Embed Size (px)
Citation preview

†Trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA
INVANZ™†
(ertapenem)
Updated Results in Complicated Intra-abdominal Infections

2
Yellin AE et al. Int J Antimicrob Agents 2002;20:165-173. Solomkin JS et al. Ann Surg 2003;237:235-245. Pacelli P et al. Arch Surg 1996;131:641-645.
The Clinical Impact of Intra-abdominal Infection (IAI)
• Intra-abdominal infections are among the most common infections in general surgery.
• Surgery, supportive care, and antibiotic therapy are key in managing IAI.
• In a retrospective study of 604 patients, morbidity rates of 59% and mortality rates of 21% were reported.
IAI is a major cause of morbidity and mortality.

3
Treatment of patients for IAI is costly worldwide.
1. Walters DJ et al. Pharmacoeconomics 1999;16(5):551-561.2. Attanasio E et al. Dig Surg 2000;17:164-172.3. Cattan P et al. Eur J Clin Microbiol Infect Dis 2002;21:787-793.4. Davey P et al. Presented at the International Society of Pharmacoeconomics and Outcomes Research Sixth Annual
International Meeting, 2001. 5. Lyu R et al. Presented at the 10th International Congress of Infectious Disease, 2002.
The Economic Burden of IAI
US: USD$7678 to USD$12,523 per patient1
Italy: €1859 to €2324 per patient2*
France: €4625 to €15,548 per patient3
Scotland: £4190 to £7705 sterling per patient4
Australia: AUS$5053 to AUS$5316 per patient5
*Converted from Lira at the exchange rate on 10 March 2000, where 3.6 million Lira = €1859 and 4.5 million Lira = €2324.

4
Yellin AE et al. Int J Antimicrob Agents 2002;20:165-173. Solomkin JS et al. Ann Surg 2003;237:235-245.Mazuski JE et al. Surg Infect 2002;3:161-173. Fry DE. Surg Infect 2001;2(Suppl 1):S3-S11.
Appropriate Antibiotic Therapy for IAI
• Antibiotic therapy is an important adjunct to surgery and supportive therapy.
• Antibiotic treatment should cover appropriate gram-positive and gram-negative, aerobic and anaerobic bacteria.
• Most of the available antibiotics for the treatment of IAI generally require multiple daily doses or combination multidrug therapy to provide adequate coverage of all important pathogens.

5
Considerations in determining appropriate therapy:
Raymond DP et al. Surg Infect 2002;3:375-385.
Moellering RM. In: GL Mandell, JE Bennett, R Dolin, eds. Principles and Practice of Infectious Diseases, 5th ed, 2000.
Fry DE. Surg Infect 2001;2:S3-S11.
Defining Appropriate Therapy
• Spectrum of activity
• Timing of therapy
• Dose and dosing frequency
• Drug interactions and tolerability
• Adequate drug levels
• Prior antibiotic treatment
• Potential for engendering antibiotic resistance

6
Possible Outcomes of Appropriate Therapy
• Improved chance of successful clinical outcome
• Reduced mortality
• Probable decrease in need for re-operation and second-line therapy
• Probable reduction in number of IV antibiotic days
• Possible decrease in length of hospital stay
• Probable reduction in hospital costs

7
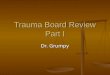
81.9%
58.9%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Empiric AntibioticTherapy Appropriate
(n=238)
Empiric AntibioticTherapy Inappropriate
(n=56)
Pati
en
ts w
ith
C
lin
ical
Su
ccess,
%
p<0.05
*Successful outcome was defined as resolution with no change in treatment.Davey P et al. Presented at the International Society of Pharmacoeconomics and Outcomes Research Sixth Annual International Meeting, 2001.
In an observational study (n=348) in patients with acute peritonitis, IAI patients with adequate empiric therapy were significantly more likely to have successful clinical outcomes.*
Appropriate Empiric Therapy for IAI: Successful Clinical Outcome

8
Appropriate versus Inappropriate Empiric Therapy for IAI: Mortality
In a retrospective analysis (n=365), mortality was substantially higher for IAI patients who received inappropriate versus appropriate therapy.
12%
23%
0.0%
10.0%
20.0%
30.0%
40.0%
Empiric AntibioticTherapy Appropriate
(n=290)
Empiric AntibioticTherapy Inappropriate
(n=75)
Mo
rtal
ity,
%
Bare M et al. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases, 2002.

9
Sendt W et al. Presented at the 12th Annual European Congress of Clinical Microbiology and Infectious Diseases, 2002.
In a retrospective study (n=425), patients given appropriate initial empiric therapy for IAI were less likely to undergo re-operation and require second-line antibiotic therapy.
Appropriate Empiric Therapy for IAI: Decreased Need for Re-operation and Use of Second-Line Therapy
Patient died
Resolved afterre-operation
Resolved withsecond-linetherapy
Resolved withinitial or step-down therapy
8157
12
27
311
4 5
0
20
40
60
80
100
Appropriate InitialEmpiric Antibiotic
Therapy
Inappropriate InitialEmpiric Antibiotic
Therapy
Per
cen
t

10
*This retrospective analysis of patients with complicated intra-abdominal infection appeared to show correlation between appropriateness of initial empiric therapy and days of antibiotic therapy.
Burke J et al. Presented at the 39th World Congress of Surgery, 2001.
12.1
10.6
10.0
7.5
0 2 4 6 8 10 12 14
Antibiotic Days
Median
Mean
In a retrospective analysis (n=428), appropriate treatment of IAI was associated with a decrease in antibiotic therapy days.*
Appropriate Therapy for IAI: Fewer IV Antibiotic Days
Inadequate Initial Empiric Therapy (n=38)
Adequate Initial Empiric Therapy (n=390)

