-
8/3/2019 0c6bSedation and Analgesia in ICU
1/100
Sedation and analgesiain ICUAHMAD F. MADY MD
Lecturer of Anesthesia &ICU,
Tanta university hospitals,Tanta,Egypt
Senior registrar,ICU,KSMC
-
8/3/2019 0c6bSedation and Analgesia in ICU
2/100
Objectives
Algorithm for Sedation TechniqueApplication
Clinical practice guidelines for the sustained use of sedatives
and
analgesics in the critically ill adult
-
8/3/2019 0c6bSedation and Analgesia in ICU
3/100
introduction
In critically ill patients there are three rationales for
adequateanalgesia and sedation (A&S).
Firstly,A&S ensure an optimal level of comfort; the patient
should have no
more than moderate pain and should be calm and alert.
Secondly,
A&S are thought to reduce the stress response that is
relatedto inflammation and trauma.
Thirdly,
A&S facilitate diagnostic and therapeutic procedures, as
well asnursing care.
-
8/3/2019 0c6bSedation and Analgesia in ICU
4/100
Analgesia is the act of blunting pain,through administration of
drugs, but also through positioning ofthe patient, stabilising
fractures and minimising harmful physical
stimulation .
4582% of critically ill patients suffer from pain depending
ontheir degree of activity . They are exposed to numerous
noxiousstimuli
Bernhard Walder, Martin R. TramrSWISS MEDWKLY 2004;134:333346
www.smw. c h
Sedation in critical care is the act of calming,especially
through administration of centrally acting drugs, but
also through reassurance, information and music.
71% of critically ill patients have been shown to suffer
fromanxiety, confusion and agitation
-
8/3/2019 0c6bSedation and Analgesia in ICU
5/100
INDICATIONS FOR A&S
1- Pain, MV. trauma, invasive operations, routine nursing care,
ETTsuctioning, and prolonged immobility.
2- Anxiety & agitation life-threatening illness,
Inadequatelycontrolled pain, sleep deprivation, isolation, and the
presence ofinvasive tubes and catheters are frequently listed as
sources of
stress and anxiety3- Delirium:
4- Facilitate Patient Care
5- Decrease Oxygen Consumption particularly important in
patientssuffering from acute lung injury or shock.
6- Reduction of seizures: Sedation appears to be an attractive
optionin reducing seizures in the NICU
-
8/3/2019 0c6bSedation and Analgesia in ICU
6/100
7-amnesia
Some studies have shown that patients with a greater recallof
adverse experiences may be likely to developposttraumatic stress
disorder (PTSD), leading some tosuggest that deep sedation be
routinely used to bluntpatient awareness of the ICU experience
More recently,investigators have demonstrated thatpatients who
were most awake, or the most unresponsive,
during mechanical ventilation had the lowest
PTSD-likesymptoms.
Weinert CR, Sprenkle M. Post-ICU consequences of patient
wakefulness and sedative
exposure during mechanical ventilation. Intensive Care Med 2008;
34(1):8290.
-
8/3/2019 0c6bSedation and Analgesia in ICU
7/100
8- Weaning from Mechanical Ventilation It is now well known that
patients being weaned from MV require
appropriate sedation for a successful outcome.
Non pharmacologic intervention at the time of weaning may
relievemild anxiety. Such interventions include changing the
environment,
using relaxation techniques, reassuring the patient, and
providingadequate rest and psychological support. However, for
patientswho do not respond to these interventions, pharmacologic
therapyshould be instituted
Cohen IL, Gallagher TJ, Pohlman AS, Dast JF, Abraham E,
Papadakos PJ:Themanagement of the agitated ICU patient. Crit Care
Med 2002; 30: 97125.
-
8/3/2019 0c6bSedation and Analgesia in ICU
8/100
GOALS FOR S&A
To minimise physical discomfort or pain for procedures To
control behaviour, particularly movement
To minimise psychological disturbance & distress To maximise
the potential for amnesia
To guard patient safety
-
8/3/2019 0c6bSedation and Analgesia in ICU
9/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
10/100
Clinical practice guidelines for the sustaineduse of sedatives
and analgesics in the
critically ill adult(1995,2002,2005)
American College of Critical Care Medicine (ACCM)
the Society of Critical Care Medicine (SCCM)
the American Society of Health-System Pharmacists (ASHP)
the American College of Chest Physicians
Judith Jacobi, PharmD, FCCM, BCPS; Gilles L. Fraser, PharmD,
FCCM; Douglas B. Coursin, MD;Richard R. Riker, MD; Dorrie Fontaine,
RN, DNSc, FAAN; Eric T. Wittbrodt, PharmD; Donald B.Chalfin, MD,
MS, FCCM; Michael F. Masica, MD, MPH; H. Scott Bjerke, MD; William
M. Coplin, MD;David W. Crippen, MD, FCCM; Barry D. Fuchs, MD; Ruth
M. Kelleher, RN; Paul E. Marik, MDBCh,FCCM; Stanley A. Nasraway,
Jr, MD, FCCM; Michael J. Murray, MD, PhD, FCCM; William T.
