Embed Size (px)
Citation preview

~~
..t'-- CL -l 'Z K-10
Review
Sr. J. Surg. 1993. Vol. 80. June,689-704 Prophylaxis of postoperative
thromboembolism with lowmolecular weight heparins
To evaluate the thromboproph}'lactic use of 1011' molecular 11!eightheparins (LMWHs), publications fi"om 27 orthopaedic trials -and 35studies of patients undergou1g general or gynaecological surgerj' 11'erescrutulized and subjected to a partial meta-anal)'sis. In orthopaedicsurgery, LMTVHs 11!ere superior to placebo or de.\"tran and at least asefficient as ul¡jI"actionated heparill il1 the prerention of Jeep veinthrombosis (D VT). Compared 11'ith ul¡jI.actionated heparin, one of theLMWH preparations significantly reduced the total incidence of DVT.The rafe of non-fatal pulmonary embolism 11:as 0.49 per cent in patientsreceiving L.l¡.fTVH and 1.22 per cent in controls. Seren orthopaedicpatients (0.15 per cent) died fi.om puhnonary embolism, none of 1\'homreceived LMWH. -, -.
~ w1jl'actionated, did marta/ir}' rafe, nor
did they cause haemorrhage. LMWHs proz."ide sale and efficient
pr°J!/~.,:is by~dl1~nistration 01~t!ail})"
L. N. Jorgensen,P. Wille-Jorgensen*and O. Hauch*
Department of SurgicalGastroenterology, HvidovreHospital and *Department ofSurgical Gastroenterology K,Bispebjerg Hospital, University of
Copenhagen, Copenhagen,Denmark
Correspondence lo:Dr L. N. Jorgensen, Department of
Surgery, Sundby Hospital,DK-2300 Copenhagen S, Denmark
suppression of platelet aggregation by LMWHs8 and theiraffinity for several plasma proteins are less pronounced9.
During the past 7 years, se\eral clinical studies usingLMWHs for thromboprophylaxis in surgical patients have beenpublished. Controlled trials ha\e been carried out with thefollowing LMWH products: Fluxum (Alfa LMWH; AlfaFarmaceutici, Bologna, Italy), C]exane (Enoxaparin; Rhóne-Poulenc Rorer, Gennevilliers, F rance), F ragmin (Dalteparin;Kabi Pharmacia, Stockholm, S\\'eden), Fraxiparin (CY 2]6;Sanofi, Paris, France), Logiparin (Tinzaparin; Novo Nordisk,Bagsvrerd, Denmark) and Sandoparin (Sandoz LMWH;Sandoz, Nuremberg, Germany). Although there are differencesbetween the LMWHs usedlO, the type of operations and themethods of screening for DVT, the present aim is to obtain anoverall impression of the clinical value of LMWHs inthromboprophylaxis by analysing the available data.
Methods
To diminish the risk of publication bias! 1, this analysis triedto include all published reports, including abstracts fromconferences, of randomized control]ed trials using LMWHs forthromboprophylaxis in orthopaedic, general or gynaecologicalsurgery. Trials in which the recently developed heparinoids ordermatan sulphates were evaluated were not included. Thesurvey ofthe literature included a computer-aided MEDLINEsearch from 1980 to 1991, a search of the reference lists ofrelevant papers by two of the authors (L.N.J., P.W.-J.)independently, and a contemporary computer-aided search ofCurrent Contents (field: Clinical Practice and Life Sciences)until the end of 1991. The following keywords were used: lowmolecular weight heparin, heparin, deep venous thrombosis,thromboembolism, pulmonary embolism, surgery and ortho-paedic surgery. When data were missing from published reports,the authors responsible for correspondence were contacted. Ifno answer was received, a reminder wa5 sent after 1 month. Ifthe data were still not forthcoming, the study was excluded
The use of conventionallo\\'.dose unfractionated heparin is awell established method in the prevention of postoperativethromboembolic complications. The administration of lowdoses of heparin has reduced the incidence of postoperativedeep vein thrombosis (DVT) and even fatal pulmonaryembolismJ.2. Ho\\.ever, some types of surgery, especiaIJyorthopaedic, stiIJ carry an unacceptably high risk of DVT,reported by some to be about 30 per cent despite the use ofunfractionated heparin in combination with dihydroergotamine(DHE )3. Furthermore, the administration of unfractionatedheparin is associated with certain side-effects such as anincreased bleeding tendency (albeit seldom of clinicalsignificance), aIJergic manifestations, aIteration of plateIetfunction and changes in levels of lipoprotein lipase and liver
lipase4.Unfractionated heparin is a heterogeneous mixture of
molecules of different molecular weights, ranging from 3 to40 kDa, and with varying amounts of specific biological activitydepending on molecular structure and size. Low molecuJarweight heparins (LMWHs) are derived from unfractionatedheparin by either enzymatic cracking or filtration; LMWHsare believed to possess les ser effects on overaIJ clotting asreflected in activated partial thromboplastin and thrombinclotting time assayss.
Experimental studies have led to the theory that antifactorXa actiyity correlates with antithrombotic efficacy, whereasantifactor lIa activity relates to the influence on bleeding.LMWHs have ]ess abi]ity to inactivate thrombin re]ative totheir capacity to inhibit factor Xa, as the inactivation ofthrombin by heparins is dependent on the size of the heparinmo]ecu]e. The specific antifactor Xa:antifactor lIa activity ratiofor LMWHs is thus higher than for unfractionated heparin.Therefore, in equipotent antithrombotic doses, LMWHs shouldcause less bleeding than unfractionated heparin; this has beenverified on]y in animal mode]s6. 7. Compared with unfractionatedheparin, LMWHs exhibit a different pharmacokinetic profilewith a longer half-]ife and higher bioavailability. Also, the
6890007-1323,193/060689-=16 :r: 1m Butterworth-Heinemann Ltd

r¿¡¡¡11111
Low molecular weight heparins: L. N. Jorgensen et al.
Table 1 Dl:finition o/ high-qualit)' studies (011 criterio must be met)
DVT diagnosisOrthopaedic surgery
l. Venography2. J 2-'I-radiolabelled fibrinogen uptake test with or without
impedance plethysmography, or plasmin scintimetry ifpositive results are verified with venography for all the tests
General or gynaecological surgeryl. Venography2. 12~I-radiolabelled fibrinogen uptake test
Follow-up~ 7 days for regular DVT screening and ~ 30 days for verificationof symptomatic DVT, symptomatic pulmonary embolism or death
Completion of triall. No or limited selection of patients2. < 15% of patients drop out after inclusion
Bleeding and transfusionComplete data on amount and type of bleeding, and transfusion
, requirements,
DVT. deep vein thrombosis
of follow-up and drop-out rate (Table 1), a separation wasmade into two cJasses of scientific quality (high and low). Whendifferent studies had uniform selection of patients and doseregimen, some results were evaluated by combining the datain 2 x 2 tables (Mantel-Haentszel-Pet02.12.13 method); thisallows comparison across studies to obtain an overview of theefficacy and safety of LMWHs compared with different controltreatments. Only results from trials with uniformity in theselection of patients and dose regimen were analysed in thisway. For each study, the number of observed events (O) (DVTor pulmonary embo)ism) in patients treated \\-ith LMWH wascompared with the number expected (E) if the treatmenthad an effect that was identical with that in the control group.With reference to the variapce (V ar) of each trial, thedifferences (O -E) were summed and a X2 test applied to evaluatewhether the number of observed events differed significantlyfrom the number expected if the treatments did not differ.Two-tailed analyses were used, irrespective of the fact thatone-tailed statistics had been employed in some publications.Typical odds ratios derived from exp[}:; (O-E}}:; Var(O-E)],with the 95 per cent confidence interval derived fromexp[}:; (O -E)!}:; Var(O -E)]:t 1'96/}:; \Tar(O -Ef/2, are
presented2.Tests for heterogeneity have not been performed, since these
lack statistical power and a certain degree of heterogeneity isalways present2.14. Instead, heterogeneity has been evaluatedfrom the graphical presentation ofthe odds ratios for each trial.The overall typical odds ratios are presented in this forro onlywhen derived from studies of similar design using identical
pharmaceutical products.In the evaluation of the prophylactic effect on DVT, each
drug was tested separa tely against each main group of controls:placebo, dextran and unfractionated heparin. Three patientpopulations were assessed, undergoing: elective major ortho-paedic operations, hip fracture surgery, and general surgeryincJuding abdominal, thoracic, vascular, urological andgynaecological procedures. Studies in which the dose of therespective LMWH tested differed considerably from therecommendations of the manufacturer were excJuded from theanalysis. No regard was made to supplementary prophylactictreatment (e.g. compression stockings or DHEJ if it \vas usedin both the LMWH-treated and control groups. Two sets ofanalyses \vere carried out: the first incJuded all studiesirrespective of quality and the ~cond evaluated onlyhigh-quality investigations. The same I methods \vere appliedwhen the effects on the incidence of pulmonary embolism anddeath were examined.
Results
Orthopaedic surgeryReports of 27 investigations were found. In most trials, patientsundergoing elective hip arthroplasty or hip fracture surgerywere studied. Without prophylaxis these patients are consideredto carry a risk of DVT of approximately 50 per cent, and arisk of pulmonary embolism and fatal pulmonary embolism of1-2 per cent and 2-10 per cent respectively15.
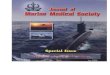
Controls receiring placebo. Compared with placeta, threeLMWHs have in separate trials pro ved to be significantlysuperior with respect to prophylaxis of DVT 'in patientsundergoing elective hip arthroplasty3.16, knee arthroplasty ortibia!. osteotomyl7, or repair of femoral neck fracture18(Table 2). Although not all the trials show significantdifferences, the individual odds ratios all point towards athromboprophylactic effect of the LMWH that is better thanthat of placeta, irrespective of the quality rating (Figure 1). Intwo studies3.19 the LMWH was supplemented with DHE;graded compression stockings were used in both treatmentgroups in one triaI2°. In all studies reporting the incidence ofproximal DVT, a reduction was found in the active treatmentgroup3.16.17.20; this was statistically significant in three3.r6.17.
from the respective statistical calculations, but still reported,AIso excluded from the analysis were dose-finding studieswithout a control group given another prophylactic treatmentfor comparison.
The efficacy endpoints assessed were the objectively verifiedincidences of DVT and pulmonary embolism. Only controlledtrials using objective paraclinical diagnostic methods, such asvenography, 12SI-radiolabelled fibrinogen uptake test, plethys-mography, 99Tc-radiolabelled plasmin scintimetry and thermo-graphy for the detection of DVT, and pulmonary scintigraphy,pulmonary angiography and autopsy for the verification ofpulmonary embolism, were included; the authors are awarethat not all of these tests are adequate for diagnosis. Theincidence of DVT was based on results of venography in allthe studies that applied this method to a majority of patientsfor the verification of DVT (after initial detection by screeningwith another objective diagnostic method). In a substantialproportion of studies, separation of results into proximal anddistal DVT was not presented: for this reason the total incidenceof DVT has been considered. Whenever the relevant data wereprovided, the incidences of DVT, pulmonary embolism anddeath were derived from the complete period of follow-up, notjust that ofthromboprophylaxis or hospital stay. The incidenceof DVT was based on patients completing the trial protocoloWhenever possible, data describing the incidences ofpostoperative pulmonary embolism, postoperative mortality,bleeding complications and transfusion requirements werederived from all patients randomized in the respective trials(i.e. analysis on an intention to treat basis). This was done toavoid the bias that occurs in certain trials from excludingpatients beca use of severe bleeding episodes or death beforecompletion of the trial.
Side-effects such as bleeding complications and requirementfor transfusion were not uniformly recorded in the differenttrials. The studies were scrutinized for significant differences inthe total amount ofbleeding and transfusions given, irrespectiveof. the time after operation. Bleeding complications includedintracranial and gastrointestinal episodes, wound haematomaand significantly raised total blood loss (perioperative andpostoperative, including volume in drains). Injection haema-tomas were not considered in the analysis. A distinction wasmade between statistically significant differencesand tendenciesbetween treatment groups. Whenever there was a significantindication of (1 ) a higher incidence of life-threatening bleedingepisodes, (2) wound haematoma requiring evacuation or(3) discontinuation of prophylaxis because of bleeding,differences between the groups were considered clinicallyrelevant. Transfusion was expressed as the total sum (calculatedas the number ofunits oferythrocyte-containing blood productstransfused) given during the period of prophylaxis.
In some analyses relating to diagnóstic methods, duration
Br. J. Surg., Vol. 80, No. 6, June 1993690

J. Surg..
Vol.
80,
..§.~'"~'"t>~~"'"~,.,.~~;:i;,.:sM..:c..¡-
E1=
o~
~S
E
..Jc ..
..1~
>
~c
I~
~
.J
o8~ ~1
0Q
. ""
§'~-
~~c..:? ~
:I: "~
~~
c..J~ ~jJ
'5-="
c." E~
8
~::;
o ~o; E.:
~~
;~
O
"
¡¡~~~ ~I
~~
Ic
'" :¿¡¡"B.J
~
~
-c.~-c.
:f: ~
:f:
-:¡ ~
-:¡
~ ~
= -
¡¡ ~
~ ~
lo.
6. June 1993
¡
1c~c~~
..,'-
-"
) ! if il
~;- ~.,.
;Jj
5-]
l!~"8 ~
~~
~
i!i
li i~
~;:.~
~~ J
~ ;
"é¡-
=-
i.c
!! c
" =
~
" c
~o:¡
~;~:!.~;1,
~ .'oa~'o\; ~e.~
Low
molecular
weight
heparins: L
-~'"1.::¡
~..=c
~ ~'"'¿¡
..} ~§.
