Embed Size (px)
Citation preview


Pediatrics
OSCE & Mini-OSCE
Past Years Questions
عدإد إلفكرة إلتي تحيا على نبض قلوبكم –لجنة إلطب إلبشري : إ
يحتوي هذإ إلملف على جميع أ س ئلة
إلس نوإت إلسابقة إلموجودة في إلسي
على إلموقع حيث يجتوي دي أ و على
عامأ س ئلة إلدفع حتى
2013

Name the causing microorganism :
1
4
Hand , foot and
mouth disease .
Organism :
Coxsackie A virus and
Enterovirus
5

This procedure is used to rule out
what?
2
6

Meningitis
or
CSF 7

- What is this tube?
- What is it used for?
3
The picture in the exam
was for an infant with a
tube inserted next to the
nipple
8
1.Hickman or central venous line or dialysis line .
2. Used to : - Give antibiotic for a long period of time.
- TPN . - chemotherapy . - dialysis.
9

6 year-old baby with this scar on his abdomen… what vaccines would you like to give him:
4
The picture in the exam
was more clear that it is
a splenectomy scar
10
Post splenectomy Patient should receive :
Pneumococcal vaccine or Meningococcal vaccine .
11

This child presented with Hydrocephalus they used this device to decrease the intracranial pressure
1. What is this device?
2. Mention one indication to use it:
5
12
1. External Ventricular Line .
2. Used in infected shunt or obstruction .
13

A 7 month-old boy has weepy, crusted dermatitis around his nose, mouth and perianal area as you can see .
What is the Most likely nutrient to be deficient?
6
14
(Acrodermatitis
enteropathica) suplementation of
Zinc
15

This X-ray is for an intubated child, What is the first step in the management?
7
16

Chest tube
17
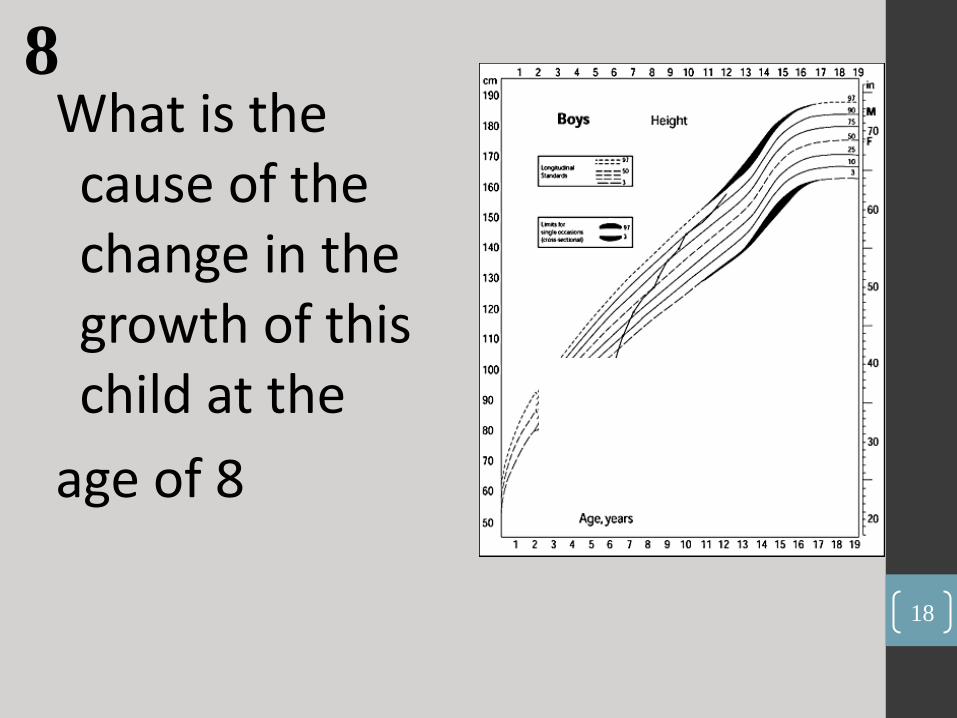
What is the cause of the change in the growth of this child at the
age of 8
8
18
Receiving Growth hormone
19

A breastfed baby present with this rash, what is it?
9
20
Oral thrush secondary to candida , mucosal
candidiasis , oral Candida / fungal infection .
21
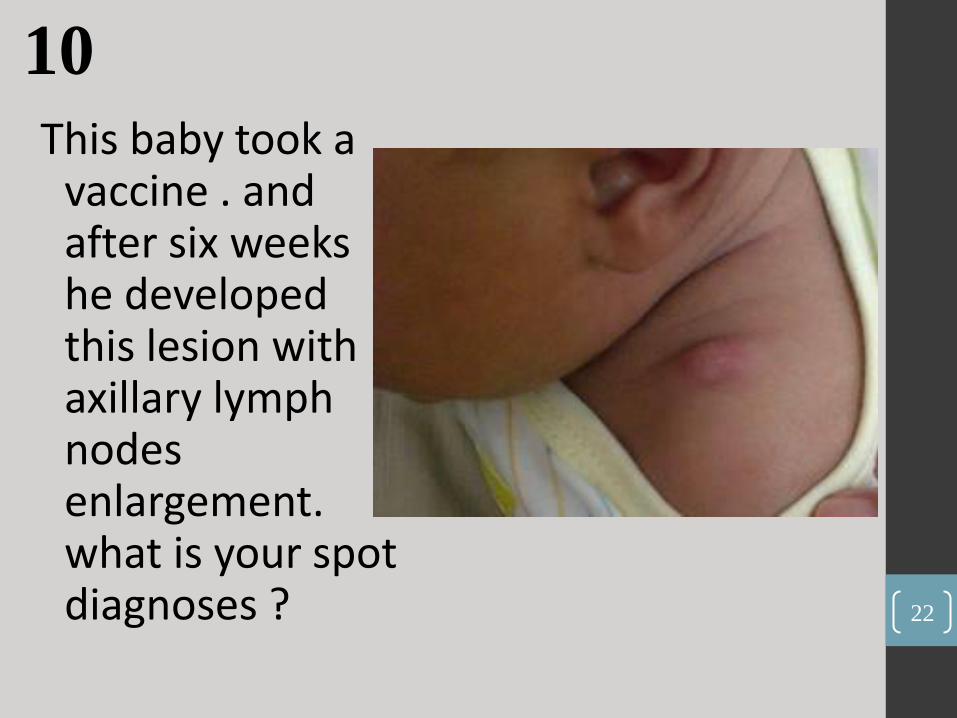
This baby took a vaccine . and after six weeks he developed this lesion with axillary lymph nodes enlargement. what is your spot diagnoses ?
10
22
Post BCG vaccin abscess formation with regional
lymphadenitis .
23
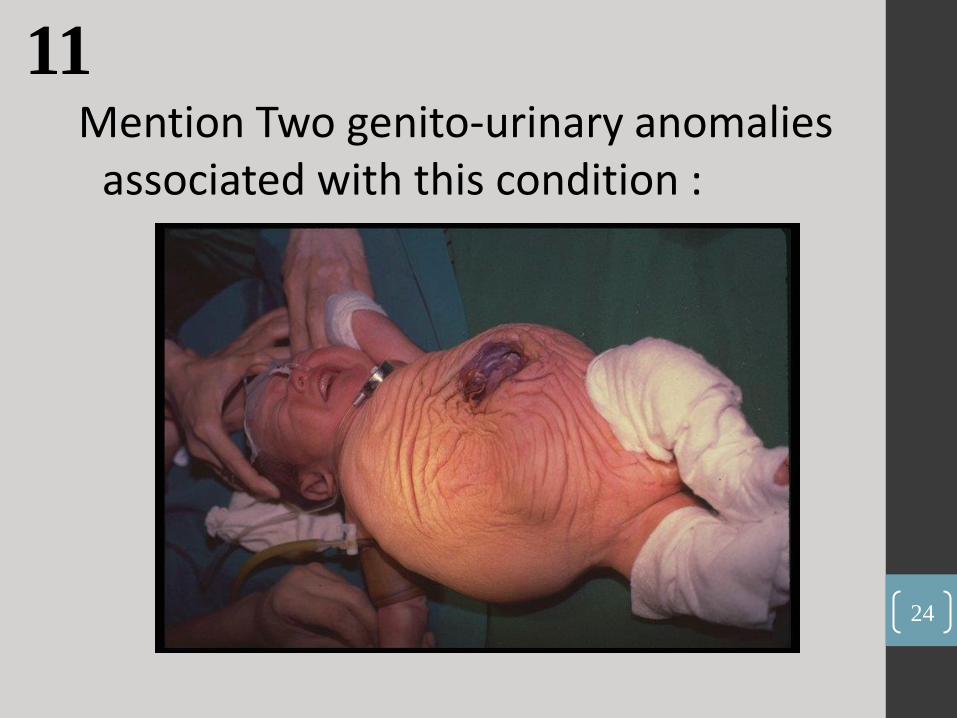
Mention Two genito-urinary anomalies associated with this condition :
11
24
High grade vesicoureteral reflux ,
neurogenic (distended , large ) bladder
Undescended testes in males
and hydronephrosis .
The condition is : Prune-belly syndrome is a rare, genetic, birth defect affecting about 1 in 40,000 births .
25
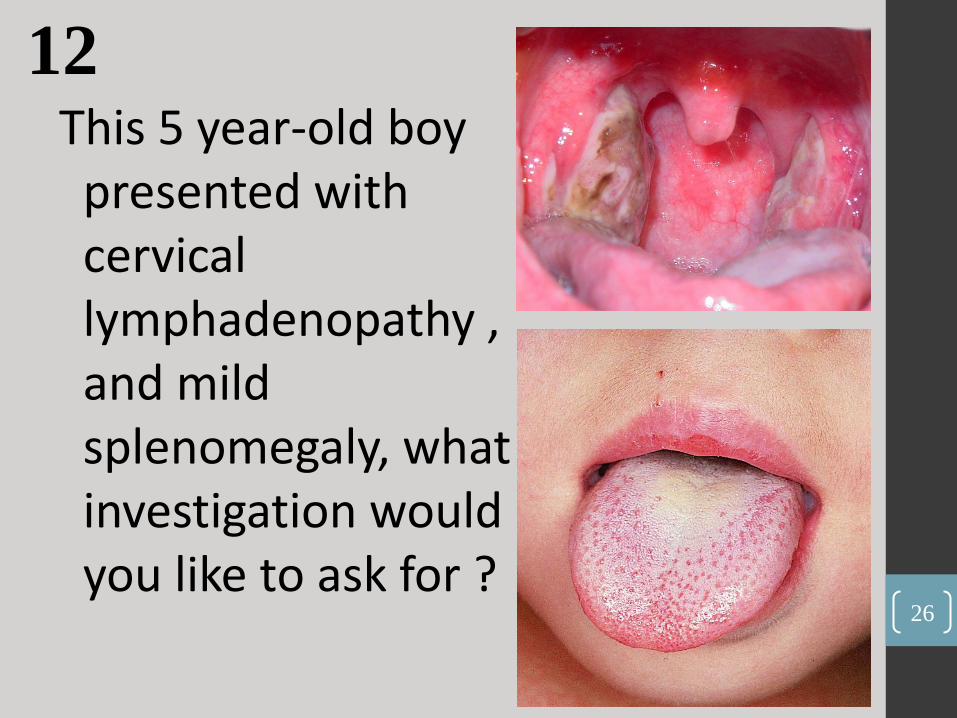
This 5 year-old boy presented with cervical lymphadenopathy , and mild splenomegaly, what investigation would you like to ask for ?
12
26
Infectious mono , diagnosed by positive Paul-Bunnell heterophile
antibody test , mono test , PCR
27

This child didn’t take any vaccine till this age . and now he presented with paroxysmal cough and coryza:
- What is your spot
diagnosis : - What is the cause of
this condition :
13
28
1. pertussis , Whooping cough .
2. Bordetella pertussis .
29
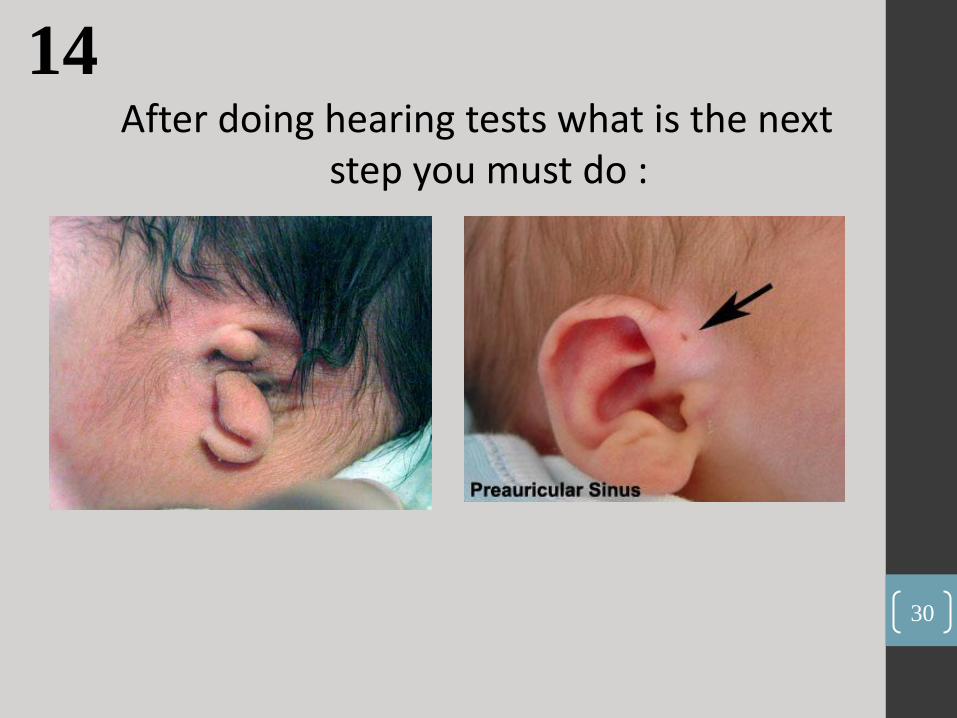
After doing hearing tests what is the next step you must do :
14
30
Renal ultrasound ,
Renal study , KFT
31

1. The age of
this child is
at least :
2-The age
of this child is
at least :
15
32
1. Three years .
2. Three – Four months .
33

OSCE : • Station 1:
• A Children patient , presented to the clinic complaining of limping for 1 day duration,
• take a history and do a focused physical exam.
• I. Hx. Note: this condition has a DDX : trauma , arthritis , malignancy (such as leukemia , although it is rare for leukemia to cause a limping but actually it was the diagnosis of this case as Doctors said . So be sure to ask about leukemia symptoms ) .
34
• II . Physical exam :
• Start with general look , then go to vital signs (doctor will tell you skip) , go to growth measurement (also skip) , then examine the both limbs (inspection ,palpation) and ask the patient to move and walk , then go to the abdomen and search for hepatomegaly and other lymph nodes, finally look to the skin and comment if there is rash .
35
•Station 2 : • A 7 year-old patient , presented with vomiting 1
day ago, take a good history and do a physical examination .
• I. History : when you Finnish you will discover that the cause is food poisoning .
• II : Physical Examination
• -start with general look, the vital signs (here the doctor will ask you which one is the most
• important in this case? It is BP or pulse for dehydration) , growth parameters (skip) Then look for signs of dehydration (here comment in all signs ).
36

• III. Questions :
• Then the doctor will tell you ,this is enough and he will start to ask questions :
• What is your diagnosis : food poisoning
• What is the most common organism that cause poisoning? Satph.aureus
• Shall I give the patient antibiotic or not ? no , only supportive treatment
• What test would you like to do to know the causative agent ? stool analysis! (the doctor told
• me so the answer was
• What is the color of staph. under gram stain ? purple/blue color .
37

• 3. Counseling : • Read this case then answer the questions :
• A 2 year old patient presented with recurrent vomiting for the last 2 months .
• He is the first child , mother age was 28 , his blood group was O+ , his mother
• was A+ , he is on formula .
• - Give Five DDX :
• 1- overfeeding 2- pyloric stenosis 3- GERD 4- systemic infection (UTI) 5- allergy to milk ( try to give as much as you can , because the doctor will not tell you “give me more” , in this question you should give 5 DDX , so if you said 3 DDX you will lose 2 marks as simple as this.
• If the cause was overfeeding , how can you support your diagnosis ?
• -See Wight changes . 38

• Ask the mother how she prepare the formula if the cause was pyloric stenosis ?
• What are the suspected electrolytes in lab investigation?
hypochloremic hypokalemic metabolic alkalosis , hypeonatremia.
• What are the signs & symptoms that may support this diagnosis?
• visible olive mass , non-bilious vomiting , visible peristalsis, projectile vomiting.
• What are the things ? in this history that suggest pyloric stenosis?
• First child , mother age 28 , blood group O , recurrent vomiting .
• The doctor gave you an ABG result and ask you to interrupt it .
39
• Station 4 :
• - A 6 years old girl come to you with swelling in her eye for 5 days PTA taking
• history and doing Physical examination to this patient .
• ■ First: the History like this:
• - You must ask these Questions, and if you lose any of them you will lose one
• mark:
• 1. Ask if bilateral or unilateral eye swelling and about red, pain, tender, warmth of
• the eye.
• 2. When the eye swelling increase like in morning?.
• 3. Urinary symptoms " frequency of urination, urine color, if there is blood in it or not “.
40
• 4. Ask about urinary disease.
• 5. Ask about if this is first attack or not.
• 6. Ask about past history of drug.
• 7. Ask about liver disease and (jaundice) .
• 8. Ask about heart disease.
• 9. Ask about malnutrition of protein "feeding ".
• 10. Ask about Shortness of Breath.
• 11. Ask about past history of upper respiratory tract infection.
• 12. Ask about diahhrea, vomiting and allergy.
• 13. Ask about if there is swelling in other place in the body.
• This case was Nephrotic syndrome.
41

• ■ Second: Physical Examination “10 marks”:
• 1. Vital sign “BP”
• 2. Examine tow eyes "bilateral” . (Swelling, redness, hotness, discharge, jaundice).
• 3. Leg edema “bilateral“.
• 4. Ascites.
• 5. Scrotal edema.
• 6. Basal crepitation .
42

• Station 5 :
• - A 8 years old female come to you in daily pediatrics clinic with unsteadiness for
• 1 week PTA , and she was have clumsiness take focused history and do related physical examination.
• ■ First: the History “has 10 marks":
• you must analysis the chief complaint like this:
• “When it is beginning?, it is increasing with time or not ? If this first time or not?”
• 2. Ask about Difficulty with fine-motor tasks, such as eating, writing or buttoning a
• shirt “Lose muscle coordination in a hand, arm or leg”
• 3. Change in speech.
• 4. Change in vision.
• 5. Change in hearing.
• 6. Involuntary back-and-forth eye movements (nystagmus) .
• 7. Difficulty swallowing.
43
• 8. Ask about car accident or falling down or about Head trauma.
• 9. Difficulty in walking.
• 10. Ask about school performance.
• 11. Ask about chickenpox “pervious skin rash, previous attack, and vaccine “.
• Because Ataxia can be a complication of chickenpox.
• 12. Ask about some Questions about developmental history, family history and
• perinatal period like hypotonia and developmental delay.
• 13. Ask about drugs.
• This case was Cerebellar ataxia.
44
• ■ Second: Physical Examination “10 marks”:
• - Growth parameter “HC”, and head overview.
• - Cereebreal examination you must see this :
• http://www.osceskills.com/e-learning/subjects/cerebellar-examination/
• - And this exam includes:
• A. Gait so ask the patient to walk.
• B. Ask the patient to walk heel-to-toe to assess balance “Heel-totoe
• tandem walking”.
• C. alternating hands “ask patient to clap by alternating the palmar and dorsal
• surfaces of the on hand” and doing this bilateral “very important”.
• D. finger-to-nose test “bilateral very important”.
• E. heel-to-shin test “bilateral very important”.
• 3. If you have time does nystagmus test.
45
Station 6 : ~ The counseling topic about “breast and milk feeding” and you must answer all these questions:
؟متى أبدأ بإرضاع ابني بعد الولادة . 1
As soon as possible.
؟هل يعتمد كمية الحليب على حجم الثدي . 2
No
؟الحليب من الثدي " شفط"كم هي المدة اللازمة لاستخراج . 3
10-15 min.
؟ما هي نسبة الماء في حليبي . 4
85-90 %.
؟ما هي فوائد الرضاعة الطبيعية بالنسبة لي . 5
• 5. Reduced risk of breast, ovarian, cervical, and endometrial cancers. Develops a special emotional relationship and bonding with her child.
46
ما هي فوائد الرضاعة الطبيعية للطفل ؟. 6
• Children receive the most complete and optimal mix of nutrients & antibodies and The varying composition of breastmilk keeps pace with the infant's individual growth and changing nutritional needs.
كيف اعرف إن كان طفلي شبع من إرضاعي له أم لا ؟. 7
7. by all of these things:
• Sleeping 2-4 hrs after feeding.
• Voiding & stooling patterns of the infant.
• -Rate of Wt gain.
47

ما اسم الحليب الذي في أول أيام الرضاعة ؟. 8
ما هي أهميته ؟. 9
كم المدة التي يستمر بها في النزول ؟. 10
ما هي مكونات هذا الحليب ؟. 11
mature milkبما يختلف عن . 12
• 8-12. breasts produce Colostrum beginning during pregnancy and continuing through the early days of breastfeeding. This special milk is yellow to orange in color and thick and sticky . It contains lower amounts of carbohydrates, lipids, and potassium and high in carbohydrates, protein, vitamin A, antibodies, and sodium chloride.
48
ماذا نسمي الحليب في بداية الرضاعة ؟ وبماذا يتميز ؟ وما لونه؟. 13•
• 13. Foremilk, the milk released at the beginning of a feed, is watery, low in fat, and
• high in carbohydrates relative to the creamier hindmilk.
• ماذا نسمي الحليب في اية الرضاعة ؟ وبماذا يتميز ؟ وما لونه ؟. 14
• 14. Hindmilk is the milk that the baby obtains at the end of a feeding, especially when the breast is much softer. is present after a mother's milk supply is established. It is very high in fat and is released after the milk ejection reflex occurs
• (during the foremilk phase).
كم المدة التي يمكن أن أضع بها حليبي في الثلاجة ؟. 15•
• 15. Up to five days.
كم المدة التي يمكن أن أضع بها حليبي في الفريزر ؟. 16•
• 16. Three to six months.
سنة فهل 17إذا وضعت هذا الحليب في الثلاجة وشرب منه أخاه الذي عمره . 17•
.سيتضرر
• 17. No .
49

• Station 7 :
• asthma
• 10 year-old boy comes to the emergency diagnosed as asthma . evaluate the patient by history and examination , and decide if he need admission or not .
• Station 8 :
• 13 Patient come to you complaining of altered consciousness , take history and do related examination , what do u thing the diagnosis ?
50

• Station 9 : • Counseling “ Kerosene ingestion “ :
• four – year old boy comes to you with kerosene ingestion . Answer these Qs .
• 1. is the patient need gastric lavage ?
• 2. do you advice the patient to drink milk ?
• 3. if you know that the patient come 2 time before this complaining on ingestion , what this do mean to you ?
• 4. What do you think the complication will be ?
51

ا القلب الندي بالإيمان المتصل بالرحمن، أم
فلا ييأس ويقنط مهما أحاطت به الشدائد،
ت به الخطوب، ومهما غام ومهما ادلهم
الجو وتلبد، وغاب وجه الأمل في ظلام
الحاضر وثقل هذا الواقع الظاهر فإن
رحمة الله قريب من قلوب المؤمنين
المهتدين، وقدرته تنشئ الأسباب كما
تنشئ النتائج وتغير الواقع كما تغير
. الموعود52

1. What’s your diagnosis?
53

Orbital Cellulitis
54

2. 1. Describe the abnormality in the picture. 2. Name the condition associated with this
abnormality.
55

Answers :
1. Absent thumb
2. Fanconi's anemia
56
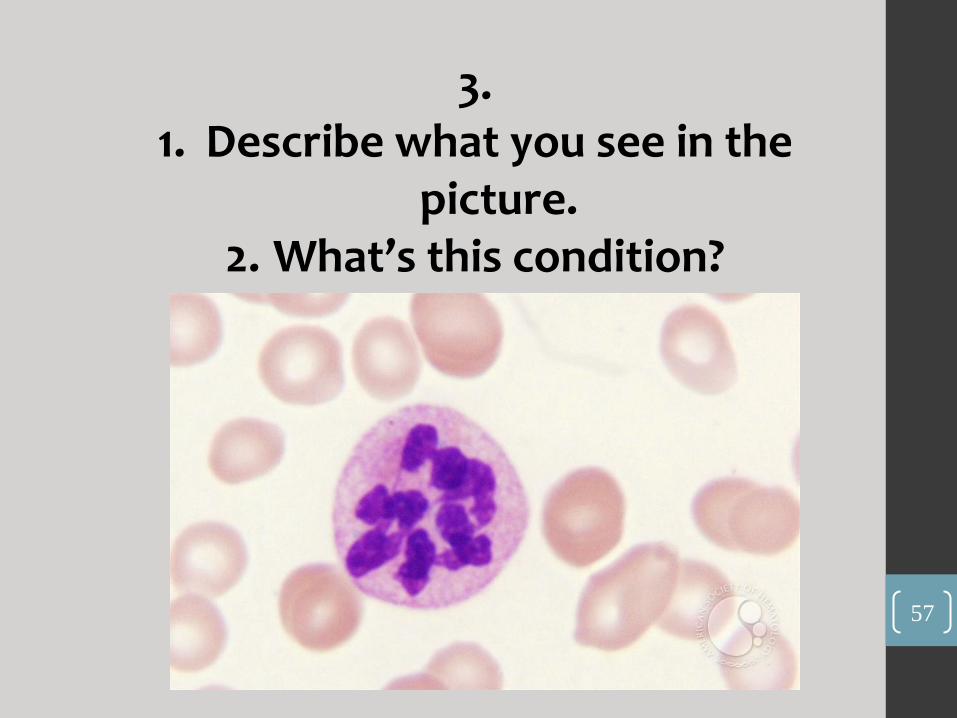
3. 1. Describe what you see in the
picture. 2. What’s this condition?
57

Answer :
1. Hyper-segmented neutrophil
2. Macrocytic anemia due to Vit B12 deficiency
58

4. Name a condition associated with
this sign.
59
Answer:
Retinoblastoma
(the sign is “absent red reflex”)
60

5. 1. What is the abnormality in the picture?
2. Name the condition associated with this.
61
Answer:
1. Brushfield spots
2. Down Syndrome
62

6. 1. Name the disease.
2. Mention 2 specific features for this disease.
Imagine it’s a picture of a baby!
63
Answer:
1. Shingles
2. Dermatomal distribution, cluster of vesicles on an erythematous base
64
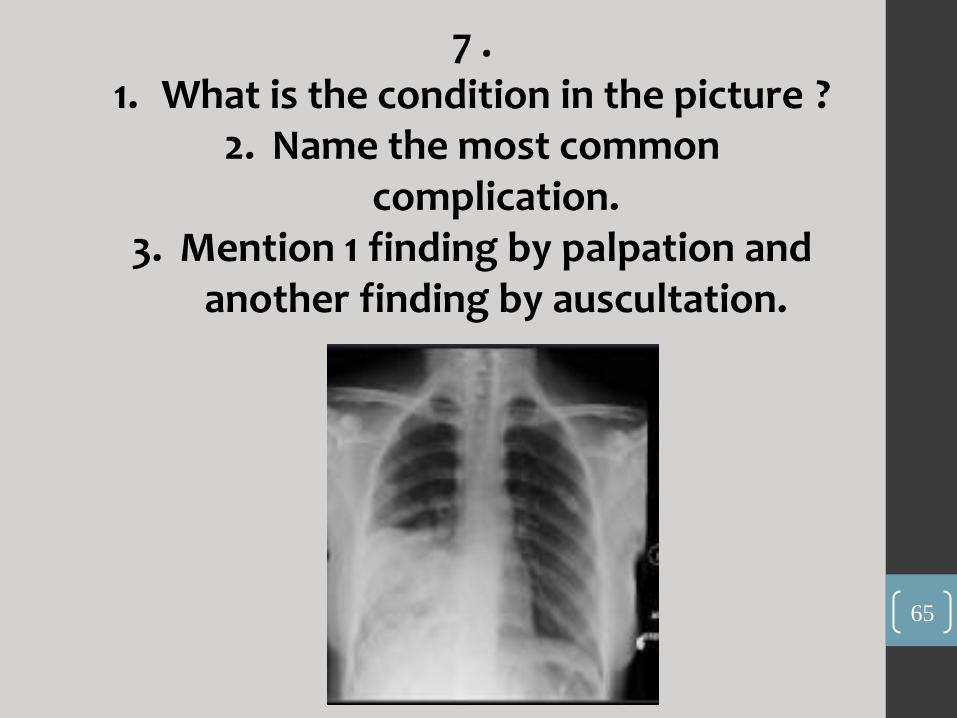
7 . 1. What is the condition in the picture ?
2. Name the most common complication.
3. Mention 1 finding by palpation and another finding by auscultation.
65

Answer:
1. Right lower lobe pneumonia
2. Pleural effusion
3. By palpation: decreased chest expansion on the right side
By auscultation: decreased air entry on the right side
66
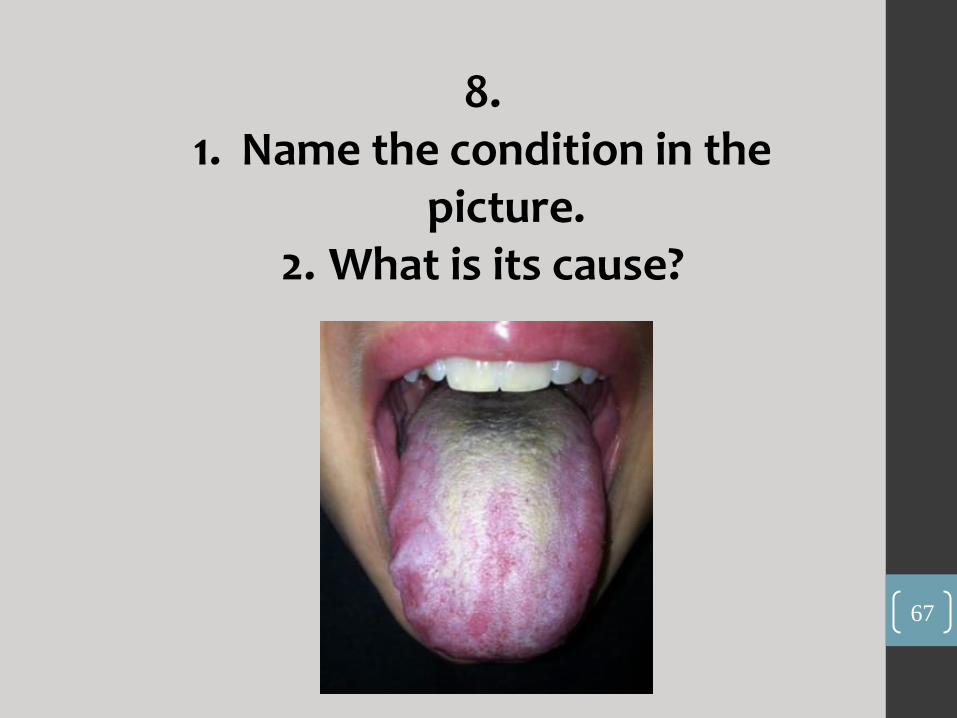
8. 1. Name the condition in the
picture. 2. What is its cause?
67
Answer:
1. Oral thrush
2. Fungal infection (Candida)
68

9. 1. What’s your diagnosis? 2. What is the treatment?
69

Answer:
1. Pneumopericardium
2. Pericardiocentesis
70

OSCE : First Station -A father of a 15-month old baby complaining that his baby isn’t growing well. Take a focused history. Diagnosis: Failure to thrive – IUGR . Second Station -Physical examination related to the previous case. You need to assess the growth parameters of the child.
71
Third Station -A mother brought her child complaining of difficulty in his breathing. Take a focused history. Diagnosis: Foreign body aspiration! Forth Station -Physical examination related to the previous case. Respiratory system examination.
72

Fifth Station Counseling for Hepatitis A. -How do we test for it? -How does it spread? -Is there a vaccine for it? When is it given? -When should the mother send her child back to school? -When do we need to admit the child to hospital?
73
74
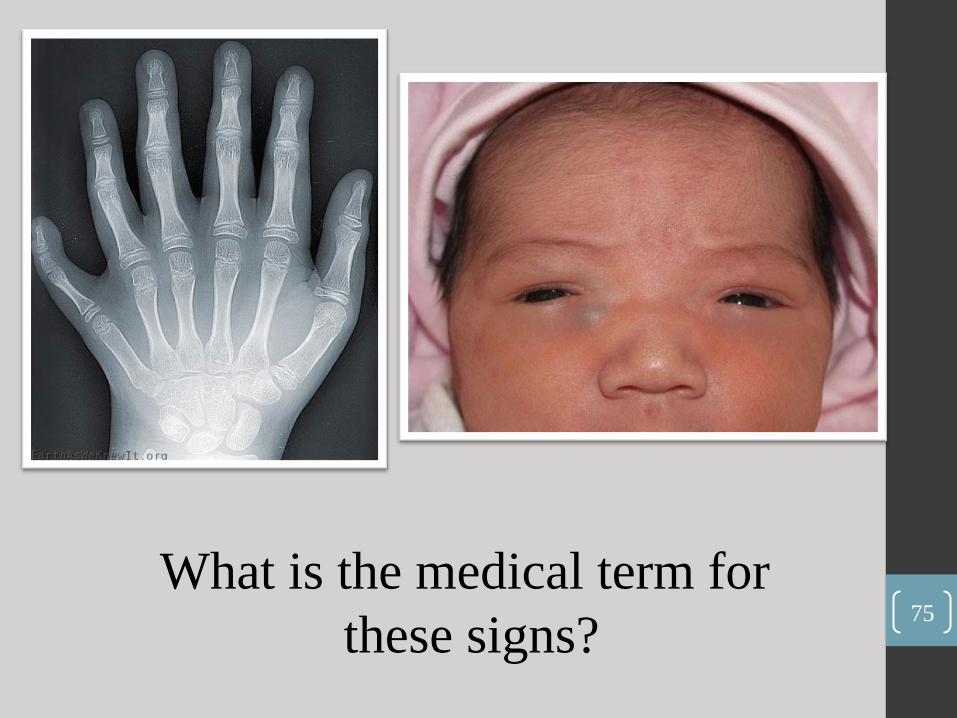
What is the medical term for
these signs? 75

1- a- Polydactyly b- hypertelorism & flat
nasal bridge
76

-what we call this vaccine and
- what the age of this child ? 77
78
2- OPV AT 91 DAY (& more)

- what is the treatment for this disease ? 79
80
3- topical corticosteroids ( Not sure)
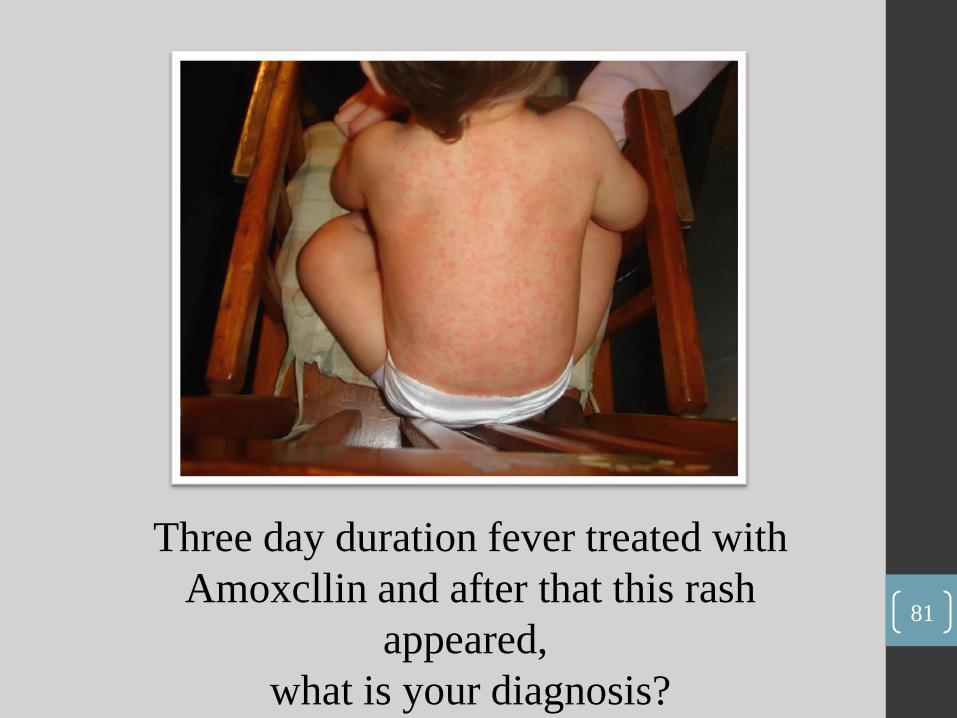
Three day duration fever treated with
Amoxcllin and after that this rash
appeared,
what is your diagnosis?
81

82
roseola infantum

Mention three other symptoms
for this disease? 83

84
abdominal pain
arthralgia
renal manifestation
(hematuria)
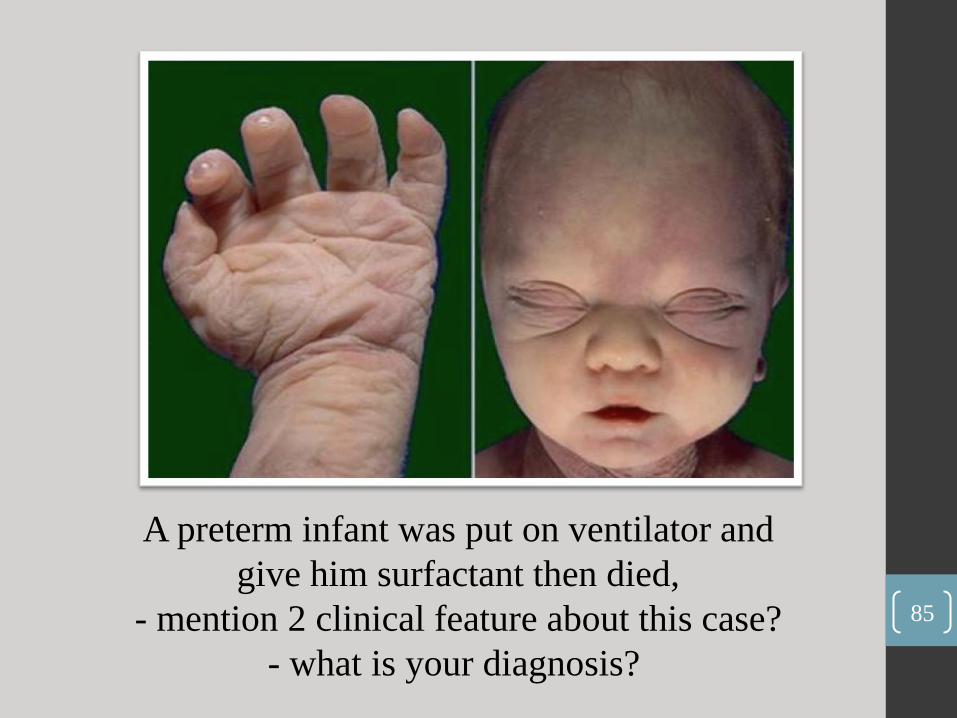
A preterm infant was put on ventilator and
give him surfactant then died,
- mention 2 clinical feature about this case?
- what is your diagnosis?
85
86
1. Bilateral renal agenesis (BRA)
clubbed feet ,
pulmonary hypoplasia ,
Skin fold ,
and cranial anomalies
related to the oligohydramnios.
2. Potter's syndrome,

A seven year old patient came with this on his back ,
what we will ask as taking history (mention 2 Q) ?
And what investigation you will ask for him ? 87

88
a) if he has a lower limb
weakness ad if he has a
urine incontinence
b) MRI

- What is the next step in investigation ? 89
90
HB
electrophoresis

- what we call this on the face
of old girl ?
- what is your diagnosis? 91
92
a) Malar rash
b) SLE
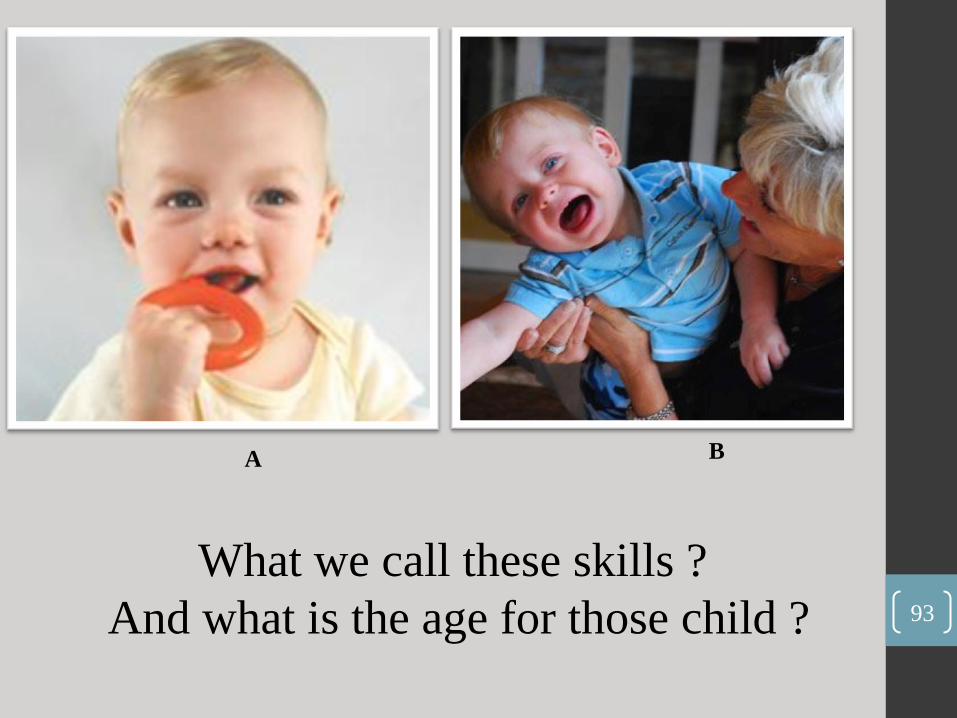
A B
What we call these skills ?
And what is the age for those child ? 93
94
A. mouthing at 4-5 month .
B. Separation anxiety at 9
month .
OSCE :
1st Station :
a 7 year old patient came with vomiting,
take history and physical exam ?
2nd Station :
a 12 year old patient came with musical sound ,
take history and physical exam ?
95

