Embed Size (px)
Citation preview

0009COR0009COR11
A CRUSADE to Improve A CRUSADE to Improve Quality of Care for ACS PatientsQuality of Care for ACS Patients
A CRUSADE to Improve A CRUSADE to Improve Quality of Care for ACS PatientsQuality of Care for ACS Patients
Eric D. Peterson, MD, MPHAssociate Professor of Medicine
Director of CV Outcomes and QualityDuke Clinical Research Institute (DCRI)
Duke University Medical Center
Eric D. Peterson, MD, MPHAssociate Professor of Medicine
Director of CV Outcomes and QualityDuke Clinical Research Institute (DCRI)
Duke University Medical Center

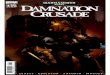
Annual Admissions for Acute Coronary Syndrome (ACS)
Annual Admissions for Acute Coronary Syndrome (ACS)
1.4 MillionNon-ST-segment
elevation ACSAND GROWING!
600,000ST-segment elevation
MI
~ 2.0 MM patients admittedto CCU or telemetry annually

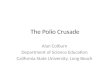
DiscoveryDiscoveryDiscoveryDiscovery
OutcomesOutcomes
Clinical Clinical TrialsTrials
Clinical Clinical TrialsTrials
GuidelinesGuidelinesGuidelinesGuidelines
PerformanceIndicators
PerformanceIndicators
AssessmentAssessmentAssessmentAssessment
The Cycle of Clinical TherapeuticsThe Cycle of Clinical Therapeutics
Califf R, Peterson, E JACC 2002;40:1895-901Califf R, Peterson, E JACC 2002;40:1895-901

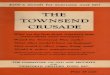
ST-segment Elevation
Time Dependent: Emergency Evaluation of ACS
Time Dependent: Emergency Evaluation of ACS
Chest pain or Short of Breath
Unstable Angina
ST-segment Depression
– + +
Presentation
ECG
Diagnosis
Braunwald E,2002 http://www.acc.org/clinical/guidelines/unstable/unstable
Normal
Markers
Acute MI
–+
Rule-Out

Troponin as a Marker of Increased Risk in ACSTroponin as a Marker of Increased Risk in ACS
30%
12% 11%
34%
22%19% 19%
23%
2%4% 4%
12%
1% 0%
6% 6%
0%
10%
20%
30%
40%
Hamm(1992)
FRISC(1996)
TRIM(1999)
Pettijohn(1997)
Hamm(1997)
Hamm(1997)
Polanczyk(1998)
Galvanni(1997)
Dea
th o
r M
I
Troponin +
Troponin -30%
12% 11%
34%
22%19% 19%
23%
2%4% 4%
12%
1% 0%
6% 6%
0%
10%
20%
30%
40%
Hamm(1992)
FRISC(1996)
TRIM(1999)
Pettijohn(1997)
Hamm(1997)
Hamm(1997)
Polanczyk(1998)
Galvanni(1997)
Dea
th o
r M
I
Troponin +
Troponin -

10 ng/mL troponin standard material, measured by 13 participating cTnI assays, in duplicate samples:
10 ng/mL troponin standard material, measured by 13 participating cTnI assays, in duplicate samples:
Value 1 Value 2 Mean143.7 135.7 139.746.9 47.9 47.419.9 19.9 19.949.2 50.1 49.74.3 4.1 4.2
12.5 12.6 12.67.4 8.9 8.26.0 6.1 6.0
16.5 17.4 17.012.6 13.2 12.912.6 12.4 12.5
Systematic Variation Between cTnI AssaysSystematic Variation Between cTnI Assays
Conclusion: Within assay reproducibility good, but across assay results varied >30-fold different!
Clin Chem 2001;47:431-437Clin Chem 2001;47:431-437

US PURSUIT Results: Treatment Effect of Eptifibatide in High Risk Subgroups
Death or MI
US PURSUIT Results: Treatment Effect of Eptifibatide in High Risk Subgroups
Death or MI
MenMen
Old age tertileOld age tertile
No diabetes mellitusNo diabetes mellitus
Low age tertileLow age tertile
Middle age tertileMiddle age tertile
WomenWomen
Diabetes mellitusDiabetes mellitus