~'-
E
x~
~
'02 ~
8E
-1c
uu
>.
"0--..u
c':0
E-;;o.
1-1:
I~>
~
-
Q
~
'o'
...
~6~
c.~~~~
2 +
- --
~
-N=
X_X
;1:." "x:x"..E..
~x
=0
So,,~
"~
~...
"o o
'"~
'"~
~ -=
]. ~
~
~
g.~
g..9.-'=
- \.;
"" -'
-'
o ¡¡"
E..:~~
5..~"
1~
~
~ ~
" ¡JJ
=
::)
;:- ;:-
;:- ;:-
c.~
c.~
c.~
c.~:E
"Q.:E
"Q.:E
"Q.:E
"E.
"o "o
"o "o
>~
>~
,.~>
~--=
--=
--=
--
-a~
-a~
-a~-a~
~
~
~
~
~
I~~
..
..o,. =
5 ~
-;;"~ Ec."~cc
~
i¡:..oc~
~'"u~~
~ E;-~S~i::"
¡;: J0rgensen et
al
~ I
"O~13 5->0->
-E
ü8 ::
~¡j
=;¡;o
] ~
: "2
.cc.~
o
~=
-"'"=
0=
0u V
~~~
~.cc.o.~~
5.o."=
u
u ->
"~
~1-":;¡;¡:""~o;~]~E
~o
=:r. ~-c= "¡¡ E>
"0.:::
;.."
".~
1-->
5Q
o.;0
=
u
"o".c¡¡.~.c
~-".c
~oou
.¡¡ ¡:,
~
uo:.:r.
-:;¡:,"
~u
u
o~E "~
~o';:-.~;¡:
~~
=~
.:!-,.9 >
-;2-
!~..:¡¡~
>
" --'""
~~
o~
."00-=
~
c¿,,+-
'" .0-c--~-~
.0-=
..,.,." .~
:J:=
~~
~c-'~
~
" o
~:B
'ñ.c
" c
-c "
c ::
~~
~ "
"'"=
~
~-o
:@]
!! "
~.c0-:=
-0."o-c.U"E
~E
~
~;,
&:a
~o
-c"'~"É
.:;:'..~~
~c ~
= =
" ~
~;;~
e~
o
~E
.o e.::-~c;:i3
o-=
..2 C
~~I ~
691

Low molecular weight heparins: L. N. J0rgensen et al.
a non-sígníficantly higher incidence of bleeding complicationsin the LMWH-treated group, which did not lead to dis-continuation of prophylaxis for any patient1S.l0. Similarly,transfusion requirements were slightly higher in the groupreceiving active treatment in these studies.
~co
"O
"¿;
c.,1/)c.,0\Lo~~
c"E0\lO..
u.
~o.
~...Q¡
cQ¡'"'"
ro..J~
C'i:roQ.
.gCro
ti)
.-,.,..:c...Q,
Cal
11)11)lO
-J~
C.;:lOQ.O
"CClO
ti)
'"'"'O
tE
"O.cLo
¡!~
c'E:01lOLo
LL
o'"~...~CGI'"'"'"-J
c'ca'5>o
-J
~'O-~"¿;
CJ
Q"-:J
f-
QJc:la)(QJ
U
"O
'¿;
ULo"
Ü"-J
'"c:lOX'"
U100
10
.grc..1"'
1'01'010 0'1
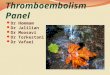
Colltrols receiving dextrall. Three LMWHs have beencompared with dextran in patients undergoing hip arthro-plasty23-26 (Table 3). The administration of C.lexane,Fragminand Logiparin caused a reduction in the incidence of DVT,which was statistically significant for Clexane and Fragmin(Figure 3). In one investigation25 only a limited reduction wasfound (odds ratio 0'71), which may be related to use of aninsufficient dose of Logiparin (35 rather than the recommended50 antifactor Xa unitsjkg daily). The incidence of proximalDVT was not significantly lowered in any trial.
There were only a few pulmonary embolisms and deaths,and no indication of a reduced incidence of either inLMWH-treated patients. In two of the studies=3.=4 the amountof bleeding was found to be significantly higher in patientsgiven dextran.
!
I' i
0.01
Figure 1 Prophylacfic (:tf~cr I!fWII' molecular lI'eighr heparins (lI'i/h orlI'i/houl dihydroergorallline) versus placebo lI'irh respecr lO Jeep rein!Ihrombosi,~ in or/hopaedic ,~urger.1" Bar,f are 95 per cen/ colljidence!inrerral,~, * Hip ,frac//lre ,~urgery
«"'~
"o
'¿;
r:"2"01'-~~
r:E01.,
¡j:
«~~
'O.."c:.,'"'"
ro-J
c:°;::roQ.o
"Cc:~
ti)
~",o-
~c:CJti)ti)'"
-J~
~
';::'"O-o
"Oc:'"
(/)
",'""'"~...QJ
E"o-.cLo~
1-~
.oS
EO>
10Lo
Lj.
~o'"~tcalti)ti)lO
-J
C'ClOQ.
'0,O
-J
"o''¿j
U1-CI
UCI
..J~
alCro)(al
U
'"
-o..."CJ
5-Lo:J1-~
'"C
10X'"
U
100
10
~ti)Lo 1
'""Q
!"Q
10 0.1
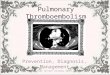
Co/ltrols recen'ing unfractionated heparin I¡"ith or II"ÍthoUIdihydroergotamine. The antíthrombotíc efficacy of LMWHscompared wíth unfractíonated heparin has been evaluated ín18 trials (Table 4), mostly on patíents undergoíng electíve híparthroplasty. Overall, LMWHs exhíbíted an effect on theíncidence of DVT at least as great as that of unfractíonatedheparin. Indeed, ín 11 of 14 híp arthroplasty IríaIs the oddsratío was < 1.0, favouring the useofLMWHs (Figure 4). Whena meta-analysís ofthe results from the two hígh-quality studíescomparing Clexane wíth unfractíonated heparin 15000 unitsper day was performed, a sígnificant reduction ín the DVT ratewas found ín patíents treated wíth Clexane (odds ratío 0,67(95 per cent confidence ínterval (c.Í.) 0.47-0.96)). Treatmentof the control group ín the Fragmin studíes was not homo-geneous, makíng stratíficatíon necessary. The typícal odds ratío(95 per cent c.Í.) for the trials ofFragmín agaínst unfractíonatedheparin 5000 uníts subcutaneously three tímes daily was 0,54(0'27-1.11)31.32 and 0.65 (0.27-1.57) (both P not signíficant)for studies wíth controls receívíng unfractíonated heparin 5000uníts plus DHE 0,5 mg subcutaneously twice daily33.34. Thus,there is evidence that Fragmín ís at least as efficíent as theseconventíonal prophylactíc regímens.
Compared wíth unfractíonated heparin-DHE, Fragmínappears to be at least as antíthrombotíc33.34 (T able 4). The
..
--,
.0--'"~
'6"
~
u'"
:::'=
~~
'1:'=O-'c>o
..;
,..~'"~...~c:o
'"'"
~"..~c:
"§O)
10
¡J:
O-O' L.,'"~
"¿:"
u'"N
ro~c:'í::roQ.
'o,O
-J
Figure 2 Prophylactic t:[fect of 101\' malecular I\'eight heparins (\I'ith or
\l1thout dihydroergotamine) versus placebo \11th respectto mortality rate
in orthopaedic surger.,. Bars are 95 per cent confidence imeroals. .Hip
fracture surgery,.,~'"
(,)
'IJ]Q~
alc:lO)(al
U.~
1- I--
It is worth noting that in two trials the prophylactic treatmentwas initiated after surgeryI6.17. To the authors' knowledge thesestudies, including that of Levine and colleagues21 , are the onlyreports on postponing the start of LMWH prophylaxis untilafter surgery.
With respect to the incidence of pulmonary embolism, nooveral1 tendency was detected between the groups when patientsundergoing elective surgery were analysed3.16.1 7,20,22; however,the three cases of fatal pulmonary embolism were confined tothe placebo-treated group in the two hip fracture studiesl8,19(Table 2).
When mortality was evaluated, great heterogeneity betweenthe trials was obvious and no overall tendency shown(Figure 2). For this reason, meta-analysis was omitted.
In only one study was there a significantly higher operativeblood loss in patients receiving LMWH compared with that inthe placebo-treated group3 (Table 2). Two other trials reported
Figure 3 Effect o[ lo", molecu/ar ",eight heparins versus dextran on theincidence o[ deep vein thrombosis in e/ective hip arthroplasly. Bars are95 per cent confidenfe interva/s
Br. J. Surg., Vol. 80, No. 6, June 1993692

c-'"O:
S'""~~~-::~~.~
}~'"'§c.:¿
I;:~~'"'"~~::~'""'"t:-.~;:~-::
~.~::..;:~"~~~::~-.J
~":E"¡-
~
I-:C~
>
3: ~
Q
~
~~
.J
o8~15 ...
¡¡ ~
-c
~
"O
N
-=
~=O
-
" -c
=
~:;
~
:E
~
o
~
..¡ o
'o]~
5.g>
.'ü
~.sg
~
~E
"O
..,
-~
~~
c
Oo.
8 N
~:s
O
5~
E
al!~ 'S
~[
o
~2"5~ ---o. -
"8 E
1
:Ss
iS
:1:~~
o
.?: .J
o..t:o
N~
..,..,"óO
~"~c.2
~]
-=-
N~
~
=
~~
! ~
":;E.~
~ ::.
-x
.i ~
=
N-"
U-X
c
~.
"~
i ~
%-
1c
w-~o"
~"-~
-
"8 1-
-c.~
O
"E
~
~
~
~ i~
~;,
...5:"
~
>
¡;i5
¡;: >
=
=
=~
2.
"B
j ¡f ¡f ft I ¡f ¡f Jt fi
~
;;u
u¡¡
="D
~
~
-'
~~:::;
.~'o'" ~~'"óo ~'Oo ~'oo-...;;o:
=xx~""
~'6o ~'5o ...NX.~~ ~
..':~'-~~:¡::.,
-,"=~
~
oN
~
'o 'o
...~
~
~'o
'o"'
r-
~
~'o
'o-o ~
¡'o
'oo
o
~
~'o
'oM
O
~
!i'o
'oo
-~.;~
. "E
x ~
~
;;,~
. ~
N
r,¡"
"8
~~
, ~
N
N
5 §
~ !
:E:
c."~g~o-::
::-~
"E
.
I ~
i- =
~
"...>..~~
-'
-' "
~
~c:
¿
:! ~
Br. J. S
urg.. Vol. 80. N
o. 6. June 1993 ~'oo-.x~x~ ~x~.~ >
,.c;-~~¡::-~ .-'oN-"~~~
~"5oNX'"~~~~~ -x~! !-~ ~'" 8'o'"' lB'oo :z'oo i3'"5o~~~= ...
a- ~
..,
.., ..,
-o'o
'o 'o
.., N
a-
--r-o
"6 "6
"6o
o - c
'o 'o
'oo
o o
~
~
.!x
x x
§ ~
. §
'" N
'"
=
=
=~
~
~
E ~
E
~'oo>,
-=;-t.o~~-c.t::~ ~M'"5...
~'oo=~~~~ ~-5]~';'<
~'o~.N -¡¡"c~ ~§~ o--c'o'" $'o~'-c~~~ ~xX'"'
"'. .,~~=¡¡;>...
'lc.~
c.~' ~
:=-o.:=
-o.~
i~ jl! ."."'oo ~'ooNX'":rO;"E
..~
. ""x~~ 2 ~... ~'o-o "§2~.¡.
..~
~t.E-g1]
r--o
~~
~.,-
-o N
".o;
EE
~
e.p.=
.."85
~-
."c --
~
u ~
~
ü~
o'""
u -
w.=
:. -o~
~'6.., 'D~'o...-."~~ -x;;~~ ~~~s~~c;'"""~~~
~~'o~ ...~'oo~'c.".'o-~~,:;r-<::'" r...
,0.'::~
o.
~.E
i; ;~
.
>.
~;:.g;;
§~!f; ~:::~x
§-
~ a Low
m
olecular w
eight heparins:
L. N. Jorgensen
et al
~'o~N ;!'6:::
;;- '"
"'- '"
"'0;3
'o-o::. -
~'o ~':o'" ~'ot""~"5'.. "-~~¡¡;> -O
'
'.~~~j -.
;e-
~~
~
~ ~
~i
&~
&
~&
~""
~~
~~ i~
I
~'Qo ~'oo'..-c.
8..,~~g;';'
~N N'"'o'" I'5 '"'"'oo&i~~! ,.x""'"';¡~
:~
g i
i -;;
ju j~ l~
i~ i
..,...'o'" ~'o ~'6o ~'oo ~'ooNX'"'~
~"E.
~~ f-:¡lo.
+O'--
-;¡
~~'o '"..,'oo ..,..,'O '"...'oo~~a,=~¡::-?;
..,..,'o~ '"..,'o~. o
~"to'"
"-xc
~ ~
!;'i~
15
-'J ~
, ~ ~
x =
c.
-¡j ~
~ ~
~ ~'o~ '"'"'oo ='oQ a'oe ~'oQ~
~"E
. "E
.8
8~
~
¡: x
¡: x
" "
c.", c.",
2z ~
z~
o 50
ti: ti:
~'o~
-"~,.-'
c.~Q
.~
É-~
~
.c" "
u ~
;
~,:
~~
:; t r:"sQ ~'o.~'o;:¡
~'o~ o ~'o ..'o'"'"xw:I:o~"E.
