Embed Size (px)
Citation preview
Detect.Connect.Control.Preventing a Million Together
NLA Spring Clinical Lipid UpdateFebruary 27, 2015
• Million Hearts overview• Progress report• Detect.Connect.Control.
– Hypertension Cholesterol: Questions for You
Agenda
• What is working in cholesterol management?• What is missing?• Who’s on the Design Team to fill key gaps?• Who are the Implementers?• How quickly can we act?
Hypertension CholesterolQuestions for You
Million Hearts®
• National initiative co-led by CDC and CMS• In partnership with federal, state, and private
organizations
4
Goal: Prevent 1 million heart attacks and strokes by 2017
Key Components of Million Hearts®
Keeping Us HealthyChanging the context
Excelling in the ABCSOptimizing care
Prioritizing the ABCS
Health tools and technology
Innovations in care delivery TRANS
FAT
Health Disparities
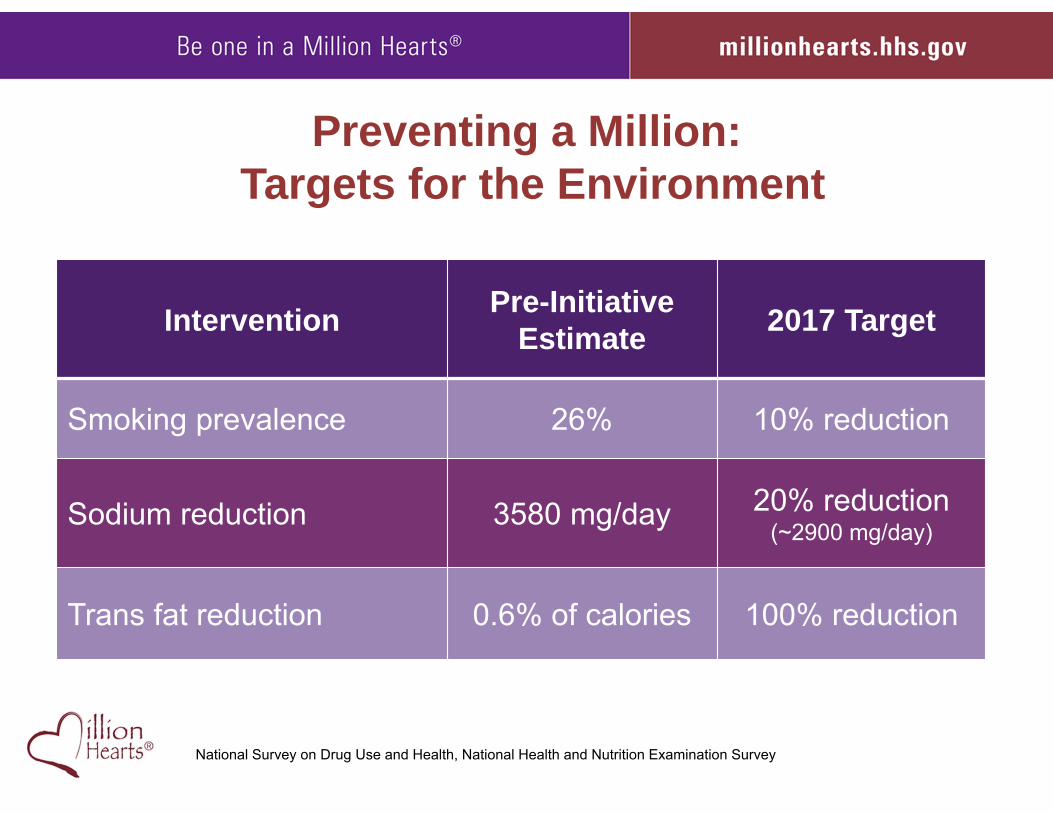
Preventing a Million: Targets for the Environment
Intervention Pre-InitiativeEstimate 2017 Target
Smoking prevalence 26% 10% reduction
Sodium reduction 3580 mg/day 20% reduction (~2900 mg/day)
Trans fat reduction 0.6% of calories 100% reduction
National Survey on Drug Use and Health, National Health and Nutrition Examination Survey
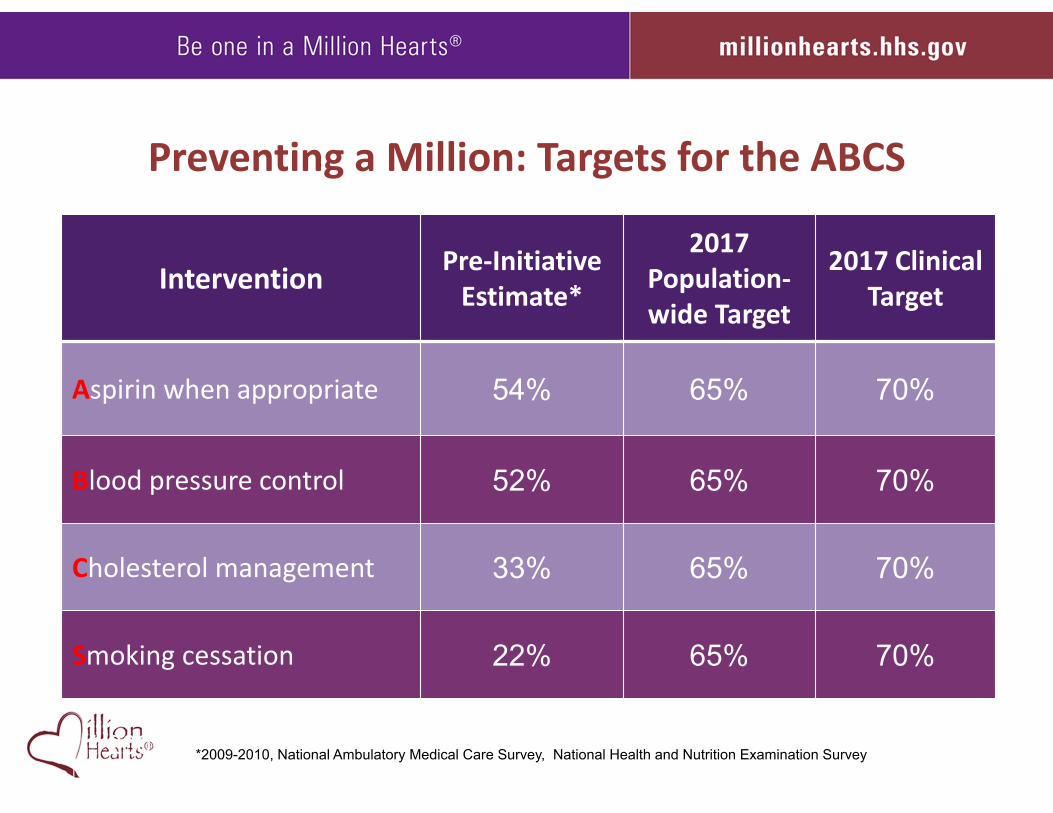
Preventing a Million: Targets for the ABCS
Intervention Pre‐InitiativeEstimate*
2017 Population‐wide Target
2017 ClinicalTarget
Aspirin when appropriate 54% 65% 70%
Blood pressure control 52% 65% 70%
Cholesterol management 33% 65% 70%
Smoking cessation 22% 65% 70%
National Ambulatory Medical Care Survey, National Health and Nutrition Examination Survey* 2009-2010*2009-2010, National Ambulatory Medical Care Survey, National Health and Nutrition Examination Survey