11
22
12
0
5
10
15
20
25
Appropriate EmpiricAntibiotic Therapy
(n=129)
Inappropriate Empiric Antibiotic Therapy (n=33)
Len
gth
of
Sta
y (D
ays)
Davey P et al. Presented at the International Society of Pharmacoeconomics and Outcomes Research Sixth Annual International Meeting, 2001.
10 days
Appropriately treated IAI patients (n=348) experienced on average 10 fewer hospital days.
Appropriate Therapy for IAI: Decreased Length of Hospital Stay (LOS)

12
0
2,000
4,000
6,000
8,000
Ho
spit
al C
ost
s (P
ou
nd
s S
terl
ing
)
Mean
Medianp<0.05
* From 3 Scottish hospitalsDavey P et al. Presented at the International Society of Pharmacoeconomics and Outcomes Research Sixth Annual International Meeting, 2001.
Appropriately treated IAI patients (n=348) incurred significantly lower hospitalization costs versus inappropriately treated patients.*
Appropriate versus Inappropriate Therapy for IAI: Cost of Hospital Stay
£4190
£2862
£7705
£4770
Appropriate Empiric Antibiotic Therapy (n=129)
Inappropriate Empiric Antibiotic Therapy (n=33)

13
*Ertapenem is not appropriate for nosocomial infections where Pseudomonas and Acinetobacter spp. have been identified. Ertapenem had potent in vitro activity against the majority of the anaerobic clinical isolates tested; limited activity was noted against C. difficile. Methicillin-resistant staphylococci including Staphylococcus aureus (MRSA) and enterococci including Enterococcus faecalis and E. faecium are resistant.
Dorso KL et al. Presented at the American Society of Microbiology, 2002. Mazuski JE et al. Surg Infect 2002;3:161-173. Solomkin JS et al. Ann Surg 2003;237:235-245. Data on file, MSD.
Ertapenem: Appropriate Therapy for Intra-abdominal Infection
• US Surgical Infection Society (SIS) guidelines recommend ertapenem for patients with IAI
• Proven clinical efficacy
• Broad spectrum includes gram-positive and gram-negative aerobic and anaerobic pathogens*
– May eliminate the need for combination or multidose regimens
• Rapidly bactericidal (as shown in vitro)
• Proven tolerability profile
• Low risk for resistance selection
• Once-daily dosing simplifies administration

14
Was as effective as pip/tazo in complicated IAI. Appropriate gram-positive and gram-negative, aerobic and anaerobic coverage, appropriate for community-acquired polymicrobial infection.14* Ertapenem is active against ESBL and AmpC beta-lactamase-producing Enterobacteriaceae.15
Ertapenem
Limited anaerobic coverage that may require combination therapy.4 Possible high-level cephalosporin resistance among ESBL producers.5 Risk for selecting ESBL-producing and AmpC beta-lactamase-producing Enterobacteriaceae.6,7
Ceftriaxone
Resistance found among E. coli in some countries.1-3Ampicillin/sulbactam
Issues Agent
ESBL=Extended-spectrum beta-lactamase*Ertapenem is not appropriate for infections where Pseudomonas, Acinetobacter spp., MRSA, C. difficile, or resistant enterococci have been identified.
1Pelak BA et al. J Chemother 2002;14:227-33; 2Neuhauser MM et al. JAMA 2003;289:885-888; 3Mandell GL et al. Principles & Practice Infect Disease, 5th ed., 2000. 4Livermore DM et al. Antimicrob Agents Chemother 2001;45:1860-1867; 5Paterson DL et al. J Clin Microbiol 2001;39:2206-2212; 6Paterson et al. Ann Intern Med 2004;140:26-32; 7Livermore DM et al. JAC 2003; 52:331-344; 8Fridkin SK et al. Emerg Infect Dis 2002;8:697-701; 9Blázquez J. Clin Infect Dis 2003;37:1201-1209; 10Livermore DM. Clin Infect Dis 2002;34:634-640; 11Beaber JW et al. Nature 2004;427:72-74; 12Mazuski JE et al. Surg Infect 2002;3:161-173; 13Mazuski JE et al. Surg Infect 2002;3:175-233; 14Solomkin JS et al. Ann Surg 2003;237:235-245; 15Shah PM et al. J Antimicrob Chemother 2003;52:538-542.
Ertapenem: An Advantage Over Current Therapy
Fluoroquinolones Limited anaerobic coverage. Increasing prevalence of ciprofloxacin-resistant gram-negative bacilli.8 May select for or promote multidrug-resistant gram-negative bacilli.9-11
Piperacillin/tazobactam Expanded coverage (e.g., Pseudomonas) may not be advantageous in IAI; more useful in higher-risk patients.12-13
Aminoglycosides Not widely used due to risk of toxicity (e.g., ototoxicity, nephrotoxicity) and difficulty of obtaining therapeutic drug levels within a narrow therapeutic range.14

ErtapenemEfficacy in IAI

16
*Includes patients with severe infections, multiple infectious processes, and infections at different intra-abdominal sites.
Yellin AE et al. Int J Antimicrob Agents 2002; 20:165-173; Solomkin JS et al. Ann Surg 2003;237:235-245.
Ertapenem:Excellent Clinical Efficacy in IAI
• Proven as effective as piperacillin/tazobactam or ceftriaxone plus metronidazole in patients with IAI
• Effective across a broad range of pathogens, disease severities, and patient types* with complicated IAI requiring surgical intervention
• Proven tolerability profile
• An important advance because of the excellent efficacy, antimicrobial spectrum, tolerability, and once-daily dosing

17
Ceftriaxone2 g once a day
Metronidazole500 mg every 8 hours
Piperacillin/Tazobactam
3.375 g every 6 hours
In two worldwide clinical trials patients with complicated intra-abdominal infection were randomized to one of the following regimens:
Yellin AE et al. Int J Antimicrob Agents 2002; 20:165-173; Solomkin JS et al. Ann Surg 2003;237:235-245.
Intra-abdominal Infections
Ertapenem1 g once a day
Ertapenem1 g once a day
vs.
OR
vs.