USING THE TIMI RISK SCORE TO PREDICT BENEFIT OF GP IIb-IIIa THERAPYUSING THE TIMI RISK SCORE TO PREDICT BENEFIT OF GP IIb-IIIa THERAPY
7.7 9.9
23.327.3
37.3
6.3
15 17.322.8 21.3
0
10
20
30
40
50
1//2 3 4 5 6//7
14 d
ay e
nd
po
int
(%) placebo
GP IIb/IIIa
7.7 9.9
23.327.3
37.3
6.3
15 17.322.8 21.3
0
10
20
30
40
50
1//2 3 4 5 6//7
14 d
ay e
nd
po
int
(%) placebo
GP IIb/IIIa
Morow DA,Eur HeartJ 2002;23:223-229
Number of risk factors
NNT 72 NA 17 22 6.2

Benefits of GP IIb-IIIa by Troponin Status in Clinical Trials
Benefits of GP IIb-IIIa by Troponin Status in Clinical Trials
TnT-negativeTnT-negativeTnT-positiveTnT-positive
PARAGONPARAGON BB
PRISMPRISM
CAPTURECAPTURE
COMBINEDCOMBINED
0.1250.125 1111 22 22
Newby, Circulation 2001Newby, Circulation 2001
0.1250.1250.50.50.50.5

In-hospital Mortality By Early GP IIb-IIIa Inhibitor Use (within 24 hrs) †
Cumulative Q1 2003 Data
In-hospital Mortality By Early GP IIb-IIIa Inhibitor Use (within 24 hrs) †
Cumulative Q1 2003 Data
∆ 42%P < 0.0001∆ 42%
P < 0.0001
*Includes patients who received late GP IIb-IIIa inhibitor (> 24 hrs) therapy.† Unadjusted for risk.
2.71%
4.68%
0%
2%
4%
6%
8%
% In-hospital Mortality
No Early GP IIb-IIIa Inhibitor (n = 26,596)
Early GP IIb-IIIaInhibitor (n = 14,296)

Mortality Benefits of Early GP IIb-IIIa Inhibitor: Results from Clinical Trials, NRMI and CRUSADE
Mortality Benefits of Early GP IIb-IIIa Inhibitor: Results from Clinical Trials, NRMI and CRUSADE
NRMI NSTEMINRMI NSTEMI##
(N=60,770)(N=60,770)
95% CI Odds Ratio
1.0 2.00.5 No Early GP IIb-IIIa Inhibitor Better
Early GP IIb-IIIa Inhibitor Better
0.91 (0.81, 1.03)
CRUSADE ACSCRUSADE ACS††
(n=31,257)(n=31,257)
0.88 (0.79, 0.97)
0.90 (0.78, 1.04)
6 RCTs ACS6 RCTs ACS** (n=31,402)(n=31,402)
Boersma Lancet 2002;359:189-98 # Peterson JACC 2003;42:45-53††Adjusted for risk, treatment, hospital factorsAdjusted for risk, treatment, hospital factors
Boersma Lancet 2002;359:189-98 # Peterson JACC 2003;42:45-53††Adjusted for risk, treatment, hospital factorsAdjusted for risk, treatment, hospital factors

Adjusted Mortality by Early GP IIb-IIIa Inhibitor Results by Troponin Status
Adjusted Mortality by Early GP IIb-IIIa Inhibitor Results by Troponin Status
95% CI Odds Ratio
1.0 2.00.5 No Early GP IIb-IIIa Inhibitor Better
Early GP IIb-IIIa Inhibitor Better
CRUSADE OverallCRUSADE Overall(n=31,257)(n=31,257)
0.90 (0.78, 1.04)
0.84 (0.71, 0.99) CRUSADE Trop PosCRUSADE Trop Pos (n=25,848)(n=25,848) CRUSADE Trop PosCRUSADE Trop Pos (n=25,848)(n=25,848)
CRUSADE Trop NegCRUSADE Trop Neg (n=5,964)(n=5,964) CRUSADE Trop NegCRUSADE Trop Neg (n=5,964)(n=5,964)
0.95 (0.46, 1.35)
Excludes pts transferred out, GP IIb-IIIa contraindications Excludes pts transferred out, GP IIb-IIIa contraindications

