Embed Size (px)
Citation preview
Kaiser Permanente Georgia 1
u Formulary Additions . . . . . . . . . . . . . . 1
I S S U E 6 V O L U M E 14 D E C E M B E R
Formulary Update
A P U B L I C AT I O N O F T H E G E O R G I A P H A R M A C Y A N D T H E R A P E U T I C S ( P & T ) C O M M I T T E E . The Formulary Update contains information regarding formulary additions, deletions, exclusions, brief descriptions of products, and current drug related news. It also lists items to be discussed at upcoming P&T meetings. Please refer to the web site http://kpnet.kp.org:81/ga/healthcare/formularies.html or http://providers.kaiserpermanente.org/ for the full KP GA Drug Formulary.
At A Glance
u Additions/Updates to QRM . . . . . . . . 2 u Other Formulary Changes. . . . . . . . . 3
� National Medicare Part D Formulary . . . . . . . . . . . . . . . . . . . . 4 - 5
Formulary RemovalsThe following medications will be removed from the Commercial Formulary:• Removal effective 01.06.2021
o Meperidine oral formulationso Migranal (dihydroergotamine) nasal spray
• Removal effective 03.31.2021o Testosterone 1% Gel Pump
Upcoming Formulary Items
An important aspect of the formulary process is the involvement of all practitioners. Please contact your P&T Committee representative or your clinical service chief by January 26, if you wish to comment on any of the medications, class reviews, or other agenda items under consideration. To make formulary addition requests, you must submit a Formulary Additions/Deletions Form and Conflict of Interest Form to Drug Information Services or call (404) 949-5331
Interregional Practice RecommendationsThe Emerging Therapeutics Strategy Program (ETSP) is a centralized effort that applies our evidence-based model to develop interregional practice recommendations with KP physician specialists, coordinates KP HealthConnect clinical content for decision support, and monitors outcomes to measure uptake of the clinical and strategy recommendations. Through the collaboration of Pharmacy, Permanente physicians, and Federation partners, the ETSP offers a unified approach in the provision and management of specialty drugs, to help ensure that our members derive the greatest value from these products.
The following IR Practice Recommendation additions/updates have been recently approved:
• Additions:o Dojolvi (triheptanoin): Indicated as a source of calories and fatty acids for the treatment of molecularly
confirmed long-chain fatty acid oxidation disorders in adults and pediatric patients.o Tecartus (brexucabtagene autoleucel): Indicated for the treatment of relapsed or refractory mantle cell
lymphoma (MCL) in adults.• Updates:
o Palynziq (pegvaliase): Changes to maximum recommended dose, baseline labs, monitoring recommendations, and criteria for discontinuation.
o Exon skipping therapies (eteplirsen, golodirsen, and viltepso): Changes included the addition of viltepso to recommendations and revision to exclusion criteria.
ETSP Guidelines as well as pipeline candidates can be found here: https://secure.sp.kp.org/teams/emergingtsc/SitePages/Home.aspx. Please note: Newly marketed medications requiring ETSP review will also receive prior authorization (PA) review. These medications will not be eligible for consideration of drug benefit coverage until completion of drug specific ETSP and PA criteria review processes.
Additions to QRM (Prior Authorization)Effective 01.06.21:
• Darzalex Faspro (daratumumab and hyaluronidase-fihj): Indicated for the following:
o Treatment of newly diagnosed multiple myeloma (in combination with bortezomib, melphalan, and prednisone OR in combination with lenalidomide and dexamethasone) in adults who are ineligible for autologous stem cell transplant.
o Treatment of relapsed or refractory multiple myeloma (in combination with lenalidomide and dexamethasone OR in combination with bortezomib and dexamethasone) in adults who have received at least 1 prior therapy.
o Treatment of relapsed or refractory multiple myeloma (as monotherapy) in adults who have received at least 3 prior lines of therapy, which included a proteasome inhibitor and an immunomodulatory agent, or who are double refractory to a proteasome inhibitor and an immunomodulatory agent.
• Mycapssa (octreotide acetate): Indicated for the long-term maintenance treatment of acromegaly in patients who have responded to and tolerated treatment with octreotide or lanreotide.
• Nurtec ODT (rimegepant): Indicated for the acute treatment of migraine with or without aura in adults.
• Oriahnn (elagolix, estadiol, and norethindrone acetate; elagolix): Indicated for the management of heavy menstrual bleeding associated with uterine leiomyomas (fibroids) in premenopausal women.
• Reyvow (lasmiditan): Indicated for the acute treatment of migraine with or without aura in adults.
• Ubrelvy (uprogepant): Indicated for the treatment of migraine with or without aura in adults.