~~
-;; -;;
.c .c
g- g-
;, ;,
~~
~
~~
~
~ ~
E =
E
=~
.. ~
..o:
o:""~~.J
;;~ ~-
~~
;:~OM
~e;¡~~':'.
-~-"o'"2:;
:;)-"'~:~o~"'-
B~
~'"0"-
...s
N~--~"ó~
~~
...;;;--:,!
'O~
N.o
~::.
":; -
~R
~
o -
c.~~
~
:É:C
"F:.~
~
~uo~
~
u>
-g~
::
~~
~~
~¡¡j
.:
-¡¡~
~-
-"..~
~0-0
N~
~¡
'o:'~
¿ N~¡'o~
OQ
~
..r---~-"o'"-c~
=--~o..,
.-'"~
:2
..,:::;:¿o'¡:j~
"'~~
':=.o
"'cC-
B
-=
I
"~8~
"'C"'~
" ,,>
-iS
.E-"
=~
~~
c50,E~
"",o~
~~
.5 -.:;.".g g ~
: 8-.,,:oC
'~.!!..~
...]-~
~..~~
~
"O ~
:;
~'Q
~"'~
..o ..c
~~
.c="
::- >."" '"
:: ~
-;;..;~
.2~",
~ 1:'~
."~
!!.~~
=~
oc~
S!~
=~
;
~
~u~
=."
~~
+.C
~E
~:::~
o. ~
~~
~
O"
~
O-""
c~
.0.."~
o:¡:~~
-~:"~
,,~
c'
c u
;;)S!¿
=,.
"-;;..J;'.::-;,;~
~.
~-o.~
-
.8~
E~cÜ"
u
O
~
O
=E
u-=.o
o~~
~o
~
c -..~
.c-co.!l-"'000;c
!J ::!. ~
u
~:o",~
g~
o""e-°°.cE""v.."o-o;;..-iS
.t-":.
~ E
>
..O'"
" ~
0.."
~
-0=
>.
.-0.,,=">
.~co
E:
8 +
+'"
C
~
..++
~
.
o u..
.~
=u>
.>.
..-~
~
"=
;'",~-o
E~
:¡:!:oJ2
.~
~""
~I~
!!~~
'..J
0-
u ~
~
"
~cu.81:
-ou.c O
"'E-.cE
':5~~
~c
':"cco.~
!!
u ~
'?
~
E-"
cu~o
cS!!:=
~=o
u ~
O
E.:~
-o:;:"¡i
~ .:
~
:.
~~
-g¿~
::0*5~
0-
,.
Ifi~1
""U~
~c
o.:o~~
"o.
00.:=
c
-
;:~~
~:.
~~
~;.;;;
-::~~
~~
i~~
~]
u¡js==
¡:¡i ~¡
~""'u-
¿]3.g~
!ti!i-":ó"¡i¡¡'~:¡: :':'~
;.'~
.: -~
.
~Ij~
i3-:f;],;:;c~
u.ocuu -
o.~
u
~
~
o,."
ij~~
~o.uuc_o..c=.c-,.
-'1
~'~
~
~
p-o O
;!;'.." "=
. --,.
";J =
=
u
~~
..-
.u -
u",=-~
~~
~~
.:g-oo~
~-
I~l~
;~o.~
o.u.c"
=
~-E
~=
.,;~
o.
~
~
,11
""."u-:o.o
~uc~o-~
o.1.c-".8~
~~
~-~
~u:i:;:;~
=
,. :.. c
O=
?c~--¿
u-;
~
:: o
>o...J~
c
693
~

low molecular weight heparins: l. N. Jorgensen et al
-",'Q ~M
-M Q '"~ ~.., lON o. .lO -..-~ O M M... X '-
~~'_MM O-'-~"'o. M...' Q, M
NM I)N":.~-o..,-:3..."O'-o"-o"q¡ :°-o.,...M e~~O
O... C~":UN ..
~...~tCC°I-~,o.:~~ ~ N ~ ,o.: Lo ~ O ( > ,~ Vt
OJ",:..,';i"IO"'~X>-"1OC.,Q,Lo",>-.c"""UOJLoIO"> C ,~ Lo C ., U = lO -J u. XOJ lO .c lO '- Lo ., Lo lO ~ ~ ~ ~
.:: ~ U ~ ~ ~ .9. ~ .=. ,5 ,5 ,5 ,5~ Lo Lo Lo LoOIOI E cCCCCClOlOlO1O C '- '- ,- ,- '- '- Q, Q, Q, Q,lO ~ :. E E E E E E '- '- O OX X X 0)0)0)0) 0)0) X X "0"0
'" '" :. lO lO lO lO lO lO lO lO C C---Lo Lo Lo Lo Lo Lo Lo Lo lO lOU
U u. u. u. u. u. u. u. u. u. V) V)
b...q,
r;.,VIVI'Q
o"OclO
VI
1-
1--1
.2
~'-'""C"C("")
~l'1...1
t
Figure 4 E.
dihy(lrllery()¡,
-101,' molecular weight heparins (with or Il'ithoutversus u/!fractionated heparin (Irith or lI'ithout
'nine) on the incidence I?f deep rein thrombosis in electire'y- Bars are 95 per cent co/!fidence interrals- .T:.pical oddsper cent co/!fidence interral 0-47-0-96) (P < 0-05)
hipo!
cutaneously once daily appears at least as effective as that withunfractionated heparin 5000 units plus DHE 0.5 mg sub-cutaneously twice daily. In one study of patients with hipfracture the thromboprophylactic action of Sandoparin wastested against that of unfractionated heparin followed by theadministration of a vitamin K antagonist; no significantdifference was found between the groups37.
In eight of the nine trials reporting on the incidence ofproximal DVT the odds ratio was < 1.0, again in favour ofLMWHs (Figure 5). The typical odds ratio (95 per cent c.i.)for the Clexane studies21.38 was 0.57 (0'34-0'97) (P < 0'05)and for the two Sandoparin studies3.36 0.51. (O.28-"-Ü.94)(P < 0,05).
Except for the reports of Eriksson et al.32 and Monreal andcolleagues41, no regular screening for pulmonary embolism wasperformed in any trial. From 13 elective hip trials comparingLMWHs and unfractionated heparin, the incidence ofpulmonary embolism could be obtained (T able 4). The resultsfavour the LMWHs, as seven studies showed a higher incidencein the control group (odds ratio < 1) and none a higherincidence of pulmonary embolism in LMWH-treated patients(odds ratio >1) (Figure 6). In all the orthopaedic trialsreviewed, reporting the results from 4615 patients, fatalpulmonary embolism was reported in seven cases (0.15 percent )18.19.37.39.4°, four of whom underwent femoral neckrepair. No patient with fatal pulmonary embolism was treatedwith LMWH prophylaxis. Eleven cases ofpulmonary embolism(0.49 per cent) were reported in 2230 patients receiving LMWHcompared with 23 (1.22 per cent) of 1884 controls receivingeither unfractionated heparin, unfractionated heparin-DHE,dextran or unfractionated heparin-vitamin K antagonists. Thenumber of deaths was too small to permit comparison between
groups.With respect to the rate ofbleeding complications, no overall
reproducible difference was found between groups. This wasalgo the case when the data were analysed for each compound.In one investigation comparing Fragmin with unfractionatedheparin, significantly less bleeding was observed in patientsreceiving the LMWH32. The dose regimen was unique, asprophylaxis was started 12 h before surgery instead of 2 h.
No obvious pattern was detected when transfusion require-
o.Ma.;,OLo
(.)
1-o(:r9
o...~.,c:c:/O>/O
.c:u.,
C~
lO
tN~'-
>>-al
-J~
C.í:~Q.'x~~
"OC/O
""U
'o;Lo
LL
c'C/OQ.O
"Oc/O
V)
...~co
'"'".x
"¡:~c"e01roLou.
"iJ"
.,'-'-ro
QJ
c"E:C1ro
c">'"-J
"'¡:
lOO-O
"O1:lO
V)
~"ClOX~
;oO-'xlO
..~
'" x vi'""O -.:c olO
"~;>::uCJ
r"\
iJ cCI'" '"
" '"" "J: ..J~ ~
C C'¡:: '¡::" "a. a.o o
"C "CC C" "
u'C;Lo
u.~
r-t 1"I I-o"Oo
c c.C .C'" '"o. o.'x
'x'" '"
Figure 5 Effect of 1011' molecular lI'eight heparins (1I1th or lI'ithoutdill)'droergotamine) versus unfi'octio/lated hepari/l (lI'ith or lI'ithoutdih)'droergotamine) on the incidence ofpro inlal Jeep rein thrombosisin electit'e hip arthroplast)'. Bars are 95 per cent confide/lce inten'als-Typical odds ratio (95 per cent co/Ijidence interva/): .0-57 (0-34-0-97)(P < 0-05); tO'51 (0'28-0-94) (P < 0-05)
~
.2
~'-VI
"O"OO
1
.--+- --
efficacy of a combination of Sandoparin and DHE comparedwith unfractionated heparin -DHE has been investigated in fourtrials3.19,3S,36 (Table 4). A meta-analysis performed on thethree studies of patients undergoing elective hip arthroplastyshowed no significant difference in antithrombotic effectbetween the two regimens (odds ratio 0.89 (95 per cent c.i.0.58-1-36)). Similar results were found in patients undergoinghip fracture surgery19. Prophylaxis of postoperative DVT usingSandoparin 4800 units combined with DHE 0.5 mg sub-
Figure 6 Effecl of /ow mo/ecu/ar weighl heparins (,..ilh or ,..ilhoUldihydroergolamine) versus unfraClionaled heparin (,.'ilh or wilhouldihydroergolamine) on lhe incidence of pu/monary embo/ism in e/eclivehip arlhrop/asly. Bars are 95 per cenl confidence inlerva/s. * Al/easl 30
da}'S' fo//o}t'-up
Br. J. Surg.. Vol. 80. No. 6. June 1993694

Low molecular weight heparins: L. N. Jorgensen et al.
ments in each treatment group wcre analysed (Table 4).Clinically relevant differences were observed in only two trials.Eriksson and co-workers32 reportcd that Fragmin- andunfractionated heparin-treatcd paticnts required a mean of 2.3and 3,3 red cell units respectively, whercas Haas andcolleagues34 found the opposite effect. The regimens testedwere, however, not identical.
r--'"" ~o '""-'""'- '-o o
-~
o-~~..., ~cN c~
'-~O""0-8
:J:~~
~ ."r-. N0\ N
O ON ~
cx¡V-M
N~c'-.,.,Ocx¡°6N~
o-o-..,N'-O
~3~O~~ON9~~""
r;:.~N'-'";¡;
~~
'"-¡;.B"'"
r- ~~~-~-,= '" ,==, ~ =,o~~r-N~~-:-~~'"'
General and gynaecological surgery
Controls receiving placebo. Of the thrce studies available,regular screening for DVT with an acceptable method wascarried out only by Ockelford and co-workers42 (Table 5).Prophylactic treatment with Fragmin 2500 units subcutaneouslyonce daily reduced the rate of DVT diagnosed by the fibrinogenuptake test from 17.0 per cent (95 per cent c.i. 10.7-25.0 per cent)to 4.2 per cent (95 per cent c.i. ).4-9.5 per cent) (P < 0.01).There was no difference in the bleeding tendency. Fatalpulmonary embolism was assessed as the endpoint in alarge-scaIe assessor-blind study randomizing 4498 patients totreatment with placebo or Fraxiparin 2500 units once daily44.Four patients in the placebo-treated group and two receivingLMWH died from pulmonary embolism. The total morta)ityrate was reduced from 0.80 to 0,36 per cent.
'"o-'--;:r~-~'-o000~é:!.
!;o ~¿
~'a~U
t:=
'"OQ
.~
I;,;'aO)
E~
-5C'~co
-¡;;..='"c
goCQc
'50),O)
::c.:8cO)
~'5'a~
.g'"
CQ.¡;;
~-;;-=~-;"'"oc
Ó
"'"E.u~c.:c,.-cLI
.§
;:§.".:doÜ
~~~....
¡..:~...;,,-;;;
~~
-5
~>c.,.-"."
¡..:>O
..~~
~.~~..
.§u"CE~
.9-
:I:~::;:..J
~~'-n
~~Ñ
J:~~..!.¿s..J.:=
~ ~ ~~ .J:) .J:)'3 '3 'd'" '" '"
.~..'=~
i
Controls receiving UlifraCliol/ated heparil/ Il'ilh or 11'ithoutdihydroergotamine, The prophylactic use of low-dose unfrac-tionated heparin has been intensively studied. With thistreatment the incidence of DVT, pulmonary embolism andfatal pulmonary embolism is approximately 10, 0,5 and0,2 per cent respectively4S. Most trials in which the prophylacticeffect of LMWHs was investigated were conducted .usingunfractionated heparin for controls- From 32 studies, 38comparisons between LMWHs and unfractionated heparinhave been published, with supplementary DHE administeredto both treatment groups in six investigations46-S1 andexclusively to the unfractionated heparin-treated group in oneS2(Table 6)- In all studies, the incidence ofDVT was the endpoint.The diagnostic method most often used was the fibrinogenuptake test, sometimes with verification by venography- Asignificant reduction in the incidence of DVT by administrationof a LMWH was obtained in three studies. The treatmentregimens were Fragmin 5000 units subcutaneously once daily,Fraxiparin 2500 units subcutaneously once daily andSandoparin 8000 units plus DHE O-S mg subcutaneously oncedaily47,S6,S7 and the respective odds ratios (95 per cent c.i.)O-53 (0.31-0.90),0-26 (0.10-0-69) and 0-31 (0-12-0-82).
