to Methotrexate
** p < 0.001 ^ p < 0.01
JSN = Joint Space Narrowing
31
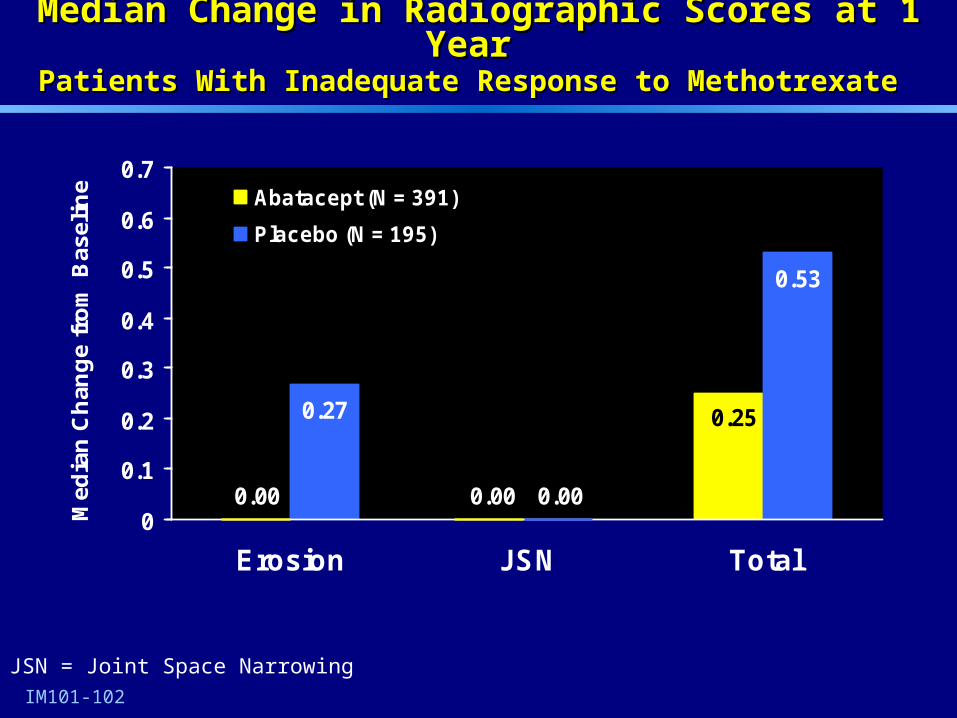
0.00 0.00
0.53
0.25
0.00
0.27
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
Erosion JSN Total
Med
ian
Ch
ang
e fr
om
Bas
elin
e Abatacept (N = 391)
Placebo (N = 195)
IM101-102
Median Change in Radiographic Scores at 1 Year Median Change in Radiographic Scores at 1 Year Patients With Inadequate Response to MethotrexatePatients With Inadequate Response to Methotrexate
JSN = Joint Space Narrowing
32
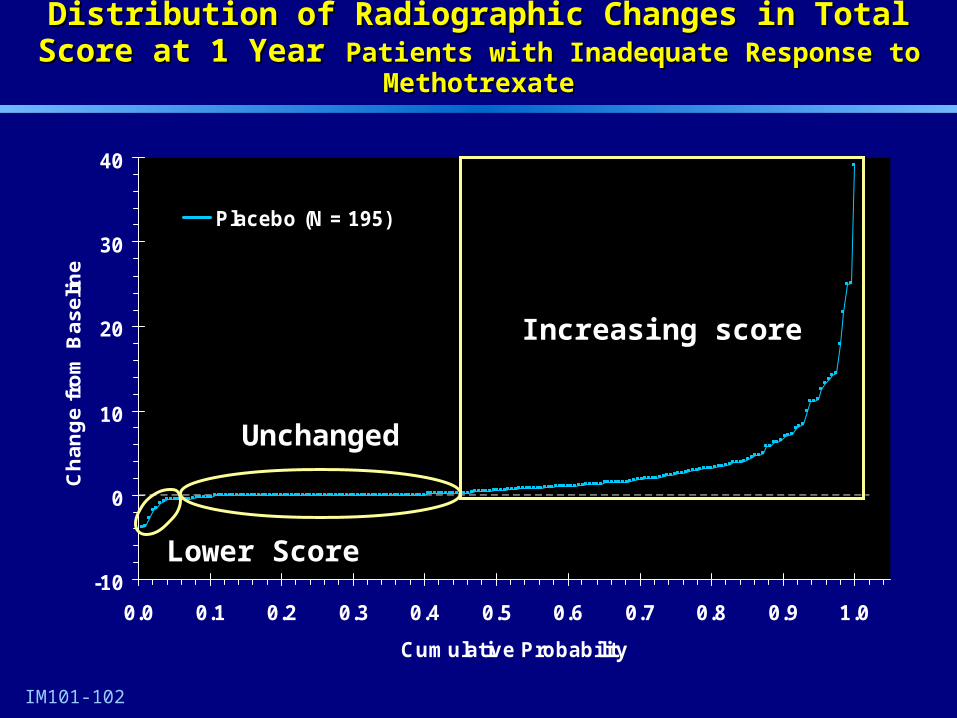
Distribution of Radiographic Changes in Total Score at 1 YearDistribution of Radiographic Changes in Total Score at 1 Year Patients with Inadequate Response to MethotrexatePatients with Inadequate Response to Methotrexate
-10
0
10
20
30
40
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
Cumulative Probability
Ch
an
ge
fro
m B
as
eli
ne
Placebo (N = 195)
Increasing score
Unchanged
Lower Score
IM101-102
33
-10
0
10
20
30
40
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
Cumulative Probability
Ch
an
ge
fro
m B
as
eli
ne
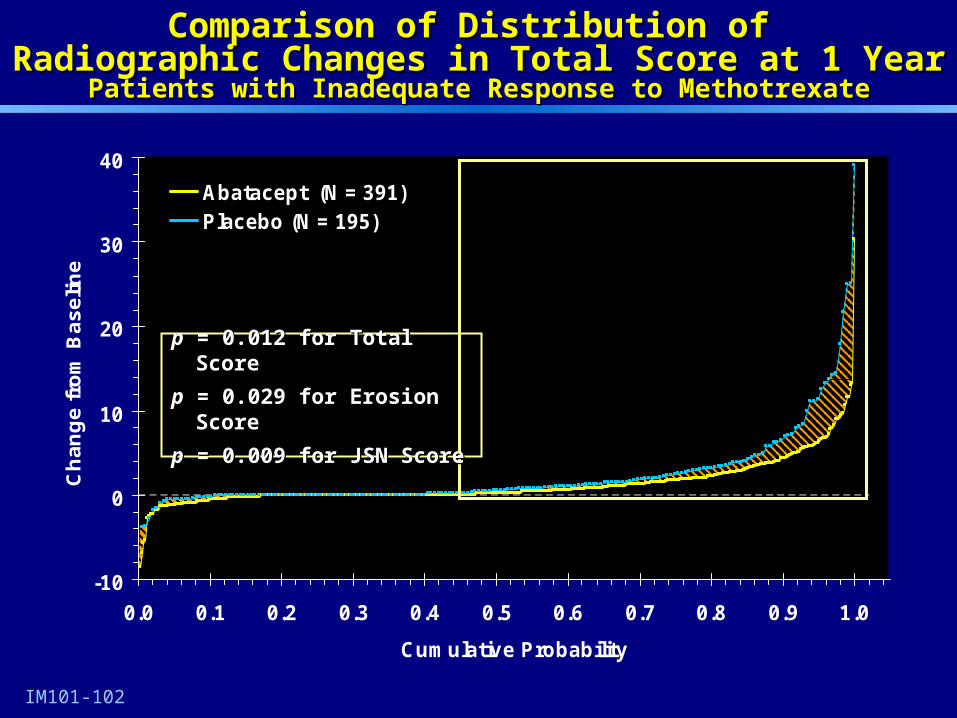
Abatacept (N = 391)Placebo (N = 195)
IM101-102
Comparison of Distribution of Comparison of Distribution of Radiographic Changes in Total Score at 1 YearRadiographic Changes in Total Score at 1 Year
Patients with Inadequate Response to MethotrexatePatients with Inadequate Response to Methotrexate
pp = 0.012 for Total Score = 0.012 for Total Score
pp = 0.029 for Erosion Score = 0.029 for Erosion Score
pp = 0.009 for JSN Score = 0.009 for JSN Score
34
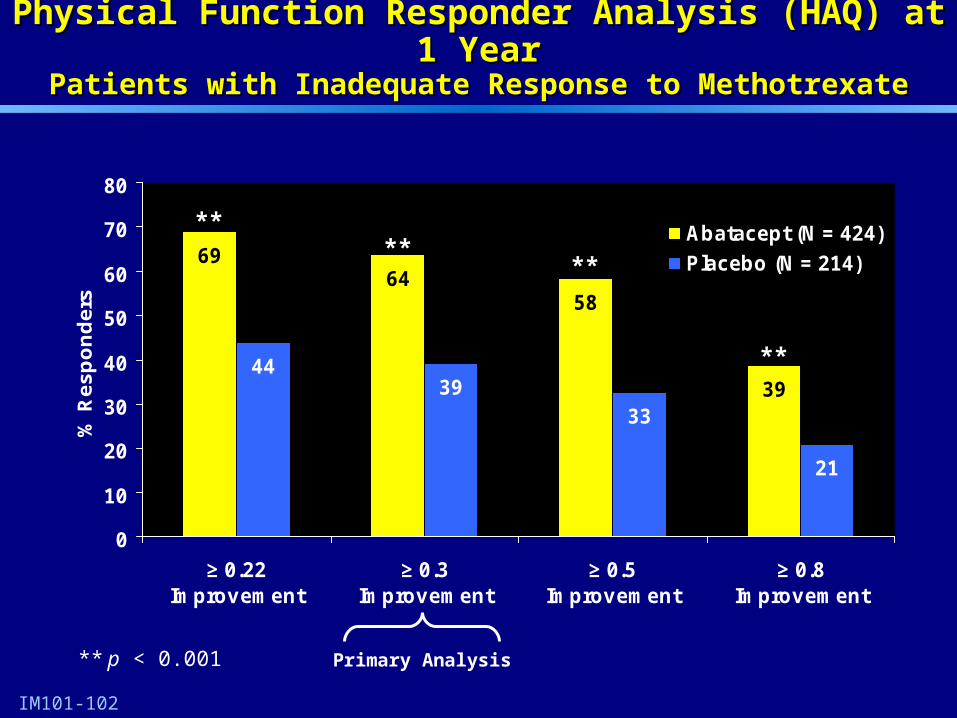
Physical Function Responder Analysis (HAQ) at 1 YearPhysical Function Responder Analysis (HAQ) at 1 YearPatients with Inadequate Response to MethotrexatePatients with Inadequate Response to Methotrexate
IM101-102
6458
393933
21
69
44
0
10
20
30
40
50
60
70
80
≥ 0.22Improvement
≥ 0.3Improvement
≥ 0.5Improvement
≥ 0.8Improvement
% R
es
po
nd
ers
Abatacept (N = 424)
Placebo (N = 214)
** p < 0.001
****
**
**
Primary Analysis

35
0
10
20
30
40
50
60
70
80
1 29 57 85 113 141 169 197 225 253 281 309 337 365
Visit Days
% R
es
po
nd
ers
(d
ec
rea
se
≥ 0
.3)
Abatacept (N = 424)
Placebo (N = 214)
15
Clinically Important Improvement in Physical Function Clinically Important Improvement in Physical Function (Decrease in HAQ (Decrease in HAQ ≥ 0.3≥ 0.3))
Patients with Inadequate Response to MethotrexatePatients with Inadequate Response to Methotrexate
IM101-102
*** ** ^ ** ** ** **
** p < 0.001^ p < 0.01* p < 0.05
ITT analysis; All patients who D/C are considered non-responders