18
Ertapenem1 g once a day
Ceftriaxone2 g once a day or 1 g twice a day
Metronidazole500 mg every 8 hours or
30 mg/kg every 6, 8, or 12 hr1
Piperacillin/Tazobactam
3.375 g every 6 hours or 4.5 g every 8 hours2
In two post-marketing clinical trials, patients with complicated intra-abdominal infection were randomized to one of the following regimens:
1Navarro N et al. Presented at 3rd ACCP, Oct, 2003; 2Dela Pena AS et al. Presented at 14th ECCMID, May, 2004.
Intra-abdominal Infections
Ertapenem1 g once a day
vs.
OR
vs.

19
Clinical Response at Test of Cure in Clinically and Microbiologically Evaluable Patients
Trial Ertapenem Comparator
Protocol 0041 (Phase II)
84% 85%*
Protocol 0172 (Phase III)
87% 81%**
OASIS-13 (Post-marketing)
90% 93%
OASIS-24,*** (Post-marketing)
97% 97%*
*Ceftriaxone + metronidazole;**Piperacillin/tazobactam; ***Following initial analyses, a post hoc analysis was conducted after correcting errors and missing data in the prior evaluability determinations.
1Yellin AE et al. Int J Antimicrob Agents 2002;20:165-173. 2Solomkin JS et al. Ann Surg 2003;237:235 245.
3Dela Pena AS et al. Presented at 14th ECCMID, May, 2004; 4Navarro N et al. Presented at 3rd ACCP, Oct, 2003.

“Ertapenem Monotherapy versus Combination Therapy with Ceftriaxone plus Metronidazole for Treatment of Complicated Intra-abdominal
Infections in Adults”
Albert E. Yellin, James M. Hassett, Alvaro Fernandez, James Geib, Ben Adeyi, Gail L. Woods, Hedy Teppler, and the Protocol 004 Intra-abdominal Infection Study Group
Published in International Journal of Antimicrobial Agents Vol 20, No. 3, September 2002, 165–173.

21
0
20
40
60
80
100
Su
cc
es
s r
ate
, %
Clinical and Microbiological Success (4–6 weeks post-therapy)
84% 85%
Yellin AE et al. Int J Antimicrob Agents 2002;20:165-173.
Ertapenem versus Ceftriaxone plus Metronidazole: High Microbiological and Clinical Success Rates at Test of Cure
Ertapenem 1 g once a day (n=31)
Ceftriaxone 2 g a day plusmetronidazole 500 mg every 8 hours (n=41)
Success rate was defined as clinical and microbiologic resolution of the index infection requiring no additional antimicrobial therapy.

22
87% (27 of 31)100% (20 of 20)B. fragilis
86% (30 of 35)86% (19 of 22)E. coli
Ceftriaxone(2 g once daily) plus metronidazole (500
mg every 8 hr) n=96
Ertapenem (1 g once daily)
n=59
Yellin AE et al. Int J Antimicrob Agents 2002;20:165-173.
Ertapenem versus Ceftriaxone plus Metronidazole: In a Clinical Study of Patients with Complicated IAI, Ertapenem Showed High Eradication Rates in Microbiologically Evaluable Patients

23Yellin AE et al. Int J Antimicrob Agents 2002; 20:165-173.
Ertapenem versus Ceftriaxone plus Metronidazole: Conclusions
In patients with IAI:
• Ertapenem, one gram, one dose, once a day, was effective compared with 2 g of ceftriaxone administered once daily plus 500 mg metronidazole administered in three divided daily doses.
• The tolerability of ertapenem was comparable to ceftriaxone plus metronidazole.

“Ertapenem versus Piperacillin/Tazobactam in the Treatment of Complicated
Intraabdominal Infections” Results of a Double-Blind, Randomized Comparative Phase III Trial
J. S. Solomkin, Albert E. Yellin, Ori D. Rotstein, Nicolas V. Christou, E. Patchen Dellinger, Jose M. Tellado, Osvaldo Malafaia, Alvaro Fernandez, Kyuran A. Choe, Alexandra Carides,
Vilas Satishchandran, Hedy Teppler, and the Protocol 017 Study Group
Published in Annals of Surgery Vol 237, No. 2, February 2003, 235–245.

25
Objectives of the Study
• To determine the clinical and microbiologic efficacy and tolerability of ertapenem one gram, once a day, for patients with complicated intra-abdominal infections, compared with piperacillin/tazobactam administered at 3.375 grams every 6 hours (with dose adjustments as per product label for patients with renal insufficiency)
• To analyze the adequacy of surgical source control as a component of evaluability in a prospectively generated and well-documented group of patients

26
Patients Randomized N=633
EarlyFinal
(test of cure)
Treatment (4–14 days) Follow-Up Assessment
Clinical Evaluation
Piperacillin/Tazobactam IV
3.375 gevery 6 hours
n=193
Piperacillin/Tazobactam IV
3.375 gevery 6 hours
n=310
1–2 weeks post-therapy
4–6 weeks post-therapy
Ertapenem1 g
once a day
n=323
1–2 weeks post-therapy
4–6 weeks post-therapy
Ertapenem1 g
once a day
n=203
Ertapenem versus Piperacillin/Tazobactam: Study Design
Solomkin JS et al. Ann Surg 2003;237:235-245.