، ، وأحبه بحق وصدق عرف اللهمن
، ، فأصبح سيدها لا عبدها هانت عليه الدنيا
واستطاع أن يستقيم فيها مع الحق والواجب
، وأن يشمخ برأسه دائما وسائر المثل العليا
في مواجهة الطاغوت، وأن يرتقي فيها أعلى
رى، وينجز أجل الأعمال . الذ
عصام العطار .أ

name both reflexes and at what age the
1st pic appear
&
the 2nd pic dissappear ..
97

1. Mature Pincer grasp at 12 month
2. Stepping at 4-6 weeks
98
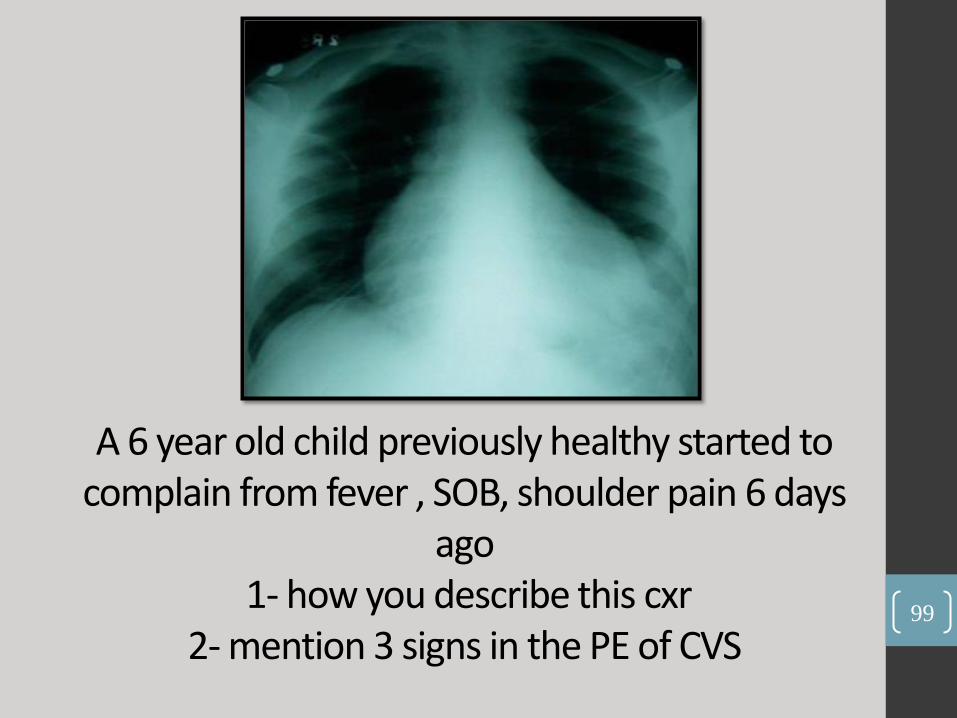
A 6 year old child previously healthy started to complain from fever , SOB, shoulder pain 6 days
ago 1- how you describe this cxr
2- mention 3 signs in the PE of CVS
99

1) pericardial effusion 2) muffled heart sounds, friction rub,
hypotension, distended neck veins
( not sure about the last 2 points )
100
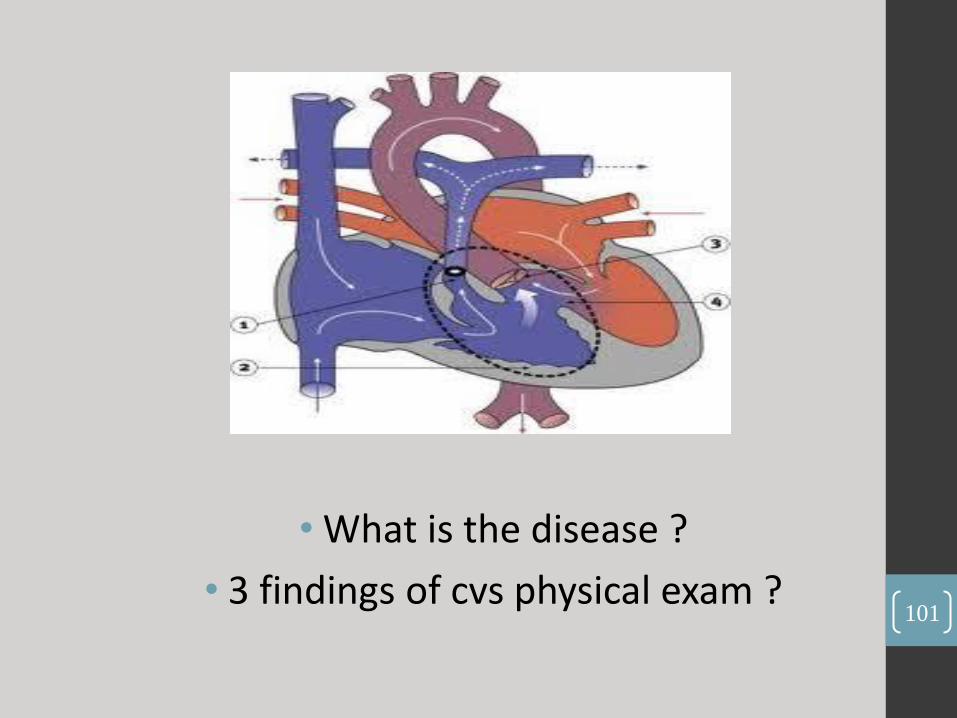
• What is the disease ?
• 3 findings of cvs physical exam ? 101
1.TOF
2.Ejection systolic murmur, thrills, single S2, cyanosis .
102

Multiple X-RAYs about ricketts in a 17 minth old child come with difficulty in walking .
• How u describe it ?
• 2 abnormalities in the lower limbs ?
103
1. Cupping in the distal end of long bone, thin cortex .
2. Bowing , valgus & varus deformity, club foot
104
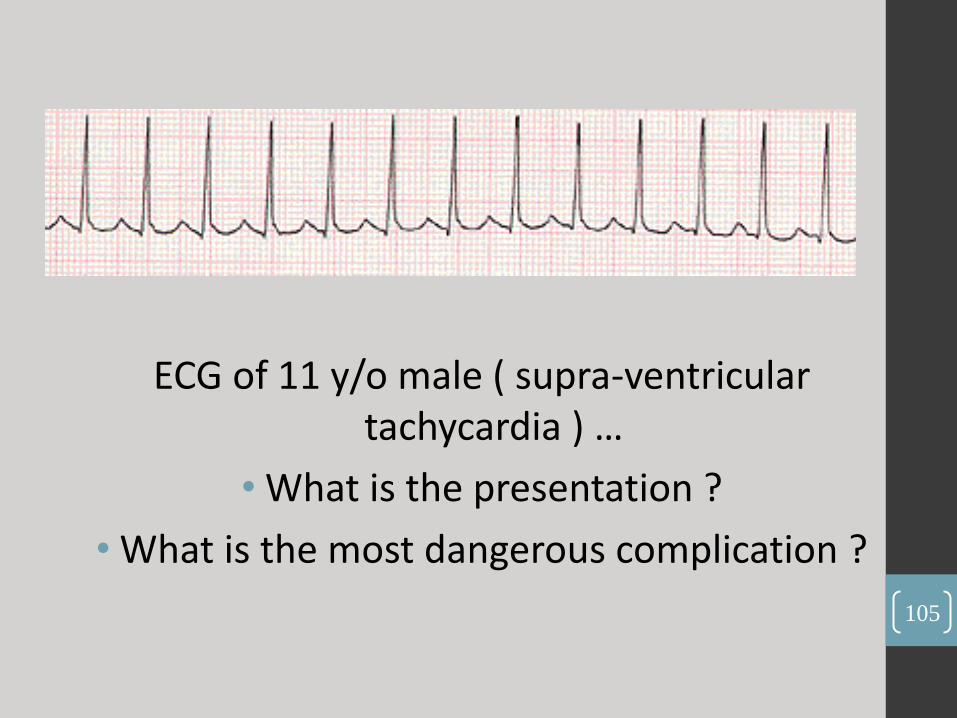
ECG of 11 y/o male ( supra-ventricular tachycardia ) …
• What is the presentation ?
• What is the most dangerous complication ?
105
1. Palpitation, loss of consciousness .
2. Heart block (not sure) .
106
PH=7.5 pco2=30 HCO3=22 BE=10
1. Read this ABG ? 2. Mention 2 causes ?
107

1. Noncompensated respiratory alkalosis .
2. Hyperventilation, panic attack, acute anemia, salecylate
overdose .
108

•What is the type of inheritance ?
•Mention one example ? 109
1. X-linked dominant
2. Fragile x syndrome, alport disease , rett
syndrome .
110

• Pic .of a tall male with long hands
( not the same pic the one in the exam was so clear) and his brother have the same findings
with pan systolic murmur .
• What is the syndrome ?
• Mention 2 other organs you want to examine ? 111

•Marfan syndrome
•Eye, mouth, joints
112
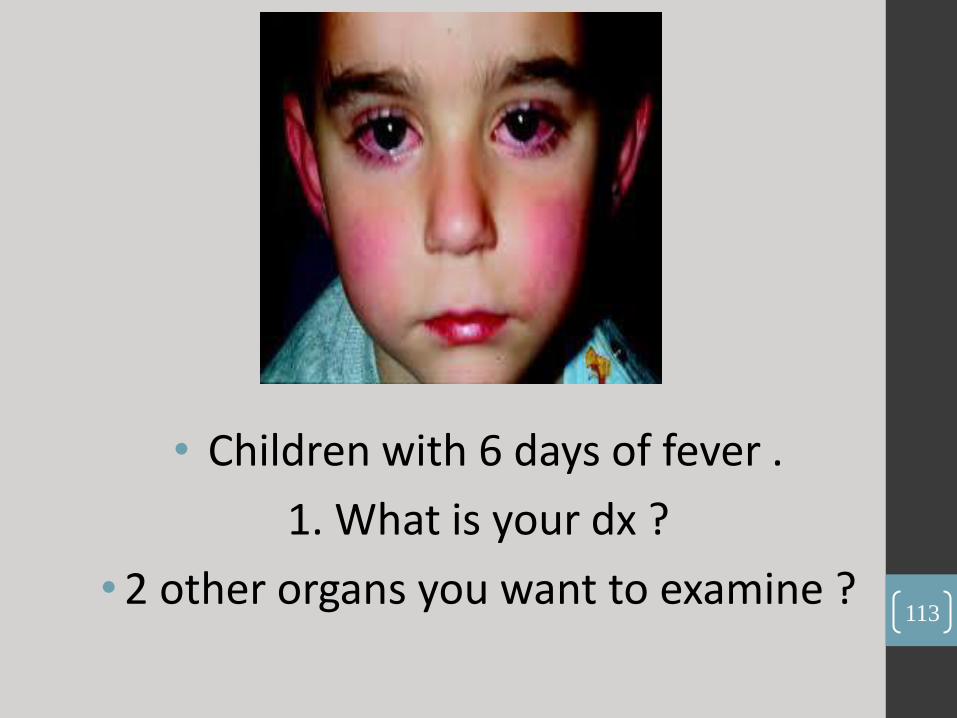
• Children with 6 days of fever .
1. What is your dx ?
• 2 other organs you want to examine ? 113
1. Kawazaki .
2. Hands & feet (peeling) trunk (rash) tongue
strawberry) .
114
• What is abnormal in this Neonate list :
• Hb=12 (low) , HC=35 , glucose= 3 (low) Subconjuctival hemorrhage (ab.)
cephalohematoma (ab.)
2 veins 1 artery ,
epestein pearls (ab.) .
115
OSCE
1st Station : CC :abnormal gate ( Hx . PE . Discussion )
• Bte6la3 post chickenpox cerebellitis :P
Ex: cerebellar signs : dysarthria, nystygmus, tremor, alternative, foot to toe, romberg’s, wide ataxic gate, dysmetria (finger-nose), .. etc
Discussion:
1) diagnosis: post- chickenpox cerebellitis..
2) Complication of chickenpox: encephalitis, necrotizing fasciaitis, pneumonitis, etc
3) days prior to rash till all lesion crusted 2لمتى بضل معدي
4) In hospital: isolation ( negative pressure room, small droplet isolation
5) His brother has leukemia & get infected , what to do in hospital: isolaion , IV acyclover till all lesion crusted
6) Mother has another 2 child & want to vaccinate ( 6m , 18 m) what u tell her & how many doses? 2 doses only for 18 month
7) Type of vaccine? Lie attenuated
116
2nd Station : RED URINE ( Hx . PE . Discussion )
• DD: post streptococcal GS
• Ex: jaundice, pallor, periorbital edema, leg edema against tibial shaft, crypitation ( heart failure bcoz of hypertension) blood pressure ( كان في جهاز ضغط ومطلوب تقيسو
• Discussion:
• Ddx: stones ( against it no colicky pain, with it +ve family hx) , UTI ( againist it no fever or lower UTI symptoms)
• Investigation: urine analysis check for RBC & RBC cast, proteinurea.. KFT, CBC, complement level ( low C3 , normal C4)
• Manegment: admision , observe vital signs (hypertension & heart failure), low salt diet .. IV maintainence & deficit (if he need & no oral intake)
117
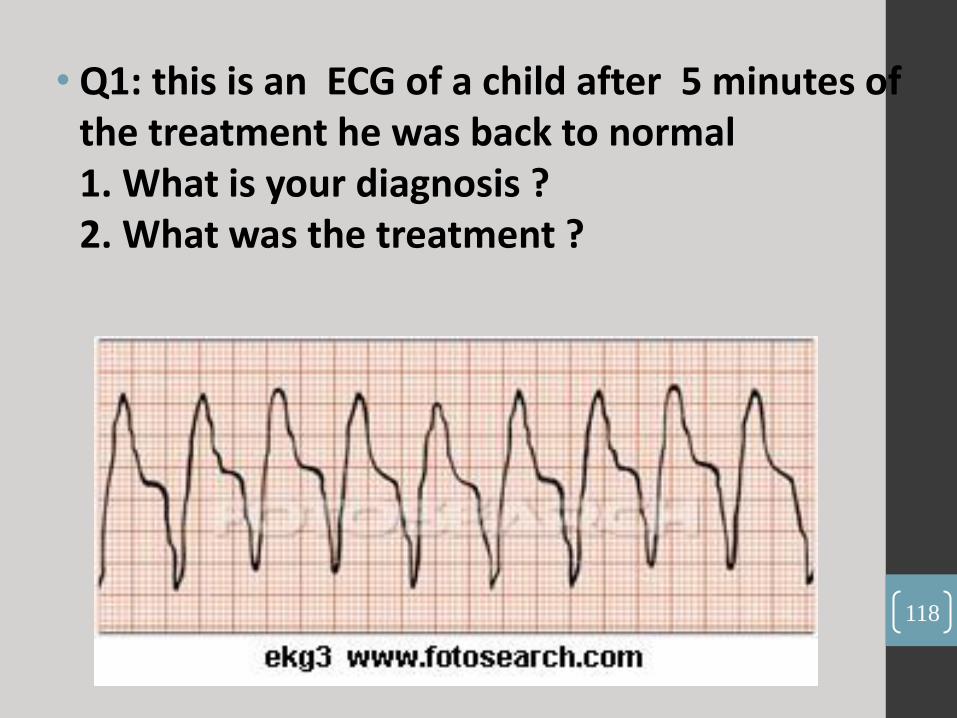
• Q1: this is an ECG of a child after 5 minutes of the treatment he was back to normal 1. What is your diagnosis ? 2. What was the treatment ?
118

1. Ventricular Tachycardia
2. Synchronized Electrical Cardioversion
119

2. Give 2 microorganism causes this condition?
120
This is erythema nodosum - group A strep
-mycoplasma tuberculosis - chlamydia
121

1. Give 2 signs seen in the X-ray?
2. What is your next step in anagement?
122
- Tension Pneumothorax - Needle Thoracostomy., Chest
Tube
123
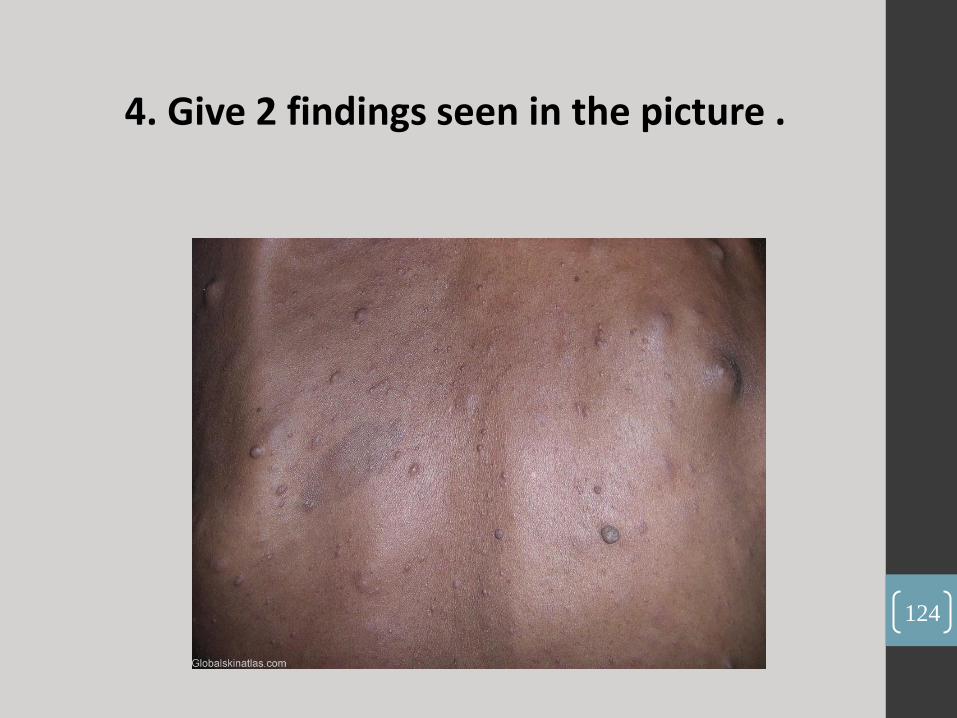
4. Give 2 findings seen in the picture .
124

Picture Of Neurofibromatosis .
A. Café Au Lait Spot
B. Neurocatunios Nodules
125

1. What is your diagnosis? 2. What is your treatment?
126

- X-ray of pneumopericardium .
- Pericardiocentesis .
127

• Q6: picture of 12 y/o female with heart rate 130/min .
- give 2 findings
128

neck mass & ptosis or exophthalmos
129
Q7: patient with Biliary atresia and liver failure there was a Na, K, Mg, Ca, PO4 and ALP values, everything was normal except the ALP was high 1. What is your diagnosis ?
130
• Q8: CSF analysis for a 1 week old male neonate ( and it was normal 1. What is your interpretation to this CSF ?
• Remember .. In neonates (less than 7 days ) WBC up to 30, RBC up to 50
131
• Q9: urine analysis for 8 y/o male with vomiting and diarrhea, it was normal except the specific gravity was high 1. What is your interpretation to this urine analysis? 2- Give two possible reason for this abnormality in this patient ? Its concentrated urine due to dehydration, there is increase in the specific gravity, otherwise it’s normal .
132

1. What is your diagnose ?
2. Give 2 findings .
133
Shingles
134
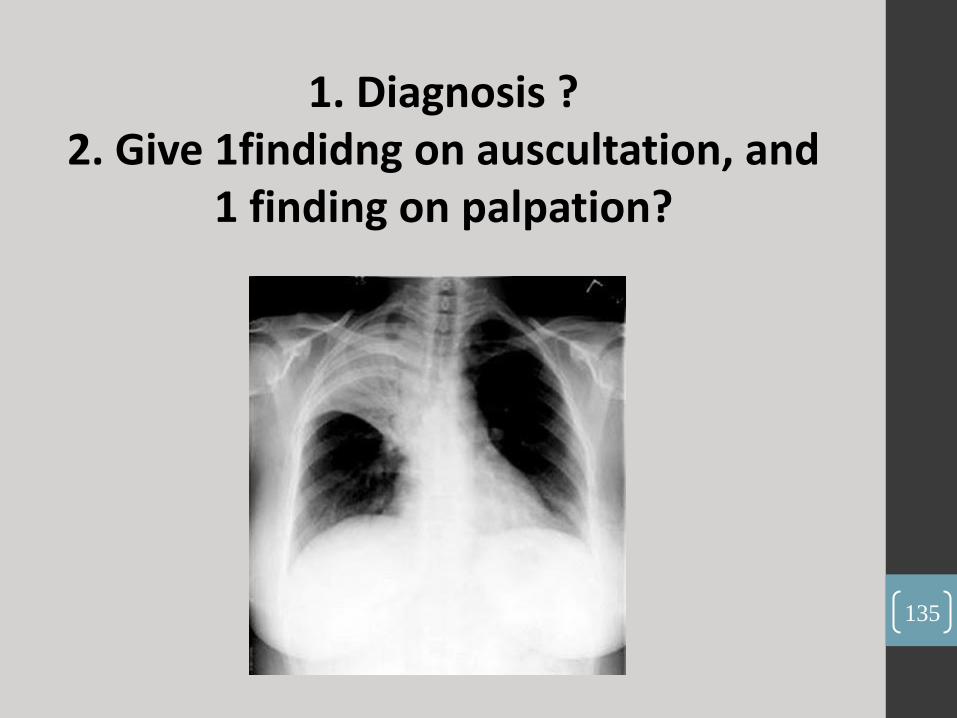
1. Diagnosis ? 2. Give 1findidng on auscultation, and
1 finding on palpation?
135
Right upper lobe pneumonia
136

• Q12: a baby of female with hyperthyroidism , he had tachycardia,
heat intolerance and decrease in weight with good appetite.
1. What do you expect the TSH and T4 values ?
137

Increase T3,T4 and decrease TSH .
138
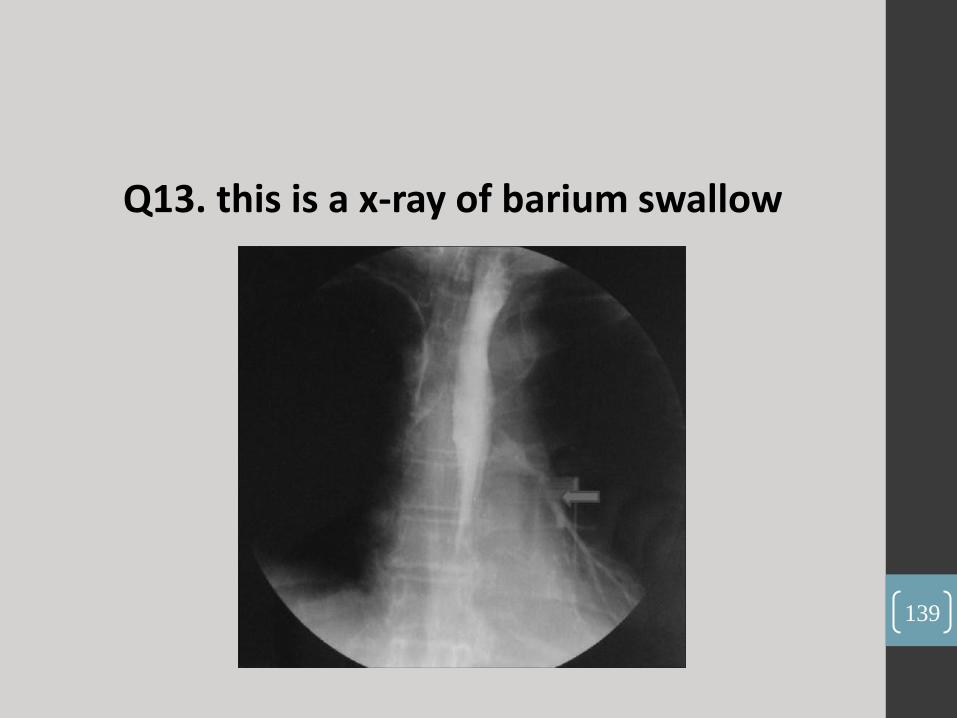
Q13. this is a x-ray of barium swallow
139

Trachio-esophageal Fistula
140

OSCE : • Case 1 :
• a 7 y/o male presented with pallor for several months
• Station 1:
• Take a relevant Hx : (bruises history, many infections and admissions and fevers, family history >> a brother with the same symptoms he died at the age of 8, good nutrition, no jaundice, no change in urine colour) .
• Station 2 :
• Do physical examination according to your Hx : -examination for a patient with pallor - plus focus examination for fanconi anemia , thumb and radius absence or hypoplasia , hyper-pigmentation, and short stature (growth parameters ) .
141
Station 3 (Discussion) :
• The case was :
• (bone marrow failure – Fanconi anemia ) . 1.give me a short assessment 2.DDx .. fanconi leukemia 3. Investigations 4. Management
142
Case 2 :
• A 1 y/o male presented with fever (40), and vomiting, hypoactivity, with intact tympanic membrane and clear ear examination .
- Station 1:
• Take a relevant Hx .
- Station 2 :
• Do physical examination to the previous case, but assume that the age of the pt is (10-13 year old) >>"depends on the doctor "
• -meningeal signs and cranial nerves examination especially the abducens and trigeminal nerves -renal angle tenderness .
143

Station 3 (Discussion):
• About DDx .. UTI (pyelonephritis ) & meningitis case . 1.DDx 2. Most important lab test: lumbar puncture 3. For where you send the CSF? For gram stain, chemistry, WBCs & RBCs count, and culture 4. Then the Dr gave you values suggest bacterial meningitis? 5. The most microorganism in this case? 6. Then he asked about treatment 7. Then he asked about prophylaxis: in which cases we should consider it, what we give for prophylaxis, to who we give prophylaxis?
144

• What is your diagnosis ?
• What is the major abnormality in this ECG ?
145
1. Cong. complete heart block.
2. Bradychardia
146

•What are these reflexes and what age they disappear? 147
•Pic A = baby doing asymmetrical tonic neck reflex = 3 -4 months .
• Pic B = palmar grasp = 3 months
148
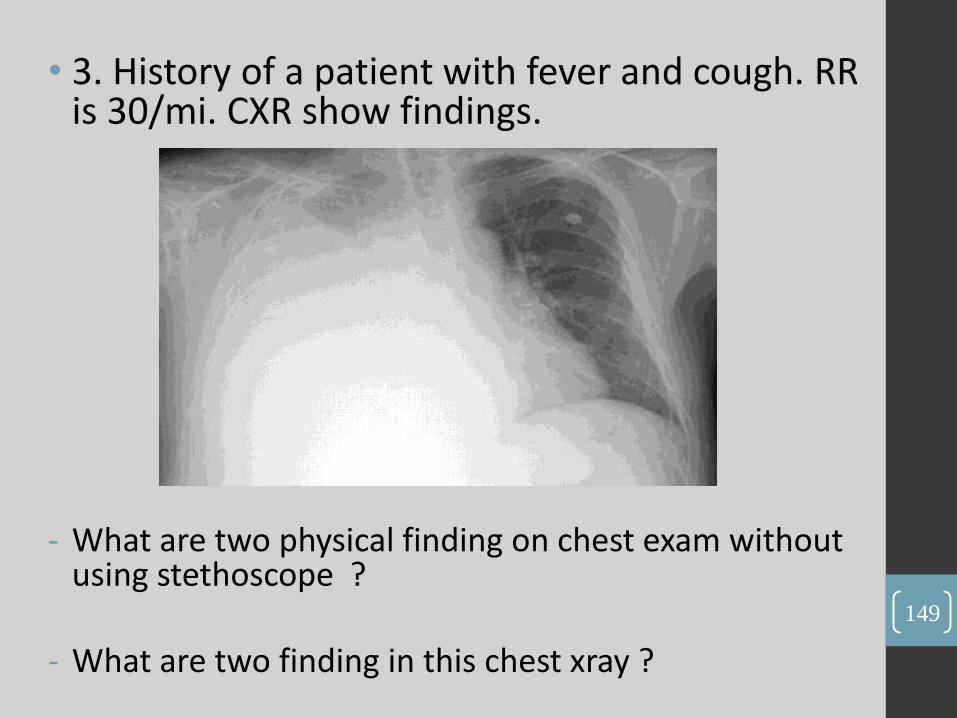
• 3. History of a patient with fever and cough. RR is 30/mi. CXR show findings.
- What are two physical finding on chest exam without using stethoscope ?
- What are two finding in this chest xray ?
149

• 1. Dullness in percussion in right side .
2. Asymmetrical chest expansion .
• 1. Hyperdense or consolidation on the right side .
2. costophrenic angle obliterated or absent
150
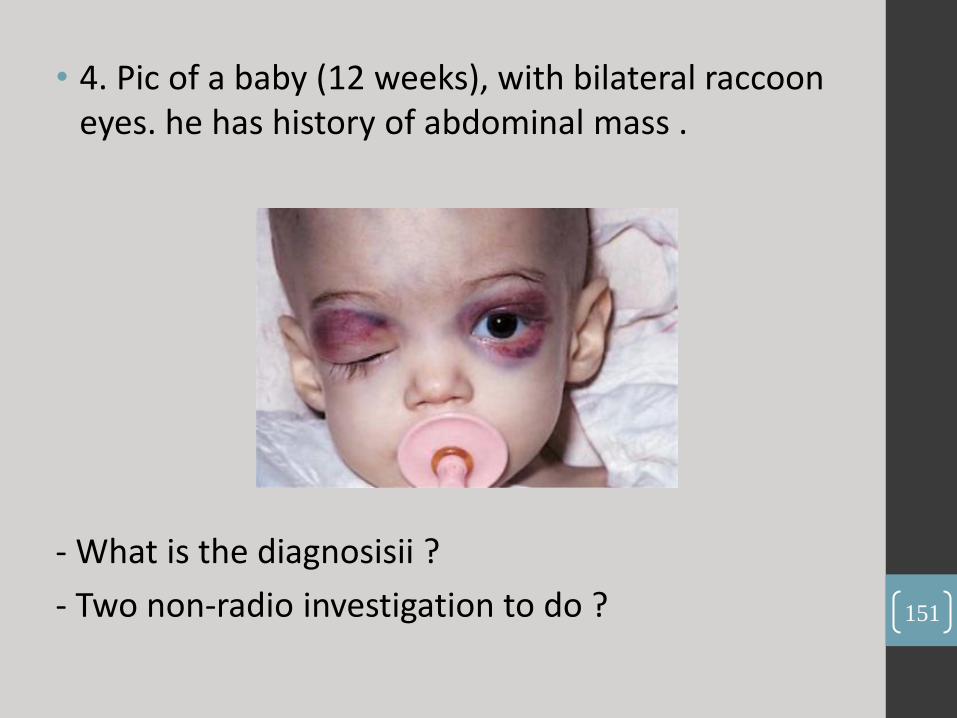
• 4. Pic of a baby (12 weeks), with bilateral raccoon eyes. he has history of abdominal mass .
- What is the diagnosisii ?
- Two non-radio investigation to do ? 151
•Neuroblastoma .
•1. VMA 2. Bone marrow bionsy
152

• 5. PCO2 = 10, HCO3 = 5, pH = 7.05 .
- what are the abnormalities in this ABG?
- what are two most common cause of this ABG in pediatric?
153

•partly compensated metabolic acidosis .
•1. DKA 2. Renal failure 3. Diarrhea
154
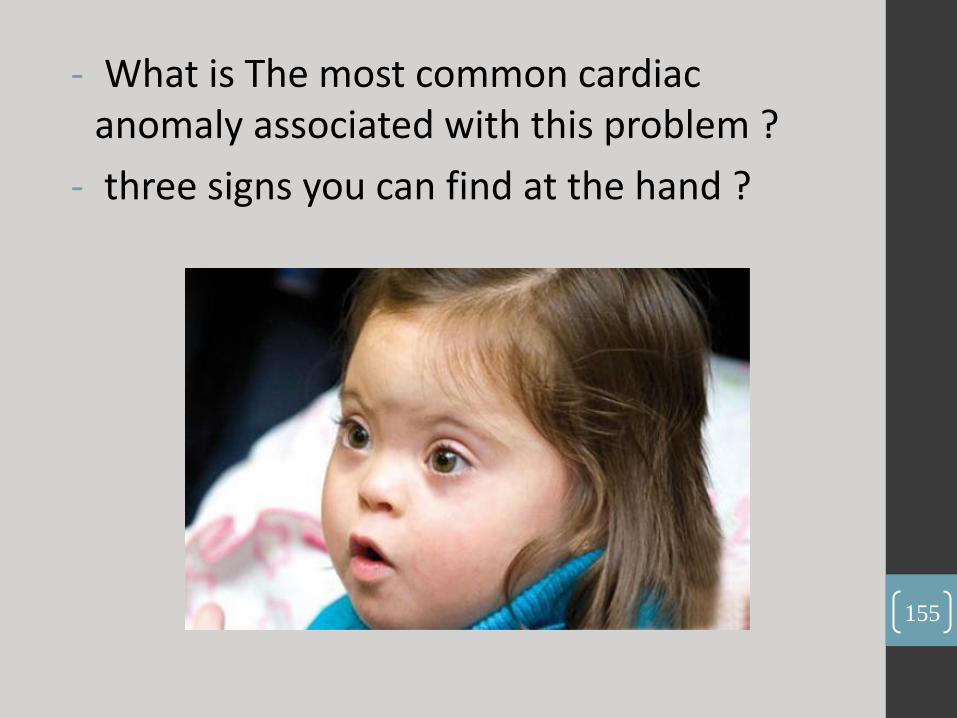
- What is The most common cardiac anomaly associated with this problem ?
- three signs you can find at the hand ?
155

• AV canal .
• 1. Clindactaly 2. Cemian creases 3. Short fingers .
156
7. A case of a baby who underwent brain resection 2 days ago. This is the lab result result Na = 155, Cl = 110, K = 4, Urine spec graviti = 1.003 .
- what is the diagnosis ?
- what is the treatment?
157

- Diabetes insepidus .
- Desmopressin .
158

•8. Cartoon pic of 4 years old healthy boy
•What is this ?
•Two findings on auscultation?
159

- ASD .
- 1. Systolic murmer 2. Fixed splitted S2 .
160
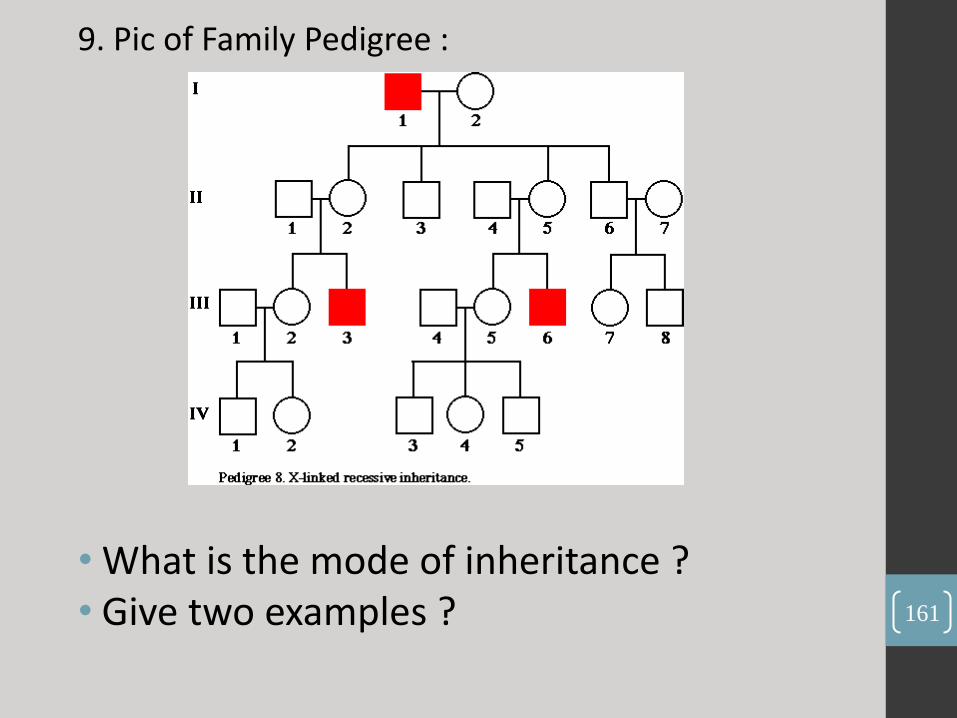
9. Pic of Family Pedigree :
• What is the mode of inheritance ? • Give two examples ? 161

• (X-linked recessive)
• 1. G6PD 2. Hemophilia A & B
162

• What are three findings during ear exam of this patient ?
• What is the most dangerous complication ?
163

• Mastoditis
• 1. Bulging tympanic membrane 2. Loss of light reflexes and cone shape 3. Red color .
164

OSCE : Case 1 (Acute Exacerbation of Asthma) :
6 years old male presented with cough for 3 days.
Hx --> hx of recurrent cough since a long time ago. occur at night, no sputum, no cyanosis. there was audible wheeze. took regular nebulizer. normal growth (weight and height). no fever, no change in bowel habit. past medical history of atopic eczema, family history positive with astma. No hx of contact with patients with respiratory infection.
Physical --> general, signs of respiratory distress and complete chest examination
165
Discussion :
i. What is your diagnosis?
ii. How do you work up this case?
iii. Is there any role of chest xray?
iv. How do you classify/categorize this problem?
v. What is status asthmaticus. What are the signs?
vi. What are the line of treatments in this case.
vii. If you stabilize the patient, sometimes later the nurse calls you and says that the patient deteriorate. What do you think ?
viii. If you want to discharge this patient, what advices you want to give to the parents. 166

• Case 2 (Thallasemia) :
• Hx --> hx of 10 days pallor and jaundice. The patient is a known case of a hemotology problem, but the mother doesnt know what is it. Took regular blood transfusion. Family history positive of hemotological disorders. No hx of recurrent chest infection/chest pain/abdominal pain. He fail to gain weight since birth, and always looks tired. No hx of fava beans ingestion, no hx of splenectomy .
• Physical --> examination of face (pallor or jaundice) and check for liver and spleen. (vertical clean scar on left flank, liver span is 17.5 cm)
167
Discussion :
i. What do you think about this case? Give me your diagnosis?
ii. What test you are going to do to confirm your diagnosis? What are the findings?
iii. How about his parents?
iv. If you look at the blood film, what findings will be there?
v. What do you think about the RBCs of this patient?
vi. What CBC indices that may indicate microcytosis?
vii. Okay, what are things you want to tell the parents?
168
الإسلام لا يحصر نفسه في تلك الحدود الضيقة ، ولا
الصالح ، وإنما يسعى لتحقيق" المواطن"يسعى لإعداد
.الصالح " الإنسان"هدف أكبر وأشمل ، هو إعداد
. الإنسان على إطلاقه ، بمعناه الإنساني الشامل
.الإنسان بجوهره الكامن في أعماقه ....الإنسان من حيث هو إنسان

• Case1:
• LP was done for a 5 days old neonate, the CSF results were: WBCs = 22, RBC = 0 , proteins = 50, Sugar = 3, Blood sugar = 5 .
• Your interpretation .
• Two other CSF tests you will order .
170
- Normal CSF "for neonate“ .
- Gram stain, CSF Culture, PCR, latex agglutination .
171

Case 2:
A 4 y/o girl presented with skin rash. The rash as in picture and was purpuric, and non-blanchable
- What other body organs you will examine.
- Two important lab tests you will order.
172

- Joints, abdomen, eyes .
- KFT, Skin biopsy from the lesion, Urine analysis .
173

Case 3 :
A 7 year old male patient woke-up in the mornings as in the picture below, he has hx of URTI 10 days ago, in the clinic his blood pressure was normal
- Describe what you see :
- What first and rapid test you want to do .
- Two other things you want to examine .
174

• Bilateral peri-orbital edema .
• Urine dipstick for proteinuria .
• Abdomen " ascites” , scrotal swelling, lower limb edema.
175