36
Clinically Important Improvement in Physical Function Clinically Important Improvement in Physical Function (Decrease in mHAQ ≥ 0.3) Over 3 Years(Decrease in mHAQ ≥ 0.3) Over 3 Years
Dose-Ranging StudyDose-Ranging Study
Patient PopulationPatient Population
(Randomized 10mg/kg; (Randomized 10mg/kg; Entered open-label)Entered open-label) 1 Yr1 Yr 2 Yr2 Yr 3 Yr3 Yr
As ObservedAs Observed All PatientsAll Patients Number of Patients Number of Patients % Response% Response
848455%55%
737353%53%
646453%53%
IM101-100
Patients Who Discontinue Considered Non-respondersPatients Who Discontinue Considered Non-responders
All Patients (N = 84)All Patients (N = 84) % Response% Response 55%55% 46%46% 42%42%
mHAQ Responders at 1 year (N = 46)mHAQ Responders at 1 year (N = 46) % Response% Response —— 67%67% 57%57%
37
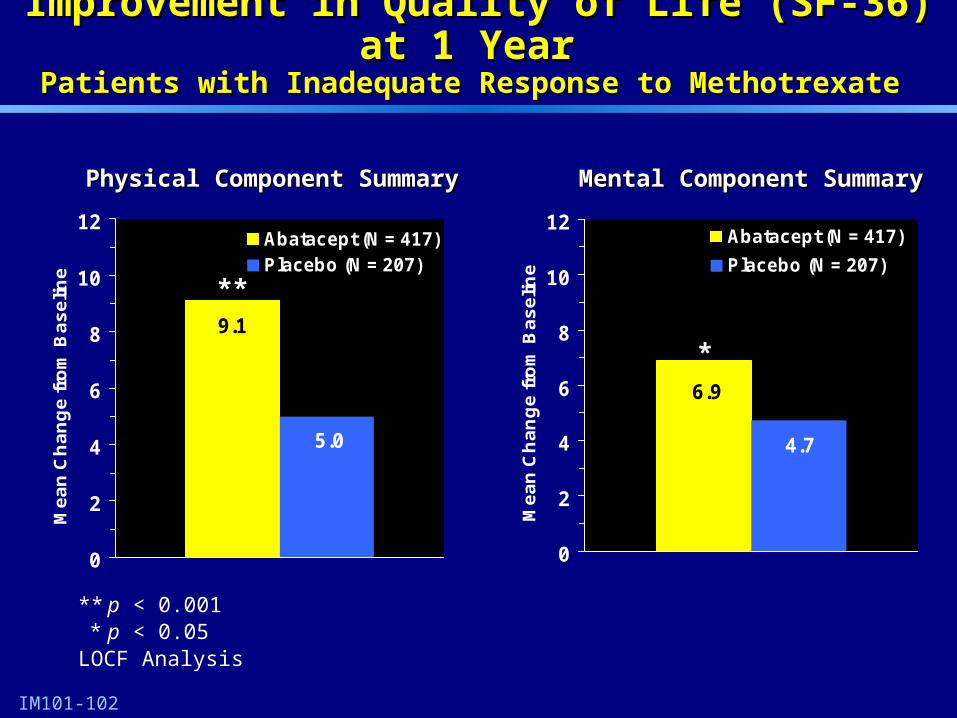
Improvement in Quality of Life (SF-36) at 1 Year Improvement in Quality of Life (SF-36) at 1 Year Patients with Inadequate Response to Methotrexate Patients with Inadequate Response to Methotrexate
IM101-102
9.1
5.0
0
2
4
6
8
10
12
Me
an
Ch
an
ge
fro
m B
as
elin
e
Abatacept (N = 417)Placebo (N = 207)
**
Physical Component SummaryPhysical Component Summary
6.9
4.7
0
2
4
6
8
10
12
Me
an
Ch
an
ge
fro
m B
as
elin
e
Abatacept (N = 417)
Placebo (N = 207)
*
** p < 0.001* p < 0.05
LOCF Analysis
Mental Component SummaryMental Component Summary
38
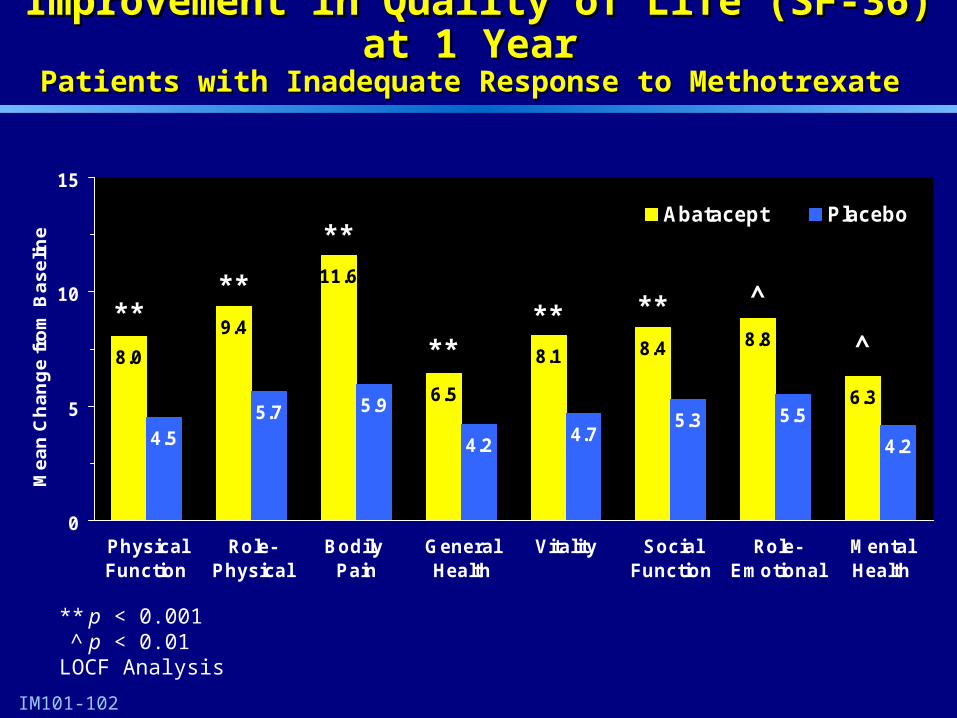
8.0
9.4
11.6
6.5
8.1 8.4 8.8
6.3
4.55.7 5.9
4.24.7
5.3 5.5
4.2
0
5
10
15
PhysicalFunction
Role-Physical
Bodily Pain
GeneralHealth
Vitality SocialFunction
Role-Emotional
MentalHealth
Me
an
Ch
an
ge
fro
m B
as
elin
e
Abatacept Placebo
Improvement in Quality of Life (SF-36) at 1 YearImprovement in Quality of Life (SF-36) at 1 Year Patients with Inadequate Response to Methotrexate Patients with Inadequate Response to Methotrexate
IM101-102
****
**
**** ** ^
^
** p < 0.001^ p < 0.01
LOCF Analysis

39
Phase III Pivotal StudyPhase III Pivotal Study
Patients with Inadequate Response Patients with Inadequate Response to Anti-TNF Therapyto Anti-TNF Therapy

40
Placebo (N = 133)
Abatacept (N = 258)
RandomizationRandomization
Day 1
Double-blind Open-label
6 Months
Co-primaryCo-primary endpointendpoint ACR 20ACR 20 Physical FunctionPhysical Function
IM101-029
Treated (N = 391)
Stratified Recent vs PriorStratified Recent vs Prior
DMARDs continued
AntiTNF washout period
(28–60 days)
10mg/kg
Phase III Pivotal StudyPhase III Pivotal StudyPatients with Inadequate Response to Anti-TNF TherapyPatients with Inadequate Response to Anti-TNF Therapy
41
Key Requirements for EntryKey Requirements for EntryPatients with Inadequate Response to Anti-TNF TherapyPatients with Inadequate Response to Anti-TNF Therapy
Only patients with lack of efficacy on Anti-TNF eligibleOnly patients with lack of efficacy on Anti-TNF eligible
Minimum of 10 swollen and 12 tender joints with Minimum of 10 swollen and 12 tender joints with elevated CRP despite at least 3 months of Anti-TNF elevated CRP despite at least 3 months of Anti-TNF therapy required therapy required
Lack of efficacy occurred immediately before Lack of efficacy occurred immediately before enrollment (‘recent user’) or more distantly (‘prior user’)enrollment (‘recent user’) or more distantly (‘prior user’)
Lack of efficacy directly observed in recent usersLack of efficacy directly observed in recent users
Source Documentation of inadequate response Source Documentation of inadequate response required for prior usersrequired for prior users
IM101-029
42
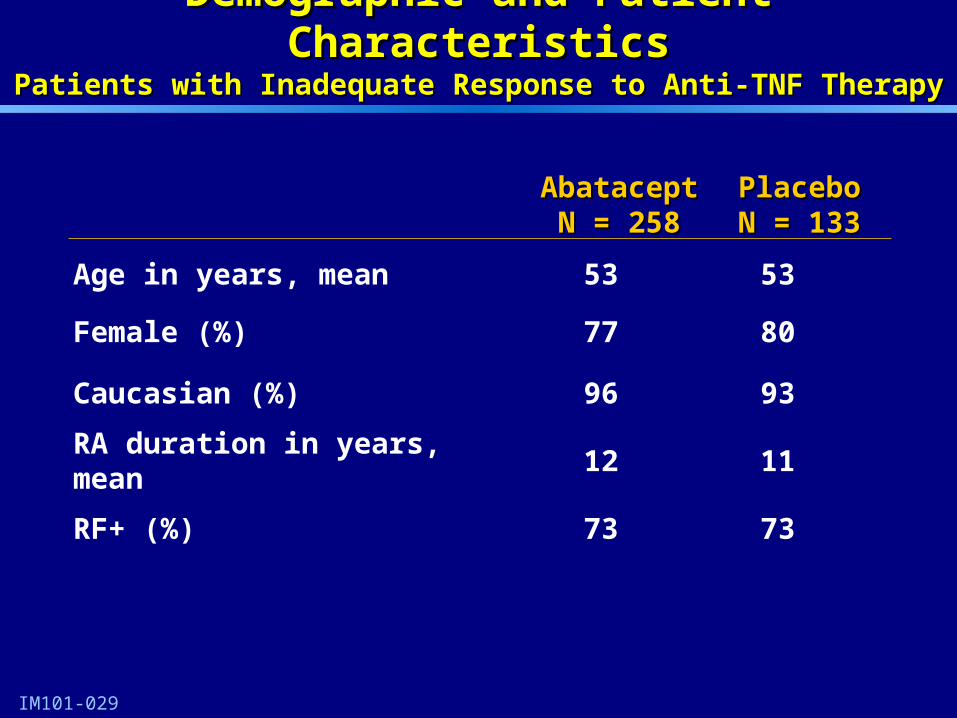
Demographic and Patient CharacteristicsDemographic and Patient CharacteristicsPatients with Inadequate Response to Anti-TNF TherapyPatients with Inadequate Response to Anti-TNF Therapy
IM101-029
AbataceptAbataceptN = 258N = 258
PlaceboPlaceboN = 133N = 133
Age in years, mean 53 53
Female (%) 77 80
Caucasian (%) 96 93
RA duration in years, mean 12 11
RF+ (%) 73 73
43
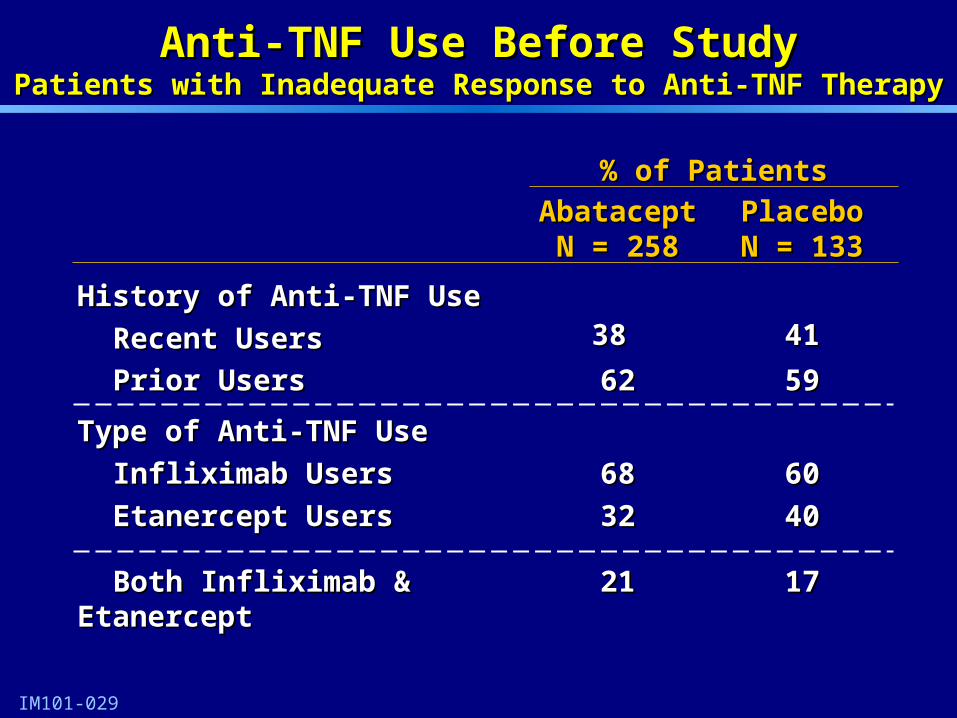
Anti-TNF Use Before StudyAnti-TNF Use Before StudyPatients with Inadequate Response to Anti-TNF TherapyPatients with Inadequate Response to Anti-TNF Therapy
IM101-029
% of Patients% of Patients
AbataceptAbataceptN = 258N = 258
PlaceboPlaceboN = 133N = 133
History of Anti-TNF UseHistory of Anti-TNF Use
Recent UsersRecent Users 38 38 4141
Prior UsersPrior Users 6262 5959
Type of Anti-TNF UseType of Anti-TNF Use
Infliximab UsersInfliximab Users
Etanercept UsersEtanercept Users
6868
3232
6060
4040
Both Infliximab & Etanercept Both Infliximab & Etanercept 2121 1717

44
Clinical CharacteristicsClinical CharacteristicsPatients with Inadequate Response to Anti-TNF TherapyPatients with Inadequate Response to Anti-TNF Therapy
IM101-029
MeanMean
AbataceptAbataceptN = 258N = 258
PlaceboPlaceboN = 133N = 133
Number of tender jointsNumber of tender joints 3131 3333
Number of swollen joints Number of swollen joints 2222 2222
Physical function, HAQ scorePhysical function, HAQ score 1.81.8 1.81.8
CRP, mg/dLCRP, mg/dL 4.64.6 4.04.0
DAS-28 (ESR)DAS-28 (ESR) 6.96.9 6.96.9

45
Patient Disposition at Six MonthsPatient Disposition at Six Months Patients with Inadequate Response to Anti-TNF TherapyPatients with Inadequate Response to Anti-TNF Therapy
Number (%) of PatientsNumber (%) of Patients
AbataceptAbataceptN = 258N = 258
PlaceboPlaceboN = 133N = 133
Completed Double Blind periodCompleted Double Blind period 223 (86)223 (86) 99 (74)99 (74)
Discontinued Discontinued 35 (14)35 (14) 34 (26)34 (26)
Adverse eventsAdverse events 9 (3.5)9 (3.5) 5 (3.8)5 (3.8)
DeathDeath 00 00
Lack of EfficacyLack of Efficacy 14 (5.4)14 (5.4) 27 (20)27 (20)
Lost to Follow-upLost to Follow-up
Withdrawal of consentWithdrawal of consent
OtherOther
5 (1.9)5 (1.9)
5 (1.9)5 (1.9)
2 (0.8)2 (0.8)
00
2 (1.5)2 (1.5)
00
IM101-029
46
0
10
20
30
40
50
60
70
80
1 29 57 85 113 141 169
Visit Days
% R
es
po
nd
ers
Abatacept (N = 256)
Placebo (N = 133)
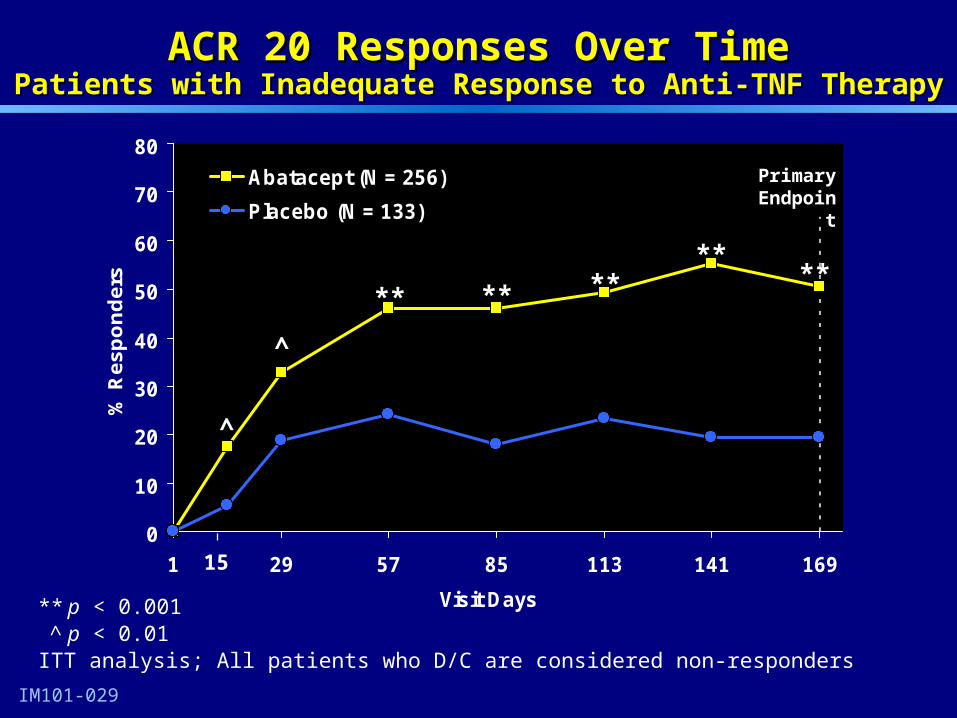
ACR 20 Responses Over TimeACR 20 Responses Over TimePatients with Inadequate Response to Anti-TNF TherapyPatients with Inadequate Response to Anti-TNF Therapy
IM101-029
** ****
**
^
^
**
** p < 0.001^ p < 0.01
ITT analysis; All patients who D/C are considered non-responders
15
Primary Endpoint