Peruzzi,MD, FCCM; Philip D. Lumb, MB, BS, FCCM
-
8/3/2019 0c6bSedation and Analgesia in ICU
11/100
Grades of Recommendations(A) Methods strong, results consistent,
prospective, randomized,
controlled trials, no heterogeneity
(B) Methods strong, results inconsistent, prospective,
randomized,controlled trials, heterogeneity present
(C) Methods weak, observational studies
-
8/3/2019 0c6bSedation and Analgesia in ICU
12/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
13/100
ANALGESIAICU patients commonly have pain and physical discomfort
fromobvious factors, such as
preexisting diseases,
Invasive procedures, or trauma.
Monitoring and therapeutic devices (such as catheters,
drains,noninvasive ventilating devices, and endotracheal tubes)
Routine nursing care (such as airway suctioning,
physicaltherapy, dressing changes, and patient mobilization)
prolonged immobility
-
8/3/2019 0c6bSedation and Analgesia in ICU
14/100
Unrelieved pain may contribute to
inadequate sleep, possibly causing exhaustion and
disorientation.
Agitation.
Stress response characterized by tachycardia, increased
myocardial oxygen consumption,
hypercoagulability,immunosuppression, and persistent
catabolism,
pulmonary dysfunction.
Recommendation:All critically ill patients have the right to
adequateanalgesia and management of their pain. (C)
-
8/3/2019 0c6bSedation and Analgesia in ICU
15/100
Because patients can complete the NRS by writing or speaking,
andbecause it is applicable to patients in many age groups, NRS may
bepreferable to VAS in critically ill patients.
-
8/3/2019 0c6bSedation and Analgesia in ICU
16/100
Pain Assessment The most reliable and valid indicator of pain is
the patients self-
report. The location, characteristics, aggravating and
alleviatingfactors, and intensity of pain should be evaluated.
Assessment ofpain intensity may be performed with unidimensional
tools, such as
verbal rating scale (VRS),
visual analogue scale (VAS), and numeric rating scale (NRS)
RecommendationsThe level of pain reported by the patient mustbe
considered the current standard for assessment of pain andresponse
to analgesia whenever possible. Use of theNRSisrecommended to
assess pain.(B)
-
8/3/2019 0c6bSedation and Analgesia in ICU
17/100
As critically ill patients are often unable to communicate
theirlevel of pain if sedated, anesthetized, or receiving
neuromuscularblockade. Neither the VAS nor the NRS will resolve
this problemas they rely on the patients ability to communicate
with the careprovider
RecommendationsPatients who cannot communicate should be
assessed throughsubjective observation of pain-related behaviors
(movement, facialexpression, and posturing) and physiological
indicators (heart rate,
blood pressure, and respiratory rate) and the change in
theseparameters following analgesic therapy. (B)
-
8/3/2019 0c6bSedation and Analgesia in ICU
18/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
19/100
Recommendations:
Pain assessment and response to therapy should beperformed
regularly by using a scale appropriate to thepatient population and
systematically documented. (C)
The level of pain reported by the patient must beconsidered the
current standard for assessment of pain and
response to analgesia whenever possible. Use of the NRS
isrecommended to assess pain.(B)
Patients who cannot communicate should be assessedthrough
subjective observation of pain-related behaviors(movement, facial
expression, and posturing) and physiological
indicators (heart rate, blood pressure, and respiratory rate)and
the change in these parameters following analgesictherapy. (B)
-
8/3/2019 0c6bSedation and Analgesia in ICU
20/100
Analgesia Therapy
NONPHARMACOLOGIC TREATMENT
Stabilization of fractures Encouragement of patients to
communicat.
Music Minimizing irritating stimuli, such as traction on the
ETT. Proper positioning of patients.
Prompt treatment of anxiety and delirium
-
8/3/2019 0c6bSedation and Analgesia in ICU
21/100
PHARMACOLOGIC TREATMENTopioids,
NSAIDs,
PCMIn critically ill patients opioids are most often used for
acute pain treatmentOpioids mediate analgesia by interacting with a
variety of central andperipheral opioid receptors and . The
analgesic agents most commonly usedin ICU patients (fentanyl,
morphine, and hydromorphone)
-
8/3/2019 0c6bSedation and Analgesia in ICU
22/100
Intravenous opiates can be delivered in three different
modes:
Bolus intravenous injections are often used for moderate
pain,with doses titrated to analgesic requirements and the
avoidance ofrespiratory depression and hemodynamic instability
.
Continuous intravenous infusions of opiates are used for
moderate-to-severe pain which is poorly controlled with repeated
bolusinjections. After an initial bolus dose, a low continuous
infusion
rate is set with subsequent adjustment for adequate analgesia
.
