Embed Size (px)
Citation preview
10/29/2008
1
THE CURRENT STATE OF INFLUENZA: PREVENTION, TREATMENT, AND , ,MECHANISMS OF RESISTANCE
R J dd Ph DRuss Judd, PharmDPGY2 Infectious Diseases Pharmacy Resident
UK HealthCare
Objectives
o Review the history and epidemiology of influenza
ib h d f i f i lo Describe the structure and function of viral proteins, including targets for anti‐influenza medications
o Discuss CDC recommendations for prevention and treatment of influenza
o Review the global impact of H5N1 infection and discuss treatment recommendations
10/29/2008
2
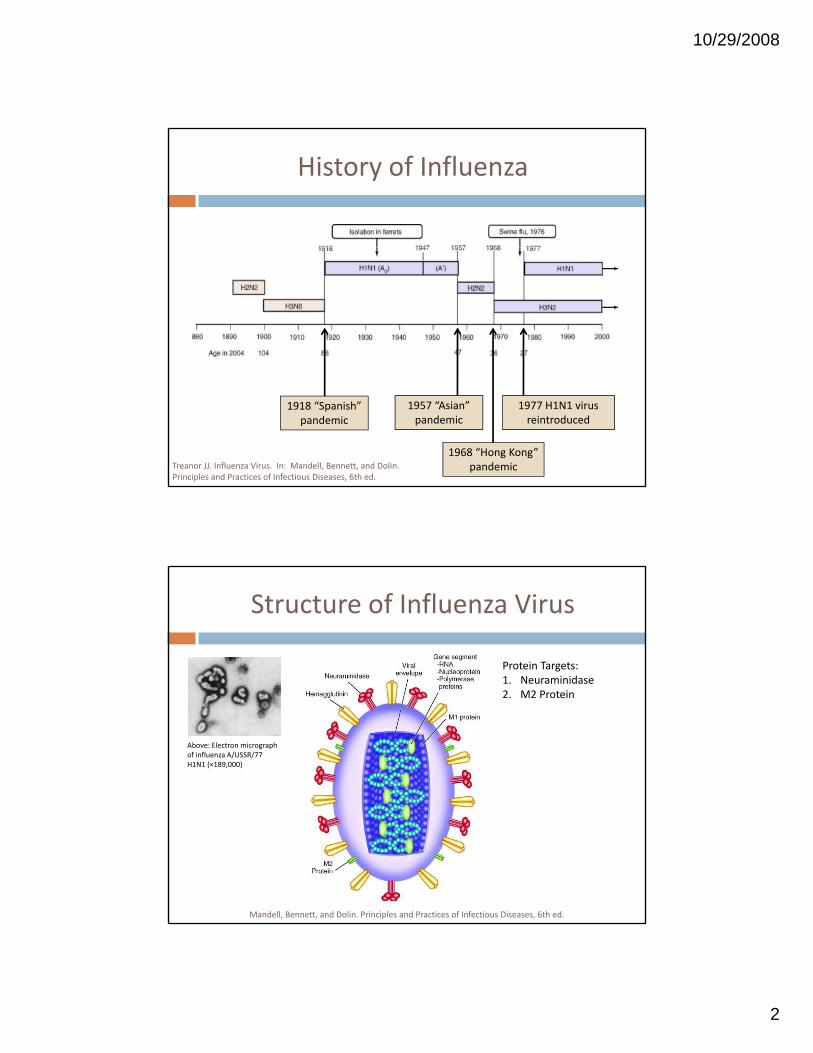
History of Influenza
1918 “Spanish” pandemic
1957 “Asian” pandemic
1968 “Hong Kong” pandemic
1977 H1N1 virus reintroduced
Treanor JJ. Influenza Virus. In: Mandell, Bennett, and Dolin. Principles and Practices of Infectious Diseases, 6th ed.
Structure of Influenza Virus
Protein Targets:1. Neuraminidase
Above: Electron micrograph of influenza A/USSR/77 H1N1 (×189,000)
2. M2 Protein
Mandell, Bennett, and Dolin. Principles and Practices of Infectious Diseases, 6th ed.