• Uplizna (inebiluzumab - cdon): Indicated for the treatment of neuromyelitis optica spectrum disorder (NMOSD) in adults who are anti-aquaporin-4 (AQP4) antibody positive.
Effective 03.31.21:
• Mytesi (crofelemer): Indicated for the symptomatic relief of noninfectious diarrhea in patients with HIV/AIDS on antiretroviral therapy.
• Opsumit (macitentan): Indicated for the treatment of pulmonary arterial hypertension (PAH) (WHO Group I) to reduce risks of disease progression and hospitalization.
• Prevymis (letermovir): Indicated for the prophylaxis of cytomegalovirus (CMV) infection and disease in adult CMV-seropositive recipients [R+] of an allogeneic hematopoietic stem cell transplant (HSCT).
• Relistor (methylnaltrexone): Indicated for the treatment of opioid-induced constipation in adults with chronic non-cancer pain, including patients with chronic pain related to prior cancer or its treatment who do not require frequent (e.g. weekly) opioid dosage escalation/opioid-induced constipation in adults with advanced illness or pain caused by active cancer who require opioid dosage escalation for palliative care.
Kaiser Permanente Georgia 2
QRM Criteria Updates• Cimzia (certolizumab): Addition of criteria for use in treating plaque psoriasis.
• Evenity (romozozumab): Criteria updated to include diagnosis of osteopenia.
• Parathyroid hormone analogs - Tymlos (abaloparatide) and Forteo (teriparatide): Note added to allow use in severe osteoporosis without a previous trial of preferred bisphosphonate therapies.
• Subcutaneous Immune Globulin products: Updates allow use without a trial of intravenous immune globulin products.
• Ruconest (C1 inhibitor - recombinant): Criteria changed to allow use in pregnancy without a trial of Berinert.
• Xgeva (denosumab): Criteria updated to allow use for additional FDA approved indications.