Patient-controlled analgesia (PCA) may be preferable in
consciouspatients, particularly in the postoperative setting.This
techniqueallows self-dosing with opiates up to a predetermined
limit set bythe clinician.
-
8/3/2019 0c6bSedation and Analgesia in ICU
23/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
24/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
25/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
26/100
Recommendations: A therapeutic plan and goal of analgesia should
beestablished for each patient and communicated to all caregivers
toensure consistent analgesic therapy. (Grade of recommendation
C)
If intravenous doses of an opioid analgesic are required,
fentanyl,hydromorphone, and morphine are the recommended
agents.(Grade of recommendation C)
Scheduled opioid doses or a continuous infusion is preferred
over an
as needed regimen to ensure consistent analgesia. A PCA
devicemay be utilized to deliver opioids if the patient is able
tounderstand and operate the device. (Grade of recommendation
B)
Fentanyl is preferred for a rapid onset of analgesia in
acutelydistressed patients. (Grade of recommendation C)
Fentanyl or hydromorphone are preferred for patients
withhemodynamic instability or renal insufficiency. (Grade of
recommendation C)Morphine and hydromorphone are preferred for
intermittent therapy
because of their longer duration of effect. (Grade
ofrecommendation C)
-
8/3/2019 0c6bSedation and Analgesia in ICU
27/100
Recommendations: NSAIDs or acetaminophenmay be used as adjuncts
toopioids in selected patients. (Grade ofrecommendation B)
Ketorolac therapy should be limited to amaximum of five days,
with close monitoringfor the development of renal insufficiencyor
gastrointestinal bleeding.Other NSAIDs may be used via the
enteral
route in appropriate patients.(Grade of recommendation B)
-
8/3/2019 0c6bSedation and Analgesia in ICU
28/100
SEDATION
Sedation in critical care is the act of calming,
especially through administration of centrally acting drugs,
butalso through reassurance, information and music.
71% of critically ill patients have been shown to suffer
fromanxiety, confusion and agitation
Bernhard Walder, Martin R. TramrSWISS MED WKLY
2004;134:333346
-
8/3/2019 0c6bSedation and Analgesia in ICU
29/100
GOALS
the optimal depth of sedation (or sedation score) must
beindividualized. Some patients can be well ventilated
withoutsedation or analgesia, while others require deep sedation to
avoidventilator asynchrony or significant agitation.
The optimal target sedation score is best established by
frequent
assessments while titrating the sedative dose downward.
Theguiding principle should be to provide just enough medication
tominimize patient discomfort, agitation, and ventilator
asynchrony.
-
8/3/2019 0c6bSedation and Analgesia in ICU
30/100
GOALS
The appropriate target level of sedation will primarily depend
on apatients acute disease process and any therapeutic and
supportiveinterventions required.
A common target level of sedation in the ICU is a calm patient
thatcan be easily aroused with maintenance of the normal
sleep-wakecycle, but some may require deep levels of sedation to
facilitate MV.
The desired level of sedation should be defined at the start
oftherapy and reevaluated on a regular basis as the clinical
condition ofthe patient changes.
-
8/3/2019 0c6bSedation and Analgesia in ICU
31/100
Goals
those ventilated by a spontaneous breathing mode
neededsignificantly less midazolam and sufentanil compared with
those oncontrolled mechanical ventilation.
Patients with spontaneous breathing also had a significantly
shorter mean duration of ventilation (15 vs 21 days) and of
ICUstay (23 vs 30 days).
Putensen C, Zech S, Wrigge H, Zinserling J, Stuber F, Von
Spiegel T, et al. Long-term effects ofspontaneous breathing during
ventilatory support in patients with acute lung injury. Am J Respir
CritCare Med 2001;164:439.
-
8/3/2019 0c6bSedation and Analgesia in ICU
32/100
GOALS
Mechanical ventilation
Pressure support ventilation, CPAP, SIMV good pt cooperation
Ramsay 2, GCSC 13-15, SAS 4, RASS 0
Assisted controlled Ramsay 3, GCSC 8-12, SAS 3, RASS -1~-3
Pressure controlled Ramsay 4-5, GCSC 8-12, SAS 2, RASS -4
Agitation and delirium Ramsay 2-3, SAS 3-4, RASS 0~-2
IICP
Ramsay 5, SAS 1, RASS -5
-
8/3/2019 0c6bSedation and Analgesia in ICU
33/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
34/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
35/100
On-target sedation:
Decreases weaning period
Is not associated with muscular atrophy1
Decreases LOS and cost2
Provides cardiovascular1 and intraoperative
hemodynamic stability3
Improves patient safety1,3
Facilitates neurological assessment 1McGaffigan PA. Crit Care
Nursing. 2002;Feb Suppl:29-36. 2Dasta et al. Pharmacotherapy.
2006;26:798-805.