10/29/2008
3
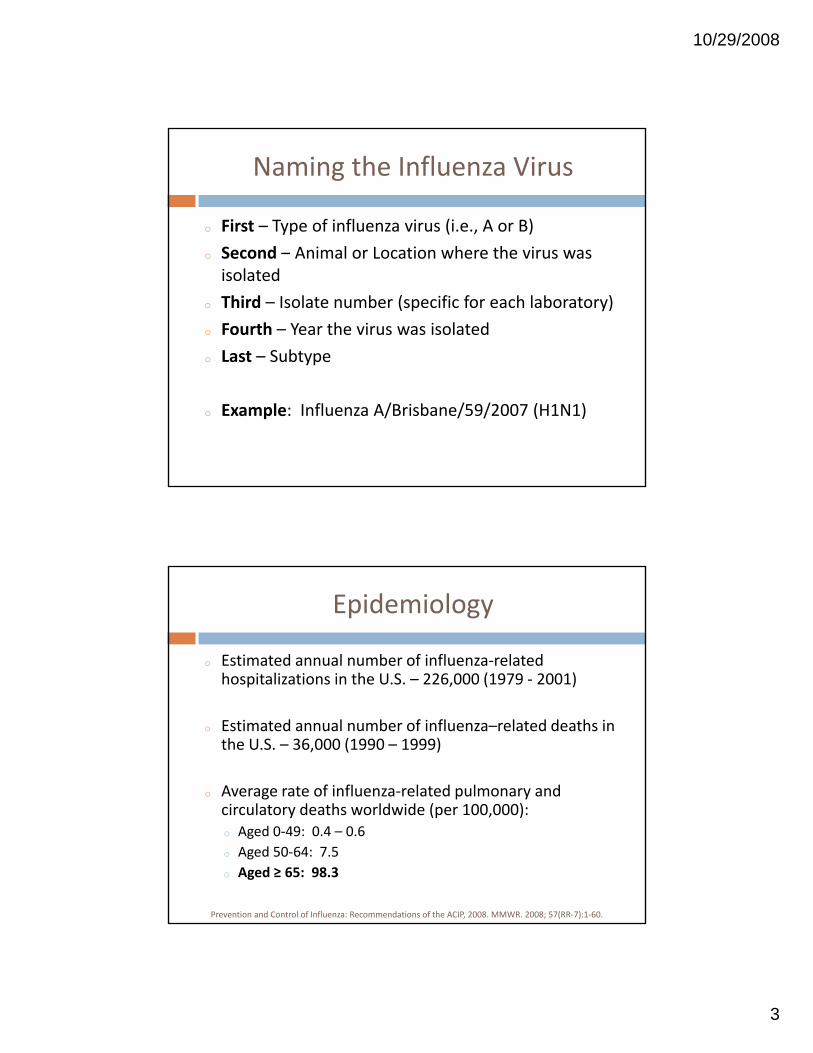
Naming the Influenza Virus
o First – Type of influenza virus (i.e., A or B)
S d A i l L i h h io Second – Animal or Location where the virus was isolated
o Third – Isolate number (specific for each laboratory)
o Fourth – Year the virus was isolated
o Last – Subtype
o Example: Influenza A/Brisbane/59/2007 (H1N1)
Epidemiology
o Estimated annual number of influenza‐related hospitalizations in the U.S. – 226,000 (1979 ‐ 2001)p , ( )
o Estimated annual number of influenza–related deaths in the U.S. – 36,000 (1990 – 1999)
o Average rate of influenza‐related pulmonary and i l d h ld id ( 100 000)circulatory deaths worldwide (per 100,000):
o Aged 0‐49: 0.4 – 0.6
o Aged 50‐64: 7.5
o Aged ≥ 65: 98.3
Prevention and Control of Influenza: Recommendations of the ACIP, 2008. MMWR. 2008; 57(RR‐7):1‐60.
10/29/2008
4
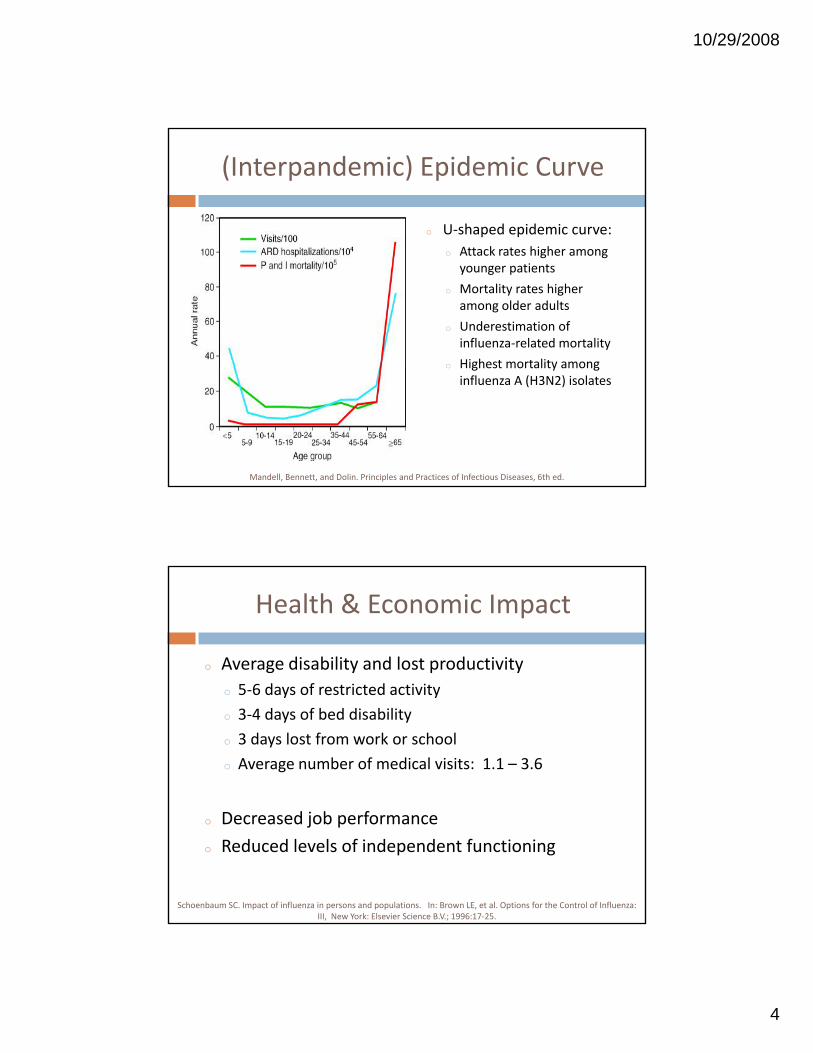
(Interpandemic) Epidemic Curve
o U‐shaped epidemic curve:
Att k t hi ho Attack rates higher among younger patients
o Mortality rates higher among older adults
o Underestimation of influenza‐related mortality
o Highest mortality amongo Highest mortality among influenza A (H3N2) isolates
Mandell, Bennett, and Dolin. Principles and Practices of Infectious Diseases, 6th ed.