• Case 4:
• What's your diagnosis
• What is the most common presentation in neonates.
• Name one medical treatment.
176
-Transposition of great vessels .
-Cyanosis .
-PGE1
177
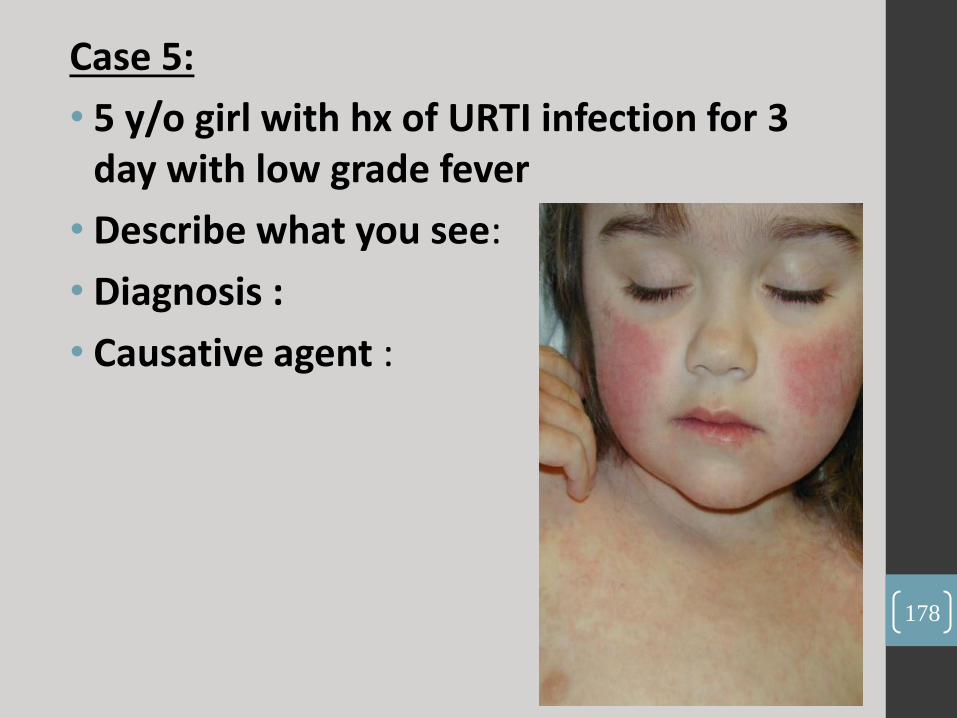
Case 5:
• 5 y/o girl with hx of URTI infection for 3 day with low grade fever
• Describe what you see:
• Diagnosis :
• Causative agent :
178
•slapped cheeks appearance
•Erythema infectiosum
•parvovirus B-19
179
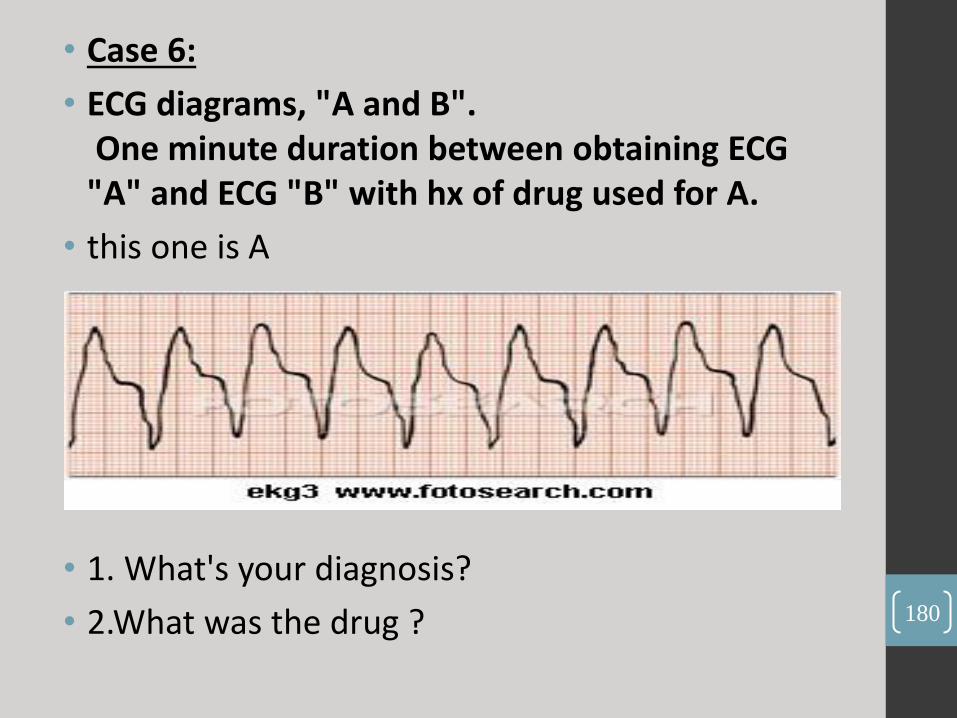
• Case 6:
• ECG diagrams, "A and B". One minute duration between obtaining ECG "A" and ECG "B" with hx of drug used for A.
• this one is A
• 1. What's your diagnosis?
• 2.What was the drug ? 180
- Ventricular tachycardia
- Lidocaine, Amiodarone .
181
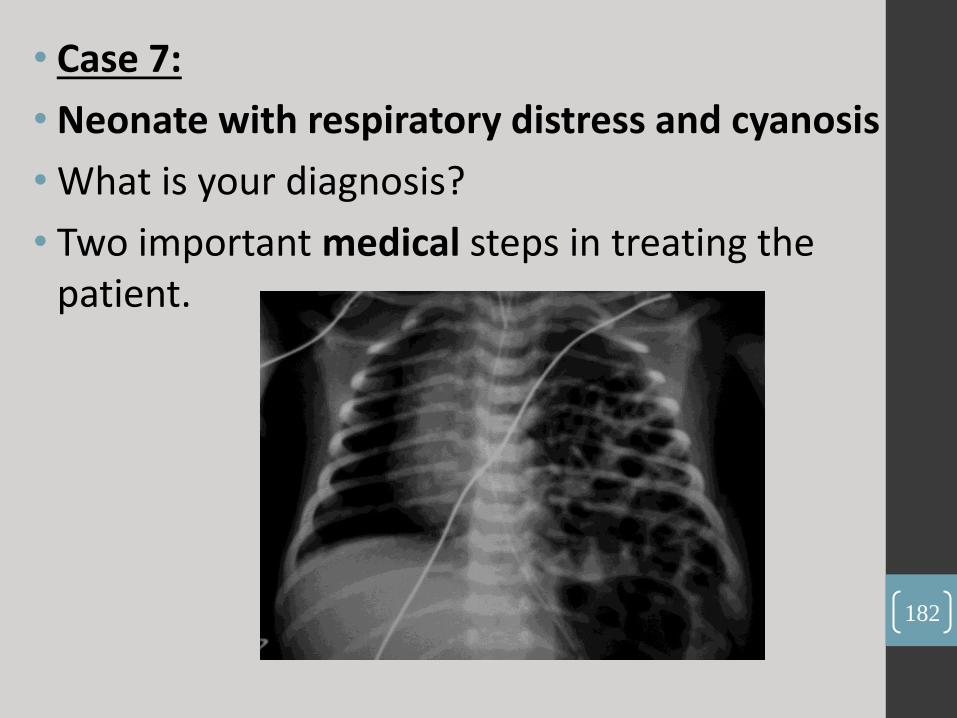
• Case 7:
• Neonate with respiratory distress and cyanosis
• What is your diagnosis?
• Two important medical steps in treating the patient.
182

•Congenital diaphragmatic hernia .
•1. Intubation 2. Decompression by NG tube? .
183

Case 9:
- What is your diagnosis ?
- Two causative MO.
184

•Bullous Impetigo
•1. Staph aureus. 2. Group A beta-hemolytic strep. (pyogenes)
185
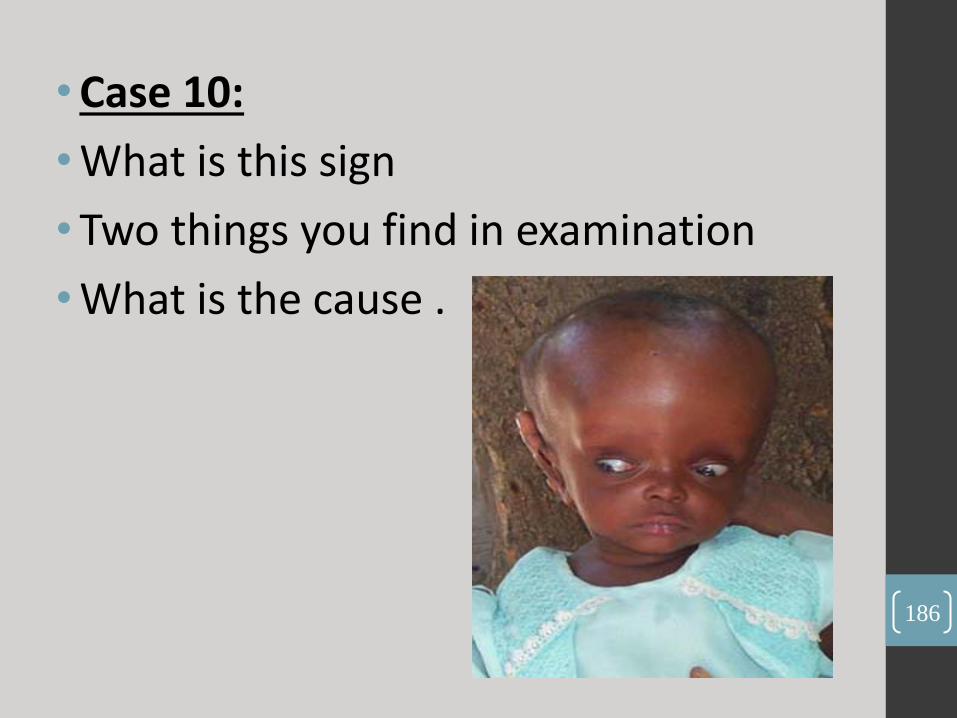
• Case 10:
• What is this sign
• Two things you find in examination
• What is the cause .
186

1. Sunset eyes
2. Increase HC , Bulging fontanel .
3. Increased intracranial pressure " hydrocephalus"
187

OSCE Case 1 : 10 years old boy complain from unsteadiness ( ataxia ) .
Take focused History
Do focused physical exam (finger nose test ,rapid alternative movement , rebound phenomenon, heel shin test , gait ( on soles, on heels, on toes, tandem gait ), nystagmus , fundoscopy , speech ( dysarthria))
Discussion
1. DDx
- Cerebellar ataxia caused by tumor.. other differentials trauma, drugs, infection(chicken pox)
2. What investigations do you want?
- MRI
3. Can you do LP for this patient
- No, due to increase ICP
188
Case 2 : 10 years old boy complain from abdominal pain
Take History
Known case of thalassemia, there was jaundice with history of contact with jaundice patient … You should ask about blood transfusion, Hepatitis B vaccine, hx of Gall bladder stones, hx of cough, family history …
Do physical exam
Discussion
- Diagnosis
Hepatitis A
- Lap investigations
CBC, LFT, serology
- Complications
Fulminant Hepatitis
- How to treat fulminant hepatitis ?
lactulose , Vit K
- What investigations do you want for complications
PT, PTT, Glucose level
189

190

Q1: this anemic child comes to you with splenomegaly :
A: What is the type of his anemia?
B: what is the diagnostic test
in this case?
191
A. Thalassemia Anemia .
B. Hb-electrophoresis .
192
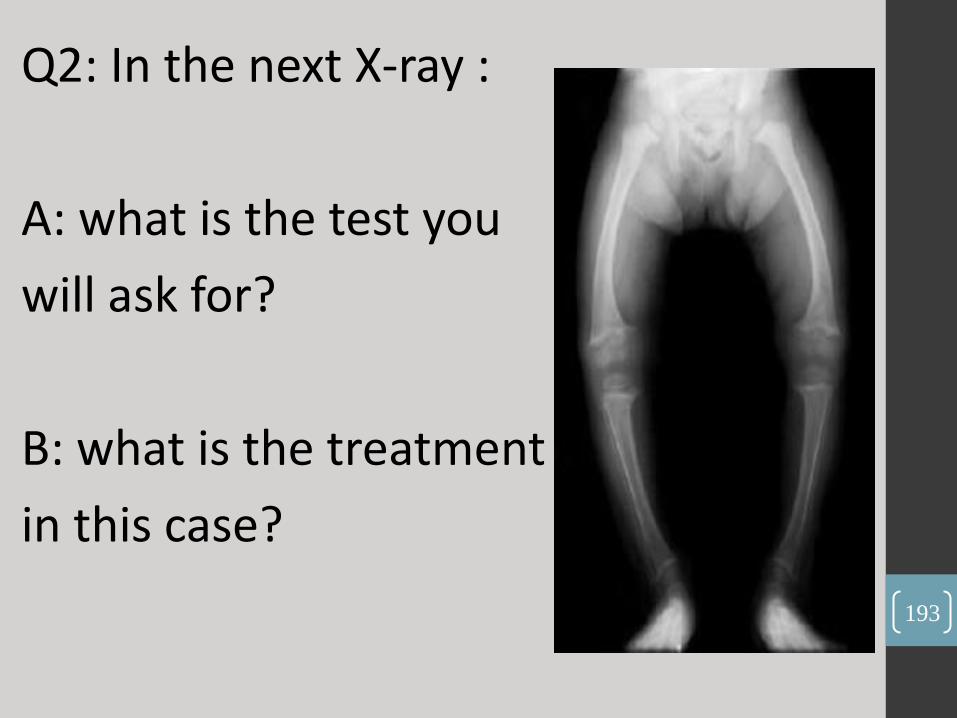
Q2: In the next X-ray :
A: what is the test you
will ask for?
B: what is the treatment
in this case?
193

A. Serum Ca+ and phosphate level.
B. Vitamin D with Ca+ supplement
194

Q3: What is The most Prominent feature in this child?
195

Muscle wasting
196

Q4: In the following image?
A: what is the name
of this test?
B: what is your next test?
197

A. VCUG
B. DMSA
198

Q5. in the following image:
a. what is the main
abnormality you can find it in this
patient?
CVS abnormality (VSD).
b. name the test you want to
confirm your diagnosis?
cytogenetic test 199

A. CVS abnormality (VSD).
B. cytogenetic test .
200

Q6: In the following picture :
A : what is your diagnose :
B: what do you expect to find in his lower extremities?
201

A: myelomeningocele.
B: hypotonia.
202

A B
Q7: what’s the expected age in :
203

A : 4 months
B : 9 months
204
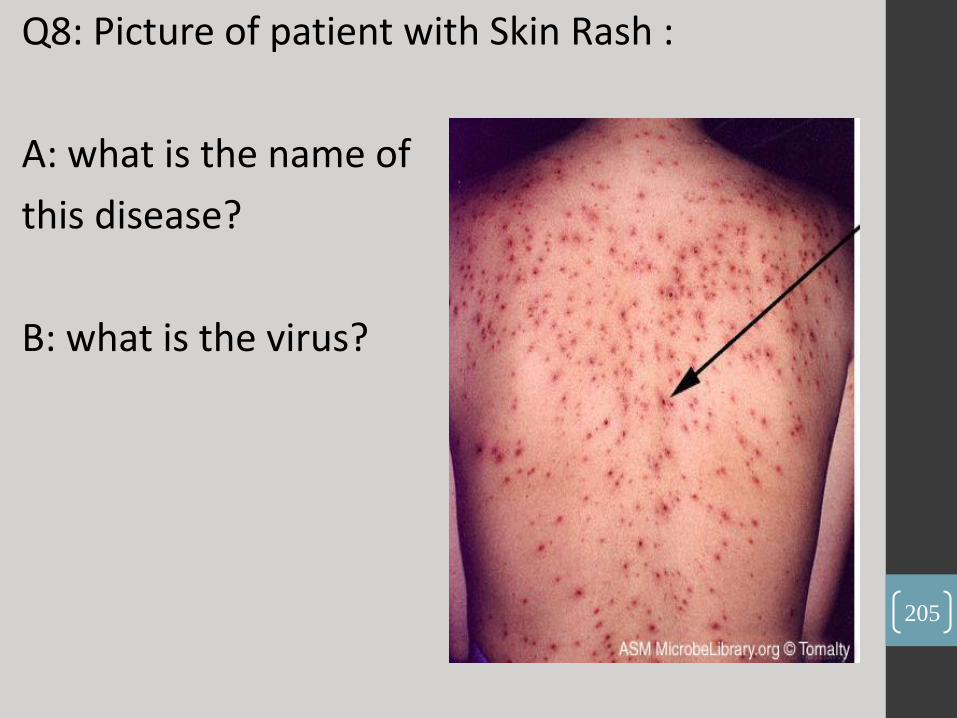
Q8: Picture of patient with Skin Rash :
A: what is the name of
this disease?
B: what is the virus?
205

A: Chickenpox
B: Varicella zoster virus.
206

Q9: in the following image:
A: what is the name of this sign?
B: what is the next examination?
207
A: sunset eyes (setting sun sign).
B: Head circumference.
208

Q10: Q: picture of patient with purpuric rash in the lower limbs.
A: what is the diagnosis?
B: mention 2 other clinical findings in this patient?
209
A: HSP .
B: 1. Arthralgia 2. Abdominal pain
210
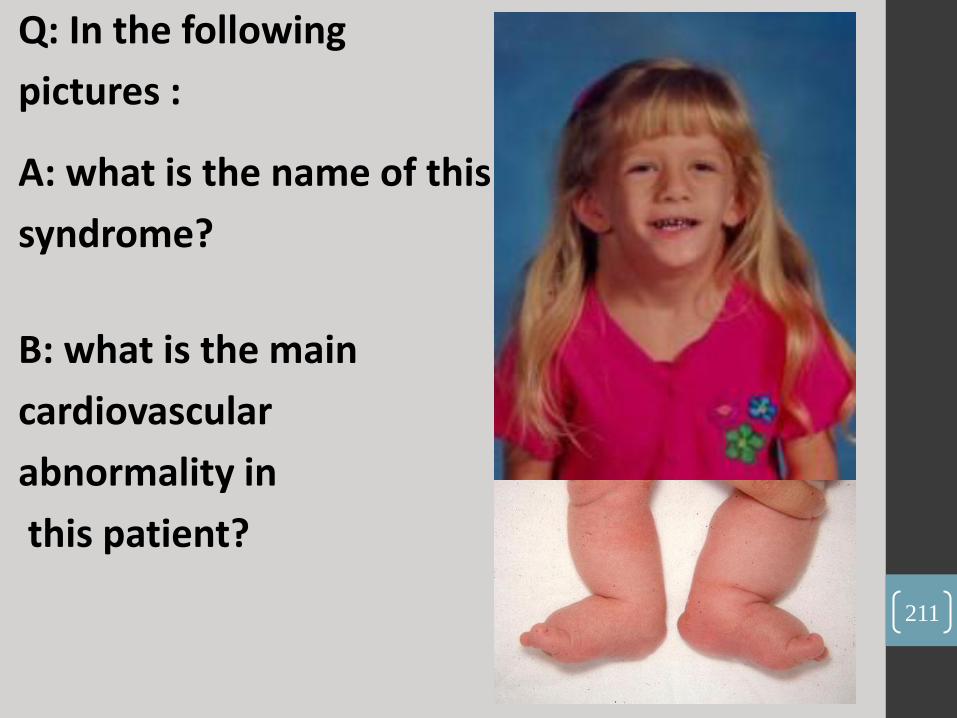
Q: In the following
pictures :
A: what is the name of this
syndrome?
B: what is the main
cardiovascular
abnormality in
this patient?
211

212
A. Turner syndrome .
B. coarctation of the aorta.

1. whats the most likely diagnosis ?
2. mention tow abnormal vital signs in this
baby ?
213

•cushing syndrome.
•high body temperature, high blood pressure, high heart rate
214

Q1: what’s the name of this test ?
Q2: mention tow abnormalities you expect to
find in the lower extremities of this child?
215
1. babinski sign.
2. clonus, hyperreflexia “brisk tendon reflexes”
216
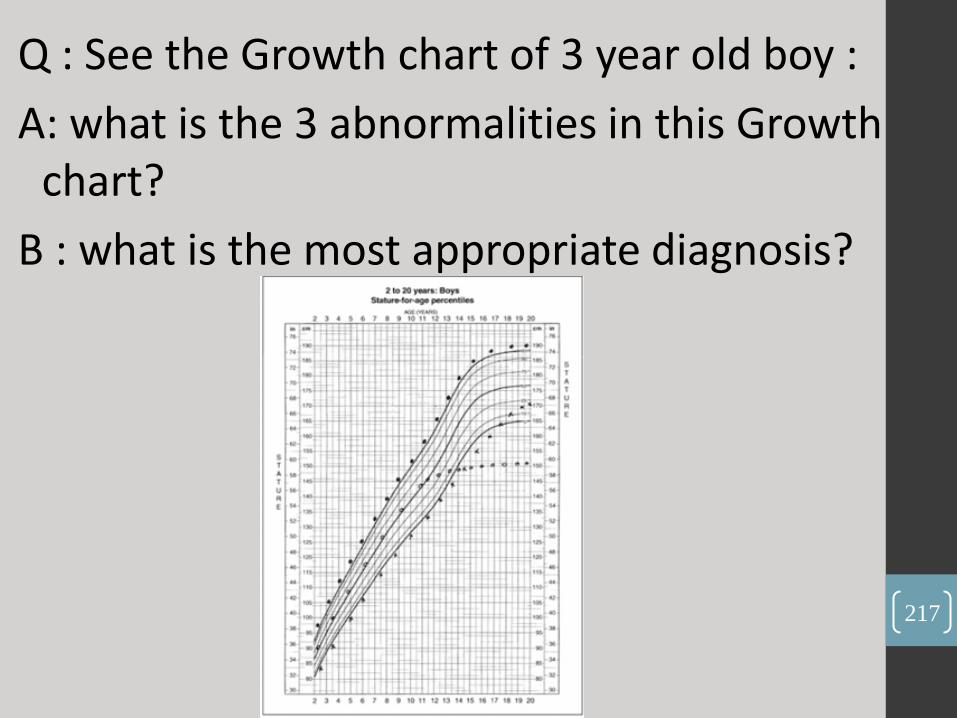
Q : See the Growth chart of 3 year old boy :
A: what is the 3 abnormalities in this Growth chart?
B : what is the most appropriate diagnosis?
217

Celiac disease.
218

1. in this image:
a. mention two clinical findings in this patient?
b. What system do you want to examine for this patient?
219
a. Clubbing - Cyanosis
b. CVS or RS
220

2. Infant with head bulging in the first week of life :
a. what is the diagnosis?
b. mention two complication That may occur in that patient?
221

a. Cephalhematoma.
b. Anemia , Jaundice
222

3. in the following image:
a. what is the main abnormality You can find it in this patient?
b. name the test you want to Confirm your diagnosis?
223
A. CVS Abnormality (VSD).
B. Cytogenetic Test
224

4. in the following image: a. what is your diagnosis? b. what you want to do for that patient, & why?
225

a. Mangolian spots
b. Nothing, because it normally disappears 3 – 5 years after
birth
226
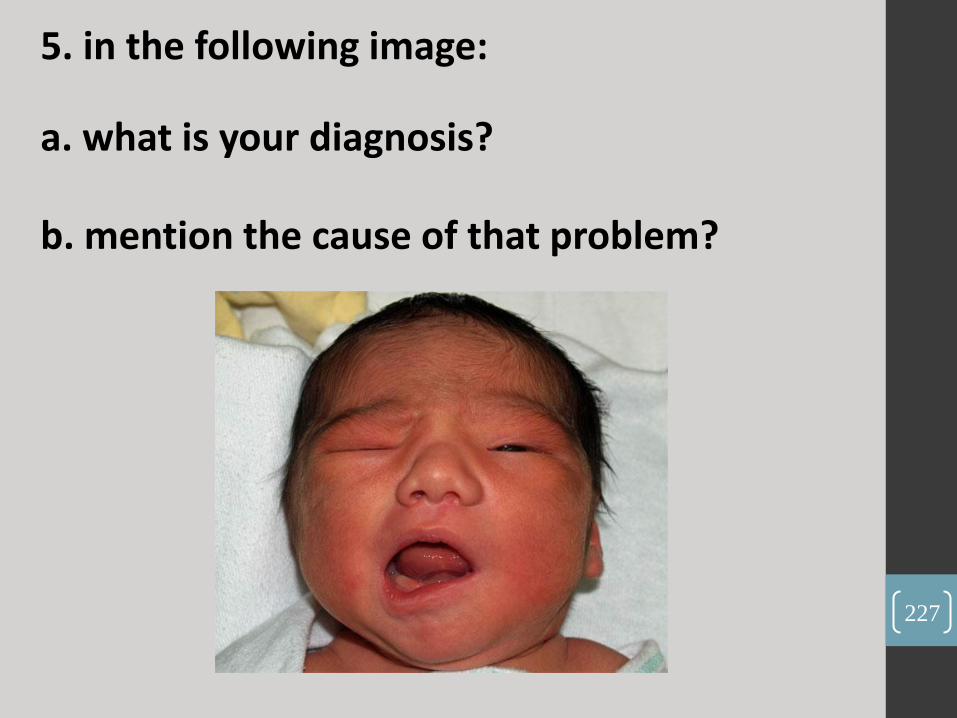
5. in the following image:
a. what is your diagnosis?
b. mention the cause of that problem?
227

a. Facial Palsy .
b. Birth injury (Injury To facial nerve)
228

6. in the following image:
a. mention two clinical findings in the physical examination?
b. what is the cause of these manifestations?
229

a. Head Lag , C-shape or Drapes over in horizontal suspension.
b. Hypotonia
230

8. In this X-ray: a. name the lesion that you see in this X ray ? b. what is your diagnosis ?
231

a. Consolidation in the right lung / or
collapse in the same lung
b. Pneumonia / or obstruction by foreign body
232
9. Case with CSF analysis:
In that analysis was Leukocytosis, high protein concentration, High glucose concentration, High number of neutrophils.
What is your diagnosis?
233
Bacterial Meningitis
234
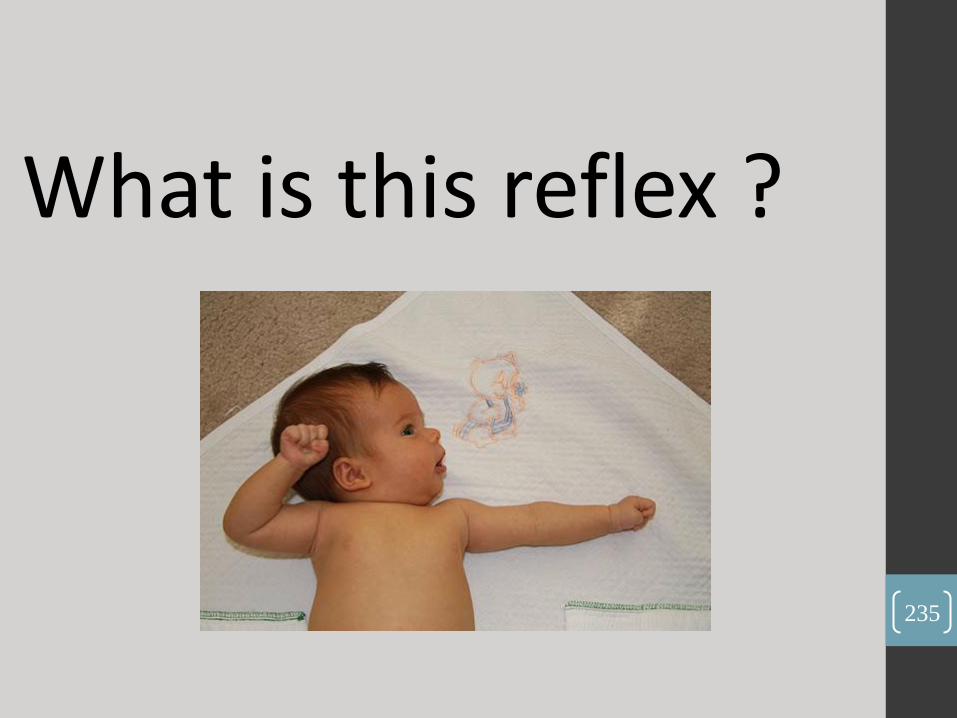
What is this reflex ?
235

Asymmetrical Tonic
neck reflexes
disappears by 3-4
months
236
:عن النبي صلى الله عليه وسلم ، قال
س عن مؤمن كربة من كرب الدنيا من نف )
س الله عنه كربة من كرب يوم القيامة ، نف
ومن يسر على معسر يسر الله عليه في الدنيا
والآخرة ، ومن ستر مسلما ستره الله في
الدنيا والآخرة ، والله في عون العبد ما كان
العبد في عون أخيه ، ومن سلك طريقا
يلتمس فيه علما سهل الله له به طريقا إلي
(. ....... ةالجن237

1- What is your Diagnosis?
2- Give other 4 physical findings related to this disorder ? (not seen in the image)
238
Down Syndrome
239

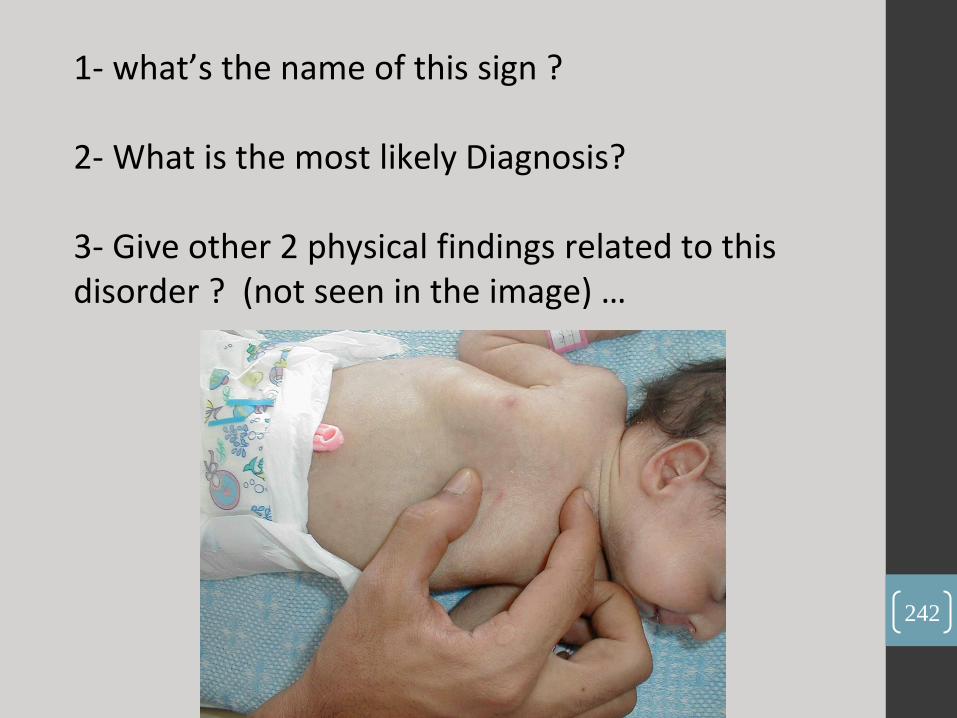
1- what’s the name of this sign ?
2- What is the most likely Diagnosis?
3- Give other 2 physical findings related to this
disorder ? (not seen in the image) …
240
Rocker bottom feet in Trisomy 18 .
Edwards syndrome
241
1- what’s the name of this sign ? 2- What is the most likely Diagnosis? 3- Give other 2 physical findings related to this disorder ? (not seen in the image) …
242
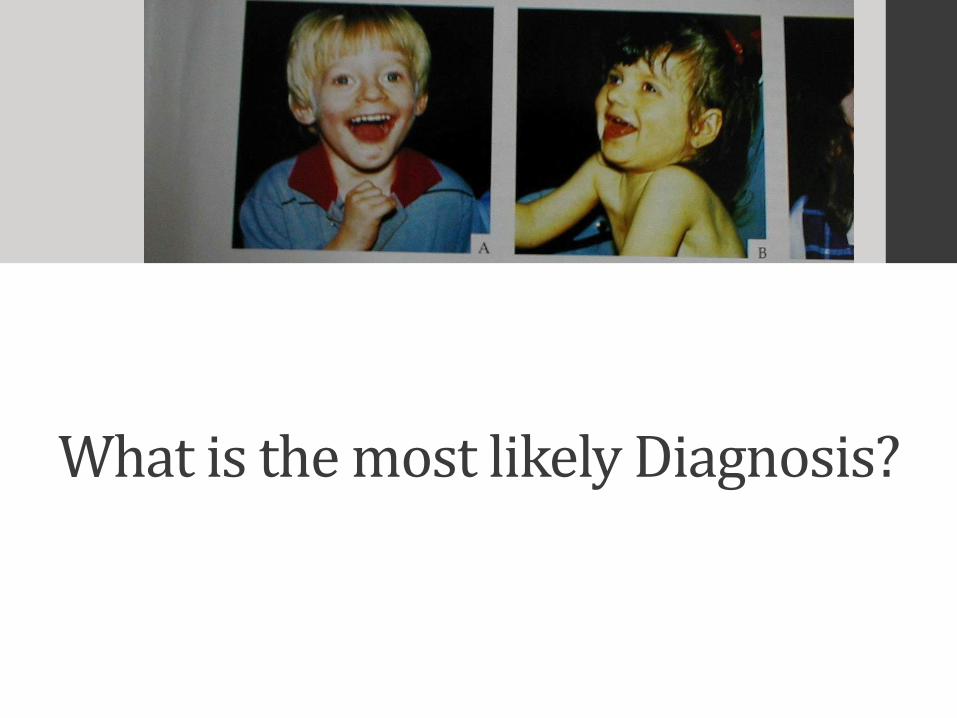
What is the most likely Diagnosis?
243
Angelman Syndrome
244

2- What is the most likely Diagnosis?
245
Prader–Willi syndrome
246
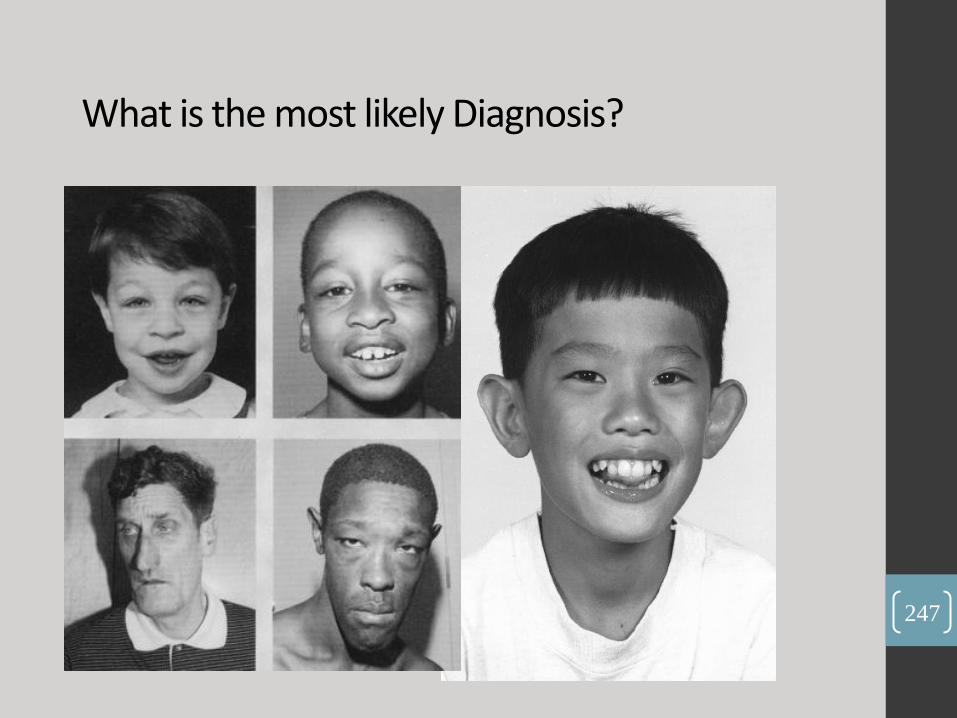
What is the most likely Diagnosis?
247
•Fragile X Syndrome
248

6 year old boy came to your clinic complaining of cough and
fever …
1- mention the prominent finding ?
2-What is the most likely Diagnosis?
3- name the most common microorganism .. ?
249

Right Side consdilation
250
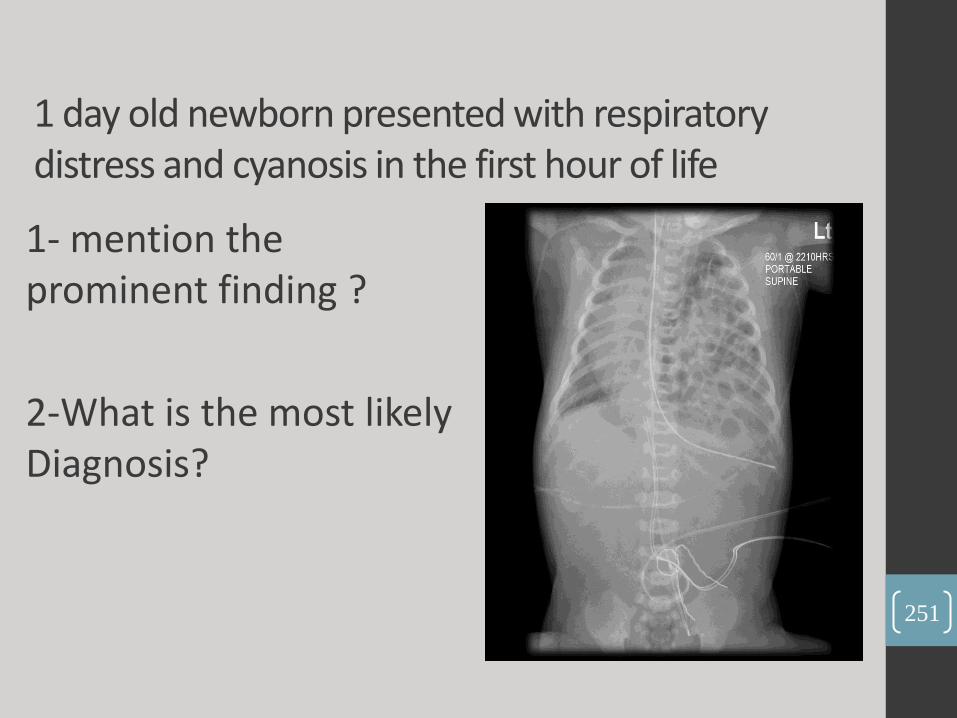
1 day old newborn presented with respiratory distress and cyanosis in the first hour of life
1- mention the prominent finding ?
2-What is the most likely Diagnosis?
251

Diaphragmatic Hernia
252

1- mention the prominent finding ?
2-What is the most likely Diagnosis?
253

254
Pneumothorax
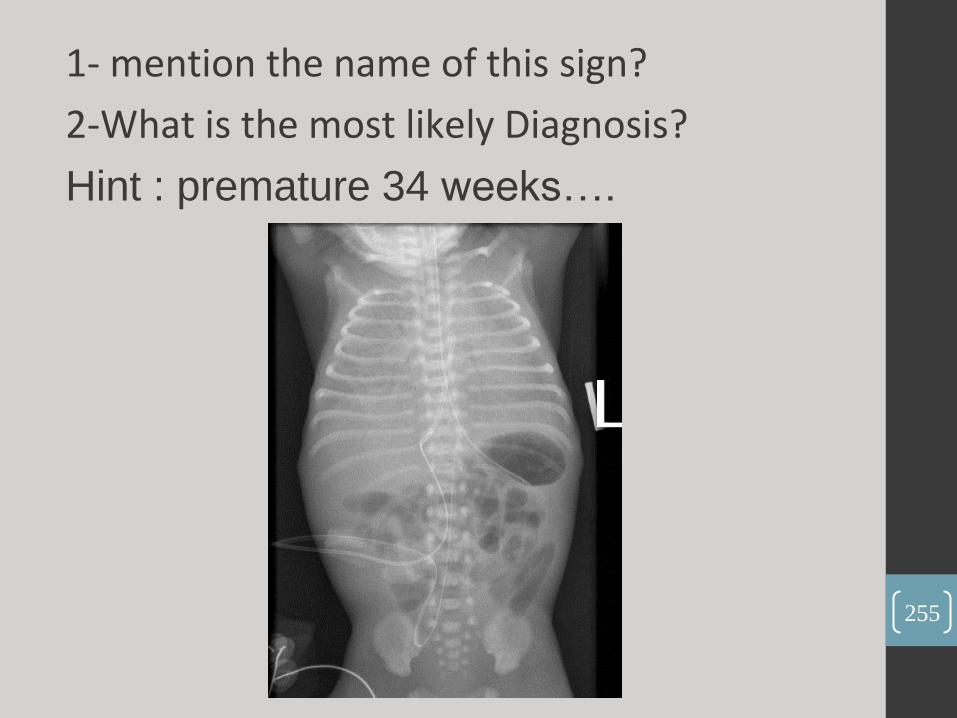
1- mention the name of this sign?
2-What is the most likely Diagnosis?
Hint : premature 34 weeks….
255
256
Respiratory Distress Syndrome

• 1- mention the name of this sign?
• 2-What is the most likely Diagnosis?
257
258
Sail sign of
thymus .
Normal x-ray
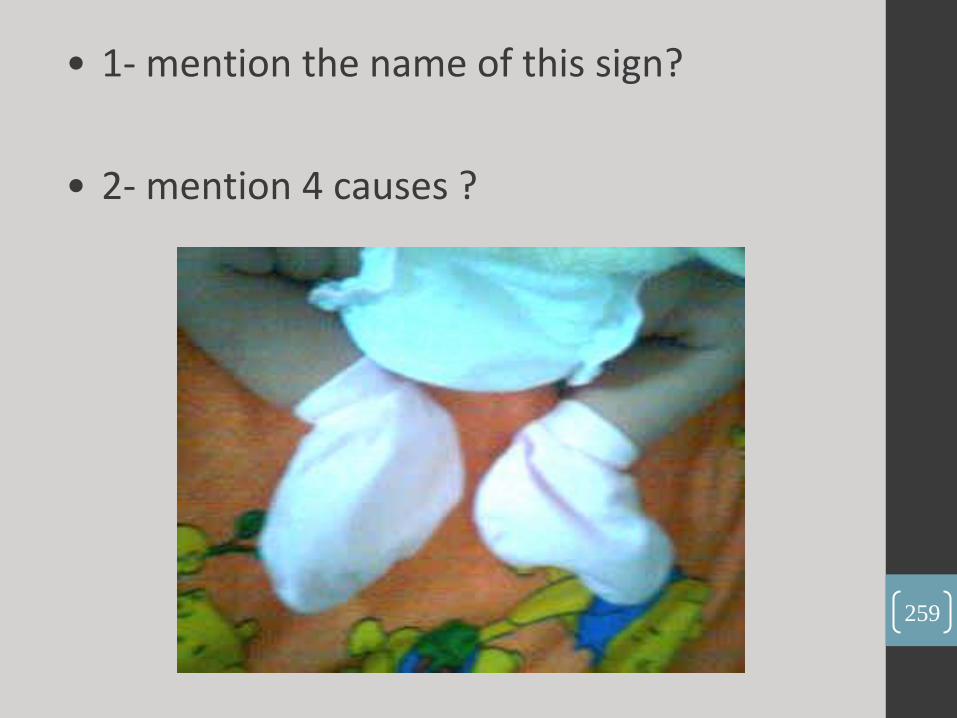
• 1- mention the name of this sign?
• 2- mention 4 causes ?
259

