Embed Size (px)
Citation preview

ABSTRACT
Fractures of the distal femur account for 7% of all femoral fractures, whether
supracondylar or intercondylar have been historically difficult to treat because of their
unstable nature and degree of comminution. The proximity of these fractures to knee
joint further makes full range of motion and function difficult. The incidence of
malunion, nonunion, and infection is also high. Anatomical reduction of the articular
surface, restoration of limb alingement, and early mobilization have shown to be
effective ways of managing most distal femoral fractures
INTRODUCTION
Distal femoral fractures are much less common than hip fractures and account for
7% of all femoral fractures. If the fractures around hip are excluded, 31% femoral
1

fractures involve distal portion . Studies done in 1960’s (Neer et al., 1967)
documented better outcomes for patients treated non-operatively. However,
complications of non-operative treatment included angular deformity, joint
incongruity, knee stiffness and delayed patient mobilization. Associated complications
of prolonged immobilization and increased hospital stay also limit their utility.
Anatomical reduction of the articular surface, restoration of limb alingement, and early
mobilization have shown to be effective ways of managing most distal femoral
fractures. Despite the advances in techniques and the improvement in surgical
implants, treatment of distal femoral fractures remained a challenge. Long term
disability can occur in patients with extensive articular cartilage damage, marked bone
comminution and severe soft tissue injury (Schatzker et al., 1998). Osteoarthritis may
occur if intra-articular step is 3 mm or more.
Dissatisfied with these results surgeons started looking for newer ways to reduce
fractures under direct vision and, fix and stabilize them with various implants.
These devices were helpful in following aims:-
Restoration of bony continuity
Maintenance of good reduction
Restoration of articular congruity
Restoration of joint movements
The methods used earlier for stabilization of distal femoral fractures were:-
2

Closed reduction and casting
Skeletal traction alone
Angled blade plate (Schatzker et al., 1979)
Rush rods (Shelbourne et al., 1982)
Enders nail (Kolmert et al., 1986)
Zickle device (Zickle et al., 1986)
However all these devices were technically demanding and did not achieve rigid
fixation of articular surface and good purchase of osteopenic bone.
Some of the devices still used for the treatment of distal femoral fractures are-
Dynamic condylar screw (Institut Straumann AG, Waldenberg, Switzerland)
GSH (Green Seligson Henry) nail.
Dynamic condylar screw can only be used when atleast 4 cms of area above the
intercondylar notch is uncommunited.
GSH nail is a retrograde nail. Its entry point is from the lower intra-articular
surface of femur. Its carries the problem of septic arthritis of knee joint and if not
counter sunk properly causes chronic irritation and late osteoarthritis of knee joint.
However, as the complexity of fractures needing treatment has changed from
simple extra-articular Supracondylar types to intercondylar and metaphyseal
communited types, these implants may not be ideal.
3
External fixation with devices such as the hybrid fixator and the Ilizarov external
fixator are excellent treatment of communited fractures associated with bone loss. In
addition to maintaining reduction whilst awaiting union, these devices also can be used
to lengthen the bone. However, pin tract infections and joint contractures are common
complications of these techniques.
Double plating has been advocated in the treatment of comminuted intercondylar
types. But with double plating there is often extensive soft tissue stripping on both
sides of femur, resulting in reduced blood supply, delayed or non union and failure of
implants.
With the development of improved internal fixation devices by AO
(Arbeitgemeinschaft fur Osteosynthesefragen) group treatment of Supracondylar and
intercondylar fractures of femur began to change after 1980 and so did the outcome of
management of these fractures (81% had good functional results with open reduction
and internal fixation with plate and screws as reported by Healy and Brooker, 1983
where as only 35% of cases treated with closed methods had good results).
Mode of trauma in distal femoral fractures is usually severe varus, valgus or
rotational force with axial loading sustained in young as a result of high energy trauma
as in road traffic accidents and in elderly as a result of minor slip or fall on a flexed
knee.
4
After fracture the deformities observed are usually those of femoral shortening,
apex posterior angulation and posterior displacement of the distal fragment. Varus
deformity may result because of pull of adductor muscles. If an intercondylar fracture
is present there will be rotational misalignment because of separate attachments of
gastronemius muscle to each condyle.
Complications of distal femoral fractures include malunion, non union, varus
angulation, limb length discrepancy, infections, and secondary osteoarthritis of
patellofemoral and tibio femoral joints. Implant failure, periprosthetic fractures,
disruption of fixation can also occur with any device used for internal fixation
especially in communited varieties and in elderly because of osteoporosis.
The fracture of this area means the fracture of cancellous bone and the region is
supplied by abundant blood supply provided by numerous muscle attachments in this
area. The fracture usually stabilizes within 8 weeks and allows weight bearing after 12
weeks. However, varus deformity, joint incongruency and limb length discrepancy
results in short leg gait, a limp, pain and future osteoarthritis.
As already stated various treatment modalities have been recommended, each
having their pearls and pitfalls. The Dynamic condylar screw as designed and
recommended by AO (Institut strauman AG, walden berg, switzerland is an impressive
method of treatment of these structures with following advantages .
Active knee joint motion can be started on the first post operation day.5

Full range of movements is preserved
Stable internal fixation does not allow maluion to occur.
Maintenance of joint congruity is there.
Duration of hospital stay is shortened.
Time taken for union is shortened.
Lag screw provides good purchase in ostopaenic bones as well.
Disadvantages of dynamic condylar screw are.
Dynamic condylar screw can only be used when atleast 4 cms of area
above the intercondylar notch is uncommunited.
For insertion of dynamic screw a large amount of bone stock has to be
removed.
A newer implant distal femoral-locking compression plate has been designed by
A.O. (Institut Straumann AG, Waldernberg, Switzerland) to overcome many of the
pitfalls of earlier implants. It allows higher elastic deformation than the other systems
putting between rigid fixation and intramedullary nailing. It is devised to provide an
implant that combines biologically friendly minimally invasive submuscular plate
placement with screws that lock into the plate to create fixed angle contact. The plate
is anatomically precontured to match lateral side of femur. Several biomechanical
6
studies showed its superiority against conventional plating. The locking compression
plate mechanism is more justified in:-
a) Metaphyseal areas
b) Comminuted fractures
c) Osteoporotic bones
d) Periprosthetic fractures (Ezekiel Tan and Balogh, 2009)
The use of angled devices such as the condylar blade plate and dynamic condylar
screw (DCS) require a certain amount of bone stock present, which limits their use in
some types of fractures. Because of this appalling state of affairs we decided to
undertake a study of internal fixation of distal femoral fractures with distal femoral
locking compression plate considering that it will provide better stability and
functional outcome. The angular stability makes it ideal for communited fractures. The
locking plate is slid extraperiosteally without much dissection thus reducing the
operation time and beeding which is advantageous.It has the potency to reduce
infection rate, better stability in intra-articular fractures and fractures in elderly.
Following are the advantages-
Active range of motion can be started on first postoperative day.
Maximum range of motion is preserved
Stable internal fixation does not allow mal union to occur.
Incidence of implant failure is less.
7
Maintenance of joint congruity.
Locking screws forms fixed angle construct with plate, therefore screw
cutout rate is less
Duration of hospital stay shortened hence the cost.
CLASSIFICATION OF DISTAL FEMORAL FRACTURES A.O. (Muller et al.,
1950)
The A.O. classification gives code no. 33 to the distal femur.
(A) Distal femur: extra-articular
A1 Extra-articular fracture: simple
1. Apophyseal
2. Metaphyseal oblique or spiral
3. Metaphyseal transverse
A2 Extraarticular fracture: metaphyseal wedge
1. Intact
2. Fragmented, lateral
3. Fragmented, medial
A3 Extra-articular fracture: metaphyseal complex
1. With an intermediate split fragment
2. Irregular, limited to metaphysis
3. Irregular, extending to diaphysis
8

(B) Partial articular fracture
B1 Partial articular fracture, lateral condyle, saggital
1. Simple through the notch
2. Simple through the load bearing surface
3. Multifragmentary
B2 Partial articular fracture, medial condyle saggital
1. Simple through notch
2. Simple through load bearing surface
3. Multifragmentary.
B3 Partial articular fracture, frontal
1. Anterior and lateral flake fractures
2. Unicondylar posterior (HOFFA)
3. Bicondylar posterior
(C) Complete articular fractures
C1 Complete articular fracture: articular
simple, metaphyseal simple
1. T or Y shaped, with slight displacement
2. T or Y shaped, with marked displacement
3. T shaped epiphyseal
C2 Complete articular fracture: articular simple, metaphyseal,
multifragmentary
9
1. With intact wedge
2. With a fragmented wedge
3. Complex
C3 Complete articular fracture, multifragmentary
1. Metaphyseal simple
2. Metaphyseal multifragmentary
3. Metaphyseodiaphyseal, multifragmentary
ANATOMY
The lower end of the femur is larger than the upper, is somewhat cuboid in form, but
its transverse diameter is greater than its antero-posterior. It consists of two oblong
eminences known as the condyles. In front, the condyles are but slightly prominent,
and are separated from one another by a smooth shallow articular depression called the
patellar surface; behind, they project considerably, and the interval between them
forms a deep notch, the intercondyloid fossa. The lateral condyle is the more
prominent and is the broader both in its antero-posterior and transverse diameters, the
medial condyle is the longer and projects to a lower level. The condyles are not
quite parallel with one another. The long axis of the lateral is almost directly antero-
posterior, but that of the medial runs backward and medialward. Their opposed
surfaces are small, rough, and concave, and form the walls of the intercondyloid fossa.
This fossa is limited above by a ridge, the intercondyloid line, and below by the central
part of the posterior margin of the patellar surface. The posterior cruciate ligament of
10

the knee-joint is attached to the lower and front part of the medial wall of the fossa and
the anterior cruciate ligament to an impression on the upper and back part of its lateral
wall.
Each condyle is surmounted by an elevation, the epicondyle. The medial
epicondyle is a large convex eminence to which the tibial collateral ligament of the
knee-joint is attached. At its upper part is the adductor tubercle, already referred to,
and behind it is a rough impression which gives origin to the medial head of the
Gastrocnemius. The lateral epicondyle, smaller and less prominent than the medial,
gives attachment to the fibular collateral ligament of the knee-joint.
Directly below lateral epicondyle is a small depression from which a smooth well-
marked groove curves obliquely upward and backward to the posterior extremity of
the condyle. This groove is separated from the articular surface of the condyle by a
prominent lip across which a second, shallower groove runs vertically downward from
the depression. In the fresh state these grooves are covered with cartilage. The
Popliteus arises from the depression; its tendon lies in the oblique groove when the
knee is flexed and in the vertical groove when the knee is extended.
Above and behind the lateral epicondyle is an area for the origin of the lateral head
of the Gastrocnemius, above and to the medial side of which the Plantaris arises.
The articular surface of the lower end of the femur occupies the anterior, inferior, and
posterior surfaces of the condyles. Its front part is named the patellar surface and
11

articulates with the patella. It presents a median groove which extends downward to
the intercondyloid fossa and two convexities, the lateral of which is broader, more
prominent, and extends farther upward than the medial.
The lower and posterior parts of the articular surface constitute the tibial surfaces for
articulation with the corresponding condyles of the tibia and menisci. These surfaces
are separated from one another by the intercondyloid fossa and from the patellar
surface by faint grooves which extend obliquely across the condyles. The lateral
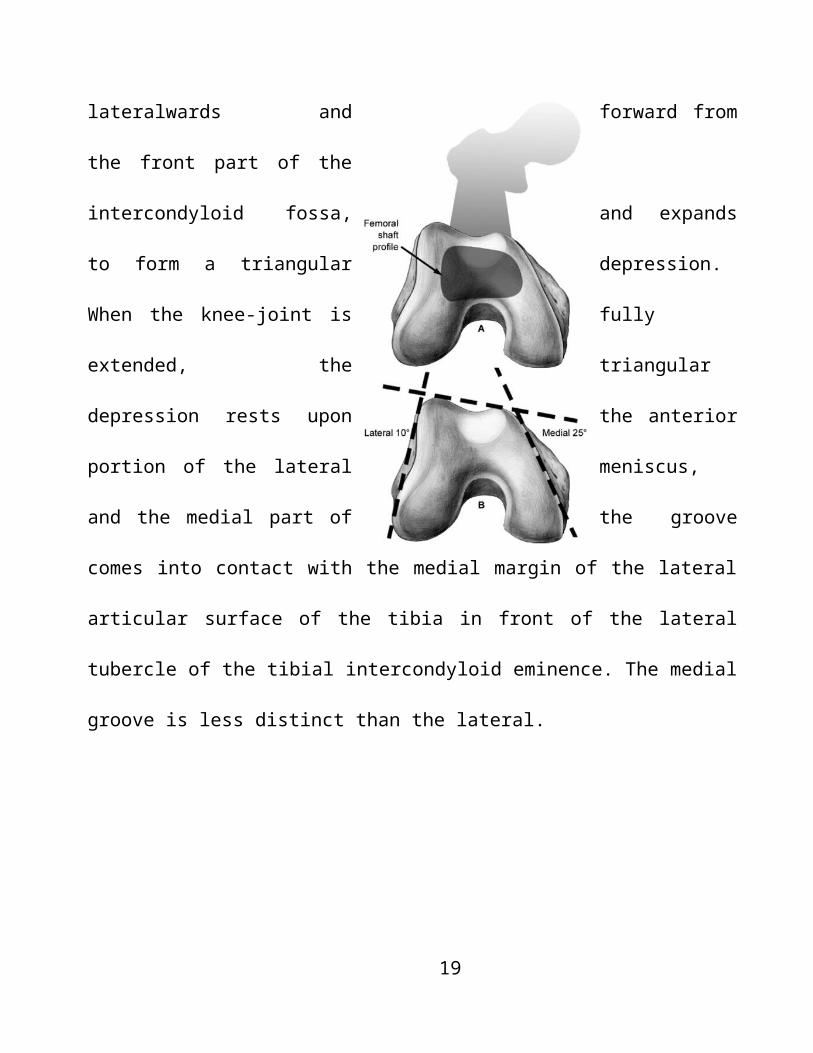
groove is the better marked; it runs lateralwards and forward from the front part of the
intercondyloid fossa, and expands to form a triangular depression. When the knee-joint
is fully extended, the triangular depression rests upon the anterior portion of the lateral
meniscus, and the medial part of the groove comes into contact with the medial margin
of the lateral articular surface of the tibia in front of the lateral tubercle of the tibial
intercondyloid eminence. The medial groove is less distinct than the lateral.
12
Curtsey: www.chestofbooks.com
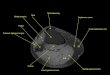
The distal femoral anatomy as it relates to plate applications: The lateral
metaphysis is angulated 10 degrees from the sagittal plane; the medial metaphysis is
angulated 25 degrees from the sagittal plane. To avoid a medial translational deformity
of the articular surface, lateral plate applications should follow the sloped, lateral,
metaphyseal surface. To ensure that screws are contained within the distal femur, the
anterior location of the metaphysis must be appreciated. Anterior implants are shorter
than those angulated or placed more posteriorly.
13
It does not reach as far as the intercondyloid fossa and therefore exists only on the
medial part of the condyle; it receives the anterior edge of the medial meniscus when
the knee-joint is extended. Where the groove ceases laterally the patellar surface is
seen to be continued backward as a semilunar area close to the anterior part of the
intercondyloid fossa; this semilunar area articulates with the medial vertical facet of
the patella in forced flexion of the knee-joint. The tibial surfaces of the condyles are
convex from side to side and from before backward. Each presents a double curve, its
posterior segment being an arc of a circle, its anterior, part of a cycloid.
Muscles attachments on the distal femur and their clinical relevance-
The anterior muscles of thigh are the Sartorius, the quadriceps muscle comprising of 4
muscles namely rectus remoris, vastus lateralis, medialis and intermedius. Articularis
genu is attached to the distal femur on the anterior surface.
The Sartorius, the longest muscle in the body, is narrow and ribbon-like; it arises by
tendinous fibers from the anterior superior iliac spine and the upper half of the notch
below it. It is inserted, in front of the Gracilis and Semitendinous, into the upper part of
the medial surface of the body of the tibia, nearly as far forward as the anterior crest.
The Quadriceps femoris (Quadriceps extensor) includes the four remaining muscles
on the front of the thigh. The Rectus femoris is situated in the middle of the front of the
thigh. It arises by two tendons: one, the anterior or straight, from the anterior inferior iliac
spine; the other, the posterior or reflected, from a groove above the brim of the
14