27
Ertapenem 1 g once a day (n=203)
Piperacillin/Tazobactam 3.375 g every 6 hours (n=193)
Success rate was defined as clinical and microbiologic resolution of the index infection, requiring no additional antimicrobial therapy.
100
80
60
40
20
0
Su
cces
s ra
te, %
92%88% 87%
81%
End of IV Therapy(approximately 8 days)
Final Assessment(test of cure, primary endpoint; 4–6 weeks
post-therapy)
Data computed from statistical model adjusted for strata.
Ertapenem versus Piperacillin/Tazobactam: Over 90% Success Rate at End of IV Therapy
Solomkin JS et al. Ann Surg 2003;237:235-245.

28
41 (9/22)75 (15/20)Postoperative infection
74 (39/53)83 (50/60)Generalized peritonitis
88 (61/69)87 (65/75)Localized disease
50 (2/4)89 (8/9)Multiple abscesses
82 (55/67)90 (53/59)Single abscess
100 (10/10)92 (12/13)Biliary system
88 (7/8)100 (9/9)Stomach/duodenum
73 (8/11)85 (11/13)Small bowel
69 (25/36)78 (26/36)Colon
90 (102/113)89 (109/123)Appendix
Infection Site or Process
*Number of patients with favorable response assessment/total number of patients with assessment. Success required favorable clinical and microbiological responses, with success defined as requiring no additional antimicrobial therapy and favorable defined as absence of all causative organisms at the end of therapy.
Ertapenem versus Piperacillin/Tazobactam Showed Excellent Efficacy in Microbiologically Evaluable Subgroup
Solomkin JS et al. Ann Surg 2003;237:235-245.
Ertapenem 1 g once a day (n=203)
% (n/N)*
Piperacillin/Tazobactam 3.375 g every 6 hr (n=193)
% (n/N)*

29
*Pathogens in the B. fragilis group include B. caccae, B. distasonis, B. eggerthii, B. merdae, B. fragilis, B. ovatus, B. thetaiotaomicron, B. stercoris, B. vulgatus, and B. uniformis.
**n/N refers to the number of isolates with a favorable response/total number of isolates.
Ertapenem versus Piperacillin/Tazobactam: High Per-Pathogen Microbiologic Response Rates at Test of Cure (4–6 weeks post-therapy)
K. pneumoniae
90% (189/210)B. fragilis group*
90% (142/158)**E. coli
B. fragilis
Ertapenem
(n=203)
87% (65/75)
71% (12/17)
94% (193/206)
84% (114/135)
Piperacillin/Tazobactam
(n=193)
88% (60/68)
93% (13/14)

30Solomkin JS et al. Ann Surg 2003;237:235-245.
Ertapenem versus Piperacillin/Tazobactam: Conclusions
• Ertapenem, one gram, one dose, once a day, provided comparable efficacy to 13.5 grams of piperacillin/tazobactam administered in four divided daily doses
• Ertapenem can eliminate the need for combination and/or multidosing antibiotic regimens for the empiric treatment of intra-abdominal infections
• In patients with IAI, the tolerability profile of ertapenem was comparable to piperacillin/tazobactam

OASIS-1 and OASIS-2 Bowel Colonization Sub-studies

32
Bowel Colonization Sub-study Methods: OASIS-1
Friedland I et al. Presented at 13th ECCMID, Glasgow, UK, May 2003.
• OASIS-1 was a prospective, open-label, multicenter trial of ertapenem (1 g once a day) versus piperacillin/tazobactam (3.375 g every 6 hours or 4.5 g every 8 hours) in patients with intra-abdominal infection
• The objective of the bowel colonization sub-study of OASIS-1 was to compare the frequency with which ertapenem and piperacillin/tazobactam selected for resistant Enterobacteriaceae and imipenem-resistant P. aeruginosa
• Emergence of resistance was defined as resistant organisms detected at discontinuation of therapy but not present at baseline
• Rectal swabs were collected at baseline, discontinuation of therapy, and 2 weeks post-therapy
• Samples were shipped to Merck Research Laboratories for testing

33
• OASIS-2 was a prospective, open-label, multicenter, multinational trial of ertapenem (1 g once a day) versus ceftriaxone (2 g once a day or 1 g every 12 hours) plus metronidazole (30 mg/kg/day, in 2–4 divided doses) in patients with intra-abdominal infection
• The objective of the bowel colonization sub-study of OASIS-2 was to compare the frequency with which ertapenem and ceftriaxone plus metronidazole selected for resistant Enterobacteriaceae, ESBL-producing Enterobacteriaceae, and imipenem-resistant P. aeruginosa (n=450)
• Rectal swabs were collected at baseline, discontinuation of therapy, and follow-up (2–4 weeks post-therapy)
• Samples were shipped to Merck Research Laboratories for testing
Bowel Colonization Sub-Study Methods: OASIS-2
Navarro N et al. Presented at 3rd ACCP, October 2003. Friedland I et al. 3rd ACCP, Santa Margherita, Portofino, Italy, October 2003.

34
CTZ
ETP
P/T
IMP
Microscan
ESBL Test
Double Disk Test
Bowel Colonization Sub-study: Testing Methods in OASIS-1
E-test
Artistic RenditionCTZ = ceftazidime, ETP = ertapenem, IMP = imipenem, P/T = piperacillin/tazobactam, ESBL = extended-spectrum beta-lactamase. Friedland I et al. Presented at 13th ECCMID, Glasgow, UK, May 2003.