The odds ratios for all the trials were < 1.0 in 15, 1-0 in nineand > 1-0 in six; these generally favour the use of LMWHs(Figure 7). If only the high-quality studies are included, thecorresponding numbers of trials with these odds ratios are four,three and three, with some of the largest studiesS6,S8-60belonging to the group favouring LMWHs- Many of theFragmin studies were not homogeneous and so do not allowproper meta-analysis. This is so even after stratification withrespect to clase regimens in the LMWH-treated and controlgroups of patients. Three studies compared unfractionatedheparin 5000 units subcutaneously three times daily withSandoparin 4800 units subcutaneously once daily60-62 , forwhich a typical odds ratio of 0.73 (95 per cent coi. 0,44-1.23)was found, a non-significant reduction in the DVT rate in
Sandoparin-treated patients.The total incidence of symptomatic pulmonary embolism
reported for patients receiving LMWH and unfractionatedheparin was 0.16 per cent (fatal embolism 0.02 per cent) and0,60 per cent (fatal embolism 0-13 per cent) respectively(Table 6). In none of the studies was regular screening forpulmonary embolism performed. Data on the incidence ofpulmonary embolism could be obtained in 27 of the 32published studies, often only by direct communication with theauthors, As the number of observations ofpulmonary embolismin each trial was small, the confidence intervals for each odds
J ..
=>.o "t:.~ '""..,.
'.;."5~~;;;
~~~'"
:E'"r-
695Br. J. Surg.. Vol. 80. No. 6. June 1993
co°;ñ.E'"
Crd'::.
";§..o'"c
09
~"Q.EoutICC
;:¿;uu
:o'o
()
"id....u
..cOi)
:i:.?;oCrdUc:°2..o
°;ñ
+Q.~o..Oi)
"8"id
~J:~¿..Ju-=o:
;~~
°5C"~""oo::c""§~o'""~u~~~oo¡;:
¿'"~
o~
o~o~"E.~ouOi)c
'E":E'c
()
";..'¿¡~
.2
.,~."-o;~u-=.".,~
.~'",~00c
:;:-Oc
,~C
.2üu:5'-o;...t:
~~~.cN
~
X~r-."a>.~O{j.."'"u
..2u.o
N~¡¡>
';j¡
,~
g"',r-
.~~c'-
~.;;;
()*
~~O{j
~~~.,:.
~¿..J
-5::~~~5-u..
~cc
:c;u"O..:~...cv:U>-U
]>-~
c.~~S?
~.,"O~, ~
.,-=..e8c.,
"Q'yC
"Q.,
""~Q.:.,.'oS
-5
.sü}ou~:.§
~
~u~u
"1~>.'"~o+-+
!j'"".u'"~
.~"O~¡¡t'
gI
-+-~
~u
..e:i.
,..,,
tj,.';;'.~
x x 8'"' c ~~ o ".¡~ ~~ N .S
~ '-;: = "-~ c." c .-~ ~ ~.= ~ ~
;".:"E..2"¡j~uo
..",
'o;
"O~~ou.

low
molecular
weight
heparins: l.
N. J0rgensen
et al
696
~'"''"'-~~'"'.~c~'"'"'""""''"~""~'-'"'"'"''"".~~~~~".9';:;"~.:.~é~:4:
~'":1'"::;'"".~"""'"'..,~'".~~'"'~cE~c..JID..:E..E
-
",rr o
o ~
~~
r- 00
~
;O
..~O
O
~
N1-
:1: -~
~
00 N
N
~
-..>
,.. ~
~~
~
~
~
~
~
~
~
~""
000 O
O
O
O
00
O
OQ
~
-C
M"
-M
M
-"'- ~
. -
'0.- -N
8C
OO
OM
..~
N
~
~
~
~-M
~
~
;O
..M
.o '"
O'"
N""
~
e ~
~~
~
~
~
~
~
~
~
~
--000 o
o o
o 00
o o
5 N
M~
-C
M
..M
r-N
O
r-
U
-~=
--- -~
.
":j:
~5¿
"E~0.2
E ~
"'c -~
~.
~
N
N
N
N
N
~
N
N"§=
2 X
XX
X
X
X
X
X
X
X
X
§~~
§§§
§ §
§ §
§§ §
§U
=--=
"""'"
'" '"
'" '"
""" '"
~
,--'--, --xxx
x x
x x
xx x
x
~
x88 8
x x
x xx
~
~=
~
~~
~
~
~
~
~
~
;;; ;;;
~""""
E-"
EE
E""
-x """
,,- _E
"~
, """
" "
" "
"" "
=
~~
~
~
~
~
~
~~
'"
'"jK
000
;: ;:
;: ;:
~~
~
E
>-
~;'"c.~;O
-S
? ~~
~
r-,.,r-:ti
-o'""~
...,o
---~=
~
~~
~
c 000
O0000
,.,U
Irr
:c ~
~r;;
~
~
::: :
~
000 O
.J --N
N
." ...
" o.:
~
-o.-:=
" ..
" ---;,
s ~
~
~
o"
o. o.
o.s~
-g-
g- g-~
" .!!
o o
00.:~
f-f-f-
6: f-
~
~
~]
f- f-
" ;););)
O;)
;) ;)
;)0. ;)
;)::)
""""'" O
'"
"" ""
"" '"
""
"8
~c
S!!
"~
S
~
:, u¡¡"
~~ ;
; ;
c '¡:
--"
"..a.g:§'E;
~
&
Gu
u '"
>
"¡j ~
-;; Q
¡ ~
-¡;
~
o "
~u
-u "
c o
~
cu
~
..u"
;:J >
"
~
~
~~
.
~
: rr
E
~
"~,,
o ~
'"
~~
.oN
,,", ~
o.
~~
-o
o~
~
~
---~
N
N~
N
'"
-~
.&
~
'0'0'0 'o
'o~.
'0'0 'o
'o 'o
"E
..¡ 000
o o
~
-o o
o o
c "
.g>.¡¡~
I~
"..",
~~
""
oc
c _o
.oN~
""'
o. ..,.0
-0.- -
-o ~
---~
N
--N
~
... -
E-~
~~
~
~
~
~
~
~-
~-C
000
o o
00 o
O,g
o
5. 8
00- o
o ~
. ~
. o..,
-""':::. o
C$J
o C
-u~ E
.:U~=
---
;;. +
I
I¡::
e 000
o ~
~
. ~
---
~o -
~~
~
'5"c. 'i'
gEl
I I
I ~
=8000
o o
o o
00 +
I I
+~
~
~
o
~.-,.~]~ r-
~¡;~
~
gN
..,
'o 'o
.., ::
~
~N
V
'o 'o
~
:=
~.
~.
';; "¡;
~
~
&
&~
~
~
~
~
~
";§ ";§
g g
o o
~'oo 2'oo:@'oo ""ij"=~+ ~5~+-:E
-
c. >
,,,>
' ->
,
~~
~~
lf Ir ~
-'ooNX~ -xX~~""."~o:o "!jo.o"8:ic>,
(;
Br. J.
Surg.,
Vol.
80, No.
6, June 1993
Q;
"oc ~'oo ~'Ec~ - ~'oo-xX~~ ~'cNX.,.ES
"E.
X~~~~ "~1¡;,
~
~'o...~'oo1;;
~'oM§;.--
~~,ox~~NXX~¡¡u ;2.
o o
N
V
'o 'c
'" -
oo o
N
..'o
'o'"
-
N
~.
X
X
~
~ -x
x:5
so;(¡
~
~ ~
.~
:.-¡:
~g
-¡:
8. ]
u ,..
U
t
~.
;a;
~'oNc.,.'oj~~1-
¡::-:¡
:¡""
:..
-J -::
'" ;¡
TI ]
f,.."
u >
-~
~
~
~'o -c~'o-c-c... -
o N
..,'"
'" .-
..-: N
r- N
-
~
~,,~
- ~
~
O
O';
00 O
O
~.
O
-"'- 00
O
O,0-
N
0""-'-~
:§ =
~
~:::
~
:::O
';; O
'; 00
O
O~
. ~
.- -"'-
0- O
N
>.
~~~2 '"'o'" ~'o'"NXX~ x~~-a"~":1:
u¡¡"~
o.., ...
'0'0 'o
F..,'" '"
N.-.
N'0'0
'o00
O
..'-'0 ..,
r-N
r- N
N
"0"0 "o
"oO
N
-N
j~~+0
"¡j5"E-i
+15
o
000 ...'"
N-o
N
'"'0'0
'o 'o
0- O
N
NN
N
N
X
X
X
X
S,. ,.
,.V
'.~ ~
~
~
----xxx
x ;¡
c~
;¡ ;;;
c- ~
N
;:: ~ "'.
==
=
=
~
"" "
O-
Si¡ S
i¡ S
i¡ ;¡
"" "
,..;:.;:
~
~
>,
"E.
"~o5~~~"u-o~ ~ ~¡¡v
>,
>,
-=
-="-
"-"
"~
~
o o
=
="
"¡::,
¡::,=
' =
'"-
""
~
~1:
~E
';;
¡¡ -
.r: ~
~
.c
g ;
O
~
:i%,
-;¡ -;¡
t; t;
=
=:)
:)-~~

Br. J. S
urg., V
ol. 80, N
o. 6, June
1993
~."6...;.c"C
;:,."
"-"
-,,~
,.
,.,. ~
o e
g.c-
u1-
o
~o~]~:o-~x~ ~x~N:::;O
-
~ ~c."1;,o~¡:;
;:¡u.
;'O -o'oo O'
~~o !i'o
~...'" ~"-~'"'
=
:1 :8:::
x
~~
~
,,"- "
~§
~
~;:¡"" -c~'o~ ~~'o.. o $ ~
c- -
'o 'o
-c"'- g:
0:3 ---,.!
--o
o ..~
::. -~
-c~"ó~ $'"'o~
~:;¡""..,~
"~
:-c.~..,~
N
c.X
=
x
~8
~ ~'c,.,
;,~;~-g=~'"'"~ ]~u'" ~';:! +O'
~'o.o ~'c'"
F
~;;;
8 o.
N
o.00
O
O~
~
--'--,,--'
~
8 8
..N
-O
O
'c
o. -N
oro '"
..,- o.
"~
.., -~
~~
~
~
..o
o o
o"::
Ñ
-=
--00
o O
-+00
O'
~
.-0-;';''0'0-..'~..'oN.t!1~2j uÜ,-v >
-
~~¡¡~ ~~'o
" "
!1 !1
¡¡ ¡¡
o o NX'":I:~
~.
~x
"E.
~
13~
~
~
~-~'S
'S
~
".."6...e
~
~
~'=
--:;"
..'"
e"
"."
"<
:= E~~1
i- i-
¡;: ¡;:
",'1;..""...5¡;:I: ~... "¡j;;,o"O~..cO
'
..,x~
~-
~
---x
"E.
x
X;
8 8
8~
x x
x ~
..:.~ :
:- =
]} f f~ i '>
;oC"-" '"'.oC..c.o "E
¡¡,
-~
o ~
~ ~
E
c: Ü
~"5-o ~'o'" IO'
~'oo ~"so
~';¡cc~o:c NX~ ..:.;;'"óo~ .,.~¡¡o r~N'oO I'O ~'Oo¡:¡'Oo ~N'oQ ~'oo
:,.."~.».»"~ ...gc NX'":cQ;"Q.
~ ;:'o~ ~~'o~ ~~'o...i.-;,o~~;J¡., +"5 o:'oo
".;: ~
" ..:
" "
~
-..".c
..~
]
Q.
..o
~~
'"
-; -;
~
~~
~
>.
>.
.c .c
o. o.
" "
;, ;,
o o
g g
¡:: ¡::
~
~
:;: ~
'Q
'Qr-
~ .;;:; ~
'o 'o
.~ -+';5 oNX!;:'25
.., ~
x "E
.
§ §
'" '" ...::¡'6o-.'6~~
::1'O !3'O...
-=:'
~
~'o
'o~
o r-
~
~'o
'oo
o' '...'oo
0=
., ';'
'o 'o
o N
' ";'-g.og;§~
---"--+
Q
5
:2,
-;¡~;¡o ~'oo ~'oo~~~ E
~gx E
"
2 ~
~ '"'
]~+
o~"~¡;, '",;"ig..,~ '"
'"x-
x"
"'=
'"~
I ~=
. =
-c.=
-c.~
~
$2
,",' '"'
O':
O':
uc:o~~o -=g:'o ~~'Qo g:'oo '"o-'oo
~..,."..,o;..
~ ~
~ ~
~
~
-~
;:;~;:;~
~
~
~
"E.
"E.
x "E
. xgxg"E
. "E
. "E
.8
8 8
8 X
"X":8
:8 ~
~
~
~
~
~=
~=
~
~
~
~
~
~
~
~"v",
~
~
~
i~
i~
i i~
i~i!
i~
i~
i~"-...
0- o
,,- "-,,
-,,- ,,~
0-
~
~...
~
~-
~3~
3 ~
~
~-
~-
=0
=0
=
=~
=
"" '.)
=-
=~
=
0~
~
~
~
~
~'"
'" '"
'" '"
'" '"
V)
'"
>,
~~9tü ..~'o ..§'o §'o-o~~o §'oo~'o r-~'O..