Health & Economic Impact
o Average disability and lost productivity
5 6 d f t i t d ti ito 5‐6 days of restricted activity
o 3‐4 days of bed disability
o 3 days lost from work or school
o Average number of medical visits: 1.1 – 3.6
o Decreased job performance
o Reduced levels of independent functioning
Schoenbaum SC. Impact of influenza in persons and populations. In: Brown LE, et al. Options for the Control of Influenza: III, New York: Elsevier Science B.V.; 1996:17‐25.
10/29/2008
5
Epidemics, Pandemics, Shifts & Drifts
o Epidemics
C fi d t l ti (i it t t )o Confined to one location (i.e., city, town, or country)
o Average overall attack rates – 10‐20%
o Occur almost exclusively during the winter months
o October to April in the Northern hemisphere
o May to September in the Southern hemisphere
Often associated with a single strain of influenzao Often associated with a single strain of influenza
Mandell, Bennett, and Dolin. Principles and Practices of Infectious Diseases, 6th ed.
Epidemics, Pandemics, Shifts & Drifts
o PandemicsE t l id t i io Extremely rapid transmission
o Concurrent outbreaks throughout the world
o Associated with the emergence of a new virus (e.g., H5N1)
o Overall population possesses no immunity
o Multiple waves of disease
o Influena A viruses ONLYo Influena A viruses ONLY
Simonsen L, Clarke MJ, et al. Pandemic versus epidemic influenza mortality. J Infect Dis. 1998; 178:53‐60.
10/29/2008
6
Epidemics, Pandemics, Shifts & Drifts
o Antigenic Drifts
Minor antigenic variations in HA and NAo Minor antigenic variations in HA and NA
o Gradual accumulation of altered amino acid sequences
o Immunologic selection
o Antigenic Shift
New viruses to which the population has no immunityo New viruses to which the population has no immunity
o Cause of influenza pandemic
o Little to no relationship between HA/NA antigens of the new and wild‐type viruses
Pathogenesis
o Person‐to‐person transmissiono Virus‐containing respiratory secretionsg p y
o Large‐particle aerosols (sneezing, coughing, & talking)
o Attachment and penetration of columnar epithelial cells
o Activation of host‐defense mechanismso Secretory IgA
o Mucociliary apparatusy pp
o Viral replication and cell death – Limited to the respiratory tracto Inhibition of host‐cell protein synthesis
o Apoptosis (induction of Fas ligand)
o Systemic manifestations
10/29/2008
7
Clinical Signs and Symptoms
o Influenza A
Ab t t ft 1 4 i b ti i do Abrupt onset after a 1‐4 incubation period
o Systemic symptoms: fever (100‐104oF), chills, rigors, HAs, myalgias, malaise, and anorexia
o Respiratory symptoms: dry cough, pharyngeal pain, nasal obstruction & discharge
Elderly patients: fever debility or confusiono Elderly patients: fever, debility, or confusion
o Convalescent period: 1‐2 weeks for full recovery
Prevention and Control of Influenza: Recommendations of the ACIP, 2008. MMWR. 2008; 57(RR‐7):1‐60.
Clinical Signs and Symptoms
o Influenza B
S t bl i fl A i f tio Symptoms may resemble influenza A infection
o Lower severity symptoms (compared to influenza A)
o Influenza C
o Often afebrile
o Similar to the common cold
o Rarely associated with influenza syndrome
Mandell, Bennett, and Dolin. Principles and Practices of Infectious Diseases, 6th ed.
10/29/2008
8
Complications of Influenza
o Primary influenza viral pneumonia
Hi t f CV di ( h ti f ) h io History of CV disease (e.g., rheumatic fever) or chronic pulmonary disorders
o Viral cultures yield high titers of influenza A
o Gram stain negative
o No response to antibiotics
Hi h t lit to High mortality rate
Complications of Influenza
o Secondary Bacterial Pneumonia
P d i tl ld d lto Predominantly among older adults
o Chronic pulmonary, cardiac or metabolic disorders
o Cough, sputum production and consolidation on CXR
o Gram stain and sputum culture positive
o Streptococcus pneumoniae
H hil i flo Haemophilus influenza
o Staphylococcus aureus
Morens DM, TaubenbergerJK, et al. Role of Bacterial Pneumonia as a Cause of Death in Influenza. J Infect Dis. 2008.
