Embed Size (px)
Citation preview

A Novel Approach to Proactive Primary Care-Based Case Finding and Multidisciplinary
Management of Falls, Syncope and Dizziness in a One-Stop Service: Preliminary Results
Parry SW1,2, Hill H 3, Lawson J2, Lawson N 4, Green D5, Trundle H6, McNaught J7, Strassheim V1,
Caldwell A8, Mayland R9, Earley P10, McMeekin P11
1Institute of Cellular Medicine, Newcastle University UK
2Falls and Syncope Service, Newcastle Hospitals NHS Foundation Trust, Royal Victoria
Infirmary, Newcastle upon Tyne NE1 4LP UK
3The School of Dentistry, Manchester University UK
4Monkseaton Medical Centre, Whitley Bay, North Tyneside UK
5Institute of Neurosciences, Newcastle University UK
6Cramlington Sports Physiotherapy, North Tyneside UK
7Department of Physiotherapy, South Tyneside District General Hospital UK
8Age UK North Tyneside UK
9Tyne Health General Practice Federation, North Tyneside UK
10ITS Fitness, Newcastle upon Tyne, UK
11Faculty of Health and Life Sciences, Northumbria University, Newcastle upon Tyne UK
Corresponding author:
Dr Parry at the address above
1
1
2
3
4
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20

Phone: +44 191 282 5893
Fax: +44 191 282 5338
Email [email protected]; [email protected]
Alternative corresponding author:
Dr J Lawson at the address above
Phone: +44 191 282 5237
Fax: +44 191 282 5338
Email [email protected]
Funding Sources: Funding for service evaluation was from the UK Department of Health’s
Integrated Care Pilot (2009-2011).
Abbreviated Title: Proactive casefinding in falls in the community
Key words: Falls, syncope, elderly, community, screening
Word count: 3991 words
2
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36

Abstract (250 words)
National and international evidence and guidelines on falls prevention and management in
community dwelling elders recommend that falls services should be multifactorial, and their
interventions multicomponent. The way in which patients are identified as having had, or
being at risk of falls in order to avail of such services however is far less clear. We designed a
novel multidisciplinary, multifactorial falls, syncope and dizziness service model with
enhanced case ascertainment through proactive, primary care-based screening (of
individual case notes of those age 60 years and over) for individual falls risk factors. Our
service model identified 4039 individuals, of whom 2232 had significant gait and balance
abnormalities per senior physiotherapist assessment. We uncovered significant numbers of
patients with new diagnoses ranging from cognitive impairment through Parkinson’s disease
to urgent pacemaker indications. We found more than 600 individuals who were at high risk
of osteoporosis per FRAX score, 179 with benign positional paroxysmal vertigo and 50 with
atrial fibrillation. Through such screening and our approach, Comprehensive Geriatric
Assessment Plus (Plus falls, syncope and dizziness expertise), we targeted unmet need on a
scale far outside the numbers seen in clinical trials. Further work is needed to determine
whether this approach translates into improved falls, syncope and dizziness-related health
improvement.
3
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55

Introduction
National and international evidence and guidelines on falls prevention and management in
community dwelling elders1-4 clearly recommend that falls services should be multifactorial,
and their interventions multicomponent. The way in which patients are identified as having
had, or being at risk of falls in order to avail of such services however is far less clear. The
UK’s National Institute for Clinical Excellence (NICE) recommends that “older people who
present for medical attention because of a fall, or report recurrent falls in the past year, or
demonstrate abnormalities of gait and/or balance”2 be offered a multifactorial falls risk
assessment, while the American Geriatrics Society/British Geriatrics Society Falls Guidelines
suggest screening for falls during encounters with healthcare providers.1 However, there are
no studies addressing the issue of how patients are appropriately targeted for such an
assessment other than “present[ing] for medical attention”,2 with current practice
worldwide relying on opportunistic case ascertainment. The inherent flaw in this approach is
the assumption of a level of awareness in health and social care professionals, patients and
their carers that is manifestly absent. In consequence, patients with these problems do not
have the opportunity to improve their falls-related health and well-being, while health and
social services subsequently fail to reap the benefits of falls prevention. As falls cost more
than £1 billion (US $1.5 billion) in the UK alone,5 this is far from simply an academic issue.
In addition, the literature on the wider health and health economic benefits of multifactorial
falls interventions are poorly documented outside the realms of clinical trials. Indeed, there
are significant doubts regarding the cost effectiveness of such interventions6-10.
4
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78