35
CTZ
CRO
ETP
IMP
Microscan
ESBL Test
Double Disk Test
Bowel Colonization Sub-study: Testing Methods in OASIS-2
E-test
Artistic RenditionCTZ = ceftazidime, CRO = ceftriaxone, ETP = ertapenem, IMP = imipenem, ESBL = extended-spectrum beta-lactamase. Friedland I et al. 3rd ACCP, Santa Margherita, Portofino, Italy, October 2003.

36
ertapenem (1 g once daily); n=152
piperacillin/tazobactam (3.375 g every 6 hr or 4.5 g every 8 hr); n=153
*p<0.00, **At baseline, n=169 (ertapenem) and n=172 piperacillin/tazobactam; DCOT=Discontinuation of therapy.Friedland I et al. Presented at 13th ECCMID, Glasgow, UK, May 10-13, 2003.
Enterobacteriaceae resistant to study drug
OASIS-1 Sub-analysis in Patients with IAI (n=341): Low Risk for Resistance Selection among Enterobacteriaceae in the Bowel
Baseline** DCOT Any time after therapy
initiated
No
. of
Pat
ien
ts
0(0%)1(0.6%) 1(0.7%)*
0
5
10
15
20
25
18(11.8%)*
1(0.7%)*
21(13.7%)*

37
P. aeruginosa resistant to imipenem
Baseline DCOT
DCOT and/or TOC
Ertapenem 0/169 (0%) 0/152* (0%) 0/153* (0%)
Piperacillin/tazobactam 2/172 (1.2%) 1/153 (0.7%) 1/153 (0.7%)
Friedland I et al. Presented at 13th ECCMID, Glasgow, UK, May 10-13, 2003.
OASIS-1 Sub-analysis in Patients with IAI (n=341): Low Risk for Resistance Selection among P. aeruginosa in the Bowel
Ertapenem did not select for imipenem-resistant P. aeruginosa in the bowel.
DCOT=Discontinuation of therapy; TOC=Test of cure, 2 weeks post therapy.
*One patient had an imipenem-intermediate P. aeruginosa at discontinuation of therapy.

38
Enterobacteriaceae resistant to study drug
ertapenem (1 g once daily); n=196
ceftriaxone (2 g, once a day or 1 g twice daily) plus metronidazole (30 mg/kg/day in 2–4 divided doses after loading dose of 15 mg/kg); n=193
*p<0.001Friedland I et al. 3rd ACCP, Santa Margherita, Portofino, Italy, October, 2003.
OASIS-2 Sub-analysis in Patients with IAI (n=389): Low Risk for Resistance Selection among Gram-Negative Bacilli in the Bowel
Baseline DCOT DCOT and/or TOC
No
. of
Pat
ien
ts
1(0.5%)4(2.1%)
1(0.5%)*
31(16.1%)*
1(0.5%)*
50(25.9%)*
0
10
20
30
40
50
60

39
OASIS-2 Sub-analysis in Patients with IAI (n=389): Low Risk for Resistance Selection among Enterobacteriaceae in the Bowel
ESBL-producing E. coli or Klebsiella spp.
ertapenem (1 g once daily); n=196
ceftriaxone (2 g, once a day or 1 g twice daily) plus metronidazole (30 mg/kg/day in 2–4 divided doses after loading dose of 15 mg/kg); n=193
*p<0.001Friedland I et al. 3rd ACCP, Santa Margherita, Portofino, Italy, October, 2003.
Baseline DCOT DCOT and/or TOC
No
. of
Pat
ien
ts
8(4%)
4(0.5%)
1(0.5%)*
18(9.3%)*
5(2.6%)*
39(20.2%)*
0
5
10
15
20
25
30
35
40

40
P. aeruginosa resistant to imipenem
Baseline DCOT
DCOT and/or TOC
Ertapenem 0/196 (0%) 2/196 (1%) 2/196 (1%)
Ceftriaxone plus metronidazole 0/193 (0%) 0/193 (0%) 0/193 (0%)
OASIS-2 Sub-analysis in Patients with IAI (n=389): Low Risk for Resistance Selection among P. aeruginosa Bacilli in the Bowel
Friedland I et al. 3rd ACCP, Santa Margherita, Portofino, Italy, October, 2003.
Imipenem-resistant P. aeruginosa were rarely detected in the ertapenem-treated group.
DCOT=Discontinuation of therapy; TOC=Test of cure, 2 weeks post therapy

41
Ertapenem:Low Risk for Resistance Selection
• The emergence of ertapenem-resistant Enterobacteriaceae in the bowel after ertapenem treatment was low (<1%)
• Emergence of piperacillin/tazobactam-resistant and ceftriaxone-resistant Enterobacteriaceae in each treatment group was significantly higher at discontinuation of therapy (p<0.001)
• ESBL-producing Enterobacteriaceae decreased in the ertapenem group but increased in the ceftriaxone group during and in the 2 weeks post-therapy (p<0.001)
• Imipenem-resistant P. aeruginosa were rarely detected in the ertapenem group at discontinuation of therapy (<1%)

ErtapenemTolerability Profile

43
Tolerability Profile: Incidence (%) of Drug-Related Clinical Adverse Experiencesa Reported in 1% of Patients Treated with Ertapenem in Clinical Studies
1%1%1%Phlebitis/thrombophlebitis
3%6%5%Infused vein complications
Local1%2%1%Vomiting1%1%2%Headache2%3%3%Nausea2%7%5%Diarrhea
Systemic
Ertapenemb,c 1 g
once a dayn=1022
Piperacillin/ Tazobactamb
3.375 g 4 times a day n=775
Ceftriaxonec,d 1 or 2 g once a day plus metronidazole
500 mg every 8 hours n=183
aDetermined by the investigator to be possibly, probably, or definitely study-drug relatedbIncludes patients with renal dose adjustmentscMay include patients randomized to 1 g but dose adjusted to 2 gdIncludes patients who received metronidazole
Skin and Skin AppendagePruritis 1% 1% 1%Rash 1% 2% 1%