• Gonadotropin Releasing Hormone Agonists - Supprelin LA (histrelin): Revisions include addition of Vantas as the preferred GnRH agonist and criteria to allow use in transgender youth for gender dysphoria.
Kaiser Permanente Georgia 3
Questions and Conce rns?
If you have any questions or concerns, please contact any of
the following P&T Committee members and designated alternates:
P&T Chair:
Carole Gardner, MD
P&T Committee Members:
Debbi Baker, PharmD, BCPSClinical Pharmacy
Gary Beals, RPhExecutive Director, Pharmacy
Karen Bolden, RN, BSNClinical Services
Hector Clarke, PharmD, BCOP Ambulatory Pharmacy
Alyssa Dayton, MDObstetrics and Gynecology
Pierson Gladney, MD Hematology/Oncology
Patrick Hall, MDAdult Primary Care
Craig Kaplan, MDAdult Primary Care
Amy Levine, MDPediatrics
Sophie Lukashok, MDInfectious Disease
Felecia Martin, PharmDPharmacy/Geriatrics
Shayne Mixon, PharmDPharmacy Operations
Jay Polokoff, MDPediatrics
Rachel Robins, MDHospitalist
Jennifer Rodriguez, MDBehavioral Health
Designated Alternates:Jacqueline Anglade, MD Obstetrics and Gynecology
Lesia Jackson, RNClinical Services
Satya Jayanthi, MDHospitalist
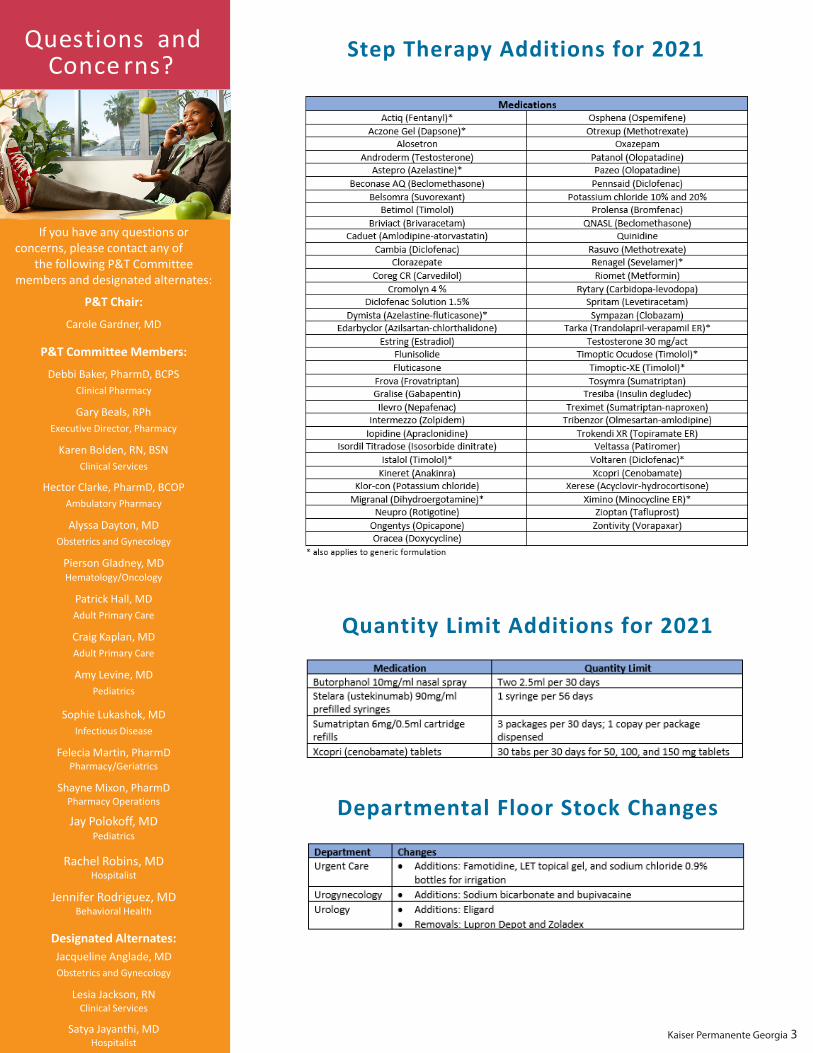
Q uantity Limit Additions for 2021
Step Therapy Additions for 2021
Departmental Floor Stock Changes
Kaiser Permanente Georgia 4
Cl ass Review
February 2021:
Medication Class Reviews Antianginal
AntiarrhythmicsAntihistamines
AntihyperlipidemicsAntihypertensives
Beta Blockers
Calcium Channel Blockers
Cardiovascular Agents -- MiscCough/Cold/Allergy
Diuretics
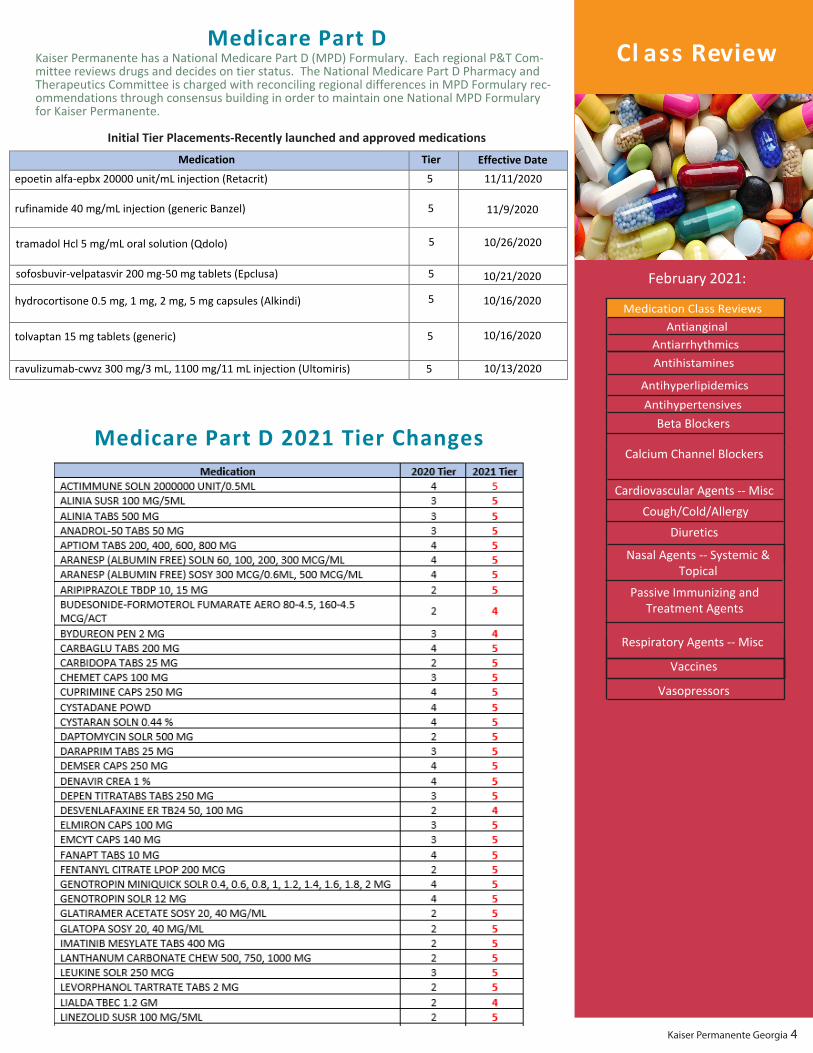
Medicare Part DKaiser Permanente has a National Medicare Part D (MPD) Formulary. Each regional P&T Com-mittee reviews drugs and decides on tier status. The National Medicare Part D Pharmacy and Therapeutics Committee is charged with reconciling regional differences in MPD Formulary rec-ommendations through consensus building in order to maintain one National MPD Formulary for Kaiser Permanente.