47
Substantial Clinical ResponsesSubstantial Clinical ResponsesPatients with Patients with Inadequate Response to Anti-TNF Therapy
0
2
4
6
8
10
12
14
1 29 57 85 113 141 169
Visit Days
% R
es
po
nd
ers
Abatacept (N = 256)
Placebo (N = 133)
15
*
^
** ^
*
** p < 0.001^ p < 0.01* p < 0.05
IM101-029
ACR 70
1
7.97.5
1.50.8
0
2
4
6
8
10
No Swollen Joints No Tender Joints
% o
f P
ati
en
ts
Abatacept (N = 254)
Placebo (N = 130)
% of Patients with Joint Counts of Zero
**
LOCF AnalysisITT analysis; All patients who D/C are considered non-responders

48
Summary of ACR 20 Subgroup Analyses at 6 MonthsSummary of ACR 20 Subgroup Analyses at 6 MonthsPatients with Inadequate Response to Anti-TNF TherapyPatients with Inadequate Response to Anti-TNF Therapy
IM101-029
-20 0 20 40 60 80
All (N = 389)
< 65 years (N = 318)
≥ 65 years (N = 71)
Female (N = 304)
Male (N = 85)
< 60 kg (N = 68)
60-100 kg (N = 266)
> 100 kg (N = 53)
Recent (N = 152)
Prior (N = 237)
Etanercept (N = 104)
Infliximab (N = 208)
Etanercept and Infliximab (N = 77)
All PatientsAll Patients
AgeAge
GenderGender
Anti-TNF HistoryAnti-TNF History
Body weightBody weight
Type of Anti-TNFType of Anti-TNF
Abatacept Better
Placebo Better
Treatment Difference with 95% CI
49
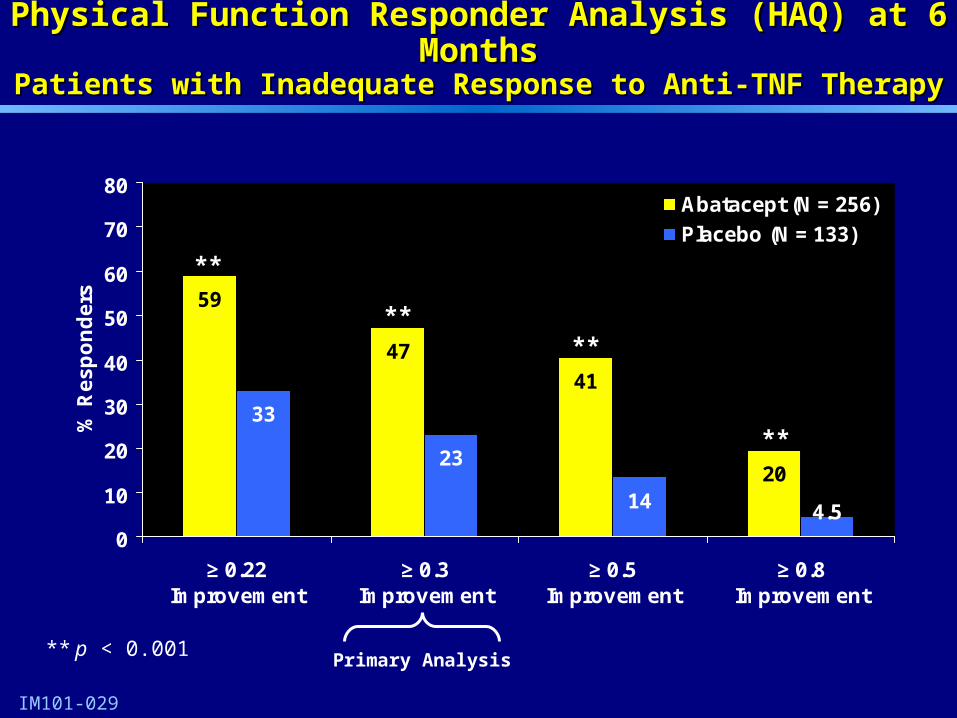
Physical Function Responder Analysis (HAQ) at 6 MonthsPhysical Function Responder Analysis (HAQ) at 6 MonthsPatients with Inadequate Response to Anti-TNF TherapyPatients with Inadequate Response to Anti-TNF Therapy
IM101-029
47
41
2023
14
59
4.5
33
0
10
20
30
40
50
60
70
80
≥ 0.22Improvement
≥ 0.3Improvement
≥ 0.5Improvement
≥ 0.8Improvement
% R
es
po
nd
ers
Abatacept (N = 256)
Placebo (N = 133)
** p < 0.001
**
****
**
Primary Analysis
50
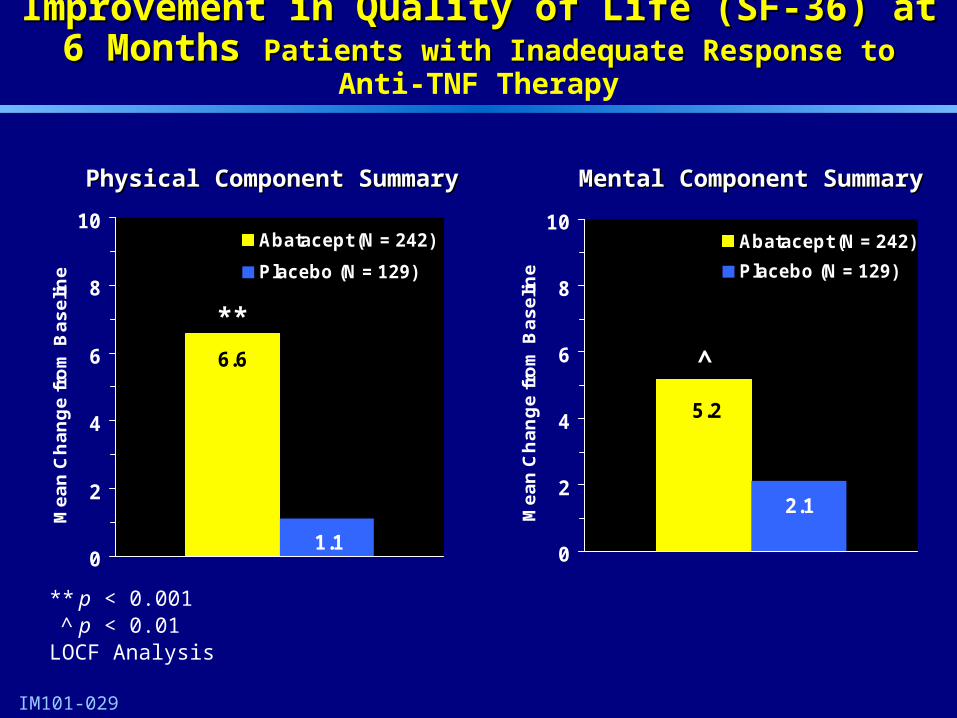
Improvement in Quality of Life (SF-36) at 6 Months Improvement in Quality of Life (SF-36) at 6 Months Patients with Inadequate Response to Patients with Inadequate Response to Anti-TNF Therapy
IM101-029
6.6
1.10
2
4
6
8
10
Me
an
Ch
an
ge
fro
m B
as
elin
e
Abatacept (N = 242)
Placebo (N = 129)
**
Physical Component SummaryPhysical Component Summary
5.2
2.1
0
2
4
6
8
10
Me
an
Ch
an
ge
fro
m B
as
elin
e
Abatacept (N = 242)
Placebo (N = 129)
^
Mental Component SummaryMental Component Summary
** p < 0.001^ p < 0.01
LOCF Analysis

51
Improvement in Quality of Life (SF-36) After 6 Months Improvement in Quality of Life (SF-36) After 6 Months Patients with Inadequate Response to Patients with Inadequate Response to Anti-TNF Therapy
5.3
6.5
8.7
4.0
6.67.3
6.0
4.3
1.3 1.32.5
0.7 1.82.4 2.5
1.60
5
10
15
PhysicalFunction
Role-Physical
Bodily Pain
GeneralHealth
Vitality SocialFunction
Role-Emotional
MentalHealth
Me
an
Ch
an
ge
fro
m B
as
elin
e
Abatacept Placebo
IM101-029
** p < 0.001^ p < 0.01* p < 0.05
LOCF Analysis
****
**
**
****
*
^
52
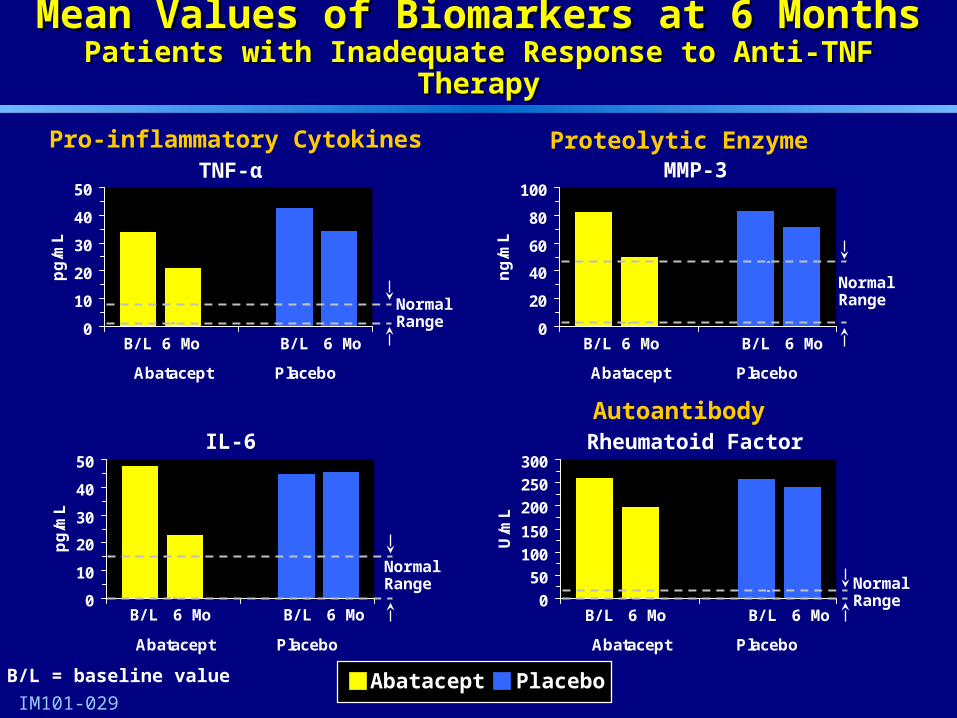
Clinical Biomarker DataClinical Biomarker Data
53
0
10
20
30
40
50
Abatacept Placebo
pg
/mL
Mean Values of Biomarkers at 6 MonthsMean Values of Biomarkers at 6 MonthsPatients with Inadequate Response to Anti-TNF TherapyPatients with Inadequate Response to Anti-TNF Therapy
IM101-029
TNF-α
0
10
20
30
40
50
Abatacept Placebo
pg
/mL
IL-6
MMP-3
Rheumatoid Factor
Pro-inflammatory Cytokines Proteolytic Enzyme
Autoantibody
0
20
40
60
80
100
Abatacept Placebo
ng
/mL
0
50
100
150
200
250
300
Abatacept Placebo
U/m
L
Abatacept Placebo
B/L 6 Mo B/L 6 Mo
B/L 6 Mo B/L 6 Mo
B/L 6 Mo B/L 6 Mo
B/L 6 Mo B/L 6 Mo
Normal Range Normal
Range
Normal RangeNormal
Range
B/L = baseline value
54
ConclusionsConclusions
All primary and key secondary outcomes achieved:All primary and key secondary outcomes achieved:– Consistent effect on ACR 20, 50 and 70Consistent effect on ACR 20, 50 and 70– Inhibition of structural damage Inhibition of structural damage – Improvement in physical function and Improvement in physical function and
quality of lifequality of life
Major reductions in disease activity:Major reductions in disease activity:– ACR 70 responseACR 70 response– Major clinical responseMajor clinical response– Proportion of patients with no swollen or Proportion of patients with no swollen or
tendertender jointsjoints

55
Daniel J. MacNeil, M.D.Daniel J. MacNeil, M.D.Executive DirectorExecutive Director
Global PharmacovigilanceGlobal Pharmacovigilance Bristol-Myers Squibb Bristol-Myers Squibb
Abatacept:Abatacept:Summary of SafetySummary of Safety