The overlap between the falls, syncope and dizziness is well characterised.11-13 Each can be
mislabelled as the other, and effective management of the presenting symptom can only be
done with appropriate history taking and subsequent investigation and treatment taking
into account all three symptom complexes.
Our aim therefore was to design a novel multidisciplinary, multifactorial falls, syncope and
dizziness service model with enhanced case ascertainment through proactive, primary care-
based screening for individual falls risk factors. Through such screening, we hoped to target
unmet need on a scale far outside the numbers seen in clinical trials in this area, while
investigating the extent of unmet need in a sub-group of family practices and their patients.
In addition to falls-related diagnoses, we also wished to assess the impact of such screening
on case finding for additional diagnoses relevant to health promotion. as well as assessing
the financial sustainability of our service model by searching for clinical and cost changes.
5
79
80
81
82
83
84
85
86
87
88
89
90
91
92

Methods
North Tyneside Community Falls Prevention Service: Aims and Ethos
The North Tyneside Community Falls Prevention Service (NTCFPS) began in 2009, and its
aims were to provide falls and syncope prevention and management through a process of
proactive case ascertainment for those at risk of falls as well as those who had experienced
falls.1-4 Our ethos was one of upstream prevention, attempting to reach patients at risk
before falls had resulted in a downward spiral of increasing debility and dependency and
eventual care home placement.
1. Primary care-based population screening for falls risk factors
Primary care in the UK is provided by groups of general (family) practitioners (GPs) and
associated professionals with local population list sizes of up to 44,000 patients in each
general practice. The North Tyneside ward has a population of 192,000 people, 44,106 of
whom are over 60 years of age. North Tyneside has 29 general practices serving between
1,567 and 16,378 patients each. Unlike existing guidance where screening for falls relies on
questions asked during face to face healthcare encounters,1 our Service moved from one
practice to the next, screening all case notes of patients ≥ 60 years of age. Screening was
electronic (as all GP case records are now housed in electronic format), with scrutiny of
individual records by Service staff if there was any lack of clarity. The following falls and
syncope risk factors were screened for:
a. Four or more prescribed medications that are psychoactive and/or blood pressure
lowering, and excluding appliances, dietary products and minor ailments eg antacids,
topical dermatological agents
6
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116

b. Presentation to acute settings with falls or syncope in the previous 5 years
c. Fragility fracture (femoral neck, vertebra, wrist, pelvis, humerus) in the previous 5
years.
Patients were excluded if they were:
a. Unable to mobilise independently with or without a walking aid
b. Resident in a care home or housebound because of inability to walk
c. Already attending specialist services with relevant multidisciplinary expertise
including falls and Parkinson’s disease services.
d. Receiving palliative care.
Any patient with one or more of the falls and syncope risk factors from the initial screening
of GP case notes with no exclusion criteria were then sent a postal screening questionnaire
(Online Appendix) to further clarify risk. Patients answering no to Question 1, and yes to any
of the remaining questions, were then invited to an appointment at the Service.
NTCFPS team composition and service model
The NTCFPS multidisciplinary team comprised a geriatrician, health care assistant (HCA) and
senior physiotherapist. Patients were seen as a one-stop assessment using the
Comprehensive Geriatric Assessment model, with an emphasis on falls and syncope (CGA
Plus, the “Plus” referring to falls and syncope expertise). Patient pathways and assessments
and tests are provided in Figure 1. Each assessment was initially by the HCA and
physiotherapist with a comprehensive medical review by the geriatrician and actions as per
Figure 1, with advice to the patient supplemented by relevant information leaflets. The HCA
performed a baseline oscillometric blood pressure followed by beat-to-beat blood pressure
7
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140