44
Tolerability Profile: Incidence (%) of Drug-Related Laboratory Adverse Experiencesa Reported in 1% of Patients Treated with Ertapenem in Clinical Studies
0 4% 4%Alkaline phosphatase (>2.5 x ULN)
1% 4% 3%Platelet counts (<75,000)
5% 5% 5%AST (>2.5 x ULN)
5% 4% 5%ALT (>2.5 x ULN)
Ceftriaxonec,d
1 or 2 g once daily plus metronidazole
500 mg every 8 hours (n=41)
Piperacillin/ Tazobactamb
3.375 g 4 times daily
n=750
Ertapenemb,c 1 g
once a day n=1766
ALT = alanine transaminase AST = aspartate transaminase
ULN = upper limit of normal
aDetermined by the investigator to be possibly, probably, or definitely study-drug relatedbIncludes patients with renal dose adjustmentscMay include patients randomized to 1 g but dose adjusted to 2 gdIncludes patients who received metronidazole

45
No clinically relevant drug interactions were reported in the clinical program to date.*
*Monitoring of valproic acid levels should be considered if coadministered with carbapenems.
Ertapenem: Drug-Drug Interactions
In vitro, Ertapenem:
• Does not inhibit metabolism mediated by any of the six major CYP-450 isoenzymes
• Is not an inhibitor of, nor a substrate for, P-glycoprotein–mediated transport

46
*There are inadequate data on the safety and efficacy of ertapenem in patients with advanced renal insufficiency (creatinine clearance 30 mL/min/1.73 m2) to support a dose recommendation. Therefore, ertapenem should not be used in these patients.
Ertapenem in Special Populations*
No dose adjustments recommended:
• In elderly patients
• In patients with hepatic insufficiency
• In patients with mild or moderate renal insufficiency* (creatinine clearance >30 mL/min/1.73 m2)

47
*There are inadequate data on the safety and efficacy of ertapenem in patients with advanced renal insufficiency (creatinine clearance 30 mL/min/1.73 m2) to support a dose recommendation. Therefore, ertapenem should not be used in these patients.
Solomkin JS et al. Ann Surg 2003;237:235-245; Cunha BA et al. Drugs of Today 2002;38(3):195-213.
Once-a-Day Dosing Advantages
One-gram*, once-a-day dosing:
• Reduces the number of IV antibiotic medication doses patients may receive compared with multidose regimens
• May decrease the possibility of misdosing

Microbiology

49
Prevotella spp.Porphyromonas asaccharolyticaPeptostreptococcus spp.Eubacterium spp.Clostridium spp. (excluding C. difficile)Bacteroides fragilis group
Anaerobic Microorganisms
Streptococcus pneumoniae*Streptococcus agalactiaeStaphylococcus aureus (MSSA)
Aerobes and Facultative Anaerobic Gram-Positive Microorganisms
Moraxella catarrhalisKlebsiella pneumoniaeHaemophilus influenzaeEscherichia coli
Aerobes and Facultative Anaerobic Gram-Negative Microorganisms
MSSA = methicillin-susceptible S. aureus *Ertapenem is not appropriate for nosocomial infections where Pseudomonas and Acinetobacter spp. or E. faecalis and E. faecium have been identified. The efficacy of ertapenem in the treatment of community-acquired pneumonia due to penicillin-resistant S. pneumoniae has not been established.
Ertapenem: Active against Important Pathogens in IAI*

50
Ertapenem: Highly Active In Vitro against Clinical Isolates in Trials
Pip/tazo = piperacillin/tazobactam *B. fragilis, B. distasonis, B. uniformis, B. avatus, B. vulgatus, B. thetaiotaomicron. **Only methicillin-susceptible S. aureus are included because these agents are considered ineffective against methicillin-resistant S. aureus regardless of MIC. Friedland I et al. J Chemother 2002;14:483-491.
9932.499.4
112816
0.5322
0.015–80.06–1280.03–128
Ertapenem (479)Ceftriaxone (281)Pip/tazo (509)
B. fragilis group*
10099.695.5
0.0160.125
8
0.0160.06
2
0.008–0.060.03–64
0.125–128
Ertapenem (759)Ceftriaxone (461)Pip/tazo(404)
E. coli
100100100
0.2544
0.2541
0.125–0.51–8
0.125–8
Ertapenem (187)Ceftriaxone (43)Pip/tazo (144)
S. aureus**
10091.993.4
0.030.25
8
0.0160.06
4
0.008–0.250.03–641–128
Ertapenem (149)Ceftriaxone (74)Pip/tazo (61)
Klebsiella spp.
% Susceptible
90%50%RangeAgent (No. isolates)
Organism
MIC (g/mL)

51
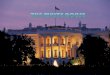
Ertapenem: Rapidly Bactericidal In Vitro against ESBL- E. coli
Kill Rate vs. ESBL- E. coli CL 9305
0 2 4 6 8 10 12 14 16 18 20 22 24
1010
108
106
104
102
1Time (Hours)
CF
U/m
L
Ertapenem 10 μg/mLCeftriaxone 28 μg/mLPiperacillin/Tazobactam 11.5/1.4 μg/mLGrowth Control
CFU/mL Reduction (log10)
24 Hours5.565.345.26
6 Hours5.565.343.57
ErtapenemCeftriaxonePiperacillin/Tazobactam
ESBL= Extended-spectrum beta-lactamase CFU = colony-forming unitsDorso K et al. Presented at the American Society of Microbiology, May 2002, Salt Lake City, Utah, USA.