• Engagement and activation• Clinical Quality Measure alignment• Understand what works, where, and why• Resources that help• Focus on what makes a difference
Million Hearts Progress to Date
>110 partners, 50 states, >53K e‐subscribers, 110 Congregations>110 partners, 50 states, >53K e‐subscribers, 110 Congregations
Progress: Addressing Health Disparities
• CDC-Association of State and Territorial Health Officials Million Hearts® Hypertension Control Project• Ohio improved control among African American males
• CMS’ Quality Improvement Organizations• Special projects in 3 states, 1.9M patients, 400+ practices
and partners has led to QIO-wide priority in 2015.• Community and faith-based organizations
• NAACP, National Alliance for Hispanic Health, South Asian Heart Center
• “100 Congregations” for Million Hearts®
• PCORI funding
• Engagement and activation• Clinical Quality Measure alignment• Understand what works, where, and why• Resources that help• Focus on what makes a difference
Million Hearts Progress to Date
As of July 2013
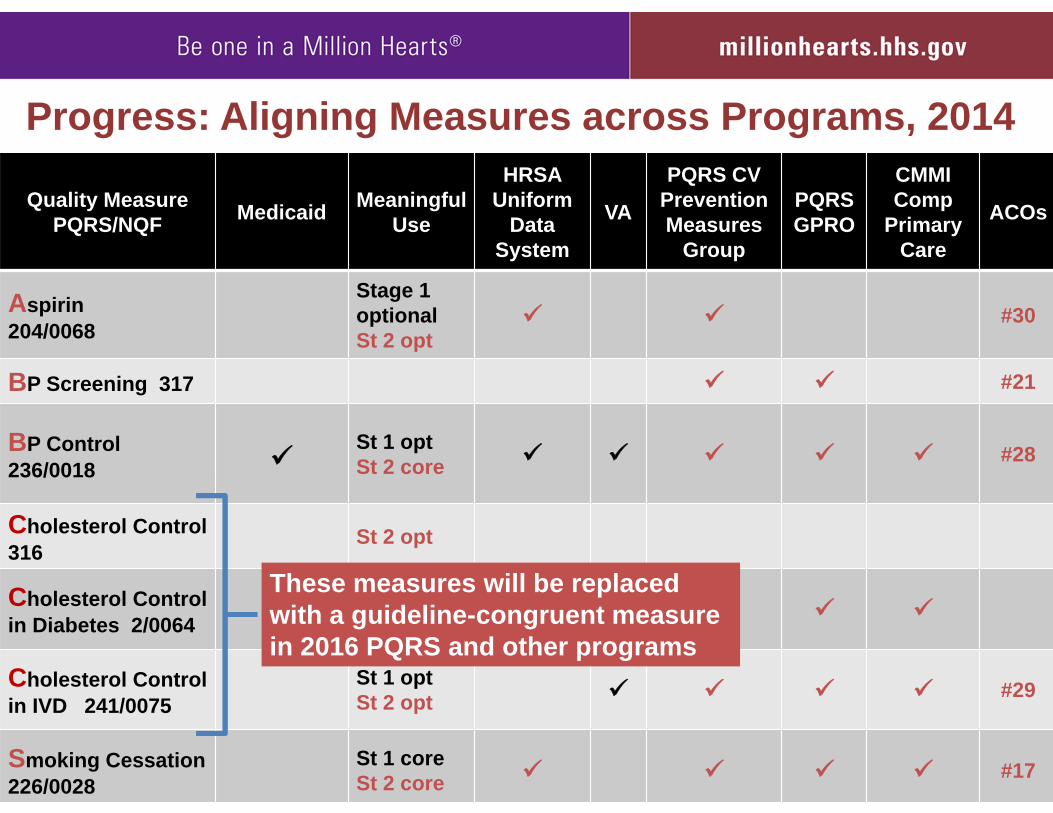
Quality MeasurePQRS/NQF Medicaid Meaningful
Use
HRSA Uniform
DataSystem
VA
PQRS CV Prevention Measures
Group
PQRS GPRO
CMMI Comp
Primary Care
ACOs
Aspirin204/0068
Stage 1 optionalSt 2 opt
#30
BP Screening 317 #21
BP Control236/0018
St 1 optSt 2 core #28
Cholesterol Control 316
St 2 opt
Cholesterol Control in Diabetes 2/0064
St 1 optSt 2 opt
Cholesterol Control in IVD 241/0075
St 1 optSt 2 opt #29
Smoking Cessation226/0028
St 1 coreSt 2 core #17
Progress: Aligning Measures across Programs, 2014
These measures will be replaced with a guideline-congruent measure in 2016 PQRS and other programs
• Engagement and activation• Clinical Quality Measure alignment• Understand what works, where, and why• Resources that help• Focus on what makes a difference