and heart rate monitoring (CNAP 500, Graz, Austria) during active stand for three minutes to
look for orthostatic hypotension, a 12 lead ECG as well as visual acuity and relevant scale
per Figure1. The physiotherapy assessment comprised assessments of gait and balance
(visual assessment, timed up and go test,14 gait speed, five times sit to stand test15), hip
knee, ankle and foot range of motion and muscle power (resisted through range as per the
Oxford scale), neurological assessment of reflexes and dermatome/myotome sensation as
well as proprioception tests. Any highlighted abnormalities were examined in detail, for
example knee instability, hip/knee osteoarthritis, significant muscle weakness suggestive of
polymyalgia, myelopathy, spinal stenosis etc. The geriatrician review included a
comprehensive clinical assessment incorporating data from the physiotherapy and HCA
reviews. Diagnoses were based on clinical history taking, physical examination including for
example Dix-Hallpike manoeuvre, and supporting data from the HCA and physiotherapy
reviews. GPs retained control of onward specialist referrals with the exception of DEXA
scanning and day hospital referrals, which were requested by the NTCFPS. Patients with
severe fear of falling and/or significant gait and balance abnormalities were referred to our
voluntary sector partner (Age UK North Tyneside) for 10-week duration strength and
balance training classes with a bespoke exercise regime developed by senior
physiotherapists and a dedicated personal trainer. All patients received health promotion
advice on smoking, diet, alcohol intake and exercise in addition to individualised advice.
Data and Definitions
The Service database was housed on the SystmOne (TPP, Leeds UK) primary care database,
and was paperless other than the comprehensive care plan and surface ECG given to
patients and forwarded to GPs, and advice and exercise leaflets provided at the end of the
8
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164

assessment. The record included full symptom, history and examination details, GP
summary care record, test results, diagnoses and eventual care plan. A fall was defined as
coming to rest inadvertently on the ground or other lower level;1-4 syncope was defined as
transient loss of consciousness with loss of postural control and spontaneous recovery;12,13
drop attacks as sudden drops to the ground in apparent full consciousness in the absence of
a trip or a slip;16 and vertigo as a sensation of self-motion when no self-motion was
occurring, or the sensation of distorted self-motion during an otherwise normal head
movement.17 Significant gait abnormality was defined as gait speed less than predicted for
normal age and sex; pain, i.e. antalgic gait; and limp. Balance abnormalities were defined by
a five times sit to stand test score of > 14 seconds.14
Unmet need and audit of onward referral from general practice
Two of the top performing practices summary case records were scrutinized for reports of
falls and syncope and compared with patient self-report of these symptoms during their
assessment at the NTCFPS. We audited a random sample of 6 general practices for
compliance with NTCFPS recommendations regarding onward referral.
9
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182

Results
Population screened and subsequently reviewed at NTCFPS
The 19 participating general practices have a total patient list size of 153,424 patients. From
October 1st 2009 to January 31st 2013, we screened the individual case records of the 35,288
(23%) patients ≥ 60 years of age. Of these, 16,877 (11%) fulfilled initial screening inclusions
and exclusions and were sent screening questionnaires. Of these whom 11,476 (68%)
responded with 5,508 (48%) fulfilling criteria for invitation to attend the Service. Per our
screening criteria, none were known to existing falls specialist services. Four thousand and
fifty-one patients were seen at the Service, with complete records available for 4039; 2510
(62%) were female and the mean age was 74.9 years (standard deviation 8.4, range 59 -99
years, median 75 years). Presenting symptoms are found in Table 1 of the Online Appendix.
New diagnoses, conditions and issues relevant to falls and syncope and to national screening
targets
These are listed in Table 1 as well as the need for further action by patients, primary and
secondary care. Note these are new diagnoses not pre-existing. There were 347 patients
with a Mini-mental State Examination (MMSE)18 score of < 24/30, 360 patients with Geriatric
Depression Scale 15-item (GDS-15)19 score of ≥ 10 but the table lists only those with new
diagnoses referred back to the GP for further action.
Unmet need and onward referrals
10
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203

In addition to the unmet need evidenced by the new diagnoses, conditions and issues
presented in Table 1, results of screening of GP records compared to patient self-report of
falls and syncope are shown in Table 2 in the Online Appendix. Substantial numbers of
patients reported falls, syncope and dizziness that their primary care teams were unaware
of (Table 2, Online Appendix). Onward referrals following assessment at the Service with
examples of the reasons for referral are shown in Table 3 in the Online appendix. Ninety six
per cent of referrals had been made to secondary care per our suggestions in an audit of six
randomly selected practices.
11
204
205
206
207
208
209
210
211
212
213