3Arbour R. Am J Crit Care Nursing. 2004;13:66-73.
-
8/3/2019 0c6bSedation and Analgesia in ICU
36/100
Incidence of Inadequate
Sedation
Dasta JF, et al. Crit Care Med. 2005;33:1266-1271.
-
8/3/2019 0c6bSedation and Analgesia in ICU
37/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
38/100
Recommendation: Sedation ofagitated
critically ill patients should be started only after providing
adequateanalgesia and treating reversible
physiologicalcauses. (Grade of recommendationC)
-
8/3/2019 0c6bSedation and Analgesia in ICU
39/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
40/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
41/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
42/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
43/100
Pain control in ICU
-
8/3/2019 0c6bSedation and Analgesia in ICU
44/100
An ideal sedation scale Good reliability and validity
determination of the degree of sedation and
agitation,
behavioral descriptors, Applicability
require minimal training
easy to score For diverse patient populationguide the titration
of therapy to a defined
sedation endpoint
Man scales are available but a true
-
8/3/2019 0c6bSedation and Analgesia in ICU
45/100
The Ramsay Scale The Glasgow Coma Scale modified by Cook and
Palma, GCSC
The Sedation Agitation Scale, SAS The Richmond Agitation and
Sedation Scale,RASS
The Bloomsbury sedation scale
the Adaptation to the Intensive Care Environment(ATICE)
scale
The Avripas sedation scale the Comfort scale for pediatric
patients.
Subjective methods
-
8/3/2019 0c6bSedation and Analgesia in ICU
46/100
Objective Assessment of
Sedation
-
8/3/2019 0c6bSedation and Analgesia in ICU
47/100
Ramsay Scale The most commonly scale used today
-
8/3/2019 0c6bSedation and Analgesia in ICU
48/100
BIS Recommending results good relationship with subjective
monitoring tools a decreased use of opioids and analgesics using
BIS-
guided sedation therapy
Conflicting results poor correlation with subjective monitoring
tools intra-individual variation in BIS values even in
chemically
paralyzed patients underestimation of sedation in non-chemically
paralyzed
patients.
the use of the BIS monitor in the ICU is stillunclear.
-
8/3/2019 0c6bSedation and Analgesia in ICU
49/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
50/100
Recommendations: A sedation goal or
endpoint should be established and regularlyredefined for each
patient. Regularassessment and response to therapyshould be
systematically documented.(Grade of recommendation C)The use of a
validated sedation assessmentscale (SAS, MAAS, or VICS)
isrecommended. (Grade of recommendationB)
Objective measures of sedation, such asBIS, have not been
completely evaluatedand are not yet proven useful in the ICU.(Grade
of recommendation C)
-
8/3/2019 0c6bSedation and Analgesia in ICU
51/100
Sedation Therapy BenzodiazepinesPropofol.
Central-Agonists
-
8/3/2019 0c6bSedation and Analgesia in ICU
52/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
53/100
Pharmacology of selected
sedatives
-
8/3/2019 0c6bSedation and Analgesia in ICU
54/100
Rapid onset of action Easily titratable level of adequate
sedation Short acting, allowing patient assessment, rapid recovery
following discontinuation, easy weaning from MV, and early
extubation. No or few adverse effects. No anaphylaxis or allergic
reaction. No nausea, vomiting, or phlebitis. Minimal metabolism;
not dependent on normal hepatic, renal, or pulmonary function
Minimal respiratory depression. Minimal effect on cardiovascular
function No pain on injection.
No active or toxic metabolites. No suppression of cortisol
production by the adrenal cortex. No or minimal interactions with
other commonly prescribed ICU drugs Ease of administration. Lack of
accumulation with prolonged administration Does not promote growth
of pathogens. No tolerance and withdrawal of pathogens Cost
effective. Easily prepared and long shelf-life. Safe for all ages
with no age-related changes in pharmacokinetics. Provides
facilitation of ventilator synchrony and the performance of various
procedures and nursing interventions Lack of abuse potential
Cohen et al., 2002)
-
8/3/2019 0c6bSedation and Analgesia in ICU
55/100
Recommendations: Midazolam or diazepamshould be used for rapid
sedationof acutely agitated patients.(Grade of recommendation
C)Propofol is the preferred sedative whenrapid awakening (e.g., for
neurologicassessment or extubation) is important.(Grade of
recommendation B)Midazolam is recommended for shorttermuse only, as
it produces unpredictable
awakening and time to extubationwhen infusions continue
longerthan 4872 hours. (Grade of recommendationA)Lorazepam is
recommended for the sedationof most patients via intermittenti.v.