Frog Like Posture Hypotonia
260
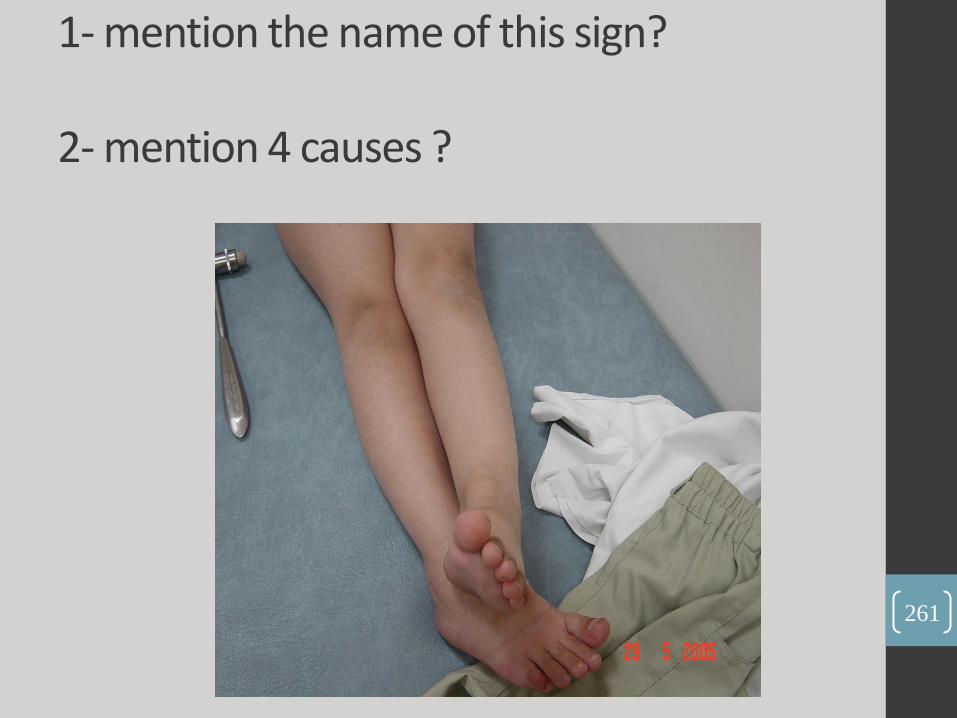
1- mention the name of this sign? 2- mention 4 causes ?
261

Scissoring posture
262

What is the name of those reflexes ?
1 2 3 263

1. parachute reflex . 2. asymmetrical tonic neck
reflex . 3. symmetric tonic neck
reflex
264

1- what’s the name of this sign ? 2- What is the most likely Diagnosis?
3- name the causing microorganism .. ?
265
266
• slapped cheeks appearance
• Erythema infectiosum
• parvovirus B-19

1- what’s the name of this sign ?
2- What is the most likely Diagnosis?
3- What other signs do you expect on examination?
267
268
Double Bubble Duodenal Atresia
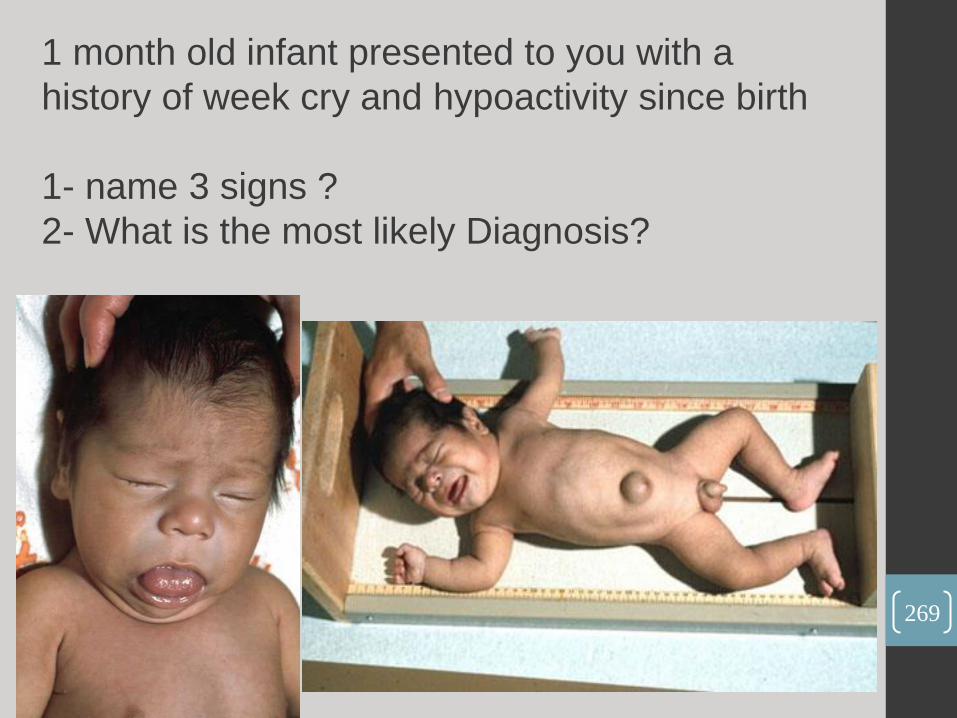
1 month old infant presented to you with a
history of week cry and hypoactivity since birth
1- name 3 signs ?
2- What is the most likely Diagnosis?
269

Congenital Hypothyroidism
270
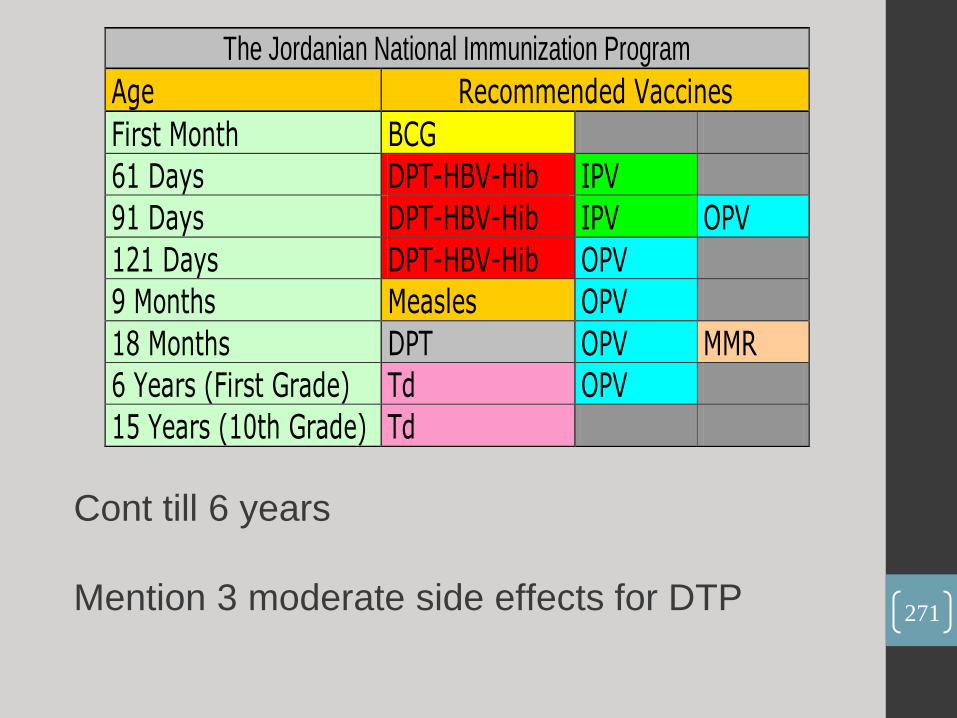
The Jordanian National Immunization Program
Age Recommended Vaccines
First Month BCG
61 Days DPT-HBV-Hib IPV
91 Days DPT-HBV-Hib IPV OPV
121 Days DPT-HBV-Hib OPV
9 Months Measles OPV
18 Months DPT OPV MMR
6 Years (First Grade) Td OPV
15 Years (10th Grade) Td
Cont till 6 years
Mention 3 moderate side effects for DTP
271
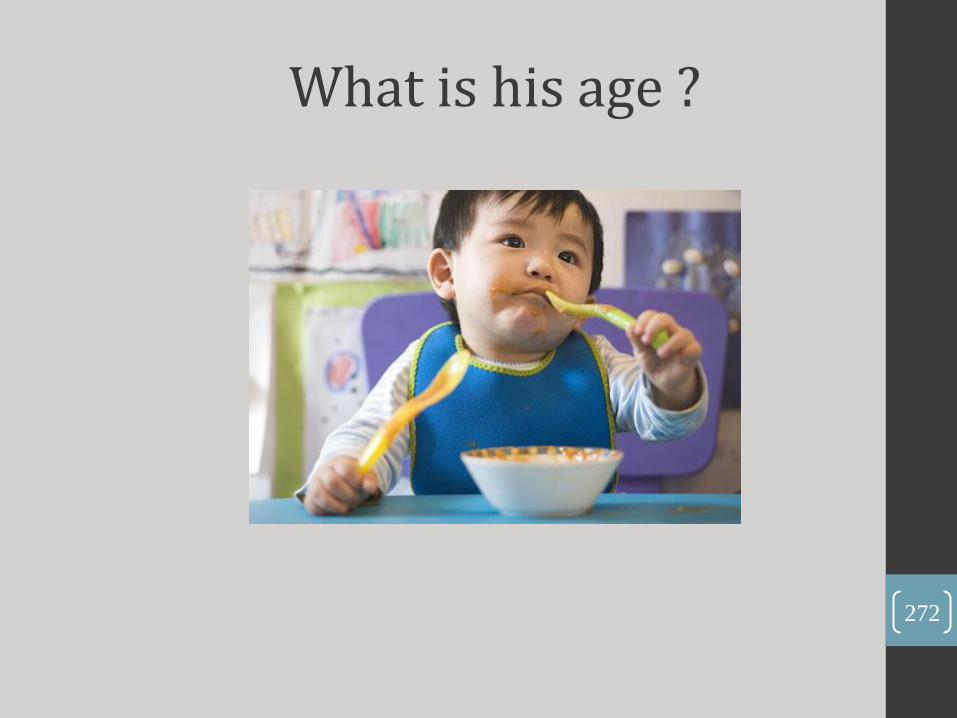
What is his age ?
272
2 Years
273

What is his age ?
274

Age 10-11 months
275

What is his age ?
276

277
4 months

What is his age ?
278
279
2 months
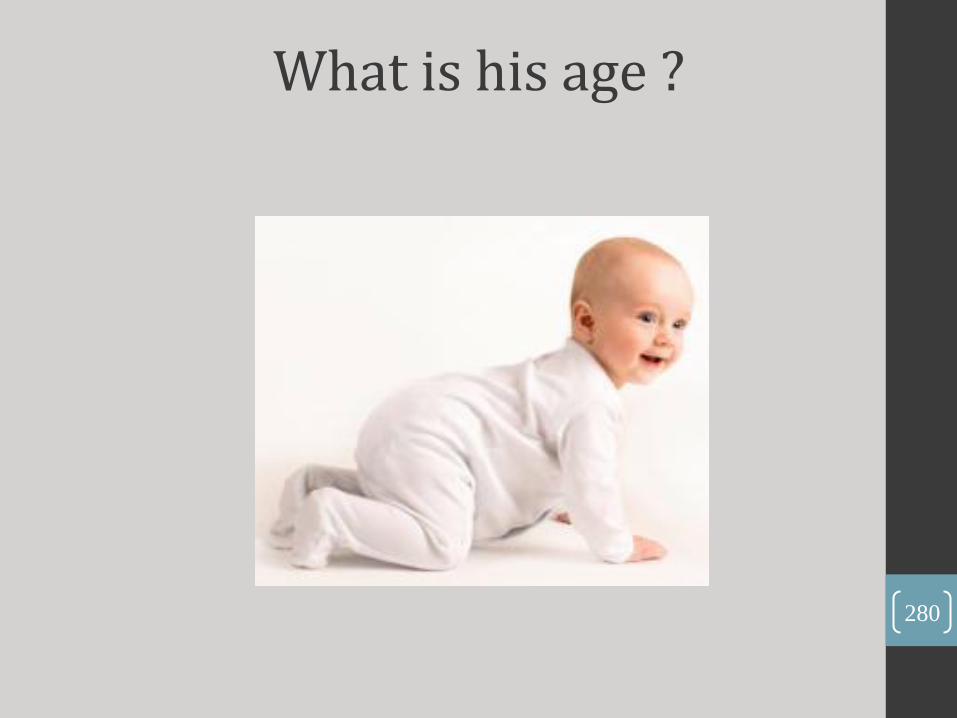
What is his age ?
280
281
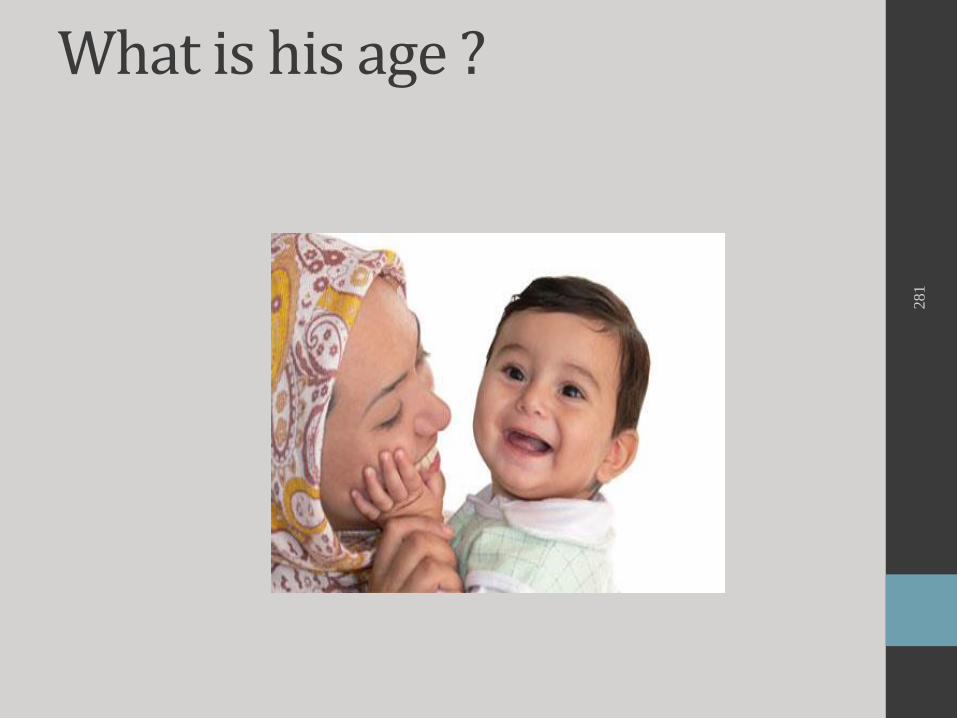
What is his age ?

•Age 6-7 months Prefers mother
282

What is his age ?
283
284
Age 12 months
Mature pincer’s
grasp
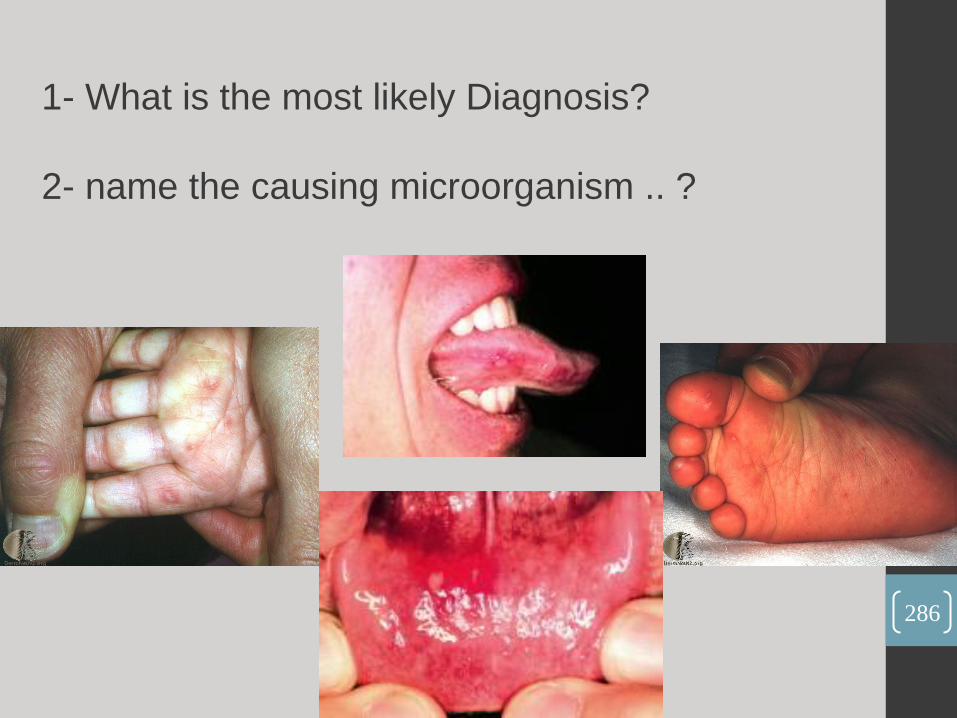
1- What is the most likely Diagnosis?
2- name the causing microorganism .. ?
286
Hand , foot and
mouth disease .
Organism :
Coxsackie A virus and
Enterovirus
287
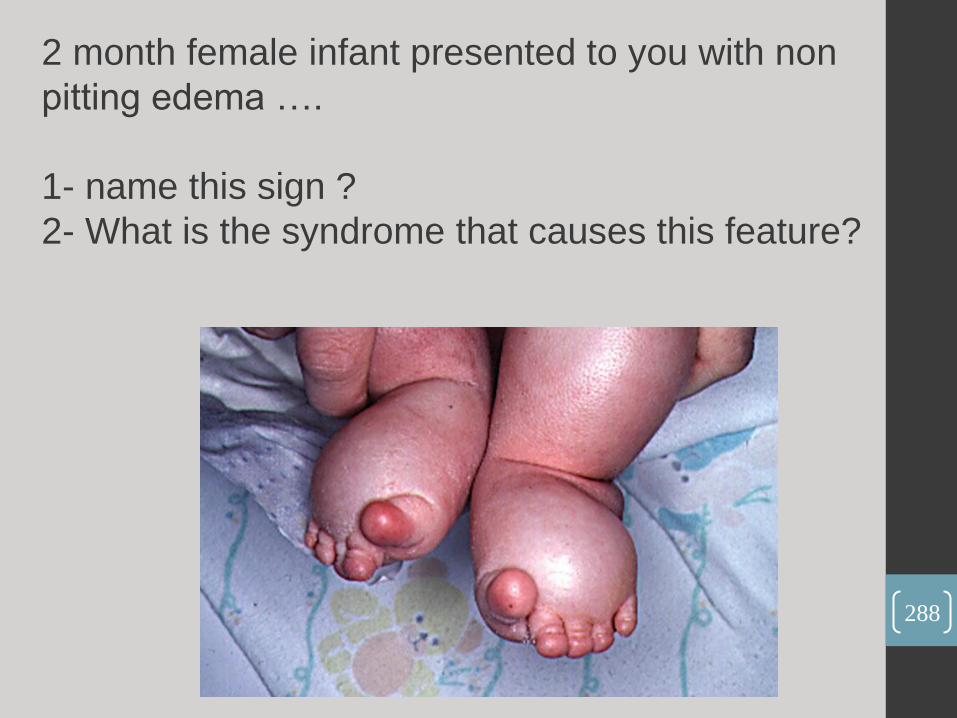
2 month female infant presented to you with non
pitting edema ….
1- name this sign ?
2- What is the syndrome that causes this feature?
288

289
Turner syndrome .
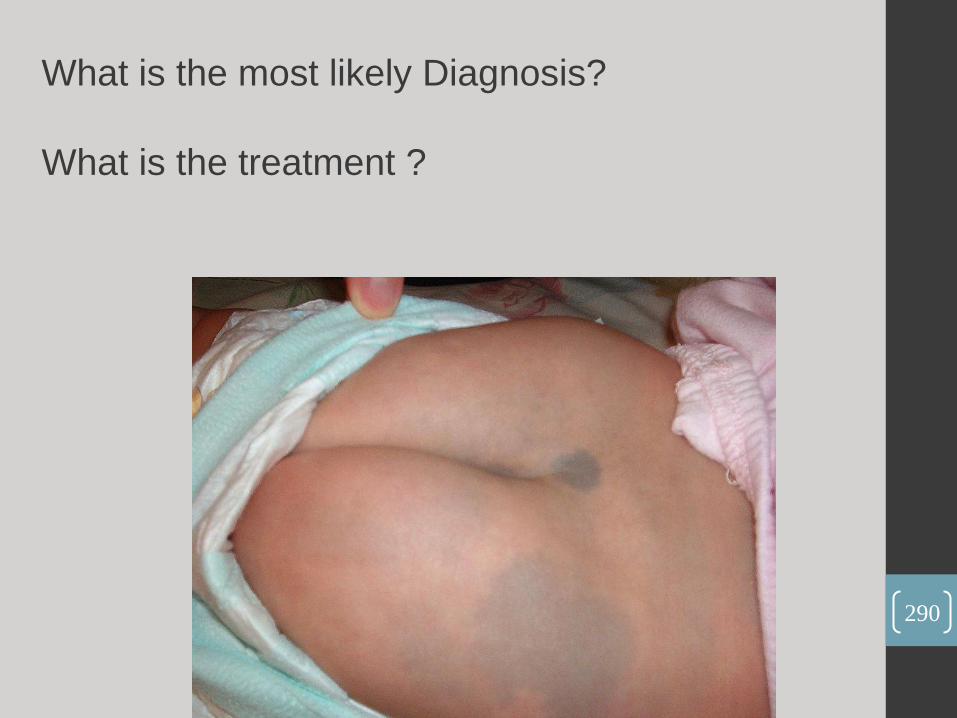
What is the most likely Diagnosis?
What is the treatment ?
290

a. Mangolian spots
b. Nothing, because it normally disappears 3 – 5 years after
birth
291

4 year patient presented with rash, abdominal pain and ankle pain What is the most likely Diagnosis?
292
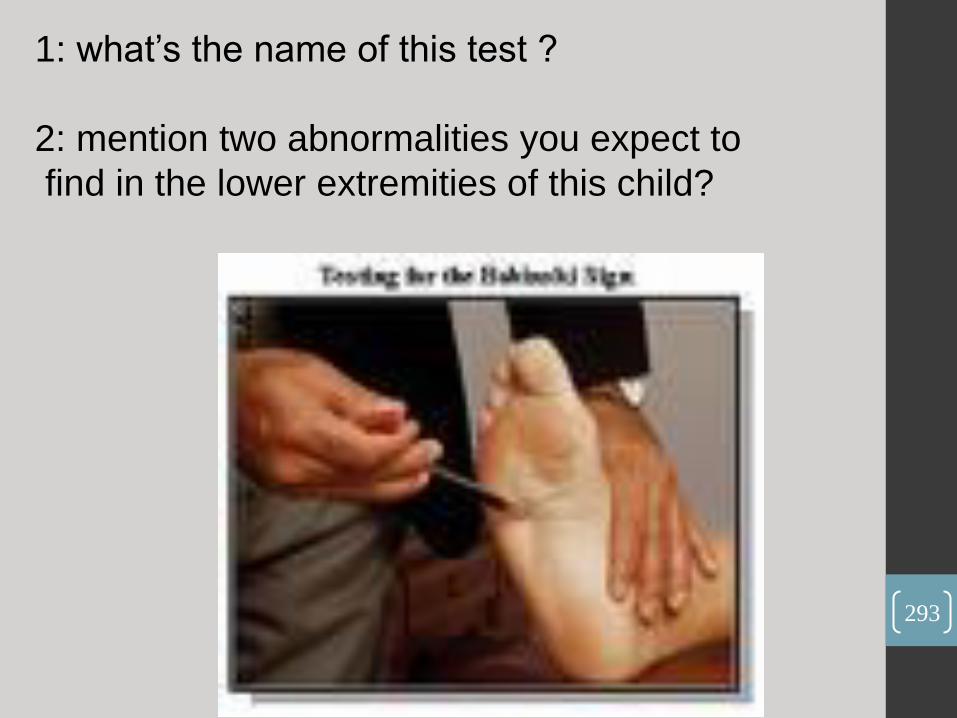
1: what’s the name of this test ?
2: mention two abnormalities you expect to
find in the lower extremities of this child?
293
1. babinski sign.
2. clonus, hyperreflexia “brisk tendon reflexes”
294
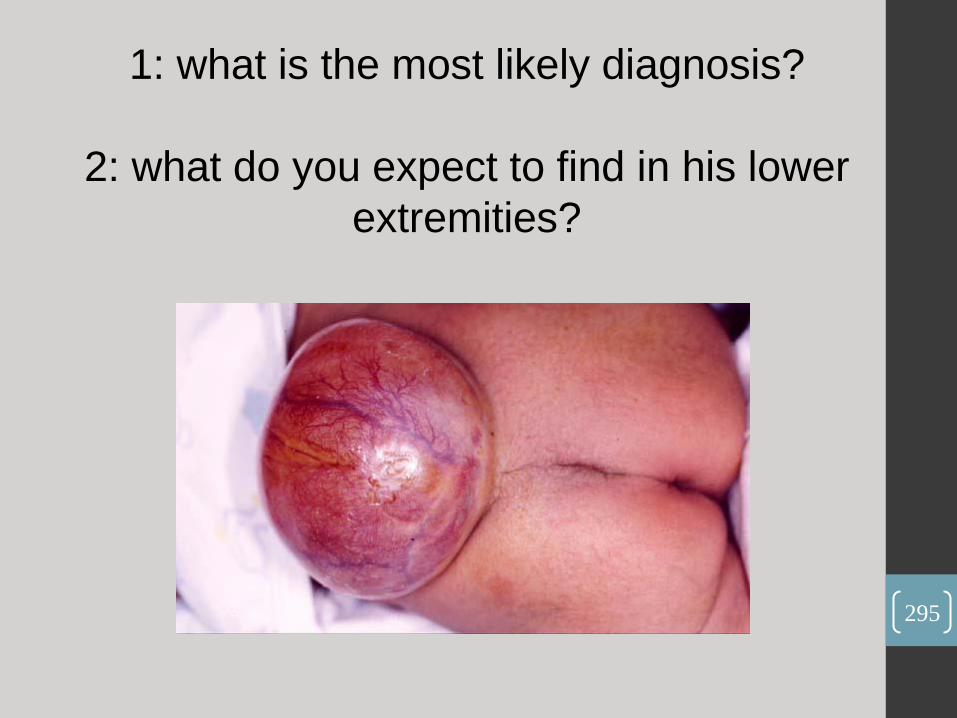
1: what is the most likely diagnosis?
2: what do you expect to find in his lower
extremities?
295

•Meningomylocele caused by
hdrocephelus craini.
•Hypotonia .
296
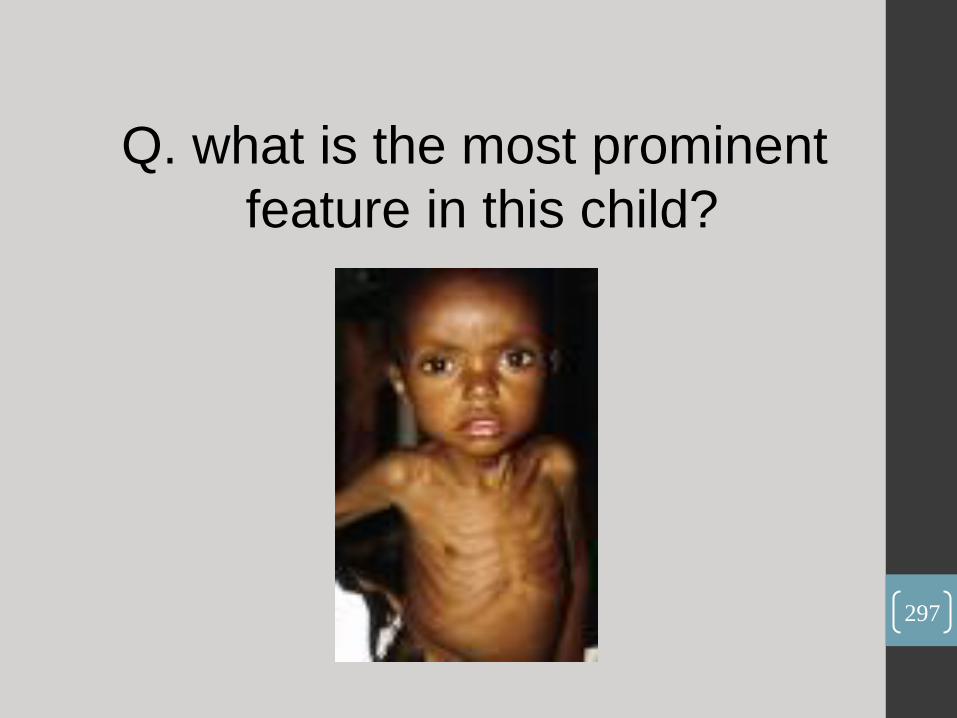
Q. what is the most prominent
feature in this child?
297

298
Muscle
Wasting

1: what is the most likely diagnosis? 2: mention two abnormal vital signs in this baby?
299
•cushing syndrome.
•high body temperature, high blood pressure, high heart rate
300
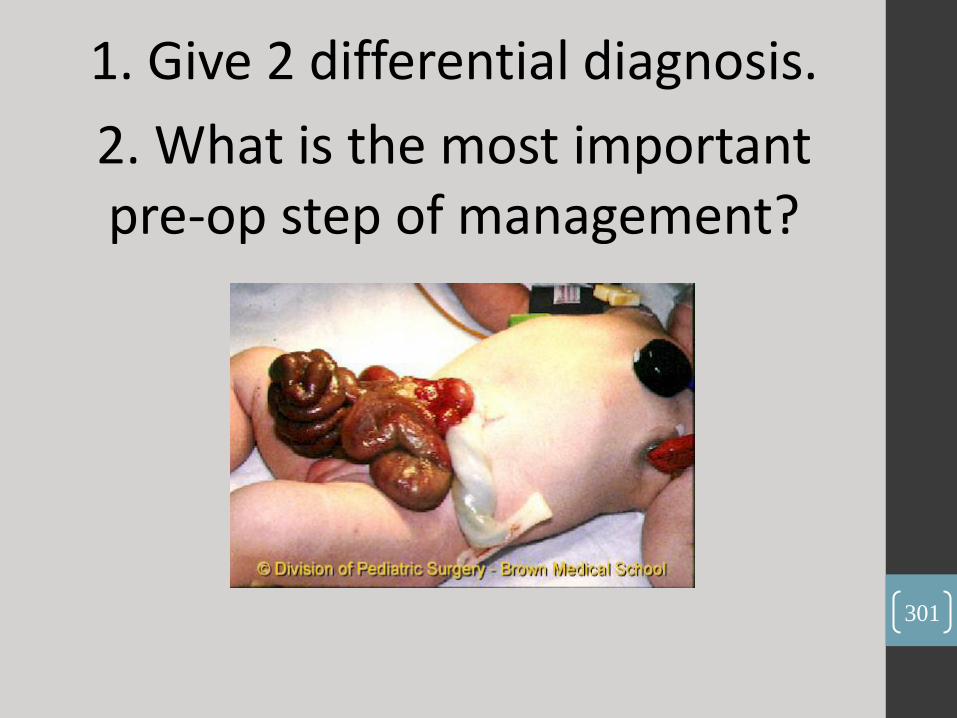
1. Give 2 differential diagnosis.
2. What is the most important pre-op step of management?
301

•1. Gastroschisis, Omphalocele.
•2. Covering.
302

• In exam there were arrows indicating P waves.
•1.What is the diagnosis?
•2.Mention one cause.
303
•1.Congenital (complete) heart block.
•2.Maternal SLE.
304
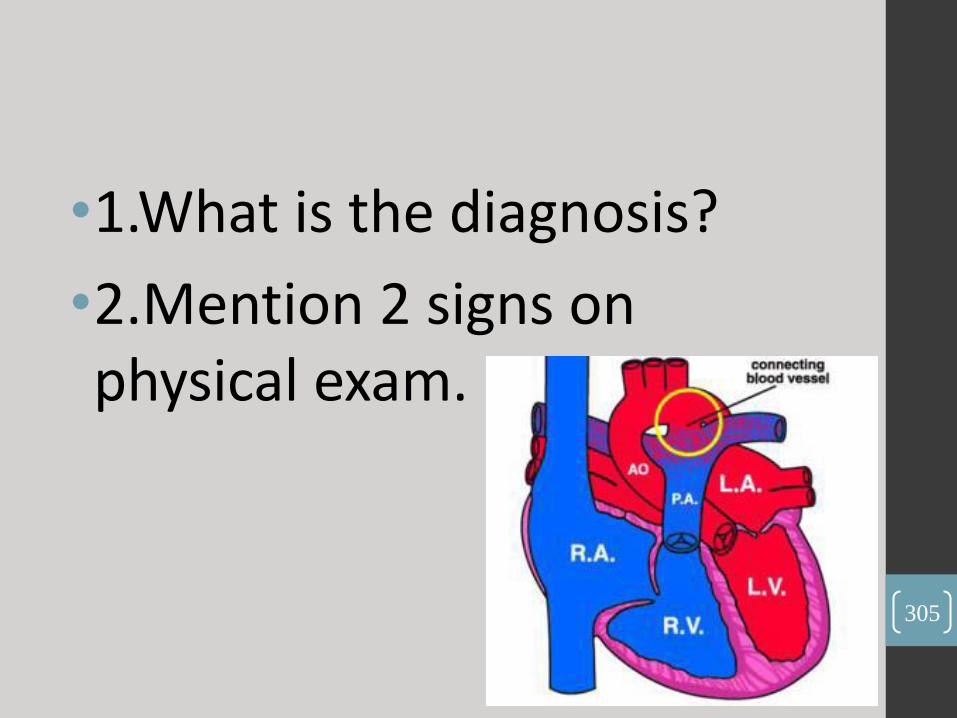
•1.What is the diagnosis?
•2.Mention 2 signs on physical exam.
305
•1.PDA.
•2.Machinery like murmur, bounding pulse.
306
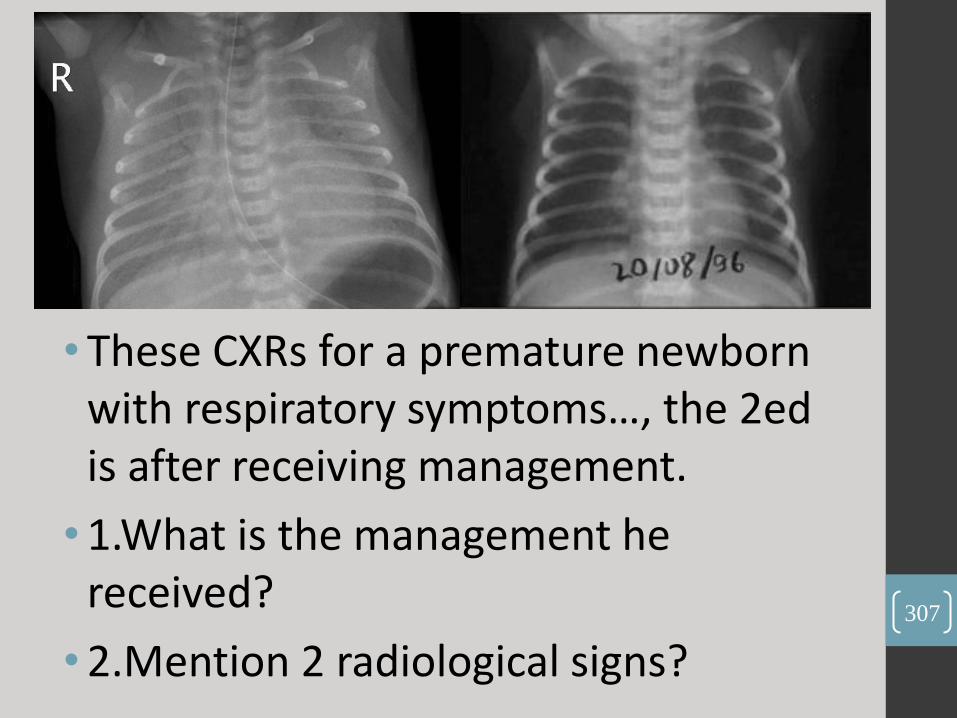
• These CXRs for a premature newborn with respiratory symptoms…, the 2ed is after receiving management.
• 1.What is the management he received?
• 2.Mention 2 radiological signs?
307
•1.Surfactant.
•2.Ground glass appearance, air bronchogram.
308
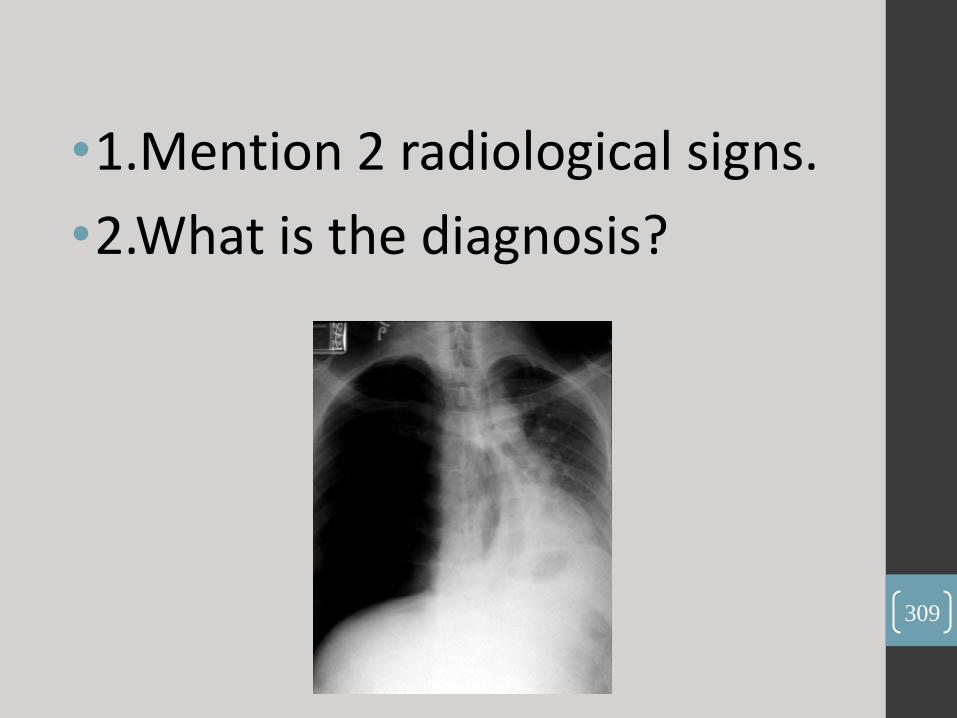
•1.Mention 2 radiological signs.
•2.What is the diagnosis?
309
• I think it was on the left side (flip it horizontally ), shifted mediastinumwere obvious, even drQuteishsaid this patient has no dexocardia…
• 1.Hyperlucentexpanded hemithorax, shifted mediastinum.
2.Tension pneumothorax.
310

• Hx: Mentally retarded, his brother has similar condition (Autosomal Dominant)
• 1.Mention 2 signs.
• 2.What is the diagnosis?
311

1. Shagreen patch, ungual fibromas, adenoma sebaceum.
2. Tuberous sclerosis.
312
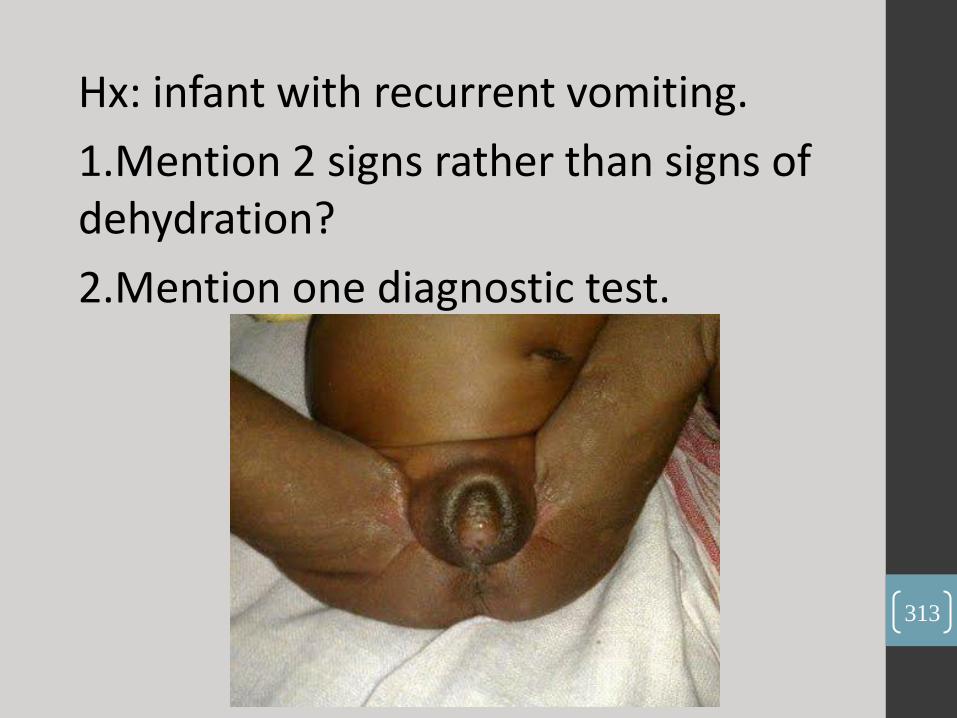
Hx: infant with recurrent vomiting.
1.Mention 2 signs rather than signs of dehydration?
2.Mention one diagnostic test.
313
• It is a case of congenital adrenal hyperplasia.
• 1.Dark scrotum, ambiguous genitalia.
• 2.Definitive test according to KAPLAN >>> measure 17-OH progesterone before and after an IV bolus of ACTH.
314

• ABGs for a patient with chronic renal failure on diuretics: pH increased, bicarbonate increased, PaCO2increased, K decreased.
• 1.What is the diagnosis?
• 2.What is the cause?
315
•1. Partially compensated metabolic alkalosis.
•2. Diuretics (Hypokalemia).
316

• CSF profile: results go with viral meningitis, RBC +ve, he had one attack of convulsion.
• 1.What is the causative agent?
• 2.What is the treatment?
• 3.Is there need for anticonvulsants?
317
•1.Herpes simplex.
•2.Acyclovir.
•3.No need.
318

• A mother of 6-month old baby comes to you on summer asking about vaccinations:
• 1.Mention 3 vaccines not in JNP you can give him.
• 2.She asks about vaccine prevents gastroenteritis, do you give him?
• 3.He did not receive his BCG, do you give him now?
319