10/29/2008
9
Complications of Influenza
o Risk factors for Bacterial Superinfection
M ili t b litio Mucociliary apparatus abnormalities
o Increased bacterial adherence to virus‐infected cells
o Loss of epithelial cell barrier to infection
o Upregulation of cell‐surface receptors
o Alterations in host immunity (e.g., PMNs)
Complications of Influenza
o Pulmonary Complicationso Mixed viral/bacterial pneumonia/ po Localized viral pneumoniao COPD exacerbations
o Non‐Pulmonary Complicationso Myositiso Myocarditis/pericarditisy /po Toxic shock syndromeo CNS complications (e.g., Guillain‐Barré syndrome)o Reye’s syndrome
Prevention and Control of Influenza: Recommendations of the ACIP, 2008. MMWR. 2008; 57(RR‐7):1‐60.
10/29/2008
10
Antiviral Agents for Influenza
o General Considerations
Early initiation of therapy is required (< 48 hours)o Early initiation of therapy is required (< 48 hours)
o Optimal therapy within 24 hours of symptom onset
o Duration of fever reduced by ~24 hours
o Less viral shedding at 48 hours
o Combination antiviral therapy PLUS vaccine
o NOTE: Due to high levels of resistance, M2 inhibitors (i.e., amantadine & rimantadine) should NOT be used for treatment or prophylaxis during the 2007‐08 season
Prevention and Control of Influenza: Recommendations of the ACIP, 2008. MMWR. 2008; 57(RR‐7):1‐60.
Antiviral Treatment Recommendations
o High‐Priority Patients (NA inhibitors ONLY)
H it li d ti t ith l b t fi do Hospitalized patients with laboratory‐confirmed influenza
o Patients with laboratory‐confirmed influenza who are at higher risk for influenza‐related complications
o Patients with laboratory‐confirmed influenza within 48 hours of symptom onset who want to decrease thehours of symptom onset who want to decrease the duration or severity of their symptoms
10/29/2008
11
Antiviral Prophylaxis Recommendations
o Patients at risk during the 2 wks post‐vaccination
i h i k i bl i h io High‐risk patients unable to receive the vaccine
o Unvaccinated family members or health‐care providers in close contact with high‐risk patients
o High‐risk patients and close contacts during seasons with unmatched vaccines
o Patients with immune deficiencies or those who might not respond to the vaccine
Antivirals for Influenza ‐M2 Inhibitors
o Amantadine (Symmetrel®)Protein target: M2 proteino Protein target: M2 protein
o Susceptible strains of influenza A ONLY
o Adverse effects: orthostatic hypotension; CNS effects (insomnia, dizziness, hallucinations); GI effects (N, D, anorexia); seizures; livedo reticularis*
o PK considerations: Elderly patients and renal failure
o Adult dose (influenza A) o Treatment: 100mg PO BID (w/in 24‐48 hrs of symptoms)
o Prophylaxis: 100mg PO BID
Lexi‐Comp Online: Amantadine. Last updated 8/14/2008.
10/29/2008
12
Antivirals for Influenza ‐M2 Inhibitors
o Rimantadine (Flumadine®)
P t i t t M2 t io Protein target: M2 protein
o Susceptible strains of influenza A ONLY
o Adverse effects: CNS effects (similar to placebo); GI effects (N, V, abdominal pain, anorexia)
o PK considerations: Elderly, severe renal impairment
Ad lt d (i fl A)o Adult dose (influenza A)
o Treatment: 100mg PO BID
o Prophylaxis: 100mg PO BID
Lexi‐Comp Online: Rimantadine. Last updated 8/14/2008.
Antivirals for Influenza ‐ NA Inhibitors
o Oseltamivir (Tamiflu®)
P t i t t N i ido Protein target: Neuraminidase
o Susceptible strains of influenza A and B
o Adverse effects: GI effects (N, V, abdominal pain)
o PK considerations: Dosage adjustment in renal failure
o Adult dose (influenza A and B)
o Treatment: 75mg PO BID x 5 days
o Prophylaxis: 75mg PO once daily
o Close contact: Initiate w/in 2 days of contact; Duration of 10 days
o Community outbreaks: Duration of up to 6 weeks
Lexi‐Comp Online: Oseltamivir. Last updated 9/9/2008.
10/29/2008
13
Antivirals for Influenza ‐ NA Inhibitors
o Zanamivir (Relenza®)o Protein target: Neuraminidaseo Protein target: Neuraminidase
o Susceptible strains of influenza A and B
o Adverse effects: CNS effects (HA, fever, chills, hallucinations, seizures); GI effects (N, V, D, throat/tonsil discomfort); Respiratory effects
o PK considerations: Poor oral bioavailability
o Dose (influenza A and B)o Dose (influenza A and B)o Treatment: 2 inhalations (10mg) BID x 5 days
o Prophylaxis: 2 inhalations (10mg) once dailyo Household contact: Initiate w/in 1.5 days of contact x 10 days
o Community outbreak: Initiate w/in 5 days of outbreak x 28 days
Lexi‐Comp Online: Zanamavir. Last updated 8/14/2008.