'."¡;'Z:g~ ]"c13 NXOJ
:1:Q~"Q
.
~ ¡..
~ §:'o~ ;.~'"5~
'";--~o'ob~
~;;;~-
-~o'.c~.c
.N
~
;;; ..-o.~
-~
~.'!
~-~
°6~--.o~
:i.=..'¡¡~
.3-6..M
~
...o¡.. ~-
~~
'o~~
.:.-0-
;;;~~
~'o~~
.:.'0-
-c-~c
o ~
~
..-oc'¡;u~
-~
.,. .'"
CcC
>,
!' ..2
..W
~-"Q
-U>
'_uc=
";;'0~
0-~
::~~
ooc5-W
~
W
W
C
u
OO
':=W
c -~.~
.co~
",o.¡;~
::.;"
8W
5
5 ,,~
.E~
§§8.=
~c
3",8~
:o-<>
'_u¿.cO
Wo
c. 0-
"U"Q
-~
- ..
~."Q
~o~
c8.~
~
8
o>
.r: u
u~
~~
u-. o
>.r:>
,~
~:?:,~
2,o-~
.r:=
5~'"
.~~
~~
W.c>
~ ';.r:.;'
~
'" ~
S-'"C
~~
~
o
~g;'"Q
~~
-o
-wc"Q
~~
-,,"oc.E
;§uocu
.r:"8~
8-:=
::;!:¡"82,~
-~.;!~
~~
2"'.g~"Q
u
~".r:--~
-~~
""c-=c
~ :~
~.r:~
~o
-u u
c-
5~
-~
~
-u ~
.."~
~c'O
~[~
~~
~-2,~
>~
"&.r:o:?:'
~o"'t)~
~:o-.:=
~"
u c
" u
~o
~.r:E
O.r:~
~o
~~
-~~
~5~
2~1-
c ~
"
~G
~2~
"->'2:7;;
,.g~"'5
~~
"'"Qo
g:';;"cc.->
""'5ct).g>
,>,
"--t)~:'cw
">,
"'g:.;c~
~:~
:os§~
:B"ji
""-;;..,..r:~1-"0
.'" ~
>-::c"
Oc~
~~
"~~
,,Oc5"'~
""':w
c;:'"
B
~
~
"
~'E
.~8§
=5_~
c.5
° °
=
-""%5>
-",.--~"~
8->
,~
=
~
-u""-ucou",c.c
~~
90~>
, o-o
':CV
o~""
>,.
~~
""='"
"'"";¡
i~c.c",
~
"=¡;~
6*cu
° ~
"
c-"~5
;¡ >
'"8 -=
>
,
g"'§;~::
..u u !S
~,g "
...'O~
cX5~
~~
~~
c
c .¿
c
5u
1... ~
°-c.
§¡j
c.,. U
~
~-'.r:
~~
. ~
-;; ~
.:'"
5 -~
::u~"'~
O:'¡;';'u
~
u "
.".5
~
ocu
>"0
~~
g.§~c.o=
c~u~
'lc:?:'.r:~
~
.""
~;
-;,c"Qu
-"0"5~
".2;0~
.c~.:
~
c"
.!!~""
-"0 u
~c.r:';¡'O
u~>
u=u"",.c-~
I!~.r:~
c:oo"""~
C~
-r,,->
.c.-u
c.8
" >
°
::c~.-:
u.r:"'..~
~-u~
~~
~~
~-u-o
"'"Q--
Low
molecular
weight
heparins: L. N
. J0rgensen et
al
697ti
N
O~
g:
~'o
'o 'o
O
-O
S
s- ~
N
---"
,,- O
-O
-"'-
O

Low molecular weight heparins: L. N. Jorgensen et al
,,~.o
~ ~...:~ 0\ ()". "" .o
..., ~. '...> , ,.. ~ ~ ~ Q,
..lO" ()- ~ v~~~ ~~ L.. -O -O ..."" L
"'-O ~. """"~ L"'~~',,"Q,""'~-O..., ~ "" '-~'" ~ o v,.. ,.. 1:~-.. ~ ~~ ~~."" ..., ~ .""'" :J v (). () ~""""", -~ 0\ 0\0 """:-0 "" .~ "" ~ -O L O 1: ~""...,"-o-o-o,,()O"~ -.:.o~.oOO"': '¿j'""", .,...",.....: ."-.: " ..,.."" ()...:".o () 'O ,.. 1: Q, ...0)Q,:J ()()~O()~~~'¿j'~()"" ...0" 1:"()- LI: Q,!E~:r...v v v v ~. .,.. Q, ~ ...U '. ,
..."""- -,.. Q,"'OO Q,~~IO_-Q,IOI:LI:L"Q,
Q,'Qj~Q,'Qj'Qj'Qj",~~0.0~ ...1:':; 1: "" ~ 0>,,-g.1O~.,!E"~~"-' ,- "'Q,'-~ ,,'Y ,=I:-Q.-~-IOIOO" »YQ,O\ LLQ, .,.c 10 '-'-XL O;'--XQ.IO,= "
1:._'0.,."0"0"00-0-2 ...,.,& L.c'-.cV1.:.:°"OIO-C;IOO~.c"QjIOI:IO._'-'-'-O)O)",-I:Q.-=.,'-IOIOIJ.IO" m :.:~"U~
1:10'-"10 IOIOLL'--~ .,.,.!¿ ,--IOQ)QW:':.C;«~:r~...V1V1~10-'-;1'- '-'-".,0'- 10'-'- IOOI:~~~~-J~~~ ~~~~
V11O0Q.~~~Q)Q)Q)Q)UUIJ.:r:.:Q ~ 1:1: 1: 1:1:1:1: 1:~UUV1---~~~~~~~ ~I:I:I:I: "-~~~~~~ ~~ '-1: '-'-L '-L'-,-,,-
., 1:1:1:1:1:1:1:1:1:1:'-'-'-'-.-10101010101010101: 1: 1: 1: 1: 1: 1: "- 3. lO lO 10 L Q. Q. Q. Q. Q. Q. Q.flO :J ;, ;, :J :J :J 1: 1: 1: 1: 1: 1: 1: 1: 1: 1: .--9- ,3- 3- 3. O O O ~ O O OX X X X X X X O) O) O) O) O) O) O) O> O> O> X X X X.- "O "O "C Y"C "C "C
., :J ;, ;, ;, ;, ;, LIO '-lO lO 10 10 LIO '-lO '-lO lO '-lO '-lO lO lO lO O) 1: 1: 1: 1: 1: 1: 1:,-,-,- '- '-'-'-010101010101010
UIJ.IJ.IJ.IJ.IJ.IJ.IJ.IJ.IJ.IJ.IJ.IJ.IJ.IJ.IJ.IJ.IJ.IJ.IJ.IJ.-JV1V1V1V1V1V1V1V1
T100
10 T
-J--I-i--!.~
...
't-t-¡
'"'O'Oo
f
011
Figure 7 E.ffecl C!f 1011' molecular lI'eighl heparins (lI'Ílh or Il'ilhoUl dih)'droergolamine) versus unfraClionaled heparÚl (lI'Írh or lI'Írhoulergoramine) on rhe incidence of deep reúlrhrombosis in general and gynaecological surgery, Bars are 95 per cem corljidence imerrals, * High-quali,
regimens related to the prophylactic use of Fragmin have beenintensively studied in patients undergoing general surgery.Bergqvist et al.63 foundthat Fragmin 5000 units daily initiated2 h before surgery was significantly more haemorrhagic(excessive peroperative bleeding, wound haematomas andnumber of reoperations for bleeding) than conventional heparin5000 units twice daily. Similar findings were made by Borstadel al.65 using a similar dose re gimen in gynaecological patients.If the time of the first 5000-unit Fragmin dose was advancedto 12 h before surgery, the regimen was sti]l more likely to causebleeding than the use of unfractionated heparin, but thebleeding episodes were only minor and efficacy wasmaintained56. Another safe and efficient approach57,64 has beento reduce the dose of Fragmin given 2 h before surgery to 2500units, repeated after 12 h. Koller et a./.66 and Schmitz-Huebnerand colleagues67 used higher LMWH doses than nowrecommended in some of their studies (Fragmin 7500 unitsdaily, Sandoparin 5600 units twice daily) and experienced asignificantly higher number of clinically relevant bleedingcomplications, leading to interruption of the study of Koller elal. Prophylaxis with Fluxum 5000 units once daily68-71,Clexane 1600 units (20 mg) once daily 72, Fraxiparin 2500 unitsonce daily57.58. 73. 74, Logiparin 3500 units once daily"5 or
Sandoparin 4800 units (with or without DHE) o\}ce daily haspro ved to be efficient without causing significantly morebleeding than standard low-dose heparin46.48-51.60-62."76. Itappears, however, that there is no basis for the claim that theprophylactic use of LMWHs as a group causes fewer bleedingcomplications than that of unfractionated heparin (Table 6).
Higher transfusion requirements in Fragmin-treated patientsthan in those receiving unfractionated heparin were found intwo studies65.66 (Table 6) in which Fragmin 5000-7500 unitswas given 2 h before surgery. Lowering the preoperative doseto 2500 units, but withholding a 5000-unit daily dose in thedays after operation, led to the elimination of this tendency52.64.
ratio appear wide, especially if few patients were allocated inthe respective trial (Figure 8). In 13 studies the odds ratio was< 1.0 (in favour ofLMWH), whereas a ratio > 1.0 was observedin only three. In ten investigations no case of pulmonaryembolism occurred, leading to an apparent odds ratio of 1.0.If one includes only the high-qua1ity studies, a higherhomogeneity appears with no odds ratio > 1.0. There were nocases ofpulmonary embolism reported in the three Sandoparintrials. Prophylaxis with Fragmin, Fraxiparin or Logiparin ledto a reduced risk of pulmonary embolism although without aclear statistical significance in each single investigation.Meta-analysis ofthe three high-quality studies56.63,64, in whichthe LMWH-treated patients received the high-risk patient claseof Fragmin 5000 units daily, showed a typical odds ratio of0.13 (95 per cent c.i. 0'04-0'42) (P < 0'01), suggesting anoverall reductive effect on the incidence of postoperativepulmonary embolism of Fragmin compared with that ofunfractionated heparin.
There were even fewer cases of postoperative fatalpulmonary embolism; in 21 of 28 trials there were no fatalpulmonary embolisms, leading to an apparent odds ratio of1.0 in each (Figure 9). Again, no trial showed a significantdifference between treatment groups. However, there is a weakvisual impression of an overall superior prophylactic efficacyof LMWHs ayer unfractionated heparin. Meta-analysis of thethree Fragmin studies mentioned above showed a lowerincidence of fatal pulmonary embo1ism in the Fragmin-treatedgroup that was not statistically significant (typical odds ratio0.13 (95 per cent c.i. 0'01-2,15)),
With respect to total postoperative mortality, no clearoverall difference was found between treatment groups, eitherfor all studies available or for those ofhigh quality (Figure 10).
A significantly increased amount of bleeding in LMWH-treated patients was observed in five studies56.63.65-67 andconsidered clinically relevant in four (Table 6). Different clase
698 Br. J. Surg., Vol. 80. No. 6, Jun~ 1993

Br. J. S
urg., Vol. 80. N
o. 6, June 1993
.,g~Lo&ti
"O"OO .9~...1/\"O"OO
."'~\O
~
...:~
~
()
"'. ~
'" ~
.. ...
>.'"
,.. ~
~
~
~
..~'"
(),:;- \O
~
~
'- ~
..,~~
~
~
"... "'\0-
..0\O
."'~
~
'-"'~~
"- .-",~
~--~
IO
"'",~
~
"""", :J()O
~
,..-,..C-
~..,-~
~O
\~"':'IO
~
~
..'" "¿
...IO,-
()...:().o...:",",'"
lO
\O
()~
.~
10.\0 ~
~.
~.""'...
()..." ()
....:
:.. ,..""
...:",~\O
~~
~"O
~
C~
~...~
:J...'"()
~
() ~
~
'¿
; '¿;
()"'. ()'"
.~...
.C
N
t c
c ~
ro:¡;
Q, ()
...,.. .~
"
~
...~
lO U
...'-
I ...
,¿;"',¿
;"""--~~
."'~
,-Q,C
O
,-'>~
~C
C'-~
~'-Q
,q¡
Q,Q
,I/)I/) ~
~
...E-
c"'IO
O"-
EE
~E"ro.c'-"-
-'-'-"O"'~
...Q
,'-- '"
'-- y
Ec
,.,.O'-,-»"~
,,, '-Q
, .,.010
-XO
°:J-""~~
,-01
E,-"O
"O"O
o-o-- .,
,-.c'-.cV¡-X
N"O
~o;,,-~
I/).c.,°O~
C
~
'-
'- 0101
I/)"CJ
C
-X
~.,
'- 10,.
u. 10,-
~!!):¡;
O
~,J,
U
tí>
~12t
'.:t.'"¿¡¿
¡ gol:
g.';!:o~
'r!.~9.~
':::.3 ~
~~
.:::~~
~~
~v¡~
0" "!!)!!)!!)!!)U
u.:¡;~
O
~
CC
C
C
C
C
c: C
C
~
U
U
>
>
~
~
~
~
~
~
~
C
C
.C
C
'- '-.-
.-°-~
~~
~
~
~
C,-,-,-,-,-,-,-'-'-
..C
CC
CC
CC
C,-,-'-'-o_,.~
~,.ro~
~""
C
E
E
E
E
°- .E
°-
'- '-
.-0_.- .-3.
,. 3.