Discussion
Our evidence-based natural experiment has shown clearly that a novel, primary care-based
case finding approach to falls prevention is not only effective in finding at-risk individuals
and uncovering a wide range of unmet clinical need. No previous study or service has, to our
knowledge, taken this approach. Case finding traditionally rests on falls interventions for
those who have already fallen and been referred to specialist services, and for those in
whom health care professionals have opportunistically noted falls risks. This approach
however fails to reach the majority of those at risk. With 30% of older people falling
annually,1-4 13,248 of the 44,160 individuals in the North Tyneside ward over 60 years of age
would be expected to fall each year. Local services see no more than 800 of these, with
neighbouring Newcastle and its more extensive falls services seeing around 1,100 new
patients with falls each year. There are no data to suggest that these are unusual figures.
Our review of GP records versus patient report (Table 2, Online Appendix) reinforces the
inadequacy of current approaches to falls case ascertainment, and echoes work on much
smaller samples.20 GPs are either unaware of their patients’ falls-related symptoms
(sometimes because patients and carers assume falls are a “normal” part of ageing), or do
not feel that further intervention is warranted, national and international guidance
notwithstanding. The unmet need, and by extension the effect on personal health and
health and social costs, is considerable. Our method of case finding provides the first
attempt to target this unmet need in a systematic and evidence based manner, with the
huge response to our postal screening questionnaire (68%) emphasising the importance of
these symptoms to patients.
12
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235

A significant number of individuals had new diagnoses relevant to the related symptoms of
falls, syncope and dizziness at the Service, alongside a high proportion of over 60s with
significant gait and balance abnormalities (2232 [55%]; Table 1). While our population was
screened for such issues, the extent of the problem and subsequent risk of falls and their
associated individual and societal costs is extraordinary. A recent cross sectional study in
488 community dwelling elders found impaired gait in only 32% of subjects,21 with a
systematic review of balance disorders recently finding a life time prevalence of dizziness of
17-30%.22 In contrast 44% of our patients suffered from dizziness, with the attendant risks of
falls and impaired quality of life.23
Similarly, the range and number of previously undiagnosed cardiovascular and neurally
mediated disorders was unexpected. We uncovered 13 immediate pacing referrals, 50 cases
of atrial fibrillation, and 106 individuals with bradycardia (as low as 32 beats per minute)
who required intervention for culpable medications. Thirty-seven patients with
asymptomatic bifascicular block and their GPs were counselled regarding rapid cardiology
assessment in the context of unexplained falls and syncope. In addition, there were 212
cases of neurally mediated syncope and 252 of orthostatic hypotension. As these were new
diagnoses, none had previously had the benefit of advice on how to abort and avoid
symptoms nor had their culpable medications reviewed. The common and treatable
peripheral vestibular disorder benign positional paroxysmal vertigo was found in 173
patients, many of whom had suffered years of disabling vertigo and accompanying falls
(Table 1).
13
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257

New cases of cognitive impairment and significant depression accounted for 334 individuals
in whom evidence suggests that interventions substantially improve quality of life and
clinical outcomes, as well as falls risks. More than 600 individuals were of intermediate to
high risk of osteoporosis per FRAX risk assessment, with initial audit of two practices
suggesting that 30% of these subsequently required drug treatment for osteoporosis, again
with significant effects on future bone health.
Our Service provided a “one stop shop” approach in all respects other than the associated
strength and balance training classes. In line with current recommendations,24,25 the classes
used aids like resistance bands, kettle bells and exercise balls to maximise strength and
balance. Just over 25% of our patients were referred, with 72% completing the 10-week
course. Initial analysis of 187 consecutive attendees at the classes showed a drop in mean
TUG from 15.3 seconds at baseline to 11.4 at week 10 (p< 0.001),26 though we have no data
on the longevity of this effect.
There is no guidance on which type of falls service using which skill and professional mix is
the most clinically and cost effective in preventing falls and their consequences. NICE for
example defines multifactorial as “An assessment with multiple components that aims to
identify a person's risk factors for falling”2 and as a result there are numerous
interpretations of what constitutes a multifactorial falls assessment, and no information on
which iteration is most beneficial to patients and the wider health economy. Much of the
available information from randomised studies suggest that a medical assessment is an
important component of any multifactorial assessment, but this is far from universal in
14
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280