4.15%
5.02%
1.65%1.32%
0%
1%
2%
3%
4%
5%
6%
Death Death/MI
"In-lab Only" GP IIb-IIIa (n =3,642)
"Upfront" GP IIb-IIIa (n = 2,191)
In-hospital Events by “Upfront” vs. “In-lab Only” GP IIb-IIIa Inhibitor Use
(Patients receiving PCI < 48 hrs + GP IIb-IIIa; n= 5,833)
In-hospital Events by “Upfront” vs. “In-lab Only” GP IIb-IIIa Inhibitor Use
(Patients receiving PCI < 48 hrs + GP IIb-IIIa; n= 5,833)
Adjusted OR 0.95; (95% CI 0.60-1.15)Adjusted OR 0.95; (95% CI 0.60-1.15)
Adjusted OR 0.83; (95% CI 0.63-1.09)Adjusted OR 0.83; (95% CI 0.63-1.09)
Peterson ACC 2003Peterson ACC 2003

14.5
24.2
16.914.3
0
5
10
15
20
25
30
TnT - TnT +
14.5
24.2
16.914.3
0
5
10
15
20
25
30
TnT - TnT +
6 m
o D
eath
/ MI/
Reh
osp
(%
)
CONS INV
TACTICS-TIMI 18Early Intervention vs Conservative
By Troponin Status
TreatmentTreatmentInteractionInteraction
P<0.001P<0.001
N=414N=414 N=396N=396 N=463N=463 N=495N=495

11.8
20.3
12.816.1
19.5
30.6
0
5
10
15
20
25
30
35
Low 0-2 Intermed. 3-4 High 5-7
11.8
20.3
12.816.1
19.5
30.6
0
5
10
15
20
25
30
35
Low 0-2 Intermed. 3-4 High 5-7
6 m
o D
eath
/ M
I/ R
eho
sp (
%) CONS INV
TACTICS-TIMI 18Early Intervention vs Conservative
By TIMI Risk Score

CRUSADE: Benefits of Early Catheterization within 48 hrs by Risk GroupCRUSADE: Benefits of Early Catheterization within 48 hrs by Risk Group
0
2
4
6
8
10
12
Low Risk Moderate Risk High Risk
% I
n-H
os
pit
al
Mo
rta
lity
Early Cath No Early Cath
0
2
4
6
8
10
12
Low Risk Moderate Risk High Risk
% I
n-H
os
pit
al
Mo
rta
lity
Early Cath No Early Cath
- Bhatt AHA 2002- Bhatt AHA 2002

Does Current Practice Mirror Guidelines Recommendations?
Does Current Practice Mirror Guidelines Recommendations?

AK(0)
WA(11)
OR(5)
CA(43)
ID(1)
NV(1)
MT(0)
WY(0)
CO(4)
NM(2)
ND(1)
SD(2)
NE (3)
KS(7)
OK(5)
TX(19)
MN(6)
IA(4)
MO(12)
AR(5)
LA(5)
WI(5) MI
(23)
MI
UT(1)
AZ(14)
HI (3)
IL(14)
IN(9)
KY(13)
TN (14)
MS(8)
AL(9)
GA(12)
FL(49)
SC(7)
NC(13)
VA(17)
OH(34)
WV(4)
PA(48)
NY(40)
MD (13)
ME(1)
VT (1)
NH (2)
NJ (14)
MA (14)
CT (9)
DE (3)
RI (0)
DC (4)
Active sites = 43056,400 Patients
CRUSADE Site Distribution

