Embed Size (px)
Citation preview

111/4/2015
UCSB Human Resources, Benefits
This presentation is intended for communication purposes only. Please see the UCnet website (http://ucnet.universityofcalifornia.edu) and plan documents for complete information.
Medical Plan Comparison

2
Resources• Open Enrollment Website
http://ucnet.universityofcalifornia.edu/oe
• Insurance Plan Websites ◊ Plan booklets◊ Provider directories
• Benefits Education Videos https://uc.a.guidespark.com/ ◊ Medical Terms and Concepts◊ Medical Plan Comparisons

3
Topics
• What is your priority?• Preventive care• Residence requirements• Choice of physician• Cost of care & prescription drugs• Out of Pocket Maximum• Health Savings Account• Behavioral Health• Chiropractic and Acupuncture

2016 Medical Plans
HMO
Health Net Blue & Gold
Kaiser
PPO
UC Care
Blue Shield Health Savings Plan
Core

5
What is your priority?
• Cost to enroll – monthly premium
• Cost of care ◊ Predictable, low cost copays◊ Pay a % of each service
• Choice of providers◊ HMO medical group physicians◊ PPO preferred network or any provider
• Effort to manage – coordinating care &
bills

6
Preventive Care
• All medical plans cover preventive care at 100% with in-network providers
• Preventive care includes:◊ Annual well visit and labs◊ Well woman visits and labs◊ Preventive screening tests◊ Immunizations
• See list of preventive services on the plan websites

7
Residence LimitationsHMO (Health Net, Kaiser)
• Employee must live in California
• PCP must be within 30 miles of where you live or work (in most cases)
Blue Shield Health Savings• Employee must live in US
• Employee may live anywhere
• Worldwide services
CORE
UC Care
• Employee may live anywhere
• Worldwide services
• Employee may live anywhere
• Worldwide services

8
When traveling out of USHMO (Health Net, Kaiser)
• Limited to emergency and urgent care only
• No routine care when away from medical group
Blue Shield Health Savings• Limited to emergency and urgent care only
• No routine care
• Comprehensive coverage
• Plan pays Preferred/Tier 2 benefit.
CORE
UC Care
• Comprehensive coverage
• Plan pays out-of-network benefit.

9
Choice of PhysicianHMO (Health Net,
Kaiser)• You choose PCP• PCP coordinates care• PCP refers to specialists• Specialists limited to
physicians in medical group
Blue Shield Health Saving
Out-of-Network• Non-Blue Shield
CORE
UC Care
In-Network• Blue Shield PPO
Out-of-Network• Non-Blue Shield
You choose
In-Network • UC Select• Blue Shield Preferred
PPO
You choose
In-Network • Blue Shield PPO
Out-of-Network• Non-Blue Shield
You choose

10
UC Care Networks/Tiers
UC Select(Tier 1)
UC Medical Centers
&Select
Blue Shield PPO
Blue ShieldPreferred
(Tier 2)
In CABlue Shield PPO
Out of CABlue Cross Blue
Shield
Out of USAny provider
Non-PreferredOut-of-Network
(Tier 3)
Out of the UC Select
or Blue Shield Preferred
In Network Providers

11
UC Care – Santa Barbara Network
Providers Status
Sansum Clinic UC Select/Tier 1
Quest Diagnostic LabUnilab
UC Select/Tier 1
Cottage Hospitals UC Select/Tier 1
Pacific Diagnostic Lab UC Select/Tier 1
Pueblo Radiology UC Select/Tier 1
Santa Barbara Preferred Health Partners
Some physicians are in Blue Shield Preferred/Tier 2
NEW in
2016

12
UC Care - UC Select near UCSB
• UC Select/Tier 1 providers in◊ Santa Barbara ◊ Santa Maria◊ Lompoc◊ Ventura
• UC Care Provider Directoryblueshieldca.com/uccareppo
Blue Shield Concierge 1-855-702-0477

13
Find a UC Care Provider

14
Plan Costs• HMOs have predictable copays for services
• PPOs have deductibles and % coinsurance
◊ Deductible is the amount you pay each year before the plan starts sharing the cost with you
◊ Coinsurance is your share of the cost after you pay the deductible
◊ Your costs are based on the network that the provider is in and the service you receive
◊ You pay discounted rates for “in-network” providers
◊ You pay more for “out-of-network” providers

15
PPO Allowed Amount – In Network
In-Network Example
Discounted rate that plan negotiates for each service with “preferred” or participating providers
• You pay the in-network coinsurance on the discounted rate.
• Provider can’t “balance bill”
20% Coinsurance
Provider charge: $200Allowed amount: $100
Plan pays 80%: $80
You pay 20% $20
Provider write-off:$100
PPO plans negotiate “allowed” rates to process claims.