acetabulum. It is inserted into the base of the patella. The Vastus lateralis (Vastus
externus) is the largest part of the Quadriceps femoris. It arises by a broad aponeurosis,
which is attached to the upper part of the intertrochanteric line, to the anterior and inferior
borders of the greater trochanter, to the lateral lip of the gluteal tuberosity, and to the
upper half of the lateral lip of the linea aspera; this aponeurosis covers the upper three-
fourths of the muscle, and from its deep surface many fibers take origin. It is inserted into
the lateral border of patella.
The Vastus medialis (Vastus internus) arises from the lower half of the
intertrochanteric line, the medial lip of the linea aspera, the upper part of the medial
supracondylar line, the tendons of the Adductor longus and the Adductor magnus and
the medial intermuscular septum. It is inserted into the medial border of the patella
and the Quadriceps femoris tendon.
The Vastus intermedius (Crureus) arises from the front and lateral surfaces of the
body of the femur in its upper two-thirds and from the lower part of the lateral
intermuscular septum. Its fibers end in a superficial aponeurosis, which forms the deep
part of the Quadriceps femoris tendon.
The Articularis genu (Subcrureus) is a small muscle. It arises from the anterior
surface of the lower part of the body of the femur, and is inserted into the upper part of
the synovial membrane of the knee-joint.
They are all supplied by 2nd, 3rd and 4th lumbar nerves through femoral nerve.
15

Actions.—The Sartorius flexes the leg upon the thigh, and, continuing to act, flexes the
thigh upon the pelvis; it next abducts and rotates the thigh outward.
The Quadriceps femoris extends the leg upon the thigh. The Rectus femoris assists the
Psoas major and Iliacus in supporting the pelvis and trunk upon the femur. It also assists
in flexing the thigh on the pelvis. The Vastus medialis draws the patella medialward as
well as upward.
The medial thigh muscles consist of Gracilis, adductor longus, magnus and brevis.
Pectineus is also attached to medial femur.
Nerves.—The three Adductores and the Gracilis are supplied by the third and fourth
lumbar nerves through the obturator nerve; the Adductor magnus receiving an additional
branch from the sacral plexus through the sciatic. The Pectineus is supplied by the second,
third, and fourth lumbar nerves through the femoral nerve, and by the third lumbar
through the accessory obturator when this latter exists.
Actions-In consequence of the obliquity of their insertions into the linea aspera, they
rotate the thigh outward, assisting the external rotators, and when the limb has been
abducted, they draw it medialward, carrying the thigh across that of the opposite side. The
Pectineus and Adductores brevis and longus assist the Psoas major and Iliacus in flexing
the thigh upon the pelvis. In progression, all these muscles assist in drawing forward the
lower limb. The Gracilis assists the Sartorius in flexing the leg and rotating it inward; it is
also an adductor of the thigh.
16
The posterior muscles of thigh are called hamstrings. They comprise of 3 muscles
namely Biceps Femoris, Semimembranous and Semitendenous.
Nerves.—The muscles of this region are supplied by the fourth and fifth lumbar and
the first, second, and third sacral nerves; the nerve to the short head of the Biceps
femoris is derived from the common peroneal, the other muscles are supplied through
the tibial nerve.
Actions.—The hamstring muscles flex the leg upon the thigh. When the knee is
semiflexed, the Biceps femoris in consequence of its oblique direction rotates the leg
slightly outward; and the Semitendinosus, and to a slight extent the
Semimembranosus, rotate the leg inward, assisting the Popliteus. Taking their fixed
point from below, these muscles serve to support the pelvis upon the head of the
femur, and to draw the trunk directly backward.
Muscles of the calf-
The Posterior Crural Muscles—The muscles of the back of the leg are subdivided into
two groups—superficial and deep. Those of the superficial group constitute a powerful
muscular mass, forming the calf of the leg. Their large size is one of the most
characteristic features of the muscular apparatus in man, and bears a direct relation to his
erect attitude and his mode of progression.
The superficial group consists of Gastronemius, Soleus and the Plantaris.
17
The Gastrocnemius is the most superficial muscle, and forms the greater part of the
calf. It arises by two heads, which are connected to the condyles of the femur by strong,
flat tendons. The medial and larger head takes its origin from a depression at the upper
and back part of the medial condyle and from the adjacent part of the femur. The lateral
head arises from an impression on the side of the lateral condyle and from the posterior
surface of the femur immediately above the lateral part of the condyle. The aponeurosis,
gradually contracting, unites with the tendon of the Soleus, and forms with it the tendo
calcaneus which is inserted into the calcaneus.
The Soleus is a broad flat muscle situated immediately in front of the Gastrocnemius.
It arises by tendinous fibers from the back of the head of the fibula, and from the upper
third of the posterior surface of the body of the bone; from the popliteal line, and the
middle third of the medial border of the tibia. The fibers end in an aponeurosis which
covers the posterior surface of the muscle, and, gradually becoming thicker and narrower,
joins with the tendon of the Gastrocnemius, and forms with it the tendo calcaneus.
Nerves.—The Gastrocnemius and Soleus are supplied by the first and second sacral
nerves and the Plantaris by the fourth and fifth lumbar and first sacral nerves, through the
tibial nerve.
Actions.—The muscles of the calf are the chief extensors of the foot at the ankle-joint
Ligaments attached on distal femur-
18
The femur and tibia are connected together by the following ligaments and soft
tissues:
The Articular Capsule, the anterior and posterior cruciate ligaments, tibial and fibular
collateral ligament, ligament patellae, the medial and lateral menisci, oblique popliteal
ligament, transverse and coronary ligament.
The ligamentum patellae is the central portion of the common tendon of the Quadriceps
femoris, which is continued from the patella to the tuberosity of the tibia. It is a strong,
flat, ligamentous band, about 8 cm. in length, attached above to the apex and adjoining
margins of the patella and the rough depression on its posterior surface; below to the
tuberosity of the tibia; its superficial fibers are continuous over the front of the patella
with those of the tendon of the Quadriceps femoris.
The tibial collateral ligament is a broad, flat, membranous band, situated nearer to
the back than to the front of the joint. It is attached above to the medial condyle of the
femur immediately below the adductor tubercle; below to the medial condyle and medial
surface of the body of the tibia.
The fibular collateral ligament is a strong, rounded, fibrous cord, attached above to
the back part of the lateral condyle of the femur, immediately above the groove for the
tendon of the Popliteus; below to the lateral side of the head of the fibula, in front of the
styloid process.
The Anterior Cruciate Ligament (ligamentum cruciatum anterius; external crucial
ligament) is attached to the depression in front of the intercondyloid eminence of the
19

tibia, being blended with the anterior extremity of the lateral meniscus; it passes upward,
backward, and lateralward, and is fixed into the medial and back part of the lateral
condyle of the femur.
The Posterior Cruciate Ligament (ligamentum cruciatum posterius; internal crucial
ligament) is stronger, but shorter and less oblique in its direction, than the anterior. It is
attached to the posterior intercondyloid fossa of the tibia, and to the posterior extremity of
the lateral meniscus; and passes upward, forward, and medialward, to be fixed into the
lateral and front part of the medial condyle of the femur.
The medial meniscus (meniscus medialis; internal semilunar fibro-cartilage) is
nearly semicircular in form, a little elongated from before backward, and broader behind
than in front; its anterior end, thin and pointed, is attached to the anterior intercondyloid
fossa of the tibia, in front of the anterior cruciate ligament; its posterior end is fixed to the
posterior intercondyloid fossa of the tibia, between the attachments of the lateral meniscus
and the posterior cruciate ligament.
The lateral meniscus (meniscus lateralis; external semilunar fibro-cartilage) is
nearly circular and covers a larger portion of the articular surface than the medial one. It is
grooved laterally for the tendon of the Popliteus, which separates it from the fibular
collateral ligament. Its anterior end is attached in front of the intercondyloid eminence of
the tibia, lateral to, and behind, the anterior cruciate ligament, with which it blends; the
posterior end is attached behind the intercondyloid eminence of the tibia and in front of
the posterior end of the medial meniscus.
20

The evolution of treatment of fractures has kept pace with evolution of human race and
its knowledge about various aspects of life through clinical sciences.
Review of literature in respect to the management of Supracondylar and
intercondylar fractures of femur shows that the different methods have their own pros
and cons. These methods have been modified from time to time, but no method has
been found to be satisfactory till date.
21

Tees et al (1937) discussed management of fractures of distal femur using skin
traction for reduction and immobilization.
Robert et al (1945) in their study of healing times of fracture shaft femur and tibia
reported average of 18 weeks of healing times for fracture distal 1/3 femur and that the
healing time depended on multiple factors like degree of comminution, compound or
simple , type of fracture, site of injury, age of patient and method of treatment.
Umansky et al (1948) gave description of technique of internal fixation of
Supracondylar fracture using blade plate.
Alfons and Shorkey (1949) reported good results in four fractures of distal third
femur treated by plate. They concluded that rigid internal fixation can be achieved and
early joint mobilization started.
Marcus et al. (1958) reviewed 172 cases of distal 1/3rd of femur and
recommended skeletal traction with two pins for at least 6 weeks and later on
immobilization in a Plaster of Paris (POP) cast. They recommended operative
treatment for simple condylar fragments with displacement.
Peter et al. (1958) reported treatment results of series of 36 patients of
Supracondylar and intercondylar fracture of femur using open reduction and internal
fixation using a Jewett Supracondylar nail (triflanged) which affords better fixation of
condyles of femur. Union was found to be good in all these cases and range of
22
movements were also good in all cases. Emphasis was put on early knee motion after
surgery.
Preston et al. (1959) found that Supracondylar fractures of femur are usually
sustained by aged females with markedly osteoporotic bones and resulted from minor
trauma usually. Unnatural leverage at the suracondylar area predisposing to knee joint
instability may also be a cause to the occurrence of these factors. Such patients cannot
stand long period of immobilization and operative techniques are behest with
complications. So meticulous operative treatment is required.
Carter and Rowe (1965) emphasized that the fractures of lower end of femur are
usually caused by severe violence and are accompanied by injuries to popliteal vessels
and nerves, intraarticular fractures or damage to epiphyseal plates in adults. They
recommended closed reduction and immobilization in 450 to 500 flexion at knee when
lower fragment remains with proximal fragment.
Marcus (1966) studied 442 patients over 20 years who had fracture of distal 1/3rd
of femur. They reported 54% good to excellent results of operative methods. They
recommended two pin traction using K-wires and a spreader. They advocated exercise
of thigh muscles which prevents adhesion of knee joints which is primary cause of
knee stiffness.
Stewart et al. (1966) from Campbell’s clinic retrospectively reviewed 213
supracondylar and intercondylar fractures of femur and reported satisfactory results in
23