Hospital PresentationCharacteristics in CRUSADEHospital PresentationCharacteristics in CRUSADE
Qualifying CriteriaQualifying CriteriaST-segment depressionST-segment depression 39% 39%Transient ST-segment elevationTransient ST-segment elevation 11% 11%Positive cardiac markersPositive cardiac markers 88% 88%
Baseline cardiac markersBaseline cardiac markers DrawnDrawnPositivePositive
CK-MBCK-MB 85%85%35%35%TnT/TnITnT/TnI 97%97%84%84%
Bedside assaysBedside assays CK-MBCK-MB 9%9%TroponinTroponin 11%11%
Qualifying CriteriaQualifying CriteriaST-segment depressionST-segment depression 39% 39%Transient ST-segment elevationTransient ST-segment elevation 11% 11%Positive cardiac markersPositive cardiac markers 88% 88%
Baseline cardiac markersBaseline cardiac markers DrawnDrawnPositivePositive
CK-MBCK-MB 85%85%35%35%TnT/TnITnT/TnI 97%97%84%84%
Bedside assaysBedside assays CK-MBCK-MB 9%9%TroponinTroponin 11%11%

Baseline Characteristics:CRUSADE vs. ACS Clinical TrialsBaseline Characteristics:CRUSADE vs. ACS Clinical Trials
Variable PURSUITPURSUIT PRISM-PLUSPRISM-PLUS GUSTO-IV ACSGUSTO-IV ACS CRUSADECRUSADE(n = 9461) (n = 1915) (n = 7800) (n =
41,267)
Mean age ± SD (yrs) 63 ± 11 63 ± 12 65 ± 11 68 ± 13
Female sex (%) 36 32 38 40
Diabetes mellitus (%) 23 23 22 33
Prior MI (%) 32 43 31 31
Prior CHF (%) 11 10 8 17
Prior PCI (%) 13 10 10 21
Prior CABG (%) 12 15 8 20
ST depression (%) 50 58 80 39
Variable PURSUITPURSUIT PRISM-PLUSPRISM-PLUS GUSTO-IV ACSGUSTO-IV ACS CRUSADECRUSADE(n = 9461) (n = 1915) (n = 7800) (n =
41,267)
Mean age ± SD (yrs) 63 ± 11 63 ± 12 65 ± 11 68 ± 13
Female sex (%) 36 32 38 40
Diabetes mellitus (%) 23 23 22 33
Prior MI (%) 32 43 31 31
Prior CHF (%) 11 10 8 17
Prior PCI (%) 13 10 10 21
Prior CABG (%) 12 15 8 20
ST depression (%) 50 58 80 39
NEJM, 1998 NEJM, 1998 Lancet, 2001Lancet, 2001NEJM, 1998 NEJM, 1998 Lancet, 2001Lancet, 2001

CRUSADE vs. ACS Clinical Trials:Early Mortality RatesCRUSADE vs. ACS Clinical Trials:Early Mortality Rates
0
1
2
3
4
5
6
0
1
2
3
4
5
6
PURSUIT PURSUIT (n = 9,461)(n = 9,461)
PRISM-PLUSPRISM-PLUS(n = 1,915)(n = 1,915)
GUSTO IV-GUSTO IV-ACSACS
(n = 7,800)(n = 7,800)
CRUSADE CRUSADE (n = 41,267)(n = 41,267)
1.8%1.8% 1.9%1.9% 1.8%1.8%
4.7%4.7%
7-day mortality rate7-day mortality rate
In-hospital mortality rate
In-hospital mortality rate
NEJM, 1998 NEJM, 1998 Lancet, 2001Lancet, 2001NEJM, 1998 NEJM, 1998 Lancet, 2001Lancet, 2001