clinical practice. In addition, there is a dearth of information on clinical and cost
effectiveness outside the realms of clinical trials, and even within research studies,
consistent and robust data are lacking.6-10, 27 Our study is the first to show the benefits of a
very specific multifactorial, multicomponent intervention in a real world setting in
uncovering previously unidentified and hence untreated falls, syncope and dizziness-related
risk factors and associated culpable diagnoses. The number of patients (4039) helps
outweigh the inherent weakness in observational data; in comparison, a recent meta-
analysis and systematic review of multiple component interventions for falls prevention
found only 18 suitable studies from 2002 – 2012, with a total of 5034 patients.4 Concerns
about the ability of randomised controlled trials in this area to reflect the potential benefits
of such multicomponent interventions rests on whether content, process and choice of
target group are accurately characterised and acted upon.28 All three components are
unambiguous in our study, with the consequence that there is no confusion over what has
been done and to whom. However, while the evidence base is robust in suggesting that our
Service should have improved fall and fracture rates,1-5 further work is needed to determine
whether this theoretical benefit translates into clinical practice.
Limitations
There are several major limitations to our study that do not preclude its message regarding
case finding for falls, syncope and dizziness. The very nature of a “one-stop shop” model
excludes within-service follow-up and attendant evidence of efficacy, and though we have
evidence of a high rate of onward referral to secondary care per our recommendations, we
do not have any further data on the outcome of these referrals; we also have no hard data
15
281
282
283
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303

on the total number of treatments for osteoporosis. In addition, while a great deal of time
and effort was spent on lifestyle, behavioural and dietary advice, it is impossible within our
current database and lack of follow-up to gauge the effect, if any, on our patients’ future
health from perspectives other than falls and syncope. Further work is needed to determine
if there is a longer term benefit of the Service to the population of older people in North
Tyneside and to explore attending health economic benefits of the intervention, such as cost
savings to the NHS or to wider public services.
Conclusion
In summary the NTCFPS was highly effective in case finding patients with falls, syncope and
dizziness symptoms who had not been seen by specialist services recommended by relevant
clinical guidelines. Not only did we uncover numerous modifiable risk factors for these
symptoms, the Service also found other diagnoses, conditions and issues relevant to health
and wellbeing promotion. To establish the health effect of the intervention will require
patient level data from those seen by the Service in comparison with matched patients who
have not been seen.
In conclusion, our approach, namely of case ascertainment with “CGA Plus” (the Plus
referring to falls, syncope and related expertise) uncovers a significant symptom burden
with accompanying disease processes and risk factors susceptible to evidence-based
modification. Further work is needed to examine the potential clinical and health economic
impact of such an approach. In conclusion, our approach, namely of case ascertainment
with “CGA-Plus” (the Plus in our case referring to falls, syncope and related symptoms), may
16
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326

be relevant to other symptom complexes in older patients, including for example shortness
of breath, with attendant health and health economic benefits. Further work is needed to
explore whether health benefits from this model become apparent when data is utilised
from individual patients in contrast to our approach of establishing effect at the level of the
regional population.
17
327
328
329
330
331
332
333

References
1. Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British
Geriatrics Society. Summary of the updated American Geriatrics Society/British
Geriatrics Society clinical practice guideline for prevention of falls in older persons. J
Am Geriatr Soc 2011;59(1):148-57.
2. Centre for Clinical Practice at NICE (UK). Falls: Assessment and Prevention of Falls in
Older People. London: National Institute for Health and Care Excellence (UK); 2013
Jun.
3. Gillespie LD, Robertson MC, Gillespie WJ et al. Interventions for preventing falls in
older people living in the community. Cochrane Database Syst Rev 2012;9:CD007146.
4. Goodwin VA, Abbott RA, Whear R et al. Multiple component interventions for
preventing falls and fall-related injuries among older people: systematic review and
meta-analysis. BMC Geriatr 2014 Feb 5;14:15.
5. Davis JC, Robertson MC, Ashe MC et al. International comparison of cost of falls in
older adults living in the community: a systematic review. Osteoporos Int
2010;21(8):1295-306
6. Peeters GM, Heymans MW, de Vries OJ et al. Multifactorial evaluation and treatment
of persons with a high risk of recurrent falling was not cost-effective. Osteoporos Int
2011;Jul;22(7):2187-96.
7. Robertson MC, Devlin N, Scuffham PE et al. Economic evaluation of a community
based exercise programme to prevent falls. J Epidemiol Community Health
2001;55(8):600-6.
18
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355