16
PPO Allowed Amount – Out of Network
Out-of-Network Example
Value that plan assigns to a service when provider is NOT a “preferred provider” (not participating)
• Plan pays out-of-network coinsurance on the allowed amount.
• Provider can “balance bill”
50% Coinsurance
Provider charge: $200Allowed amount: $100
Plan pays 50%: $50(50% of $100)
You pay 50%: $50
You pay balance: $100
PPO plans assign “allowed” rates to process claims.

17
Office Visit Cost
Medical Plan Copay
Deductible Coinsurance
HMO $20 None None
UC Care PPOUC Select/Tier
1$20 None None
Preferred/Tier 2
$250 indiv $750 family
You pay 20%
Out-of-Network
$500 indiv$1,500 family
Plan pays 50% of allowed rate
You pay balance

18
Deductible: Individual vs Family
$250 Individual / $750 Family
Coinsurance
Adult 1 Paid $250 20%Adult 2 Paid $100
Child 1 Paid $ 75
Child 2 Paid $250 20%
Adult 2 Paid $175 20%
20%
UC Care ExampleFamily Deductible
Blue Shield Preferred (Tier 2)

Office Visit Costs
19
Blue Shield HSP
In-network$1,300 single$2,600 family
You pay 20%
Out-of-Network
$2,500 single$5,000 family
Plan pays 60% of allowed rate
Full family deductible must be met before plan shares cost
COREIn-network
$3000 per individual
You pay 20%
Out-of-Network
Plan pays 80% of allowed rate
Medical Plan Copay
Deductible Coinsurance

20
How does each plan work?
Scenario
• Office visit to a general practitioner who recommends you see a dermatologist
• Office visit to dermatologist who conducts a biopsy in the office to remove a lesion.
1. How do you access these providers?2. What will you pay for these services?

21
Hospital Costs
Medical Plan Copay
Deductible Coinsurance
HMO $250 None None
UC Care PPOUC Select/Tier
1$250 None None
Preferred/Tier 2
$250 indiv $750 family
You pay 20%
Out-of-Network
$500 indiv$1,500 family
Plan pays 50% of allowed rate
You pay balance

Hospital Costs
22
Blue Shield HSP
In-network$1,300 single$2,600 family*
You pay 20%
Out-of-Network
$2,500 single$5,000 family*
Plan pays 60% of allowed rate
*Full family deductible must be met before plan shares cost
COREIn-network
$3000 per individual
You pay 20%
Out-of-Network
Plan pays 80% of allowed rate
Medical Plan Copay
Deductible Coinsurance

23
Outpatient Surgery Center Costs
Medical Plan Copay
Deductible Coinsurance
HMO $100 None None
UC Care PPOUC Select/Tier
1 $100None
None
Preferred/Tier 2
$250 indiv $750 family
You pay 20%
Out-of-Network
$500 indiv$1,500 family
Plan pays 50% of allowed rate
You pay balance

Outpatient Surgery Center Costs
24
Blue Shield HSP
In-network$1,300 single$2,600 family*
You pay 20%
Out-of-Network
$2,500 single$5,000 family*
Plan pays 60% of allowed rate
*Full family deductible must be met before plan shares cost
COREIn-network
$3000 per individual
You pay 20%
Out-of-Network
Plan pays 80% of allowed rate
Medical Plan Copay
Deductible Coinsurance

25
How does each plan work?
Scenario
• Surgery for orthopedic problem(medical facility, surgeon, anesthesiologist)
• Follow-up physical therapy
1. How do you access these providers?2. What will you pay for these services?

26
Emergency Room Costs
Medical Plan Copay
Deductible Coinsurance
HMO $75 None None
UC Care PPOUC Select/Tier
1 $200None
None
Preferred/Tier 2 $200 Waived None
Out-of-Network $200 Waived None

Emergency Room Costs
27
Blue Shield HSP
In-network$1,300 single$2,600 family*
You pay 20%
Out-of-Network
$2,500 single$5,000 family*
You pay 20%
*Full family deductible must be met before plan shares cost
COREIn-network
Waived for facility fee
You pay 20%
Out-of-Network
You pay 20%
Medical Plan Copay Deductible Coinsurance

28
Out-of-Pocket Maximum
• The most the insurance plan requires you to pay in a calendar year
• Once you have paid this amount, the insurance plan pays 100% of future expenses.
• Includes deductible, copay, coinsurance for medical services, behavioral health and prescription drugs
• Does not include amounts “not allowed” by insurance plan when using out-of-network providers.