•The idea is to choose vaccines appropriate for ageand
season…
320
OSCE • 5-day old newborn with cyanosis, answer examiner questions:
• 1.What are the differential diagnosis?
• Congenital heart dis, sepsis, hypoglycemia (according to check list)
• 2.What are your investigations?
• CBC, ABG, CXR, ECG, Hyperoxiatest… (you are in ER, no echo)
• 3.ABG results were…, what is your interpretation?
• Metabolic acidosis.
• 4.CXR , cardiomegally, narrow heart base (egg on a string) what is your diagnosis?
• TGA.
• 5.It is TGA, what is your treatment?
• PGE1 (keep PDA patent).
• Balloon arterial septostomy.
• Arterial switch surgery.
321

• 15-month old boy with recurrent bruising, take relevant hx & answer the mother concerns.
• 1.Hx.
• –Duration, bleeding from other sites (nose, gum…), joint swelling, bleeding after circumcision, family hx,…
• 2.Its FVIII deficiency, what does this mean?
• 3.From where my baby got this? What is the type of inheritance? If I am totally healthy (not carrier) how did he get the disease?
• –From you, XR, mutation.
• 4.What is the chance that I will have another baby with this disease?
• –25% of all (50% of males).
• 5.What are the possible complications?
• –Hemarthrosis, intracranial hemorrhage.
• 6.What is the treatment? What can I give him at home?
• –FVIII for treatment & prophylaxis, desmopressin.
322

• 10-year old with staring & unresponsiveness:
• 1.Take relevant hx. (as examiner: only analyze his complaint, don’t look for differentials)
• –Analyze seizure as you know it, don’t forget to ask about school performance.
• 2.Perform cerebellum examination:
• –Gait, dysdiadochokinesis, nystagmus, heel shin test, heel-to-toe walking, Romberg’s test, resting tremor, finger-to-nose test, heel-to-shin test…
323

324
• Q1
• 13 y old male, he has a brother with the same condition.
• What's your diagnosis?
• Mention 2 organs you'd like to examine. 325

•(Marfansyndrome) .
•(Heart & Eye)
326
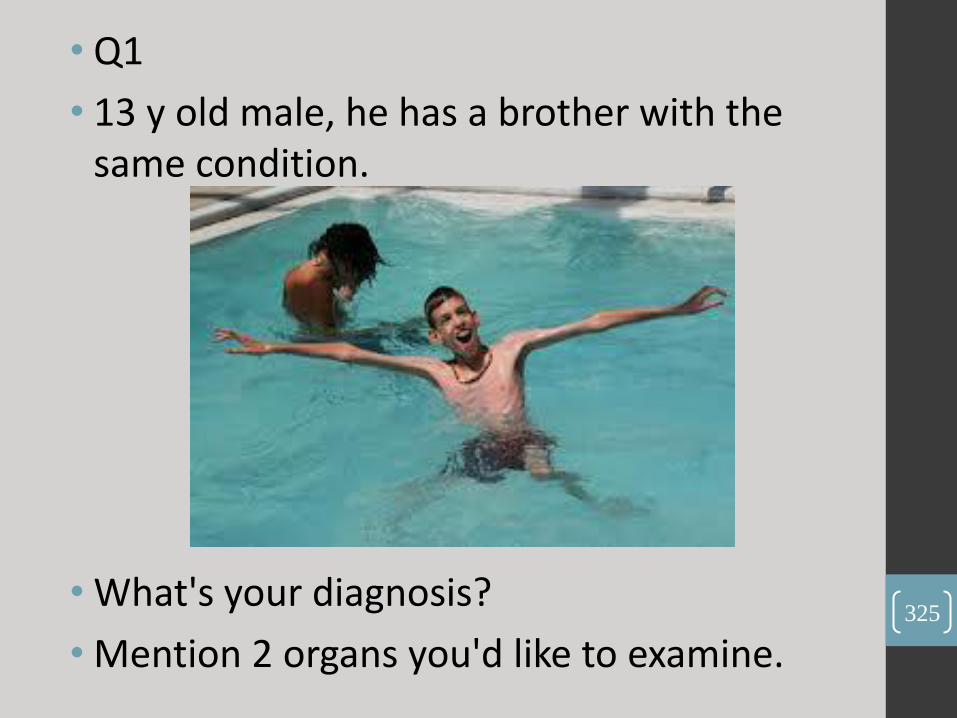
Q2 -This is skull x-ray of 10 y old male pt.
- What is this x-ray sign?
- What other 2 findings in the face you look for ?
327

- (sun ray appearance) .
- (frontal posing, protruded maxilla) .
328

Q3 13 month old has an abdominal mass.
• What's your diagnosis ?
• Mention 2 non-radiological tests for confirmation .
329

- (Neuroblastoma) .
- (VMA, bone marrow biopsy)
330
• Q4
- What's your diagnosis ? - Mention 2 things you'll hear by auscultation.
331
- ASD .
- (Ejection systolic murmur, fixed splitting S2)
332

•Mention two causes of Metabolic acidosis .
333

- chronic renal failure .
- DKA .
334

• Q6- 2 y old child previously health, developed sudden onset of shortness of breath and hypotension.
- What's the diagnosis ?
- 2 things you'll hear by auscultation.
335
•Pericardial effusion .
•(Friction rub, muffled heart sounds)
336
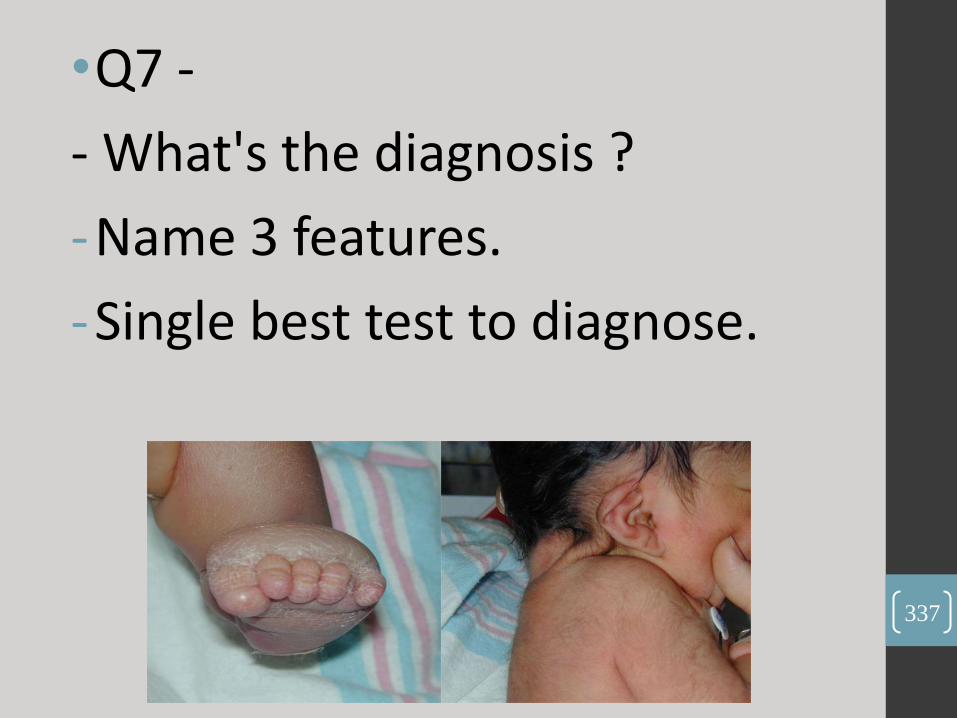
•Q7 -
- What's the diagnosis ?
-Name 3 features.
-Single best test to diagnose.
337
- Turner syndrome .
- (web neck, wide spaced nipples, lymphedemaof limbs)
- (karyotyping)
338

Q8
- What's the diagnosis ?
- 2 causes.
339

- (Congenital cataract)
- (Rubella, galactosemia)
340

• Q9
• Hx of a boy who had RTA, and he underwent craniotomy and hemi-spherectomy His urine output increased to 6 L / day. Urinalysis and electrolytes results were given showing low specific gravity, low osmolarity and hypernatremia.
• What's your dx ?
• What's the treatment of choice?
341

Diabetes Insipidus)
(Desmopressin)
342
• Q10
• long hx of a 4 year old boy who developed high fever and rash, admitted to PICU where he developed thrombocytopenia, respiratory distress and other stuff I can't remember!
• Explain what happened ?
343
Meningiococemia , leasing to respiratory distress and DIC!
344
OSCE
• 1. A case for 7 yr old female ( not sure about age ) complain from pallor since age 6 months take hx and PE exam .
• She has mild jaundice, change in the color of urine (brown) no change of stool color, mild abdominal pain, family hx of spleenectomy .
345

• A case about LOC 1 week ago for 10 years old previously healthy This is the second time, the first one was before 1 month ago, no hx of trauma or drug ingestion, it's associated with palpitation and passing urine (SVT) , not associated with chest pain SOB or cyanosis , no seizure and no frothy secretion, no family hxof CHD, you should ask about deafness
• Physical exam mainly CVS and tell the doctor the possible finding that u may find
• At the end the doctor asked me how can we monitor him 24 hours (by Holter Monitor!)
346

• 1 yr old with FTT take history and respond for mother concerns
His problem start at age of 6 yrs after introduction of food but there is no diarrhea, there was abdominal distention no vomiting, and he has pallor, family hxof celiac disease.
So the mother asked:
• What is celiac disease?
• What food I should avoid and what I can give, and for how long?
• Can I give her a piece of bread every now and then?
• Is it familial? yes
• What investigation should I do to be sure? biopsy and celiac antibodies
• What could I do to increase his weight ? (u should mention iron also because the patient has anemia )
347

1) dx
2) mode of inheritance
3) complications
348
1. achondroplasia
2. (AD)
349
• 2-chart of growth hormone deficiency (lecof short stature)
• 1)Dx
• 2)2) what was given to him to catch up?(GROWTH HORMONE)
350
3-acid base balance values (metabolic alkalosis)
• 1) dx (uncompensated metabolic alkalosis(uncompensated 3alaiha 3alameh )
• 2) 2 possible causes?(SYSTIC FIBROSIS, BARTER SYNDROME)
351
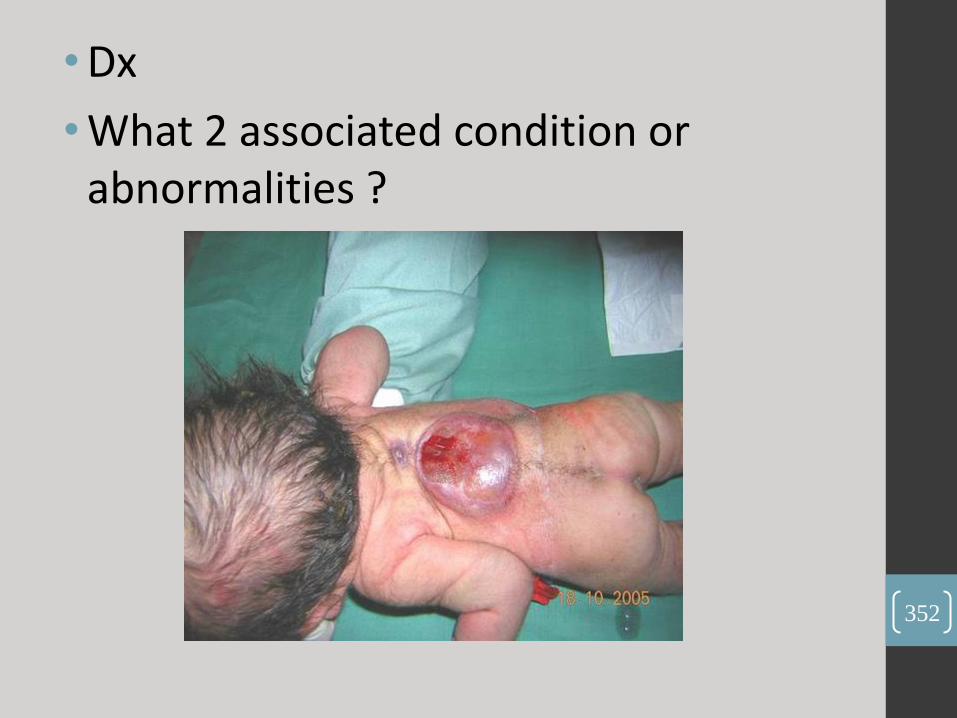
• Dx
• What 2 associated condition or abnormalities ?
352

• myelomeningocele .
• arnold chiari, renal abnormalities)
353
•5- a case of seizure with lab values has hypocalcemia
•1) dx .
•2) next step lab test u want to do .
354
•(Hypoparathyroidism)
•(Parathormone Level)
355

Q6 : 13 Year old boy came with is pic. :
1) dx :
2) 2 possible causes :
356

1.Erythema Nodosum
2.TB , Strep , Sarcoidosis
357

• 7- an ECG with HR=180
1) Dx :
2) 2 drugs for treatment .
358

1. (Ventricular Tachycardia)
2. (Lignocaine, Amiodarone)
359

•1. What Your notes on palpation , percussion, and auscultation
•2. next step of treatment .
360
- This case for left Pleural effusion .
• palpation : reduced expansion on left side .
• percussion : stony dull .
• auscultation : diminished vesicular breathing on left side .
•2. (chest tube)
361
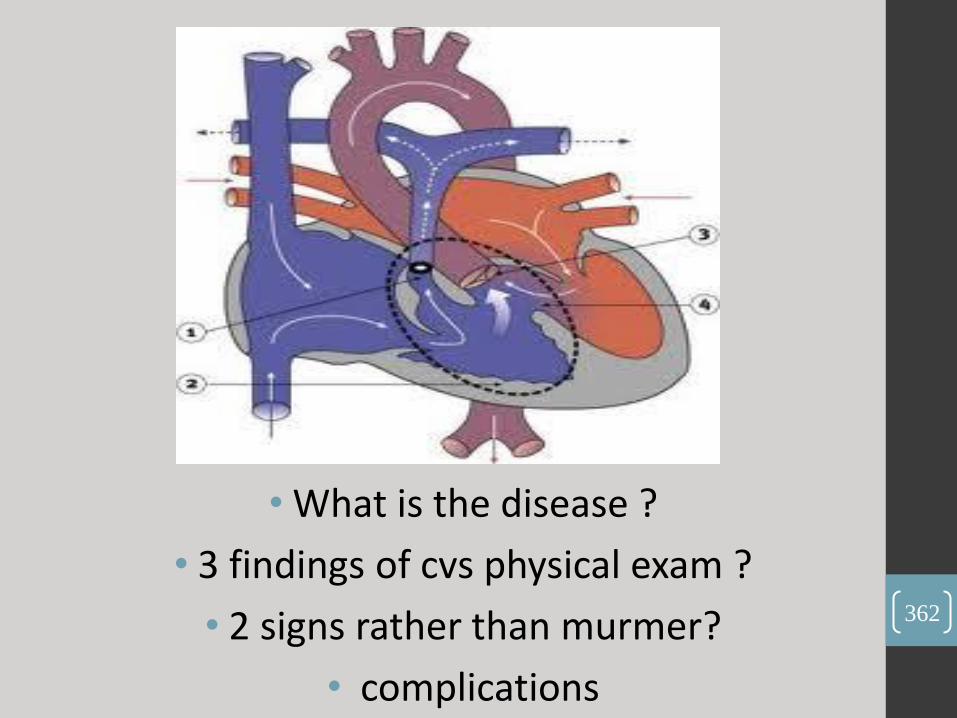
• What is the disease ?
• 3 findings of cvs physical exam ?
• 2 signs rather than murmer?
• complications
362

1.TOF
2.Ejection systolic murmur, thrills, single S2, cyanosis .
3.(clubbing, FTT).
363
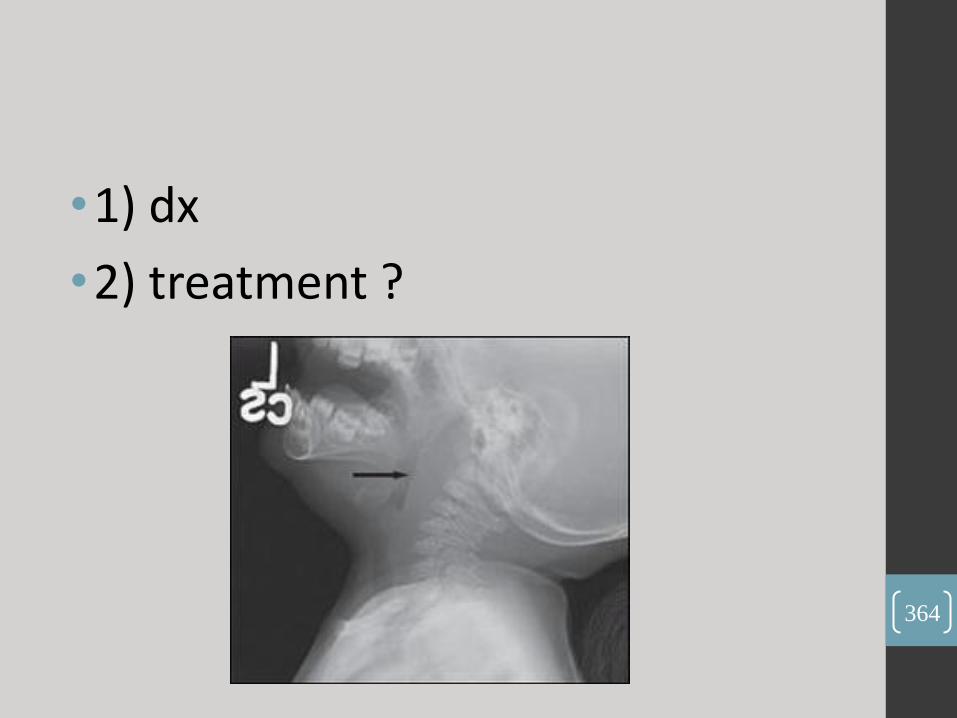
•1) dx
•2) treatment ?
364
•retropharyngeal abscess
•(IV antibiotics and drainage)
365
OSCE :
•1-A case of ITP history and exama 5 yr old boy presented with easy brusibilityand rash(note: dontforget to examine the mouth for bleeding gum and ask about abdominal pain and joint pain )
366
• 2-A case of meningitis history and exam andCSF results with the ddxan 8 yr old boy presented with headache 5 hours ago take hxand do exam , 1stly analysethe headache as usual and ask about associated symptoms : he had projectile vomiting and photophobia and decease activity etc .... on exam he had neck rigidity. the drasked what ddxfor neck rigidity ??? (retropharyngeal abscess, apical pneumonia), the he gave us CSF results which indicates viral meningitis or partially treated meningitis .
367

• 3-A case of DOWN syndrome and questions about the problems he could have in the systems , what type of abnormality (non-dysjunction) , causes of death ?and why ? avgage of death ? yearly based test u do it (hearing assessment ) .
368
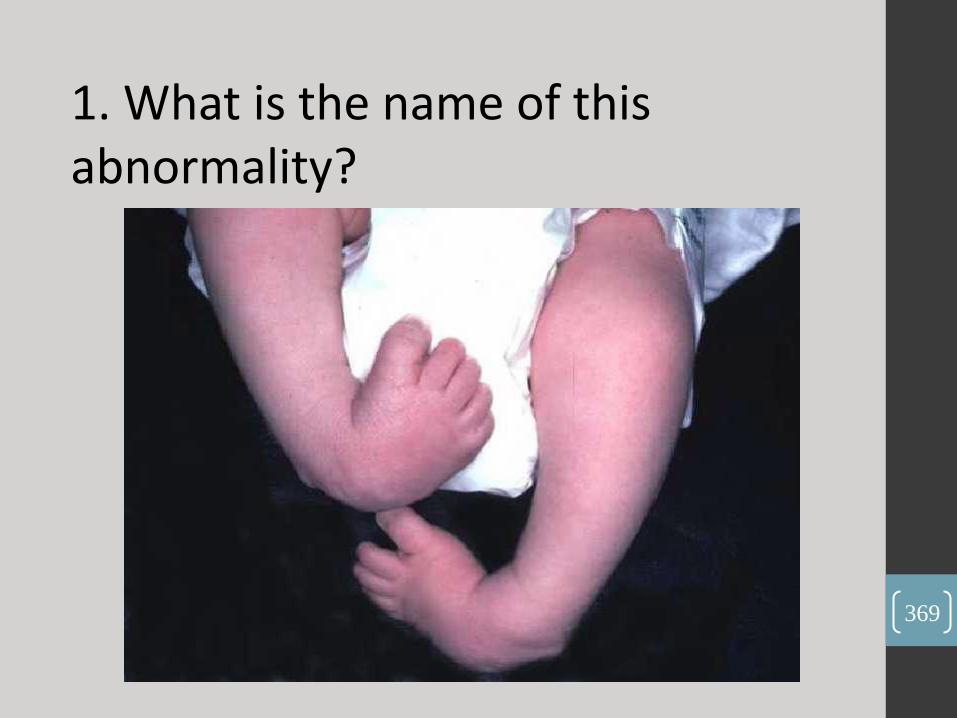
1. What is the name of this abnormality?
369

(Bilateral club foot
370
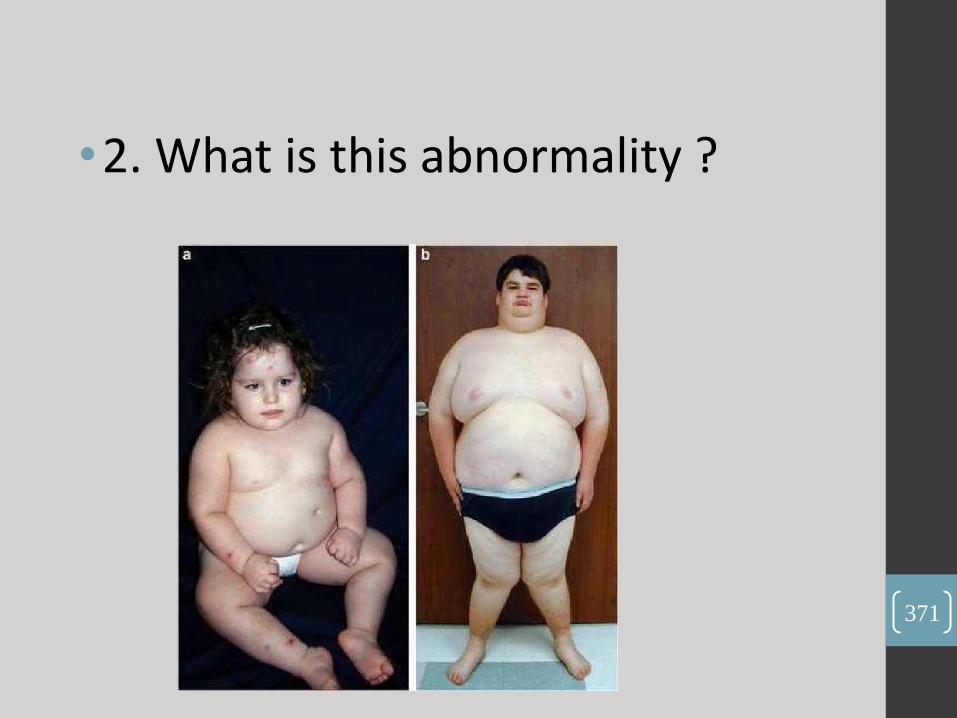
•2. What is this abnormality ?
371

(Prader willi syndrome)
372
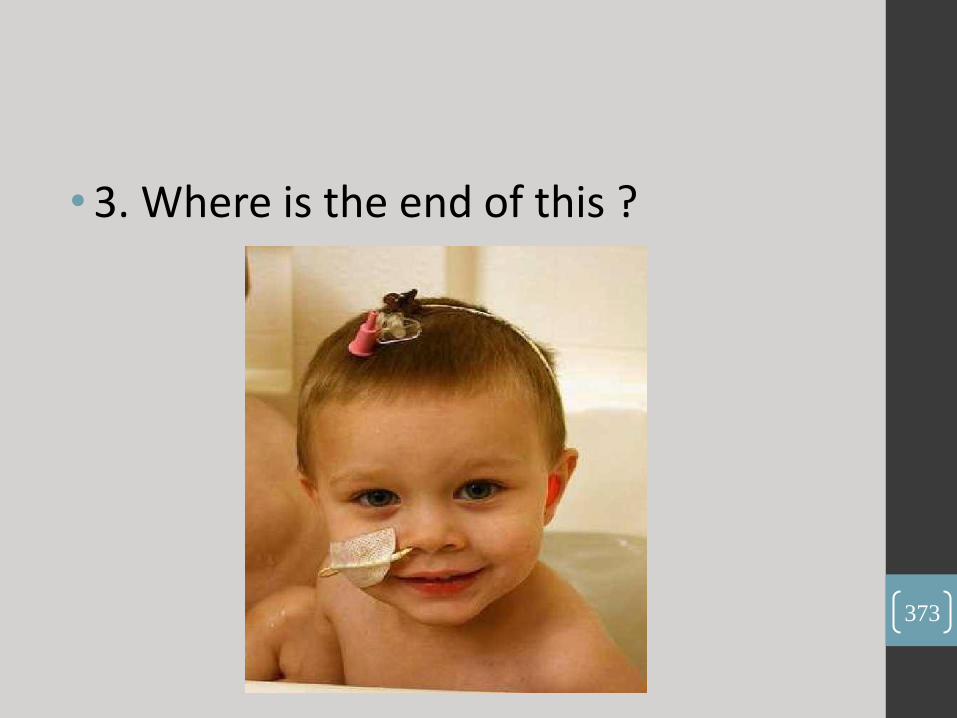
• 3. Where is the end of this ?
373

(Stomach)
374

4. The Question starts with history and some findings related to this picture, So
what is the type of this anemia?
375

(Sickle cell anemia)
376

•5. in this figure, these Numbers
Indicated What?
377
• 99 : O2 saturation
• 82 : Pulse Rate
378

• 6. Look to This Picture, & Answer the following Questions:
• A. What is this this type of treatment ?
• B. What is the mechanism of action in the body ?
379

• Phototherapy .
• Isomiration of bilirubin to luminrubin to excrete it out the
body in Urine.
380

• 7. In this patient, mention 22 abnormalities you find in his hand ?
381
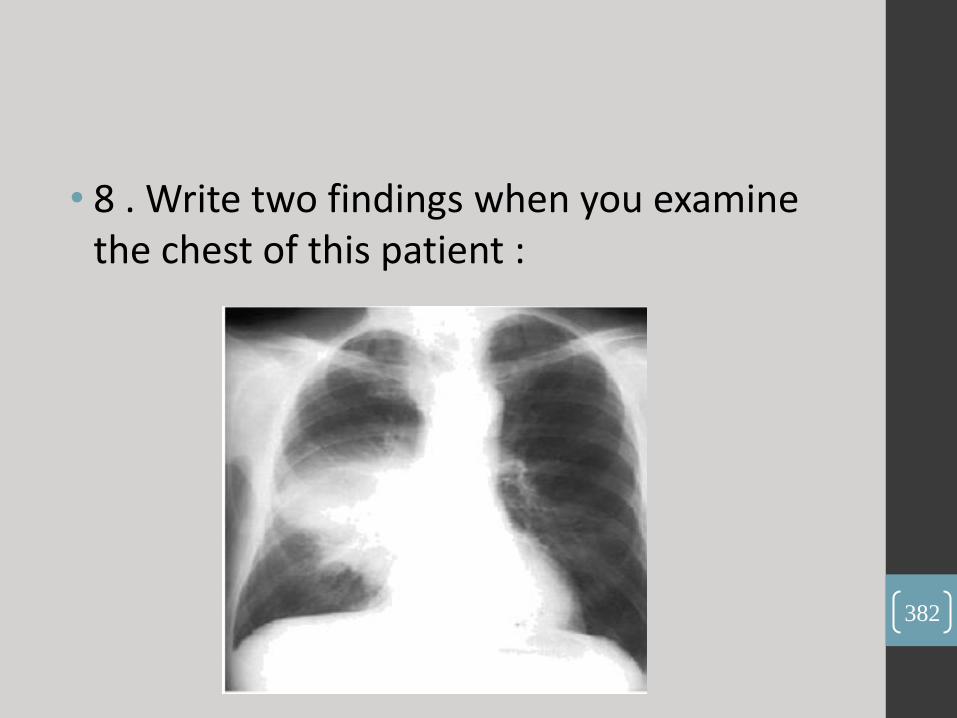
• 8 . Write two findings when you examine the chest of this patient :
382

1. Decrease air entry
2. Dulness in percussion
383
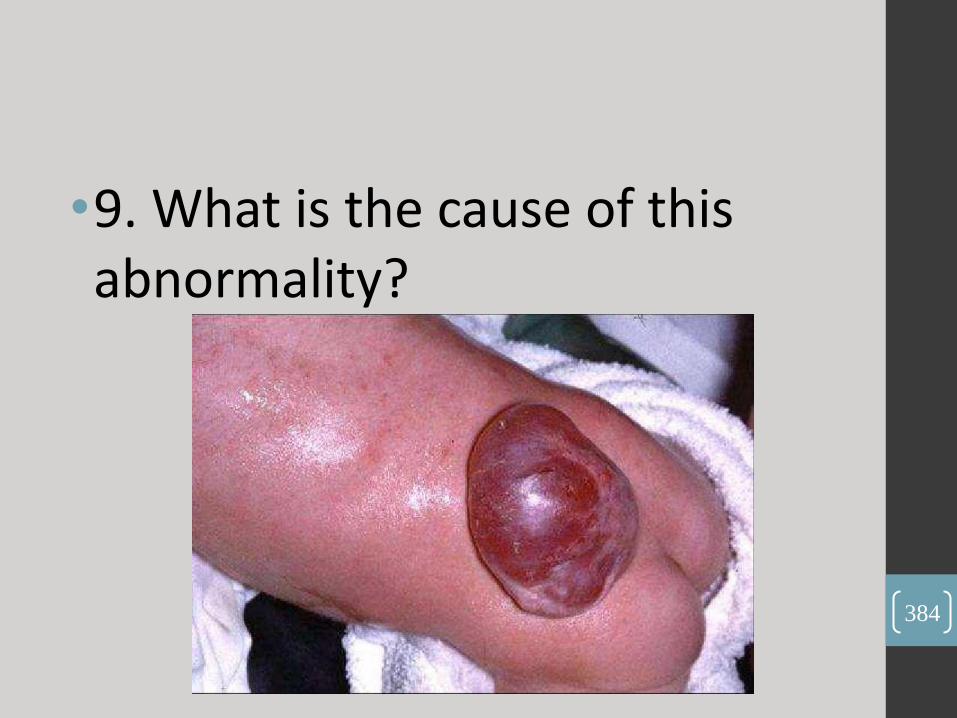
•9. What is the cause of this abnormality?
384

•Meningomylocele caused by
hdrocephelus craini.
385
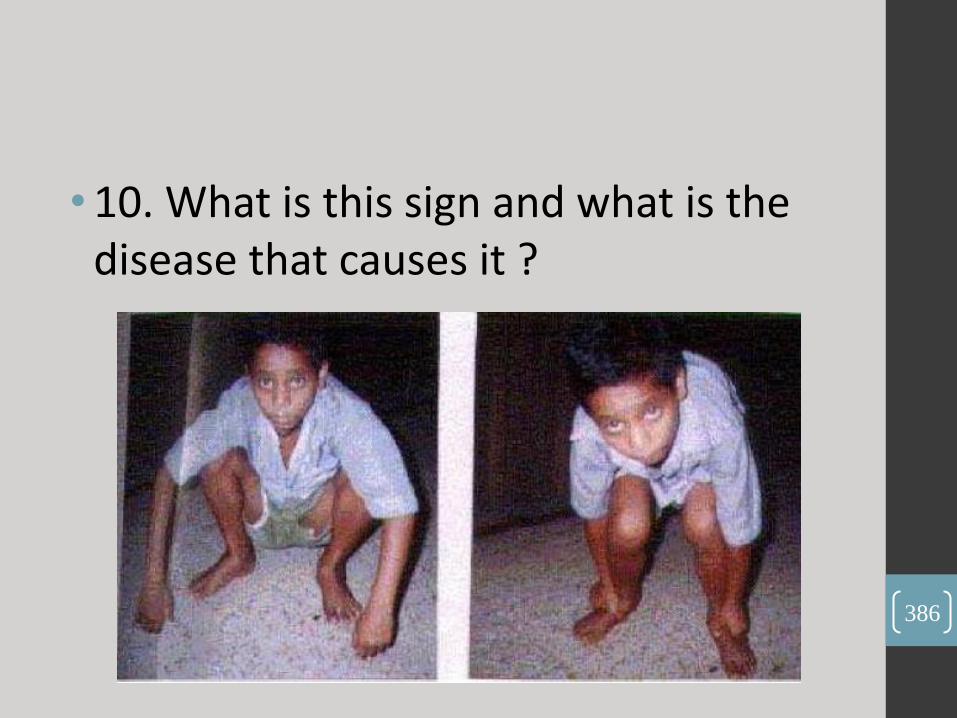
• 10. What is this sign and what is the disease that causes it ?
386

•1.Gower sign.
•2.Proximal muscle wasting.
387

• 11. in this picture :
• A) Name the sign observed at the eyes?
• B) What is the most serious complication?
• (Inflammation of coronary arteries) . 388
•(Non suppurative conjunctivitis).
•(Inflammation of coronary arteries) .
389
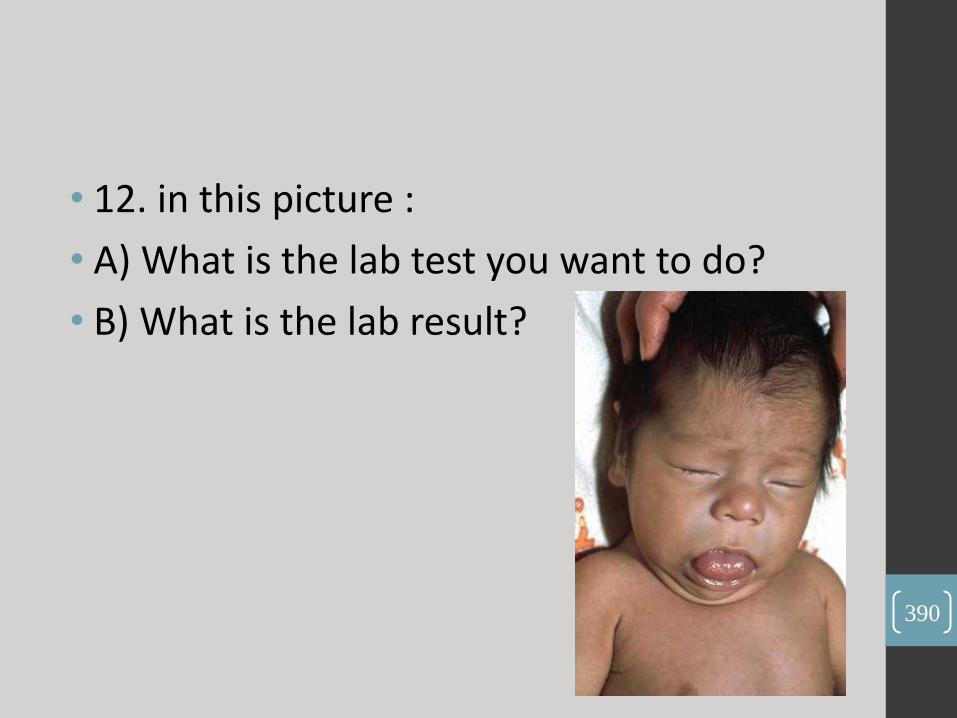
• 12. in this picture :
• A) What is the lab test you want to do?
• B) What is the lab result?
390
- (serum T 3,T4, TSH) .
- TSH and low T3 & T4 .
391
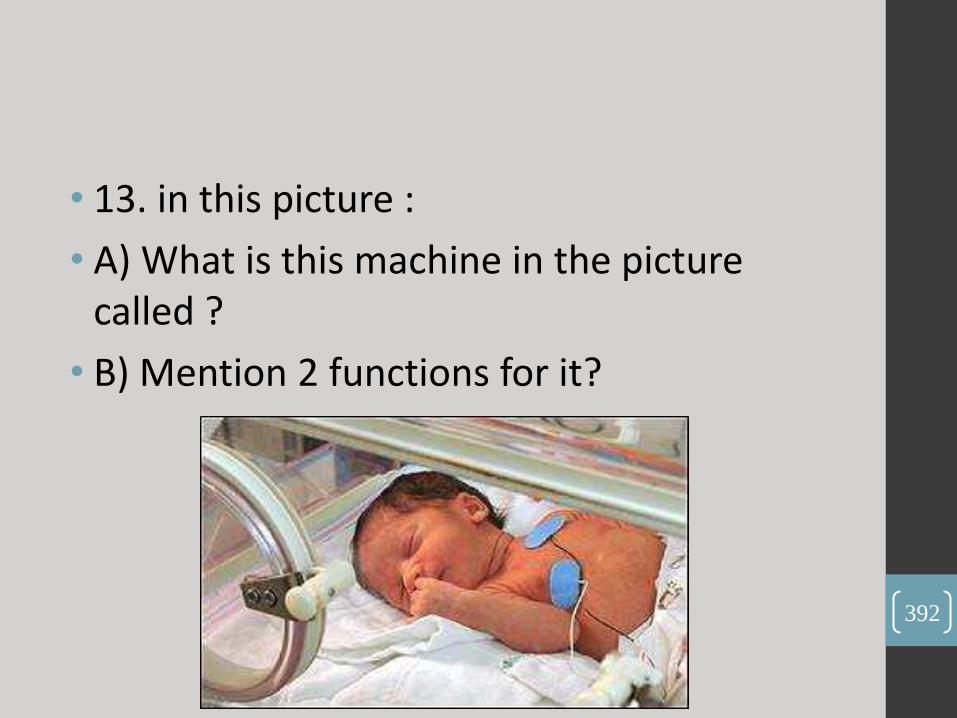
• 13. in this picture :
• A) What is this machine in the picture called ?
• B) Mention 2 functions for it?
392

A.
(incubator).
B.
- thermoregulation .
- isolation from infections).
393

• 14. in this picture :
• A) What is the name of this test ?
• B) What does it test for ?
394
• (Distraction test).
• (auditory function, hearing , cochlear branch of
vestibulocochlear nerve).
395
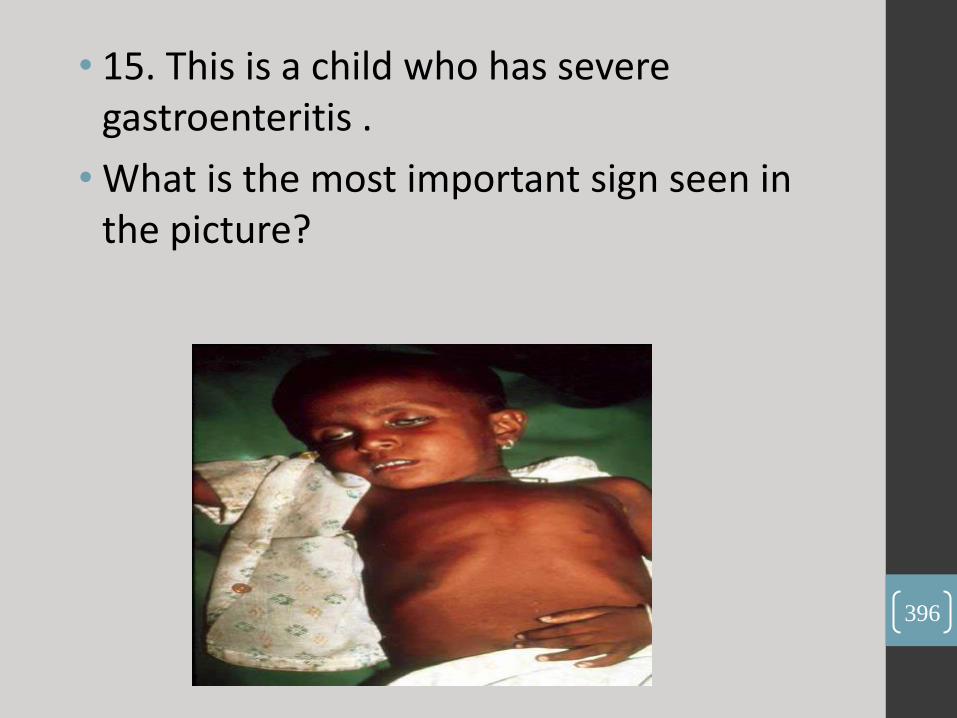
• 15. This is a child who has severe gastroenteritis .
• What is the most important sign seen in the picture?
396
(sunken eyes).
397

•16. This is a 32-week old infant's X-ray :
• What's is the finding in this X-ray ?
398
(ground glass appearance).
399
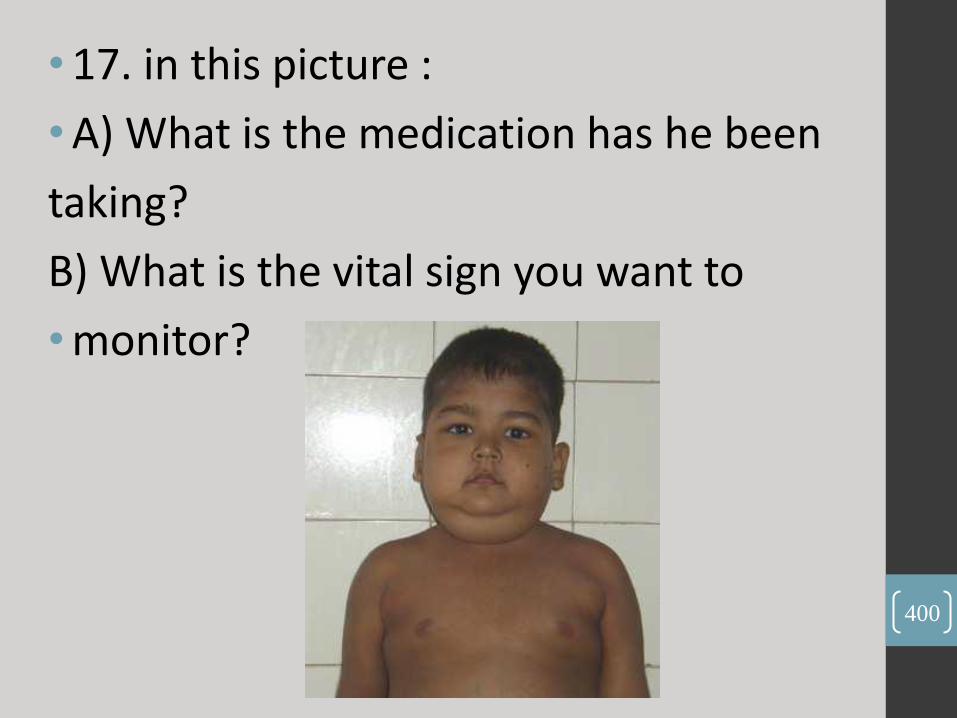
• 17. in this picture :
• A) What is the medication has he been
taking?
B) What is the vital sign you want to
• monitor?
400