8. Church J, Goodall S, Norman R et al. The cost-effectiveness of falls prevention
interventions for older community-dwelling Australians. Aust N Z J Public Health
2012; 36(3):241-8.
9. Irvine L, Conroy SP, Sach T et al. Cost-effectiveness of a day hospital falls prevention
programme for screened community-dwelling older people at high risk of falls. Age
Ageing. 2010 Nov;39(6):710-6.
10. Jenkyn KB, Hoch JS, Speechley M. How much are we willing to pay to prevent a fall?
Cost-effectiveness of a multifactorial falls prevention program for community-
dwelling older adults. Can J Aging 2012;31(2):121-37.
11. McIntosh S, Da Costa D, Kenny RA. Outcome of an integrated approach to the
investigation of dizziness, falls and syncope in elderly patients referred to a 'syncope'
clinic. Age Ageing. 1993 Jan;22(1):53-8.
12. Moya A, Sutton R, Ammirati F et al. Guidelines for the diagnosis and management of
syncope (Version 2009). The Taskforce for the Diagnosis and Management of
Syncope of the European Society of Cardiology (ESC). Eur Heart J 2009;30(21):2631-
2671
13. Parry SW, Tan MP. An approach to the evaluation and management of syncope in
adults. BMJ 2010;34:c880.
14. Mathias S, Nayak U, Isaacs B. Balance in elderly patients: the get-up and go test. Arch
Phys Med Rehabil 1986;67(6):387–389.
15. Csuka M, McCarty DJ. Simple method for measurement of lower extremity muscle
strength. The American Journal of Medicine. 1985;78(1):77–81.
16. Parry SW, Baptist M, Kenny RA. Drop attacks in older adults: systematic assessment
has high diagnostic yield. J Am Geriatr Soc 2005;53(1):74-78.
19
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379

17. Bisadorff A, Von Brevern M, Lempert T et al. Classification of vestibular symptoms:
towards an international classification of vestibular disorders. J Vestib Res 19(2009)
1-13.
18. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for
grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189–
98.
19. Burke WJ, Roccaforte WH, Wengel SP. The short form of the Geriatric Depression
Scale: a comparison with the 30-item form. J Geriatr Psychiatry Neurol. 1991;4:173–
78.
20. Rubenstein LZ, Solomon DH, Roth CP et al. Detection and management of falls and
instability in vulnerable elders by community physicians. J Am Geriatr Soc
2004;52(9):1527-31.
21. Mahlknecht P, Kiechl S, Bloem BR et al. Prevalence and burden of gait disorders in
elderly men and women aged 60-97 years: a population-based study. PLoS One 2013
Jul 24;8(7):e69627.22.
22. Murdin L, Schilder AG. Epidemiology of balance symptoms and disorders in the
community: A systematic review. Otol Neurotol 2015 Mar;36(3):387-92.23.
23. Hsu LC, Hu HH, Wong WJ et al. Quality of life in elderly patients with dizziness:
analysis of the Short-Form Health Survey in 197 patients. Acta Otolaryngol 2005
Jan;125(1):55-59.
24. Sherrington C, Tiedemann A, Fairhall N et al. Exercise to prevent falls in older adults:
an updated meta-analysis and best practice recommendations. N S W Public Health
Bull 2011;22(3-4):78-83.
20
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402