Million Hearts Progress to Date
Champions, AMGA MUPDChampions, AMGA MUPD

2013 Million Hearts®
Hypertension Control Champions
• Dr. Luz Ares, Broadway Internal Medicine; Queens, NY • Cheshire Medical Center/Dartmouth-Hitchcock; Keene, NH• Dr. Jen Brull; Plainville, Kansas• Dr. Nilesh V. Patel; Audubon, PA• Pawhuska Indian Health Center; Pawhuska, OK • Kaiser Permanente Northern California• River Falls Medical Clinic; River Falls, WI• ThedaCare; Appleton, WI• Veterans Health Administration
9 ChampionsSolo to 70,000 Clinicians
8.3M People3.4M with Hypertension
~81% Control Rate
High Performers’ Secrets to Success• Make hypertension control a priority • Deploy a team—working off the same playbook
– Use an evidence-based protocol– Connect to community resources that help people achieve & maintain
control • Use the EHR as a tool for quality
– Maintain a registry of those with hypertension and proactively reach out to those uncontrolled
– Return timely performance data to the team—and the patient– Provide a patient portal for prompt exchange of readings and advice– Comb through EHR data for those “hiding in plain sight”
• Eliminate/minimize obstacles to good control– Teach self-monitoring and good technique to staff and patients– Prescribe 90 day; simplify regimen; encourage mail-order and pillboxes– No cost-share for BP checks
• Recognize and reward patients and staff
• Engagement and activation• Clinical Quality Measure alignment• Understand what works, where, and why• Resources that help• Focus on what makes a difference
Million Hearts Progress to Date
Guides, Healthy Eating Center, CQM Dashboard, Protocols
Guides, Healthy Eating Center, CQM Dashboard, Protocols
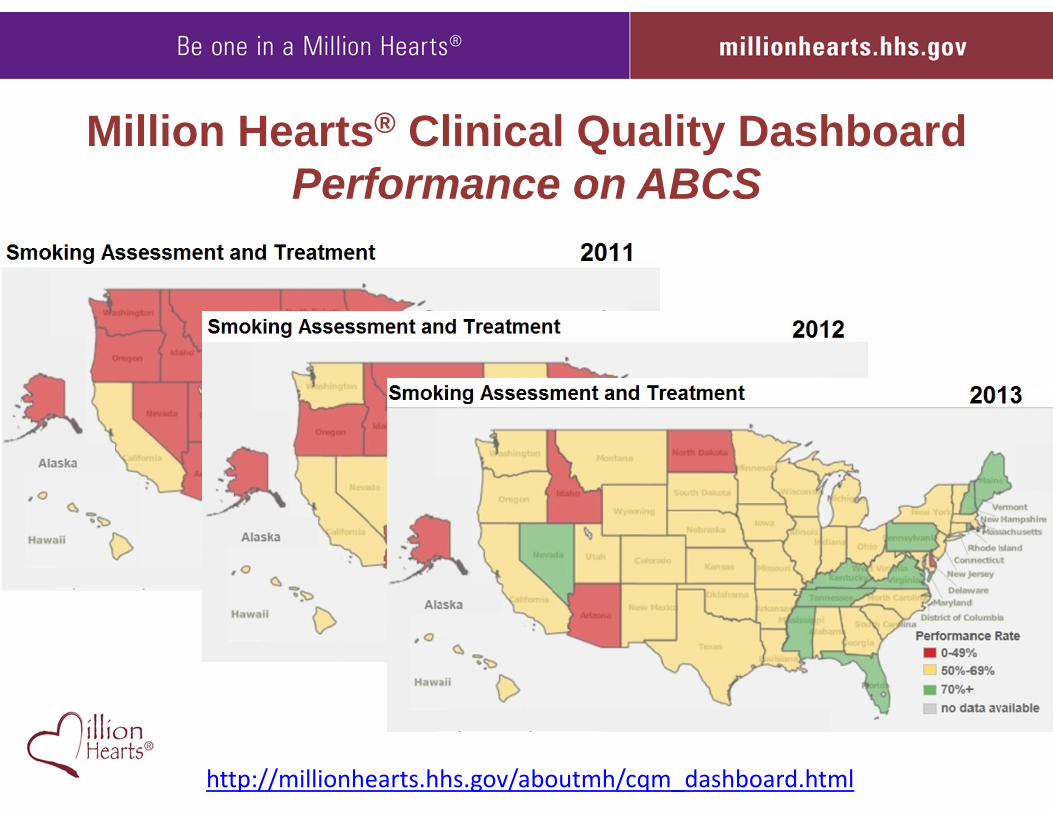
Million Hearts® Clinical Quality DashboardPerformance on ABCS