56
Abatacept Safety Presentation TopicsAbatacept Safety Presentation Topics
Description of patient population and overview Description of patient population and overview
of general safety and tolerabilityof general safety and tolerability
Clinical findings on infection and malignancyClinical findings on infection and malignancy
Plans for further assessment of safety profile Plans for further assessment of safety profile post-approvalpost-approval
57
Safety Assessment Methods Safety Assessment Methods
Based on safety data provided to and reviewed by Based on safety data provided to and reviewed by FDA in BLA and 4 Month Safety Update FDA in BLA and 4 Month Safety Update
Tables include events occurring up to 56 days Tables include events occurring up to 56 days post last dose of study drug (5 half-lives) post last dose of study drug (5 half-lives)
Adverse events classified using standard coding Adverse events classified using standard coding dictionary, MedDRA dictionary, MedDRA
Severity classified by investigator according to Severity classified by investigator according to regulatory and functional criteria regulatory and functional criteria
58
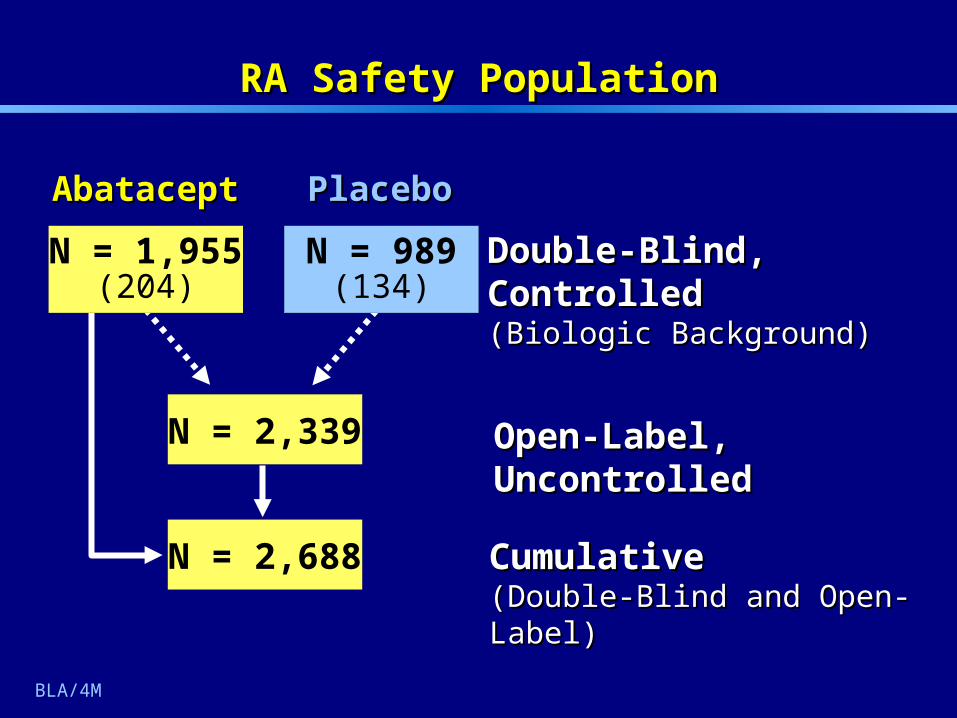
RA Safety PopulationRA Safety Population
Cumulative Cumulative (Double-Blind and Open-Label)(Double-Blind and Open-Label)
Open-Label, UncontrolledOpen-Label, UncontrolledN = 2,339
N = 2,688
PlaceboPlaceboAbataceptAbatacept
N = 1,955(204)
Double-Blind, ControlledDouble-Blind, Controlled(Biologic Background)(Biologic Background)
N = 989(134)
BLA/4M
59
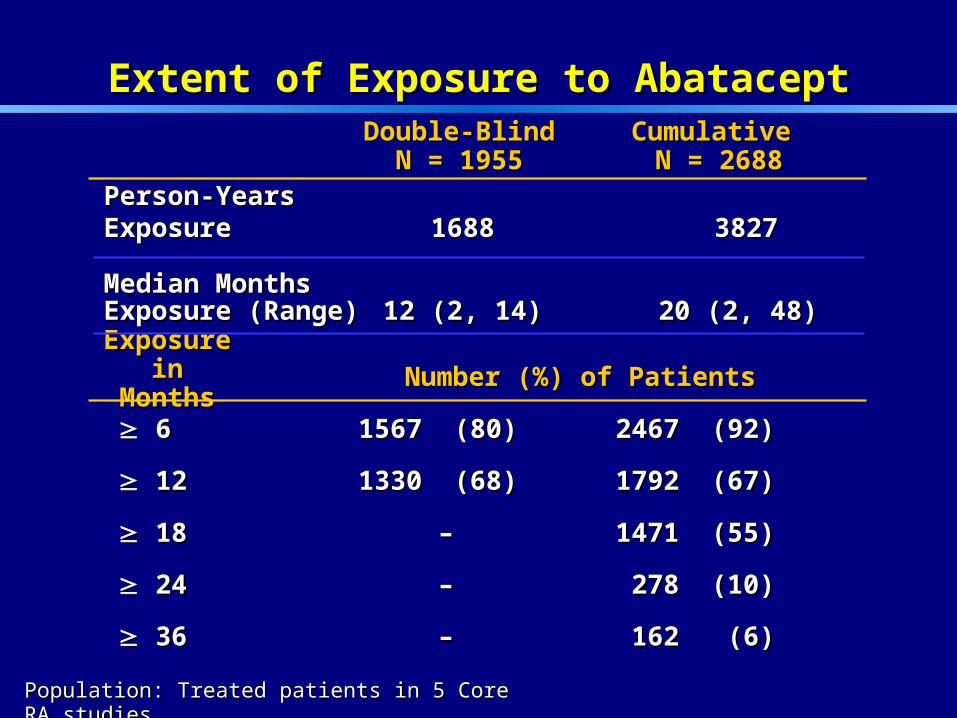
Extent of Exposure to AbataceptExtent of Exposure to Abatacept
Population: Treated patients in 5 Core RA studiesPopulation: Treated patients in 5 Core RA studies
66 1567 1567 (80) (80) 2467 2467 (92)(92)
1212 1330 1330 (68) (68) 1792 1792 (67)(67)
1818 –– 1471 1471 (55)(55)
2424 –– 278 278 (10)(10)
3636 –– 162 162 (6) (6)
Exposure Exposure in Monthsin Months Number (%) of PatientsNumber (%) of Patients
Cumulative Cumulative N = 2688N = 2688
Double-BlindDouble-Blind N = 1955 N = 1955
Person-YearsPerson-YearsExposure Exposure 16881688 3827 3827
Median MonthsMedian MonthsExposure (Range)Exposure (Range) 12 (2, 14)12 (2, 14) 20 (2, 48) 20 (2, 48)
60
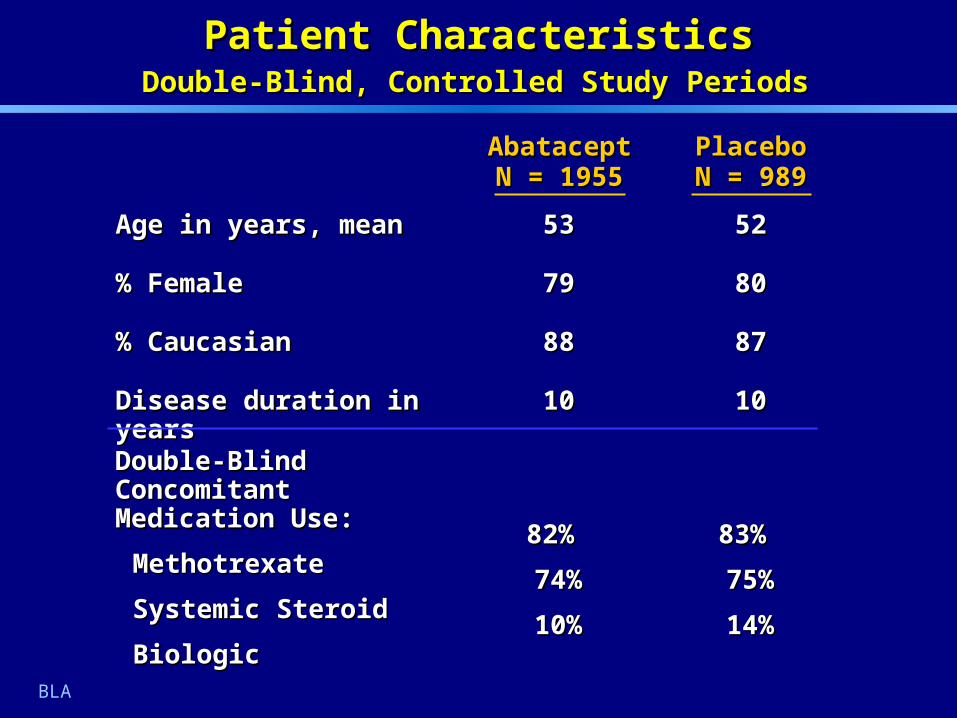
Age in years, meanAge in years, mean
% Female% Female
% Caucasian% Caucasian
Disease duration in yearsDisease duration in years
5252
8080
8787
1010
PlaceboPlaceboN = 989N = 989
5353
7979
8888
1010
Patient CharacteristicsPatient Characteristics Double-Blind, Controlled Study Periods Double-Blind, Controlled Study Periods
AbataceptAbataceptN = 1955N = 1955
Double-Blind Concomitant Double-Blind Concomitant Medication Use: Medication Use:
MethotrexateMethotrexate
Systemic SteroidSystemic Steroid
BiologicBiologic
83% 83%
75%75%
14%14%
82% 82%
74%74%
10%10%
BLA