25. Sherrington C, Whitney JC, Lord SR et al. Effective exercise for the prevention of falls:
a systematic review and meta-analysis. J Am Geriatr Soc 2008;56(12): 2234–43.
26. Parry SW, Earley P, Gray S et al. Timed up and go test results in patients found
through general practice falls risk screening. Preliminary evaluation of the North
Tyneside Falls Prevention Service (NTFPS) (abstr). Age Ageing Suppl 1 2014;A87.
27. Sach TH, Logan PA, Coupland CA et al. Community falls prevention for people who
call an emergency ambulance after a fall: an economic evaluation alongside a
randomised controlled trial. Age Ageing 2012;41(5):635-41.
28. Mahoney JE. Why multifactorial fall-prevention interventions may not work. :
Comment on “Multifactorial Intervention to Reduce Falls in Older People at High Risk
of Recurrent Falls”. Arch Intern Med 2010;170(13):1117-9.
21
403
404
405
406
407
408
409
410
411
412
413
414

Acknowledgments
The authors are grateful to the staff of Monkseaton Medical Centre, Whitley Bay and Albion
Road Resource Centre, North Shields for their administrative assistance.
Conflicts of Interest
The authors do not have any conflicts of interest to declare.
Conflict of Interest Checklist:
Elements of Financial/Personal
Conflicts
*Author 1
SWP
Author 2
HH
Author 3
JL
Author 4
NL
Yes No Yes No Yes No Yes No
Employment or Affiliation X X X X
Grants/Funds X X X X
Honoraria X X X X
Speaker Forum X X X X
Consultant X X X X
Stocks X X X X
Royalties X X X X
Expert Testimony X X X X
22
415
416
417
418
419
420
421
422

Board Member X X X X
Patents X X X X
Personal Relationship X X X X
Elements of Financial/Personal
Conflicts
*Author 5
DG
Author 6
HT
Author 7
JM
Author 8
VS
Yes No Yes No Yes No Yes No
Employment or Affiliation X X X X
Grants/Funds X X X X
Honoraria X X X X
Speaker Forum X X X X
Consultant X X X X
Stocks X X X X
Royalties X X X X
Expert Testimony X X X X
Board Member X X X X
Patents X X X X
23
423

Personal Relationship X X X X
Elements of Financial/Personal
Conflicts
*Author 9
AC
Author 10
RM
Author 11
PE
Author 12
PM
Yes No Yes No Yes No Yes No
Employment or Affiliation X X X X
Grants/Funds X X X X
Honoraria X X X X
Speaker Forum X X X X
Consultant X X X X
Stocks X X X X
Royalties X X X X
Expert Testimony X X X X
Board Member X X X X
Patents X X X X
Personal Relationship X X X X
24
424
425
426

Author Contributions
All authors apart from HH and PM contributed to the conception and design of the Service
and the recording, retrieval and interpretation of relevant data. HH and PM conceived,
designed and executed the clinical impact analysis. All authors thus had substantial
contributions to conception and design, acquisition of data, or analysis and interpretation of data;
drafting of the article and revising it critically for important intellectual content; and final review and
approval of the version to be published.
Sponsor’s Role
Not applicable.
25
427
428
429
430
431
432
433
434
435
436
437

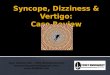
Figure 1: Patient pathway through North Tyneside Community Falls Prevention Service
*See Methods for further details
Abbreviations: MSK – musculoskeletal; TUG – Time up and go test; FTSTS – five times sit to
stand ; BP – blood pressure; FES-I – Falls Efficacy Scale International version; GDS 15 –
Geriatric Depression Scale, 15 item version; MMSE – Mini-Mental State Examination
26
Patient identified through primary care screening
New patient appointment in community falls service:Comprehensive Geriatric Assessment Plus
Physiotherapy review*[MSK examination,
TUG, FTSTS, gait speed]
Healthcare assistant review[ECG, beat to beat lying and standing BP, FES-I, GDS 15,
MMSE, visual acuity]
Geriatrician review including FRAX
Discharge with advice sheets, ECG and care plan copied to GP suggesting
onward specialist referral +/- referral to
strength/balance class
Discharge with advice sheets, ECG and care plan copied to GP re
medication changes +/- referral to
strength/balance class
Discharge with advice sheets, ECG and care plan, copied to GP +/-
referral to strength/balance class
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458