•(corticosteroids).
•(blood pressure).
401
18 . Mention 2 of the WHO recommendations
to promote breastfeeding?
402

• 1. Initiation of breastfeeding within the first hour of life .
• 2. Exclusive breastfeeding – that is the infant only receives . breast milk without any additional food or drink, not even water .
• 3. Breastfeeding on demand – that is as often as the child wants, day and night .
• 4. No use of bottles, teats or pacifiers .
• * this answer from WHO website . 403

• 19. In this picture:
• A) What is the sign you can see?
• B) Mention 2 diseases can cause it?
404
•(hand clubbing).
•(cystic fibrosis, infective endocarditis)
405

• 20 . At any age the baby can do this :
406
(mature pincer's grasp at 12 months old).
407

إن حفاظ المرأة على حجابها الشرعي
وفي أحيان أخرى على اللباس الذي
يتماشى من البيئة المحافظة التي يعيش
فيها مجتمعنا الأردني ، يدل على رقي
الفكر والأداء لأنه لا يبتعد عن زخم .المحيط الذي نعيش فيه

Q1 : Turner Syndrome
• Mention 3 signs u can see ?
• Single best test to diagnose ?
409

• 1- webbed neck
2- wide spaced nipples
3- low hair line
4- lymphedema of the limbs
• Karyotyping
410

Q2 :
• What is the type of inheritance ?
• Mention one example ??
411
• X-linked dominant
• Fragile x syndrome, alport disease , rett syndrome
412
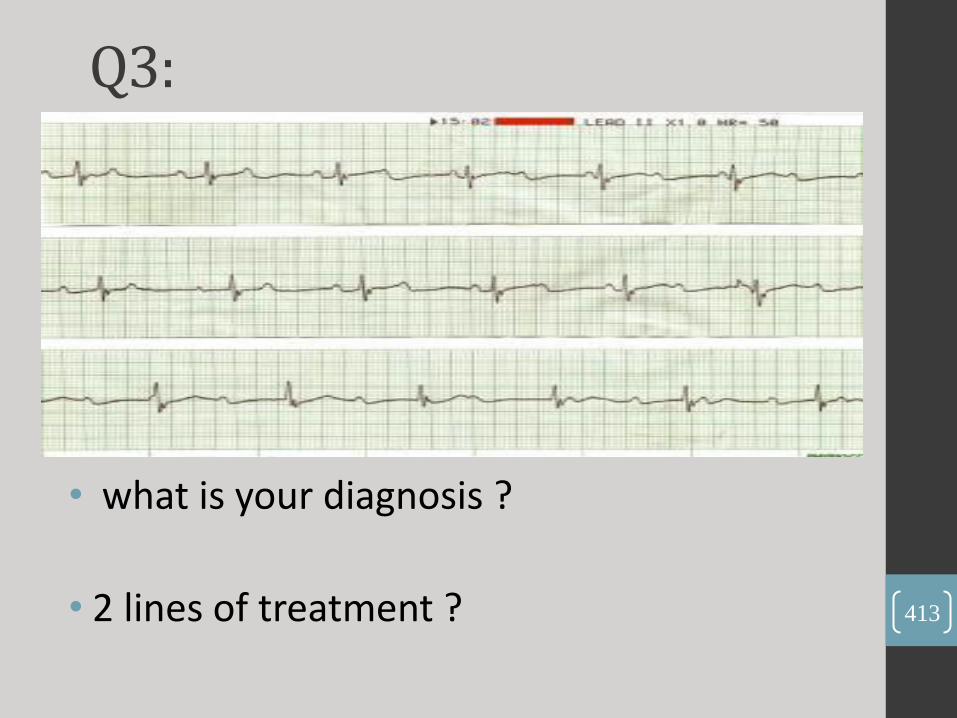
Q3:
• what is your diagnosis ?
• 2 lines of treatment ?
413

1. Cong. Comp. Heart block .
2. Corticosteroids (Dexamethasone) , Immune
globulin intravenous . Not sure
414

Q4 : 1 y old child previously health,
developed sudden onset of shortness of breath and hypotension
•What's the diagnosis?
• 2 things you'll hear by auscultation ?
415
1. Pericardial effusion
2. 1. Friction rub
2. muffled heart sounds
416
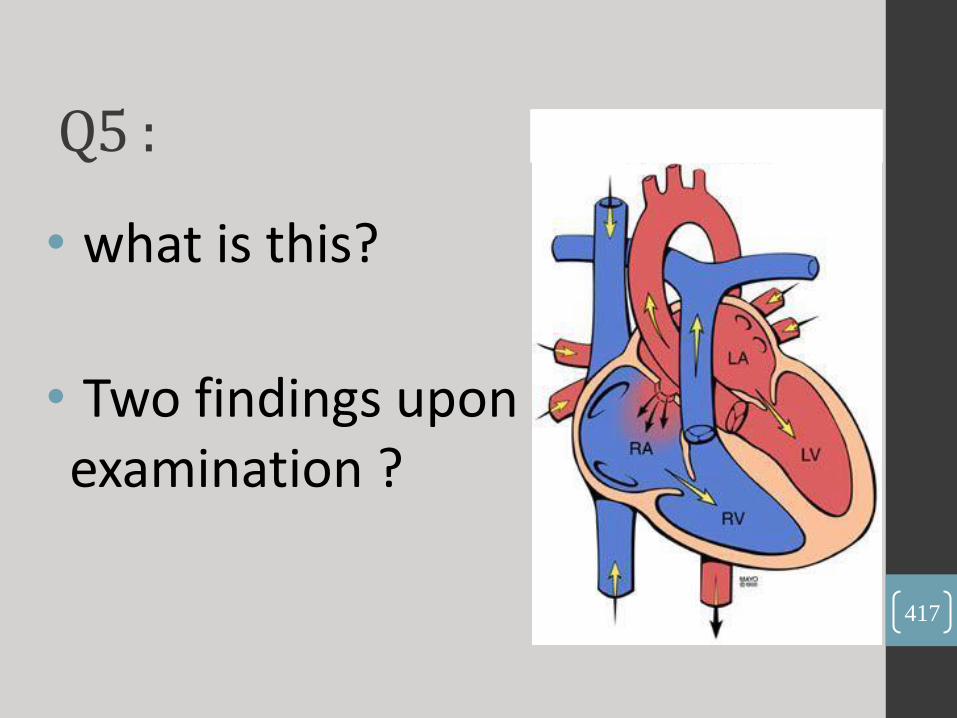
Q5 :
• what is this?
• Two findings upon examination ?
417
1. ASD
2.
1. Systolic murmer
2. Fixed splitted S2
418

• What is your diagnosis ?
• Give 2 radiological signs you can find ?
Q6 :
419

• Ricket’s
• 1- cupping of distal head of ulna
2- Widening of epiphyseal plate
3- the shafts of the long bones become osteopenic and cortices become thin
4- deformities of the shafts of the long bones are present
5- Bowing of long bones +- pathological fx
420

•What is Your diagnose ?
•What is Your Treatment ?
Q7 :
421
• Impetigo .
• antiseptic gentian violet & topical or oral antibiotics .
422

PH: 7.22 , PaCO2 : 60mmHg , HCO3- : 12 mEq /L, Base excess: 2 mEq/L.
• What is the abnormality?
• Give 3 causes ?
Q8 :
423

What are the reflexes and what is the estimated age ?
Q9 :
424

1. pulled to sit without head lag at age (3-4) months .
2. The walking or stepping reflex is present at birth; and disappears at six weeks .
425
• What is abnormal in one d/o neonate … mention 5 from the list
• Hb=12(low) ,, WBC= 8 ,, HC=35 ,, glucose= 3 mmol/l , subconjuctival hrg (ab) ,, cephalohematoma(ab) ,, 2
veins 1 artery ( abn),, epestein pearls (ab) ..
Ab= abnormal
Q10:
426

•Station 1 • Case 1 (Acute Exacerbation of Asthma)
9 years old male presented with cough for 3 days ( he was on inhaler since the age of 4 yrs ). Take a hx
• Hx --> hx of recurrent cough since a long time ago. occur at night, no sputum, no cyanosis. there was audible wheeze. took regular nebulizer. normal growth (weight and height). no fever, no change in bowel habit. past medical history of atopic eczema, family history positive with asthma. No hx of contact with patients with respiratory infection. No pets or trees around . The father is smoker
OSCE
427
Station (2) • Do physical examination for the prev. case
(asthma)
• Physical --> general, signs of respiratory distress and complete chest examination. (( never forget clubbing))
• i. What is your diagnosis?
• ii. How do you work up this case?
• iii. What are the line of treatments in this case.
• vi. If you want to discharge this patient, what advices you want to give to the parents.
428
Station (3)
• 4 yo boy presented to ur clinic by his mother with multiple bruises on lower limbs and his elbow
1- What are the question you would like to ask in the history ? Most important the he has recent viral infection
2- What are the signs that you would like to examine here ?
3- What is you DDx ? And what is the most likely Dx ?
4- What tests you would like to order ?
5- If the plt count was 5000 what is your next step ?
6- Explain how does the IV Ig works
7- If Iv ig didn't work what you will do ? Steroid
8- What is the test that you shloud do b4 giving steroids and why ? BM biopsy to exclude malignancy
9- If all of those doesn't work what is the final way ? Splenectomy 429

430

Q1: These are the CSF results for a 5-day old neonate who complained of vomiting
• WBC: 155/μL
• RBC: 0/ μL
• Protein: 80 mg/dL
• Lymphocytes: 30%
What is the diagnosis?
Mention the most specific treatment.
• CSF glucose: 2 mmol/L
• Serum Glucose: 5 mmol/L
• Neutrophils: 70%
431

• Acute bacterial meningitis
• Ampicillin + a 3rd generation cephalosporin
432

Q2: This is a cartoon drawing for the heart of a 1-day old neonate. He was cyanosed, with an O2sat=75% and PaO2 = 85 mmHg
• What is the Chest X-Ray finding
•What is the cause of his cyanosis 433

•Egg-on-string
•Two parallel circuits
434
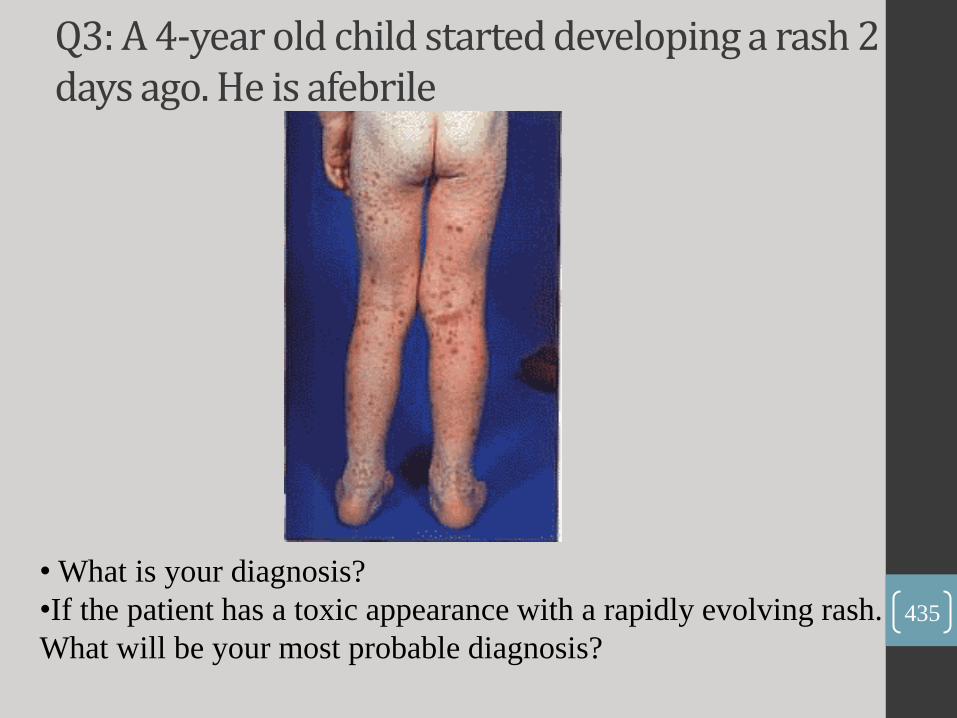
Q3: A 4-year old child started developing a rash 2 days ago. He is afebrile
• What is your diagnosis?
•If the patient has a toxic appearance with a rapidly evolving rash.
What will be your most probable diagnosis? 435

•Henoch-schonlein purpura
•Acute meningococcemia
436
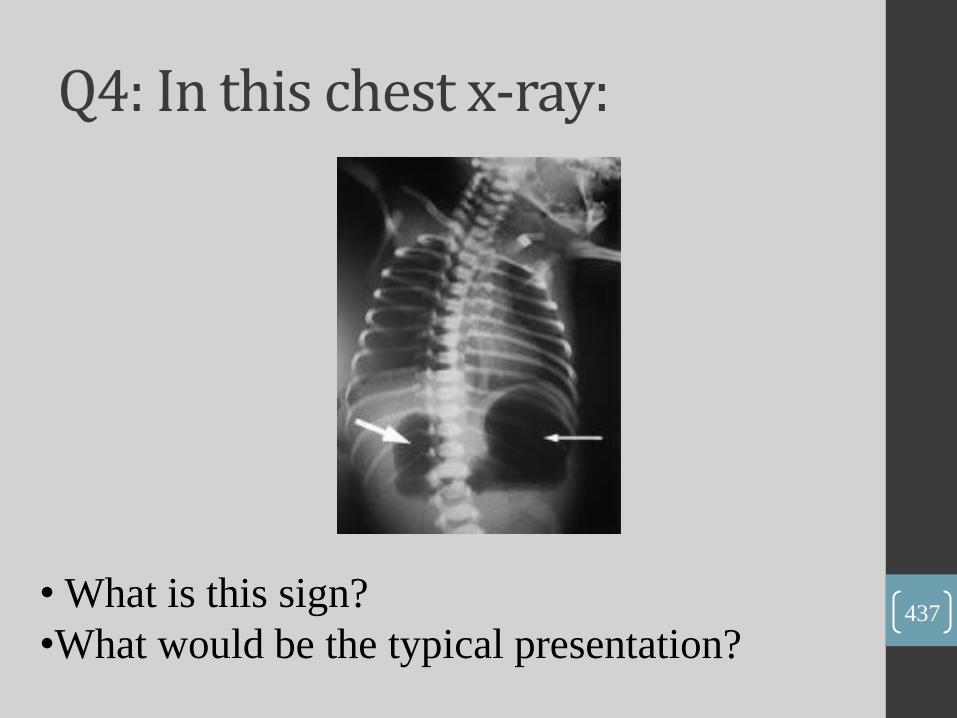
Q4: In this chest x-ray:
• What is this sign?
•What would be the typical presentation? 437

•Double-bubble sign
•Bilious vomiting after the first feed
438
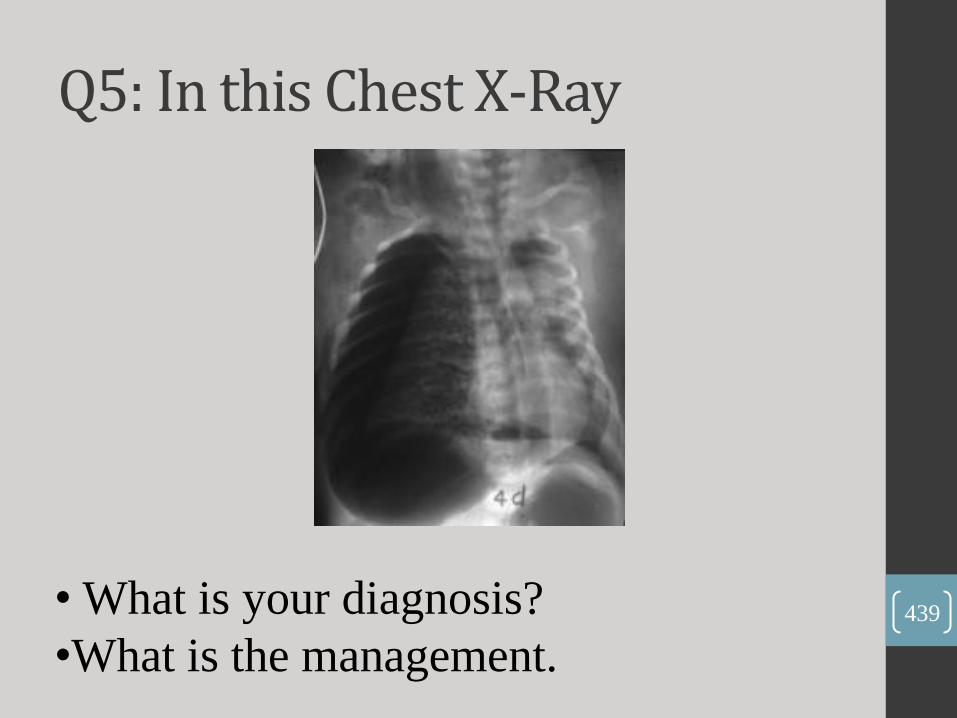
Q5: In this Chest X-Ray
• What is your diagnosis?
•What is the management. 439

• Right-sided tension pneumothorax
• Thoracocentesis then insert a chest tube
440

Q6: An ABG was done for a child, and the results were the following
•PH: 7.22, PaCO2: 60mmHg, HCO3-: 27 mEq/L, Base excess: 2 mEq/L.
How do you read this ABG?
Mention one possible cause for that.
441
• Partially-compensated respiratory acidosis
• Any cause of reduced ventilation(GBS, narcotic overdose, MG,…)
442
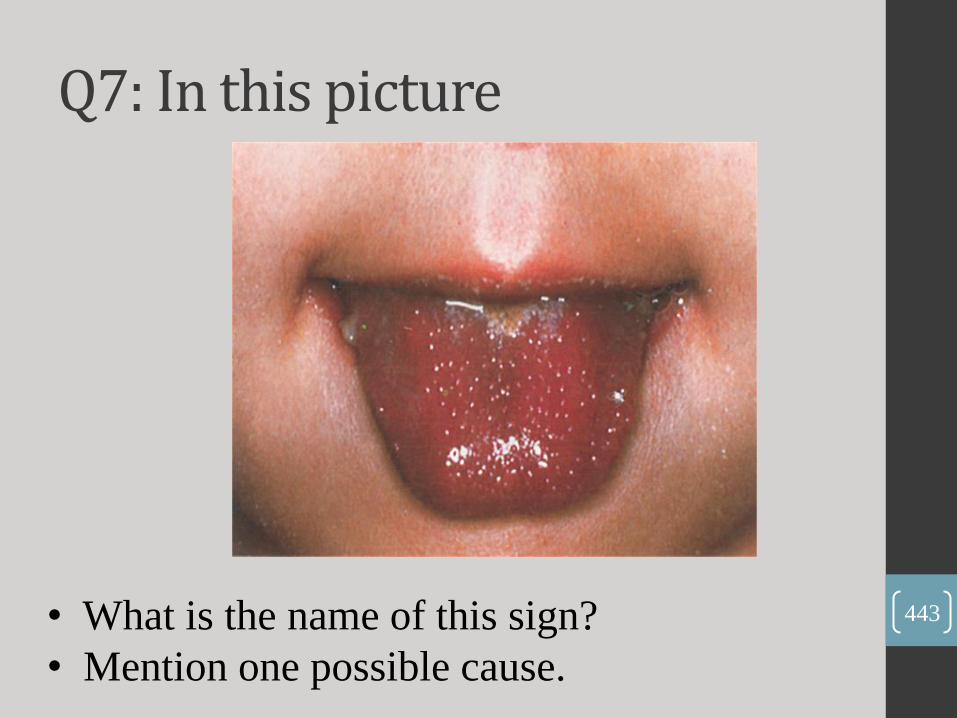
Q7: In this picture
• What is the name of this sign?
• Mention one possible cause.
443
•Strawberry tongue
•Kawasaki disease, Scarlet fever, …
444

Q8: In this picture:
• What is the name of this sign?
445
•Slapped cheek .
446

Q9: In this picture:
• What is your diagnosis?
• Mention two signs.
447
• Hydrocephalus
• A-Increased head circumference
B- Bulging anterior fontanelle
448
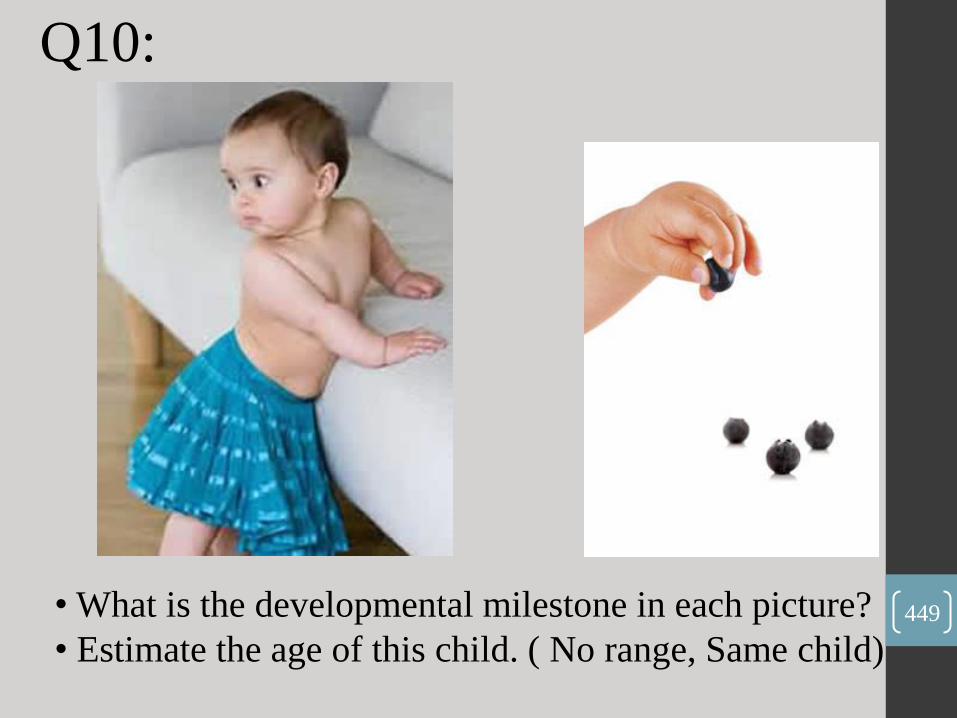
• What is the developmental milestone in each picture?
• Estimate the age of this child. ( No range, Same child)
Q10:
449
• A- Cruising B- Mature pincer grasp
• B- 10 months
450

osce Station one: • A mother of an 11-month old child is
complaining that her infant is not gaining weight appropriately. Take history!
you have to rule out cystic fibrosis and celiac disease, then take detailed nutritional, family and social history. The cause in this case was nutritional. 451

Station two:
• Do CVS exam.
• Do cerebellar exam.
-dysarthria -Finger-to-nose test - heel-shin - Hand rapid alternating movements - Romberg test (ask the patient to stand and close his eyes) - Asses the gait + Tandem gait - Nystagmus
452
Station three (management and
discussion)
• Q1: A patient presented to you with jaundice and abdominal pain, what do u think about ? - Hepatitis, Cholecystitis, Gallbladder stones, Hemolytic anemias …
• Q2: What investigations do u want to do to confirm your diagnosis? - Total serum bilirubin and conjugated. - Hepatitis titers - Liver function test - PT and PTT (PT is the most indicative of liver function) - Abdominal US - For hemolytic anemias: Hemoglobin electrophoresis, LDH, Haptoglobin, G6PD enzyme, osmotic fragility … 453
• Q3: If the diagnosis is hepatitis, what are you going to see in the results of the investigations: - Very high liver enzymes - Hepatitis titers (you will be asked to describe them in details): Hepatitis A: Acute : IgM Hepatitis B: current infection: HBsAg, HBeAg (infectiviy). Previous infection : HBsAb and HBcAb. Immunized: HBsAb Hepatitis C: Acute : IgM, Chronic: IgG
454

• If the diagnosis is Hepatitis A, how do u manage this case? - Rehydration and bed rest
• Are you going to admit this patient ? - Indications of admission: Coagulopathy, Encephalopathy, Dehydration.
• If you admit the patient, does he need any type of precautions ? - Yes, Contact precautions.
• If you send the patient home, What are you going to advice the parents: - (give advice about contact with his brothers and sisters) - Come back if he developed any signs of fulminant hepatitis (encephalopathy or coagulopathy …. )
• Are you going to allow him to go to school? - No, He can go after one week from the beginning of the jaundice 455

• How are you going to diagnose fulminant hepatitis?
• How are you going to treat fulminant hepatitis? - Vitamin K and Lactulose
• Why do we give lactulose? - To help in drawing out ammonia from the body .
456

1- What is the mode of inheritance in this
pedigree
2- Give two examples 457

- (Autosomal dominant) .
- Huntington'disease and neurofibromatosis-1
458

Hx suggestive low MCV, low MCH, low
retics, low platelets
1- What is the type of this anemia
2- What 2 investigations you want to order 459

- Microcytic Hypochromic .
- Hemoglobin Electrophoresis Ferritin Level.
460
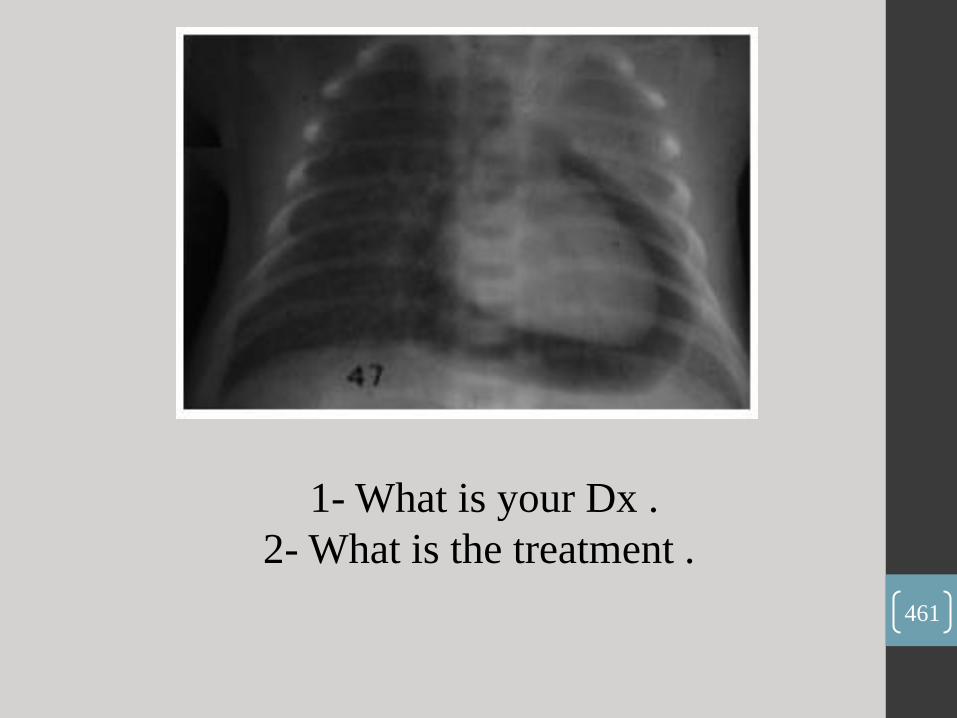
1- What is your Dx .
2- What is the treatment .
461

Answer:
1. Pneumopericardium
2. Pericardiocentesis
462

Hx about a child
who came with
acute stridor..
Neck X-Ray
1- What is the
name of this sign
2- What is your
diagnosis
463

• ………..
•retropharyngeal abscess
464
•A child that presented with abdominal pain, and vomiting, ABGs: low pH, low HCO3, low CO2, base deficit -30.. (picture of DKA)
1- What is the metabolic finding?
2- Explain this finding 465
• uncompensated metabolic acidosis
466
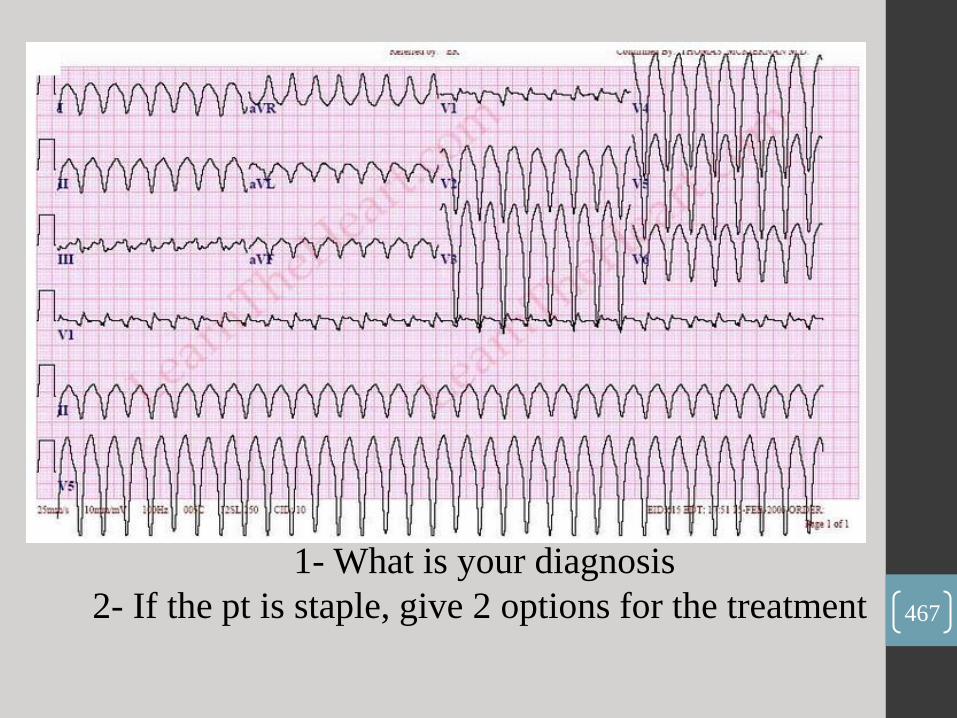
1- What is your diagnosis
2- If the pt is staple, give 2 options for the treatment 467
1. Ventricular Tachycardia
2. Synchronized Electrical Cardioversion , Defibrillation ,
Cardiac ablation , Antiarrhythmic drug therapy
( amiodarone or procainamide )
468

Hx of a pt with lymphoma who was given chemotherapy
then came with this ECG
1- What is your dx ?
2- What is the cause ? 469

• Hyperkalemia
• Tumor lysis syndrome
470

Hx about 3 months old baby that had a hx of
rhinorrhea for 3 days.
1- What is your diagnosis?
2- What is the causative virus? 471
•Herpetic whitlow .
•Herpes simplex virus (HSV) .
472

1- Give two physical findings
2- What is the definitive diagnosis 473
- (web neck, wide spaced nipples, lymphedemaof limbs)
- Turner syndrome .
474
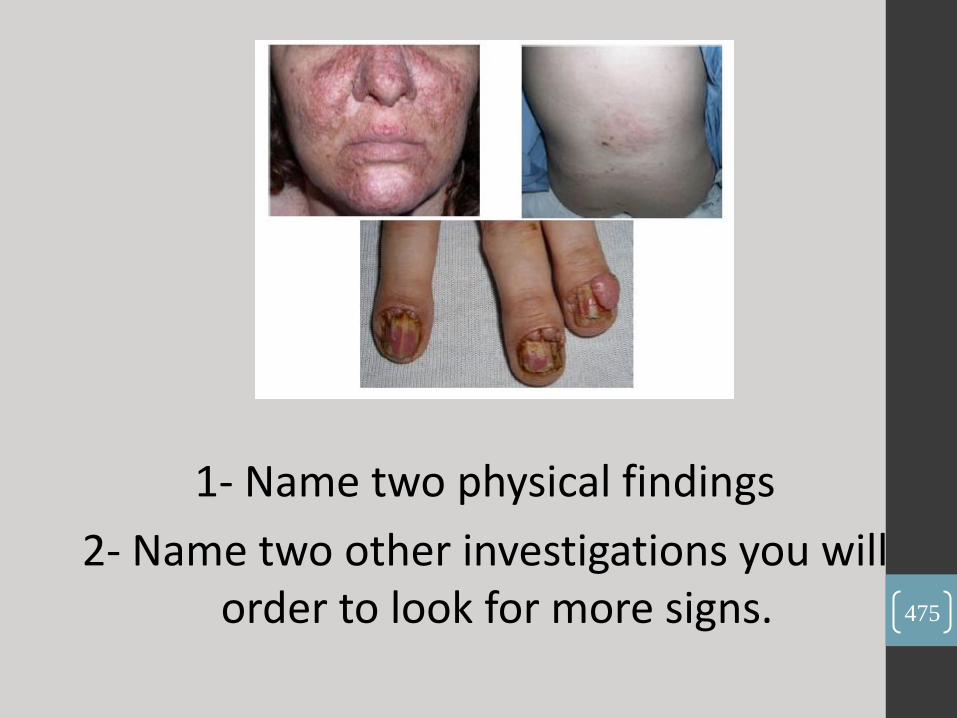
1- Name two physical findings
2- Name two other investigations you will order to look for more signs.
475
1. Shagreen patch, ungual fibromas, adenoma sebaceum.
2. Brain MRI , kidney CT .
476

1- What is your
diagnosis .
2- Mention two
findings in the
CXR
477

•congenital diaphragmatic hernia .
• Gas at left side , trachea deviation to the right .
478

Hx about asymptomatic child with this congenital
heart lesion
1- What is your diagnosis
2- Name two findings on the physical examination 479
- ASD .
- 1. Systolic murmer 2. Fixed splitted S2 .
480
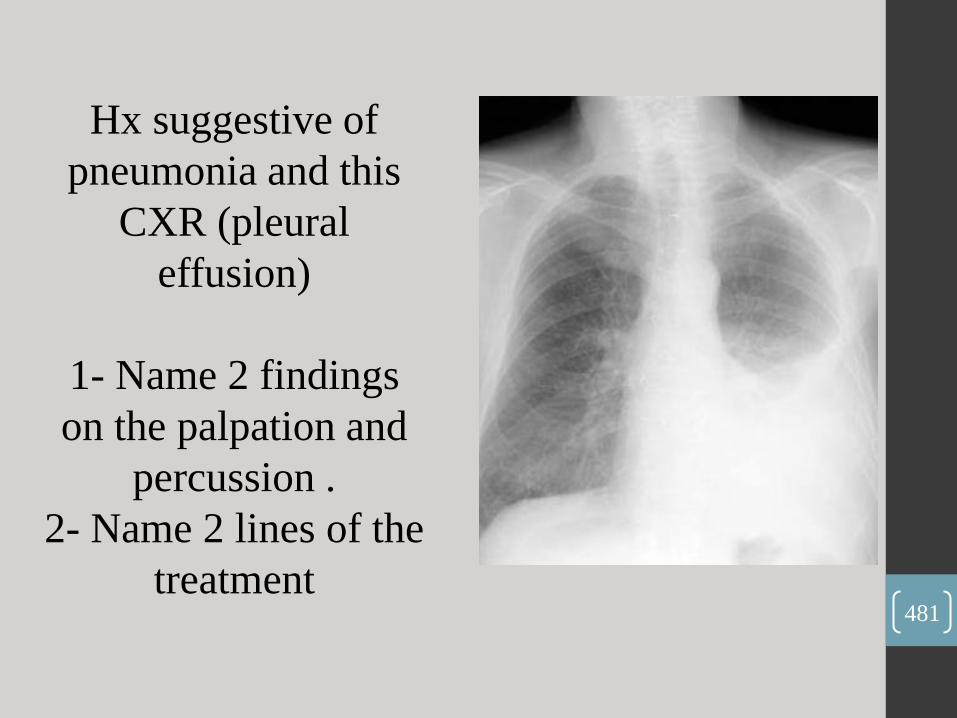
Hx suggestive of
pneumonia and this
CXR (pleural
effusion)
1- Name 2 findings
on the palpation and
percussion .
2- Name 2 lines of the
treatment 481
- This case for left Pleural effusion .
• palpation : reduced expansion on left side .
• percussion : stony dull .
• auscultation : diminished vesicular breathing on left side .
• 2. chest tube , Antibiotic .
482

Hx of a boy who had
a hx of URTI, then
developed bilateral
nodular lesions on
his lower limbs.
1- What is your
diagnosis
2- Name two micro-
organisms associated
with this disease. 483
1. erythema nodosum .
2. Tb , Strep .
484

• Hx of a boy who had RTA, and he underwent craniotomy and hemispherectomy! His urine output increased to 6 L / day. Urinalysis and electrolytes results were given showing low specific gravity, low osmolarityand hypernatremia.
1- What's your dx?
2- What's the treatment of choice?
485

(Diabetes Insipidus)
(Desmopressin)
486

Q1. what is the most prominent feature in this child ?
487
•A: muscle wasting.
488
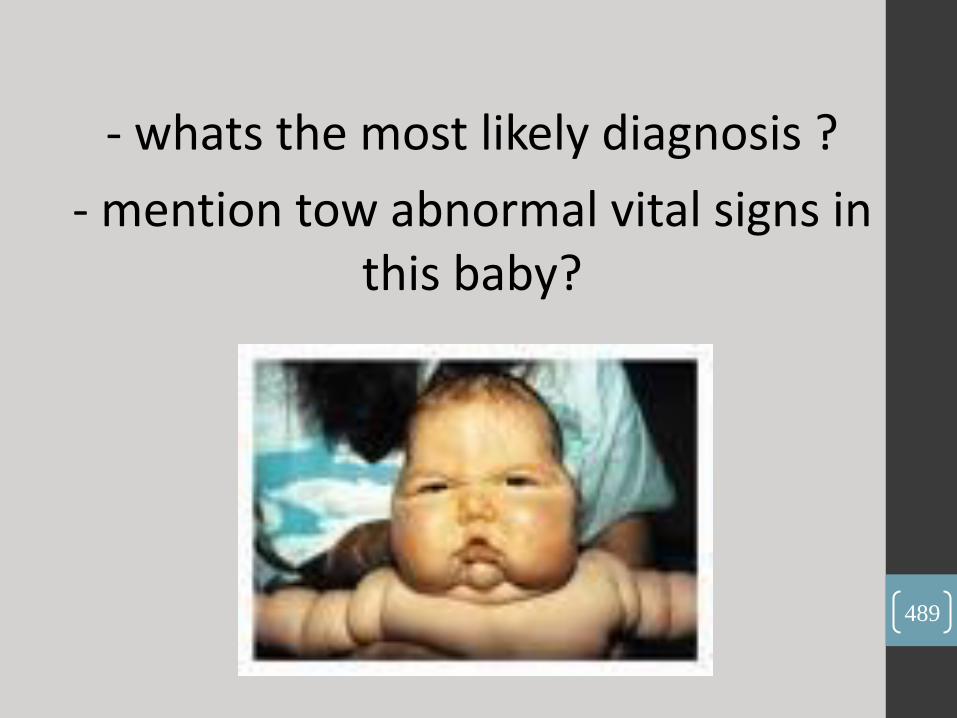
- whats the most likely diagnosis ?
- mention tow abnormal vital signs in this baby?
489

- cushing syndrome.
- high body temperature, high blood pressure, high
heart rate.
490
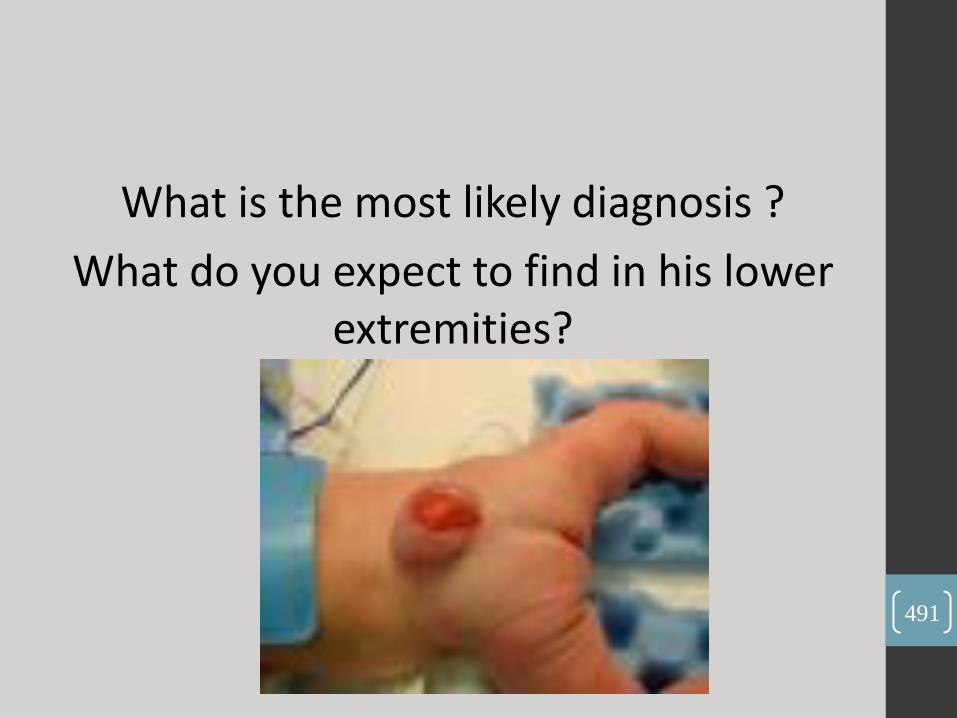
What is the most likely diagnosis ?
What do you expect to find in his lower extremities?
491
Myelomeningocele
Hypotonia.
492

Q1: what’s the name of this test??
Q2: mention tow abnormalities you expect to find in the lower extremities
of this child?
493