29
Out-of-Pocket Maximum
Medical Plan OOPM
Medical & Rx
Notes
Health Net HMO $1,000 indiv$3,000 family
Family = 3 or more
Kaiser HMO $1,500 indiv$3,000 family
Family = 2 or more

30
Out-of-Pocket Maximum
Medical Plan OOPM Medical
Notes
UC Care PPOUC Select/Tier
1$1,500 indiv
$4,500 family
Family = 3 or more
Expenses for In-Network providers
cross accumulatePreferred/Tier 2
$3,000 indiv
$9,000 family
Out of Network
$5,000 indiv
$15,000 family
Family = 3 or more
Out-of-network accumulates separately

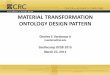
UC Care – OOPM Cross Accumulation
31
UC Select /Tier 1
Copays
Blue Shield Preferred/Tier 2Deductible & Coinsurance$
$
$$$
$1500Stop Paying
UC Select Copays (individual)
$3000Stop paying Blue Shield Preferred Coinsurance(individual)

33
Out-of-Pocket Maximum
Medical Plan OOPM Rx Notes
UC Care PPOIn-network pharmacy
$3,600 indiv
$4,200 family
Family = 3 or more
Medical and Rx do not cross
accumulateOut-of-network
PharmacyNone

34
Out-of-Pocket Maximum
Medical Plan OOPMMedical & Rx
Notes
CORE $6,350 indiv$12,700 family
Family = 2 or more
Blue Shield HSPIn-network $4,000 indiv (single)
$6,400 family
Full family OOPM must be met before plan pays 100% for
any enrollee
Out-of-Network OOPM includes
In-network providers
Out-of-Network $8,000 indiv (single)$16,000 family

35
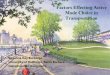
Deductible, Coinsurance, OOPM
You pay You share cost with plan
After you pay OOPM,Plan pays
100%
$1300Deductibl
e20% Coinsurance $4000
OOPM
Blue Shield Health Savings Plan Individual (Single)
In-Network Providers

36
Deductible, Coinsurance, OOPM
You pay You share cost with plan
After you pay OOPM,Plan pays
100%
$2600Deductibl
e20% Coinsurance $6500
OOPM
Blue Shield Health Savings Plan Family
In-Network Providers
The full family deductible must be met before plan shares costs

37
Prescription Drugs
HMOUC Care
Blue Shield HSP CORE
Retail (30 day)• Generic• Brand• Non-formulary
$5$25$40
You pay full cost of medication until you satisfy the deductible
After deductible, you pay 20% at preferred pharmacies
Mail Order (90 day)Selected Retail • Generic• Brand• Non-formulary
$10$50$80
Preferred Drug List (Formulary) is different for each carrier

38
Learn more about PPO costs
Fair Health Consumerhttp://www.fairhealthconsumer.org/
Health Care Blue Bookhttps://www.healthcarebluebook.com/
Good Rx – drug costshttp://www.goodrx.com
Blue Shield Member website• After you enroll, see estimator tools

39
Blue Shield Health Savings Plan
High deductible medical plan paired with a Health Savings Account
Medical CoverageBlue Shield PPO
855-702-0477blueshieldca.com/uc
Health Savings AccountHealthEquity
866-212-4729healthequity.com/ed/uc/
+

STOP Consider HSA Limitations
To own/contribute to Health Savings Account:
• May not be enrolled in Medicare A or B
◊ Did you enroll in Medicare at age 65?
◊ Were you automatically enrolled when you signed up for Social Security pension?
• May not be enrolled in other medical plan
• Must have a $0 balance in Health FSA on December 31, 2015 (complete any claims reimbursement by Dec. 31, 2015)
• May not be claimed as a dependent on someone else’s tax return

41
Health Savings Account
• You keep the money even if you change jobs or insurance plans
• You can make contributions at any time• HSA has triple tax advantage
• No Federal taxes on contributions • No taxes when funds are used• No taxes on earnings
• HSA funds rollover from year to year; no use it or lose it as with Health FSA
• You can invest funds to earn more

HSA can maximize savings
• UC Contribution (plan starting on 1/1/16) ◊ $500 individual ◊ $1000 family
• You can contribute up to (optional):
◊ Single-coverage: $3,350 – $500 = $2,850◊ Family-coverage: $6,750 – $1,000 =
$5,750 ◊ Catch-up contribution, age 55+: $1,000

43
Use the HSA to pay for…
• Deductible• Coinsurance• Any IRS Publication 502 Expenses, including:
◊ Medical◊ Dental◊ Vision◊ Prescription drug◊ Long Term Care insurance premiums
• May pay expenses for tax dependents; don’t have to be enrolled in medical plan