61
Overview of Patients with Adverse EventsOverview of Patients with Adverse EventsDouble-Blind, Controlled Study PeriodsDouble-Blind, Controlled Study Periods
AEsAEs
SAEsSAEs
Discontinuation due to AEsDiscontinuation due to AEs
DeathsDeaths
AbataceptAbataceptN = 1955N = 1955
1736 (88.8)1736 (88.8)
266 (13.6)266 (13.6)
107 (5.5) 107 (5.5)
10 (0.5)10 (0.5)
PlaceboPlaceboN = 989N = 989
840 (84.9)840 (84.9)
122 (12.3)122 (12.3)
39 (3.9)39 (3.9)
6 (0.6)6 (0.6)
Number (%) of PatientsNumber (%) of Patients
62
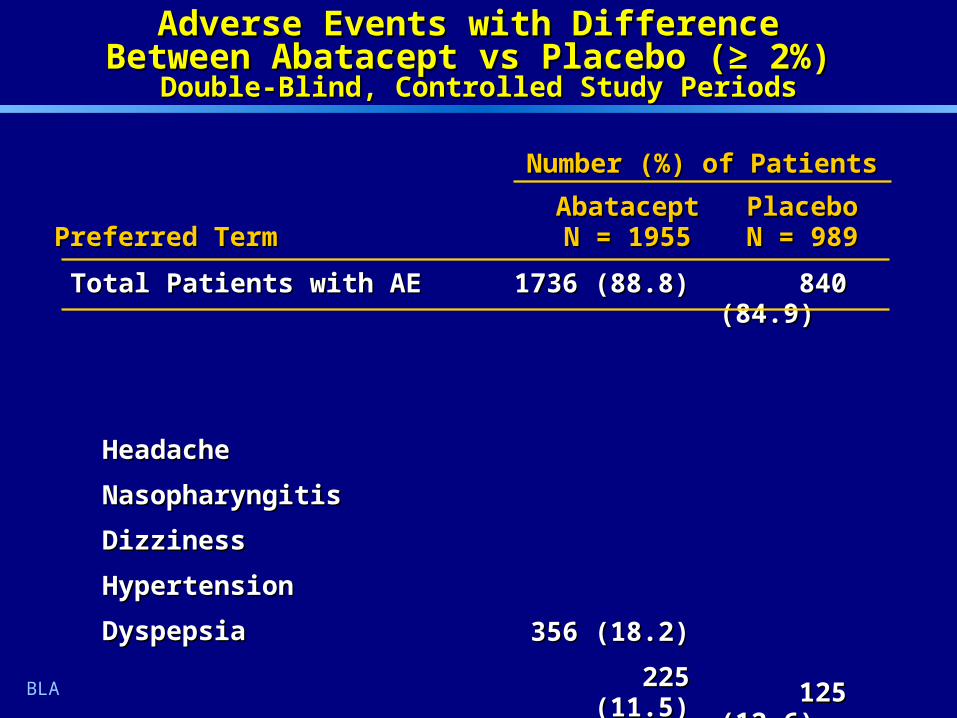
Adverse Events with Difference Adverse Events with Difference Between Abatacept vs Placebo (Between Abatacept vs Placebo (≥≥2%) 2%)
Double-Blind, Controlled Study PeriodsDouble-Blind, Controlled Study Periods
Total Patients with AE Total Patients with AE
HeadacheHeadache
NasopharyngitisNasopharyngitis
DizzinessDizziness
HypertensionHypertension
DyspepsiaDyspepsia
1736 (88.8) 1736 (88.8)
356 (18.2)356 (18.2)
225 (11.5)225 (11.5)
183 (9.4)183 (9.4)
129 (6.6)129 (6.6)
126 (6.4) 126 (6.4)
840 (84.9) 840 (84.9)
125 (12.6) 125 (12.6)
90 (9.1) 90 (9.1)
69 (7.0) 69 (7.0)
43 (4.3) 43 (4.3)
42 (4.2)42 (4.2)
Preferred TermPreferred TermAbataceptAbataceptN = 1955N = 1955
PlaceboPlaceboN = 989N = 989
BLA
Number (%) of PatientsNumber (%) of Patients
63
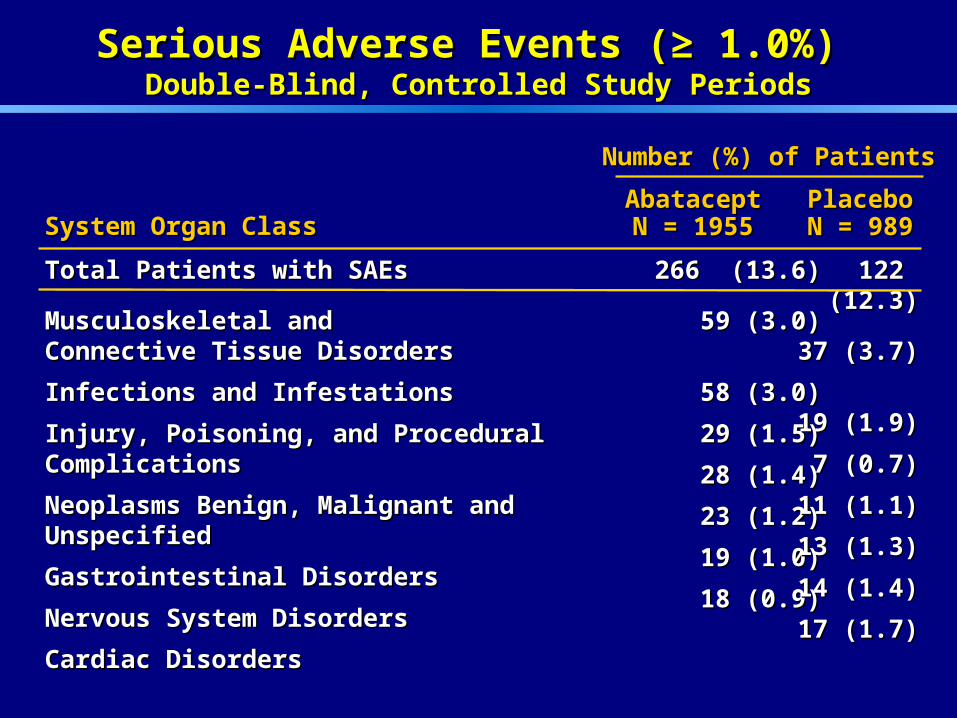
Total Patients with SAEs Total Patients with SAEs
Musculoskeletal and Musculoskeletal and Connective Tissue DisordersConnective Tissue Disorders
Infections and InfestationsInfections and Infestations
Injury, Poisoning, and Procedural ComplicationsInjury, Poisoning, and Procedural Complications
Neoplasms Benign, Malignant and Unspecified Neoplasms Benign, Malignant and Unspecified
Gastrointestinal Disorders Gastrointestinal Disorders
Nervous System DisordersNervous System Disorders
Cardiac DisordersCardiac Disorders
Serious Adverse Events (≥ 1.0%) Serious Adverse Events (≥ 1.0%) Double-Blind, Controlled Study PeriodsDouble-Blind, Controlled Study Periods
266 (13.6)266 (13.6)
59 (3.0)59 (3.0)
58 (3.0)58 (3.0)
29 (1.5)29 (1.5)
28 (1.4)28 (1.4)
23 (1.2)23 (1.2)
19 (1.0)19 (1.0)
18 (0.9)18 (0.9)
System Organ ClassSystem Organ ClassAbataceptAbataceptN = 1955N = 1955
PlaceboPlaceboN = 989N = 989
122 (12.3)122 (12.3)
37 (3.7)37 (3.7)
19 (1.9)19 (1.9)
7 (0.7)7 (0.7)
11 (1.1)11 (1.1)
13 (1.3)13 (1.3)
14 (1.4)14 (1.4)
17 (1.7)17 (1.7)
Number (%) of PatientsNumber (%) of Patients
64
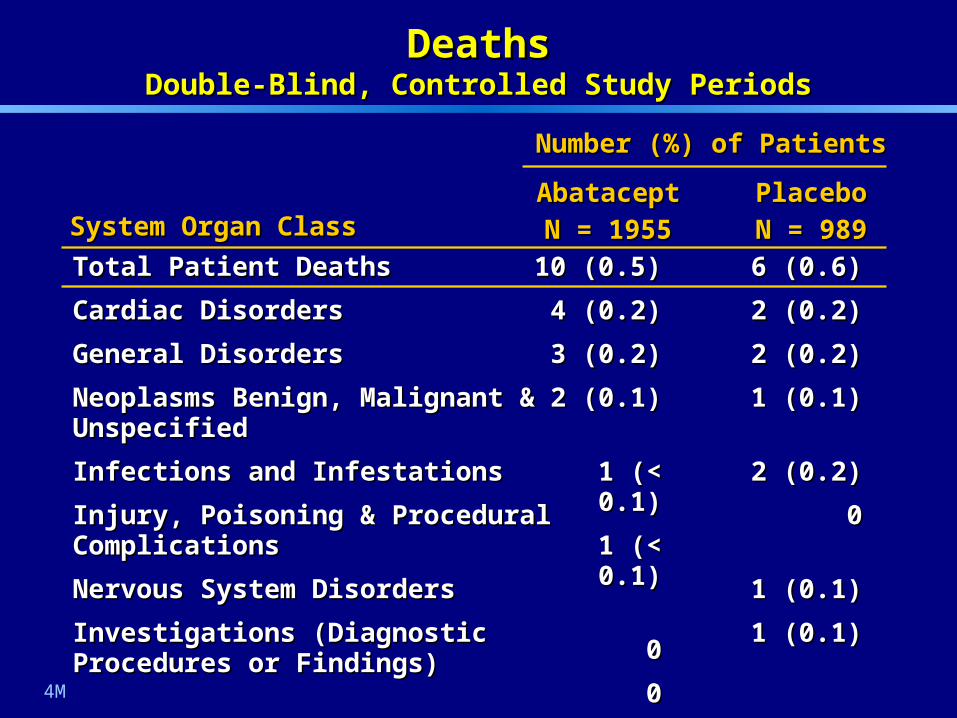
Total Patient DeathsTotal Patient Deaths
Cardiac DisordersCardiac Disorders
General DisordersGeneral Disorders
Neoplasms Benign, Malignant & Neoplasms Benign, Malignant & UnspecifiedUnspecified
Infections and InfestationsInfections and Infestations
Injury, Poisoning & Procedural Injury, Poisoning & Procedural ComplicationsComplications
Nervous System DisordersNervous System Disorders
Investigations (Diagnostic Procedures Investigations (Diagnostic Procedures or Findings)or Findings)
DeathsDeathsDouble-Blind, Controlled Study PeriodsDouble-Blind, Controlled Study Periods
10 (0.5)10 (0.5)
4 (0.2)4 (0.2)
3 (0.2)3 (0.2)
2 (0.1)2 (0.1)
1 (< 0.1)1 (< 0.1)
1 (< 0.1)1 (< 0.1)
00
00
6 (0.6)6 (0.6)
2 (0.2)2 (0.2)
2 (0.2)2 (0.2)
1 (1 (00.1).1)
2 (0.2)2 (0.2)
00
1 (0.1)1 (0.1)
1 (0.1)1 (0.1)
System Organ ClassSystem Organ ClassAbataceptAbatacept
N = 1955N = 1955PlaceboPlacebo
N = 989N = 989
Number (%) of PatientsNumber (%) of Patients
4M
65
Safety in Combination with Safety in Combination with Other Biologic TherapiesOther Biologic Therapies
66
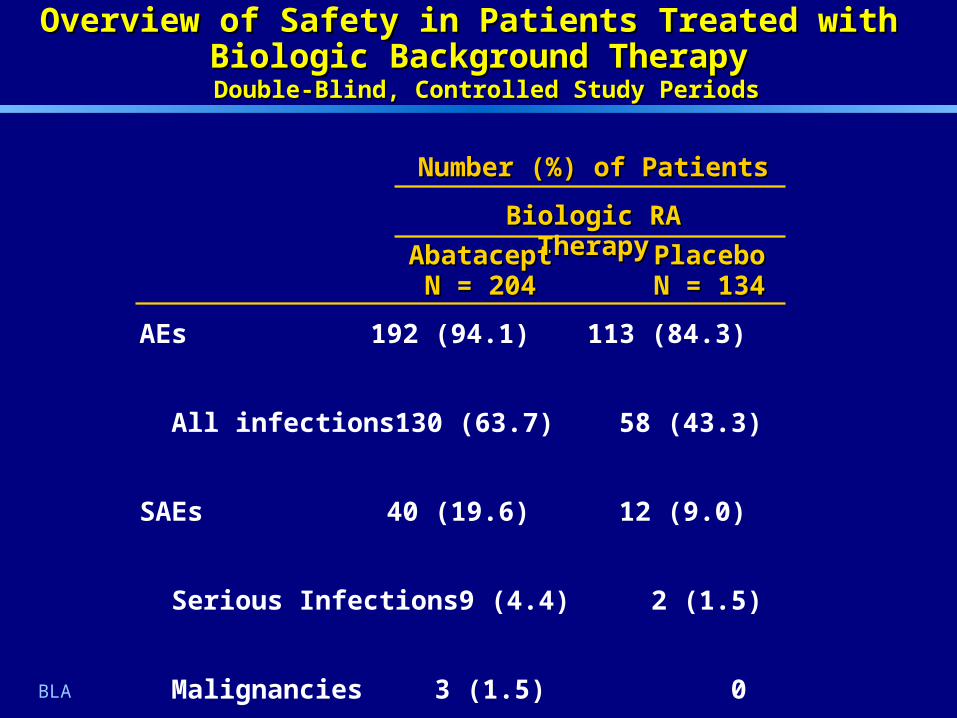
AbataceptAbataceptN = 204N = 204
PlaceboPlaceboN = 134N = 134
Overview of Safety in Patients Treated with Overview of Safety in Patients Treated with Biologic Background TherapyBiologic Background Therapy Double-Blind, Controlled Study PeriodsDouble-Blind, Controlled Study Periods
AEs 192 (94.1) 113 (84.3)
All infections 130 (63.7) 58 (43.3)
SAEs 40 (19.6) 12 (9.0)
Serious Infections 9 (4.4) 2 (1.5)
Malignancies 3 (1.5) 0
Deaths 0 0
Biologic RA TherapyBiologic RA Therapy
BLA
Number (%) of PatientsNumber (%) of Patients
67
Special Topics:Special Topics:Infections and MalignanciesInfections and Malignancies

68
InfectionsInfections
Frequency and Type of Infection Frequency and Type of Infection – Overall Overall – Most Common Most Common – Serious Serious
Severity of InfectionSeverity of Infection– % serious, % severe or very severe in intensity% serious, % severe or very severe in intensity– % IV antibiotic therapy% IV antibiotic therapy– % resulting in discontinuation of therapy% resulting in discontinuation of therapy– % resulting in death % resulting in death
Incidence Rate of Infection over time Incidence Rate of Infection over time Infections of Particular Interest Infections of Particular Interest
– Pneumonia Pneumonia – HerpesHerpes– Tuberculosis Tuberculosis

69
Total Patients with InfectionsTotal Patients with Infections
Upper Respiratory Tract InfectionUpper Respiratory Tract Infection
NasopharyngitisNasopharyngitis
SinusitisSinusitis
Urinary Tract Infection Urinary Tract Infection
InfluenzaInfluenza
BronchitisBronchitis
1051 (53.8)1051 (53.8)
248 (12.7)248 (12.7)
225 (11.5)225 (11.5)
125 (6.4)125 (6.4)
113 (5.8)113 (5.8)
111 (5.7)111 (5.7)
101 (5.2)101 (5.2)
478 (48.3)478 (48.3)
119 (12.0)119 (12.0)
90 (9.1) 90 (9.1)
68 (6.9) 68 (6.9)
45 (4.6) 45 (4.6)
52 (5.3) 52 (5.3)
45 (4.6) 45 (4.6)
Most Common Infections (≥ 5%) Most Common Infections (≥ 5%) Double-Blind, Controlled Study PeriodsDouble-Blind, Controlled Study Periods
Preferred TermPreferred TermAbataceptAbataceptN = 1955N = 1955
PlaceboPlaceboN = 989N = 989
Number (%) of PatientsNumber (%) of Patients
BLA
70
Total Patients with Serious InfectionsTotal Patients with Serious Infections
PneumoniaPneumonia
CellulitisCellulitis
Urinary Tract Infection Urinary Tract Infection
Bronchitis Bronchitis
DiverticulitisDiverticulitis
Pyelonephritis AcutePyelonephritis Acute
SepsisSepsis
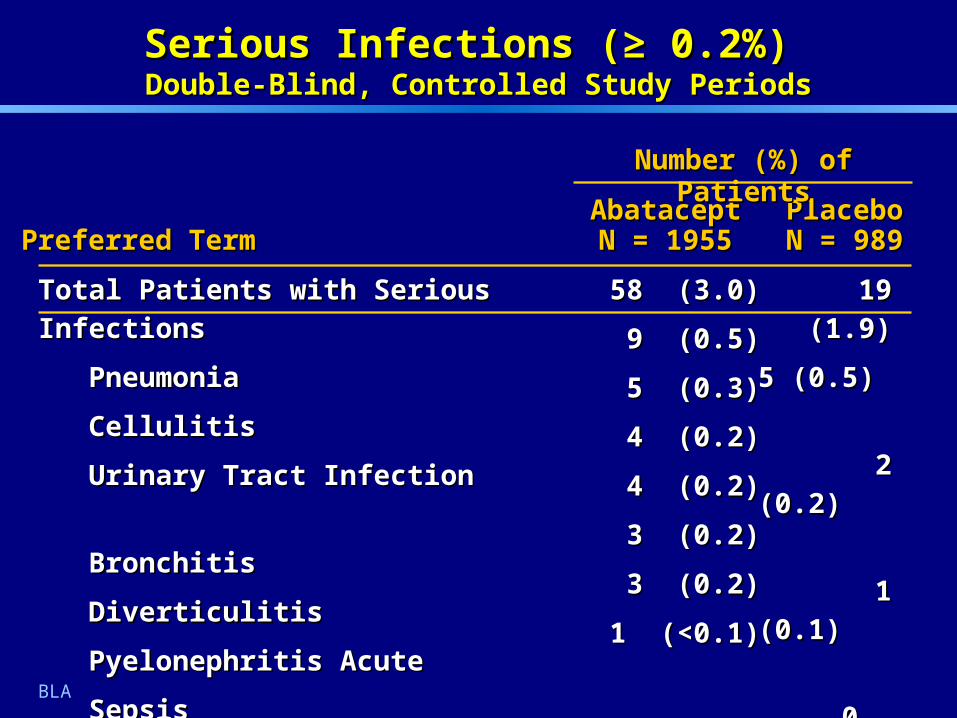
Serious Infections (≥ 0.2%) Serious Infections (≥ 0.2%) Double-Blind, Controlled Study PeriodsDouble-Blind, Controlled Study Periods
58 (3.0)58 (3.0)
9 (0.5)9 (0.5)
5 (0.3)5 (0.3)
4 (0.2)4 (0.2)
4 (0.2)4 (0.2)
3 (0.2)3 (0.2)
3 (0.2)3 (0.2)
1 (<0.1)1 (<0.1)
19 (1.9)19 (1.9)
5 (0.5) 5 (0.5)
2 (0.2) 2 (0.2)
1 (0.1) 1 (0.1)
0 0
0 0
0 0
3 (0.3)3 (0.3)
Preferred TermPreferred TermAbataceptAbataceptN = 1955N = 1955
PlaceboPlaceboN = 989N = 989
Number (%) of PatientsNumber (%) of Patients
BLA
71
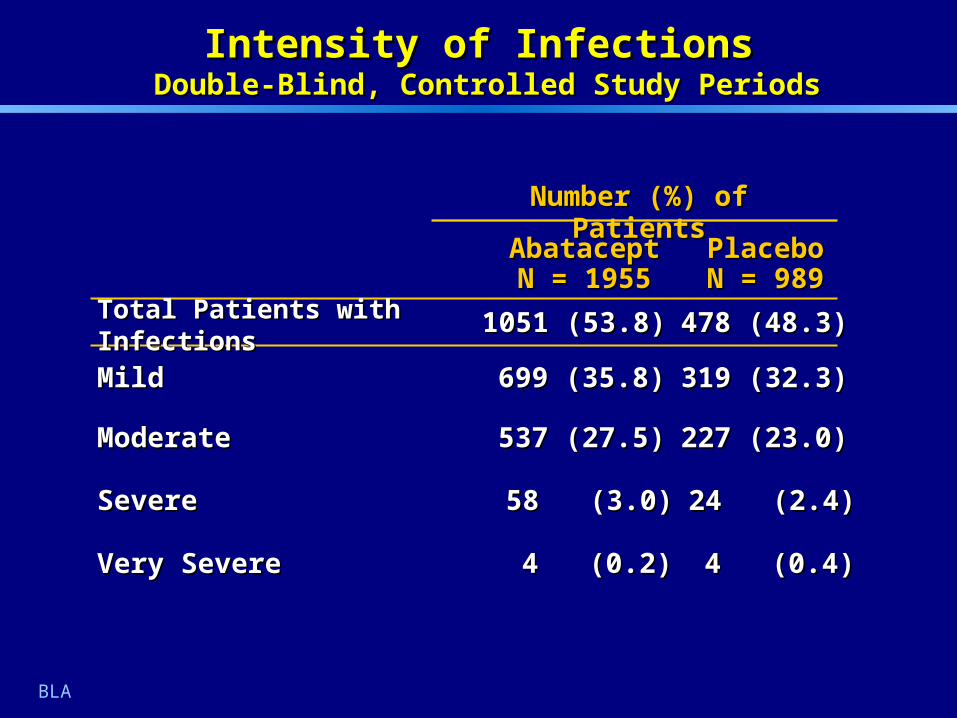
Intensity of InfectionsIntensity of Infections Double-Blind, Controlled Study Periods Double-Blind, Controlled Study Periods
PlaceboPlaceboN = 989N = 989
AbataceptAbataceptN = 1955N = 1955
24 (2.4)24 (2.4)58 (3.0)58 (3.0)SevereSevere
4 (0.4)4 (0.4)4 (0.2)4 (0.2)Very SevereVery Severe
227 (23.0)227 (23.0)537 (27.5)537 (27.5)ModerateModerate
319 (32.3)319 (32.3)699 (35.8)699 (35.8)MildMild
Number (%) of PatientsNumber (%) of Patients
BLA
478 (48.3)478 (48.3)1051 (53.8)1051 (53.8)Total Patients with InfectionsTotal Patients with Infections