Goal for CRUSADE: Improve Adherence to ACC/AHA Guidelines
Goal for CRUSADE: Improve Adherence to ACC/AHA Guidelines
Aspirin Clopidogrel
Beta Blocker
Heparin (UFH or LMWH)
GP IIb-IIIa Inhibitor All receiving PCI
Aspirin Clopidogrel
Beta Blocker
Heparin (UFH or LMWH)
GP IIb-IIIa Inhibitor All receiving PCI
Aspirin
Clopidogrel
Beta Blocker
ACE Inhibitor
Statin/Lipid Lowering
Smoking Cessation
Cardiac Rehabilitation
Aspirin
Clopidogrel
Beta Blocker
ACE Inhibitor
Statin/Lipid Lowering
Smoking Cessation
Cardiac Rehabilitation
Acute TherapiesAcute TherapiesAcute TherapiesAcute Therapies Discharge TherapiesDischarge TherapiesDischarge TherapiesDischarge Therapies
Circulation, JACC 2002 - ACC/AHA Guidelines updateCirculation, JACC 2002 - ACC/AHA Guidelines updateCirculation, JACC 2002 - ACC/AHA Guidelines updateCirculation, JACC 2002 - ACC/AHA Guidelines update

Acute Medication Use(within 1st 24 hours)
Acute Medication Use(within 1st 24 hours)
94%94%94%94%
79%79%79%79%
84%84%84%84%
36%36%36%36%
0%0%
20%20%
40%40%
60%60%
80%80%
100%100%
ASAASAASAASA BetaBetaBlockersBlockers
BetaBetaBlockersBlockers
HeparinHeparin(LMW + UFH)(LMW + UFH)
HeparinHeparin(LMW + UFH)(LMW + UFH)
GP IIb-IIIaGP IIb-IIIaInhibitorsInhibitorsGP IIb-IIIaGP IIb-IIIaInhibitorsInhibitors

95%86% 91%
50%
86%
65% 71%
21%
0%
20%
40%
60%
80%
100%
Aspirin < 24 hrs Beta Blocker < 24 Hrs
Heparin GP IIb-IIIaInhibitor
95%86% 91%
50%
86%
65% 71%
21%
0%
20%
40%
60%
80%
100%
Aspirin < 24 hrs Beta Blocker < 24 Hrs
Heparin GP IIb-IIIaInhibitor
Gap between Leading and Lagging Gap between Leading and Lagging Hospital Quartiles: Hospital Quartiles:
Acute CareAcute Care
Gap between Leading and Lagging Gap between Leading and Lagging Hospital Quartiles: Hospital Quartiles:
Acute CareAcute Care
Leading CentersLeading Centers Lagging CentersLagging Centers

Invasive Cardiac ProceduresInvasive Cardiac Procedures
62%62%62%62%
43%43%43%43%37%37%37%37%
23%23%23%23%
0%0%
15%15%
30%30%
45%45%
60%60%
75%75%
CathCathCathCath Cath < 48 hrCath < 48 hrCath < 48 hrCath < 48 hr PCIPCIPCIPCI CABGCABGCABGCABG
12%12%12%12%
PCI < 48 hrPCI < 48 hrPCI < 48 hrPCI < 48 hr
Median TimesMedian Times
• Cath - 28 hrsCath - 28 hrs
• PCI - 26 hrsPCI - 26 hrs
• CABG - 71 hrsCABG - 71 hrs

Acute Therapies (< 24 hrs)Acute Therapies (< 24 hrs)by Peak Troponin Levelby Peak Troponin LevelAcute Therapies (< 24 hrs)Acute Therapies (< 24 hrs)by Peak Troponin Levelby Peak Troponin Level
00
1010
2020
3030
4040
5050
6060
7070
8080
9090
100100 Tn 0-1 xULNTn 0-1 xULN
Tn 1-2 xULNTn 1-2 xULN
Aspirin Aspirin BB-Blockers-Blockers Heparin GP IIb/IIIa Clopidogrel Heparin GP IIb/IIIa Clopidogrel(UFH + LMWH)(UFH + LMWH)
Aspirin Aspirin BB-Blockers-Blockers Heparin GP IIb/IIIa Clopidogrel Heparin GP IIb/IIIa Clopidogrel(UFH + LMWH)(UFH + LMWH)
Tn 2-5 xULNTn 2-5 xULN
Tn > 5 xULNTn > 5 xULN
P < 0.001P < 0.001P < 0.001P < 0.001 P < 0.001P < 0.001P < 0.001P < 0.001 P < 0.001P < 0.001P < 0.001P < 0.001 P < 0.001P < 0.001P < 0.001P < 0.001 P < 0.001P < 0.001P < 0.001P < 0.001
Roe, ACC 2003Roe, ACC 2003