Table 1: New diagnoses, conditions and issues
Diagnosis, issue, condition (n = 4039) Number
Gait disorder 2232
Timed up and go test > 14 seconds 1217
Five times sit to stand test > 14 seconds 1514
Abnormal gait speed (> 1 metre per second) 975
Cognitive impairment (Mini mental state examination
score <24/30
184
Depression (Geriatric Depression Scale score ≥ 10/15) 150
Fear of falling (Falls Efficacy Scale International score >
23)
Mean FES-I score
2448
30
Culprit medications requiring review and modification 190
Benign positional paroxysmal vertigo 173
Orthostatic hypotension 252
Vasovagal syncope 196
Cough syncope 13
Micturition syncope 3
Low blood pressure (<100 mmHg systolic) requiring
further review
123
New heart murmur requiring further investigation 157
New atrial fibrillation 50
Symptomatic bradycardia requiring further
investigation
76
27
459

Asymptomatic bifascicular block flagged to patient and
GP
37
ECG and symptoms requiring permanent pacing 13
Corrected visual acuity >6/18 requiring optician review 210
28
460

Online Appendix
Online Appendix Table 1: Presenting symptoms to North Tyneside Community Falls
Prevention Service
N = 4039 Number (%)
Falls 2645 (65)
Drop attacks 126 (3)
Syncope 443 (11)
Dizziness 1763 (44)
Vertigo 520 (13)
29
461
462
463
464
465

Online Appendix Table 2: Comparison of general practice versus patient report of falls
Patients seen
at NTFPS
following
general
practice case
ascertainment
Number with falls
self-report (%)
Number with falls
recorded by GP
% of falls recorded by
GP of the number of
self-report falls by the
patient
Practice A 349 242 (69) 58 24
Practice B 213 136 (64) 0 0
Total 562 378 (67) 58 15
NTFPS – North Tyneside Falls Prevention Service
30
466
467
468

Online Appendix Table 3: Onward referrals and examples of clinical diagnoses requiring
referral
Referral to Number
(%)
Examples
General practice 1210 (25) Practice nurse blood pressure review,
medication change or review, onward
referral to secondary care, Hallpike
manoeuvre
Age UK strength and
balance training classes
1046 (25) Significant gait and balance abnormalities
DEXA scanning 616 (15) FRAX score suggesting high risk
Orthopaedic surgery 180 (4) Consideration for hip and knee replacement,
knee effusion, severe rotator cuff failure,
possible scaphoid fracture, knee joint
instability, spinal stenosis, Achilles tendonitis
and tears
Orthotics 71 (2) Knee brace, leg length discrepancy with gait
instability, new foot drop requiring ankle-
foot orthosis,
Day hospital
multidisciplinary review
110 (3) Frailty, gait and balance issues unsuitable for
classes, social and occupational health needs
Community physiotherapy 143 (3.5)
31
469
470

Community occupational
therapy
59 (1)
Neurology 107 (3) Occult stroke (eg undiagnosed hemianopia
and limb weakness, suspected recent
posterior circulation stroke), cerebellar
dysfunction, Parkinsonism, peripheral
neuropathy, foot drop, vestibular migraine,
REM sleep disorder, seizure disorder
Otolaryngology 57 (1) Benign positional paroxysmal vertigo, central
vestibular disorders, Meniere’s disease,
unexplained vertigo, tinnitus
32
471
472

Online Appendix: Screening questionnaire
Name: D.O.B:
Address:
Please tick Yes or No for each question:
Q1 Are you being seen by any specialist in a Falls or
Blackout service, or by the North Tyneside Hospital
Parkinson’s disease service? Yes No
Q2 Do you have problems with dizziness, lightheadedness Yes No
or balance that make you feel unsteady?
Q4 Have you had 2 or more falls in the last 3 years? Yes No
Q5 Have you had an unexplained blackout in the last 3 years? Yes No
33
North Tyneside Falls Prevention Service:
Keeping Older People Fit and Independent
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496

Q6 Have you suffered an injury because of falling,
tripping or blacking out in the last 3 years Yes No
Q7 Have you attended A&E (Accident & Emergency
Department at hospital) or seen your GP because of a
fall or blackout in the last 3 years? Yes No
Q9 Have you had a stroke that has affected your balance or Yes No
mobility?
Thank you for taking the time to complete this questionnaire. Please return in the envelope
provided.
34
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511