72
IV Antibiotics UseIV Antibiotics Use
StudyStudy# Months on # Months on Study DrugStudy Drug AbataceptAbatacept PlaceboPlacebo
IM101-102IM101-102(MTX-IR)(MTX-IR)
0 – 60 – 6 9/433 (2.1)9/433 (2.1) 5/219 (2.3)5/219 (2.3)
6 – 126 – 12 15/401 (3.7) 15/401 (3.7) 7/174 (4.0)7/174 (4.0)
IM101-029IM101-029(Anti-TNF IR)(Anti-TNF IR) 0 – 60 – 6 3/258 (1.2)3/258 (1.2) 4/133 (3.0)4/133 (3.0)
IM101-031IM101-031(Safety)(Safety) 0 – 120 – 12 38/959 (4.0) 38/959 (4.0) 18/482 (3.7) 18/482 (3.7)
BLA
n/N (%) of Patientsn/N (%) of Patients
73
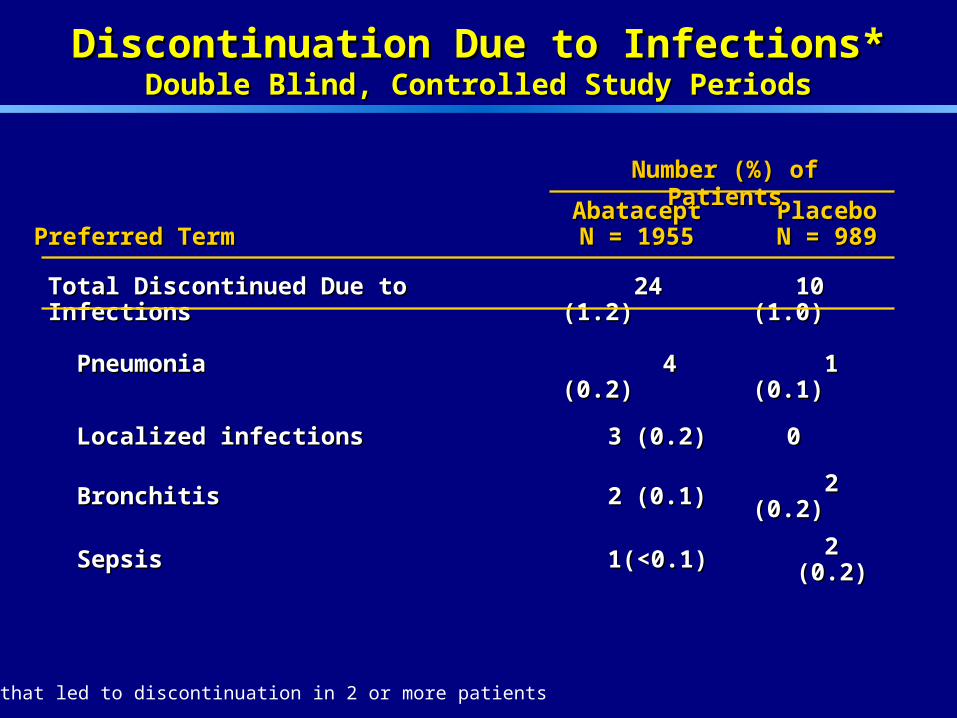
Total Discontinued Due to InfectionsTotal Discontinued Due to Infections
PneumoniaPneumonia
24 (1.2)24 (1.2)
4 4 (0.2)(0.2)
10 (1.0)10 (1.0)
1 (0.1)1 (0.1)
Localized infectionsLocalized infections 33 (0.2)(0.2) 00
BronchitisBronchitis 22 (0.1)(0.1) 2 (0.2)2 (0.2)
SepsisSepsis 11 (<0.1) (<0.1) 2 (0.2)2 (0.2)
Discontinuation Due to Infections*Discontinuation Due to Infections*Double Blind, Controlled Study PeriodsDouble Blind, Controlled Study Periods
* AEs that led to discontinuation in 2 or more patients
Preferred TermPreferred TermAbataceptAbataceptN = 1955N = 1955
PlaceboPlaceboN = 989N = 989
Number (%) of PatientsNumber (%) of Patients
74
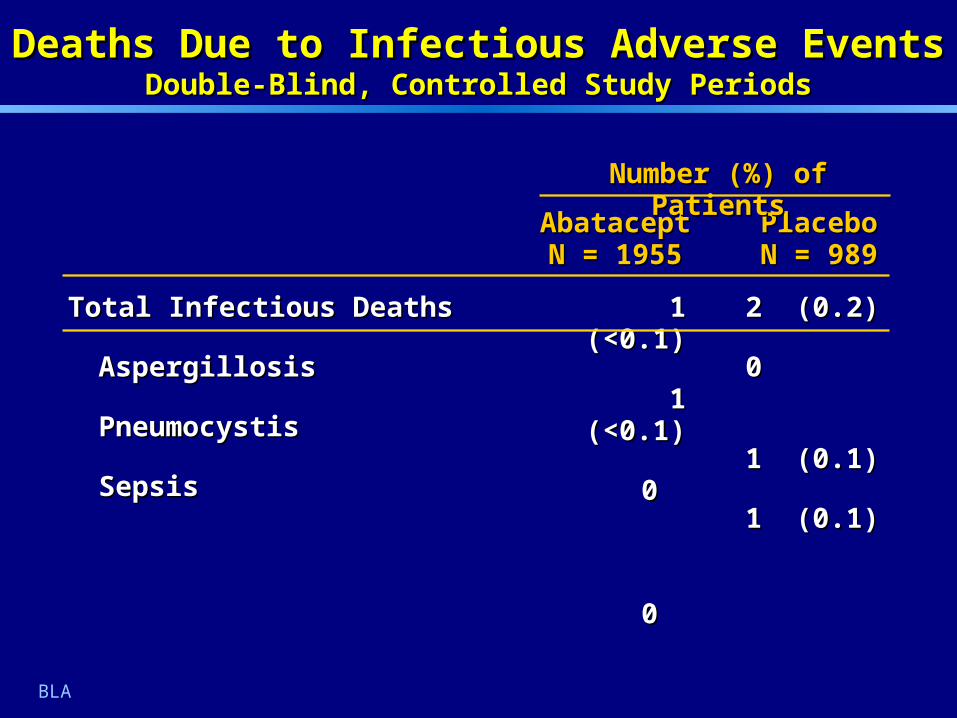
Deaths Due to Infectious Adverse EventsDeaths Due to Infectious Adverse EventsDouble-Blind, Controlled Study PeriodsDouble-Blind, Controlled Study Periods
Total Infectious DeathsTotal Infectious Deaths
AspergillosisAspergillosis
PneumocystisPneumocystis
SepsisSepsis
AbataceptAbataceptN = 1955N = 1955
1 (<0.1)1 (<0.1)
1 (<0.1)1 (<0.1)
0 0
00
PlaceboPlaceboN = 989N = 989
2 (0.2)2 (0.2)
0 0
1 (0.1)1 (0.1)
1 (0.1)1 (0.1)
Number (%) of PatientsNumber (%) of Patients
BLA

75
Time Intervals (Months)Time Intervals (Months)
0-6 0-6 6-126-12 12-1812-18 18-2418-24 24-30 24-30 >30 >30
n/p-y*n/p-y* 50/128550/1285 39/103239/1032 22/79522/795 9/3999/399 4/1174/117 3/1983/198
IR/100 p-y**IR/100 p-y** 3.923.92 3.813.81 2.782.78 2.262.26 3.453.45 1.531.53
(95% CI)(95% CI) (2.91, 5.17)(2.91, 5.17) (2.71, 5.20)(2.71, 5.20) (1.74, 4.21)(1.74, 4.21) (1.03, 4.29)(1.03, 4.29) (0.94, 8.83)(0.94, 8.83) (0.31, 4.46)(0.31, 4.46)
Serious Infection Incidence Rates by Time IntervalsSerious Infection Incidence Rates by Time IntervalsCumulative Study Periods – Through 4 Month UpdateCumulative Study Periods – Through 4 Month Update
* n/p-y = Number of patients / person-years** IR/100 p-y = Incidence rates per 100 person-years
4M
76
Number (%) of PatientsNumber (%) of Patients
AbataceptAbataceptN = 1955N = 1955
PlaceboPlaceboN = 989N = 989
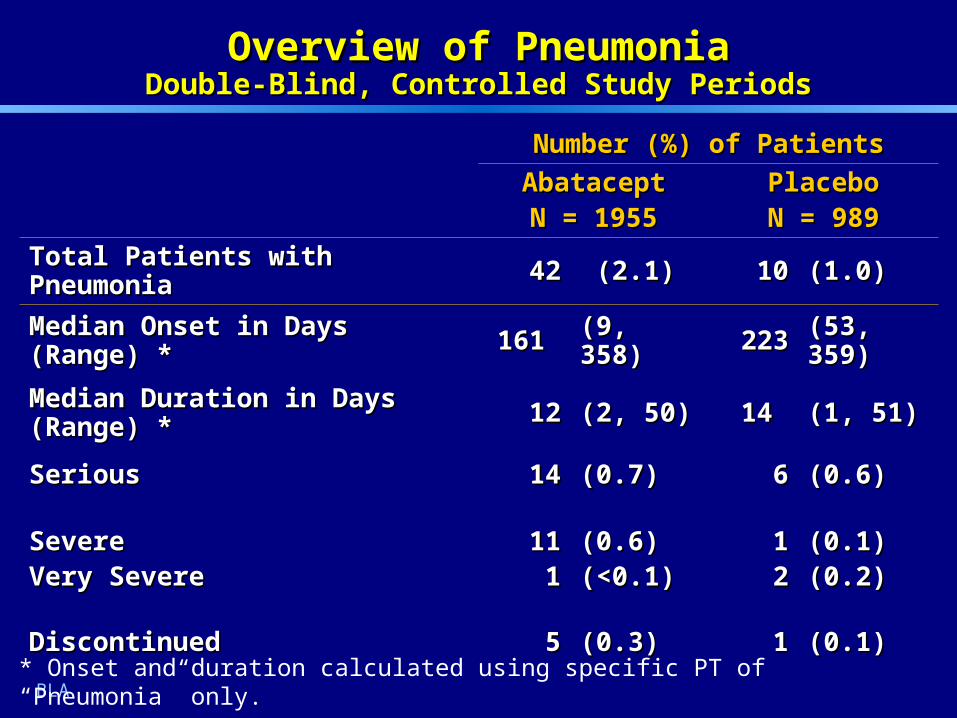
Total Patients with PneumoniaTotal Patients with Pneumonia 4242 (2.1)(2.1) 1010 (1.0)(1.0)
Median Onset in Days (Range) *Median Onset in Days (Range) * 161 161 (9, 358)(9, 358) 223223 (53, 359)(53, 359)
Median Duration in Days (Range) *Median Duration in Days (Range) * 1212 (2, 50)(2, 50) 14 14 (1, 51)(1, 51)
SeriousSerious 1414 (0.7)(0.7) 66 (0.6)(0.6)
SevereSevereVery SevereVery Severe
111111
(0.6)(0.6)(<0.1)(<0.1)
1122
(0.1)(0.1)(0.2)(0.2)
DiscontinuedDiscontinued 55 (0.3)(0.3) 11 (0.1)(0.1)
Overview of PneumoniaOverview of PneumoniaDouble-Blind, Controlled Study PeriodsDouble-Blind, Controlled Study Periods
BLA* Onset and duration calculated using specific PT of “Pneumonia” only.