http://millionhearts.hhs.gov/aboutmh/cqm_dashboard.html
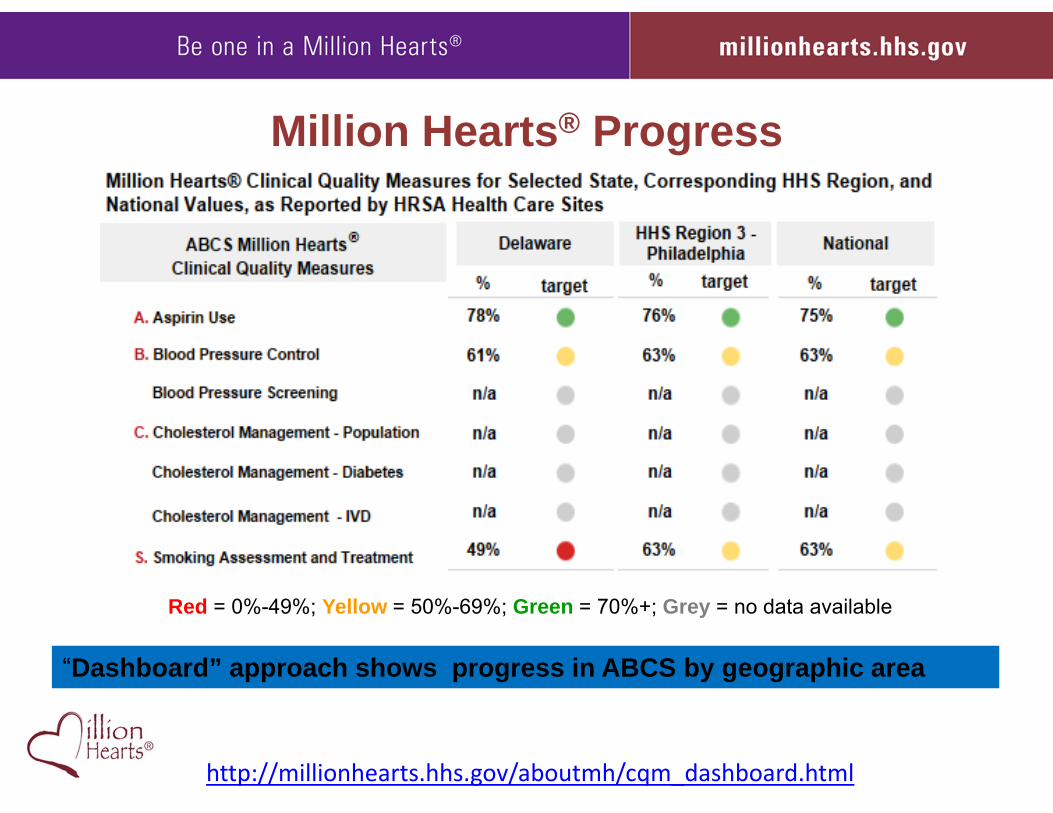
Million Hearts® ProgressOptimizing Care – Performance on ABCS
State Level Data available from HEDIS, UDS, PQRS
http://millionhearts.hhs.gov/aboutmh/cqm_dashboard.html
“Dashboard” approach shows progress in ABCS by geographic area
Red = 0%-49%; Yellow = 50%-69%; Green = 70%+; Grey = no data available
• Engagement and activation• Clinical Quality Measure alignment• Understand what works, where, and why• Resources that help• Focus on what makes a difference
Million Hearts Progress to Date
6.3M fewer smokers10M more BPs under control20% less sodium each day
Focus on those with the greatest burden and at the greatest riskStill committed to aspirin, cholesterol, and trans‐fat
6.3M fewer smokers10M more BPs under control20% less sodium each day
Focus on those with the greatest burden and at the greatest riskStill committed to aspirin, cholesterol, and trans‐fat
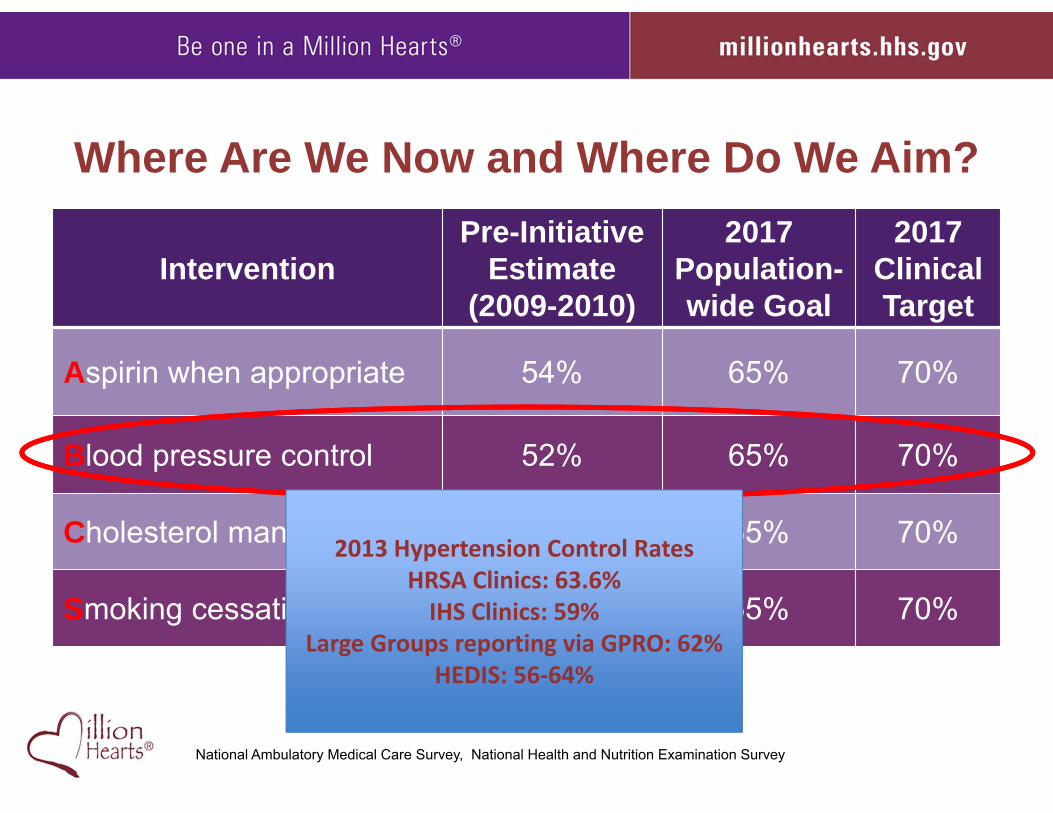
Where Are We Now and Where Do We Aim?
InterventionPre-Initiative
Estimate(2009-2010)
2017 Population-wide Goal
2017 ClinicalTarget
Aspirin when appropriate 54% 65% 70%
Blood pressure control 52% 65% 70%
Cholesterol management 33% 65% 70%
Smoking cessation 22% 65% 70%
National Ambulatory Medical Care Survey, National Health and Nutrition Examination Survey
19
2013 Hypertension Control RatesHRSA Clinics: 63.6% IHS Clinics: 59%
Large Groups reporting via GPRO: 62%HEDIS: 56‐64%
0
5
10
15
20
25
30
35
Milli
ons
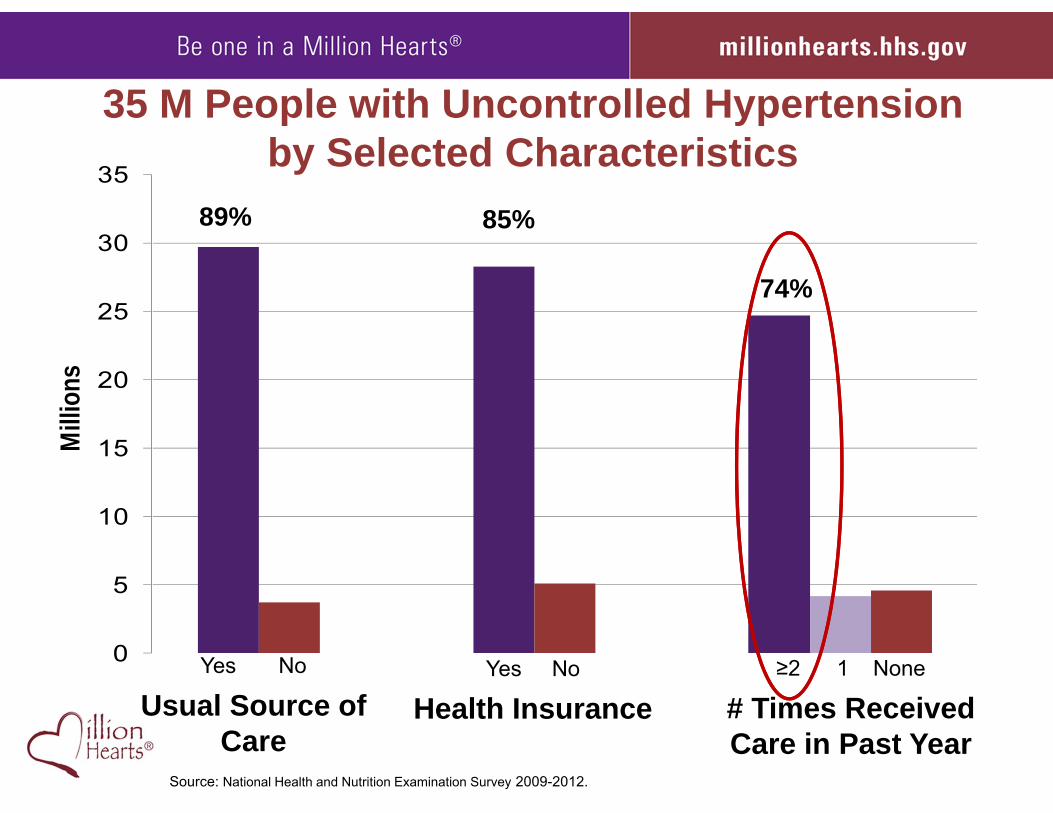
35 M People with Uncontrolled Hypertension by Selected Characteristics
6
≥2 1 None
# Times Received Care in Past Year
Yes No
Health InsuranceYes No
Usual Source of Care
Source: National Health and Nutrition Examination Survey 2009-2012.