67% of fractures of femur treated nonoperatively and 54% treated operatively.
Delayed union or nonunion occurred in 9.7% of fractures treated with closed methods
and 29% treated with open reduction and internal fixation. They recommended two pin
traction as the treatment of choice.
Neer et al. (1967) studied and compared closed treatment as well as open
reduction and internal fixation in their series of 110 patients and gave very poor final
results in 50% and condemned open reduction and internal fixation.
Austin et al. (1971) studied open reduction and internal fixation in supracondylar
and intercondylar fractures in elderly with a condylar blade plate. They found early
partial weight bearing can be started with this method.they attributed previous
disappointing results to poor methods of fixation.
Olerud (1972) obtained good results in 14 out of 15 cases treated with AO angled
blade plate in distal femoral fractures. Good results were attributed to stable
osteosynthesis that permitted early protected knee motion.
Richard et al. (1972) conducted a survey of preferred treatment of simple
Supracondylar fracture of femur. 702 out of 1000 board qualified orthopedic surgeons
preferred skeletal traction using tibial pin for 8 weeks and weight bearing at 13 weeks.
John et al. (1973) in their series of 30 patients of distal 1/3rd femur fractures
concluded that closed reduction with early ambulation in a cast brace are best suited
methods for fracture of distal part of femur and comminuted mid shaft fracture.
24

Ward law D et al (1973) investigated off loading characterstics of cast braces of
30 patients with fracture of the shaft of femur during axial loading using strain gause
transducers. It was concluded that close reduction and early mobilization in a cast
brace are best suited for fractures in the distal part of the femur and for communited
multifragmented fractures in the middle and proximal part of the shaft. Weight bearing
in the cast permitted controlled movements of the fragments and thus promoted
healing by the formation of periosteal callus.
Harlan et al. (1974) studied results of open reduction internal fixation with AO
950 angeled condylar plate. They concluded 72% of the patients treated with open
reduction internal fixation with blade plate had excellent to good results.
Schatzker et al. (1974) reviewed the results of treatment of Supra- condylar and
intercondylar fracture treated by Toronto Group of Surgeons who chiefly used AO
condylar blade plate. They concluded that 74% patients treated with condylar blade
plate had good or excellent results as compared with 32% good results obtained with
conservative methods. They also concluded that more comminuted the fracture and
more closer to the joint more the poorer results.
Robert and Zickel (1977) showed satisfactory results of open reduction and
internal fixation in 17 cases. Fixation was done with intramedullary internal device in
the form of two pre-bent rods which were inserted into the medullary canals through
25

medial and lateral condyles for fractures distal 1/3rd of femur. They found satisfactory
results.
Beal Jr (1979) treated 13 cases of non union of Supracondylar fractures of femur
with bone grafting and internal fixation with intramedullary nail driven across the knee
joint and obtained union in 10 out of 11 cases.
Baijal et al (1979) treated 13 cases of Supracondylar fracture femur by using
Wright knee plate and described the technique as bone suture rather than rigid internal
fixation. Reasonable good results were obtained by them.
Seinsheimer et al (1980) studied 47 cases of Supracondylar fractures of femur and
found Supracondylar fracture without intercondylar extension obtained better knee
movements when treated with traction followed by cast bracing. Patients with
intercondylar extension obtained better results when treated with internal fixation.
Meggit et al (1981) made a study of the biomechanics of load bearing in a series of
patients treated with a cast brace for fractures of the distal femur. They demonstrated
four biomechnical phases of the bony union which correlated well with the stages of
clinical healing. The clinical application of these results have led to improvements in
the design of the braces and the use of a cylindrical cast brace for fractures of the distal
half of the femoral shaft and of a new type of brace with a hinge at the hip attached to
the thigh cast for fractures of the proximal shaft.
26

Giles and Delee (1982) obtained good results in 26 cases of supracondylar
fractures treated by internal fixation using supracondylar plate and lag screw to
achieve 2 plane fixation.
Shelbourne found et al (1982) found 84%good results in 98 patients
Supracondylar/ intercondylar fractures of femur treated by insertion of rush pins.
Healy and Brooker (1983) compared operative treatment mainly with plate and
screws devices with non operative treatment in the fracture of distal femur and found
good results in 81% of fractures of femur treated operatively as compared to 35%
treated non operatively and recommended operative method for all fractures of distal
femur except simple non displaced fractures.
Halpenny and Rorabeck (1984) retrospectively reviewed 61 fracture of distal
femur non-operatively or with internal fixation with blade plate. In extraarticular
fractures results were better with operative treatment. In intraarticular fractures had
more unsatisfactory results overall, and results of operative and non –operative
treatment were equal. The authors stressed early mobilization of knee was important in
obtaining good results.
Kurt and Einer (1986) reviewed 36 cases of supracondylar fracture which
occurred after total knee arthroplasty. They found that such cases are better managed
by traction or application of cast or both.
27

Mize (1989) reported good or excellent results in 76% of 68 fractures of distal
femur treated with A.O. technique (most with blade plate). A lateral incision was
preferred, however 15 required extensile approach. Malunion occurred in 7.3%
fractures and incidence of infection was 4.4%. He emphasized the importance of bone
grafting defects in medial buttress to enhance healing and stability. Bone grafting was
done in 87% of cases and no non-union was reported.
Sanders et al (1989) reported good to excellent results in their series of parients
fractures of Supracondylar and intercondylar region of femur treated with dynamic
compression screw.
Rong Sen Yang et al (1990) studied 93 cases of supracondylar fracture of femur
treated with 950 angeled condylar blade plates. They showed 79% cases with excellent
results and advocated good results because of good selection of cases ans strict
adherence to principles of internal fixation.
Shewring et al (1992) in their series of 21 cases of suprcodylar and intercondylar
fractures of femur treated with AO dynamic compression screw concluded that it is an
effective and technically undemanding method of treating such fractures.
Radford et al (1992) gave similar results with the use of dynamic condylar screw
instead of condylar blade plate. They found that it was technically easier to use this
implant than condylar blade plate but its limitation was its use in osteoporotic bone.
28
Pemberton et al (1994) studied the use of carbon fibre Supracondylar plate in 22
patients of fracture distal femur. They reported that Supracondylar plate was
technically simpler to use and felt that it represented significant advantage over
existing inplants for this fracture type.
Firoozbakhsh et al. (1995) studied two common types of internal fixation of
supracondylar femur fractures. The retrograde intramedullary nail and 950 side plate
and screw in synthetic composite femur bones to determine the quantitative difference
in internal rigidity. They concluded that although the retrograde nail was less rigid in
other physiologically less critical modes of loading, it had rigidity comparable to that
of plate in varus loading.
Albert (1997) advocated that the successful management of the distal femoral
fractures was possible with adherence to the basic principle of anatomical reduction,
stable fixation and early mobilization. Closed management could achieve these goals
in selective patients, but most of supracondylar fractures were treated with operative
reconstruction. Implant selection was determined on the basis of characteristics of the
fracture, the bone quality, the needs of patient and the experience of surgeon. Surgical
options included the angled blade plate, compression screws, condylar buttress plates,
intramedullary plates, external fixation and modular distal femoral replacement.
David and Harrow (1997) compared initial stability of Green Seligson Henry
(GSH) nail and 950 condylar compression screw and side plate assembly (dynamic
29
condylar screw) for distal femoral fractures. They concluded that if a dynamic
condylar screw plate construct was selected with, a dispersed screw configuration,
including the most proximal hole in plate, provided superior stiffness in torsional
loading and equal stiffness in axial loading as compared with GSH nail construct. If a
GSH nail was selected, a grouped screw configuration which absorbed more energy
during axial loading as compared with DCS plate constructs and the nail dispersed
screw configuration was recommended.
Simonian et al (1998) studied the angular screw placement in lateral condylar
buttress plate for Supracondylar fractures. According to them certain Supracondylar
femoral fractures were not amenable to internal fixation with fixed angled devices. In
these instances, the condylar buttress plate was recommended as an alternative;
however this was a less rigid device with a screw placed diagonally across fracture
site, stiffness increased. This simple means of screw angulation in the plate
strengthened the overall construct to resist the tendency towerds varus deformity.the
attractive feature includes the ease of application , and the use of an existing construct.
Chapman and Finkemier (1999) studied the treatment of non-union femoral
fractures with plate fixation and bone graft.they concluded that rigid plate fixation and
autulogous bone grafting were an effective technique for the treatment of non unions
of the supracondular region of femur.
30

Henry (2000) studied the supracondylar femoral fractures treated percutaneously
with GSH nail. The study showed that the percutaneous treatment of supracondylar
fracture was possible and could decrease operative time, blood loss, and the need of
bone grafting.
Kregor et al (2001) studied the technique and early results of distal femoral-
locking compression plate (DF-LCP) in less invasive mode and emphasized the role of
soft tissue protection in increasing osseous healing and decreasing infections. He
emphasized on submuscular tunnel plating with least exposure of fracture site for
distal femoral fractures and named it as “internal” external fixator.
Foster (2006) reviewed the fixation methods used in distal femoral fractures using
950 angled blade plate, dynamic condylar screw (DCS), condylar buttress plate,
flexible nails, intramedullary nails, supracondylar nails, less invasive stabilization
system (LISS), external fixator and total knee replacement. He concluded that:- (i)
Locked plates may hold some biomechnical advantage over other methods; (ii) Angled
blade plate (ABP) and DCS behaved similarly for extra-articular fractures; (iii) DCS
performed better in intra-articular fractures; (iv) supracondylar nail is not as strong as
DCS or ABP; (v) LISS is better then ABP in axial loading and torsion; and (vi) LISS
is better than intramedullary (IM) nailing in torsion only.
Schandelmaier et al (2009) studied distal femoral fractures and stabilization in less
invasive mode and concluded the advantages of the LISS over conventional plating are
31
a shorter healing time and a reduced need for bone grafting. Compared with the
dynamic compression screw, the LISS represents an improvement of percutaneous
techniques. Clinical examples and mechanical investigations show a higher stability in
the treatment of osteoporotic bone. Performing an axial reduction is as difficult with
the LISS as with conventional percutaneous plates. Therefore, trauma with intra-
articular comminution and in osteoporotic patients. The Distal femoral nail should be
used for extra-articular and minimally displaced intra-articular fractures in younger
patients.
Ezekiel and Balogh (2009) gave the indications and limitations of locked plate.
Indications were: 1. Metaphyseal area. 2. Complex metaphyseal diaphyseal fractures
with communition. 3. Osteoporotic bones. 4. Periprosthetic fractures.
Limitations were- 1. Reduction cannot be achieved. 2. Not suitable in compound
fractures. 3. Expensive than conventional DCP. 4. More radiation exposure is required
in minimally invasive techniques.
Smith et al (2009) reviewed the evidence base assessing the early rehabilitation of
patients following LISS fixation for distal femoral fractures. Seventeen case series
assessing 508 patients with 535 fractures were reviewed. No clinical trials comparing
physiotherapy programmes were identified. The review identified that following LISS
fixation for distal femoral fractures, patients begin range-of-motion exercises
immediately and are initially required to restrict weight-bearing following surgery. It
32

remains unclear whether casts, braces or immobilization aids are applied during the
initial postoperative period. They concluded that the efficacy of different
physiotherapy protocols following LISS fixation for distal femoral fractures remains
unclear. Further well-designed randomised controlled trials are required to compare
different postoperative physiotherapy rehabilitation programmes for patients following
LISS fixation of distal femoral fractures in order to determine the optimal
postoperative management for this complex patient group.
Smith (2009) systematically reviewed to assess the literature evaluating the
clinical and radiological outcomes following less invasive stabilization system (LISS)
for distal femoral fractures. He studied Twenty-one studies assessing 663 patients with
694 fractures were reviewed. The findings suggest that the LISS system may be an
appropriate fixation method for the management of distal femoral fractures. However,
there remains a high incidence of loss of reduction (n = 134; 19%), delayed or non-
union (n = 40; 6%) and implant failure (n = 38; 5%). On analysis, such
complications were largely confined to articles published before 2005, therefore
during the infancy of the widespread clinical application of this trauma system. On
critical appraisal, the evidence-base remains limited by recruiting small, under-
powered sample sizes and poorly accounting for confounding variables such as
osteoporosis, diabetes, multi-trauma and fracture classification. He concluded that
further study is required to assess the outcomes of LISS fixation in specific patient
33
populations, and to compare the outcome of this fixation method to condylar plates
and intrameduallary devices, to determine the optimal management strategy for this
complex patient group.
Mongkon Luechoowong (2010) studied the clinical results of
the locking compression plate in treatment of complex distal femoral fracture. There
were 13 male and 6 female patients in this study. The mean age was 41.6±19.4 years
(13-78 years). Time to union was 12-38 weeks (median 17 weeks). Broken screw was
observed in one case caused from slipping. Replating was applied and the fracture was
union in 38 weeks with limited range of motion 0-70 degree. Infected wound was
identified in one case (opened fractures IIIC gustilo/C2 intercondylar), after repeated
debridement, infection was subsiding and bone union in 30 weeks. All fractures in this
study were union. There was no device failure in three osteoporotic patients.
Lujan et al (2010) stated that callus formation was inconsistent and irregular with
distal femoral locking plate. He concluded that Callus size varied from 0 to 650 mm2.
Deficient callus (20 mm2 or less) formed in 52%, 47%, and 37% of fractures at 6, 12,
and 24 weeks post surgery, respectively. Callus formation was asymmetric, whereby
the medial cortex had on average 64% more callus (P = 0.001) than the anterior or
posterior cortices. A longer bridge span correlated minimally with an increased callus
size at Week 6 (P = 0.02), but no correlation was found at Weeks 12 and 24 post
surgery. Compared with stainless steel plates, titanium plates had 76%, 71%, and 56%
34

more callus at Week 6 (P = 0.04), Week 12 (P = 0.03), and Week 24 (P = 0.09),
respectively.
Johnstone et al (2010) studied the challenges associated with treating distal femoral
fractures with locking plates in the elderly. The presence of significant co-morbities
e.g. Rheumatoid arthritis, long term systemic steroid use, cerebrovascular
accidents resulting in ambulatory problems, previous major joint arthroplasty including
ipsilateral knee replacements, paralysis, and severe dementia, did not appear to
influence fracture union significantly. However, old age was strongly correlated with
nonunion with all failed cases (7 patients - 10% of the study group) presenting with
failure of fixation. 2 of the LP system failures resulted in malunion and the 5 other
cases required revision surgery. Of note, all 7 patients were elderly, 6 being over 80
years of age.
Wähnert D et al (2010) studied the biomechanical stability of four different fixation
devices for the treatment of comminuted distal femoral fractures in osteoporotic bone.
Three intramedullary nails, differing in the mechanism of distal locking and one angular
stable plate were used. The findings of this study support the concept that, for
intramedullary nails, the kind of distal interlocking pattern affects the stabilization of
distal femoral fractures. Four-screw distal locking provides the highest axial stability and
nearly comparable torsional stability to that of the angular stable plate; the four-
35