77
Incidence of Infections in Herpes FamilyIncidence of Infections in Herpes FamilyDouble-Blind, Controlled Study PeriodsDouble-Blind, Controlled Study Periods
Number (%) of PatientsNumber (%) of Patients
Preferred TermPreferred TermAbataceptAbataceptN = 1955N = 1955
PlaceboPlaceboN = 989N = 989
Herpes SimplexHerpes Simplex 37 37 (1.9)(1.9) 1010 (1.0)(1.0)
Herpes ZosterHerpes Zoster 3030 (1.5)(1.5) 1616 (1.6)(1.6)
Herpes Viral InfectionHerpes Viral Infection 55 (0.3)(0.3) 22 (0.2)(0.2)
VaricellaVaricella 33 (0.2)(0.2) 00
Epstein-Barr VirusEpstein-Barr Virus 00 00
CytomegalovirusCytomegalovirus 00 00
BLA
78
TuberculosisTuberculosisCumulative Study PeriodsCumulative Study Periods
2 cases of presumed tuberculosis with abatacept2 cases of presumed tuberculosis with abatacept Tuberculous Infection (Double-Blind): Tuberculous Infection (Double-Blind):
– Presented with cervical lymphadenitis; diagnosis Presented with cervical lymphadenitis; diagnosis based on histologybased on histology
Pulmonary Tuberculosis Suspected (Open-Label)Pulmonary Tuberculosis Suspected (Open-Label)
– Presented with dry cough, fever, diaphoresis and Presented with dry cough, fever, diaphoresis and crepitus; diagnosis based on clinical presentation crepitus; diagnosis based on clinical presentation and chest radiographand chest radiograph
1 case of presumed tuberculosis with placebo1 case of presumed tuberculosis with placebo Tuberculosis - Suspect (Double-Blind): Tuberculosis - Suspect (Double-Blind):
– Unknown presentation; no definitive diagnosisUnknown presentation; no definitive diagnosis

79
Infections: ConclusionsInfections: Conclusions
Abatacept treatment associated with an increase Abatacept treatment associated with an increase in frequency of infections, including 1% increase in frequency of infections, including 1% increase in serious infectionsin serious infections
Infections occurring with abatacept were similar to Infections occurring with abatacept were similar to those occurring on placebo in type, severity, those occurring on placebo in type, severity, treatment, duration, and outcometreatment, duration, and outcome

80
MalignancyMalignancy
PresentationPresentation
– Non-clinical findingsNon-clinical findings
– Overall clinical experienceOverall clinical experience
– Malignancies of particular interestMalignancies of particular interest Evaluation based onEvaluation based on
– Frequency versus placebo in Double-BlindFrequency versus placebo in Double-Blind
– Incidence over time in Cumulative PeriodIncidence over time in Cumulative Period
– Incidence relative to reference databases Incidence relative to reference databases (both general population and RA specific)(both general population and RA specific)
– Clinical characteristicsClinical characteristics

81
Carcinogenicity Study in MiceCarcinogenicity Study in Mice
Duration: up to 88 weeksDuration: up to 88 weeks
Exposures: 0.8-, 1.9- and 3.0-fold human exposureExposures: 0.8-, 1.9- and 3.0-fold human exposure
Sustained immunomodulation at all dose levelsSustained immunomodulation at all dose levels
Increased incidence of virally mediated tumorsIncreased incidence of virally mediated tumors
– Lymphoma at all doses Lymphoma at all doses Murine leukemia virus detected in Murine leukemia virus detected in
genome of micegenome of mice
– Mammary gland tumors in females at top two Mammary gland tumors in females at top two dosesdoses Mouse mammary tumor virus detected Mouse mammary tumor virus detected
in tumorsin tumors
82
Primate Toxicology StudyPrimate Toxicology Study
Conventional toxicology study enhanced to Conventional toxicology study enhanced to evaluate lymphoid neoplasiaevaluate lymphoid neoplasia
Duration: One year study – cynomolgus monkeysDuration: One year study – cynomolgus monkeys
Exposure multiples up to 9-fold human exposureExposure multiples up to 9-fold human exposure
Oncogenic virus in genome of 38/40 monkeysOncogenic virus in genome of 38/40 monkeys
No lymphoma or pre-lymphomatous changesNo lymphoma or pre-lymphomatous changes

83
Total 26 (1.3) 11 (1.1)
Non-melanoma Skin 15 (0.8) 6 (0.6) Basal Cell Carcinoma 10 (0.5) 4 (0.4) Squamous Cell Carcinoma 6 (0.3) 2 (0.2)Solid 9 (0.5) 5 (0.5) Lung 4 (0.2) 0 Thyroid 2 (0.1) 0 Breast 1 (<0.1) 2 (0.2) Prostate 1 (<0.1) 0 Bladder 1 (<0.1) 0 Renal 1 (<0.1) 0 Endometrial / Uterine 0 2 (0.2) Melanoma 0 1 (0.1)Hematologic 2 (0.1) 0 Lymphoma 1 (<0.1) 0 Myelodysplastic Syndrome 1 (<0.1) 0
MalignanciesMalignanciesDouble-Blind, Controlled Study PeriodsDouble-Blind, Controlled Study Periods
AbataceptAbataceptN = 1955N = 1955
Placebo Placebo N = 989N = 989Type of MalignancyType of Malignancy
4M
Number (%) of PatientsNumber (%) of Patients
84
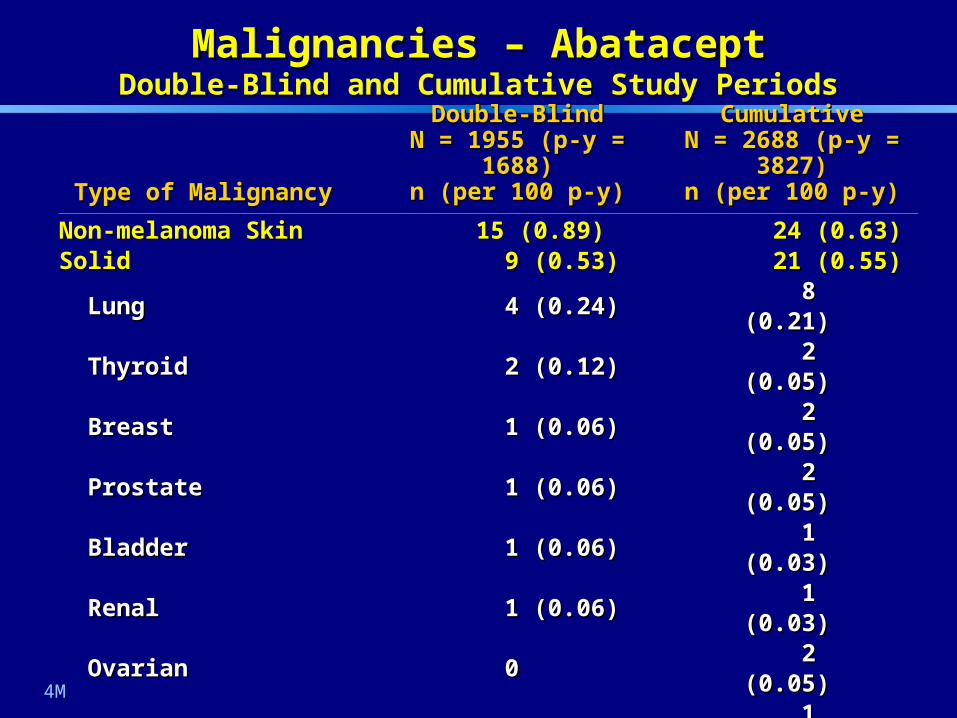
Non-melanoma Skin Non-melanoma Skin 15 (0.89)15 (0.89) 24 (0.63)24 (0.63)SolidSolid 9 (0.53)9 (0.53) 21 (0.55)21 (0.55) Lung Lung 4 (0.24)4 (0.24) 8 (0.21)8 (0.21) ThyroidThyroid 2 (0.12)2 (0.12) 2 (0.05)2 (0.05) BreastBreast 1 (0.06)1 (0.06) 2 (0.05)2 (0.05) ProstateProstate 1 (0.06)1 (0.06) 2 (0.05)2 (0.05) BladderBladder 1 (0.06)1 (0.06) 1 (0.03)1 (0.03) RenalRenal 1 (0.06)1 (0.06) 1 (0.03)1 (0.03) OvarianOvarian 00 2 (0.05)2 (0.05) MelanomaMelanoma 00 1 (0.03)1 (0.03) Endometrial / UterineEndometrial / Uterine 00 2 (0.05)2 (0.05) CervixCervix 00 1 (0.03)1 (0.03)HematologicHematologic 2 (0.12)2 (0.12) 5 (0.13)5 (0.13) LymphomaLymphoma 1 (0.06)1 (0.06) 4 (0.10)4 (0.10) Myelodysplastic SyndromeMyelodysplastic Syndrome 1 (0.06)1 (0.06) 1 (0.03)1 (0.03)
Malignancies – AbataceptMalignancies – AbataceptDouble-Blind and Cumulative Study PeriodsDouble-Blind and Cumulative Study Periods
Type of MalignancyType of Malignancy
Double-BlindDouble-BlindN = 1955 (p-y = 1688)N = 1955 (p-y = 1688)
n (per 100 p-y)n (per 100 p-y)
CumulativeCumulativeN = 2688 (p-y = 3827)N = 2688 (p-y = 3827)
n (per 100 p-y)n (per 100 p-y)
4M
85
0.01 0.1 1 10 100
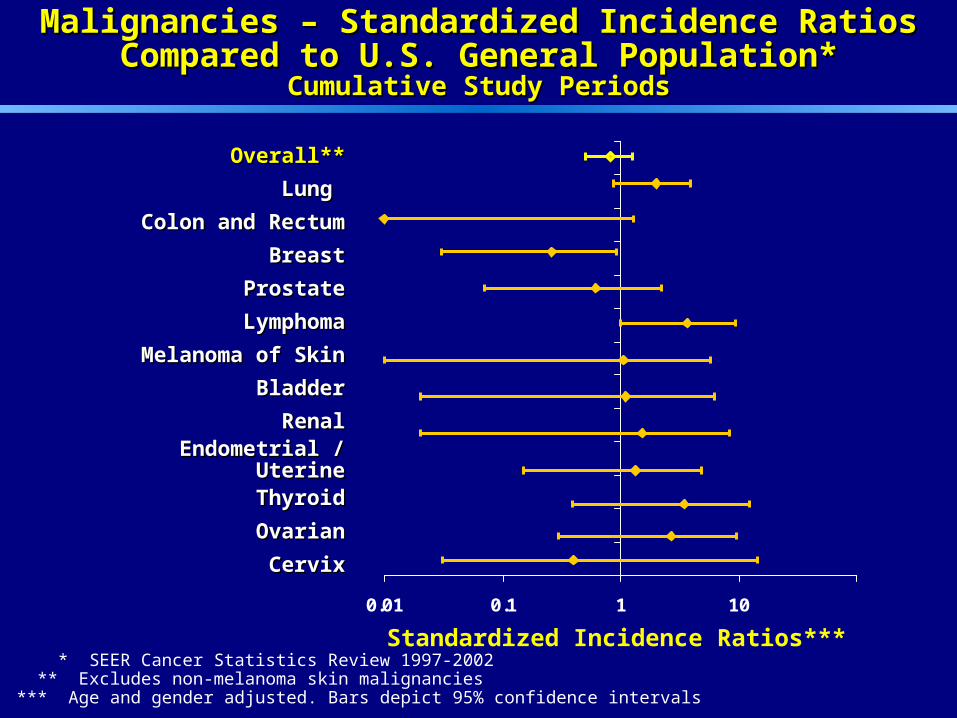
Malignancies – Standardized Incidence RatiosMalignancies – Standardized Incidence RatiosCompared to U.S. General Population*Compared to U.S. General Population*
Cumulative Study PeriodsCumulative Study Periods
Standardized Incidence Ratios***
Overall**Overall**
Lung Lung
Colon and RectumColon and Rectum
BreastBreast
ProstateProstate
LymphomaLymphoma
Melanoma of SkinMelanoma of Skin
BladderBladder
RenalRenal
Endometrial / UterineEndometrial / Uterine
ThyroidThyroid
OvarianOvarian
CervixCervix
* SEER Cancer Statistics Review 1997-2002 ** Excludes non-melanoma skin malignancies*** Age and gender adjusted. Bars depict 95% confidence intervals
86
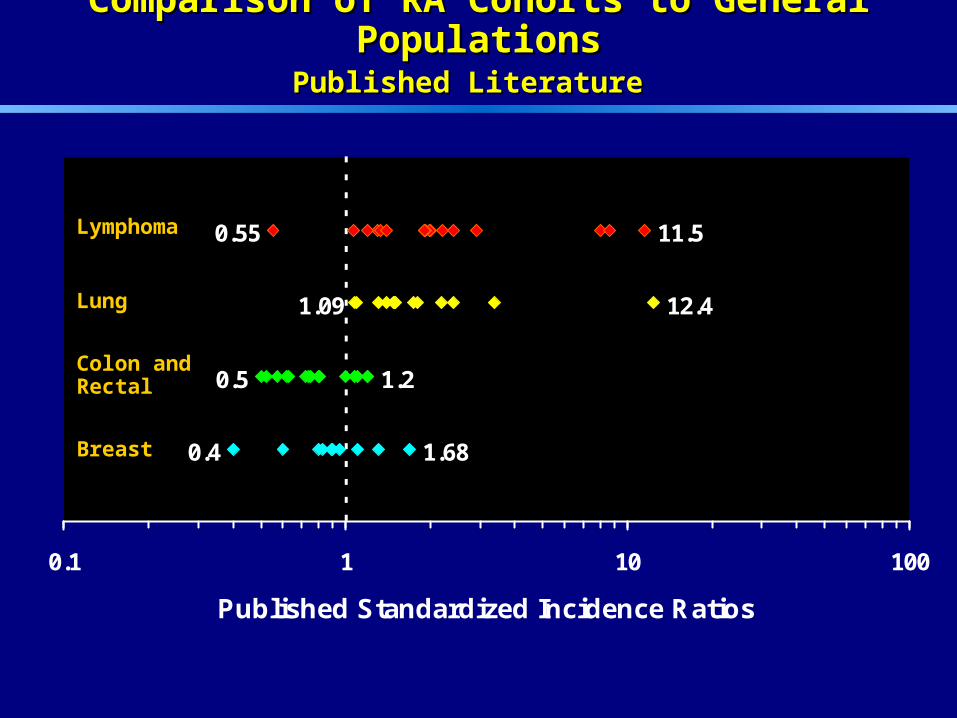
Comparison of RA Cohorts to General PopulationsComparison of RA Cohorts to General PopulationsPublished LiteraturePublished Literature
11.50.55
1.09 12.4
0.5 1.2
0.4 1.68
0.1 1 10 100
Published Standardized Incidence Ratios
LymphomaLymphoma
LungLung
Colon and Colon and RectalRectal
BreastBreast

87
RA Cohorts – DMARD SpecificRA Cohorts – DMARD Specific
Patients treated with DMARDS in the following Patients treated with DMARDS in the following RA cohortsRA cohorts
– British Columbia RA Registry (Canada)British Columbia RA Registry (Canada)
– National Data Bank for Rheumatic Diseases National Data Bank for Rheumatic Diseases (U.S.)(U.S.)
– Norfolk Arthritis Registry (U.K.)Norfolk Arthritis Registry (U.K.)