52
Ertapenem: Rapid In Vitro Bactericidal Activity against ESBL+ E. coli
Kill Rate vs. ESBL+ E. coli CL 12082
0 2 4 6 8 10 12 14 16 18 20 22 24
1010
108
106
104
102
1
Time (Hours)
CF
U/m
L
Ertapenem 10 μg/mLCeftriaxone 28 μg/mLPiperacillin/Tazobactam 11.5/1.4 μg/mLGrowth Control
CFU/mL Reduction (log10)
24 Hours
5.30
4.25
Growth
6 Hours
5.30
2.10
Growth
Ertapenem
Ceftriaxone
Piperacillin/Tazobactam
ESBL = Extended-spectrum beta-lactamaseCFU = colony-forming unitDorso K et al. Presented at the American Society of Microbiology, May 2002, Salt Lake City, Utah, USA.

53
Ertapenem: Rapidly Bactericidal against AmpC-Producing E. coli
CFU = colony-forming unitDorso K et al. Presented at the American Society of Microbiology, May 19-24, 2002, Salt Lake City, Utah, USA.
CFU/mL Reduction (log10)
24 Hours
5.52
5.35
Growth
6 Hours
5.52
3.05
1.29
Ertapenem
Ceftriaxone
Piperacillin/Tazobactam
Kill Rate vs. AmpC + E. Coli
0 2 4 6 8 10 12 14 16 18 20 22 24
1010
108
106
104
102
1
Time (Hours)
CF
U/m
L
Ertapenem 10 μg/mLCeftriaxone 28 μg/mLPiperacillin/Tazobactam 11.5/1.4 μg/mLGrowth Control

Dosing

55
Dose Schedules of Selected Antibiotics in IAI*
* Based on recommended dose for average adult patient. Dose adjustment may be required for some patients. For complete information, please consult full prescribing information for the specific product.There are inadequate data on the safety and efficacy of ertapenem in patients with advanced renal insufficiency to support a dose recommendation. Therefore, ertapenem should not be used in these patients.
** Or in equally divided doses twice a day.
Physicians’ Desk Reference© 57th ed. Montvale NJ: Medical Economics, 2003 [Rocephin® and Zosyn® prescribing information].
Ertapenem: Convenient One-Gram*, Once-a-Day Dosing
1**
4
1–2 g
7.5 mg/kg
Ceftriaxone plusMetronidazole
43.375 gPiperacillin/tazobactam
11 g*Ertapenem
Doses Per DayDoseAgent

56
Conclusions
Ertapenem represents an advance in treatment:
• Proven clinical efficacy of carbapenems in treating IAI
• Broad-spectrum coverage of the gram-positive and gram-negative aerobic and anaerobic pathogens implicated in IAI
• Rapid bactericidal activity in vitro
• Low risk for resistance selection
• Proven tolerability profiles with no clinically relevant drug interactions reported in the clinical trial program*
• Simplified once-a-day regimen that may simplify patient management and reduce the cost of patient care
* Monitoring of valproic acid levels should be considered if coadministered with carbapenems.