screw distal interlocking construct was found to have the best combined (torsional and
axial) biomechanical stability.
To study and compare the role of Dynamic Condylar Screw and distal femoral locking
compression plate in Distal Femur fractures. Final junctional results will be based on
the following criteria.
1. Union of fractures.
2. Amount of range motion of knee joint.
3. To asses the complications of each implant.
The patients will be divided into two groups :-
Group A Patients operated with Dynamic Condylar Screw.
36
Group B Patients operated with Distal femoral Locking compression plate.
.
This prospective study was conducted in the Post Graduate Department of
Orthopaedics, Government Medical College, Jammu. The study was conducted on
37
patients admitted from 1st May 2010 onwards with each patient having followed up for
6 months.
All the adult patients, of either sex with distal femoral fractures (lower 9 to 15 cm
of femur) attending the emergency services in Government Medical College, Jammu
were taken up for the study. Old and fresh cases and, simple or compound fractures
were taken up.
Fifty consecutive patients were included in the study,twenty five of them were
managed by surgery with dynamic condylar screw so they were placed in group A i.e
DCS group and another twenty five patients were managed by surgery with distal
femoral locking compression plate hence placed in group B i.e DFLCP group. The
average age at time of surgery in DCS group and DFLCP group was 43.76 yrs and
46.44years respectively. There were 19 males, 6 females in DCS group and 18 males,7
females in DFLCP group.
On admission a general physical examination followed by local examination was
done and life threatening injuries were dealt on priority.
The first aid in the form of Plaster of Paris (POP) back slab/splint, skeletal traction,
analgesics, wound debridement, antiseptic dressings as required was done. Antibiotics
and tetanus toxoid immunization was given, if required.
38
Clinical examination was followed by radiological examination and anterior-
posterior (AP) and lateral views of the knee joint and distal femur were taken to assess
the type and the displacement of the fracture.
The patients were assessed medically and fitness for general anesthesia and spinal
anesthesia was sought.
The following investigations were done:
Haemogram
Serum biochemistry (blood sugar, serum urea, serum creatinine, serum
electrolytes)
X-ray chest (PA view)
ECG
Blood grouping
Urine R/E
X-ray distal femur and knee joint both AP and lateral views.
Initially all patients were given POP slab/splint or skin traction. Patients with
compound fractures were taken up for surgery only if their wounds showed no sign of
infection after 3 to 5 days after the initial debridement within 6 to 8 hours of injury.
39
SURGICAL TECHNIQUE AND IMPLANT
Patient positioning- The patients were positioned supine on a radiolucent table that
allowed unimpeded fluoroscopic imaging in both planes. A small bump was placed
beneath the ipsilateral hip. It should be sized to ensure that the femur remained in
neutral rotation, assisting with the intraoperative assessment of extremity rotation
during and after reduction. The knee was placed in slight flexion over a custom ramp
or folded blankets with an additional small rolled bump at the fracture site. This
improved the sagittal plane reduction of the fracture by relaxing the primary deforming
forces of the gastrocnemius. In addition, this position facilitates intraoperative, lateral,
fluoroscopic imaging of the proximal thigh without obstruction from the contralateral
extremity.
The entire limb was prepared and draped from the ipsilateral pelvis to the toes,
allowing intraoperative manipulation of the leg and access to the femur proximally as
needed. If traction radiographs in the AP and lateral planes had not been obtained
previously, these could be obtained at that time. A sterile tourniquet was applied
proximally if desired.
SURGICAL APPROACH AND FIXATION TECHNIQUE:
OPERATIVE PROCEDURE FOR DYNAMIC CONDYLAR SCREW
40
After anaesthesia, patient was placed on orthopaedic table and traction was
applied to the limb so that both adductor tubercles were at same level.
After proper painting and draping of the part the fracture site was exposed using
a lateral approach with straight lateral incision made along the thigh. The incision
extended distally across midpoint of lateral condyle of femur anterior to lateral
collateral ligament, across the knee joint and then gently curved anteriorly, to end
distal and lateral to the tibial tubercle. Fascia lata was incised in line with skin
incision. Ilio tibial tract was incised at knee to expose lateral femoral condyle after
incising joint capsule and synovium. The vastus lateralis was carefully elevated from
intermuscular septum and retracted anteriorly and medially. The perforating vessels
were identified and ligated. The K-wire was inserted at a point 2 cm from joint
surface at the junction of the anterior 1/3rd and posterior 2/3rd of longest AP
dimension of femoral condyle or in middle of anterior 1/2 of lateral femoral condyle.
The K-wire was parallel to distal articular surface in frontal plane which was
controlled by putting a K-wire along distal articular surface as a guide. The wire was
950 to lateral surface of lateral femoral condyle. For the wire to course between
patellar groove anteriorly and intercondylar notch posteriorly another K-wire was
placed as control over patellar groove and the K-wire which penetrated the condyle
was made parallel to both control K-wires in frontal and transverse planes. This guide
41
wire was advanced to medial cortical surface was measured with depth gauge and
depth to be reamed was ascertained. The cannulated reamer was set at a marking
which was 10 mm less than that showed by depth gauge and wire was overreamed. A
cannulated screw tap was used in good quality bone to prepare for screw placement.
The screw of appropriate depth was inserted over guide wire (the size of screw was 5
mm less than that of cannulated reamer setting to countersink the screw in distal
fragment to allow for interfragmentry compression. Once the lag screw was in place
appropriate side plate was selected and applied so that at least eight cortices were
purchased in proximal fragment. In the intercondylar fractures, after anatomical
reduction one or two cancellous screws (6.5 mm) were put anterior and posterior to
the proposed site of insertion of lag screw to convert it into supracondylar fracture.
Axial compression was provided by using eccentric placement of drill and screws.
Plate was fitted to shaft femur with 4.5 mm cortical screws. The wound was
thoroughly irrigated and then closed over negative suction drain. Bone grafting was
done only in cases with gross communation or bone gap or loss.
In extra-articular fractures minimally invasive approach to the distal femur was
used. Two transverse 4- 5 cms incisions one at the metaphyseal end of femur and other
at desired length depending on the length of plate used were given in the skin and
42
iliotibial band was cut in line of its fibres. A submuscular tunnel under vastus lateralis
was formed with periosteal elevator or long artery forceps. The plate was slid in a
submuscular plane along the lateral aspect of the femur using a combination of tactile
feedback and visual clues from the fluoroscopic imaging. Depending on the fracture
geometry two cortex screws or locking screws were put adjacent to the fracture site on
both sides, and then the plate was secured to the bone with locking screws. Atleast 5
screw holes were secured proximal to fracture site. A lateral parapatellar approach
was used in fracture patterns with significant intercondylar comminution, coronal
plane fractures, or both. This approach allowed access to intercondylar comminution,
trochlear comminution, and most medial and lateral coronal condylar fractures. After
proper exposure temporary fixation was done by 2mm K- wires which may also act as
joysticks. Before the application of plate, intra-fragmentary lag in the articular
fragments can be achieved by 6.5 mm cannulated cancellous screws anterior and
posterior to the desired position of plate. Plate is then slid and fixed to the articular
block by locking screws. Then the plate is secured to the diaphyseal portion by giving
stab incisions at the screw sites and fixing by locking screws. Infrequently, a medial
subvastus approach may be required in conjunction with a lateral approach in cases of
severe medial articular communition. After fixation wound is closed over drains.
AFTER TREATMENT:
43

The POP back slab was applied for initial 3 to 4 days until the first dressing. Drains
were removed on the first dressing. If two consecutive dressings were satisfactory,
patient was discharged with oral antibiotics to be continued for 5-7 days.
When the wound condition was healthy POP slab was discarded and active range
of motion exercises and quadriceps strengthening exercises was started.
Patients were allowed to walk with a pair of crutches and bear partial weight till
they achieved good quadriceps power and radiological examination revealed fracture
union.
FOLLOW UP:
Patients were followed up subsequently with clinical and radiological examination
till the fracture united. Range of motion, quadriceps power and ability to bear full
weight were assessed.
Clinically the following observations were made-
1. Local condition of wound.
2. Range of motion of knee joint
3. Limb length discrepancy
4. Fracture site tenderness.
Radiologically the following assessment were made-
1. Articular surface of femur and reduction of fracture.
2. Position of the implant.
44
3. Fracture callus.
Radiological pictures were taken at-
1. Immediate postoperative
2. At 3 weeks.
3. At 6 weeks
4. At 3 months
5. At 6 months.
At six months follow-up final assessment was done. The parameters consisted of:
Clinical union
Range of motion at knee joint
Power and mobility of quadriceps
Walking distance
Functional ability in the form of ability to sit crossed leg and squat.
Radiological union
Any limb length discrepancy
Total time for union
Complications
IMPLANT:
Dynamic Condylar Screw:
45

The screw has smooth shaft with two flat sides and is partially threaded. The screw is
cannulated and has an inside thread at the outer end for the compression screw and
two holes for coupling with instruments for insertion and extraction.
IMPORTANT DIMENSIONS
SCREW LENGTH (mm)
50,55,60,65,70,75,80,85,90,95,100,105,110,115,120,125,130,135,140,145 Thread
Diameter= 12.5mm
Thread Length = 22mm
Shaft Diameter = 8mm
DCS PLATE(95o)
46
These plates have barrel length of 25mm with two internal flats to guide the screw.
The palte has staggered screws. The plates are available with 6, 8, 10,12,14 and 16
holes with length from 100mm to 260mm.
DIMENSSIONS
Thickness = 5.4mm
Width =16mm
Hole Spacing = 16mm
CANCELOUS BONE SCREWS
Thickness = 6.5mm
DCS can be used if atleast 4cm of the distal femur is intact to provide support for
implant and the medial cortex should also be intact.
DISTAL FEMORAL LOCKING COMPRESSION PLATE:
47
A distal femoral locking plate of appropriate length and side (right or left) was
taken-up such that at least five screws were above the most proximal end of fracture.
The implant was made up of either stainless steel or titanium.
IMPLANT SPECIFICATIONS-
Length :
6 hole: 155mm
8 hole: 193 mm
10 hole: 230 mm
13 hole: 286 mm
16 hole: 342 mm
19 hole: 399 mm
LCP combi-holes
Tapered ends to slide summuscularly
Undercuts
Thickness 5.8 mm
Fixation with:
5 mm locking screws
4.5 mm cortex screws
6.5 mm locking cancellous screws
Set also included
3.2mm, 4.3mm drill bits.
48
1.8mm, 2mm, 2.5mm Kirshner’s wires.
Drill sleeves.
Condylar clamps.
Bone holding and Plate holding forceps
Assessment of results were done with criteria laid down by Schatzker’s and
Lambert (1979) for supracondylar fractures which is given below.
Excellent:
1. Full extension
2. No varus, valgus or rotational deformity.
3. No pain
4. Perfect joint congruency
Good:
Not more than one of the following.
1. Loss of length not more than 1.2 cm
2. Less than 100 valgus or varus deformity
3. Flexion loss more than 200
4. Minimal pain
Fair:
1. Any of two criteria in good category.
49
Failure:
1. Flexion to 900 or less
2. Varus or valgus deformity more than 150
3. Joint incongruency
Disabling pain no matter how perfect the X- ray.
50

The present study is based on 50 cases of Supracondylar and intercondylar fractures of
femur admitted to the Department of Orthopaedics, Government Medical College,
Jammu. Out of 50 cases 25 were grouped in Group A and were managed surgical
treatment with dynamic condylar screw and other 25 were placed in Group B and were
managed by surgical treatment with distal femoral locking compression plate. Patients
were assessed and compared at regular intervals of time both clinically and radio
logically for a period of six months.
51
Table 5.1: Age Distribution
DCS GROUP DFLCP GROUP
Age in years No. of cases %AGE No. of cases %AGE
15-30 6 24 2 8
31-50 10 40 14 56
51-60 5 20 7 28
Above 60 4 16 2 8
Total 25 100 25 100
As shown in the table 1, out of 25 cases in DCS Group 6 (24%) patients were in age
group of 15-30 years, 10(40%) patients in 31 - 51 years age group and in 51 - 60 years
age group they were 5(20%) cases. In above 60 years of age group they were 4(16%)
cases. Average age in DCS Group was 43.76 years.
In DFLCP Group out of 25 cases, 2(8%) patients were in age group of 15 - 30 years,
14(56%) patients in 31-50 years age group. In 51 - 60 years age group they were
52
7(28%) cases and 2(8%) cases were above 60 years of age. Average in this group was
46.44 years.
Table 5.2: Sex Distribution
DCS GROUP DFLCP GROUP
Sex No. of cases %AGE No. of cases %AGE
Males 19 76 18 72
Females 6 24 7 28
Total 25 100 25 100
In the presence study as shown in table 2 there were 19(76%) Males and 6(24%)
Females in DCS Group.
In DFLCP Group there were 18(72%) Males and 7(28%) Females.
In the study males clearly outnumbered females.
53