administration or continuousinfusion. (Grade of recommendationB)The
titration of the sedative dose to adefined endpoint is recommended
withsystematic tapering of the dose or
daily interruption with retitration tominimize prolonged
sedative effects.(Grade of recommendation A)Triglyceride
concentrations should bemonitored after two days of
propofolinfusion, and total caloric intake fromlipids should be
included in the nutritionsupport prescription. (Grade
ofrecommendation B)The use of sedation guidelines, an algorithm,or
a protocol is recommended.(Grade of recommendation B
-
8/3/2019 0c6bSedation and Analgesia in ICU
56/100
Recommendation: The potential foropioid, benzodiazepine, and
propofolwithdrawal should be considered after
high doses or more than approximatelyseven days of continuous
therapy.Doses should be tapered systematicallyto prevent
withdrawal
symptoms. (Grade of recommendationB)
-
8/3/2019 0c6bSedation and Analgesia in ICU
57/100
Recommendations : A therapeutic plan and goal of analgesia
should be established for each patients and communicated to all
caregivers to ensure consistent analgesic therapy. ( Grade of
recommendation = C ) If intravenous doses of opioid analgesic are
required, fentanyl, hydromorphone, and morphine are the recommended
agents.
( Grade of recommendation = C ) Scheduled opioid doses or a
continuous infusion is preferred. A PCA device may be utilized to
deliver opioid if patient is able to understand and operated the
device. ( Grade of recommendation = B )
-
8/3/2019 0c6bSedation and Analgesia in ICU
58/100
Fentanyl is preferred for a rapid onset of analgesic in acutely
distressed patients. ( Grade of recommendation = B
)>>>>>c
Fentanyl or hydromorphone are preferred for patients with
hemodynamic instability or renal insufficiency ( Grade of
recommendation = B
)>>>>>>>>>>>>>>c Morphine
and hydromorphone are preferred for intermittent therapy because of
their longer duration of
effect. ( Grade of recommendation = B
)>>>>>>>>>>>>c
-
8/3/2019 0c6bSedation and Analgesia in ICU
59/100
NSAIDs or acetaminophen may be used as adjuncts to opioids in
selected patients. ( Grade of recommendation = B ) Ketorolac
therapy should be limited to a maximum of
5 days, with close monitoring for the development of renal
insufficience or GI bleeding. Other NSAIDs may be used via the
enteral route in appropriate patients. ( Grade of recommendation =
B )
-
8/3/2019 0c6bSedation and Analgesia in ICU
60/100
A sedation goal or endpoint should be established and regularly
refined for each patient. Regular assessment and response to
therapy should be systematically documented. ( Grade of
recommendation = C )
The use of a validated sedation assessment scale ( SAS, MAAS, or
VICS ) is recommended. ( Grade of recommendation = B ) Objective
measures of sedation, such as BIS, have not been completely
evaluated and are not yet proven useful in the
ICU. ( Grade of recommendation = C )
-
8/3/2019 0c6bSedation and Analgesia in ICU
61/100
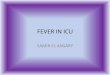
RAMSAY SEDATION SCORE Ramsay Sedation Scale Addenbrookes
Sedation Scale Rikers Sedation-Agitation Scale SAS
Motor Activity Assessment Scale MAAS Level Response 1 Anxious,
and agitated or restless, or both 2 Co-operative, orientated and
tranquil 3 Responds to commands only
4 Asleep, but brisk response to glabellar tap or low auditory
stimulation 5 Asleep, sluggish response to glabellar tap or loud
auditory stimulus 6 No response
-
8/3/2019 0c6bSedation and Analgesia in ICU
62/100
Recommendations : Midazolam or diazepam should be used for rapid
sedation of acutely agitated patients. ( Grade of recommendation =
C )
Propofol is the preferred sedative when rapid awakening ( e.g.
for neurologic assessment) is importment. ( Grade of recommendation
= B ) Midazolam is recommended for short term use only, as it
produces unpredictable awakening and time to extubation
when infusions continue longer than 48-72 hours. ( Grade of
recommendation = A ) Lorazepam is recommended for the sedation of
most patients via intermittent i.v. administration or continuous
infusion. ( Grade of recommendation = B )
-
8/3/2019 0c6bSedation and Analgesia in ICU
63/100
The potential for opioid, benzodiazepine, and propofol
withdrawal should be considered after high doses or more than
approximately 7 days of continuous therapy. Doses should be tapered
systematically to prevent
withdrawal symptoms. ( Grade of recommendation = B )
-
8/3/2019 0c6bSedation and Analgesia in ICU
64/100
an acute, reversible organic mental syndrome with disorder
ofattention and cognitive function, increased or
decreasedpsychomotor activity, and a disordered sleep-wake
cycle
-
8/3/2019 0c6bSedation and Analgesia in ICU
65/100
Delirium is an acute confusional state characterized by
analteration of consciousness with cognitive function.
characterizedby increased vigilance along with psychomotor and
autonomic
overactivity; these features are reflected in
clinicalmanifestations such as agitation, tremulousness, and
hallucinations. The most risk factors are underlying brain diseases
such as
dementia, stroke, or Parkinson disease, advanced age and
sensoryimpairment (hearing and vision loss). Elderly patients are
at thehighest risk for delirium.