89% 85%
74%
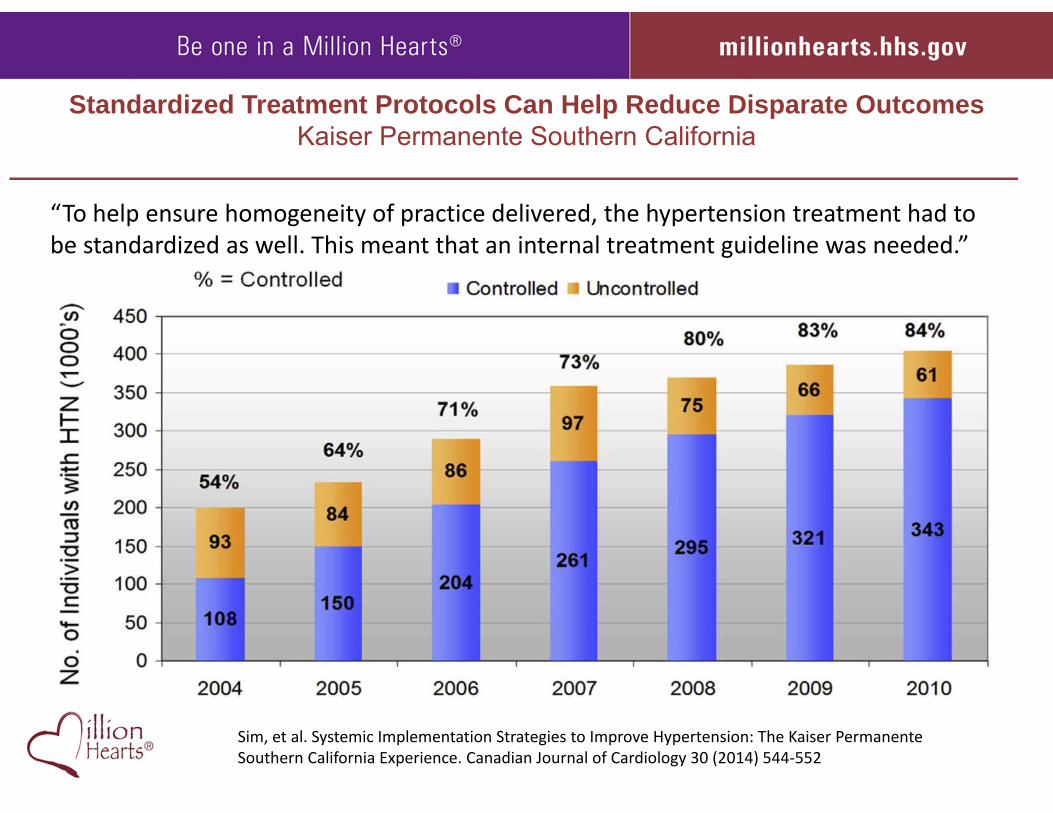
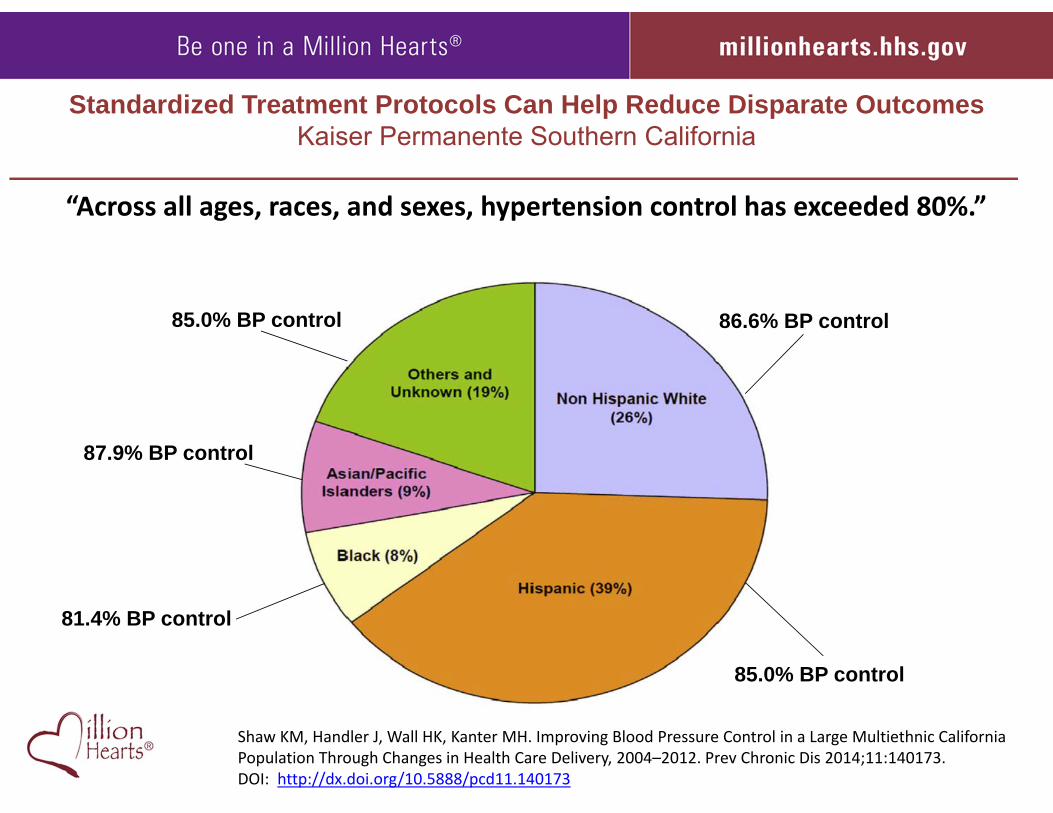
Standardized Treatment Protocols Can Help Reduce Disparate OutcomesKaiser Permanente Southern California
Sim, et al. Systemic Implementation Strategies to Improve Hypertension: The Kaiser Permanente Southern California Experience. Canadian Journal of Cardiology 30 (2014) 544‐552
“To help ensure homogeneity of practice delivered, the hypertension treatment had to be standardized as well. This meant that an internal treatment guideline was needed.”
Standardized Treatment Protocols Can Help Reduce Disparate OutcomesKaiser Permanente Southern California
Shaw KM, Handler J, Wall HK, Kanter MH. Improving Blood Pressure Control in a Large Multiethnic California Population Through Changes in Health Care Delivery, 2004–2012. Prev Chronic Dis 2014;11:140173. DOI: http://dx.doi.org/10.5888/pcd11.140173
“Across all ages, races, and sexes, hypertension control has exceeded 80%.”
85.0% BP control
87.9% BP control
81.4% BP control
86.6% BP control85.0% BP control
Why Protocol Implementation as an HHS 2015 Priority Action?