Table 5.3: Mode of Trauma
DCS GROUP DFLCP GROUP
Mode of Injury No. of cases %AGE No. of cases %AGE
Road Traffic Accident 21 84 19 76
Fall from height 4 16 6 24
Total 25 100 25 100
In DCS Group, the road traffic accidents was usual mode of trauma in 21(84%) cases
and 4(16%) cases fall from height was the mode of trauma.
In DFLCP Group, in 19(76%) cases the road traffic accidents was usual mode of
trauma and in 6(24%) case fall from height was the mode of trauma.
54
Table 5.4: Side Involvement
DCS GROUP DFLCP GROUP
Limb Involved No. of cases %AGE No. of cases %AGE
Right 13 52 16 64
Left 12 48 9 36
Total 25 100 25 100
In DCS Group right limb was involved in 13(52%) cases were as left limb was
involved in 12(48%) cases.
In DFLCP Group right limb was involved in 16(64%) cases where as left limb was
involved in 9(36%). In this group as clearly indicated right lower limb was more
frequently injured as compared to left.
55
Table 5.5: Type of Fracture (Open or Closed)
DCS GROUP DFLCP GROUP
Type of Fracture No. of cases %AGE No. of cases %AGE
Open 7 28 7 28
Closed 18 72 18 72
Total 25 100 25 100
In DCS Group the number of open fracture 7(28%) were less than closed fractures
18(72%).
In DFLCP Group also the number of open fractures were 7(28%) and the number of
closed fractures were 18(72%).
In both the groups the open fractures were less than closed fractures.
56

Table 5.6: Type of Fracture (AO/OTA) Classification
DCS GROUP DFLCP GROUP
AO Type No. of cases %AGE No. of cases %AGE
A 11 44 10 40
B 5 20 5 20
C 9 36 10 40
Total 25 100 25 100
In DCS Group there were more of type A fractures 11(44%) than, 9(36%) type C
fractures and 5(20%) type B fractures.
In DFLCP Group the type A and type C fractures were 10(40%) each and type B
fractures were 5(20%).
57

Table 5.6 (a)
DCS GROUP DFLCP GROUP
Type A Fracture No. of cases %AGE No. of cases %AGE
A1 5 45.4 3 30
A2 3 27.2 4 40
A3 3 27.2 3 30
Total 11 100 10 100
Table 5.6 (b)
DCS GROUP DFLCP GROUP
Type B Fracture No. of cases %AGE No. of cases %AGE
B1 5 100 5 100
B2 0 0 0 0
58

B3 0 0 0 0
Total 5 100 5 100
Table 5.6 (c)
DCS GROUP DFLCP GROUP
Type C Fracture No. of cases %AGE No. of cases %AGE
C1 4 44.44 5 50
C2 4 44.44 4 40
C3 1 11.11 1 10
Total 9 100 10 100
The following was observed in this study.
IN DCS GROUP
1) In type A fractures there were more type A1 fractures i.e., 5(45.4%), less of
type A2 3(27.2%) and type A3 3(27.2%). Overall there were 11(44%) patients having
type A fractures out of total 25 patients.
2) In type B fractures there were 5(100%) of type B1 fractures. Total number
of patients having type B fractures were 5(20%) of total 25 patients.
59
3) In type C fractures there were 4(44.4%) patients having type C1 fractures,
4(44.44%) patients having type C2 fractures and 1(11.11%) patients having type C3
fractures. Total number of patients having type C fractures were 9(36%) of total of 25
patients.
IN DFLCP GROUP
1) In type A fractures there were 4(40%) of Type-A2 fractures and there were
equal no. of Type-A1 and Type-A3 fractures i.e. 3(30%). Overall there were 10(40%)
patients having type A fractures out of 25 patients.
2) In type B fractures there were 5(100%) patients having Type-B1 fractures.
Total no. patients having Type-B fractures were 5(20%) of total of 25 patients.
3) In type C fractures there were 5(50%) patients having Type-C1 fractures,
4(40%) patients having Type-C2 fractures and 1(10%) patients having Type-C3
fractures. Type-C fractures were 10(40%) out of total 25 patients.
60
Table 5.7: Associated Injuries
DCS GROUP DFLCP GROUP
Associated Injuries No. of cases %AGE No. of cases %AGE
With Associated Injuries 5 20 4 16
Without Associated Injuries 20 80 21 84
Total 25 100 25 100
In DCS group 5(20%) patients had other associated injuries whereas in DFLCP group
only 4(16%) of patients had other associated injuries.
Table 5.7(a): Nature of Associated Injuries
Nature of Associated InjuriesDCS GROUP DFLCP GROUP
No. of cases No. of cases
Colle’s Fracture 1 2
Shaft of Femur Fracture 1 0
Ankle Fracture 0 1
Tibia Fracture 1 1
Both Bones forearm fracture 1 0
61
Intertrochanter fracture 1 0
Total 5 4
In DCS group one patient had colles fracture,one had fracture shaft of femur,one had
fracture tibia,one patient had fracture both bones forearm and one patient had
intertrochanteric fracture whereas in DFLCP group two patients had colles fracture,one
had ankle fracture and one patient had fracture tibia.
Table 5.8: Average Duration of Hospital Stay, Operative Time, and Union Time
DCS GROUP DFLCP GROUP
Average Hospital Stay
(Range)
15.4
(8-25)
13.08
(8-25)
Average Operative Time
(Range)
119.6
(90-150)
129.6
(100-155)
Average Union Time
(Range)
14.68
(10-24)
14.16
(12-30)
Table 5.8(a): Average Hospital Stay of Patients in Relation to AO/OTA Classification
Type of Fracture (AO/OTA) DCS GROUP DFLCP GROUP
Type A 15.1 12.3
62

(10-25) (9-22)
Type B 12
(10-12)
12
(9-22)
Type C 18.8
(8-25)
14.4
(8-25)
Table 5.8(b): Average Operative Time of Patients in Relation to AO/OTA Classification
Type of Fracture (AO/OTA) DCS GROUP DFLCP GROUP
Type A 120
(90-150)
119
(105-150)
Type B 115
(90-125)
127
(120-140)
Type C 121.7
(95-150)
141.5
(120-155)
Table 5.8(c): Average Union time of Patients in Relation to AO/OTA Classification
Type of Fracture (AO/OTA) DCS GROUP DFLCP GROUP
63
Average Union Rate
(Weeks)
Average Union Rate
(Weeks)
(Range) (Range)
Type A 14.2
(11-22)
13.4
(12-14)
Type B 12
(10-15)
13.4
(12-18)
Type C 15.8
(10-24)
14.6
(12-30)
Following Observation were noted
64
1) The average hospital stay in DCS group and DFLCP group was 15.4 days
and 13.08 days respectively.
2) Average operative time in DCS group and DFLCP group was 119.6 minutes
and 129.6 minutes respectively.
3) Average union time in DCS group and DFLCP group was 14.32 weeks and
13.88 weeks respectively.
When these parameters were studied in relation to the AO classification of distal
femoral fractures, following are the observations:
1) Average hospital stay in type A fractures in DCS group and DFLCP group
were 15.1 days and 12.3 days respectively.
In type B fractures average hospital stay for DCS & DFLCP group was 12 days & 12
days respectively.
For type C fractures average hospital stay for DCS and DFLCP group was 18.8 days
and 14.4 days respectively.
2) Average operative time in type A fractures in DCS & DFLCP group was 120
minutes and 119 minutes respectively.
Average operative time for type B fracture in DCS and DFLCP group was 115 minutes
and 127 minutes respectively.
For type C fractures, average operative time for DCS and DFLCP group was 121.7
minutes and 141.5 minutes respectively.
65
3) Average union time in type A fractures in DCS and DFLCP group was 14.2
weeks and 13.4 weeks respectively.
For type B fractures the average union time for DCS and DFLCP group was 12 weeks
and 13.4 weeks respectively.
Average union time for type C fractures for DCS and DFLCP group was 15.6 weeks
and 14.6 weeks respectively.
Table 5.9 : Union Time
Time Taken DCS Group DFLCP GROUP
66
No. of cases %Age No. of cases %Age
10 weeks or less 3 12 0 0
11-14 weeks 13 52 21 84
15-20 weeks 5 20 3 12
More than 20 weeks 4 16 1 4
Total 25 100 25 100
Most of the fractures in DCS group united with range of 11-14 weeks. Only 5
(20%) fractures united in range of 15-20 weeks and 4 (16%) fractures took more than
20 weeks.
Whereas in DFLCP group 21 (84%) fractures united with range of 11-14 weeks, 3
(12%) cases took range of 15-20 weeks and only 1 (4%) took more than 20 weeks.
Table 5.10 : Operative Time (In Minutes)
Operative time in minutes DCS GROUP DFLCP GROUP
No. of Patients No. of Patients
67
≤ 100 5 2
101-120 10 11
121-140 8 4
140-160 2 9
In majority of cases i.e. 10 in DCS group, operative time ranged 101-120 minutes,
whereas in 8 cases operative time ranged 121-140 minutes and in 2 cases it ranged
140-160 minutes.
In DFLCP group 11 patients were operated ranged from 101-120 minutes whereas
4 patients were operated from 121-140 minutes. In 9 patients the operative time ranged
140-160 minutes.
Table 5.11 : Documented Complications the Present Study
Complications DCS GROUP DFLCP GROUP
68

No. of Patients No. of Patients
Superficial Infection 1 1
Deep Infection 1 1
Disabling Pain 1 1
Minimal Pain 3 4
Angulation 2 3
Rotation Nil Nil
Revision Due to Loosening Nil 1
Refracture Nil Nil
Limb Length Discrepency 1 Nil
Knee Stiffness (Less Than 90) 2 2
The superficial infection occurred both in DCS and DFLCP group i.e. 1 case in DCS
group and 1 case in DFLCP group. The patients who had superficial infection in DCS
group also had minimal pain which costed him the range of motion of knee joint.
After repeated saline lavages and antibiotics the infection subsided, and after
union implant was removed to get rid of pain.
69

There is one case of deep infection in both DCS group and DFLCP group. Both the
cases went to failure because of knee stiffness.
Disabling pain occured in one patient in DCS group and also occurred in one
patient in DFLCP group.
Limb length discrepency occurred in one case in DCS group because of
supracondylar communition, which ultimately went into failure because of knee
stiffness. Same patient had fracture both bones same leg.
There are two cases of angulations i.e. 50 of varus angulation in DCS group and 3
patients had 50 of varus angulation in DFLCP group. Revision due to
loosening was done in one case in DFLCP group.
In DCS these were 2 cases of failure, one was due to deep infection followed by
knee stiffness and minimal pain. Other was due to massive supracondylar
comminution of femur with fracture of both bones of same leg; same patient had knee
stiffness and limb length discrepancy.
In DFLCP group there were also 2 cases of failure.One was due to deep infection and
5 degrees of varus malalignment,.the patient ultimately got knee stiffness.
The other failure was due to consistent pain which lead to knee stiffness.Implant had
to be removed after union was achieved.
70
Table 5.13 : Range of Movement of Knee Joint (Flexion in Degree)
Range of Movement (0) DCS GROUP DFLCP GROUP
No. of Patients No. of Patients
0-30 2 2
31-60 0 0
61-90 0 0
91-120 11 11
121-140 12 12
Total 25 25
The average range of motion of knee joint in DCS group was 0-108.40 whereas it was
107.60 in DFLCP group.
In DCS group 11 and 12 patient had range of motion of knee joint between 91-1200
and 121-1400 respectively. Only 2 cases in DCS group had <900 of range of motion of
knee joint.
In DFLCP group also 11 and 12 patients had range of motion of knee joint between
91-1200 and 121-1400 respectively.
71

The assessment of result was done with criteria laid down by Schatzker and Lambert
(1979) for supracondylar fractures which is given below.
Excellent:
1. Full extension
2. No varus, valgus or rotator deformity
3. No pain
4. Perfect joint congruency
Good: Not more than one of the following.
1. Loss of length not more than 1.2 cm
2. Less than 10° valgus or varus deformity
3. Flexion loss more than 20°
4. Minimal pain
Fair: Any of two criteria in good category.
Poor:
72

1. Flexion to 90° or less
2. Varus or valgus deformity more than 15°
3. Joint in congruency
4. Disabling pain no matter how perfect the X-ray
Table 5.14 : Results
Results DCS GROUP DFLCP GROUP
No. of Cases % Age No. of Cases % Age
Excellent 10 44 9 36
Good 9 36 10 40
Fair 4 12 4 16
Failure 2 8 2 8
Total 25 100 25 100
In the present study in DCS group 10 (40%) of patients had excellent results, 9 (36%)
patients had good results, 4 (16%) patients had fair results and 2 (8%) patients had
failure. So total of 76% had good or excellent results whereas in DFLCP group 9
(36%) had excellent result, 10 (40%) good results, 4 (16%) had fair results and 2 (8%)
patients had failures, so total 76% of patients had good or excellent results.
73

Table 5.15: Results according to be Type of Fracture
DCS GROUP DFLCP GROUP
Types of Fracture (AO / OTA) Types of Fracture (AO / OTA)
Results A B C A B C
No. of Cases%AgeNo. of Cases%AgeNo. of Cases%AgeNo. of Cases%AgeNo. of Cases%AgeNo. of Cases%Age
Excellent 36.3 80 22.2 60 60 10
Good 54.5 33.3 20 20 60
Fair 9.09 20 22.2 20 20 10
Failure 22.2 20
Total 100 100 100 100 100 100
For Type-A fractures in DCS group 4 (36%) patients had excellent results, 6
(54.5%) had good results and 1 (9%) had fair results, so total of 91% patients had good
to excellent results.
Whereas for Type-A fractures in DFLCP group 6 (60%) cases had excellent
results, 2 (20%) cases had good results and 2 (20%) cases had fair results. So total of
80% patients had good to excellent results.
For Type-B fractures in DCS group 4 (80%) cases had excellent results and 1
(20%) cases had fair results. So total of 80% patient had good to excellent results,
74
where as in DFLCP group,for type B fractures,4(80%) had excellent results,1(20%)
case had fair results.So total of 80% of cases had good to excellent results.
For Type-C fractures under DCS group 2 (22%) cases had excellent result 3 (33%)
cases had good results, 2(22%) cases had fair results and 2 (22%) had failure. So total
of 55% cases had good to excellent results. For Type-C fracture in DFLCP group
1 (10%) case had excellent results, 6 (60%) had good results, 1 (10%) cases had fair
results and 2 (20%) patients had failure. So total of 7 (70%) patients had good to
excellent results.
75
DISCUSSIO
N
76