A: babinski sign.
A: clonus, hyperreflexia “brisk tendon reflexes”.
494

•Q: what’s his expected age?
495
A: 4 months coz his head and chest is above body level.
9 months coz he’s saying bye bye.
496
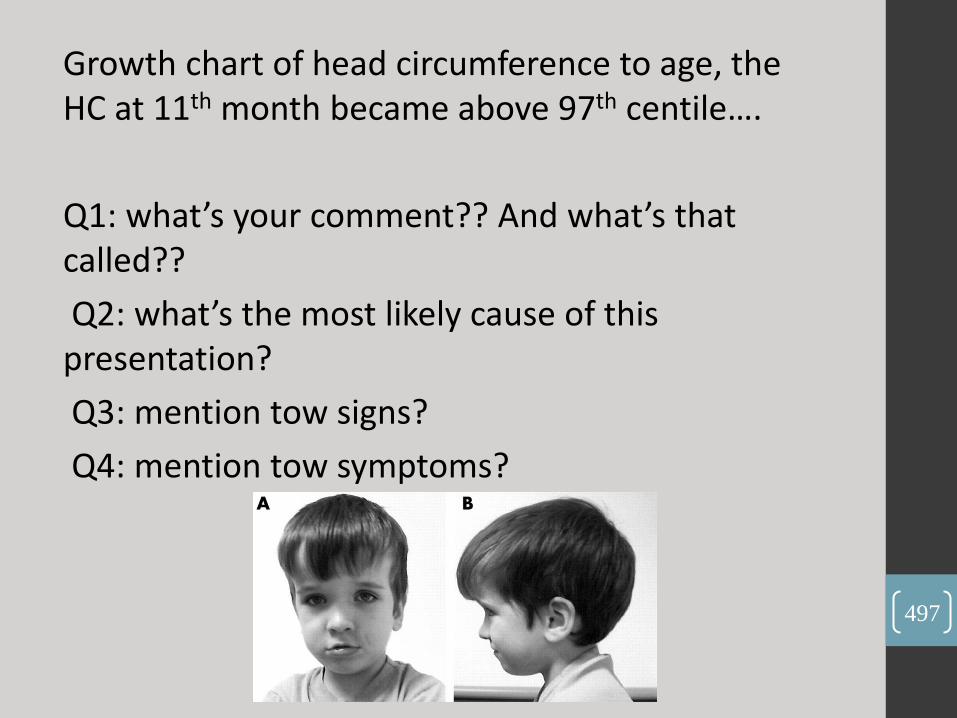
Growth chart of head circumference to age, the HC at 11th month became above 97th centile….
Q1: what’s your comment?? And what’s that called??
Q2: what’s the most likely cause of this presentation?
Q3: mention tow signs?
Q4: mention tow symptoms?
497
- macrocephaly.
- hydrocephalus.
- sun set eyes, papillodema.
- vomiting, headache.
498

499

Station 4:
A severely dehydrated child came to ER, they gave him there bolus 20 cc/kg, toe times within 1 hour or tow hours :
Q1: mention five signs you expect to find in this child ?
Q2: when he improved, he was admitted to the ward, calculate the rehydration fluid must be given to him in the comin 24 hours,,, Na: 145 meq/L,, weight: 10 kg.
500
- hypotension, sunken eyes, dry mucous membrane, capillary refill> 3 seconds, delayed skin turgor .
- Maintenance: 10*100=1000 cc.
Deficit: he is severely dehydrated so his weight loss between 10%-15%, and I’ll use 15% loss,
Deficit: 15*10*10= 1500 cc.
Na:
Maintenance: 3 * 10= 30.
Deficit: “ isotonic”
8*10=80
Total= 110
Deficit+ maintenance - bolus= 2100 cc.
2100 --- 110
1000 - ???
= 55
501

Station 5:
Examination: inspection of face and abdominal palpation for 16 years old female.
The patient was thalasemic so its important to talk about thalasemic features, pale conjunctiva and hepatomegaly.
Station 6:
Examination: patients presented with shortness of breath, examine all related to congestive heart failure.
You must talk about: JVP, blood pressure, edema, ascites, basal crepetation, pulse rate.
Station 7:
1 year old male child presented with cough and shortness of breath 2 days PTA,,, take history of present illness.
Station 8:
4 years old female child presented with jaundice and dark urine, take history of present illness.
502
• Q1: Do physical exam for this 10 year child with periorbital swelling for 2 days duration.
• You should start with inspection for the periorbital edema, do exam for lower limbs if there is edema ,examine the abdomen for ascites(shifting dullness &transmitted thrill) ,examine CVS ,liver, don’t forget kidneys ,inspect throat & skin (for impetigo) in suspension of post strep. GN.
503
Q2 : Acid Base balance for 12 cases(as table) , the student fills the table.
Examples:
*Chronic partially compensated metabolic acidosis.
Low PH \ low PCO2 \ base excess absent.
*Respiratory alkalosis (fully compensated)
Normal PH \ decreased PCO2 \ base excess absent.
504
Q3 : take history of 14 days old infant with jaundice.
- Onset. Progression. Stool & urine. Temperature (sepsis or UTI). Blood group (maternal, paternal, infant). Signs of hypothyroidism (weak cry ,macroglossia). Maternal antenatal infections (rash, fever) . Family history of jaundice or hemolysis . Abdominal distention (hepatomegaly). Ask about breast feeding & wt gain.
505

Q4 : Take history of 10 year old male with neck mass.
-Onset . Progression . Pain . Dysphagia . Exact site & size . Discharge . Mobility . Skin changes . Other masses .
-Pallor . Petichia . Fever –Night sweat –Chronic cough.
-Family hx of TB or chronic cough associated conjunctivitis . Associated oral changes . Hx of cat, dog Or rodent scratch or bite . Hx of neck trauma . First time or recurrent .
506

Q5: A fourth year medical student is asking you about meningitis case he has seen ,answer him.
A 7 month old male was diagnosed to have meningitis mostly bacterial, what antibiotics to give?
Vancomycin + 3rd generation ceph.(ceftriaxone or cephotaxime ) then according to culture & sensitivity .
507
Q. what physical examination shall u do in the second day ?
- look for signs of raised ICP, Anterior fontanel.
- Measure head circumference daily.
- BP, pulse, RR & pattern of respiration.
- Skin rashes.
- Complete CNS examination
• Q. This patient improved during the first four days on treatment, but he developed fever again on the 5th day. What happened to him?
• Mostly one of the complications of meningitis has occurred (brain abscess, meningococcemia, encephalitis).
•
508

Q. what to do for him?
Continue antibiotics And do Ct brain or MRI ,CBC , Blood culture , Electrolytes, fundoscopy , CNS exam.
Q. this child is 7 kg, what is your IV fluid order?
2\3 of maintenance.
Q. this patient come to you obtunded on the 6th day ,what is the cause?
Might be the same cause of fever (abscess or brain edema)
Q. this patient has developed seizure , what to do?
Serum glucose & serum electrolytes.
Q. his Na was 110 ,what is this? What to do?
Hyponatremia due to SIADH, we give him hypertonic saline (3%).
509

• Q6: 7 year old female come with recurrent seizures of 10 min duration without regaining her consciousness between the attacks, what is your diagnosis?
• Status epilepticus.
• Q: How to manage?
• -Admission to ICU & ECG monitoring.
• - Start with ABC’s:
• A: mouth piece, suction of secretions.
• B: O2 mask, monitor breathing, O2 %(pulse oxymeter).
• C: check the pulse, IV canuula.
-Blood sample for: Glucose, Electrolytes, Toxicology, Antiepileptic drug level, CBC.
-Glucocheck: if hypoglycemicgive glucose.
- Lorazepam (not available in Jordan ) so use diazepam IV (you can use diazepam rectally but IV is better.) 0.3 mg\kg.
-If no response after 10 min , repeat diazepam.
510
- If no reaponse give Phenytoin (fusphenytoin is better if available)15-20 mg\kg (note :phenytoin is given in normal saline).
- If no response, Intubate & give phenobarb.(15-20 mg\kg)
NOTE: Phenobarb & diazepam cause respiratory depression.
- If no response, then induce coma by Midazolam continuous infusion or any other general anesthetic. This should be under EEG monitor (not to miss non-convulsive seizure, we should see the burst suppression on EEG).
Q:What investigations to do after treatment?
EEG, Brain CT or MRI.
511

Q7: PICTURES:
1- Baby trying to eat alone with spoon, what is his age?
18 month (you should be specific ;don’t give interval).
2- Baby staring to his eyes in the midline , what is his age?
3 months.(be specific)
3- Newborn has weak cry &he is puffy & has neck swelling (his toungue is not protruded –unfortunately- )
Congenital hypothyroidism (goiter)
4- a child with portwine stain what isthis sign, this syndrome?
Port wine stain, Sturge weber syndrome.
512
Q8: X-rays
left lung collapse with mediastinal shifting
2. Double bubble sign duodenal atresia, history of vomiting since birth (the newborn is 3 days old)
What other signs do you expect on examination?
Abdominal distension, signs of dehydration, he might be dysmorphic, congenital heart disease signs
Note: duodenal atresia is common in Down syndrome.
3. Bilateral pulmonary edema (mostly)
Hx: 10 yr old male with hx of hematuria for 3 days came to you with SOB of one day duration, CXR was like this. What your diagnosis?
Its mostly pulmonary edema following acute renal failure following glomerulonephritis
513
OSCE
1) A 4 year old male complain from SOB 2 days PTA, take full history from his mother then
examine the most related system (focus examination)?
Note: -you must introduce yourself, analyze the CC in details before asking about associated
symptoms; in examination don't forget to take the RR.
2) 5 years old patient complain from diarrhea 3 days PTA, take full history from his mother then
examine the most related system (focus examination)?
Note: -ask about any probability to food poisoning; in examination don't forget the sign of
dehydration & the VS (HR, BP).
514
• 3) 4 year old patient complain from high fever for 1 hour PTA, ask about the most common
• causes for fever & examine just the specific signs that related to your DDx?
• Note: -don't forget to ask about meningitis, examine the meningial signs.
• 4)13 year old male patient, his mother noticed that he is shorter than his friends in school in last
• 1 year, take full history from his mother then measure the wt & ht & put them in the graph,
• according to your finding what is the problem in this patient?
515

5) CC: cough for 2 days PTA?
Note: in examination: -sign of respiratory distress, RR, all RS examination, examine the throat
and the ear (otitis media).
6) CC: 3 years old pt with jaundice for 10 days PTA?
Note: -ask about other similar condition in the house or school; ask about food, drugs, family
history of hemolytic anemia.
-In examination: Tm, describe the extent of jaundice, full examination of the abdomen, BP.
7) CC: per orbital swelling for 5 days PTA?
Note: ask if bilateral or unilateral, red, pain, tender, warmth with time.
-urinary symptoms, CVS, liver (jaundice), malnutrition of protein, vomiting, diarrhea, allergy.
-in examination: analyze both eyes (swelling, redness, hotness, discharge, jaundice), signs of
fluid overload (leg edema, ascites, scrotal edema, basal crepitation, BP)
516
8) Infant complains from SOB 2 days PTA, take full history from his mother then examine the
most related system (focus examination)?
Note: ask about everything of RS; examine VS, all RS examination, LN and ENT.
9) 13 years old male pt with incontinence, take history & focus examination?
-in history: analyze incontinence, renal symptoms, GIT, family hx of renal dz, drugs.
-in examination don't forget BP, Tm, growth parameter, palpate renal angle & suprapubic area,
signs of fluid overload, genitalia.
10) CC: 3 months pt with squint & irritability?
Note: in history ask about fever, vomiting, lethargy, appetite (poor feeding), activity, wt loss.
-in examination: fontanel, HC, CNS examination (mainly eyes), dilated superficial vein in scalp.
517
11) 10 year old female pt presented with difficulty of breathing of 2 days PTA? This case is cystic fibrosis.
Note: analyze the CC, RS symptoms, receives medication or nebulizer (response or not), general
symptoms, GIT symptoms.
-examination: VS, growth parameter, RS examination, hands for clubbing.
-There was finding in this case e.g. wheeze.
12) Breast feeding counseling: this 25 year old lady has delivered a baby 4 hours go & she has
some Qs to you about breast feeding?
-what is better cow's milk, formula, breast milk?
-what is the benefit of breast feeding for mother & baby?
-relation between breast milk & jaundice?
-for how long I have to breast feed him, when to introduce other food?
518
13) A mother brought her child to ER, take history?
-this pt was complained from red urine .
14) Developmental hx for 13 month old child?
-you have to start from the milestone suitable for 13 months & the descend.
-growth parameter (there were 2 growth charts wt/age, ht/age, and it showed that ht is below the
5th centile & crossed two main centiles: what happened? FTT
-there were chart for wt/ht: is the ht (length) also affected with FTT? yes because it is in 25th
centile. 519

15) a 20 month old child came to ER and cc is cough and cyanosis take hx and do examination
1.Historty : Analyze CC , duration(2hr) and onset (sudden) when the family were eating, and
there was melon seeds on the table (Bzer), it turns to be forign body aspiration
the dr asked if he need admission and why?! And to explain to father why ?
16) Examination : Respiratory distress signs, and Rs. exam..
2nd Station : Vomiting ,Diarrhea and Fever, take Hx and address the mother concerns.
The Examiner then asked if he needs addmission!
And if not; at home what to give him? (aquasal)
How we prepare and give ORS?
Does he need antibiotics?
When to bring him again to hospital (if what happens)?!
520

17) Developmental hx for 12 Months (pt of CP)
1.History : she was very delayed..
2. Examination : Assess the tone ( posture frog like, head lag, ventral and vertical suspension)
18) Recurrent vomiting
• 1.History : Age and Duration and Frequency, etc Don't forget the cough and to assess the hydration, and to ask about (weight)
• 2.Examination : examine growth parameters,.. Then what is next to do is growth charts to plot
• the numbers..
• -------------------
521

19) counselling about Neonatal Jaundice , vaccination, breast feeding
Neonatal Jaundice : Causes , why did it happen with him , how to treat , give mechanism of
phototherapy
Vaccination : BCG , when to give , how to know that he took the vaccine , any side effects .
20) 3 months old presented with cataract, intracranial calcification on CT, take hx only
,And examine the patient
1.History : Prenatal Hx. Only
2.Examination (head and neck: there was no cataract (-ve red reflx by opthalmoscope) closed fontanell, high arched palate, retrognathia, dysmorphism, microceph).
522
• 21) hx (chronic diarrhea since 6 months of age , now he is 5 years. celiac with FTT)
• exam (take growth parameters).
• 22) hx (S.O.B, +ve only fever, cough, rinorrhea, noisy breathing , hx of contact) exam
• (full resp exam). 523
23) History taking for a case of abd. Pain ? it was a functional abd. Pain
24) History taking for a case of skin rash?
I think it was HSP (there was hematuria)
25) Examination of a child with infective endocarditis?
General look, Vital signs
Eyes: Roth’s spot, subconjuctival hemorrhage
Oral cavity: Dental caries, mucous membrane bleeding
Hands: clubbing, splinter hemorrhage, osler’s nodule
Chest: Inspection: ……….
Palpation: tenderness, apex beat, tracheal deviation & TVF
Percussion (pulm. Edema)
Auscultation: S1 & S2 , murmurs. air entry, breathing type, addes
sounds, basal crackles.
Abdominal for hepatosplenomegaly
Lower limbs for petichial hemorrhage & pulses (emboli)
Neurological exams (cerebral emboli)
524

25) Station 4:
A) ECG of SVT:
Q1: what is the HR?
It was 300b/min (there was only 1 large square between each RR)
Q2: Give two modalities of treatment? 1- carotid massage
2- medical with adenosine
B) A history with recurrent vomiting & give u an ABG with electrolytes results
Q1) what is the ABG finding?
Partially compensated metabolic alkalosis
Q2) what is the electrolyte abnormality? & explain it?
Hypokalemic hypochloremic .
525

26) Syndactyly & if it happen in normal variants (answer yes).
Prader willi syndrome
Pedigree for an X-Linked dominant
Kwashiorker
Duodenal atresia (double bubble sign)
CXR: Rt Pleural effusion or teratology of fallot (boat shaped heart). I don’t know
Turner syndrome (coarctation of aorta)
Anal atresia, single investigation is pelvic X-ray to show level of obstruction.
Vaccination (remember that Pertussis is contraindicated >3years)
Age of a child standing on a Baby Trolley? 10 months.
526

أيها الشباب أنتم أصفى الناس ذهنا ،
وأقل انشغالا ، وأقوى صحة ، وأمضى
الشمس :" عزيمة أنتم كما قال الرافعي
لا تملأ النهار في آخره كما تملؤه في
أوله ، وفي الشباب تصنع كل شجرة من
أشجار الحياة أثمارها ، وبعد ذلك لا .تصنع الأشجار كلها إلا خشبا

in the following image:
• a. what is your diagnosis?
• b. what test you want to confirm your diagnosis?
528

• Hypothyrodisim
• TSH level / or T3, T4
529
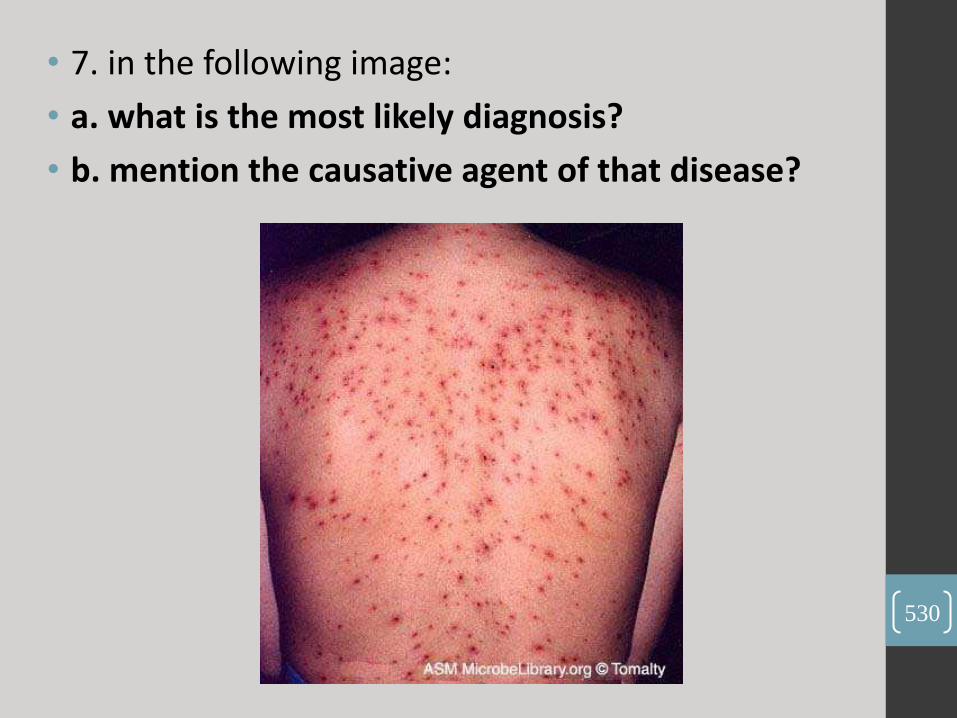
• 7. in the following image:
• a. what is the most likely diagnosis?
• b. mention the causative agent of that disease?
530
- Shingles
- Varicella zoster virus
531

OSCE 1.
a. Cough and Shortness of breath (Asthmatic Patient) – Hx & P/E
b. Dark urine ( Thalassemic patient ) – Hx & P/E
c. FTT and Counseling About Celiac Disease. – Hx
2.
a. Yellowish discoloration of the sclera (Hepatitis A) - Hx & P/E
b. SOB (Long case of cyanotic heart disease) - Hx & P/E
c. Counseling about Iron Deficiency Anemia. 532
3. A 13 year-old female patient with 2 days of abdominal pain…. Take focused history and relative physical exam.
4. An 11 year-old male who came to the ER with cough … take focused history and relative exam.
5. Take a history from a patient complaining of Headache (meningitis).
6. Do general lower limb examination (Inspection, tone, power, primitive reflexes and deep tendon reflexes) .
7. Take a history from patient (4 Month) complaining of vomiting and diarrhea (gastroenteritis) & do a physical examination, Then Answer the Questions , Asked by His Mum
“ in the next slide “ .
533
•Then Answer the Questions
·؟ ليش ما بحكي ابني•
·بهذا الوقت؟ شوالمفروض يحكي•
·متى ببلش يقعد؟ •
·متى ببلش يحكي بابا وماما وهو بعرفنا؟ •
·بدي اعطيه حليب شو رايك اعطيه •
رضعة حليب صناعي كل يوم والا بكفي الطبيعي؟•
·؟ )أعطيه صناعي(ليش ما في داعي •
·متى اوقف الرضاعة الطبيعية؟ •
·متى ابلش اعطيه اكل غير الرضاعة؟ •
·شو المطعوم اللي لازم يوخذه عندك حاليا؟ •
·اايش هو المطعوم الخامسي؟ •
·ايش ممكن يصير معاه اعراض •
جانبية للمطعوم الخماسي؟•
534 ؟)إذا صار معاه حرارة(شو اعمله •

8. A 6 month-old infant who was admitted to the hospital and was diagnosed to have bronchiolitis … answer these questions which are asked by the infant's mother:
- How do you manage/treat this patient ?
- What precautions will you take when dealing with him, and does he need isolation and if so what type of isolation?
- This infant missed his 4 month ( 121 day) vaccine, will you give it to him now or you will wait until he recovers from bronchiolitis ?
- What are the vaccines given at 121 day old ( mention them) ?
- His older brother (who is 3 or 2 years old) has leukemia and he is now on chemotherapy, will you give him the vaccine as usual or make any change in them, and why? >>> yes , use IPV instead of OPV, because … ,
- What is the virus usually causes bronchiolitis ? >>> RSV
- Mention other viruses.
- What is the severe form of bronchiolitis caused by adenovirus ?
>>> bronchiolitis obliterans.
- Is there any vaccine for RSV , if yes : what is it called and what is its type ?
- What extra vaccines can you give to this infant?
535
9. hip joint pain take history and relevant examination suspected rheumatic fever .
10. chronic diarrhea take history and relevant examination- the only positive is family history about celiac disease .
11. counselling about neonatal screening:
A mother give birth to a male born came to your office to know about screening 1- what is neonatal screening? 2-when you do it? 4 to 5 days 3- from where you take the sample? From the heal 4- name 6 diseases you know that we can screen?? 6/12, hypothyroidism, phenylketonurea, tyrosenemia, homocystinurea, galactosemia, maple syrup urine disease, congenital adrenal hyperplasia 5-is it treatable? No but can be controlled
536
12. A child presented with epistaxis & bruises + do a proper exam >>> ITP .
13. 14 year female presented with recurrent cough + do a proper exam >>> CF .
14. Counseling about vaccination >>> "
• took IVIG" a Q about Kawasaki prophylactic
• vaccines & Q about IVIG relation with vaccination
• with other Qs
15 . A child resented with LOC + do a proper exam >>> SVT "some students told me that there was a note in the paper that lead them to cardiac problem“ .
537

16. Pallor + do a proper exam >>> anemia i think it was Thalasemia .
17. Counseling about Down Syndrome :
- diagnosis antenatal
- inheritance % with problems of Down.
18. take Hx of presenting illness loss of consousness and do CVS exam. (the patient develop LOS after he did exercise and take a shower) .
19. Take Hx of presenting illness pallor and do abdominal examination. (the patient did splenctomy, and her cousin did also splenctomy )
538
20. Counseling Down syndrome:
• كيف رح تخبر الأهل
• متى بتخبر الأهل
• Can you diagnose down antenatal? And how?
• How can you confirm your diagnosis? (Chromosomal analysis)
• What is most common translocation cause of down? (14 ,21)
• What is percentage next baby having down syndrome? What things increase the percentage? (increase in mother age)
• What is most common cardiac anomaly and how you can diagnose it? (VSD AV canal, echo).
539

لا عندما يحاكي .... ل ن نبض إلحياة ...نبضكم لا يس تمر إ
فقد إرتضينا أ ن نجعل أ صابعنا شموعا تنير... ل ننا كذلك
..وروضة وردية... أ ن نجعل قلوبنا وإحة ندية .. دروبكم
تغفو على رإحتها عيونكم إلخجلى إلتي ما برحت
....تعانق عنان إلسماء
...وها نحن نقتح لكم أ بوإب قلوبنا على مصرإعيها
...وهاتوإ أ يديكم .... فكونوإ على قدر من إلحماسة
إلفكرة إلتي تحيا على نبض قلوبكم لنبقى
ما تبقى من هذإ إلملف هي ملاحظات
هامة وأ س ئلة متوقعة ينصح بدرإس تها
وليست أ س ئلة س نوإت سابقة ، قامت
عدإدها إلزميلة رلا إلقوإبعة من دفعة ب
2008

-What syndrome is this ?
- What is the
chromosomal defect here ?
- Name 2 congenital defects
that are associated with
this condition.
- Down‘s Syndrome
- the presence of an extra copy of genetic material on the 21st
chromosome, either in whole (trisomy 21) or part (such as due
to translocations) .
- AV canal (aka endocardial cushion defect), VSD, ASD, valvular
disease, duodenal atresia, annular pancreas, & imperforate anus
“Nelson p179”.
542
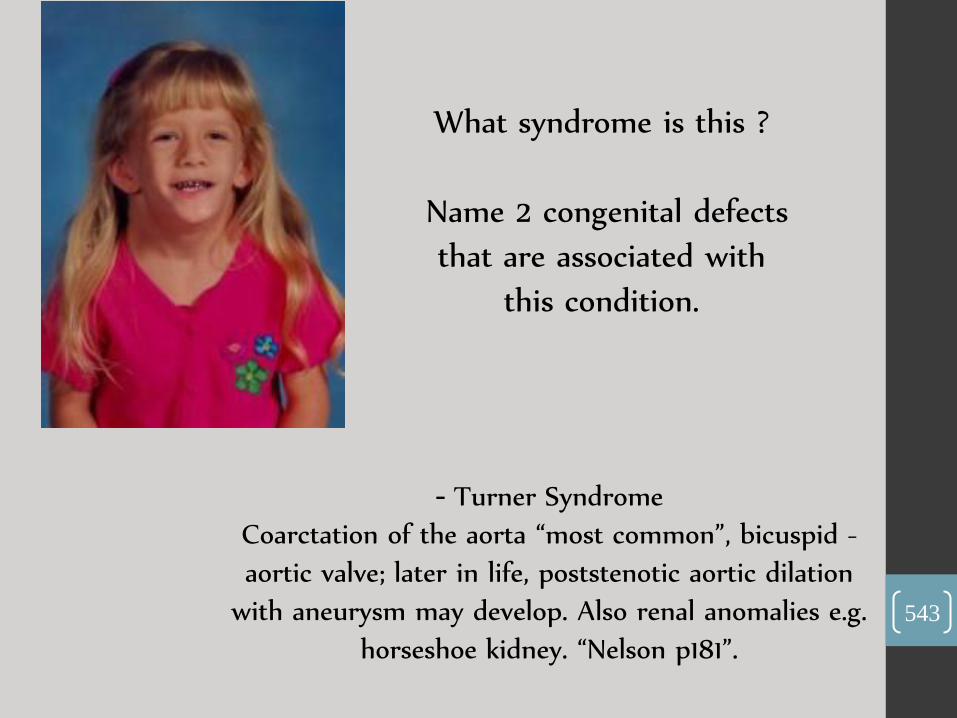
What syndrome is this ?
Name 2 congenital defects
that are associated with
this condition.
- Turner Syndrome
-Coarctation of the aorta “most common”, bicuspid
aortic valve; later in life, poststenotic aortic dilation
with aneurysm may develop. Also renal anomalies e.g.
horseshoe kidney. “Nelson p181”.
543
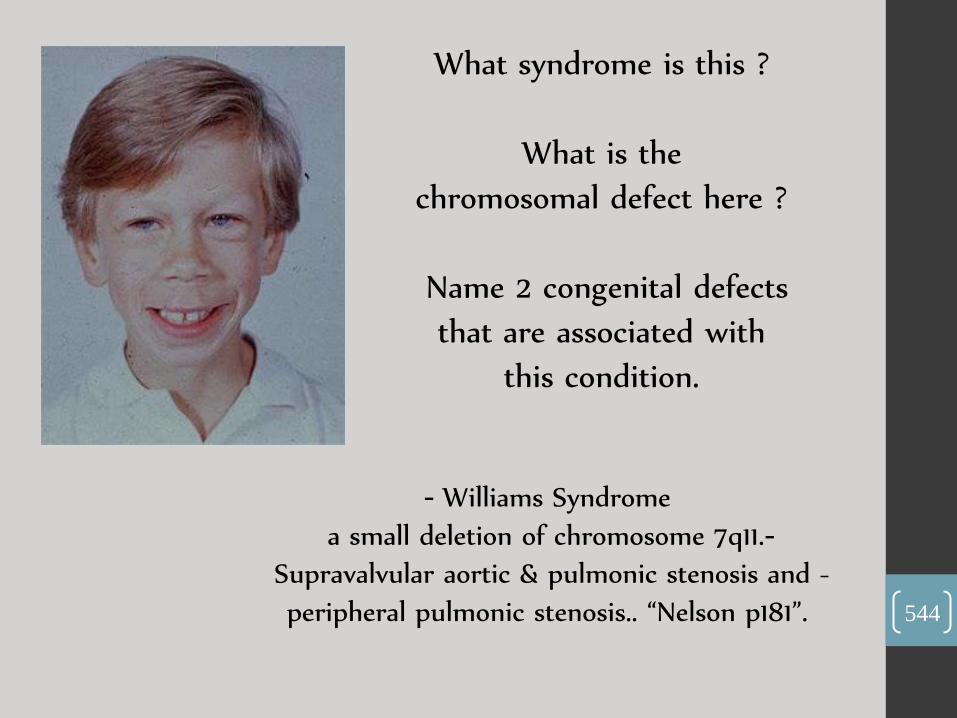
What syndrome is this ?
What is the
chromosomal defect here ?
Name 2 congenital defects
that are associated with
this condition.
- Williams Syndrome
- a small deletion of chromosome 7q11.
- Supravalvular aortic & pulmonic stenosis and
peripheral pulmonic stenosis.. “Nelson p181”.
544

What syndrome is this ?
What is the
chromosomal defect here ?
male : female ratio of
incidence is ?
- Noonan Syndrome (sometimes desrcribed as “the
male version of Turner's syndrome”).
autosomal dominant (AD) congenital disorder .
1 : 1 … as it’s AD.
545

What syndrome is this ?
Name 2 clinical
manifestaions maybe found
in this pt.
- Goldenhar syndrome.
limbal dermoids, preauricular skin tags,
and strabismus .
Note: “Chief markers of Goldenhar syndrome are
incomplete development of the ear, nose, soft palate,
lip, and mandible on usually one side of the body” …
Wiki 546

What syndrome
is this ?
Name 2 clinical
manifestaions
maybe found in
this pt.
Crouzon syndrome.
Low-set ears, brachycephaly, Exophthalmos,
hypertelorism, hypoplastic maxilla … etc. 547

Congenital Cushing’s syndrome
- What could this pt have ?
548
X – Rays …
549

Upper right lobe pneumonia.
- What could this pt have ?
550

Lower right lobe pneumonia.
- What could this pt have ?
551
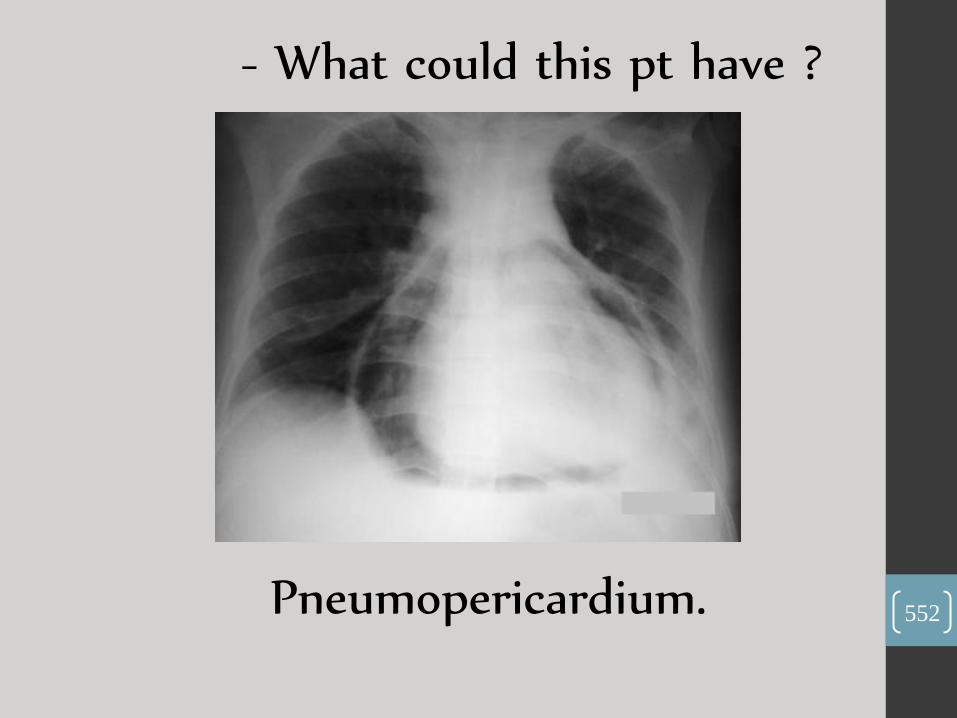
Pneumopericardium.
- What could this pt have ?
552
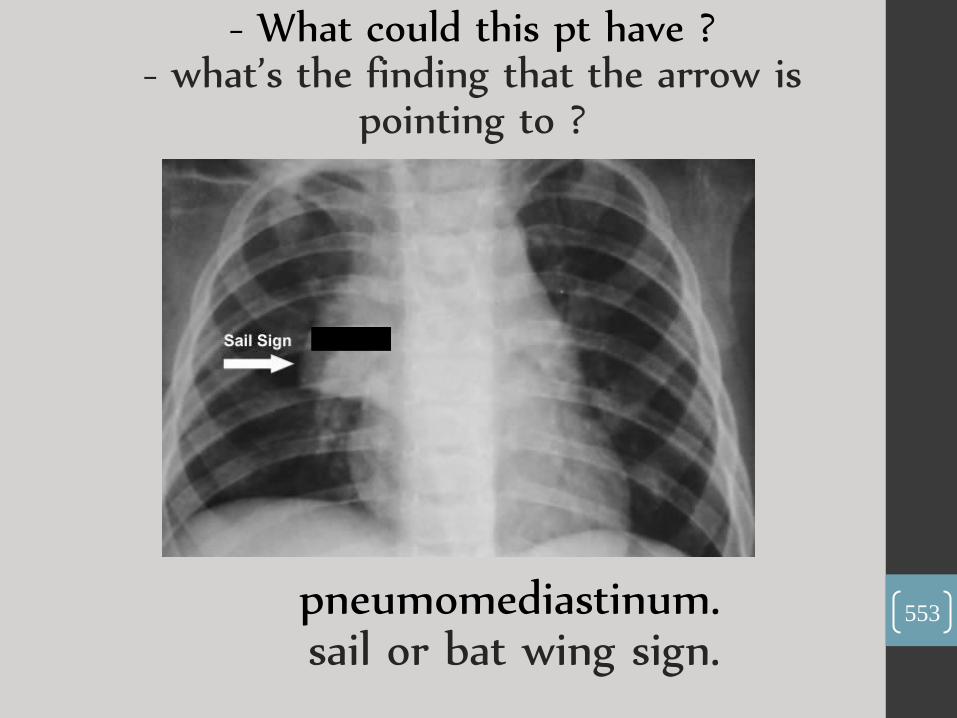
pneumomediastinum. sail or bat wing sign.
- What could this pt have ? - what’s the finding that the arrow is
pointing to ?
553
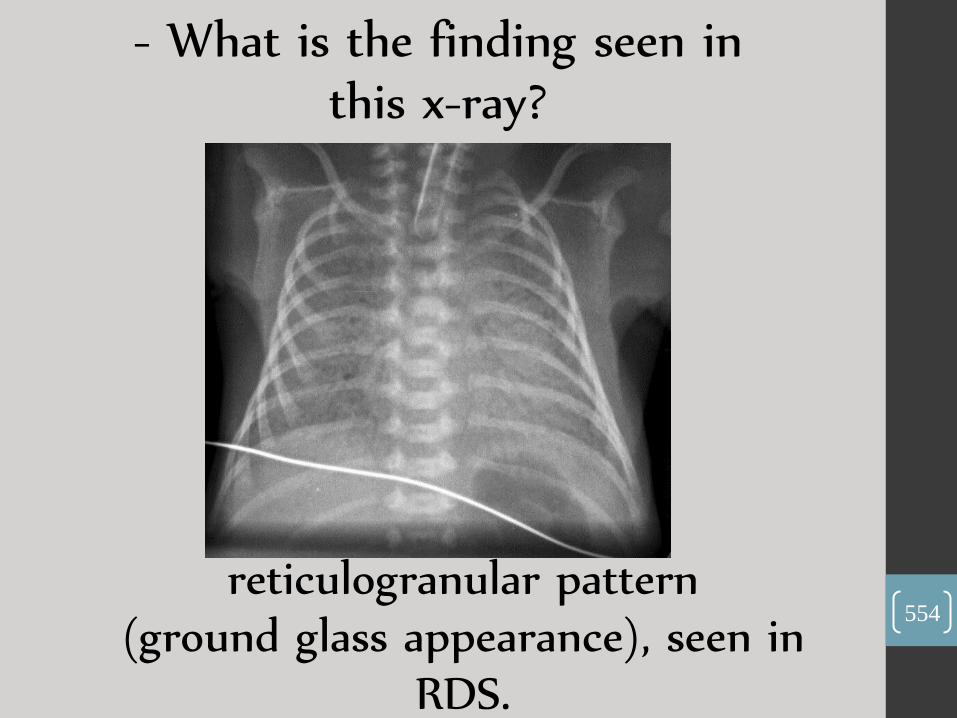
reticulogranular pattern (ground glass appearance), seen in
RDS.
- What is the finding seen in this x-ray?
554
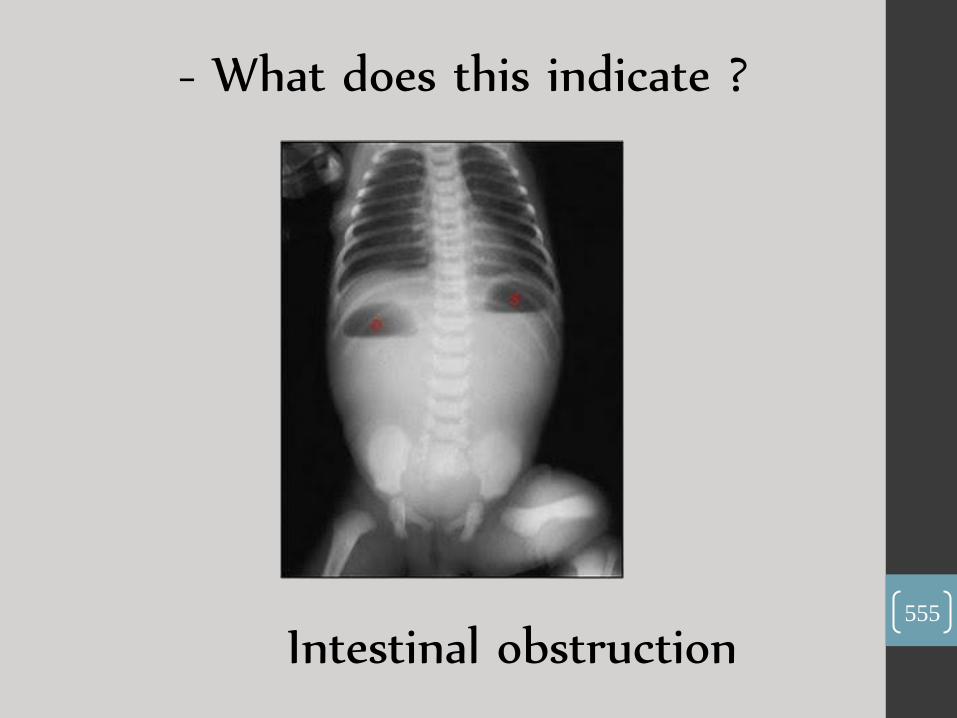
Intestinal obstruction
- What does this indicate ?
555

Massive pleural effusion
- What’s your dx ?
556

Congenital diaphragmatic hernia
- What is your dx ?
557
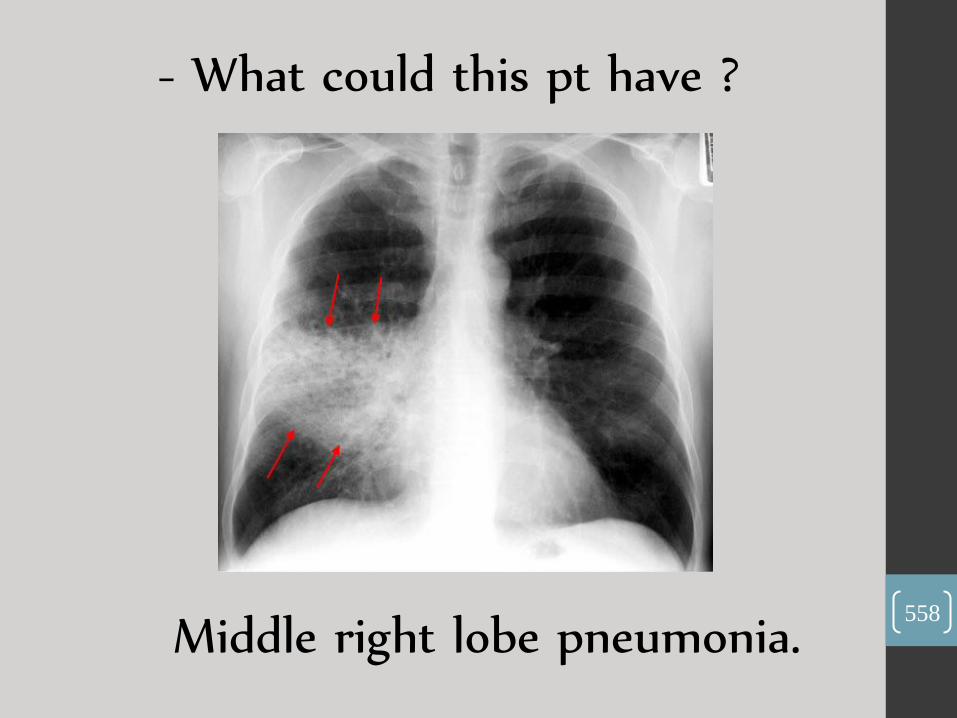
Middle right lobe pneumonia.
- What could this pt have ?
558