57
References
1. Data on file, MSD__________.2. Shah PM et al. Ertapenem, the first of a new group of carbapenems. J
Antimicrob Chemother 2003;52:538-542.3. Solomkin JS et al, for the Protocol 017 Study Group. Ertapenem versus
piperacillin/tazobactam in the treatment of complicated intraabdominal infections. Results of a double-blind, randomized comparative phase III trial. Ann Surg 2003;237:235-245.
4. Dorso KL et al. In vitro kill rates of ertapenem, ceftriaxone (CRO) and piperacillin/tazobactam (pip/taz) against intra-abdominal pathogens. American Society of Microbiology, May 19-24, 2002, Salt Lake City, Utah, USA [poster A-156].
5. Mazuski JE et al. The Surgical Infection Society guidelines on antimicrobial therapy for intra-abdominal infections: An executive summary. Surg Infect 2002;3:161-173.
6. Pacelli P et al. Prognosis in intra-abdominal infections. Multivariate analysis on 604 patients. Arch Surg 1996;131:641-645.
7. Yellin AE et al. Ertapenem monotherapy versus combination therapy with ceftriaxone plus metronidazole for treatment of complicated intra-abdominal infections in adults. Int J Antimicrob Agents 2002;20:165-173.
8. Fry DE. Basic aspects of and general problems in surgical infections. Surg Infect 2001;2(Suppl 1):S3-S11.
9. Walters DJ et al. Cost effectiveness of ciprofloxacin plus metronidazole versus imipenem-cilastatin in the treatment of intra-abdominal infections. Pharmacoeconomics 1999;16(5 Pt 2):551-561.
10. Attanasio E et al. Cost-effectiveness study of imipenem/cilastatin versus meropenem in intra-abdominal infections. Dig Surg 2000;17:164-172.
11. Cattan P et al. Cost of care for inpatients with community-acquired intra-abdominal infections. Eur J Clin Microbiol Infect Dis 2002;21:787-793.
12. Davey P et al. How important is appropriate empirical antibiotic treatment for intra-abdominal infections? Presented at the International Society of Pharmacoeconomics and Outcomes Research (ISPOR) Sixth Annual International Meeting; Virginia, USA, 2001.
13. Lyu R et al. Burden of hospitalizations among patients undergoing surgery for intra-abdominal infections in Australia between 1993 and 1999. Presented at the 10th International Congress of Infectious Disease, Singapore; 2002.
14. Moellering RC. Principles of anti-infective therapy. In: GL Mandell, JE Bennett, R Dolin, eds. Principles and Practice of Infectious Diseases. 5th ed., Churchill Livingstone, Philadelphia, 2000, pp. 223-235.
15. Raymond DP et al. Preventing antimicrobial-resistant bacterial infections in surgical patients. Surg Infect 2002;3(4):375-385.
16. Bare M et al. Excess mortality associated with inappropriate initial empiric antibiotic therapy in patients undergoing surgery for intra-abdominal infection. Presented at the 12th European Congress of Clinical Microbiology and Infectious Diseases (ECCMID), Milan, Italy; 2002.
17. Sendt W et al. Association between inappropriate initial empiric antibiotic therapy and the need for reoperation and second-line therapy among German patients undergoing surgery for community-acquired intra-abdominal infections. Presented at the 12th Annual European Congress of Clinical Microbiology and Infectious Diseases (ECCMID), Milan, Italy; 2002.
18. Burke J et al. Effect of adequate empiric antibiotic therapy on outcomes among patients with complicated intra-abdominal infections. Presented at the 39th World Congress of Surgery, Brussels, Belgium; 2001.
19. Livermore DM et al. Properties and potential of ertapenem. J Antimicrob Chemother 2003;52:331-344.
20. Goldstein EJ et al. Comparative in vitro activities of ertapenem (MK-0826) against 1,001 anaerobes isolated from human intra-abdominal infections. Antimicrob Agents Chemother 2000;44:2389-2394.
21. Livermore DM et al. In vitro activities of ertapenem (MK-0826) against recent clinical bacteria collected in Europe and Australia. Antimicrob Agents Chemother 2001;45:1860-1867.
22. Fridkin SK et al. Temporal changes in prevalence of antimicrobial resistance in 23 U.S. hospitals. Emerging Infect Dis 2002;8:697-701.
23. Pelak BA et al. Comparative in-vitro activities of ertapenem against aerobic bacterial pathogens isolated from patients with complicated intra-abdominal infections. J Chemother 2002;14(3):227-233.
24. Mazuski JE et al. The Surgical Infection Society guidelines on antimicrobial therapy for intra-abdominal infections: Evidence for the recommendations. Surg Infect 2002;3:175-233.
25. Neuhauser MM et al. Antibiotic resistance among gram-negative bacilli in US intensive care units. Implications for fluoroquinolone use. JAMA 2003;289:885-888.
26. Paterson DL et al. International prospective study of Klebsiella pneumoniae bacteremia: Implications of extended-spectrum beta-lactamase production in nosocomial infections. Ann Intern Med 2004;140:26-32.
27. Blazquez J. Hypermutation as a factor contributing to the acquisition of antimicrobial resistance. Clin Infect Dis 2003;37:1201-1209.
28. Livermore DM. Multiple mechanisms of antimicrobial resistance in Pseudomonas aeruginosa: Our worst nightmare? Clin Infect Dis 2002;34:634-640.
29. Beaber JW et al. SOS response promotes horizontal dissemination of antibiotic resistance genes. Nature 427:72-74.
30. Paterson DL et al. Outcome of cephalosporin treatment for serious infections due to apparently susceptible organisms producing extended-spectrum β-lactamases: Implications for the clinical microbiology laboratory. J Clin Microbiol 2001;39:2206-2212.
31. Physicians’ Desk Reference© 57th ed, Montvale NJ: Medical Economics, 2003 [Rocephin® and Zosyn® prescribing information].
32. Dela Pena AS et al. Ertapenem versus piperacillin/tazobactam for the treatment of intra-abdominal infections (IAI) requiring surgical intervention (OASIS-1): Results of a prospective, randomized, open-label study. 14th European Congress of Clinical Microbiology and Infectious Diseases, Prague, Czech Republic, May 2004 (Poster).
33. Navarro N et al. Ertapenem versus ceftriaxone/metronidazole for the treatment of intra-abdominal infections (IAI) requiring surgical intervention (OASIS-2): Results of a prospective, randomized, open-label study. 3rd Antimicrobial Chemotherapy and Clinical Practice, San Margherita, Italy, October, 2003 (Poster 20).
34. Friedland I et al. Isolation of resistant faecal enterics in patients treated with piperacillin-tazobactam vs ertapenem. 13th European Congress of Clinical Microbiology and Infectious Diseases, Glasgow, UK, May 2003 (Poster 789).

58
References (cont’d)
35. Friedland I et al. Emergence of resistant gram-negative bacilli in the bowel of patients treated with ceftriaxone/metronidazole vs. ertapenem for intra-abdominal infections. 3rd Antimicrobial Chemotherapy and Clinical Practice, Santa Margherita, Portofino, Italy, October, 2003 (Poster 57).
36. Cunha BA. Ertapenem. A review of its microbiologic, pharmacokinetic and clinical aspects. Drugs of Today 2002;38(3):195-213.
37. Friedland I et al. In vitro activity of ertapenem against common isolates in relation to human pharmacokinetics. J Chemother 2002;14:483-491.
38. Goldstein EJ et al. Comparative in vitro activities of ertapenem (MK-0826) against 469 less frequently identified anaerobes isolated from human infections. Antimicrob Agents Chemother 2002;46(4):1136-1140.
39. Wexler HM et al. In vitro activities of MK-826 (L-749,345) against 363 strains of anaerobic bacteria. Antimicrob Agents Chemother 2000;44(8):2222-2224.

Before prescribing, please consultthe manufacturers’ prescribing information.
Merck does not recommend the use of any product in any different manner than as described in the
prescribing information.
Copyright © 2004 Merck & Co., Inc., Whitehouse Station, NJ, USA. All rights reserved. 7-05 IVZ 2004-W-6334-SS Printed in USA
VISIT US ON THE WORLD WIDE WEB AT http://www.merck.com
INVANZ™(ertapenem)Updated Results in Complicated
Intra-abdominal Infections
59