3.:0 Q
. Q
. Q
. Q
. Q
. Q
. Q
. Q
. Q
.e:J:J
:J:JEE
E
EE
E
EE
E
.-.9 Q
. 000000000
~xx
XX
OIO
IOIO
Ic)c)OIC
)C))(X
X
Xo-
"0"0"0"0"0"0"0"0"0.E
:J
:J :J
:J ,.
ro ~
e
~
.'" ."
lO
lO
ro ,.
~
lO 01
C
C
C
C
C
C
C
C
C
ui;:i;:i;:i;:¡J:¡J:¡J:u.¡J:ti::ti::¡J:¡J:¡J:¡J:u.¡J:j """"""""""'rJ.'"
10..
1 8-"
--
0.1
0.01
Low
molecular
weight
heparins: L. N
. Jorgensen et al
-e-- -..+ .,,~ID
~
...:~
o.
O".
~'"
~..
...+
- +
- ;..!!:.
Q-~
~
~
Q
I..10
ID
ID
~~
..
~
~
+-
~
~
...«... "ID
~
..O
~"'ID
."'~
~
"~~
QI"':.~
.
C"'~
.-.ID",
~
~
"""" :J~
O
O"".""
-N
~"""-
~
~
..:2 ~
~
.." ~
...ID
.. O
0.0
...: '""
:;;' "
?¿?¿
Q
Q
.N
~
ID.~
:g Q
Q
'::; 'O
Q
I ...:
't!. Q
; ~
O
"¿j .;'
O
o;:;...'.
~
" ~
N~
w
" ~
... ~
"" ~
""
~-,
O"
' «C
~
-C
tJ ~
Q
I°O
~O
OQ
lQl.
.~tJtJ...~
IOU
"" C
101
...,..
~
QI
0- -10
C
C
N
QI
"", tJO
« tJO
E
o- ~
..>
QlO
IIOIO
IOIO
-"Q
I Q
I tJ
QI
QI
o~
o~
'O
...C\~
.. ...Q
;"- :J
CU
lO
e ~
E
E
E
~
.c"e
't!. -
lO
10 o
0- 0-
>
>
lO
~'"
..QI
J!. -e
:. V
) ::
o 0:J
==
~
~
~
.c "-
021E
"_'O'O
'Oo-o---c~
-á"IOIO
lLION
'010"0
lO
IOu2
o10
c~.!o
~
OIO
I~oE
"o!:
L=:
IOC
!)Q
UJ~
oa; ~
~.7:x
~
V)
V)
V):>
E2
.."" o
..10.. lO
oC~
~~
~-J
~
~~
~~
~~
IOIO
O
~"C
!)C!)U
lLX~
O
~C
CC
cCC
CC
CV
)U
uC
!)~~
~~
~~
~C
CC
C
0_"_0_"_0_0_0_00-~
"""~
~
"_O_O
-o-c ~
~~
~
ccccc c""""o-IO
IOIO
"""IO~
"
~
E
E
E
E
o!: o!:
.-0- .-"-
"- .!:
"- 3.
3. 3.
3..!o o.
o. o.
o. o.
o. o.
o. o.
10 :J
:J :J
:J E
E
E
E
E
E
E
E
E
"-
0- 0-
0- o.
o o
o o
o o
o o
o>
<
><
>
<
><
>
<
01 01
01 01
01 01
01 01
01 >
<
><
>
<
><
0- 'O
'O
'O
'O
'O
'O
'O
'O
'O
":J:J:J:J" 10
lO
lO
'? lO
lO
10""
lO
lO
1001 C
C
C
C
C
C
C
C
C
"" 010""10101010..10
UlLlLlLlLlLlLlLlLlLlLlLlLlLlLlLlLlL-J
V)
V)
V)
V)
V)
V)
V)
V)
V)
100
10
'o: T
~~
.l- ---8- --1-
+-
0.01
0.001
699
odds rario 0.13 (95 per
cenr cinterval 0.04-0.42) (P
< 0.05)

rl Low molecular weight heparins: L. N. J0rgensen et al
*~'C
...:~ ~ C)'"'" * ~ ...
~ ~ .* Q}* * "':;:. -o -~ co~ .~ ~ Lo 'C ~ -~'" 'C ~. * , O
-O '" ~ ~ '" ::; -O o~ Q} ...: ...: c '" --~'" ~ *", "" -O C)C).Q',-'" '" 'C 'C ~. -<... Lo ., ..."'" C) C) .~ .!.. -o... ".,... ...:J C) ....: "" ID C) " -oC"":r o
C)-o"Q}C)'" C)"" *CN -CrolQ}: -.: -O Q} ~ '" .!: ...Lo Lo N ...
Qj Qj ;;;' ;;;' Q} C) * Qj C) ...E ~ Lo ~ .::. ó', g 2.~ ~ Q}
'" '" .> .> " Qj "'~ Lo Qj ~ .¿; l) !l Lo "O 5" .§ ro f: .E ,o,E.- O" O" 2 "'.!i. -Lo .c ti) .x f, "V '" .¿; 'to u ,g .0ro C O) O) VI "Qj C u ~ .SI. Lo IL '" .-« ID :r ti) ti) ti) >E '" Lo Lo Lo .-.,.- Lo -ro W ~ ., ro~""OLoroLo"'OC""""..J "
ti) U ~ ~ ID .ID ~ .::. ~ ~ O C C E .E .E .E .s .E .5C Lo Lo Lo Lo Lo Lo ~., C C C C C C C C C :o Lo .-ro ro '" ro '" '" '"C E '- '- .-'- o. '" Lo o. o. o. o. o. o. o.
'" :J E E E E E E E E E .-.9- 3. o o o o o o oX X O) O) O) O) O) O) O) O) O) X X .-"V "V " " " " "01:J""" """"""ro"'ro"""O)CcCCCCCU-.-;- .!-.:- Lo Lo ,!- ,!- .!- Lo Lo .!- Lo o ro ro '" ro ro '" '"
~ ~~ IL IL ~ ~ ~ IL IL ~ IL..J ti) ti) ti) ti) ti) ti) ti)
No increase in transfusion requirements of Fragmin-treatedpatients was observed in any study using this LMWH at 2500units daily59.66.77 or in the second trial of Bergqvist et al.56,in which the preoperative 5000-unit Fragmin dose wasadministered 12 h before surgery. No clear difference intransfusion requirements between the treatment groups wasobserved in the large studies with Clexane 72, Fraxiparin58 andLogiparin 75. The Sandoparin trials are difficult to evaluatebeca use of inconsistent treatment regimens in both unfraction-ated heparin- and LMWH-treated groups. Most of the studieson Fluxum lack information on transfusion. If the studies areconsidered as a whole, disregarding the type and dose regimens,there is no indication of a transfusion-saving effect associatedwith LMWHs.
In this analysis the main type of surgery and treatment ofthe control group have been stratified. Instead of performingmeta-analysis of inhomogeneous data, which should beavoided 14, graphical presentation of the risk reduction in eachtrial has been preferred. As the LMWHs show differentpharmacodynamic profiles1o, a regular meta-analysis of a setof trials was carried out only when the same type of LMWHin comparable doses was tested against a uniform controlgroup. Only in such a setting do we regard meta-analysis tobe statistically ,alid, contrary to the recent reviews ofNurmohamed el al.78 and Leizorovicz and co-workers"9 in""hich meta-analyses were performed without differentiationbetween drugs. The methodology used in the above two re,iewsdiffers from that in the present in several other aspects: thedefinition of high-quality studies 78 was different, some
orthopaedic trials21.36.37.39.40 were not assessed in bothreviews, the follow-up period was often restricted to 7-14 daysafter surgery, results were pooled irrespective of the LMWHdose given 79, heterogeneous groups of bleeding complications(sometimes including postoperative transfusion requirements)were summed, and asymptomatic (screened by the use ofscintigraphy in some of the studies) and symptomatic cases ofpulmonary embolism were pooled. In addition, not all patientswith reported pulmonary embolism had the diagnosisobjectively verified, and embolism rate and mortality Tale forelective hip surgery and hip fracture repair were assessed inthe same analysis. The conclusions from different overvie""s ofthe same subject may differ substantially; compared with thetwo above reviews, the results of the present analysis forcalculation of the incidence of pulmonary embolism were morein favour o[ LMWHs than unfractionated heparin in bothorthopaedic and general surgery. A higher incidence ofembolism (especially in patients undergoing orthopaedicsurgery and receiving LMWH) was found by both Nurmohamedet al.78 and Leizorovicz and associates 79. We feel that it isjustifiable to consider only those cases of symptomatic
DiscussionDuring the past two decades the need to prevent postoperativethromboembolic complications has gained wide acceptance, thefinal goal being to eradicate the 'silent killer' -fatal pulmonaryembolism -which, despite the use of prophylaxis, is still a majarconcern. Postoperative DVT causes considerable morbidity,with the potential risk of later chronic venous insufficiency.There is no doubt that the use of proper prophylaxis reducesboth the postoperative morbidity and mortality rate fromthromboembolism. A simple prerequisite is that prophylactictreatment should not be forgotten. Many regimens are notapplied in daily practice beca use of fear of bleedingcomplications and the burden of such extra therapy to thepatient. The development ofthe LMWHs offers some promisingaspects; the drugs are effective on a once-daily basis and donot require paraclinical monitoring. When used in equivalentantithrombotic clases, LMWHs theoretically should, based onanimal experiments, cause less bleeding than conventionalunfractionated heparin as they cause less inhibition ofthrombin6. 7.
Br. J. Surg.. Vol. 80. No. 6. June 1993700

low molecular weight heparins: l. N. J0rgensen et al.
pulmonary embolism that have been verified by objectivemeasures; this leads to a much lower incidence and pro videsa more reJiable comparison between unfractionated heparinand LMWHs.
In a review by Bergqvist80, data were compiled withoutapp.lication of meta-analysis methodology, excluding thepossibility of a statistical comparison bet\\'een treatmentgroups, It was concluded in that paper that LMWHs are atleast as effective as unfractionated heparin. In the presentreview, it is not known whether publication bias from notpublishing negative results is presento Having included allabstracts from conferences, it can only be hoped that such biasis minimized,
Duration of diagnostic follow-up is a keystone of studyquality; this is especially true for postoperative fatal pulmonaryemboJism, since most deaths occur >7 days after surgery81.Indeed, Bergqvist and Fredin82 found that patients \\ho sufferedfatal pulmonary embolism after hip fracture repair died at amedian of 31 days after operation. RecentJy, Huber and co-\\'orkers83 reported the incidence of postoperative pulmonaryemboJism to be increased by 30 per cent if all cases occurring\\'ithin 30 days of hospital discharge \\'ere algo included. Theresults of a substantial proportion of the published studies areerroneously based on a short-term follow-up \\'hen thrombo-embolic complications, injection haematoma and bruising aredescribed;only limited, ifany, attention is given to the incidenceoflate pulmonary embolism. This information must be collecteddirectly from the authors but is not always possible to obtain,
Some LMWHs are more efficient than placebo and dextranin the prevention of DVT in both elective and acute hip surgery.It is algo clear that LMWHs are at least as efficient asunfractionated heparin in elective orthopaedic operations.Meta-analysis has shown that Clexane significantly reduces theincidence of DVT compared with unfractionated heparinll,38.The combination of DHE and unfractionated heparin, t\\'Odrugs with synergistic action, has been used widely, especial1yin hip surgery, Although the prophylactic use of thispharmaceutical combination has be en reported to be safe84,DHE has been withdrawn in many countries as a consequenceof reported severe arteriospastic side-effects8S, On the basis ofseveral trials of the prophylactic use of DHE, these side-effectsmust be considered extremely rare3,35,46-SI, and the use ofLMWH \\ith DHE may still appear attractive as a potentialalternative, as the daily dose of DHE may be halved. On tbeother band, it seems that LMWH \\ithout DHE is as effectiveas unfractionated heparin in combination with DHE33,34,86,
This paper has reviewed 27 trials in which LMWHs wereadministered to 2230 patients undergoing orthopaedic surgery,The reported bleeding complications and transfusion require-ments give an overall impression that LMWHs are safe incomparison with placebo, dextran or unfractionated heparinwith or without DHE. It must be stressed that there is noevidence of fewer bleeding complications in LMWH-treatedpatients than in those given unfractionated heparin with orwithout DHE, unlike reports from experimental studies.
Which LMWH has the highest efficacy:side-effect ratiowhen applied to orthopaedic patients is unknown. Comparisonsbetween compounds will probably never be performed becauseofthe large number ofpatients needed for such a study. Efficacyand safety must be documented for each LMWH in differentsurgical situations. It has been claimed for Clexane that tbereis a close relationship between the antifactor Xa level and tbeclir.cal outcome. Tbe optimal antifactorXa concentration isnarrow because levels <0.1 unitsjml are related to thedevelopment of DVT and those >0.2 unitsjml to bleedingcomplications87, Whether LMWHs are more efficient tbanother regimens in preventing pulmonary embolism in ortho-paedic surgery cannot be assessed with current knowledge,although the present review points towards a reductive effectcompared with unfractionated heparin with or without DHE.The easy once-daily administration of LMWHs, possiblyleading to a higher compliance rate, combined with a probablegain in efficacy against DVT, argues for tbe use of LMWHs
for prophylaxis in orthopaedic surgery. Whether a synergisticprophylactic effect is obtained from the supplementary use ofmechanical devices (graded compression stockings or inter-mittent pneumatic compression) has Jet to be shown.