• Strong evidence base for impact• Potential to reach millions of people• Feasible to implement in 12-24 months• Ability to track impact on an existing measure• Starter set of key resources already available
Protocols as a Floor
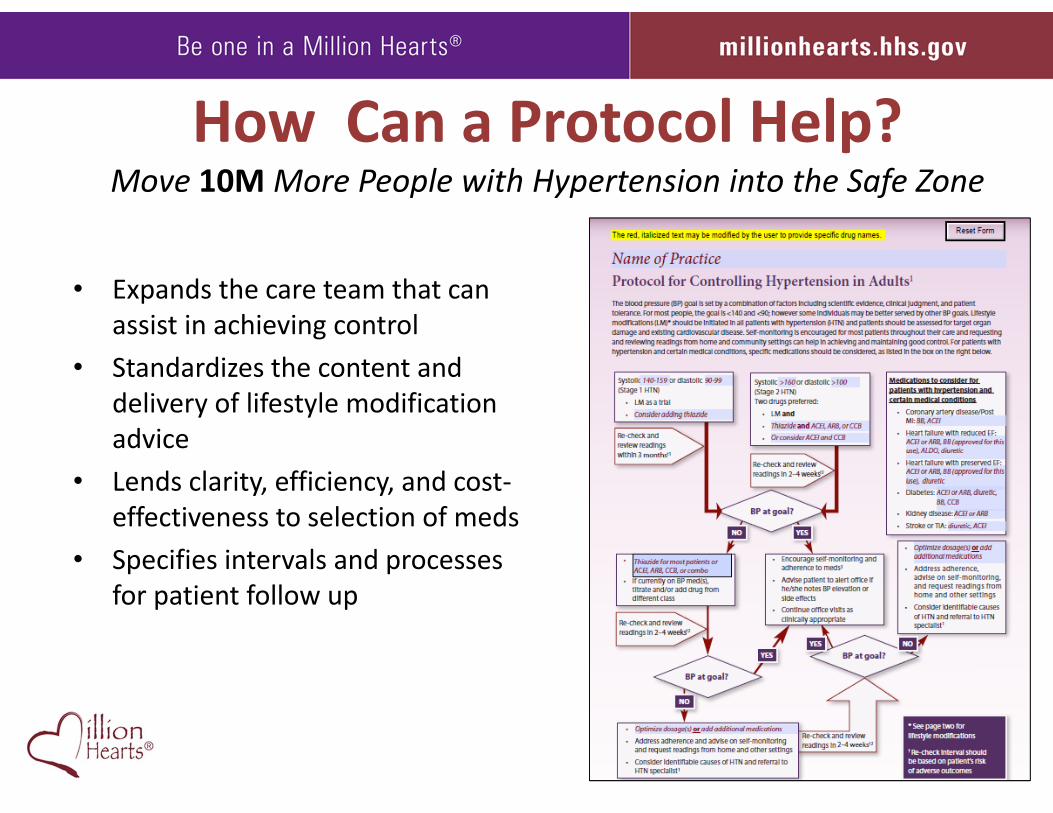
How Can a Protocol Help?Move 10MMore People with Hypertension into the Safe Zone
• Expands the care team that can assist in achieving control
• Standardizes the content and delivery of lifestyle modification advice
• Lends clarity, efficiency, and cost‐effectiveness to selection of meds
• Specifies intervals and processes for patient follow up
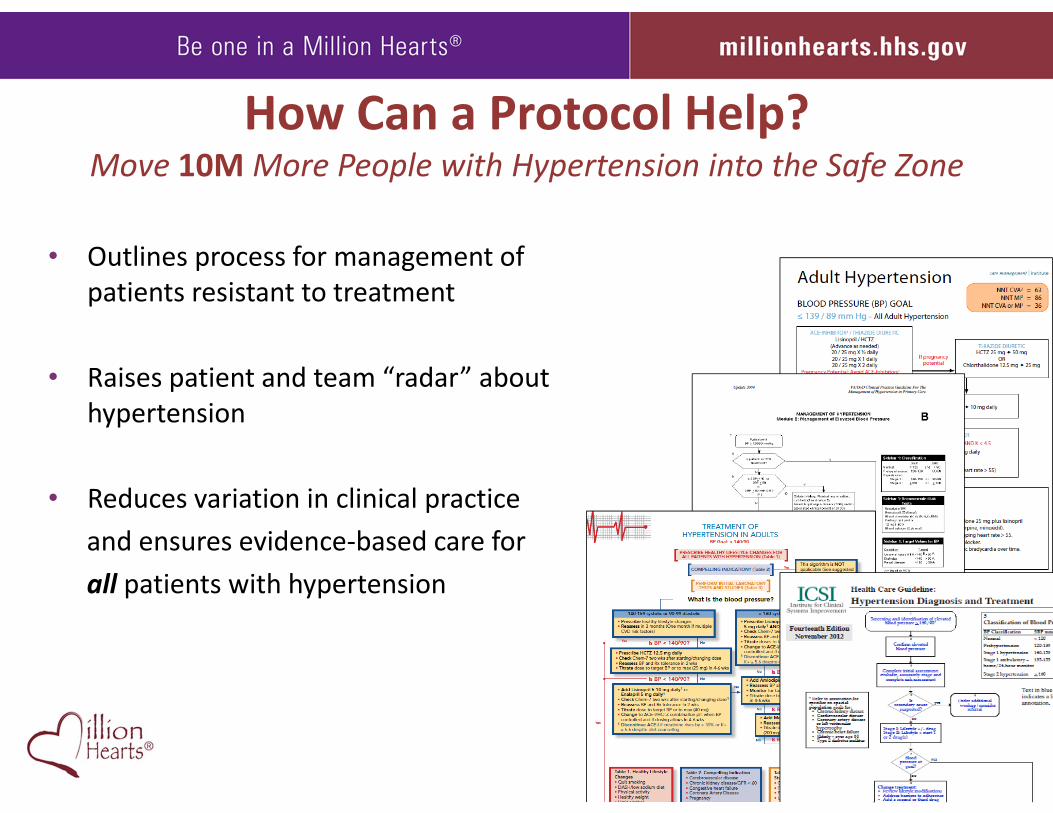
How Can a Protocol Help?Move 10M More People with Hypertension into the Safe Zone
• Outlines process for management of patients resistant to treatment
• Raises patient and team “radar” about hypertension
• Reduces variation in clinical practice and ensures evidence‐based care for all patients with hypertension
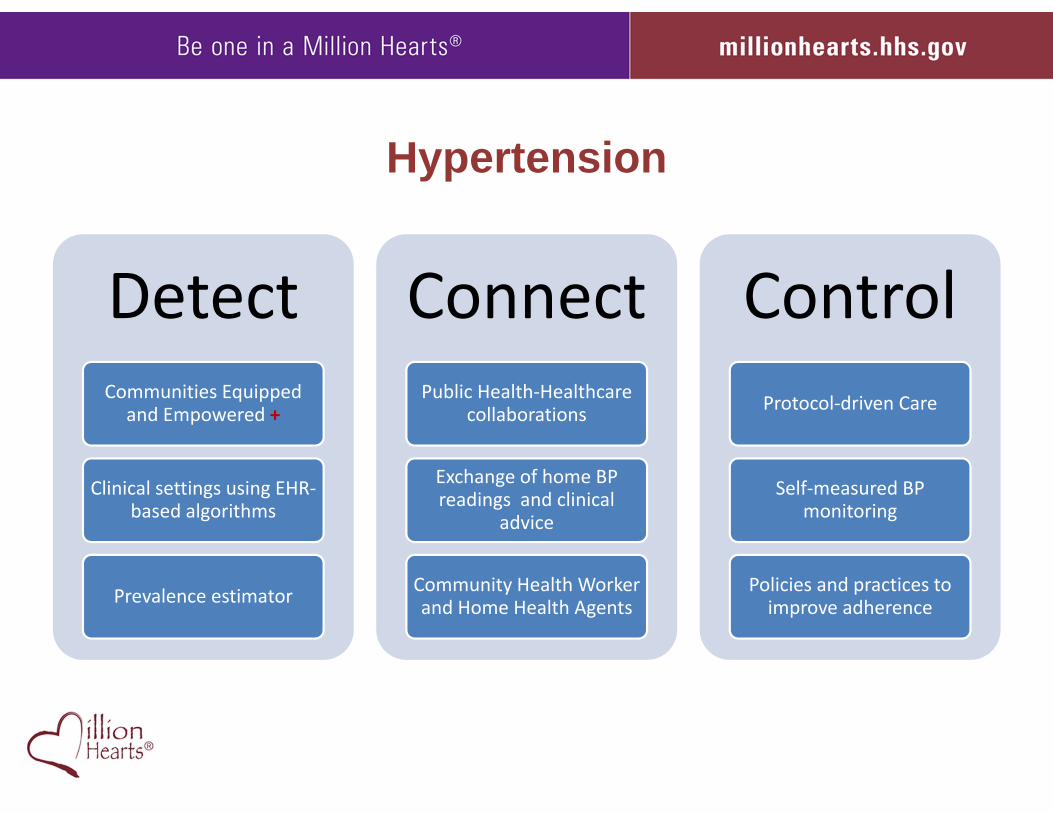
Hypertension
DetectCommunities Equipped
and Empowered +
Clinical settings using EHR‐based algorithms
Prevalence estimator
Connect Public Health‐Healthcare
collaborations
Exchange of home BP readings and clinical
advice
Community Health Worker and Home Health Agents
ControlProtocol‐driven Care