Due to increased prevalence of high energy trauma the current fracture pattern is
toward complex comminuted fractures especially in young individuals. Improved
healthcare results in longer life span and subsequently presents us with more
osteoporotic fractures which were previously treated using conservative methods. The
violent nature of injury in young individuals who sustain high velocity injuries during
road-traffic accidents and osteoporotic bones in elderly patients makes conservative
treatment an unsatisfactory option, in such cases internal fixation is better option.
The goal of treatment in such cases is to achieve a painless and stable joint with
good range of motion. This can be achieved by open reduction and internal fixation
with such devices which allows rigid fixation of articular surface, is easier to use,
gives respect to soft tissues and allows early weight bearing.
The dynamic condylar screw is a device which makes accurate reduction and
fixation easy. The purchase of lag screw in osteoporotic bone was good and it could be
easily positioned over guide wire under image intensifier. Instrumentation of dynamic
condylar screw was easy to master as compression screw is frequently used in
treatment of hip fractures. However dynamic condylar screw is a fixed angled implant
77

so proper insertion of lag screw at 950 and parallel to joint line after reduction is
recommended, otherwise it can angulate the distal fragment and malunion can occur. If
properly performed operative time is decreased and problems like angular deformity,
instability, joint incongruity and loss of motion are also taken care of. Moreover it
gives stable internal fixation so that post operative range of motion exercises can be
started on 1st post operative day.
The distal femoral locking compression plate is a single beam construct where
strength of its fixation is equal to sum of all screw-bone interfaces rather than a single
screw’s axial stiffness and pull out resistance as unlocked plates. Its unique
biomechanical function is based on splinting rather than compression resulting in
flexible stabilization, avoidance of stress shielding and induction of callus formation
when applied via minimally invasive technique, it allows for prompt, healing, lower
rates of infection and reduce bone resorption as blood supply is preserved. Locking
plates have biological advantages (Sommer C, 2003, Wagnee M, 2003) over standard
plates. A standard plate grips the bone by friction created by the compression of plate
against the bone by screws. This leads to impaired blood supply (Perren S, 1988)
resulting in decreased cortical thickness and cancellous transformation of bone. The
risk of peri implant fracture is also reduced by locking plates.
In present study of 50 cases of fractures of distal femur admitted in Department of
Orthopaedics, Govt. Medical College Jammu were divided into two groups i.e. Group-
78

A and Group-B. The patients in Group-A were operated using dynamic condoyle
screw and the patients in Group-B were operated using distal femoral locking
compression plate. All the cases had unilateral distal femoral fractures.
1) Age Incidence:
The mean age in DCS group is 43.76 years which is in contrast to study done by
Schatzker et al. (1974) where the mean age is 52.2 years. The mean age in DFLCP
group is 46.44 years which is also in contrast with Schatzker et al. study (1979)
where mean age was 52.2 years. The study done by Schatzker et al. was done in
1970’s when traffic load was less and most fractures would occur in elderly due to fall.
Distal femoral fractures occur in middle age group where RTA is the most common
cause. With the increased burden of work and stress on middle age group, they are
more prone to accidents.
2) Sex distribution:
In present study there were 19(76%) males and 6(24%) females in DCS group and
18(72%) males and 7(28%) females in DFLCP group. Sex ratio in DCS group was
(3.16 : 1) whereas sex ratio in DFLCP group was (2.57 : 1). overall sex ratio was
(2.86 : 1). This shows that the incidence of fractures of distal femur is more in males
than in females. This is in contrast with other studies (Schatzker et al. 1979) in which
the incidence of fracture was more in females. However there are some studies which
79

have shown sex ratio to be more in males (yeap and Deepak 2007) which showed that
63% affected were males.
The present study is in accordance with recently conducted studies that shows that
males suffers more trauma and thus, fracture of distal femur. This can very well be
explained by the fact that over the years, road traffic has increased and in country like
India males are predominant drivers. Also in our country especially in rural areas
females are less indulged in outdoor activities thereby decreasing the chances of
getting this fracture which is usually caused by high energy trauma.
3) MODE OF TRAUMA
In present study the predominant mode of trauma in DCS group was Road traffic
accident (84%) and in DFLCP group was (76%). The ratio of RTA to fall in DCS
group was (5.25:1) and in DFLCP group was (3.1:1). Study done by schatzker et al. in
1979 showed that fall was the most common cause of fracture of distal femur
accounting for 78%. Also study done by Kolmert and wuff in 1982 showed that road
traffic accidents accounted for 37% of fractures only.
Recently the trend has changed. Now RTA has become the most common cause of
distal femoral fractures. Study done by Yeap & Deepak in 2007 indicated that 63%
fractures were caused by road traffic accidents. Wright and Collinge in 2004 also
studied that road traffic accidents was a major cause (81%).
80

Our study is also comparable with recently done studies. With the advancing
technology and ever increase vehicle traffic majority of fractures are caused by road
traffic accident implicating high energy trauma. In our study fall as mode of trauma
was seen mostly in elderly patients and in females.
4) Type of fractures (Open or closed).
In the present study closed fractures were present in 18(72%) of patients and open
fractures were present in 7(28%) of patients with ratio of (2.5:1) in DCS group and
closed fractures were present in 18(72%) of patients and open fractures were present in
7(28%) of patients with ratio of (2.5:1) in DFLCP group.
Recent studies done by Schandelmaier et al and Schultz et al. in 2001 also
indicated that patients had more closed fractures and were 81.5% and 71%
respectively. Studies done by Schultz et al 2005 and Wright and Collinge in 2004
indicated towards the same trend. Our results in the present study all comparable with
there studies. This can be explained by the fact that unlike tibia, femur is well covered
by huge soft tissues which resists compounding from with in. All the latest literature
supports evidence of closed fractures being more than open fractures.
5) Classification of fractures AO/OTA
Most of the studies have taken account into type A fracture which are extra
articular and type C fractures which are intr articular. In present study there were 81

11(44%) cases of type A fractures and 9(36%) cases of type C fractures in DCs group
and 10(40%) cases of type A fractures and 10(40%) cases with of type C fractures in
DFLCP group.
Kolmert et al in 1982 studied the pattern of fracture of distal femur and shown
47% of type C fractures.
Kregor et al 2001 also showed 50% of type A and 50% of type C fractures. The
high percentage of type C with fractures were due to more incidence of high energy
trauma which is in accordance with the recent trend.
6) Union time and full weight bearing (in weeks)
In present study the average radiologial union time was 14.32 weeks ranging from
10-24 weeks in DCS group.
Shewring et al 1991 showed that average union time was 11.3 weeks ranging (6-
16) wks.
Iftikhar et al 2007 showed average union time to be 15 wks which is comparable
with the present study.
Some studies showed late union of fractures (Christodoulow et al showed average
union time to be 20 wks and Huang HT et al reported the average union time was
18.5 wks). The late union of fractures may be due to delayed post. operative
82
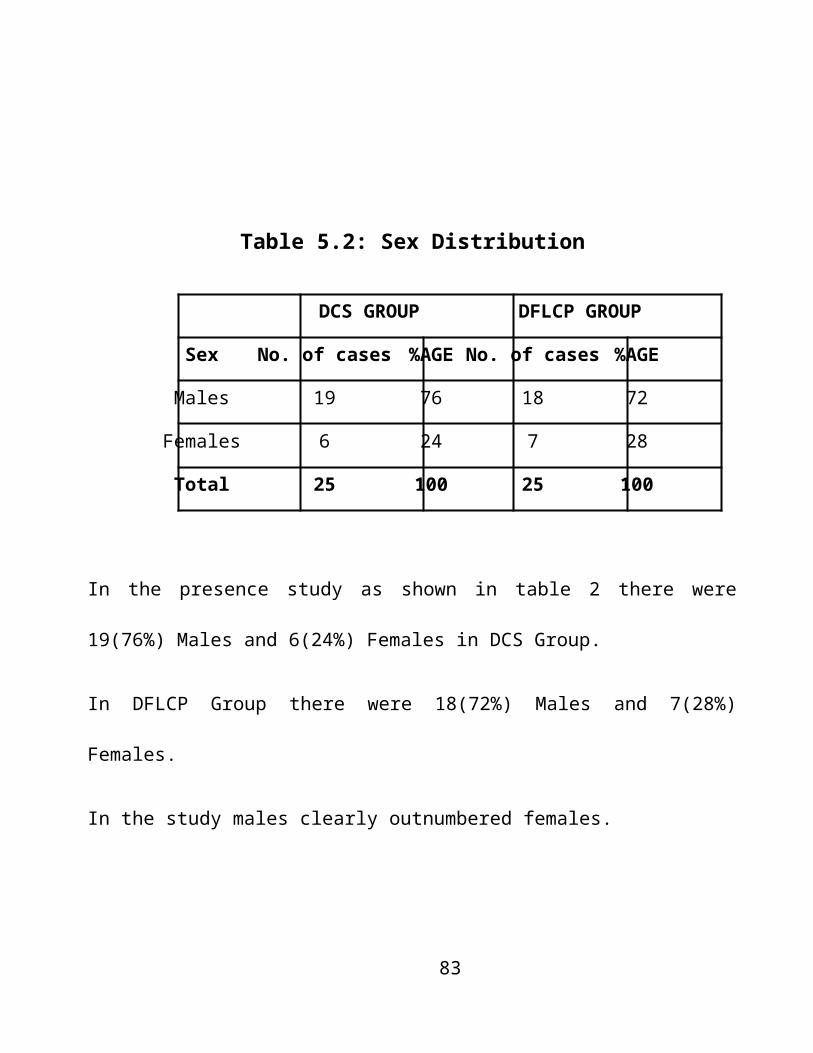
mobilization. The average radiological union time was 13.88 weeks ranging 12-30
weeks in DFLCP group. Schandelmeir et al in 2001 and Mackmiller et al in 2004.
showed similar results having full radiological union was 14.3 and 13.8 weeks
respectfully. Kregor et al in his study in 2004 showed that fracture united in 12 wks
which was earlier than our study by 2.2 weeks. Wright and collinge et al in 2004 also
showed in their study that fractures united in 13 weeks.
Union radiologically was defined which at least 3 cortices showed signs of union
and clinically which patient was able to bear full weight.
7) Range of Motion of KNEE Joint (in degrees)
The average range of motion of knee joint was 0-108.4o in one series and is
comparable with other studies. Study done by Shewring et al 1991 and Iftikhar et al
had range of motion of 0-112o and 0-111o respectively.
The average range of motion of knee joint for DFLCP group was 0-107.6o where as
studies done by Kresor et al, Schultz et al and Schandelmier et al 2001 had range of
movements of 103o, 107o and 104o respectively.
Mackmiller et al in 2004 reported average range of motion of knee joint of 110
degrees.
83

Our patients in both the groups achieved good range of motion the main reason was
early rehabilitation programme. We instituted patients to range of motion and
quadriceps strengthening excercises with in first week. Partial weight bearing was also
started when early signs of union were visible at about 4-5 weeks and patients
subsequently walked according to their tolerance. Few patients had restricted range of
motion because of high intra articular communition and compounding. Severe
ligaments injuries could also have been the reason in these cases.
8) Complications
In our series complications like superficial infections, deep infections, implant removal
due to pain and mal-alignment in the form of valgus mal-alignment was found. In all
the cases varus mal-alignment did not exceed more than 5 degrees.
Following complications were seen in our study.
a) Mal-alignment (varus or valgus deformity) In DCS group mal-alignment was
noted in 2(8%) of patients where as in DFLCP group mal-alignment was noted in
3(12%) of patients.
All had varus mal-alignment. It was about 5 degrees in all the cases.
84

Schandelmill et al 2001 and Wright in 204 reported mol-alignment of 13% and
13.6% respectivley.
b) Deep Infections In DCS group 1(4%) of patients got deep infection. Ittikhar 2007
also showed in his study the infection rate of 5.71%.
In DFLCP group one patient (4%) got deep infection. Kregor et al in 2001 and
Schultz et al in 2005 showed that deep infection occured in 3% of the patients.The
degree of soft tissue damage, severity of communition and compounding, all were
determinants in causing deep infection.
c) Removal due to Pain
In DCS group one patient (4%) had disabling pain. Pain was due to a long lag screw
which protruded on the medial side. The pain subsides after the screw was removed. In
DFLCP group there is also one patient (4%) showed disabling pain. Cause of the pain
could not be known. Even after proper pain management and physiotherapy pain could
not be relieved. Implant had to be removed in both the cases.
In some studies authors like Schultz et al in 2005 and Schandelmier et al in 2001
reported no evidence of disabling pain in their patient.
d) Revision due to Implant Loosening
85

In DCS group no revision of implant was done which is comparable to study done
by shewring et al in 1991.
In DFLCP our revision of implant 1(4%) patients was slightly less than other
studies. Schandelmier et al in 2001 and Schultz et al in 2001 reported 7.4% and 6%
incidence of revision. This may be because of the fact that we had relatively young
patients with good bone stock. Our post operative rehabilitation programme was also
good.
We did not have any non union in the study.
In Des group there is one (4%) patients having limb
shortening and was due to extreme degree of communution in supracondylar region. In
DFLCP group there is no patient with limb shortening..
Knee stiffness was found to occur in two cases (8%) in DCS group and was due to
adhesions which formed at the knee joint gentle manipulation under GA was done in
one case and some flexion at knee joint was regained.in other patient cold not
recovered from knee stiffness and ultimately went into failure.In DFLCP group two
cases (8%) of cases had knee stiffness.
Results (Good to Excellent)
86