In general surgery the results again show a tendency towardsan overall better antithrombotic prophylactic effect usingLMWHs compared with unfractionated heparin. So far,LMWHs have not been tested in acute general surgery. It isnatural to believe that LMWHs are at least as effective asunfractionated heparin, which is of pro ven effect, especiallywhen combined with compression stockings88. The combinationof graded stockings and LMWHs was used in only twostudies58.67; further evaluation of Ibis combination is lacking.By analogy with the synergistic effect of the combined use ofunfractionated heparin and mechanical devices in patientsundergoing elective surgeryS9, better prophylaxis might beexpected by combining LMWHs with compression stockings,but this has so far not been documented.
In some older studies, significantly more bleeding wasobserved in LMWH-treated patients63.65-67, but theseproblems have been solved by altering the clase regimens56.66.67.As in the orthopaedic trials, there is no overall indication thatLMWHs are associated with fewer bleeding complications thanunfractionated heparin, but serious bleeding complications areun usual when recommended clases are employed.
When the high-quality studies in general surgery wereanalysed, it was found that Fragmin reduced the incidence ofsymptomatic pulmonary embolism compared with unfraction-ated heparin. That this could not be shown statistically for theother compounds is probably related to the limited number ofinvestigations rather than to a real difference between theefficacy of different compounds. The incidence of fatalpulmonary embolism was not significantly reduced by anyLMWH. To pro ve a reduction in the number offatal pulmonaryembolisms with LMWHs in general surgery compared withunfractionated heparin, a study of over 50000 patients isneeded. To prove a reduction in total perioperative mortalityrate, even larger numbers are required. This does not seemfeasible, and it must still be remembered that the clinicalinterpretation of such a study would require a thorough analysisof cost-effectiveness, facing the fact that LMWHs are still moreexpensive than unfractionated preparations. The biggestapparent advantage of LMWHs in general surgery is theirefficacy by once-daily administration.
It has recently been stated that prophylaxis of DVT withLMWH will benefit orthopaedic but not general surgicalpatients 78.9°. The present review is partly supportive of this;the percentage reduction in the risk ofDVT appears comparablein the two groups of patients, but the incidence of suchthrom bosis is higher in orthopaedic surgery, leading toa greaterabsolute number of cases of DVT prevented. Thus, use of aLMWH may be more cost effective in orthopaedic surgerydespite the higher price of the drug. If future large-scale trialsconfirm the tendency in the present literature of a reducedincidence of pulmonary embolism through the use of LMWHsin general surgery, the statement above may have to bemodified.
The clases in LMWH prophylactic regimens have beenwidely examined. The present recommendations for orthopaedicsurgery are: 3200 units once daily or 2400 units twice daily(Clexane), 5000 units once daily or 2500 units twice daily(Fragmin), 30-50 unitsjkg once daily (Fraxiparin) and50 unitsjkg once daily (Logiparin). For general surgery, therecommended clases are: 1600 units once daily (Clexane),2500-5000 units once daily (Iow- and high-risk patients,Framin), 2500 units (equivalent to 7500 Institute Choay Units)once daily (Fraxiparin) and 3500 units once daily (Logiparin).Even though the optimal plasma concentration of antifactorXa is 0.1-0.2 units/ml, the differences between the drug clasesrecommended are considerable and may reflect the pharmaco-logical inhomogeneity of the preparations and the variation inpresent clinical documentation. Much concern has beenexpressed on the antifactor Xa:antifactor IIa ratio of LMWHs
701Br. J. Surg.. Vol. 80. No. 6. June 1993

Low molecular weight heparins: L. N. J0rgensen et al.
12.
13.
14.
15.
16.
with regard to the bleeding risk and antithrombotic efficacy.Whether this ratio is clinica\ly relevant today is a matter ofdebate. It has been shown that the plasma antifactor Xa leveldoes not correlate with the incidence of thromboembolism32or with that of excessive bleeding in patients undergoing hipsurgery91. Clinical results have shown that the early findingsin animal models of a reduced bleeding tendency with LMWHs,compared with unfractionated heparin in equiantithromboticclases, should not be extrapolated to humans.
Despite the considerable accumulation of literature onLMWHs, some problems must sti\l be solved. The optimal timefor beginning and especia\ly forstopping prophylaxis has to beestablished. Too few data on the efficacy of combinations withmechanical methods of prophylaxis are available. Although itseems safe to combine lumbar extradural or spinal anaesthesiawith a LMWH, a review of reported cases of intraspinalbleeding complications in this situation is particularly needed.
17.
18.
19.ConclusionsThe use of LMWHs for prophylaxis against post opera ti vethromboembolic complications has not been fully evaluated.In orthopaedic surgery, LMWHs are at least as efficient asother regimens in the prevention of DVT and pulmonaryembolism. In general surgery, there mar be a betterprophylactic efficacy against DVT and pulmonary embolismcompared with unfractionated heparin. However, no differencebetween LMWHs and unfractionated heparin with respect tothe number of fatal cases could be detected. With therecommended clases, the routine use of the drugs is gafe withrespect to bleeding complications and transfusion requirements.A major advantage of LMWHs is that they are efficient whenadministered once daily: this benefits nursing routines.
20.
21
22.
23.
24.
25.
26.
27.
28.
29.
30.
31
32.
References1. An International Multicentre Trial. Prevention of fatal
postoperative pulmonary embolism by 10w doses of heparin.Lancet 1975; ii: 45-51.
2. Col1ins R, Scrimgeour A. Yusuf S, Peto R. Reduction in fatalpulmonary embolism and \'enous thrombosis by perioperativeadministration of subcutaneous heparin. Overview of results ofrandomized trials in general, orthopedic, and urologic surgery.N Engl J .\fed 1988; 318: 1162-73.
3. Lassen MR, Borris LC, Christiansen HM et al. Heparinjdihydroergotamine for \'enous thrombosis prophylaxis: com-parison of low-dose heparin and 10w molecuIar weight heparinin hip surgery. Br J Surg 1988; 75: 686-9,
4. Persson E, Nordenstrom 1, Nilsson-Ehle P, Hagenfeldt L.Lipolytic and anticoagulant activities of a low molecular weightfragment of heparin. Eur J Clin Im'est 1985; 15:215-20.
5. Barrowcliffe TW, Thomas DP. Low molecular weight heparins:antithrombotic and haemorrhagic effects and standardization.Acta Chirurgica Scandinarica. Supplemenlum 1988; 543: 57-64.
6, Carter Cl, Kelton lG, Hirsch 1, Cerskus AL, Santos A V,Gent M. The relationship between the hemorrhagic andantithrombotic properties of 10w molecular weight heparins andheparin. Blood 1982; 59: 1239.
7. Bergqvist D, Nilsson B, Hedner U, Pedersen PC, 0stergaard PB.The effects of heparin fragments of different mo]ecular weight inexperimenta] thrombosis and haemostasis. Thromb Res ]984; 38:589.
8. Fabris F, Fussi F, Casonato A et al. Normal and low molecu]arweight heparins: interaction with human plateJets, Eur J ClinInvest 1983; 13: 125-30.
9. Lane DA, Pej]er G, Flynn AM, Thompson EA, Lindah] U.Neutralization of heparin-related saccharides by histidine-richg]ycoprotein and platelet factor 4. J Biol Chem 1986; 261: 3980-6.
10. Fareed 1, Walenga 1M, Hoppenstadt D, Huan X, Racanelli A.Comparative study on the in ritro and in vivo activities of sevenlow-molecular-weight heparins. Haemostasis 1988; 18(Suppl 3):3-15.
11. Collins R, Gray R, Godwin 1, Peto R. Avoidance of large biasand large random errors in the assessment of moderate treatmenteffects: the need for systematic overviews. SIal Med 1987; 6:245-50.
Mantel N, Haentszel W. Statistical aspects of the analysis of datafrom retrospective studies. J ¡Vall Cancer Insl 1959; 22: 719-48.Thompson SG, Pocock SI. Can meta-analyses be trusted? La/¡cet1991;ii: 1127-30.Furberg CD, Morgan TM. Lessons from overviews ofcardiovascular iríais. SIal Med 1987; 6: 295-303.Bergqvist D. Posloperalive Thromboembolism. FrequencJ",EliologJ", Proph_vlaxis. Berlin: Springer-Verlag, 1983.Turpie AGG, Levine MN, Hirsch 1 el al. A randomizedcontroJJed trial of a low molecular weight heparin (Enoxaparin)to prevent deep-vein thromoosis in patients undergoing electivehip surgery. ,v Engl J Med 1986; 315: 925-9.Leclerc IR. Geerts WH, Desjardins L el al. Prevention of deepvein thrombosis after major knee surgery. A randomized.double-blind trial comparing a low molecular weight heparinfragment (Enoxaparin) to placebo. Thromb HaemOSl 1992; 67:417-23.lergensen PS, Knudsen lB, Broeng L el al. The thrombo-prophylactic effect of a low molecular weight heparin (Fragmin)in hip fracture surgery: a placebo controJJed study. Clin Orlhop1992; 278: 95-100.Lassen MR, Borris LC, Christiansen HM el al. Prevention ofthromboembolism in hip-fracture patients. Comparison oflow-dose heparin and 10w-molecuJar-weight heparin combinedwith dihydroergotamine. Arch Orthop Trauma Surg 1989; 108:10-13.Lassen MR, Borris LC, Christiansen HM el al. Prevention ofthromboembolism in 190 hip arthroplasties. Comparison ofLMW heparin and placebo. Acla Orlhop Scand 1991: 62: 33-8.Levine MN, Hirsch 1, Gent M el al. Pre,.ention of deep veinthrombosis alter elective hip surgery. A randomized trialcomparing low molecular weight heparin wi¡h standardunfractionated heparin. Ann Imern ,\1ed 1991; 114: 545-51.Terholm C, Broeng L, lergensen PS el al. Thromboprophylaxisby low-molecular-weight heparin in elective hip surgery. Aplacebo controJJed study. J Sane Joillt Surg [Sr] 1991: 73-B:434-8.
Danish Enoxaparin Study Group. Low-molecular-\,eightheparin (Enoxaparin) I;ersus dextran 70. The prevention ofpostoperative deep vein thrombosis alter total hip replacement.Arch Imern .\1ed 1991; 151: 1621-4.Eriksson BI, Zachrisson BE, Teger-Nilsson A-C. Risberg B.Thrombosis prophylaxis with low mo]ecular \,eight heparin intotal hip replacement. Sr J Surg 1988; 75: 1053-7.Miitzsch T, Bergqvist D, Fredin H, Hedner U. Low moJecularweight heparin compared with dextr~n as prophylaxis againstthrombosis after total hip replaqement. .4cla ChirurgicaScandinarica 1990; 156: 445-50.Miitzsch T, Bergqvist D, Fredin H, IHedner U, Lindhagen A,Nistor L. Comparison of the thromboprophylactjc effect of a lowmolecular weight heparin rersus dextran in total hip replacement.Thrombolic and Haemorrhagic Disorders 1991; 3: 25-9.Chiapuzzo E, arengo GB, Ottria G, Chiapuzzo A, Palazzini E,FusiJJo M. The use of low molecuJar weight heparins forpostsurgical deep vein thrombosis prevention in orthopaedicpatients. J Inl Med Res 1988; 16: 359-66.Pini M, Tagliaferri A, Manotti C, Lasagni F, Rina]di E,Dettori AG. Low molecular weight heparin (Alfa L~1WH)compared with unfractionated heparin in prevention of deep-veinthrombosis after hip fractures. 1m Angio11989; 8: 134-9.Barre 1, Pfister G, Potron G el al. Comparative efficacy andtolerante of Kabi 2165 and standard heparin for preventjon ofdeep venous thrombosis after total hip prosthesis. J.\lal Vasct987; 12: 90-5.Dechavanne M, ViJJe D, Berruyer M el al. Randomized trial ofa low-mo]ecular-weight heparin (Kabi 2]65) rersus adjusted-dose subcutaneous standard heparin in the prophylaxis ofdeep-vein thrombosis alter elective hip surgery. Haemostasis1989; 19: 5-12.Binsack T, ZeJJner M, Schimming 1 el al. Thrombo~is prophylaxiswith LMW heparin and sodium heparin in patients with totalhip replacement. Thromb Res 1986; Suppl 6: 83.Eriksson BI, Kii]ebo P, Anthmyr BA, Wadenvik H, Tengbom L,Risberg B. Prevention of deep-vein thrombosis and pulmonaryembolism alter total hip replacement. Comparison of low-molecular-weight heparin and unfractionated heparin. J SaneJoinl Surg [Am] 1991; 73-A: 484-93.Breyer HG, Rahmanzadeh R, Bacher P, Wemer B. LMW-heparin versus heparin-DHE in orthopedic surgery. ThrombHaemosl ]987; 58: 241.
33.
702 Br. J. Surg.. "'°1. 80. No. 6. June 1993
~

34.
54.35.
55.36.
56,
57.
38
58.
39.59
40.60.
61
42.
62.
13 63.
4464.
45. 65.
4666.
47.
67.48
68,
49.69.
50. 70.