Types of Influenza Vaccine
o Trivalent Inactivated Vaccine (TIV)All persons aged ≥ 6 monthso All persons aged ≥ 6 months
o Patients with high‐risk medical conditions
o Live, Attenuated Influenza Vaccine (LAIV)o Healthy, non‐pregnant persons aged 2 – 49 years
o Safety and effectiveness not established in patientso Safety and effectiveness not established in patients with high‐risk medical conditions
o Not indicated in children aged 2‐4 years with RAD or children receiving aspirin or other salicylates
10/29/2008
14
Influenza Vaccine Composition
o 2008‐09 Influenza Vaccine
A/B i b /59/2007 (H1N1)o A/Brisbane/59/2007 (H1N1)
o A/Brisbane/10/2007 (H3N2)
o B/Florida/4/2006
o Viruses forecasted to be in circulation during the influenza season
o Favorable growth properties for mass production
Prevention and Control of Influenza: Recommendations of the ACIP, 2008. MMWR. 2008; 57(RR‐7):1‐60.
Target Populations
o Children and Adolescents6 months 18 yearso 6 months – 18 years
o 2 doses of influenza vaccine recommended for all children aged 6 months to 8 years who have never received an influenza vaccine (separated by ≥ 4 wks)
o Indications for TIVo Children aged 6‐23 months
Child d 2 4 ith ti i dio Children aged 2‐4 years with reactive airway disease
o Children with high‐risk chronic medical conditions
o Indications for LAIVo Healthy children aged 2‐18 years

10/29/2008
15
Target Populations
o High‐Risk Conditions
All hild d 6 th 4 (59 th )o All children aged 6 months – 4 years (59 months)
o All patients aged ≥ 50 years
o Children receiving long‐term aspirin therapy
o Pregnancy during the influenza season
o Chronic pulmonary, CV, renal, hepatic, hematological t b li di dor metabolic disorders
o Immunosuppression (iatrogenic or HIV)