Use of Invasive Procedures by Peak Use of Invasive Procedures by Peak Troponin LevelTroponin LevelUse of Invasive Procedures by Peak Use of Invasive Procedures by Peak Troponin LevelTroponin Level
CathCath
PCIPCI
0
10
20
30
40
50
60
70
80
0-1 xULN 1-2 xULN 2-5 xULN > 5 xULN
Peak Troponin Ratio
%%%%
CABGCABGRoe, ACC 2003Roe, ACC 2003

Peak Tn Ratio
1-2 X ULN
2-5 X ULN
> 5 X ULN
Peak Tn Ratio
1-2 X ULN
2-5 X ULN
> 5 X ULN
NormalNormal
11 1.51.5 2.02.0 2.52.5
Adjusted Risk of In-Hospital Mortality by Peak Troponin Level
Adjusted Risk of In-Hospital Mortality by Peak Troponin Level
P = 0.03
P = 0.02
P < 0.001
P = 0.03
P = 0.02
P < 0.001
Roe, ACC 2003Roe, ACC 2003

Discharge Medication UseDischarge Medication Use
LVEF < 40%, CHF, DM, HTNLVEF < 40%, CHF, DM, HTN
# Known hyperlipidemia, # Known hyperlipidemia, TC, TC, LDLLDL
90%90% 83%83%
0%0%
20%20%
40%40%
60%60%
80%80%
100%100%
ASAASA Beta Beta BlockersBlockers
ACE-ACE-Inhibitors*Inhibitors*
61%61%
Lipid-Lipid-LoweringLowering
AgentAgent##
79%79%
56%56%
ClopidogrelClopidogrel

Discharge InterventionsDischarge Interventions
59%59%59%59%
72%72%72%72%
42%42%42%42%
66%66%66%66%
0%0%
20%20%
40%40%
60%60%
80%80%
100%100%
Lipid Panel Lipid Panel DrawnDrawn
Lipid Panel Lipid Panel DrawnDrawn
DietaryDietaryCounselingCounseling
DietaryDietaryCounselingCounseling
Cardiac RehabCardiac RehabReferralReferral
Cardiac RehabCardiac RehabReferralReferral
Smoking Smoking Cessation Cessation CounselingCounseling
Smoking Smoking Cessation Cessation CounselingCounseling

Gap between Leading and Lagging Gap between Leading and Lagging Hospital Quartiles: Hospital Quartiles:
Discharge CareDischarge Care
Gap between Leading and Lagging Gap between Leading and Lagging Hospital Quartiles: Hospital Quartiles:
Discharge CareDischarge Care 94% 89%
68%
81%
60%
82%
69%
49%
64%
36%
0%
20%
40%
60%
80%
100%
Aspirin Beta-blocker Ace Inhibitor*
Statin Clopidogrel
94% 89%
68%
81%
60%
82%
69%
49%
64%
36%
0%
20%
40%
60%
80%
100%
Aspirin Beta-blocker Ace Inhibitor*
Statin Clopidogrel
* LVEF < 40%* LVEF < 40%# Known hyperlipidemia# Known hyperlipidemia* LVEF < 40%* LVEF < 40%# Known hyperlipidemia# Known hyperlipidemia
##
Leading CentersLeading Centers Lagging CentersLagging Centers

0009COR0009COR3232
Paradoxical Care:Failing to Treat High Risk ACS
Paradoxical Care:Failing to Treat High Risk ACS

Risk of ACS in Elderly*Risk of ACS in Elderly*
2.8
67.4
8.5
13.3
16.1
02468
1012141618
Death Death/MI CHF
<75 Years >75 Years
* Kulkarni S et al ACC 2003 CRUSADE Presentation