7151
Low molecular weight heparins: L. N. J0rgensen et al.
thrombosis by two different heparin types. Inl J Clin PharmacolTher Toxicol1988; 26: 304-9.Creperio O, Marabini M, Ciocia O, Bergonzi M, Fincato M.Evaluation ofthe effectiveness and safety of Fragmin (Kabi 2185)versus calcium heparin in the prevention of deep venousthrombosis in general surgery. Mincrl'a Chir 1990; 45: 1101-6.Onarheím H, Lund T, Heimdal A, Arnesje B. A low molecularweíght heparin (Kabi 2165) for prophylaxis ofpostoperative deepvenous thrombosis. ACla Chirurgica Scandinarica 1986; 152:593-6.Bergqvist D, Matzsch T, Burmark US el al. Low molecularweight heparin given the evening before surgcry compared withconventional low dose heparin in prevention of thrombosis.Sr J Surg 1988; 75: 888-91.Kakkar VV, Murray WJO. Efficacy and safety of low-moJecular-weíght heparin (CY216) in preventing postoperative venousthromboembolism: a co-operatí\'e study Sr J Surg 1985; 72:786-91.Tbe European Fraxiparin Study Oroup. Comparison of a lowmolecular weight heparin and unfractionated heparin for theprevention of deep vein thrombosis in patients undergoingabdominal surgery. Sr J Surg 1988; 75: 1058-63.Caen JP. A randomized double-blind study between a lowmolecular weight heparin Kabi 2165 and standard heparin in theprevention of deep vein thrombosis in general surgery. A Frenchmulticentre trial. Thromb Haemasl1988; 59: 216-20.Adolf J, Knee H, Roder JD, van de Flierdt E, Siewert JR.Prevention of thromboembolism with low-molecular-weightheparin in abdominal surgery. Dtsch Med Wochenschr 1989; 114:48-53.Heilmann L, Kruck M, Schindler AE. Thrombosis prophyl.axisin gynecology: a randomized double-blind study between lowmolecular weight heparin and unfractionated heparin. Geburl-schilfe Frauenheilkd 1989; 49: 803-7.Koppenhagen K, Matthes M, Haring R, Troster E, Wolf H,Welzel D. Prophylaxis of thromboembolism in electiveabdominal surgery. Comparison of efficacy and safety of lowmolecular weight heparin and unfractionated heparin. Münchene.~edizinische Wochenschrifl 1990; 132: 677-80.Bergqvist D, Burmark OS, Frisell J el al. Low molecular weightheparin once daily compared wíth conventionallow-dose heparintwíce daily. A prospective double-blind multicentre trial onpreventíon of postoperative thromboembolism. Sr J Surg 1986;73: 204-8.Fricker J-P, Vergnes Y, Schach R el al. Low dose heparin versuslow molecular weíght heparin (Kabi 2165, Fragmín) in theprophylaxís of thromboemboIíc complicatíons of abdominaloncological surgery. Eur J Clin Inves11988; 18: 561-7.Borstad E, Urdal K, Handeland O, Abíldgaard U. Comparisonof low molecular weíght heparin vs unfractíonated heparin ingynecological surgery. Acla Obslel Gynecol Scand 1988; 67:99-103.Koller M, Schoch U, Buchmann P, Largiader F, von Felten A,Frick PO. Low molecular weight heparin (Kabi2165) asthromboprophylaxis in elective visceral surgery. A randomized,double-blind study vs unfractionated heparin. Thromb Haemosl1986; 56: 243-6.Schmitz-Huebner U, Bünte H, Freise O el al. ~Iinical efficacyof low molecular weight heparin in postoperative thrombosisprophylaxis. Klin Wochenschr 1984; 62: 349-53.Speziale F, Verardi S, Taurino M el al. Low molecular weightheparin prevention of post-opera ti ve deep vein thrombosis invascuJar surgery. Pharmalherapeulica 1988; 5: 261-8.Verardi S, Casciani CU, Nicola E el al. A multicentre study onLMW-heparin effectiveness in preventing postsurgical thrombosis.Inl Angio/1988; 7(Suppl 3): 19-24.Verardi S, Cortese F, Baroni B, Boffo V, Casciani CU,Palazzini E. Deep veín thrombosis prevention in surgicalpatients: effectiveness and safety of a new low-molecular-weightheparin. Currenl Therapeulic Research 1989; 46: 366- 72.Corrado F, Finí M, Severini O el al. Low molecular weightheparin (Fluxum) preventíon of post-operative thrombosís inurologícal surgery. A controlled study. Clínical Trials Journal1989; 26: 138-48.Samama M, Bernard P, Bonnardot JP, Combe- Tarnzali S,Lanson Y, Tissot E. Low molecular weight heparin comparedwith unfractionated heparin in preventíon of postoperativethrombosís. Sr J Surg 1988; 75: 128-31.Dahan M, Levasseur P, Bogaty J, Bonéu B, Samama M.Preventíon of postoperatíve deep vein thrombosís (DVT) ín
72.
Haas S, Stemberger A, Fritsche H-M, Lechner F. Untersuchungenzur antithrombotischen Wirksamkeit von niedermolekularemHeparin Kabi. Die Medizinische Well 1987; 38: 714-20.Haas S, Stemberger A, Fritsche HM el al. Prophylaxis of deepvein thrombosis in high risk patients undergoing total hipreplacement with low moleclar weight heparin plus dihydro-ergotamine. Arzneimitlelforschung 1987; 37: 839-43.Freick H, Haas S. Prevention of deep vein thrombosis bylow-molecular-weight heparin and dihydroergotamine in patientsundergoing total hip replacement. Thromb Haemost 1991; 63:133-43.Kominger C, Schlag G, Poigenfúrst J el al. Randomized trial oflow molecular weight heparin rersus low dose heparinjacenocoumarin in patients with hip fracture -thrombo-prophylactic effect and bleeding complications. Thromb Haemost1989; 62: 187.Planes A, Vochelle N, Mazas F et al. Prevention of postoperativevenous thrombosis: a randomized trial comparing unfractionatedheparin with low molecular weight heparin in patientsundergoing total hip replacement. Thromb HaemOSl 1988; 60:407-10. ,The German Hip Arthroplasty Trial (GHA T) Group. Preventionof deep vein thrombosis with low-molecular-weight heparin inpatients undergoing total hip replacement. A randomized trial.Arch Orlhop Trauma Surg 1992; 111: 110-20.Leyvraz PF, Bachmann F, Hoek J el al. Prevention of deep veinthrombosis after hip replacement: randomised comparisonbetween unfractionated heparin and low molecular weightheparin. BMJ 1991; 303: 543-8.Monreal M, Lafoz E, Navarro A el al. A prospective double-blindtrial of a low molecular weight heparin once daily compared withconventional low-dose heparin three times daily to preventpulmonary embolism and venous thrombosis in patients withhip fracture. J Trauma 1989; 29: 873-5.Ockelford PA, Patterson J, Johns AS. A double-blindrandomized placebo-controlled trial of thromboprophylaxis inmajor elective general surgery using once daily injections of alow molecular weight heparin fragment (Fragmin). ThrombHaemosl 1989; 62: 1046-9.Valle 1, Sola G, Origone A. Controlled clinical study of theefficacy of a new low molecular weight heparin administeredsubcutaneously to prevent post-operative deep venous throm-bosis. Curr Med Res Opin 1988; 11: 80-6.Pezzuoli G, Neri Semeri GG, Settembrini P et al. Prophylaxisof fatal pulmonary embolism in general surgery usinglow-molecular-weight heparin Cy 216: a multicentre, double-blind, randomized, controlled, clinical trial rersus placebo. ¡nISurg 1989; 74: 205-10.Clagett GP, Reisch JS. Prevention of venous thromboembolismin general surgical patients. Results of meta-analysis. Ann Surg1988; 208: 227-40.Kakkar VV, Stringer MD, Hedges AR el al. Fixed combinationsoflow-molecular-weight or unfractionated heparin plus dihydro-ergotamine in the prevention of postoperative deep veinthrombosis. Am J Surg 1989; 157: 413-18.Welzel D, Wolf H, Koppenhagen K. Antithrombotic defenseduring the postoperative periodo Clinical documentation of lowmolecular weight heparin. Arzneimillelforschung 1988; 38: 120-3.Sasahara AA, Koppenhagen K, Haring R, Welzel D, Wolf H.Low molecular weight heparin plus dihydroergotamine forprophylaxis of postoperative deep vein thrombosis. Br J Surg1986; 73: 697-700.Baumgartner A, Jacot N, Moser G, Krahenbühl B. Preventiono, postoperative deep vein thrombosis by one daily injection oflow molecular weight heparin and dihydroergotamine. Vasa1989; 18: 152-6.Steiner RA, Keller K, Lüscher T, Schreiner WE. A prospectiverandomized trial of low molecular weight heparin-DHE andconventional heparin-DHE (with acenocoumarol) in patientsundergoing gynaecological surgery. Arch Gynecol Obslel 1989;244: 141-50.Voigt J, Hamelmann H, Hedderich J, Seifert J, Buchhammer T,K5hler A: Wirksamkeit und unerwünschte Nebenwirkungen vonniedermolekularem Heparin-Dihydroergotamin zur Thrombo-emboliprophylaxe in der Abdominalchirurgie. Zentralbl Chir1986; 111: 1296-305.Briel RC, Doller P, Hermann CuPo Thromboembolismprophylaxis with the low-molecular weight heparin Fragmin inhysterectomy cases. Geburlshilfe Frauenheilkd 1988; 48: 160-4.Catania G, Salanitri G. Prevention of postoperative deep vein
52.
73.53.
703Br. J. Surg.. Vol. 80. No. 6. June 1993

Low molecular weight heparins: L. N. J0rgensen et al.
74.
85.
75.86.
76. 87.
77.
88.
78.
89.79.
80.90.
81.
82. 91.
of perioperative thrombosis with low molecular weight heparinand dihydroergotamine. A study of the incidence of lethalpulmonary embolism and adverse effects with special regard tovasospasm and myocardial infarction. Arzneimittelforschung1988;38: 1516-19.Gatterer R. Ergotism as a complication of thromboembolicprophylaxis with heparin and dihydroergotamine. Lancet 1986;ii: 638-9.Wilson NV, Das SK, Kakkar VV. Failure of dihydroergotamineto improve the results of low molecular weight heparinprophylaxis against venous thrombosis in hip surgery. Br JHaematoI1990; 76(Suppll): 22.Levine MN, Planes A, Hirsch J, Goodyear M, Vochelle N,Gent M. The relationship between anti-factor Xa level andclinical outcome in patients receiving Enoxaparin low molecularweight heparin to prevent deep vein thrombosis after hipreplacement. Thromb Haenl?st 1989; 62: 940-4.Wille-Jorgensen P, Hauch O, Dimo B, Christensen SW,Hansen B, Jensen R. Prophylaxis of deep venous thrombosisfollowing acute abdominal surgery. An evaluation of threeprotocols. Surg G}.necoIObstet 1991; 172: 44-9.Wille-Jorgensen P, Thorup J, Fischer A, HoJst-Christensen J,Flamsholdt R. Heparin with and without graded compressionstockings in the prevention ofthrom~oembolic complications ofmajar abdominal surgery: a rando~zed trial. Br J Surg 1985;72: 579-81.Routledge PA, West RR. Low molecular weight heparin.Probably better Iban conventional heparin in orthopaedicpractice but not in general surgical practice. B...fJ 1992; 305: 906(Editorial ).The Post-surgery Logiparin Study Group. CorreJation betweenanti-Xa activity and occurrence of DVT and haemorrhage inpost-surgical patients treated with either Logiparin (LMWH) orunfractionated heparin. Thromb Res 1992; 65: 641-50.~3.
84.
malignant patients by Fraxiparin (a low molecular weightheparin). A cooperative trial. Thromb Haemosl1989; 62: 519.Barbui T, Cassinelli G, Cortelazzo S el al. Comparison of lowmolecular weight heparin CY 216 and unfractionated heparin inpreventing postoperative venous thromboembolism in generalsurgery: preliminary results ora cooperativestudy. Fibrinolysis1990; 4(Suppll): 79.Leizorovjcz A, Picolet H, Peyrieux JC, Boissel JP, HBPMResearch Group. Prevention of perioperative deep veinthrombosis in general surgery: a multicentredoubIe blind studycomparing two clases of Logiparin and standard heparin. Br JSurg 1991; 78: 412-16.Hoffmann R, Largiader F, RoethIin M. Perioperative Thrombo-embolie-ProphyIaxe: niedrig dosiertes Heparin oder lowmolecular weight Heparin-DHE, Vor- und Nachteile. Helv ChirACla 1987; 54: 521-5.Hartl P, Brücke P, Dienstl E, Vinazzer H. Prophylaxis ofthromboembolism in general surgery: comparison betweenstandard heparin and Fragmin. Thromb Res 1990; 57: 577-84.Nurmohamed MT, RosendaaI FR, Büller H el al. Low-molecular-weight heparin versus standard heparin in general andorthopaedic surgery: a meta-analysis. Lance11992; 340: 152- 7.Leizorovicz A, Haugh MC, Chapuis F-R, Samama MM,Boissel J-P. Low molecular weight heparin in prevention ofperioperative thrombosis. BMJ 1992; 305: 913-20.Bergqvist D. Review of clinical trials of low molecular weightheparins. Clinical re\iew. Eur J Surg 1992; 158: 67-78.Hauch O, Jorgensen LN, Khattar SC el al. Fatal pulmonaryembolism associated with surgery. ACla Chirurgica Scandinavica1990; 156: 747-9.Bergqvist D, Fredin H. Pulmonary embolism and mortality inpatients with fractured hips -a prospective consecutive study.Eur J Surg 1991; 157: 571-4.Huber O, Bounameaux H, Borst F, Rohner A. Postoperativepulmonary embolism after hospital discharge -an underestimatedrisk. Arch Surg 1992; 127: 310-13.Wolf H, Welzel P, Kaiser H el al. Evaluation of the prevention Paper accepted 14 December 1992
-~
~
704 Br. J. Surg.. Vol. 80. No. 6. June 1993