o Nursing home or LTCF residents
Target Populations
o Household Contacts or Caregivers
H lth ido Health care providers
o Household contacts of children aged ≤ 59 months and adults aged ≥ 50 years
o Household contacts of other high‐risk patients
h d h lik lih d fo Any person who wants to reduce the likelihood of becoming infected with influenza
10/29/2008
16
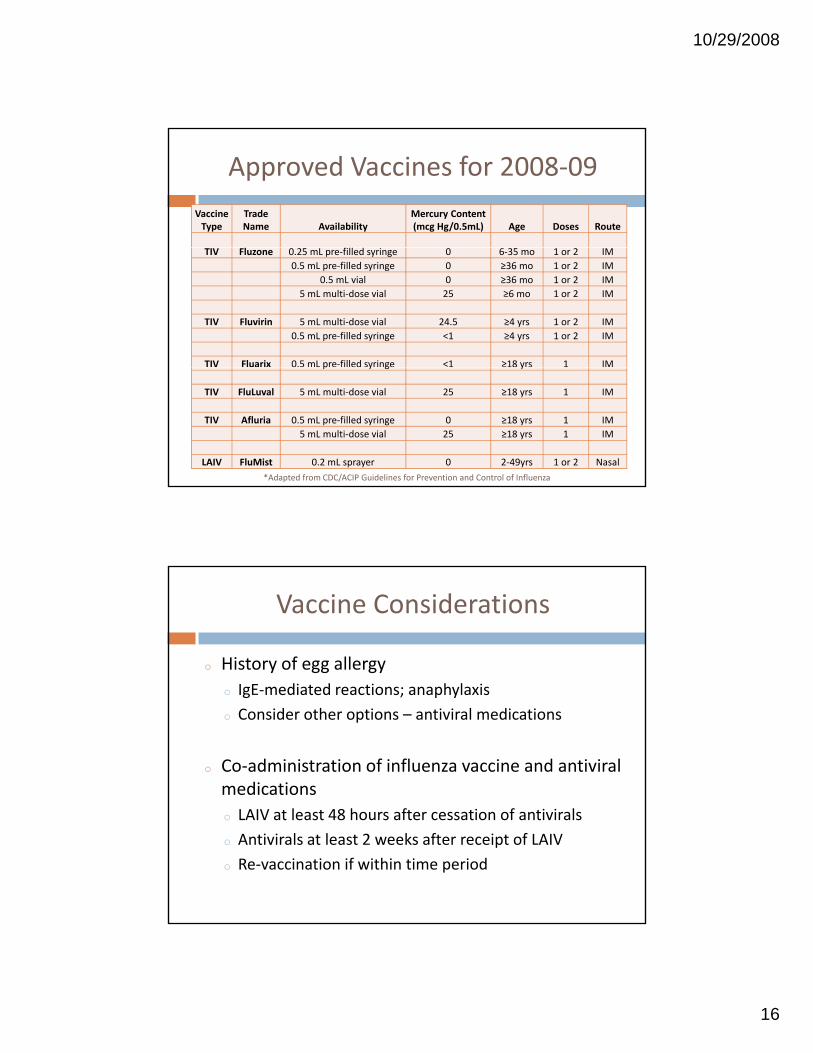
Vaccine Type
TradeName Availability
Mercury Content (mcg Hg/0.5mL) Age Doses Route
Approved Vaccines for 2008‐09
TIV Fluzone 0.25 mL pre‐filled syringe 0 6‐35 mo 1 or 2 IM
0.5 mL pre‐filled syringe 0 ≥36 mo 1 or 2 IM
0.5 mL vial 0 ≥36 mo 1 or 2 IM
5 mL multi‐dose vial 25 ≥6 mo 1 or 2 IM
TIV Fluvirin 5 mL multi‐dose vial 24.5 ≥4 yrs 1 or 2 IM
0.5 mL pre‐filled syringe <1 ≥4 yrs 1 or 2 IM
TIV Fluarix 0.5 mL pre‐filled syringe <1 ≥18 yrs 1 IMp y g y
TIV FluLuval 5 mL multi‐dose vial 25 ≥18 yrs 1 IM
TIV Afluria 0.5 mL pre‐filled syringe 0 ≥18 yrs 1 IM
5 mL multi‐dose vial 25 ≥18 yrs 1 IM
LAIV FluMist 0.2 mL sprayer 0 2‐49yrs 1 or 2 Nasal
*Adapted from CDC/ACIP Guidelines for Prevention and Control of Influenza
Vaccine Considerations
o History of egg allergy
I E di t d ti h l io IgE‐mediated reactions; anaphylaxis
o Consider other options – antiviral medications
o Co‐administration of influenza vaccine and antiviral medications
o LAIV at least 48 hours after cessation of antivirals
o Antivirals at least 2 weeks after receipt of LAIV
o Re‐vaccination if within time period
10/29/2008
17
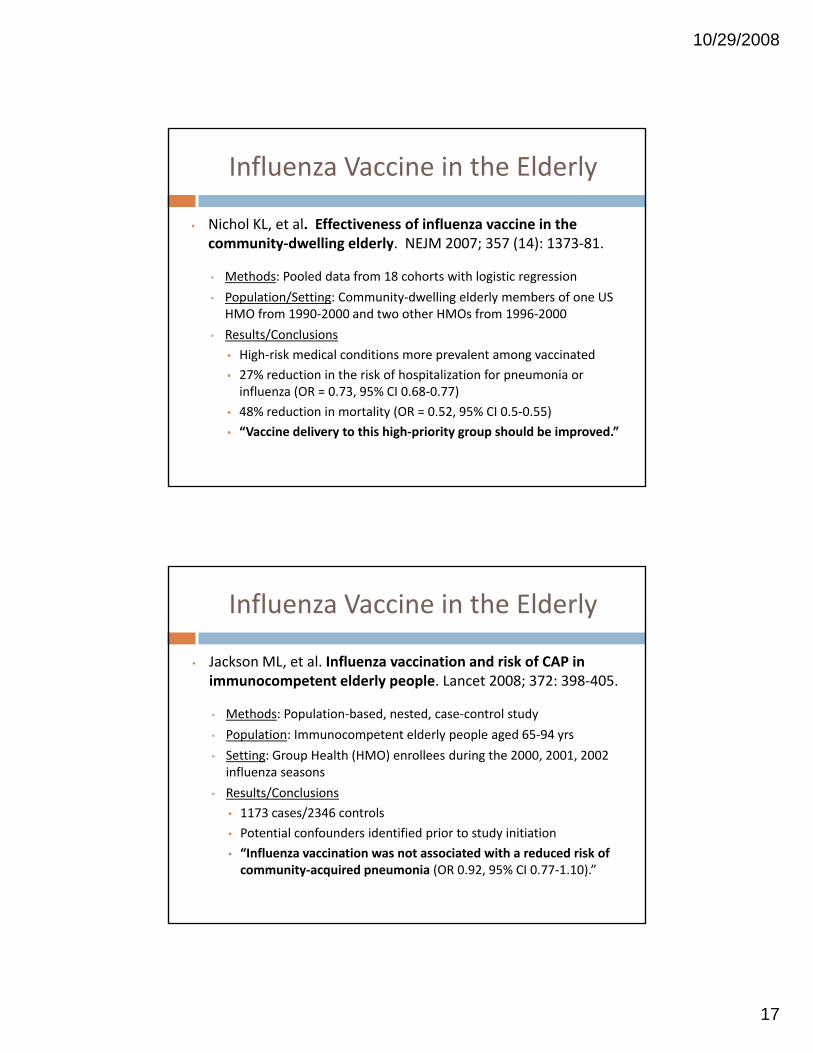
Influenza Vaccine in the Elderly
• Nichol KL, et al. Effectiveness of influenza vaccine in the community‐dwelling elderly. NEJM 2007; 357 (14): 1373‐81.community dwelling elderly. NEJM 2007; 357 (14): 1373 81.