Initial Tier Placements-Recently launched and approved medications
Medication Tier Effective Date
epoetin alfa-epbx 20000 unit/mL injection (Retacrit) 5 11/11/2020
rufinamide 40 mg/mL injection (generic Banzel) 11/9/2020
tramadol Hcl 5 mg/mL oral solution (Qdolo) 5 10/26/2020
sofosbuvir-velpatasvir 200 mg-50 mg tablets (Epclusa) 5 10/21/2020
hydrocortisone 0.5 mg, 1 mg, 2 mg, 5 mg capsules (Alkindi) 5 10/16/2020
tolvaptan 15 mg tablets (generic) 5 10/16/2020
ravulizumab-cwvz 300 mg/3 mL, 1100 mg/11 mL injection (Ultomiris) 5 10/13/2020
Nasal Agents -- Systemic & Topical
Vaccines
Respiratory Agents -- Misc
Passive Immunizing and Treatment Agents
5
Vasopressors
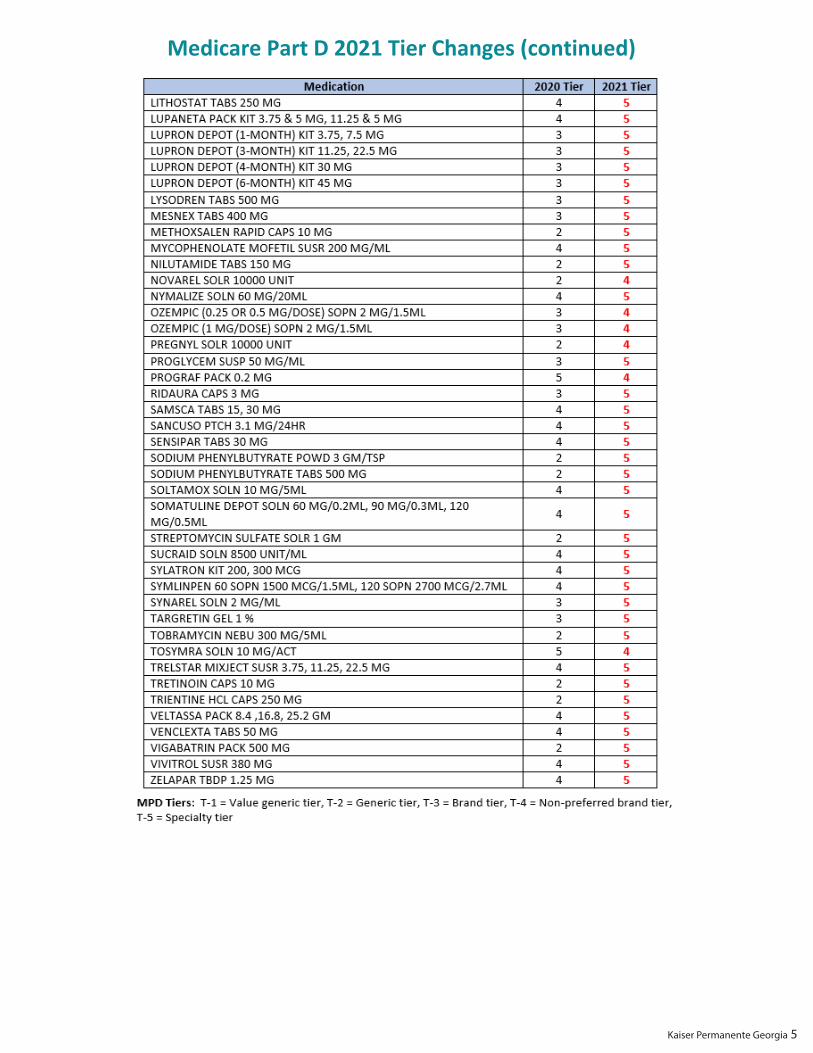
Medicare Part D 2021 Tier Changes
Kaiser Permanente Georgia 5
Medicare Part D 2021 Tier Changes (continued)





