How does HSA work?
• UC makes annual contribution for plans that start on January 1.
• You may contribute through payroll deduction or make post-tax contributions to HealthEquity
• Use a HSA debit card to pay for health expenses
• Use HealthEquity website to pay medical and other health claims
• Invest HSA dollars when account balance reaches $2000 – no fees to invest

45
Optum (formerly United Behavioral Health)
• Optum coordinates behavioral health care for all medical plans (except CORE)◊ psychiatrist◊ psychologist◊ therapist◊ substance abuse treatment
• No referral required from physician• Call Optum to notify prior to first visit

46
Behavioral/Mental Health
Medical Plan
OPTUM Network
Out of Network
Health Net Blue & Gold
Visits 1–3 no copayVisits 4+ $20
$250 inpatient hospitalization
Emergency only
Kaiser
(Optum & Kaiser Providers)
Emergency only

47
Behavioral/Mental HealthMedical Plan
OPTUM Network Out-of-Network
UC Care Visits 1-3 no copayVisits 4+ $20Inpatient $250
$500 deductiblePlan pays 50% allowed
You pay balance
Blue Shield HSP
After deductible:$1,300 indiv $2,600 family
You pay 20%
Deductible:$2,500 indiv$5,000 family
Plan pays 60% allowedYou pay balance

48
Behavioral/Mental Health
Medical Plan
Blue Shield Network
Out of Network
Core $3000 deductible
You pay 20% Plan pays 80% allowedYou pay balance
Note for all plans:• The medical and behavioral health deductibles cross-
accumulate.• The medical and behavioral health coinsurance cross-
accumulate toward a common out-of-pocket maximum.• In-network and out-of-network deductibles and out-of-
pocket maximums do NOT cross accumulate.

49
Chiropractic & AcupunctureMedical Plan Providers Costs
Health Net American Specialty Health
$20 copaySelf-referral24 visits/year combined
Kaiser American Specialty Health
$15 copaySelf-referral24 visits/year combined
Kaiser $20 copay acupuncture only

50
Chiropractic & AcupunctureMedical Plan Providers Costs
UC Care UC Select N/A N/A
Preferred Blue Shield After deductible,You pay 20%
Out-of-Network
Non-Blue Shield After deductible,
Acupuncture:Plan pays 80% allowed
Chiropractic:Plan pays 50% allowed
Note: Benefit is limited to 24 visits per calendar year combined for Acupuncture and Chiropractic visits

51
Chiropractic & AcupunctureMedical Plan Providers Costs
Blue Shield HSP
In-NetworkBlue Shield
After deductible,You pay 20%
Out-of-Network
Non-Blue Shield
After deductible,
Acupuncture:Plan pays 80% of allowed
Chiropractic:Plan pays 60% of allowed
Note: Benefit is limited to 24 visits per calendar year combined for Acupuncture and Chiropractic visits

52
Chiropractic & AcupunctureMedical Plan Provider Out of Network
CoreIn-Network Blue Shield
After deductible,You pay 20%
Out-of-network
Non-Blue Shield
After deductible,
Acupuncture:Plan pays 80% allowed
Chiropractic:Plan pays 80% allowed
Note: Benefit is limited to 24 visits per calendar year combined for Acupuncture and Chiropractic visits

53
TeleHealth Programs• Designed to enhance the care you already
receive from your personal physician:
◊ When you are considering the ER or urgent care for nonemergency medical issues
◊ After normal office hours
◊ When your primary care physician is not available
◊ With pediatric care, if your child’s primary care physician is not available
• Doctors can also diagnose, recommend and prescribe medication for many of your non-emergent medical issues

54
TeleHealth – How it works• 24/7/365 access to consultations anywhere
through online video, phone or secure email
• Staffed by Board Certified Physicians
• Preregistration on plan website is recommended
◊ Health Net – MDLive
◊ UC Care – Teledoc
◊ Blue Shield Health Savings Plan – Teledoc
◊ Core – Teledoc
• See plan benefit summary for copay/coinsurance

55
Learn more about PPO Costs
Fair Health Consumerhttp://www.fairhealthconsumer.org/
Health Care Blue Bookhttps://www.healthcarebluebook.com/
Good Rx• http://www.goodrx.com• Estimate cost of drugs

56
http://ucnet.universityofcalifornia.edu• Resources
◊ Plan contacts◊ Plan rates
• Medical Plans◊ Benefit summaries◊ Links to provider directories◊ Links to plan websites
• Other plans◊ Dental, vision, FSA

57