• Methods: Pooled data from 18 cohorts with logistic regression
• Population/Setting: Community‐dwelling elderly members of one US HMO from 1990‐2000 and two other HMOs from 1996‐2000
• Results/Conclusions
• High‐risk medical conditions more prevalent among vaccinated
• 27% reduction in the risk of hospitalization for pneumonia or influenza (OR = 0.73, 95% CI 0.68‐0.77)
• 48% reduction in mortality (OR = 0.52, 95% CI 0.5‐0.55)
• “Vaccine delivery to this high‐priority group should be improved.”
Influenza Vaccine in the Elderly
• Jackson ML, et al. Influenza vaccination and risk of CAP in immunocompetent elderly people. Lancet 2008; 372: 398‐405.immunocompetent elderly people. Lancet 2008; 372: 398 405.
• Methods: Population‐based, nested, case‐control study
• Population: Immunocompetent elderly people aged 65‐94 yrs
• Setting: Group Health (HMO) enrollees during the 2000, 2001, 2002 influenza seasons
• Results/Conclusions
• 1173 cases/2346 controls
• Potential confounders identified prior to study initiation
• “Influenza vaccination was not associated with a reduced risk of community‐acquired pneumonia (OR 0.92, 95% CI 0.77‐1.10).”
10/29/2008
18
Avian Influenza (Bird Flu)
o Naturally occurring viruses among wild birds
Sh ddi f i fl i i li lo Shedding of influenza virus in saliva, nasal secretions, and feces
o Virus transmitted from wild to domestic birds
o Two main forms of disease among domestic poultry
o Low pathogenicity (mild symptoms)
o High pathogenicity (high mortality rate)
Human Infection (H5N1)
o H5N1 infection in humans first reported in Hong Kong in 1997Kong in 1997
o Two main influenza A subtypes currently circulating among humans (H1N1, H3N2)
o Influenza A (H5N1) occurs mainly in birds
o Direct or close contact with H5N1‐infected poultry or contaminated surfaces
10/29/2008
19
Human Infection (H5N1)
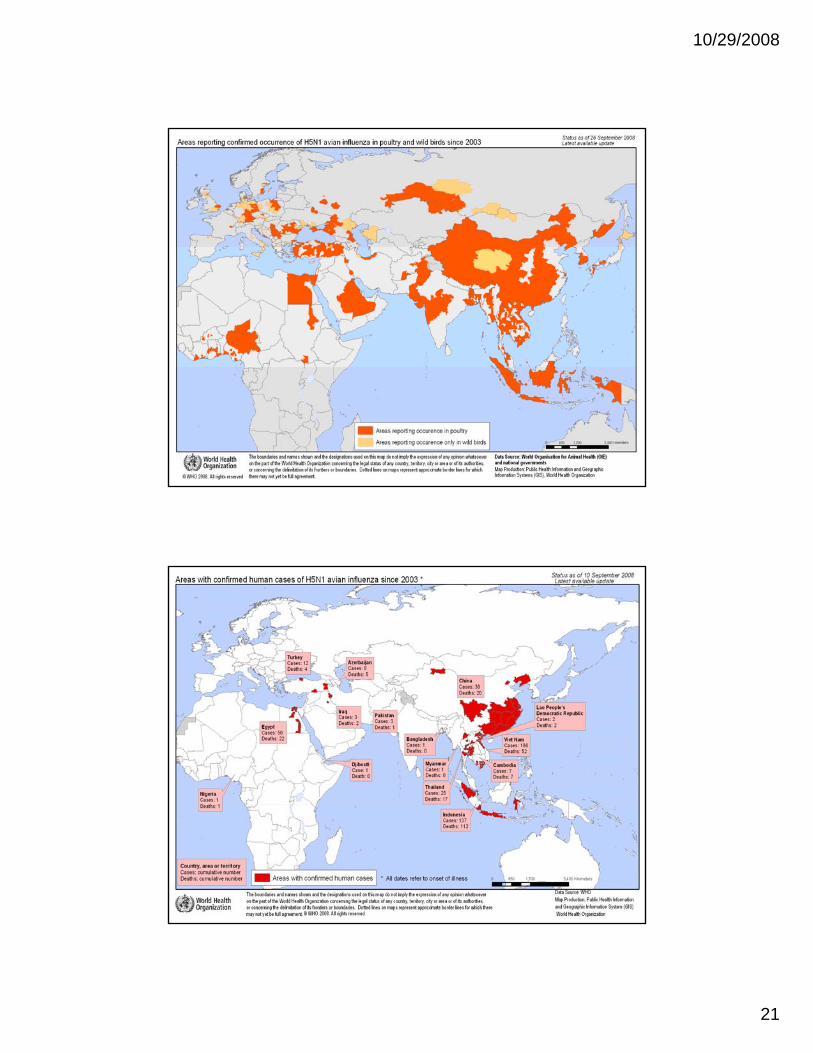
o Reported cases in Asia, Africa, and Europe
i h i id i d i d io Highest incidence in Indonesia and Vietnam
o Epidemiologic trends in H5N1 infection
o Overall mortality ~60%