Medical Therapy in the Elderly Medical Therapy in the Elderly
<75 yrs ≥75 yrs Adj. OR (95%CI)**
AcuteAspirin 92 88* 0.91 (0.83, 1.00)
Beta-Blocker 79 75* 0.91 (0.84, 0.99)Clopidogrel 41 32* 0.82 (0.76, 0.88)
Gp 2b3a 41 22* 0.64 (0.59, 0.69)
Cath (<48 hrs) 46 16* 0.51 (0.42-0.59)
PCI (≤ 48hrs) 32 14* 0.60 (0.55, 0.66)
* Unadjusted p<0.05 ** Comparison of age ≥75 with <75 yrs. Adjusted for gender, race, comorbidity, cardiac markers, insurance status, hospital features, and clustering effects (#elderly treated, similar outcomes).
<75 yrs ≥75 yrs Adj. OR (95%CI)**
AcuteAspirin 92 88* 0.91 (0.83, 1.00)
Beta-Blocker 79 75* 0.91 (0.84, 0.99)Clopidogrel 41 32* 0.82 (0.76, 0.88)
Gp 2b3a 41 22* 0.64 (0.59, 0.69)
Cath (<48 hrs) 46 16* 0.51 (0.42-0.59)
PCI (≤ 48hrs) 32 14* 0.60 (0.55, 0.66)
* Unadjusted p<0.05 ** Comparison of age ≥75 with <75 yrs. Adjusted for gender, race, comorbidity, cardiac markers, insurance status, hospital features, and clustering effects (#elderly treated, similar outcomes).

Acute Risks and Treatment of ACS in Women
Acute Risks and Treatment of ACS in Women
49
323837
20
29
0
10
20
30
40
50
60
Cath<48 PCI <48 GP IIbIIIa<24
Men Women
2003 4th Quarter CRUSADE
4.3
7.1
8.8
5.6
8.6
12.1
0
2
4
6
8
10
12
14
Death Death/MI CHF
Men Women
Risks Treatment

Acute Risks and Treatment of ACS in Diabetes*Acute Risks and Treatment of ACS in Diabetes*
4.3
7.28.5
5.7
8.6
13.8
0
2
4
6
8
10
12
14
16
Death Death/MI CHF
Non-DM DM
* CRUSADE 4th Quarter
49
30
49
39
20
39
0
10
20
30
40
50
60
Cath<48 PCI <48 GP IIbIIIa<24
No DM DM
TreatmentRisks

Acute Treatment of CHFAcute Treatment of CHF
52
30
48
25
11
32
0
10
20
30
40
50
60
Cath<48 PCI <48 GP IIbIIIa<24
No CHF CHF2003 4th Quarter CRUSADE
3.1
5.7
10.6
14.7
0
2
4
6
8
10
12
14
16
Death Death/MI
No CHF CHF
TreatmentRisks

If the guidelines are implemented, Do outcomes improved?
If the guidelines are implemented, Do outcomes improved?

0
1
2
3
4
5
6
7
<65% 65-75% 75-80% >80%
Hospital Composite Adherence Quartiles
In-h
osp
ital
Mo
rtal
ity
(%)
Performance Matters!Relationship between Process and Outcome
Performance Matters!Relationship between Process and Outcome
5.95.9
5.05.04.64.6
3.63.6
Peterson ED 2002 AHA
Peterson ED 2002 AHA

0009COR0009COR4040
Can We Improve Care?Can We Improve Care?