88
0 1 2 3 4 5 6 7 8 9 10
Lymphoma – Abatacept Observed and Expected Cumulative Study Periods and Observational Cohorts
Expected events are age-adjusted (10-year age groups) and gender-adjusted and account for exposure. Confidence intervals are based on exponential survival function.
Number of Events
4M
Expected
Observed
US General
BC
NOAR
NDB

89
0 2 4 6 8 10 12 14 16 18 20
Lung Cancer – Abatacept Observed and ExpectedCumulative Study Periods and RA Observational Cohorts
4M
Number of Events
Expected events are age-adjusted (10-year age groups) and gender-adjusted and account for exposure. Confidence intervals are based on exponential survival function.
Expected
Observed
US General
BC
NOAR
NDB
90
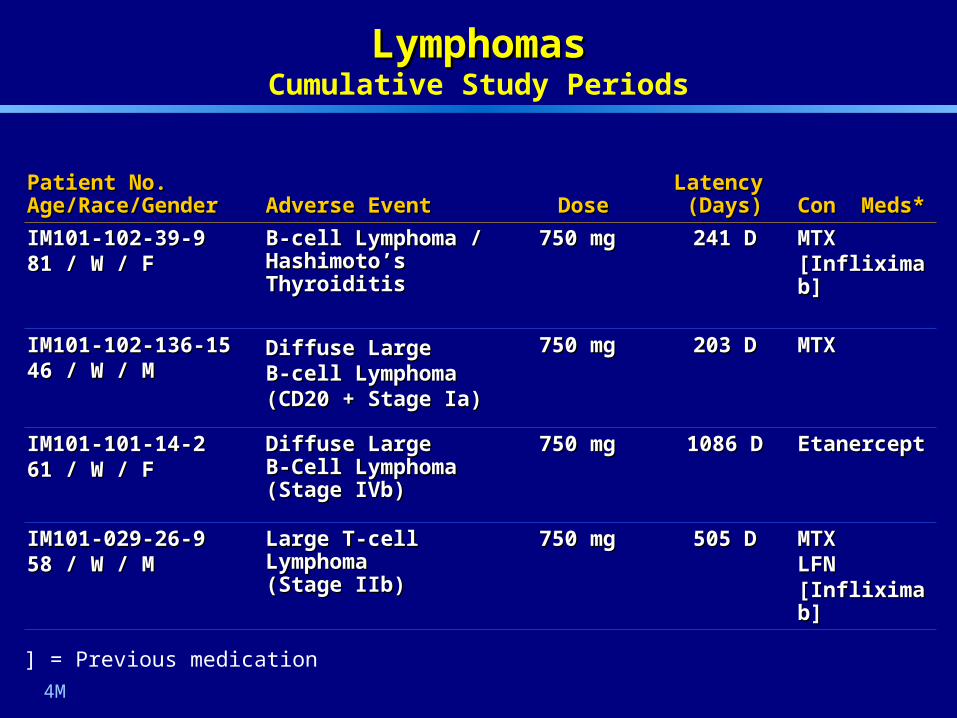
Patient No.Patient No.Age/Race/GenderAge/Race/Gender Adverse EventAdverse Event DoseDose
Latency Latency (Days)(Days) Con Meds*Con Meds*
IM101-102-39-9IM101-102-39-981 / W / F81 / W / F
B-cell Lymphoma / B-cell Lymphoma / Hashimoto’s ThyroiditisHashimoto’s Thyroiditis
750 mg750 mg 241 D241 D MTXMTX[Infliximab][Infliximab]
IM101-102-136-15IM101-102-136-1546 / W / M46 / W / M
Diffuse Large Diffuse Large B-cell Lymphoma B-cell Lymphoma (CD20 + Stage Ia)(CD20 + Stage Ia)
750 mg750 mg 203 D203 D MTXMTX
IM101-101-14-2IM101-101-14-261 / W / F61 / W / F
Diffuse Large Diffuse Large B-Cell Lymphoma B-Cell Lymphoma (Stage IVb)(Stage IVb)
750 mg750 mg 1086 D1086 D EtanerceptEtanercept
IM101-029-26-9IM101-029-26-958 / W / M58 / W / M
Large T-cell Lymphoma Large T-cell Lymphoma (Stage IIb)(Stage IIb)
750 mg750 mg 505 D505 D MTXMTXLFNLFN[Infliximab][Infliximab]
LymphomasLymphomasCumulative Study Periods
4M
*[ ] = Previous medication
91
Lung CancerLung Cancer
Typical clinical presentationTypical clinical presentation
– Older patients (all over 60 years of age)Older patients (all over 60 years of age)
– Highly associated with smoking (7/8)Highly associated with smoking (7/8)
– No predominant tumor typeNo predominant tumor type
Short latency in two cases (29 and 100 days of Short latency in two cases (29 and 100 days of treatment) making causal relationship to therapy treatment) making causal relationship to therapy unlikelyunlikely
Pre-existing radiographic abnormalities indicative Pre-existing radiographic abnormalities indicative of malignancy identified in two other casesof malignancy identified in two other cases

92
Lung Cancer Incidence Rates by Time IntervalsLung Cancer Incidence Rates by Time IntervalsCumulative Study Periods – Through 4 Month UpdateCumulative Study Periods – Through 4 Month Update
* n/p-y = Number of patients / person-years** IR/100 p-y = Incidence rates per 100 person-years
Time Intervals (Months)Time Intervals (Months)
0-6 0-6 6-126-12 12-1812-18 18-2418-24 24-30 24-30 >30 >30
n/p-y*n/p-y* 2/12852/1285 2/10322/1032 4/7954/795 0/3990/399 0/1170/117 0/1980/198
IR/100 p-y**IR/100 p-y** 0.16 0.16 0.19 0.19 0.500.50 0 0 00 0 0
(95% CI)(95% CI) (0.02, 0.56)(0.02, 0.56) (0.02, 0.70)(0.02, 0.70) (0.14, 1.29)(0.14, 1.29) (0, 0.92)(0, 0.92) (0, 3.15)(0, 3.15) (0, 1.86)(0, 1.86)
4M

93
Malignancies – AbataceptMalignancies – AbataceptCumulative Study PeriodsCumulative Study Periods
Non-melanoma SkinNon-melanoma Skin 24 (0.63)24 (0.63) 33 (0.70)33 (0.70)
SolidSolid 21 (0.55)21 (0.55) 28 (0.59)28 (0.59)
Lung Lung 8 (0.21)8 (0.21) 11 (0.23)11 (0.23)
ThyroidThyroid 2 (0.05)2 (0.05) 2 (0.04)2 (0.04)
BreastBreast 2 (0.05)2 (0.05) 4 (0.08)4 (0.08)
ProstateProstate 2 (0.05)2 (0.05) 3 (0.06)3 (0.06)
BladderBladder 1 (0.03)1 (0.03) 1 (0.02)1 (0.02)
RenalRenal 1 (0.03)1 (0.03) 1 (0.02)1 (0.02)
OvarianOvarian 2 (0.05)2 (0.05) 2 (0.04)2 (0.04)
MelanomaMelanoma 1 (0.03)1 (0.03) 1 (0.02)1 (0.02)
Endometrial / UterineEndometrial / Uterine 2 (0.05)2 (0.05) 2 (0.04)2 (0.04)
CervixCervix 1 (0.03)1 (0.03) 1 (0.02)1 (0.02)
GastricGastric 00 1 (0.02)1 (0.02)
HematologicHematologic 5 (0.13)5 (0.13) 6 (0.13)6 (0.13)
LymphomaLymphoma 4 (0.10)4 (0.10) 4 (0.08)4 (0.08)
Myelodysplastic SyndromeMyelodysplastic Syndrome 1 (0.03)1 (0.03) 2 (0.04)2 (0.04)
Type of MalignancyType of Malignancy
Through Jun 2005Through Jun 2005N = 2688 (p-y = 4764)N = 2688 (p-y = 4764)
n (per 100 p-y)n (per 100 p-y)
MAA
Through 4 Month UpdateThrough 4 Month UpdateN = 2688 (p-y = 3827)N = 2688 (p-y = 3827)
n (per 100 p-y)n (per 100 p-y)
94
Malignancy AssessmentMalignancy Assessment
Frequency similar to placebo and US general Frequency similar to placebo and US general population overall and for major categories (skin, population overall and for major categories (skin, solid, hematologic)solid, hematologic)
For malignancies of special interest – lymphoma For malignancies of special interest – lymphoma and lung cancerand lung cancer
– Incidence greater than US general population, Incidence greater than US general population, but within reported ranges for RA patientsbut within reported ranges for RA patients
– Totality of evidence, including clinical Totality of evidence, including clinical presentation and incidence over time, does not presentation and incidence over time, does not suggest increased risk with abataceptsuggest increased risk with abatacept
Virally associated malignancies uncommonVirally associated malignancies uncommon

95
Malignancy AssessmentMalignancy Assessment
Overall, data does not indicate increased risk of Overall, data does not indicate increased risk of malignancy with abataceptmalignancy with abatacept
Assessment not definitive based on number of Assessment not definitive based on number of patients and duration of follow-uppatients and duration of follow-up
Pharmacovigilance program will provide further Pharmacovigilance program will provide further information to better define risk of malignancyinformation to better define risk of malignancy
96
Pharmacovigilance PlanPharmacovigilance Plan
Enhanced data collection for Clinical and Enhanced data collection for Clinical and Spontaneous reportsSpontaneous reports
– Special event formsSpecial event forms
– Telephone contactTelephone contact
Long-term clinical study extensions up to 5 yearsLong-term clinical study extensions up to 5 years
Pregnancy RegistryPregnancy Registry
Large observational safety studiesLarge observational safety studies
97
Pharmacovigilance Plan Pharmacovigilance Plan Large Observational Safety StudiesLarge Observational Safety Studies
Purpose: Complementary assessment of abatacept use Purpose: Complementary assessment of abatacept use and its safety in the post-marketing period and its safety in the post-marketing period
Assess risks of targeted adverse events (malignancy Assess risks of targeted adverse events (malignancy and infection) in clinical practiceand infection) in clinical practice
– Estimate incidence rates overall and in subgroupsEstimate incidence rates overall and in subgroups
– Compare incidence rates with abatacept to other Compare incidence rates with abatacept to other treatmentstreatments
Monitor patterns of useMonitor patterns of use
Investigate potential signals of unanticipated adverse Investigate potential signals of unanticipated adverse eventsevents

98
Large Observational Studies:Large Observational Studies:Insurance Claims CohortInsurance Claims Cohort
Describe short-term incidence of targeted Describe short-term incidence of targeted adverse events adverse events
Confirmation through chart reviewConfirmation through chart review
Data source: UnitedHealthcareData source: UnitedHealthcare
– 2% of US prescriptions2% of US prescriptions
– Open cohort, 5 years cohort identificationOpen cohort, 5 years cohort identification
– Last enrolled patient will be followed forLast enrolled patient will be followed for2 years2 years
– Anticipate 1,200 new starts of abatacept Anticipate 1,200 new starts of abatacept patients within three years, matched to patients within three years, matched to patients on comparator drugspatients on comparator drugs

99
Large Observational Studies:Large Observational Studies:Prospective Cohort (Registry)Prospective Cohort (Registry)
Short-term and long-term incidence of adverse Short-term and long-term incidence of adverse eventsevents
Data source: Existing independent registryData source: Existing independent registry
– Enrollment through physiciansEnrollment through physicians
– 5,000 patients initiating abatacept5,000 patients initiating abatacept
– 15,000 patients initiating comparator treatments15,000 patients initiating comparator treatments
– Follow-up 5 years after last patient enrolledFollow-up 5 years after last patient enrolled
Benefit measured through HAQ and pain scoreBenefit measured through HAQ and pain score
100
Overall Safety SummaryOverall Safety Summary
Clinical development program demonstrates that Clinical development program demonstrates that abatacept is generally safe and well-toleratedabatacept is generally safe and well-tolerated
Major identified risk is infectionMajor identified risk is infection
– Frequency slightly increased (1% difference in Frequency slightly increased (1% difference in serious infection rate) but type, duration, serious infection rate) but type, duration, treatment, and outcome similar to placebotreatment, and outcome similar to placebo
Malignancy risk similar to placebo overall and for Malignancy risk similar to placebo overall and for major categories of malignancy (solid, major categories of malignancy (solid, hematologic) but current assessment is not hematologic) but current assessment is not definitivedefinitive
Pharmacovigilance plan includes 2 large Pharmacovigilance plan includes 2 large observational studies to better define risk of rare observational studies to better define risk of rare events, including lymphoma, other malignancies, events, including lymphoma, other malignancies, and serious infectionsand serious infections

101
AbataceptAbataceptSummarySummary
Brian Daniels, M.D.Brian Daniels, M.D.Senior Vice-PresidentSenior Vice-President
Global Clinical DevelopmentGlobal Clinical DevelopmentBristol-Myers SquibbBristol-Myers Squibb
102
ConsultantsConsultants
Roger B. Cohen, M.D.Roger B. Cohen, M.D.Director, Phase I Program & Director, Phase I Program & Member, Thoracic Oncology Team,Member, Thoracic Oncology Team,Fox Chase Cancer Center, Fox Chase Cancer Center, Philadelphia, PAPhiladelphia, PA
Mark Genovese, M.D.Mark Genovese, M.D.Associate Professor of Medicine, Associate Professor of Medicine, Associate Division Chief, Division of Associate Division Chief, Division of Immunology and Rheumatology, Immunology and Rheumatology, Stanford University School of Medicine, Stanford University School of Medicine, Palo Alto, CAPalo Alto, CA
Princy Kumar, M.D.Princy Kumar, M.D.Professor of Medicine and Microbiology, Professor of Medicine and Microbiology, Chief, Division of Infectious Disease, Chief, Division of Infectious Disease, Associate Dean of Students, Georgetown Associate Dean of Students, Georgetown University School of Medicine, University School of Medicine, Washington, DCWashington, DC
Harry K. Genant, M.D.Harry K. Genant, M.D.Professor Emeritus, Professor Emeritus, University of California, San Francisco University of California, San Francisco Board Member, SYNARC, Inc.Board Member, SYNARC, Inc.San Francisco, CASan Francisco, CA
Marc Hochberg, M.D., M.P.H.Marc Hochberg, M.D., M.P.H.Professor of MedicineProfessor of MedicineHead, Division of Rheumatology and Head, Division of Rheumatology and Clinical Immunology, Clinical Immunology, University of Maryland, Baltimore, MDUniversity of Maryland, Baltimore, MD
Désirée van der Heijde, M.D.Désirée van der Heijde, M.D.Professor of Rheumatology, Professor of Rheumatology, University Hospital, University Hospital, Maastricht, the NetherlandsMaastricht, the Netherlands