o Children and adults less than 40 years of age
o Highest mortality in cases 10‐19 years of age
o Significant risk factors include close contact with sick or dead poultry or exposure to live poultry markets
10/29/2008
20
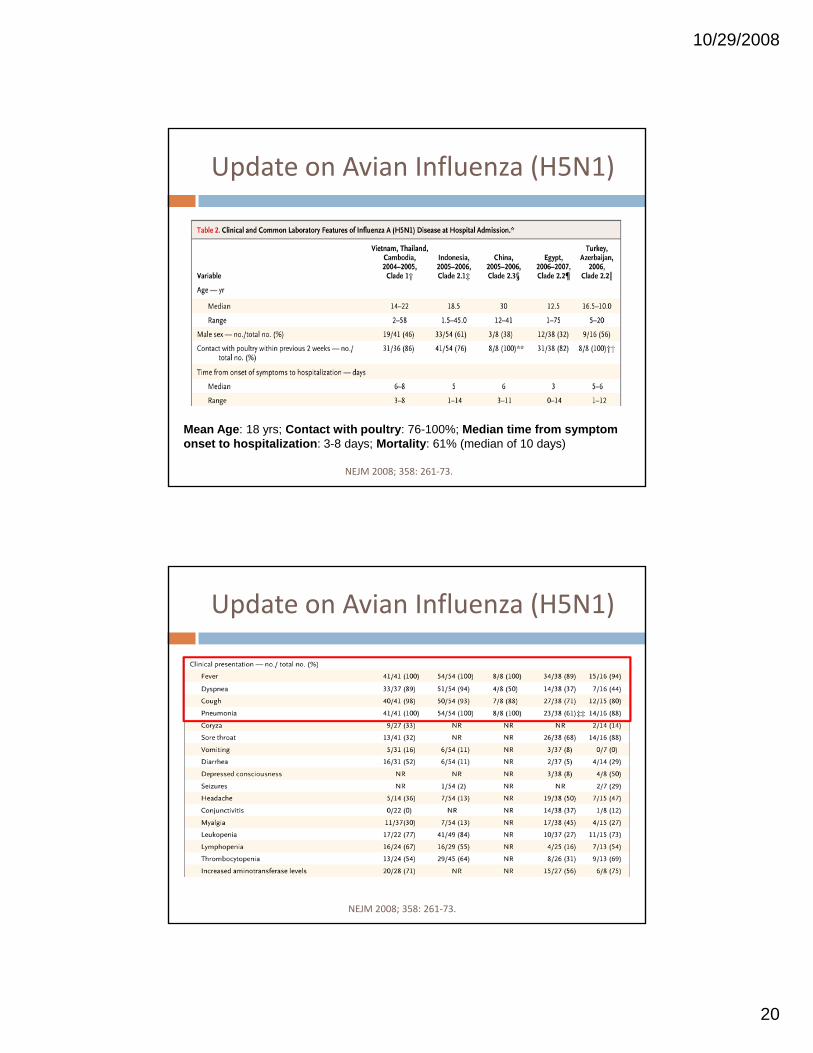
Update on Avian Influenza (H5N1)
Mean Age: 18 yrs; Contact with poultry: 76-100%; Median time from symptom onset to hospitalization: 3-8 days; Mortality: 61% (median of 10 days)
NEJM 2008; 358: 261‐73.
Update on Avian Influenza (H5N1)
NEJM 2008; 358: 261‐73.
10/29/2008
21
10/29/2008
22
Management of H5N1 Infection
o Neuraminidase Inhibitors (e.g., oseltamivir)
P ibl d ti i H5N1 i t d t lito Possible reduction in H5N1‐associated mortality
o Modified dosing regimens
o Combination therapy??
o Adamantanes (e.g., amantadine, rimantadine)
o May be considered in areas of low resistance
o Monotherapy not recommended when neuraminidase inhibitors are available
World Health Organization ‐ Clinical Management of Human Infection with H5N1 Virus
Management of H5N1 Infection
o Secondary Bacterial Pneumonia
A tibi ti h l i i NOT d do Antibiotic prophylaxis is NOT recommended
o Treatment of community‐acquired pneumonia according to evidence‐based guidelines
o Supportive Care
o Oxygen therapy
o Management of septic shock and ARDS
o Infection ControlWorld Health Organization ‐ Clinical Management of Human Infection with H5N1 Virus
10/29/2008
23
H5N1 Vaccine Development
o Early Antigenic Variation
Occurrence after initial vaccine developmento Occurrence after initial vaccine development
o Genetic variations in H5 HA genes
o FDA Press Release (4/17/2007)
o FDA Approves First US Vaccine for Humans Against the Avian Influenza Virus H5N1
o Ehrlich HJ, et al. A clinical trial of a whole‐virus H5N1 vaccine derived from cell culture. NEJM 2008; 358: 2573‐84.
World Health Organization ‐ Epidemic and Pandemic Alert and Response
THE CURRENT STATE OF INFLUENZA: PREVENTION, TREATMENT, AND , ,MECHANISMS OF RESISTANCE
R J dd Ph DRuss Judd, PharmDPGY2 Infectious Diseases Pharmacy Resident
UK HealthCare