Factors that may precipitate delirium include
polypharmacy(particularly psychoactive drugs), infection,
metabolicdisturbances, dehydration, immobility, malnutrition.
ICU-related factors contributing to the development of delirium
include sleepdeprivation, sensory overload, lack of meaningful
verbal or cognitive stimulation, andimmobilization. inadequate
analgesia ,Withdrawal of drugs such as opioids,sedatives,
-
8/3/2019 0c6bSedation and Analgesia in ICU
66/100
An interesting characteristic of delirium is that the behavior
ofthe patient can change dramatically within hours or even
minutes.Drowsiness and lethargy can change to alertness and
lucidity for atime, and then can quickly change to agitation and
aggression
-
8/3/2019 0c6bSedation and Analgesia in ICU
67/100
Deliriummay be associated with confusionand different motoric
subtypes: hypoactive,hyperactive, or mixed (179, 180).Hypoactive
delirium, which is associatedwith the worst prognosis, is
characterizedby psychomotor retardationmanifested by a calm
appearance, inattention,decreased mobility, and obtundationin
extreme cases. Hyperactivedelirium is easily recognized by
agitation,combative behaviors, lack of orientation,
and progressive confusion after sedative therapy.
The confusion assessment method for the
-
8/3/2019 0c6bSedation and Analgesia in ICU
68/100
The confusion assessmentmethod for thediagnosis of delirium in
the ICU (CAM-ICU)
(182, 185)
-
8/3/2019 0c6bSedation and Analgesia in ICU
69/100
Recommendation: Routine assessmentfor the presence of delirium
is
recommended.
(The CAM-ICU is a promisingtool for the assessment of delirium
inICU patients.) (Grade of recommendation
B)
-
8/3/2019 0c6bSedation and Analgesia in ICU
70/100
Suggested Criteria for DischargeFollowing Sedation and Analgesia
(1,2022,34)1. Patients should be easily aroused, alert and
oriented, or returned to their baselinestatus (i.e. infants,
cognitive impairment).2. Vital signs should be stable and within
acceptable limits3. Patient is not at risk for resedation (i.e.,
sufficient time has elapsed since
administration
of reversal agents)4. The patients protective reflexes have
returned, and there is no risk for airwayobstruction or
aspiration5. Pain is minimal and can be easily controlled in the
post-discharge setting6. Nausea is controlled and can be managed in
the post-discharge setting7. Outpatients should be discharged into
the care of a responsible adult8. Outpatients must be provided with
written instructions regarding medications,
activity, and emergency phone contacts
-
8/3/2019 0c6bSedation and Analgesia in ICU
71/100
Delirium (acute, reversible) Dementia (chronic, irreversible)
Depression (chronic, usually reversible)
-
8/3/2019 0c6bSedation and Analgesia in ICU
72/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
73/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
74/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
75/100
Prevention of Delirium Consider developing protocolized approach
Treat underlying infection and CHF Correct metabolic disturbances
and hypoxemia
Frequent reorientation of patient by nurse and family Goal
directed sedation/analgesia and /or daily wake-up Stop the
ventilator (SBT) each day to test readiness Early mobilization and
physical therapy Attention to optimizing sleep pattern
-
8/3/2019 0c6bSedation and Analgesia in ICU
76/100
Treatment of Delirium Identify etiologies Modify Risk Factors
Control symptoms?
No evidence that treatment reduces duration and severity of
symptoms Typical and atypical antipsychotic agents Sedatives? -
Particularly in combination with antipsychotic and for
drug/alcohol withdrawal delirium No treatment FDA approved
-
8/3/2019 0c6bSedation and Analgesia in ICU
77/100
Haloperidol Clinical Effects Hypnotic agent with antipsychotic
properties1 For treatment of delirium in critically ill adults1
Does not cause respiratory depression Haloperidol Adverse
Effects Dysphoria Adverse CV effects include QT interval
prolongation,
extrapyramidal symptoms, neuroleptic malignant syndrome (rare)
Metabolism altered by drug-drug interactions
-
8/3/2019 0c6bSedation and Analgesia in ICU
78/100
A l i d li i d ti t l f iti ll ill
-
8/3/2019 0c6bSedation and Analgesia in ICU
79/100
An analgesia-delirium-sedation protocol for critically illtrauma
patients reduces ventilator days and hospital
length of stay
Pain visual/objective pain assessment scale
Agitation Richmond Agitation-Sedation Scale RASS
Delirium Confusion Assessment Method CAM-ICU.
CONCLUSION: An objective assessment- based protocol
without daily interruption of medication infusion decreases
ventilator days and hospital length of stay in critically ill
trauma
patients .