DCS DFLCP
Good/ Excellent Results Good/ Excellent Results
Slatis et al 1967 Frank Hauser et al 2004
Schatzker et al 1974 Wong et al 2005
Silski et al 1989 Yeap and Deepak 2007
Ostrum and Geel 1995 Schatzker’s and Lambert
Present Study Present Study
According to the criteria shown by schatzker’s and Lambert , the final results in our
series in DCS showed that 19 (76%) patients had excellent or good results. The results
of our series were comparable with the benchmark done by Schatzker’s 1974. He
obtained 75.5 excellent to good results. Slatis et al 1971 also obtained 75% excellent
to good results. Neer et al 1967 obtained 50% of excellent to good results. Silski et al
1989 and Ostrum and Geel 1995 showed 84.5% and 87% good to excellent results
87
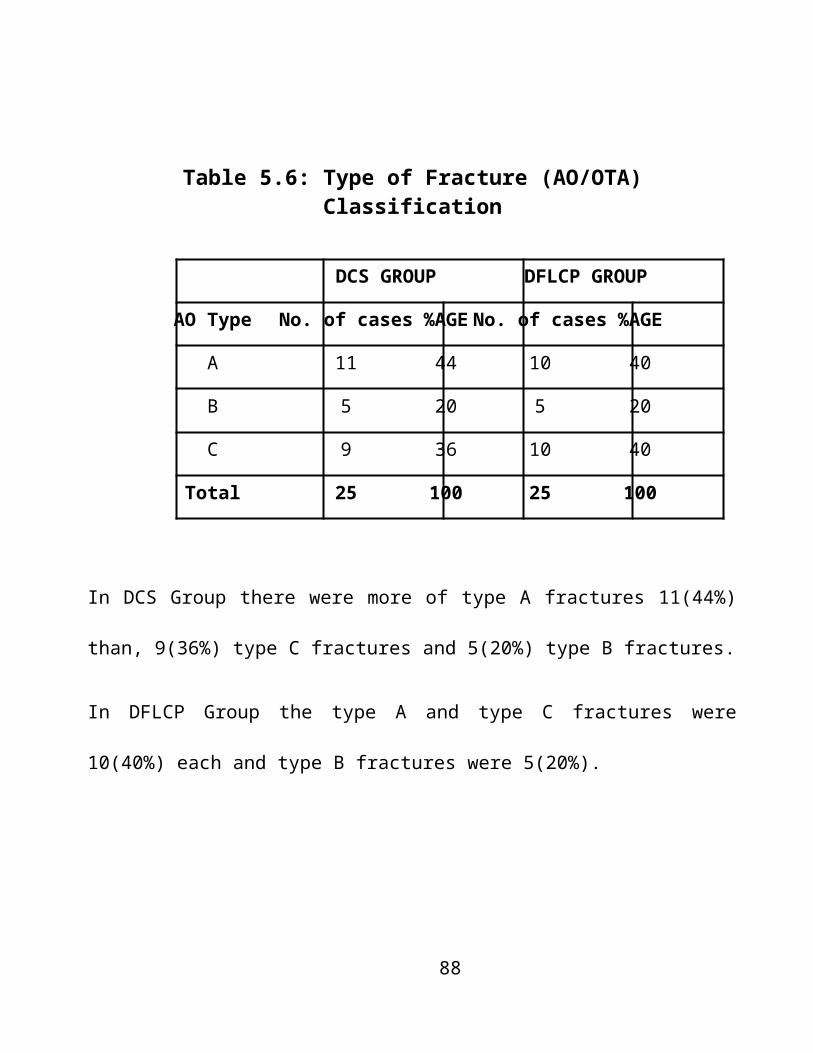
which is almost 10% more them the present study. This could be because we included
more number of type C fractures in our study compared to other studies.
The results of DFLCP in present study were 76% (19) patients had excellent or
good results.
The results of our series were comparable with study done by Schatzker’s and
Lambert in 1979. They also obtained excellent or good results in 74% of the patients.
The results obtained by Franfhauser et al in 2004, Wong et al in 2005 were also
comparable. They had 71% and 76% good or excellent results respectively.
After working on distal femoral fractures, we realized that it is one of the difficult
fractures to handle. Gastronemius muscle attached on the posterior femoral condyles
makes the reduction more difficult, keeping the posterior fragment into flexion.
Distal femur is surrendered by muscles all around so dissection had to be careful
and meticulous. Neurovascular bundle was in close proximity with the distal femur so
care had to be taken.
We often did tend to overlook the ligamentous injuries in view of severe bony
trauma made functional rehabilitation of patients difficult.
The dynamic condylar screw made accurate reduction and fixation easy..
88
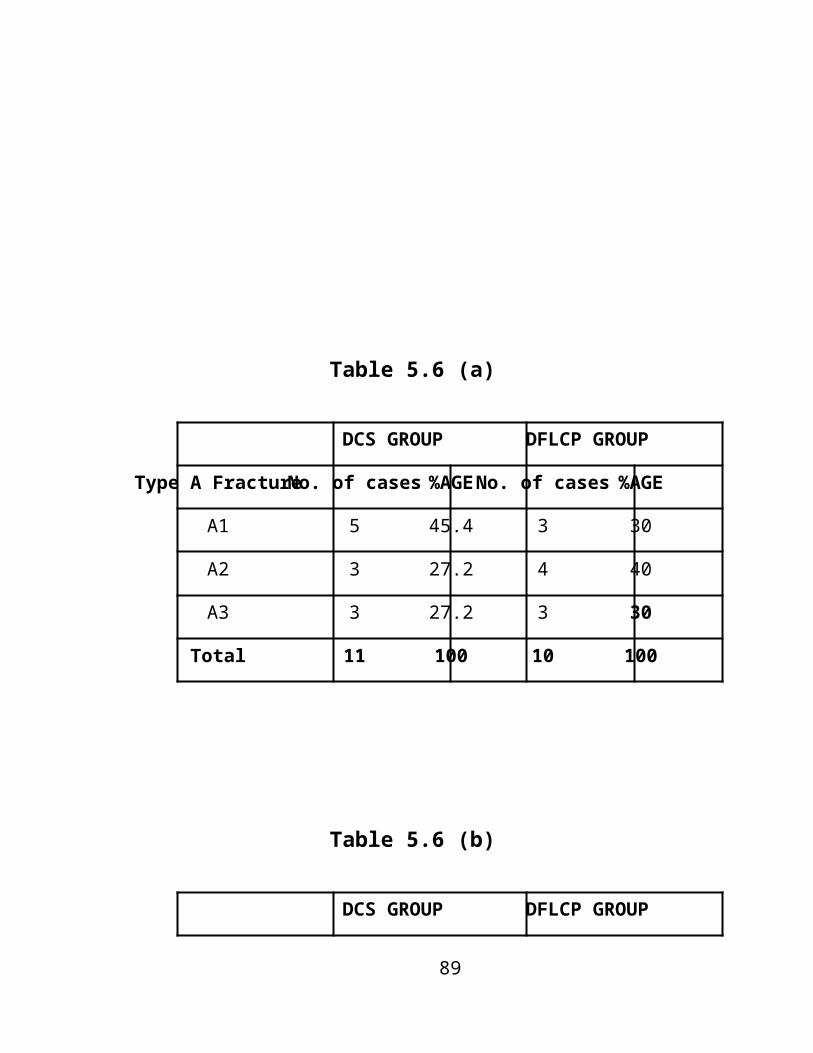
However dynamic condylar screw is fixed angled implant. So proper insertion of
lag screw at 950 and parallel to joint line after reduction is recommended. If it is
performed properly operative time is decreased and problem like angular deformity,
instability, joint incongruity and loss of motion are also taken care of, however a much
longer followup is needed to see if careful adherence to operative principle will
prevent degenerative arthritis from occuring in intraacticular fractures.
Locking plate acts as internal fixation or splint. It does not reduce the fracture so a
proper reduction is must before application of this device to avoid delayed or non-
union.
SUMMARY
89
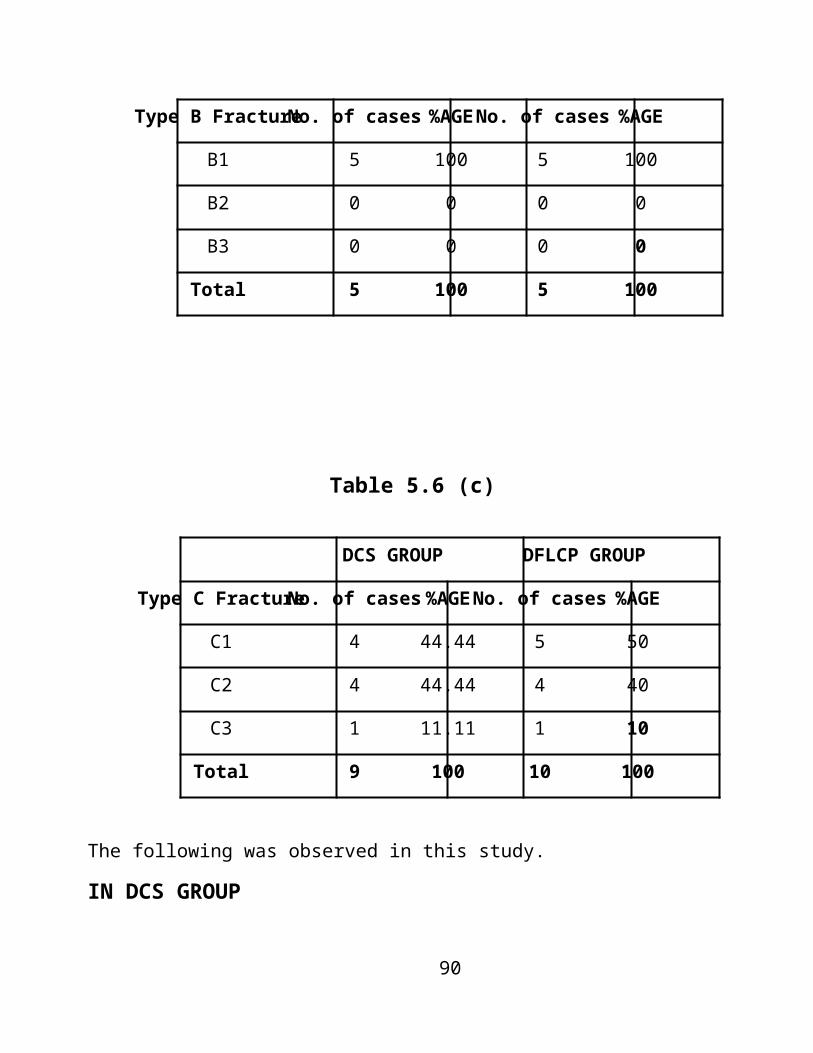
AND
CONCLUSION
The present study was aimed at assess the clinical as well as functional outcome of
Dynamic condyler screw and distal femoral locking compression plate for distal
femoral fracture.
The average age in DCS group was 43.76 years and in DFLCP group was
40.44 years. The age distribution was statistically insignificant (p value=0.45).
There were 19(76%) male cases and 6(24%) female cases in DCS group and
18(72%) male cases and 7(28%) female cases in DFLCP group. The sex distribution
was statistically insignificant (p=0.74, Chi Square-0.10).90

Mode of trauma predominantly was road accident in both groups. In DSS
group there were 21(84%) cases who had mode of trauma predominantly road traffic
accident and 19(76%) cases had mode of trauma predominantly road traffic accident.
The mode of trauma in both the groups was comparable,so the difference was
statistically insignificant (p=0.47, Chi Square-0.50).
In DCs group right side was involved 13(52%) cases and in DFLCP group
right side was involved in 16(64%) cases. The statistical difference was insignificant
(p=0.39, Chi Square-0.74).
There were more closed fracture than open fracture in both the groups i.e.
72% closed and 28% open in both groups. So the difference was statistically in
significant (P=1).
Type A fracture in DCS group were 44% where as they were 40% in
DFLCP group. Type B fracture were 20% in both the groups. Type C fracture were
36% in DCs group and 40% in DFLCP group. The difference in both groups was
statistically insignificant (p=0.95, Chi Square-0.10).
Average operation time was 119.6 minutes in DCs group whereas it was
129.6 minute in DFLCP group. The difference was statistically significant (P=0.03).
Fracture limited with average time of 14.32 weeks and 13.88 weeks in DCs
and DFLCP group respectively. The difference is statistically insignificant (P=0.68).
91
The range of motion and knee joint in DCS group and DFLCP group was
108.40 and 107.60 respectively. There wre 2 patients in each DCS and DFLCP group
who has range of motion and knee joint less than 900 and 23 patients in both groups
who had range and motion of joint more than 900. Thus the difference is insignificant
between two groups (P=1).
The average hospital stay in case of DCS and DFLCP group was 15.4 days
and 13.08 days respectively. The difference is statistically insignificant (P=0.13).
The average time from injury to surgery in DCS and DFLCP group was 81.2
days and 7.16 days respectively. The difference is statistically insignificant (P=0.53).
There were complications in both groups. The total number of complications
in DCS and DFLCP group was 11 and 13 respectively. The difference is statistically
insignificant (P=0.57).
According to the criteria laid by Schatzkers and Lambert, One excellent/Good results
in DCS group and DFLCP group were in 76% and 76% respectively. The overall
results were the same and the difference is statistically insignificant (P=1).
However, in Type A fracture the excellent / good results in DCS and DFLCP group
were in 91% and 80%. This could be because in DCS group there were more number
of Type A fracture i.e. 11(44%) and in DFLCP group there were 10(40%) of cases
92