Quality Improvement Interventions:Quality Improvement Interventions:Site Predictors of SuccessSite Predictors of Success
Quality Improvement Interventions:Quality Improvement Interventions:Site Predictors of SuccessSite Predictors of Success
Strong clinician “champions” Strong clinician “champions”
Administrative support for CQIAdministrative support for CQI
Shared targets for improvementShared targets for improvement
High-quality data feedbackHigh-quality data feedback
Strong clinician “champions” Strong clinician “champions”
Administrative support for CQIAdministrative support for CQI
Shared targets for improvementShared targets for improvement
High-quality data feedbackHigh-quality data feedback
Bradley E, JAMA 2001 - Use of Beta-Blockers Post-MIBradley E, JAMA 2001 - Use of Beta-Blockers Post-MIBradley E, JAMA 2001 - Use of Beta-Blockers Post-MIBradley E, JAMA 2001 - Use of Beta-Blockers Post-MI

Practical Steps to Improve the Use of Evidence-Practical Steps to Improve the Use of Evidence-Based Therapies for Non-ST Based Therapies for Non-ST ACS ACS
Practical Steps to Improve the Use of Evidence-Practical Steps to Improve the Use of Evidence-Based Therapies for Non-ST Based Therapies for Non-ST ACS ACS
Identify local Cardiology and ED physician championsIdentify local Cardiology and ED physician champions
Secure institutional commitment to improved pt careSecure institutional commitment to improved pt care
Develop educational materials to improve Develop educational materials to improve allall physicians’ physicians’ knowledge of the ACC/AHA guidelinesknowledge of the ACC/AHA guidelines
Track adherence to ACC/AHA recommendationsTrack adherence to ACC/AHA recommendations Identify areas for QI Identify areas for QI
Provide standard QI toolsProvide standard QI tools
Give ongoing quarterly feedbackGive ongoing quarterly feedback
Identify local Cardiology and ED physician championsIdentify local Cardiology and ED physician champions
Secure institutional commitment to improved pt careSecure institutional commitment to improved pt care
Develop educational materials to improve Develop educational materials to improve allall physicians’ physicians’ knowledge of the ACC/AHA guidelinesknowledge of the ACC/AHA guidelines
Track adherence to ACC/AHA recommendationsTrack adherence to ACC/AHA recommendations Identify areas for QI Identify areas for QI
Provide standard QI toolsProvide standard QI tools
Give ongoing quarterly feedbackGive ongoing quarterly feedback

Trends in Acute Therapy AdherenceTrends in Acute Therapy Adherence
0%
25%
50%
75%
100%
Antiplatelet Beta Blocker Heparin GP IIb- IIIaInhibitor
Q1 Q2 Q3 Q4
0%
25%
50%
75%
100%
Antiplatelet Beta Blocker Heparin GP IIb- IIIaInhibitor
Q1 Q2 Q3 Q4

Trends in Discharge Therapy AdherenceTrends in Discharge Therapy Adherence
0%
25%
50%
75%
100%
Aspirin Clopidogrel Beta blocker ACE Inhibitor Lipid-loweringAgent
Q1 Q2 Q3 Q4
0%
25%
50%
75%
100%
Aspirin Clopidogrel Beta blocker ACE Inhibitor Lipid-loweringAgent
Q1 Q2 Q3 Q4

Trends in Discharge Recommendations Trends in Discharge Recommendations AdherenceAdherence
25%
50%
75%
100%
Smoking CessationCounseling
Dietary Modification Cardiac RehabilitationReferral
Q1 Q2 Q3 Q4

Conclusions: Quality ACS CareConclusions: Quality ACS Care
Clinicians need to rapidly assess pt risk Risk factors + markers
Pts at highest risk tend to benefit from most aggressive interventions
However, current ACS care demonstrates: Wide variability between leading and lagging centers Paradoxical care
Given tight links between care and outcome We need to work together develop successful ACS
quality improvement efforts
Clinicians need to rapidly assess pt risk Risk factors + markers
Pts at highest risk tend to benefit from most aggressive interventions
However, current ACS care demonstrates: Wide variability between leading and lagging centers Paradoxical care
Given tight links between care and outcome We need to work together develop successful ACS
quality improvement efforts

How to Take This Home…How to Take This Home…
Look critically at your data Identify targets
Look at your system
Learn from your neighbors
Make practical, actionable plans
Follow-up
Never be satisfied
Look critically at your data Identify targets
Look at your system
Learn from your neighbors
Make practical, actionable plans
Follow-up
Never be satisfied