Robinson BR, J Trauma. 2008 Sep;65(3):517-26
Remifentanil-propofol analgo-sedation shortens
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Robinson%20BR%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Robinson%20BR%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
8/3/2019 0c6bSedation and Analgesia in ICU
80/100
e e ta p opo o a a go sedat o s o te sduration of ventilation
and length of ICU stay
compared to a conventional regimen.15 Dutch hospitals,Patient
cohorts were randomised to remifentanil
based regimen (n = 96) with propofol as required, for a maximum
of10 days, or to conventional regimens (n = 109) of propofol,
midazolam or lorazepam combined with fentanyl or morphine .
Rozendaal FWIntensive Care Med .2009 Feb;35(2):291-8
CONCLUSIONS: In patients with an expected short-term duration
ofMV, remifentanil significantly improves sedation and agitation
levelsand reduces weaning time. This contributes to a shorter
duration of MV
and ICU-LOS .
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Rozendaal%20FW%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Rozendaal%20FW%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
8/3/2019 0c6bSedation and Analgesia in ICU
81/100
The current practice of sedation and analgesia inintensive care
units in Malaysian public
hospitals.A questionnaire survey sent by mail to 40 ICUs. 92.5%
response rate.
35% routinely assess the degree of sedation (Ramsay scale).
A written protocol for sedation was available in only 14
centers
(38%).
36 centers (95%) routinely adjust the degree of sedation
according
to patient's clinical progress,
only 10 centers (14%) interrupt sedation on a daily basis.
Ahmad N ,Tan CC , Med J Malaysia .2007 Jun;62(2):122-6
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Ahmad%20N%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Tan%20CC%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Tan%20CC%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Ahmad%20N%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Ahmad%20N%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Ahmad%20N%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
8/3/2019 0c6bSedation and Analgesia in ICU
82/100
the selection of agents for sedation depends on familiarity
(97%),
pharmacology (97%), the expected duration for sedation
(92%),
patient's clinical diagnosis (89%) and cost (73%).
Midazolam (89%) and morphine (86%)
14% frequently use NMB, mostly in head injury patients.
CONCLUSION the standard of practice could still be
improved by implementing the practice of sedation score
assessment and daily interruption of sedative infusion as
well as having a written protocol for sedation and
analgesia.
Ahmad N ,Tan CC ,Balan S Med J Malaysia .2007
Jun;62(2):122-6
Sedation and analgesia assessment tools in ICU
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Ahmad%20N%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Tan%20CC%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Balan%20S%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Balan%20S%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Tan%20CC%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Ahmad%20N%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
8/3/2019 0c6bSedation and Analgesia in ICU
83/100
Sedation and analgesia assessment tools in ICU
patients The usefulness of the BIS in ICU for patients lightly
sedated is
limited, mainly because of EMG artifact, when subjective
scales
are more appropriated in this situation. On the other hand,
subjective scales are insensitive to detect oversedation in
patients requiring deep sedation.
The contribution of the BIS in deeply sedation patients,
patients
under neuromuscular blockade or barbiturates has to be
proved
Thuong M .Ann Fr Anesth Reanim. 2008 Jul-Aug;27(7-8):581-95
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Thuong%20M%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Thuong%20M%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
8/3/2019 0c6bSedation and Analgesia in ICU
84/100
Sedation in the intensive care unit withremifentanil/propofol
versus midazolam/fentanyl
CONCLUSION: Compared with midazolam/fentanyl, a
remifentanil- based regimen for analgesia and sedation
supplemented with propofol significantly reduced the time
onmechanical ventilation and allowed earlier discharge from the
ICU, at equal overall costs .
Muellejans BGermany .Crit Care 10(3:)2006 R91.
Dexmedetomidine vs midazolam for sedation of
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Muellejans%20B%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Muellejans%20B%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
8/3/2019 0c6bSedation and Analgesia in ICU
85/100
critically ill patients
Prospective, double-BRT conducted in 68 centers in 5
countriesbetween March 2005 and August 2007 among 375 medical/
surgical ICU patients with expected mechanical ventilation
for
more than 24 hours
CONCLUSIONS: At comparable sedation levels, dex-treated
patients spent less time on the ventilator, experienced less
delirium, and developed less tachycardia and hypertension.
The most notable adverse effect of dex was bradycardia.
Riker RR USA JAMA .2009 Feb 4;301(5):489-99
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Riker%20RR%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Riker%20RR%22%5BAuthor%5D&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
8/3/2019 0c6bSedation and Analgesia in ICU
86/100
Sedation in the neurologic intensive care unit .Providing
adequate sedation in NICU depends on
determination of proper goals for sedation,
adequate assessment of the level of sedation, and
appropriate choice of drug based on the patient's
physiology.
The management of sedation in the ICU will influence
long-term
outcome. Delirium, anxiety, and pain must be identified and
treated
separately.
The use of protocols can improve compliance with
publishedevidence - based recommendations.