Self‐measured BP monitoring
Policies and practices to improve adherence
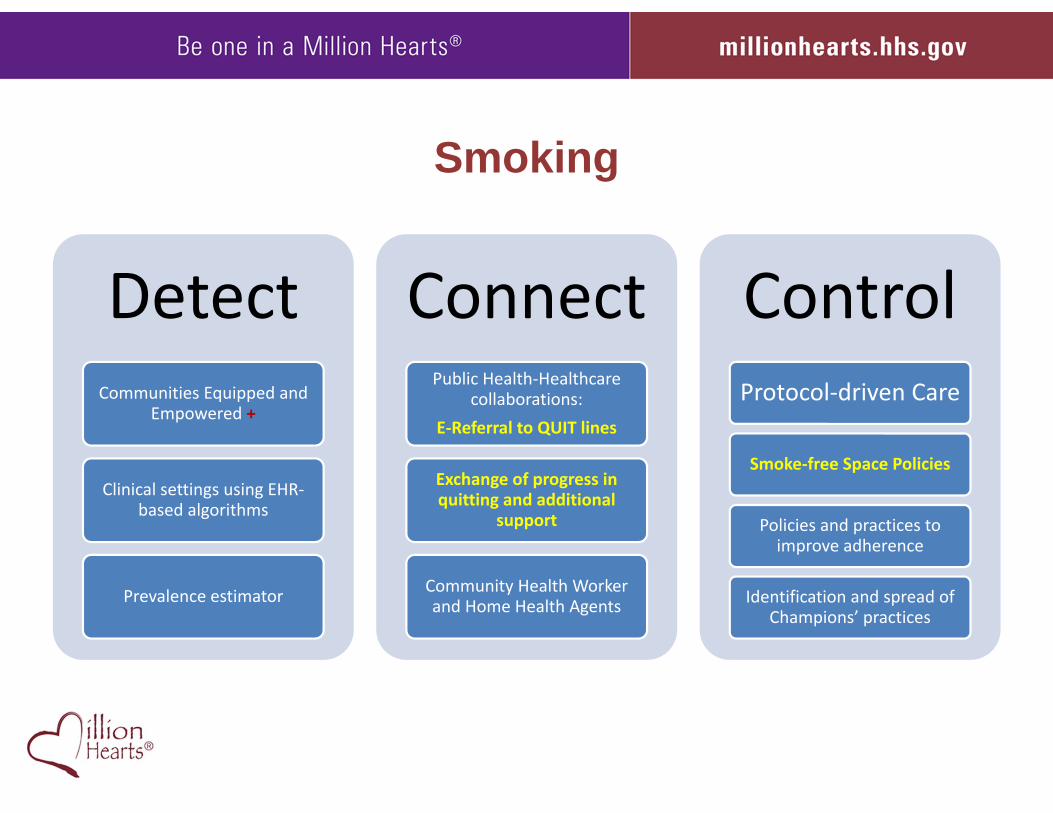
Smoking
DetectCommunities Equipped and
Empowered +
Clinical settings using EHR‐based algorithms
Prevalence estimator
Connect Public Health‐Healthcare
collaborations: E‐Referral to QUIT lines
Exchange of progress in quitting and additional
support
Community Health Worker and Home Health Agents
ControlProtocol‐driven Care
Smoke‐free Space Policies
Policies and practices to improve adherence
Identification and spread of Champions’ practices
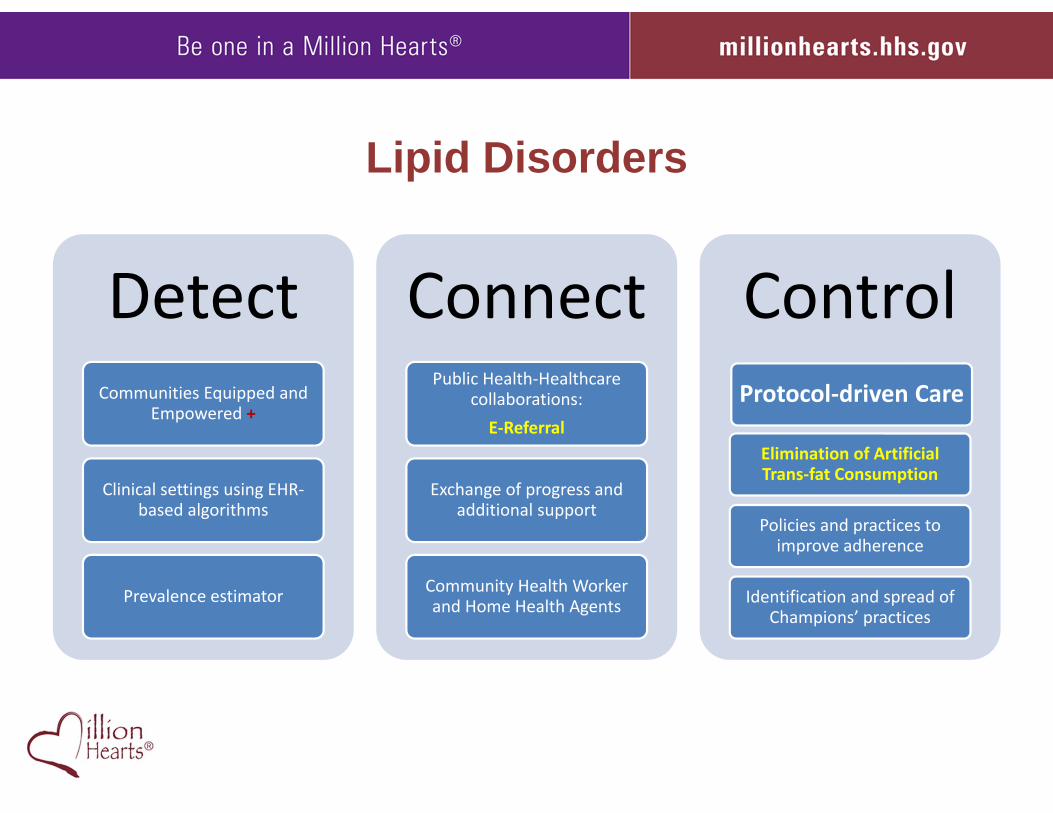
Lipid Disorders
DetectCommunities Equipped and
Empowered +
Clinical settings using EHR‐based algorithms
Prevalence estimator
Connect Public Health‐Healthcare
collaborations: E‐Referral
Exchange of progress and additional support
Community Health Worker and Home Health Agents
ControlProtocol‐driven Care
Elimination of Artificial Trans‐fat Consumption
Policies and practices to improve adherence
Identification and spread of Champions’ practices
• What is working in cholesterol management?• What is missing?• Who’s on the Design Team to fill key gaps?• Who are the Implementers?• How quickly can we act?
Hypertension CholesterolQuestions for You

Join Us
Subscribe—and Contribute to-- the E-Update