and there was one case in DFLCP group who got superficial infection and minimal
pain.
In Type B fracture the excellent / good results in DCS and DFLCP group were in
80% and 80% each suggesting both the implants are equally good in Type B fractures.
In Type C fracture the excellent / good results in DCS and DFLCP group were in
55.7% and 70% respectively suggesting distal femoral locking compression plate
could be better for intercondylar and comminuted fractures. The result in Type A,
Type B and Type C fractures could not be compared because of small sample size in
each group.
So in one study we found that DFLCP has no better overall significant results,
However DFLCP had better results in Type C Fractures, though DCS was better in one
study for Type A fractures but that was due to infection in one case of DFLCP rather
than peculiarity or specificity of implant.
There was no superiority of DFLCP over DCS in old patients. This may be because
of small number of old patients in one study.
Distal femoral fractures are difficult to treat and ideal treatment of such fratures
will include anatomical reduction, rigid fixation of articular surfaces and early
functions of knee joint. This can be provided by such an implant which holds the meta
93
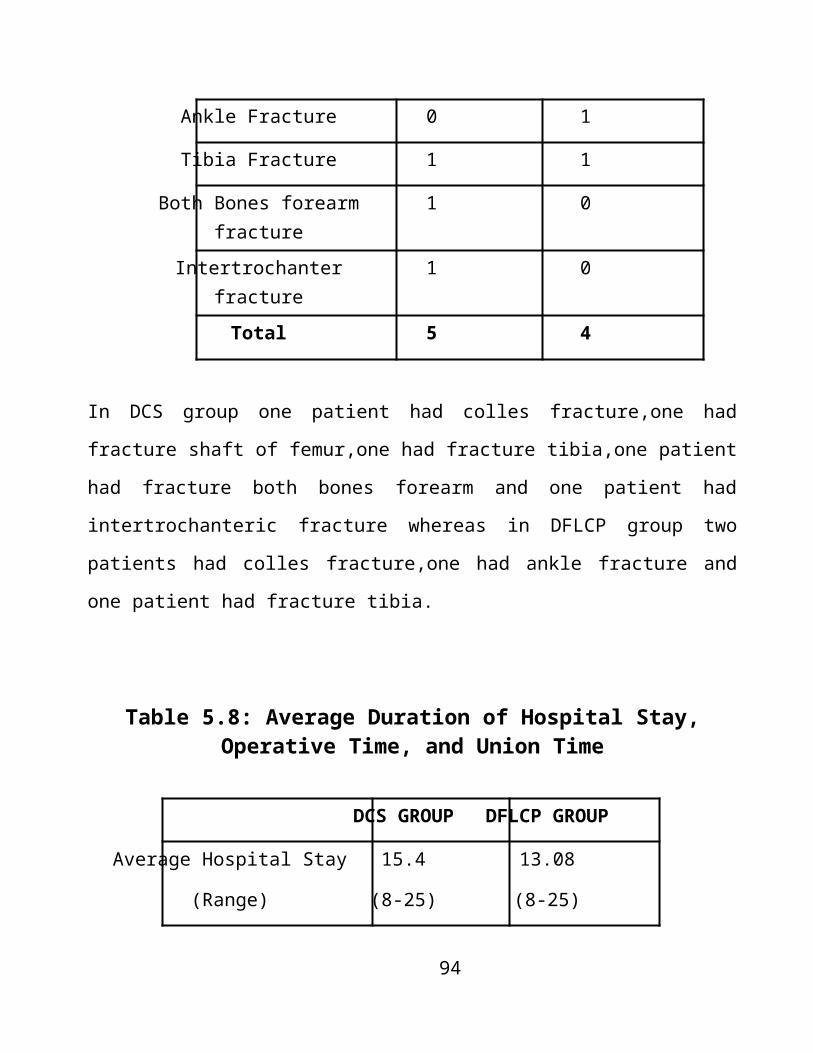
physeal bone strongly and at the same provides stable fixation of the shaft to promote
callus formation.
Keeping in view the above observations, results and facts that distal femoral
locking compression plate by virtue of its combi-holes in stem and locking bolts in the
expanded head area fulfills these criteria and dynamic condylar screw requires a
certain amount of bone stock present which limits their use in some types o fractures.
Thus it was concluded that condylar screw and distal femoral locking plate have
similar results except that distal femoral locking plate is better in communited distal
fractures and have same above mentioned additional advantages over dynamic
condylar screw, further studies are warranted to have better understanding.
1. Albert MJ. Supracondylar fractures of femur. J Am Acad Ortho Surg
1997; 5 (3) : 163-171.
94

2. Alfons R and Richards S. Blade plate fixation in non union and in
complicated fracture of supracondylar region of femur. J Bone Joint Surg 1949; 31A :
312.
3. Arneson TJ, Melton LJ, Lewallen DG et al. Epidemiology of
disphyseal and distal femoral fractures in Rochester, Minnesota, 1965-1984. Clin Orthop
Relat Res 1988; 234 : 188-194.
4. Baijal E. A method of internal fixation of Supracondylar fracture of
femur. Injury 1979, 1 (2): 115-22.
5. Beal M Jr. Transarticular fixation in treatment of non-union of
supracondylar fractures of femur. J Bone Joint Surg 1979; 53B : 420.
6. Chapman MW and Finkemier CG. Treatment of supracondylar non-
unions of femur with plate fixation and bone grafting. J Bone Joint Surg 1999; 81 (9) :
1217-1228.
7. Chiron HS, Tremoulet J, Casey P et al. Fractures of the distal third of
the femur treated by internal fixation. Clin Orthop Relat Res 1974; 100 : 160-170.
8. David SM and Harrow ME. Comparative biomechanical analysis of
supracondylar femur fixation. Locked intramedullary nail versus 950 angled plate. J Ortho
Trauma 1997; 11 (5) : 344-350.
95

9. Ezekiel Tan SL and Balogh ZJ. Indications and limitations of locking
plate. Injury Int Care Injured 2009; 40 : 683-693.
10. Firoozbakhsh K, Behzadi K and DeCoster TA. Mechanism of
retrograde nail versus plate fixation for supracondylar femur fractures. J Ortho Trauma
1995; 9 (2): 152-157.
11. Foster MC. Distal femoral fractures: A review of fixation methods.
Injury Int Care Injured 2006; 37: 97-108.
12. Frankhauser F, Gruber G et al. minimally invasive treatment of distal
femoral fractures using LISS. A prospective study of 30 patients with follow up upto 20
months. Acta Orthop Scand 2004; 75(1): 56-60.
13. Giles LB and Delee JC. Supracondylar and intercondylar fractures of
femur treatment with a supracondylar plate and lag screw. J Bone Joint Surg 1982; 6C:
864.
14. Halpenny J and Rorabeck CH. Supracondylar feacture of femur:
results of treatment in 61 patients. Can J Surg 1984, 27:606-609.
15. Healy WL and Brooker AF. Distal femoral fracture: comparison of
open and closed methods of treatment. Clin J Orthop 1983, 1974:166-171.
16. Henry SL. Supracondylar fractures of femur treated percutaneously.
Clin Orthop 2000: 51-59.
96

17. Johnstone A, Carnegie C and McCollaugh. The challenges associated
with treating distal femoral fractures with distal femoral locking plates in elderly:
Different pattern of failure in different locking plates. J bone J Surg (Br)2010.vol 92-B
Supple 4, 550.
18. Kolmert L, Persson MD and Romans B. An experimental study of
devices for internal fixation of distal femoral fractures. Clin Orthop 1982; 171: 190.
19. Kregor PJ Stannard J, Zlowodski M Cole PA. Distal femoral fracture
fixation utilizing LISS. The technique and early results. Injury Int Care Injured 2001; 32
S-C: 32-47.
20. Kregor PJ, Stannard J, Zlowodski M et al Treatment of distal femoral
fractures using Less Invasive Stabilization system. Surgical technique and early clinical
results in 103 fractures. J Orthop Trauma 2004: 18(8): 509-20
21. Kurt DM and Einer WJ. Supracondylar fractures of femur after total
knee arthroplasty. J Bone Joint Surg 1986; 68A: 29.
22. Kolmert L and wulff K. Epidemiology and treatment of distal femoral
fractures in adults. Acta Orthop Scand.1982; 53, 957-62
23. Lujan, Trevor J, Henderson et al. Locked plate for distal femur
fractures leads to inconsistent and irregular callus formation. J Orthop Trauma 2010; 24
(3): 156-162.
97

24. Marcus JS. Comparison of methods of treatment of fractures of distal
third of femur. J Bone Joint Surg 1966; 48A: 684.
25. Marcus JS. Fracture of distal end of femur. J Bone Joint Surg 1958,
40A: 235.
26. Markmiller M konard G and Sudkamp N. femur- LISS and Distal
Femoral Nail for fixation of distal femoral fractures. Clin Orthop 2004; 426:252-7.
27. Mize RD. Surgical management of complex fractures of distal femur. J
Bone Joint Surg 1989; 249 : 77.
28. Mongkon Luechoowong. The distal femoral locking plate for distal
femoral fractures. Buddhachinaraj Medical Journal 2008. Vol 25(1).
29. Muller ME, Nazarian S and Koch P. The Comprehensive
Classification of Fractures of Long Bones. Springer, New York, 1990.
30. Neer CS. Supracondylar fractures of adult femur. A study of hundred
and ten cases. J Bone Joint Surg 1967; 49A : 591-613.
31. Olerud S. Operative treatment of Supracondylar fracture. Technique and
results in 15 cases. J Bone and J surgery 1972, 54A: 1015.
32. Pemberton DJ, Evans PD, Grant A et al. fractures of the distal femur
in elderly treated with a carbon fibre Supracondylar plate. Injury 1994, 25 (5): 317-21.
98

33. Perren S, Corday J, Khan B et al. Early temperory porosisof bone
induced by internal fixation implants, a reaction to necrosis, not to stress protection?
Clin Orthop Related Res, 1988;232: 139-51.
34. Peter B, Wright and Stanford MD. Supracondylar fractures of the
femur. Clin orthop 1958, 12:256.
35. Preston A, Wade MD and Okina J. Problems of Supracondylar
fracture of femur in aged persons. Am J Surg 1959, 97:499
36. Radford PJ and Howell CJ. The AO DCS for fracture of femur. Inj brit
jour acid surg 1992, 23.
37. Richard S, Riggins MD, James G et al. Supracondylar fractures of
femur. Clin J Orthop 1972, 82:832.
38. Robert E and Zickel MD. A new intramedullary fixation device for the
distal third of femur. Clin Orthop 1997 : 125-185
39. Robert V, funsten MD and Robert W. healing time in fractures of the
shaft of tibia and femur. J Bone and J Surg 1945, 23:395.
40. Rowe CR. Pre-operative and post-operative management of injuries of
the lower end of femur and tibia. J Bone Joint Surg 1965, 47A : 1015.
99

41. Sanders R, Regazzoni P and Reudi TP. Treatment of Supracondylar
and intercondylar fractures of femur using DCS. J Orthop Trauma 1989, 3:214-222.
42. Schandelmaier P. Distal femoral fractures and LISS stabilization. Injury
Int Care Injured 2009; 32 S-C : 55-63.
43. Schatzker J and Lambert DC. Supracondylar fractures of femur. Clin
Orthop 1979; 138 : 77-83.
44. Schatzker J. Fractures of distal femur revisited. Clin Orthop Relat Res
1998; 347 : 43-56.
45. Schutz M, Muller M, Krettek C et al. minimally invasive fracture
stabilization with LISS. A prospective study. Results of clinical study with special
emphasis on difficult cases. Injury 2001.32; SC 48-54.
46. Schutz M, Muller M, Regazzoni P et al. Use of less invasive
stabilization system in patients with distal femoral fractures: a prospective multicentric
study. Acta Orthop Trauma Surgery 2005; 125(2) 102-8.
47. Schaldelmier P, Partenheimer A, Koenemamm B, et al. Distal
femoral fractures and LISS stabilization. Injury. 2001; 32: SC 55-63.
48. Seinsheimer F. Fractures of the distal femur. Clin J Orthop 1980, 153:
169-179.
100

49. Shelbourne DK and Bruckmann FR. Rush-pin fixation of
supracondylar and intercondylar fractures of femur. J Bone Joint Surg 1982; 64A: 161-
169.
50. Sherwing DJ and Meggitt BF. Fracture of distal femur treated with AO
dynamic condylar screw. J Bone and J Surg Br. 1992, 74:122-125.
51. Simonian PT, Thompson GJ, Emley W, et al. Angular screw
placement in the lateral condyle buttress plate for Supracondylar femoral fractures. Injury
1998, 29(2):101-4.
52. Sommer C, Gantier E, Muller et al. first clinical results of locking
compression plate. Injury. 2003;34:S- B 43-54.
53. Stewart MJ, Sisk TD and Wallase SL. Fractures of distal third of
femur. J Bone and J Surg Am 1966, 48: 784-807
54. Smith TO. The clinical and radiological outcomes of the LISS plate for
distal femoral fractures: A systematic review. Injury Int Care Injured 2009.
55. Syed AA. Distal femoral fractures: long term outcome following
stabilization with LISS injury. Injury Int Care Injured 2004; 35 : 599-607.
56. Tees FJ. Fractures of the lower end of femur. Am J Surg, 1937, 38:656-
659.
101
57. Umansky AC. Blade plate fixation for fractures of the distal end of
femur. Bull hosp Joint Dis 1948, 9:18
58. Wahner, Konrad L. Hoffmeier, Dipl-Ing et al. Internal fixation of
type –C distal femoral fractures in osteoporotic bones. JBJS (Am) 2010; 92:1442-52.
59. Wright M and Collinge C. Early results of less invasive stabilization
system for mechanically unstable fractures of the distal femur. J Orthop Trauma 2004:
18(8): 503-8
60. Wong MK, Leung F and Chow SP. Treatment of distal femur in
elderly using a Less Invasive Stabilization System. Int Orthop 2005; 29: 117-20.
61. Wagner M. General principles of clinical use of LCP. Injury. 2003;
34:5-B31-42.
62. Yeap EJ and Deepak AS. Distal femoral locking plate fixation in distal
femoral fractures. Malaysian orthopaedic journal 2007; 1:12-17.
63. Zickle RE, Hofeika P and Robbins DS. Zickle supracondylar nails for
fracture of distal end of femur. Clin Orthop 1986; 212: 217.
102