Keegan MT. Curr Treat Options Neurol .2008 Mar;10(2):111-25
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Keegan%20MT%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Keegan%20MT%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Keegan%20MT%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
8/3/2019 0c6bSedation and Analgesia in ICU
87/100
Propofol and dexmedetomidine may be used for rapidlytitratable
sedation, benzodiazepines for anxiolysis, neuroleptics
for treatment of delirium, and opiates for analgesia.
Unique aspects of patients with acute brain disease, such
aselevated intracranial pressure or status epilepticus,
requireadaptation of sedative regimens. Processed EEG
monitoring
and volatile anesthetic agents have not yet proven beneficial
orpractical for use in the ICU.
Keegan MT. Curr Treat Options Neurol .2008 Mar;10(2):111-25
Observational study of patient-ventilator asynchrony
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Keegan%20MT%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Keegan%20MT%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Keegan%20MT%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22Keegan%20MT%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
8/3/2019 0c6bSedation and Analgesia in ICU
88/100
y p y y
and relationship to sedation levelMETHODS: Airway pressure and
airflow were recorded for 15minutes. Patient-ventilator asynchrony
was assessed by determiningthe number of breaths demonstrating
ineffective triggering, doubletriggering, short cycling, and
prolonged cycling. Ineffective triggeringindex (ITI) was calculated
by dividing the number of ineffectively
triggered breaths by the total number of breaths (triggered
andineffectively triggered). Sedation level was assessed by
RASS,awake (yes or no), and CAM-ICU. Diagnosis of COPD,
sedativetype or dose, MV mode, and trigger method had no effect on
ITI.
CONCLUSIONS: Asynchrony is common, and deeper sedation levelis a
predictor of ineffective triggering
de Wit M USA, J Crit Care .2009 Mar;24(1):74-80
A randomized trial of intermittent lorazepam versuspropofol with
daily interruption in mechanically
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22de%20Wit%20M%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22de%20Wit%20M%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22de%20Wit%20M%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22de%20Wit%20M%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22de%20Wit%20M%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlushttp://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=Search&Term=%22de%20Wit%20M%22[Author]&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_RVAbstractPlus
-
8/3/2019 0c6bSedation and Analgesia in ICU
89/100
propofol with daily interruption in mechanicallyventilated
patients.
Median ventilator days 5.8 vs. 8.4, p = .04.
hospital survivors 4.4 vs. 9.0, p = .006.
ventilator-free survival 18.5 days vs. 10.2 p = .06.
Hospital mortality was not different
CONCLUSIONS: For medical patients requiring >48 hrs of
mechanical
ventilation, sedation with propofol results insignificantly
fewer ventilator
days compared with intermittent lorazepam when sedatives are
interrupted daily
Carson SS ; Crit Care Med. 2006 May;34(5):1326-1332.
Daily interruption of sedative infusions and complications
-
8/3/2019 0c6bSedation and Analgesia in ICU
90/100
y p pof critical illness in mechanically ventilated patients
VAP; upper GIT hge; bacteremia; barotrauma; DVT; andcholestasis
or sinusitis requiring surgical intervention.
daily interruption of sedatives(2.8%) vs. 26 (6.2%) in those
subjected
to conventional sedation techniques (p =.04).
CONCLUSIONS: Daily interruption of sedative infusions in MV
reduces ICU-LOS and, in turn, decreases the incidence of
complications of critical illness associated with prolonged
intubation
and mechanical ventilation.
Crit Care Med 2004 Jun;32(6):1272-6. University-based hospital
Chicago
Daily sedative interruption in mechanically ventilated
-
8/3/2019 0c6bSedation and Analgesia in ICU
91/100
y p ypatients at risk for coronary artery disease .
CONCLUSIONS: Myocardial ischemia is common in critically
illmechanically ventilated patients with coronary artery disease
riskfactors. Daily sedative interruption is not associated with
anincreased occurrence of myocardial ischemia in these patients
.
Kress JP ,Crit Care Med. 2007 Feb;35(2):365-71.
Administration of Sedatives and Level of Sedation:C ti E l ti i
th S d ti A it ti
-
8/3/2019 0c6bSedation and Analgesia in ICU
92/100
Comparative Evaluation via the Sedation-Agitation
Scale and the Bispectral Index
Conclusion Objective and subjective assessments of sedationare
highly correlated. Use of continuous infusions is associatedwith
deeper levels of sedation, and patients receiving continuous
infusions are more likely to be oversedated. Sedation
therapyshould be guided by subjective or objective assessment.
American Journal of Critical Care. 2003;12: 343-348
-
8/3/2019 0c6bSedation and Analgesia in ICU
93/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
94/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
95/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
96/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
97/100
-
8/3/2019 0c6bSedation and Analgesia in ICU
98/100
Before I forget...
-
8/3/2019 0c6bSedation and Analgesia in ICU
99/100
?any question..
Thank you
-
8/3/2019 0c6bSedation and Analgesia in ICU
100/100
Thank youAH
M
AD
F.
MA