Become a Partner
millionhearts.hhs.gov
Be One in a Million Hearts®

Million Hearts® Resources• Turning Point for Impact (Mid-Course Review) • Hypertension Treatment Protocols • Hypertension Action Steps for Clinicians• Hypertension Action Steps for Employers • Hypertension Control Champions • Self-Measured Blood Pressure Monitoring Guides • Spanish language website• 100 Congregations for Million Hearts• Million Hearts Healthy Eating & Lifestyle Resource Center• Million Hearts® Grand Rounds• Million Hearts® E-update• Visit www.millionhearts.hhs.gov to find more resources
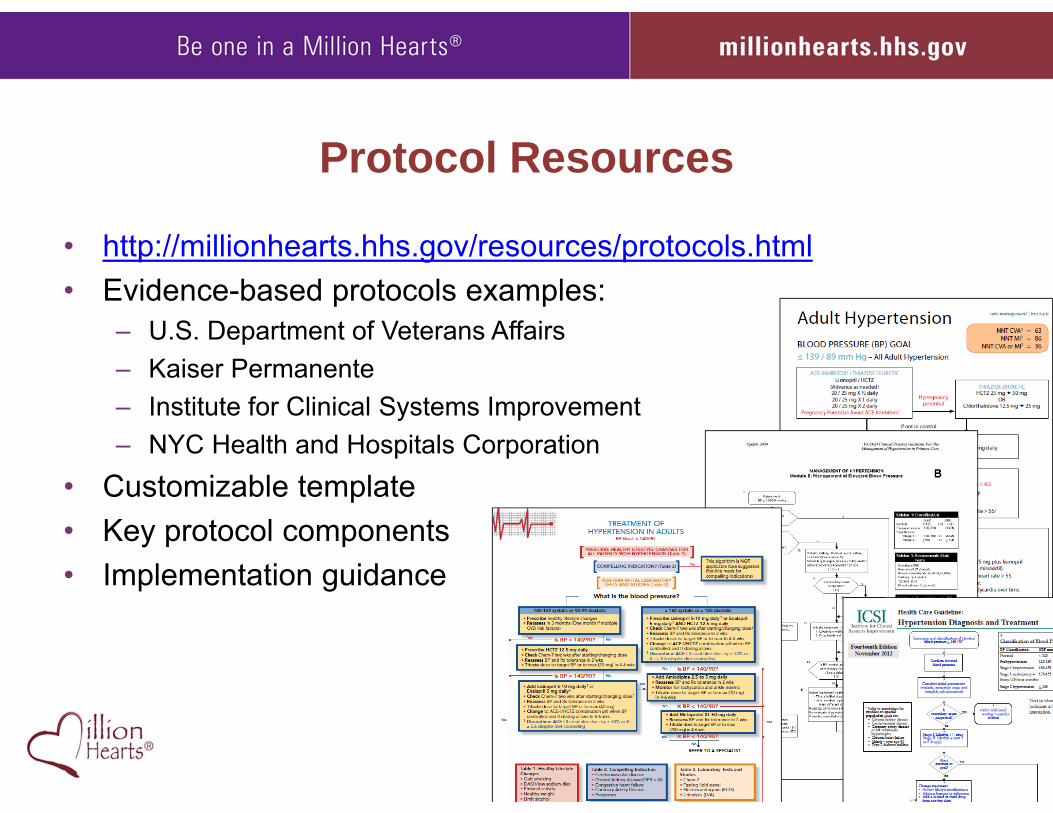
Protocol Resources
• http://millionhearts.hhs.gov/resources/protocols.html• Evidence-based protocols examples:
– U.S. Department of Veterans Affairs– Kaiser Permanente– Institute for Clinical Systems Improvement– NYC Health and Hospitals Corporation
• Customizable template • Key protocol components • Implementation guidance























![[CMMI Portugal] Cmmi implementation using open source tools](https://img.pdfslide.us/doc/110x75/554dd53fb4c905d10e8b4bb3/cmmi-portugal-cmmi-implementation-using-open-source-tools.jpg)



![Cmmi agile kulpa 2004meas cmmi[1]](https://img.pdfslide.us/doc/110x75/5455d335af795994188b4aed/cmmi-agile-kulpa-2004meas-cmmi1.jpg)