Development …
559
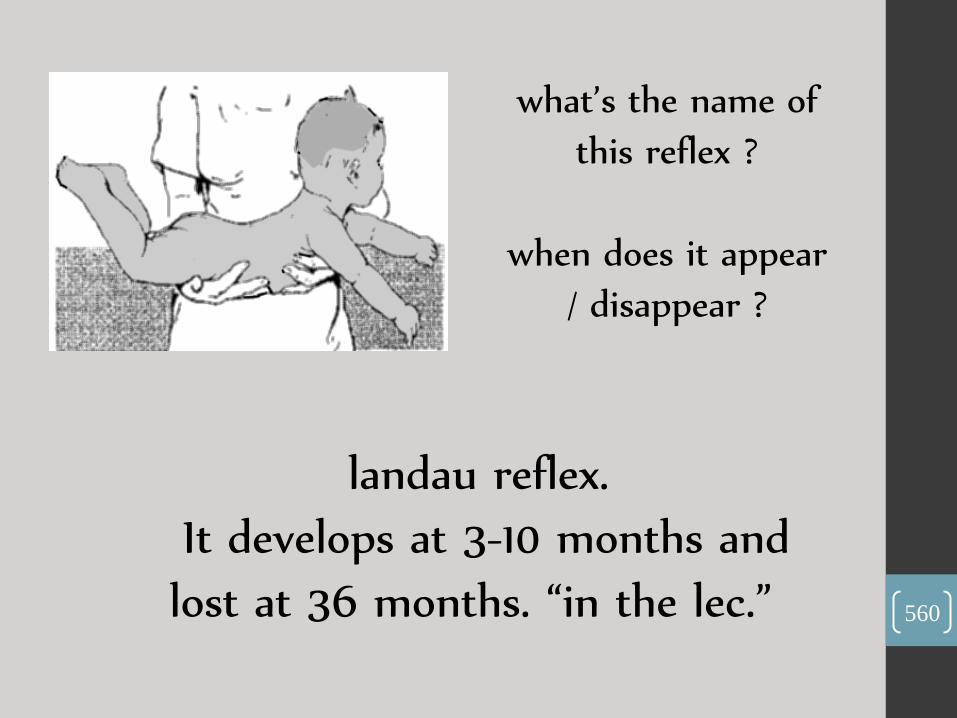
what’s the name of
this reflex ?
when does it appear
/ disappear ?
landau reflex.
It develops at 3-10 months and
lost at 36 months. “in the lec.” 560

what’s the name of this
gross motor ?
Around what age does it
appear ?
Mouthing.
It develops around (4 -5) months.
561

-what’s your rough estimation of this child’s
age ?
Around ( 9 – 10 ) months.
562

When does this reflex appear ?
symmetric tonic neck reflex
Around ( 6 - 7) months. 563

Nursery
& NICU …
564

What’s the dx ?
What other findings
could be found in
this pt?
Omphalocele.
cardiac defects, Beckwith-Wiedemann syndrome
(somatic overgrowth, hyperinsulinemic
hypoglycemia, risk for Wilms tumor), and
intestinal complications. 565

What’s the dx ?
What’s the
importance of this
condition?
Gastroschisis.
its association with intestinal necrosis; although
it’s not associated with extraintestinal anomalies,
but segments of intestinal atresia are common. 566
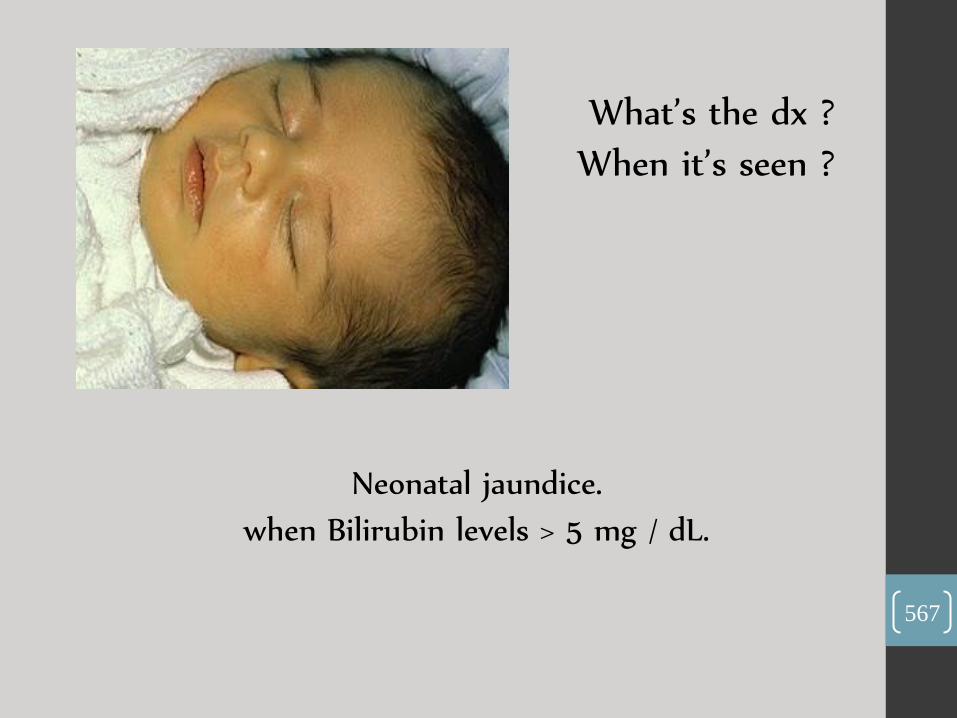
What’s the dx ?
When it’s seen ?
Neonatal jaundice.
when Bilirubin levels > 5 mg / dL.
567

What’s the dx ?
what findings could this pt present?
Meningomyelocele.
total paralysis, loss of sensation in the legs and
incontinence of bowel and bladder. In addition, affected
children usually have an associated Arnold-Chiari
malformation of the brainstem that may result in
hydrocephalus and weakness of face and swallowing.
568
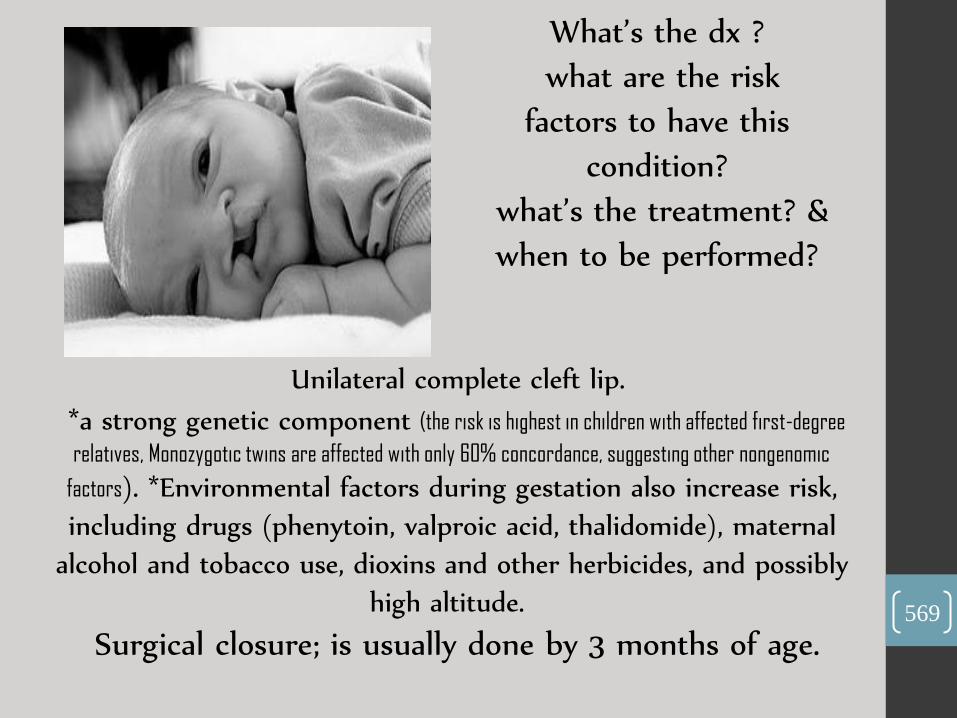
What’s the dx ?
what are the risk
factors to have this
condition?
what’s the treatment? &
when to be performed?
Unilateral complete cleft lip.
*a strong genetic component (the risk is highest in children with affected first-degree
relatives, Monozygotic twins are affected with only 60% concordance, suggesting other nongenomic
factors). *Environmental factors during gestation also increase risk,
including drugs (phenytoin, valproic acid, thalidomide), maternal
alcohol and tobacco use, dioxins and other herbicides, and possibly
high altitude.
Surgical closure; is usually done by 3 months of age. 569
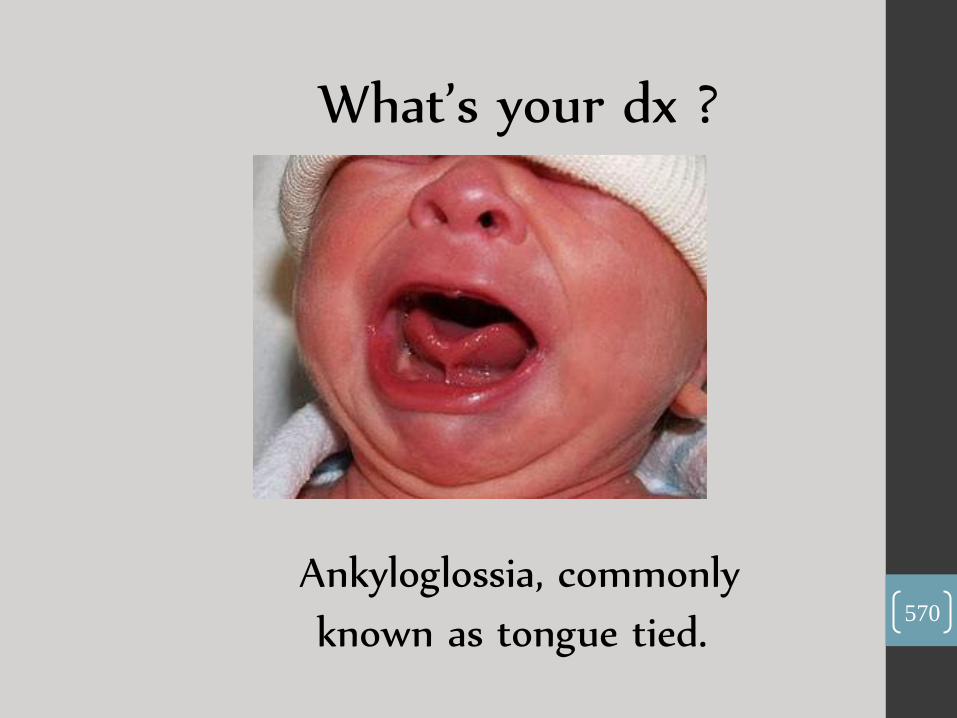
What’s your dx ?
Ankyloglossia, commonly
known as tongue tied. 570
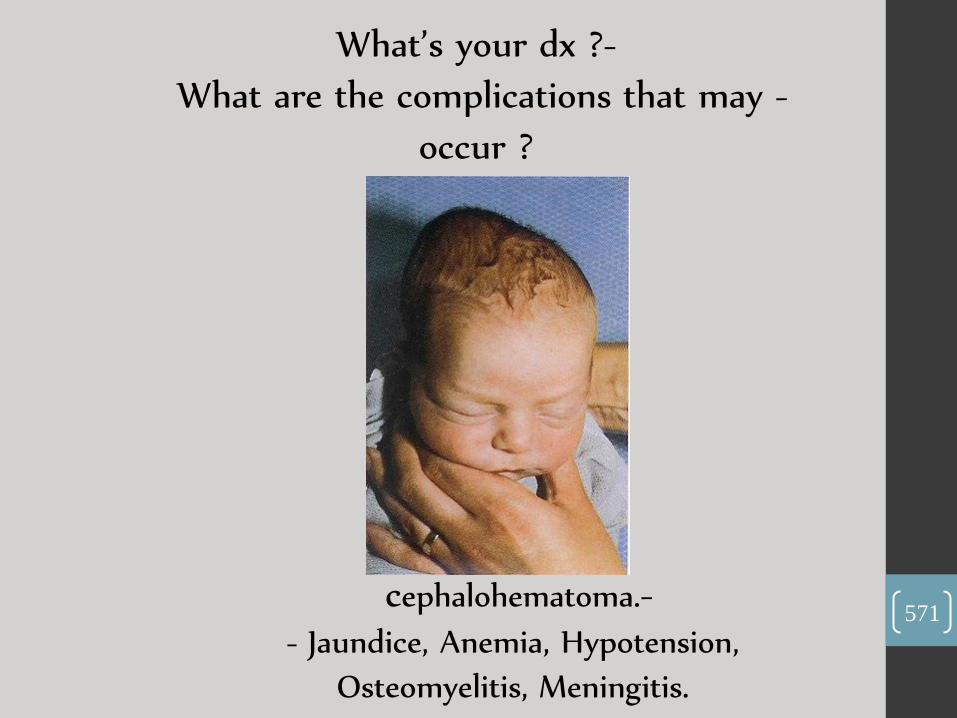
-What’s your dx ?
- What are the complications that may
occur ?
- cephalohematoma.
- Jaundice, Anemia, Hypotension,
Osteomyelitis, Meningitis.
571

What’s your dx ?
What’s the etiology 4 this
condition?
What are the
complications of both
treated or untreated pt.s ?
CLUB FOOT (TALIPES EQUINOVARUS).
can be congenital, teratologic, or positional. Congenital clubfoot (75% of
all cases) is usually an isolated abnormality. Teratologic clubfoot is associated with a
neuromuscular disorder, such as myelomeningocele, arthrogryposis, or other syndromes.
Positional clubfoot is a normal foot that was held in the deformed position in utero.
Complications of untreated clubfoot include severe disability.
Complications of treated clubfoot include recurrence and
stiffness.
572
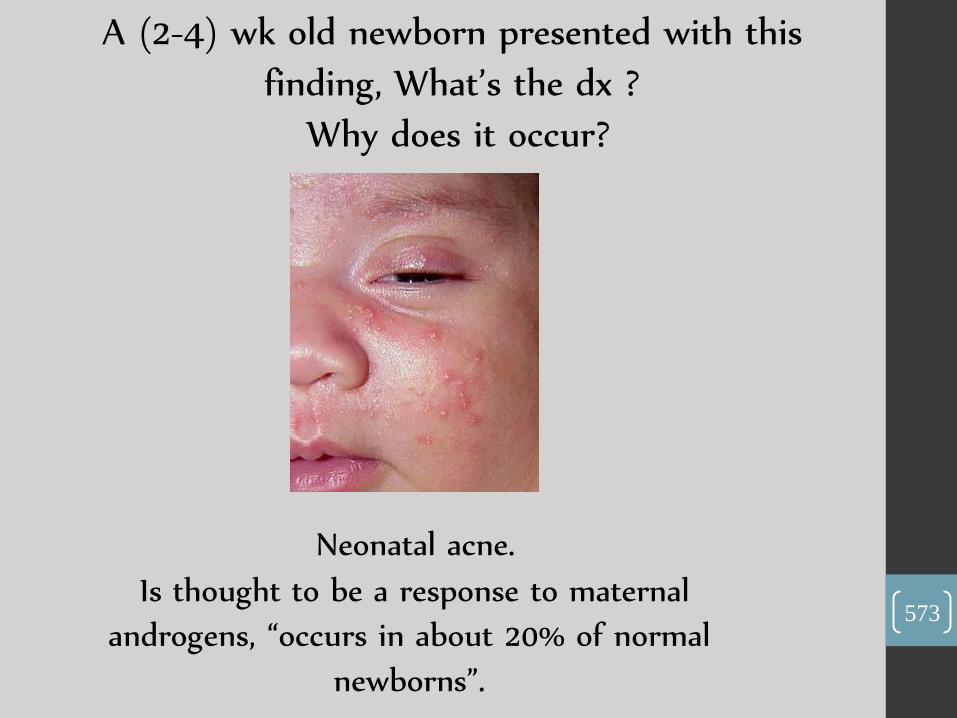
A (2-4) wk old newborn presented with this
finding, What’s the dx ?
Why does it occur?
Neonatal acne.
Is thought to be a response to maternal
androgens, “occurs in about 20% of normal
newborns”.
573

What’s the dx ?
female : male ratio is ?
what complication may develop ?
Hemangiomas. ( 3 : 1 ).
Ulceration, the most frequent complication, can be
painful and increases the risk of infection,
hemorrhage, and scarring
574

Micellaneous …
575
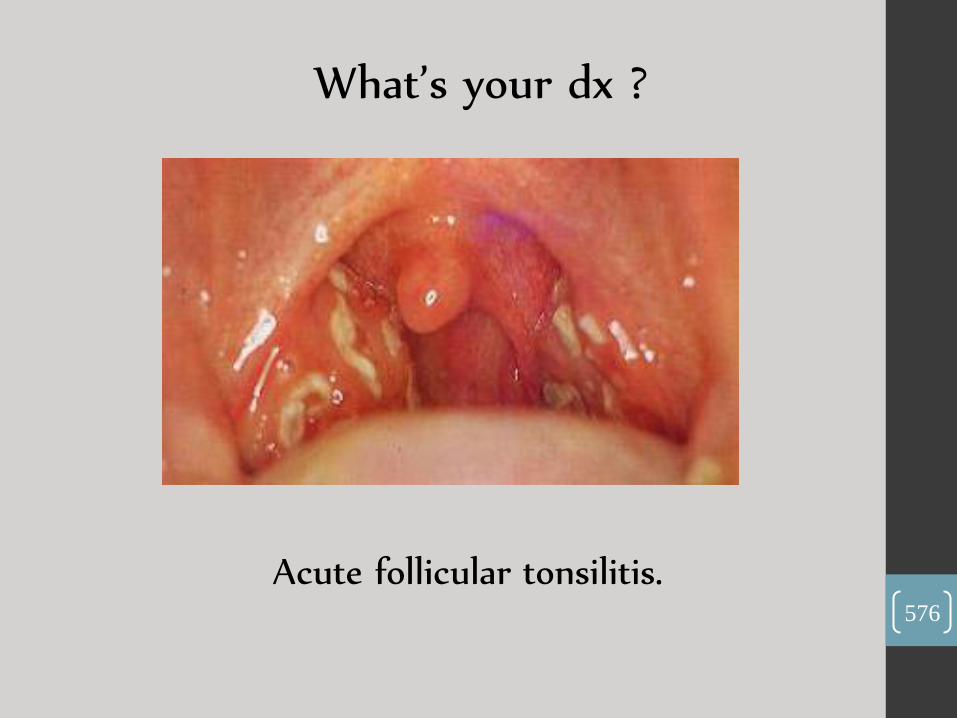
What’s your dx ?
Acute follicular tonsilitis. 576

What’s your dx ?
Angioedema. 577

What’s the finding ?
What’s your dx ?
Koplik's spot.
Measles.
578

What’s the finding?
What does it indicate?
Raccoon eyes.
A closed-head injury that results in a basilar
skull fracture.
579
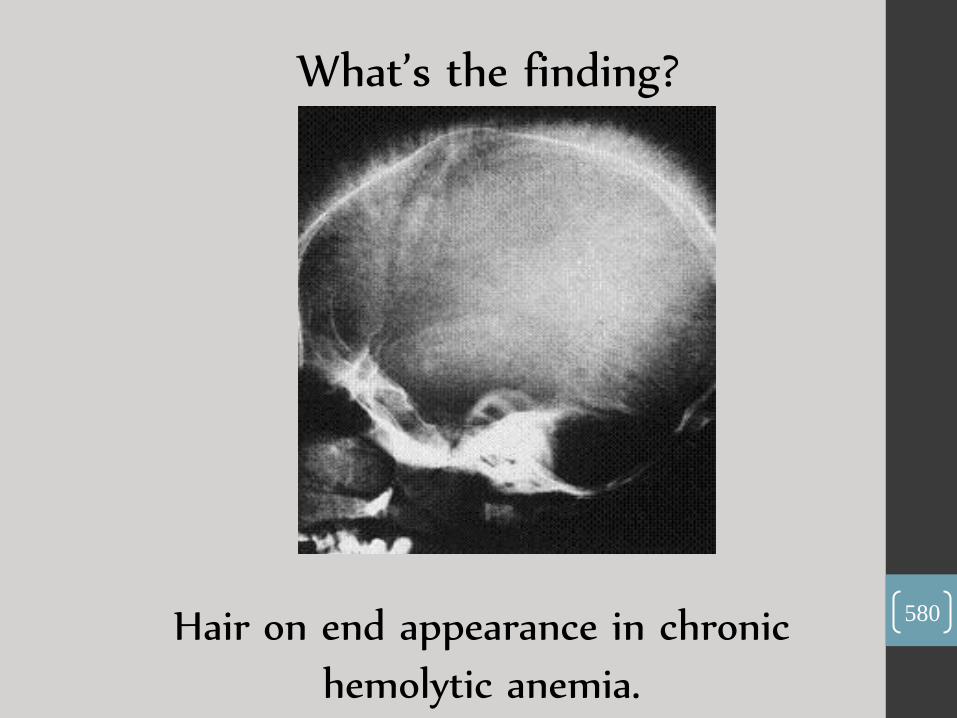
What’s the finding?
Hair on end appearance in chronic
hemolytic anemia.
580

What’s your dx ?
Microcephaly. 581

What’s your dx ?
-Erb’s palsy. 582

What’s your dx ?
Kwashiorkor. 583
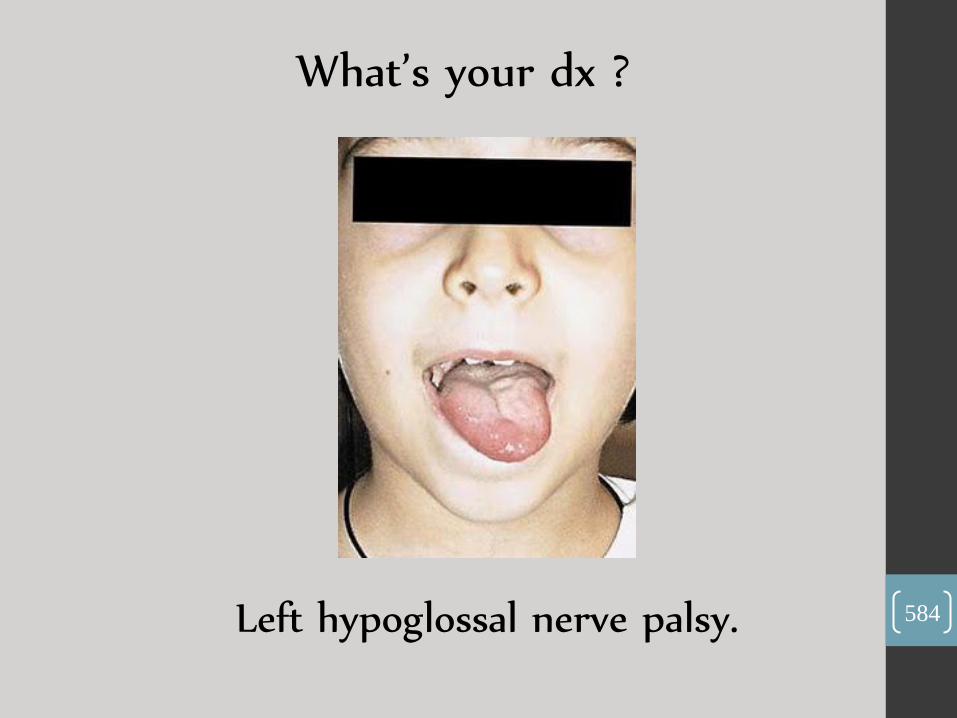
What’s your dx ?
Left hypoglossal nerve palsy. 584
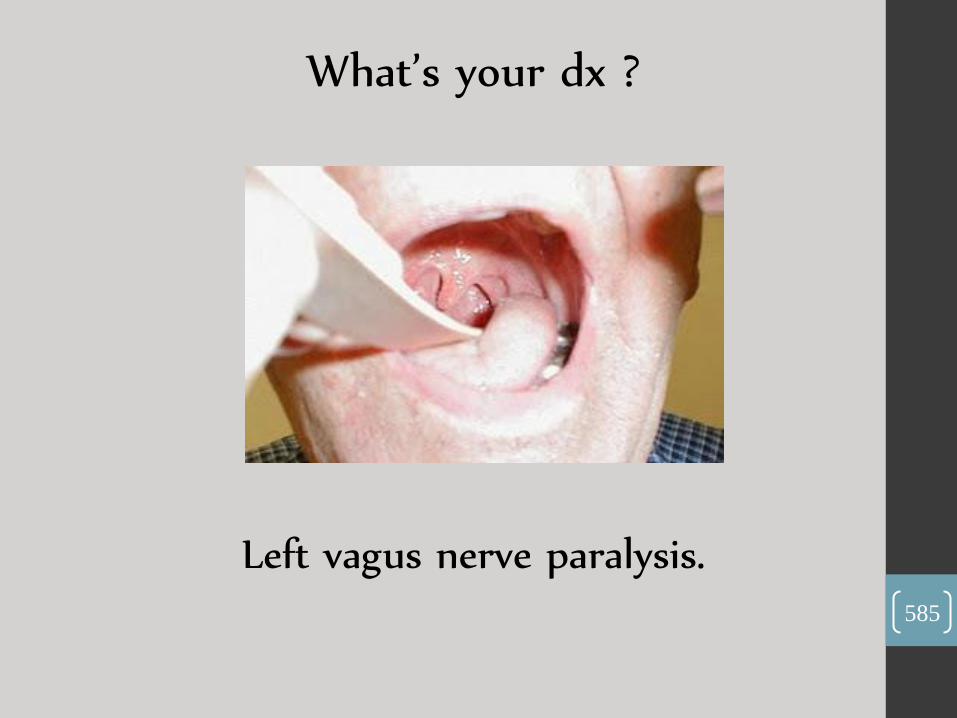
What’s your dx ?
Left vagus nerve paralysis. 585

What’s your dx ?
Scarlet fever. 586

What’s your dx ?
Impetigo. 587

-What’s your dx ?
Kawasazi Disease.
588
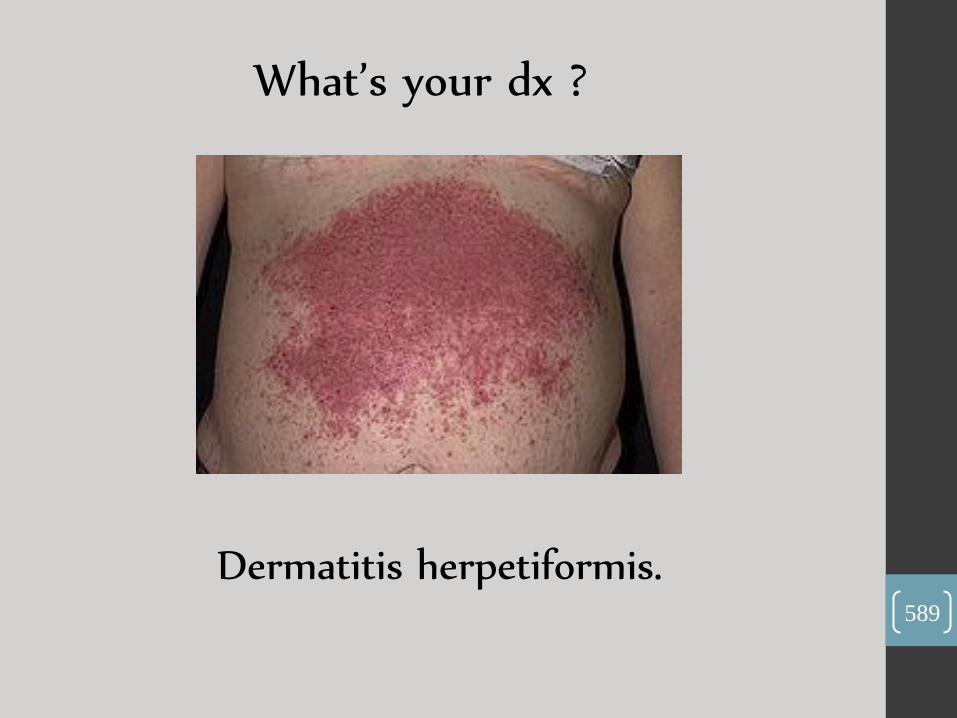
What’s your dx ?
Dermatitis herpetiformis. 589

What’s your dx ?
Warts. 590
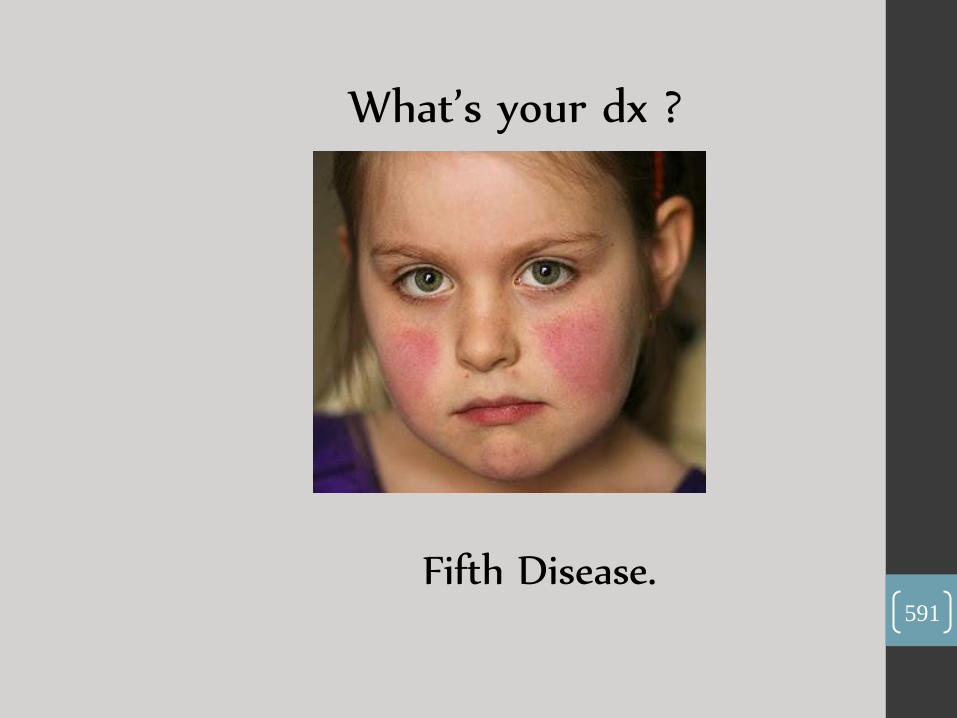
What’s your dx ?
Fifth Disease. 591
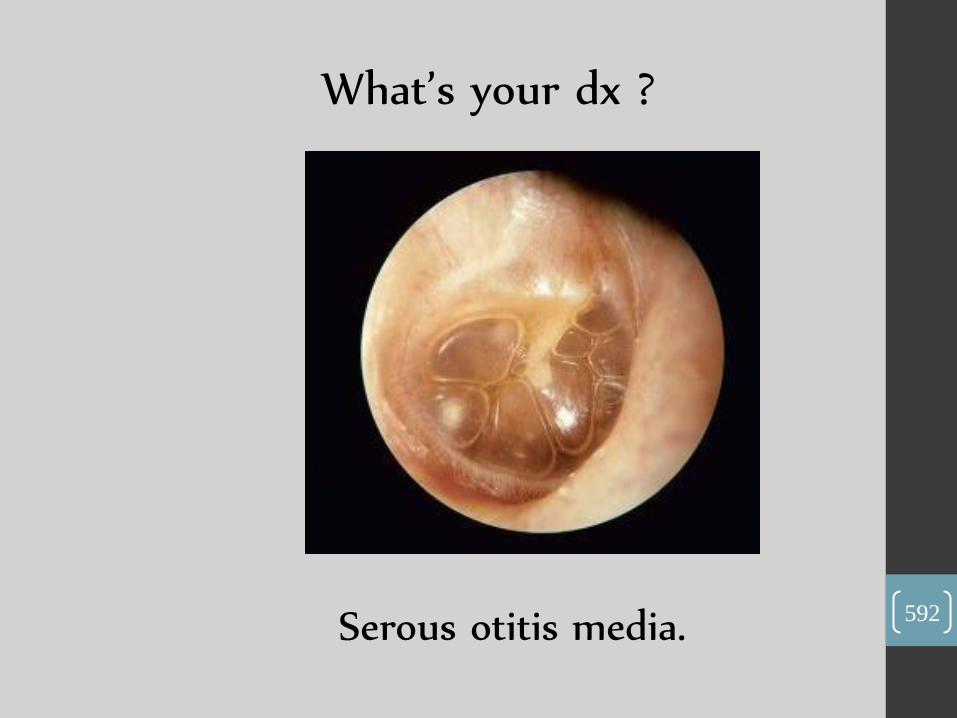
What’s your dx ?
Serous otitis media. 592

What’s the finding?
Frog-like position.
593
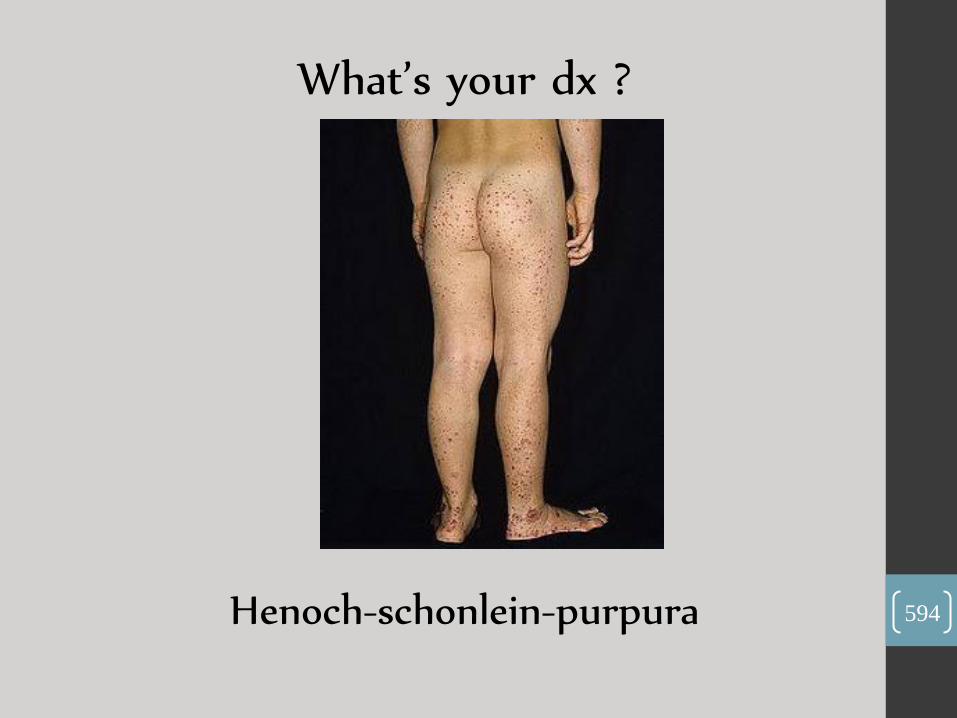
What’s your dx ?
Henoch-schonlein-purpura 594

What’s the finding?
Angular cheilitis. 595

What’s your dx ?
Mastoiditis. 596
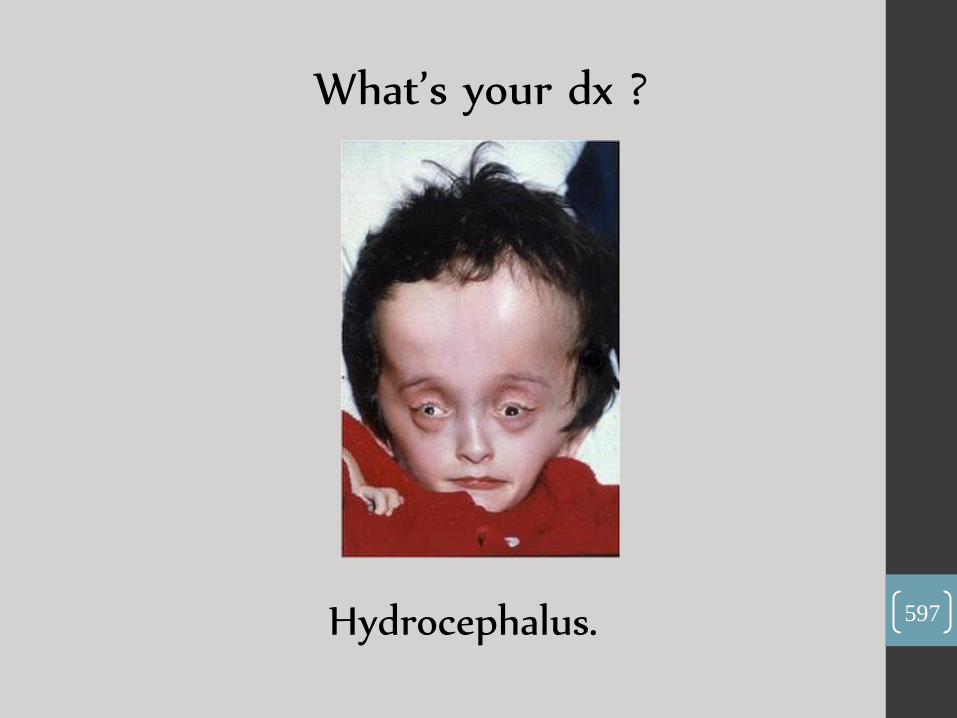
What’s your dx ?
Hydrocephalus. 597
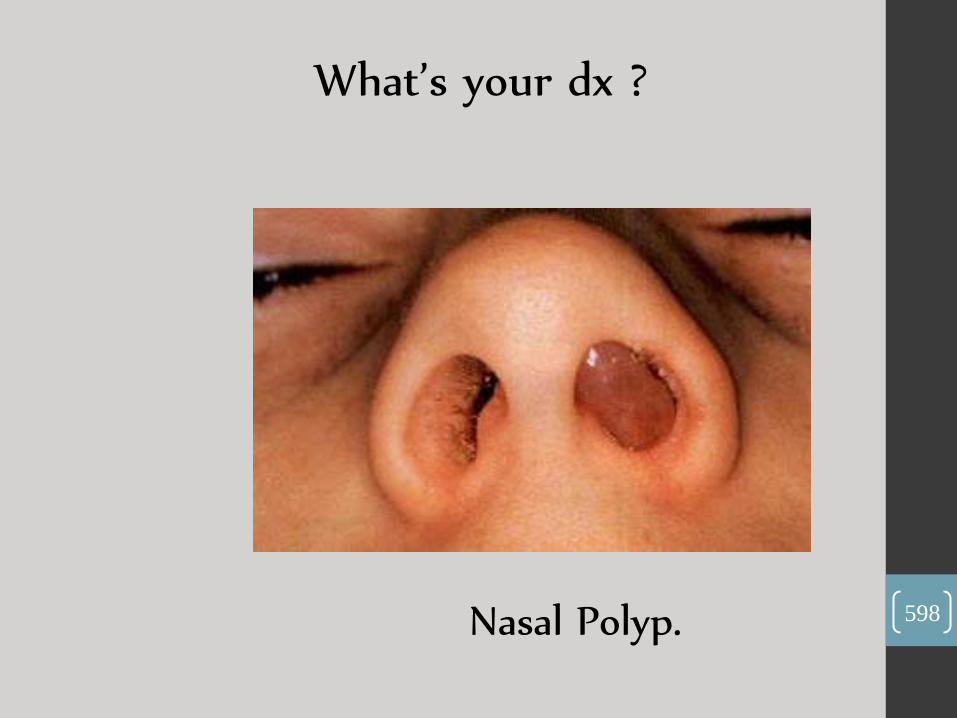
What’s your dx ?
Nasal Polyp. 598
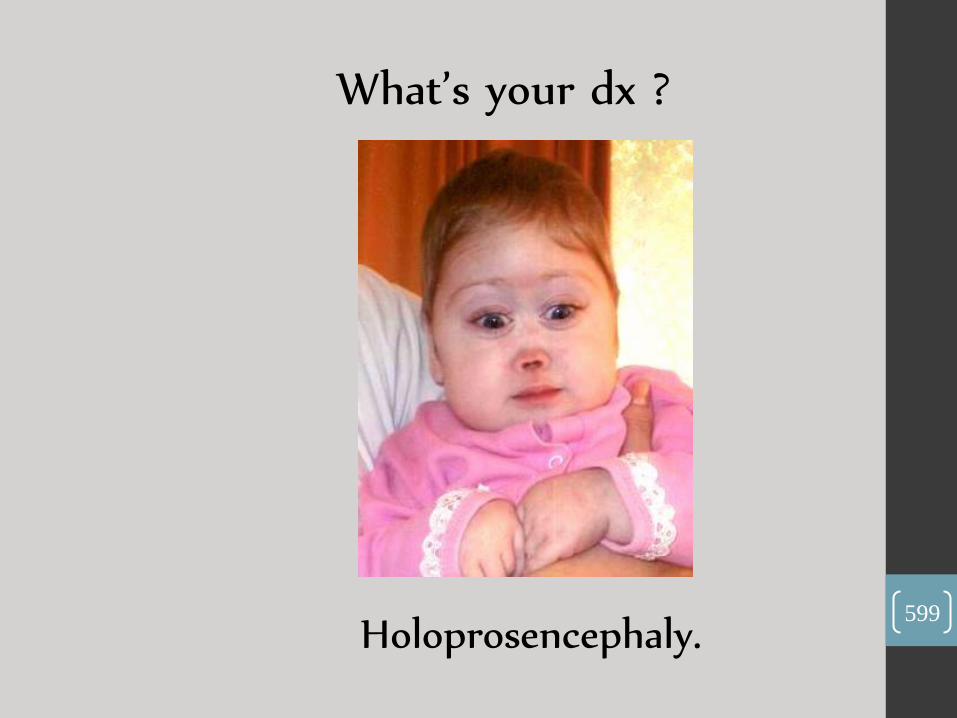
What’s your dx ?
Holoprosencephaly. 599
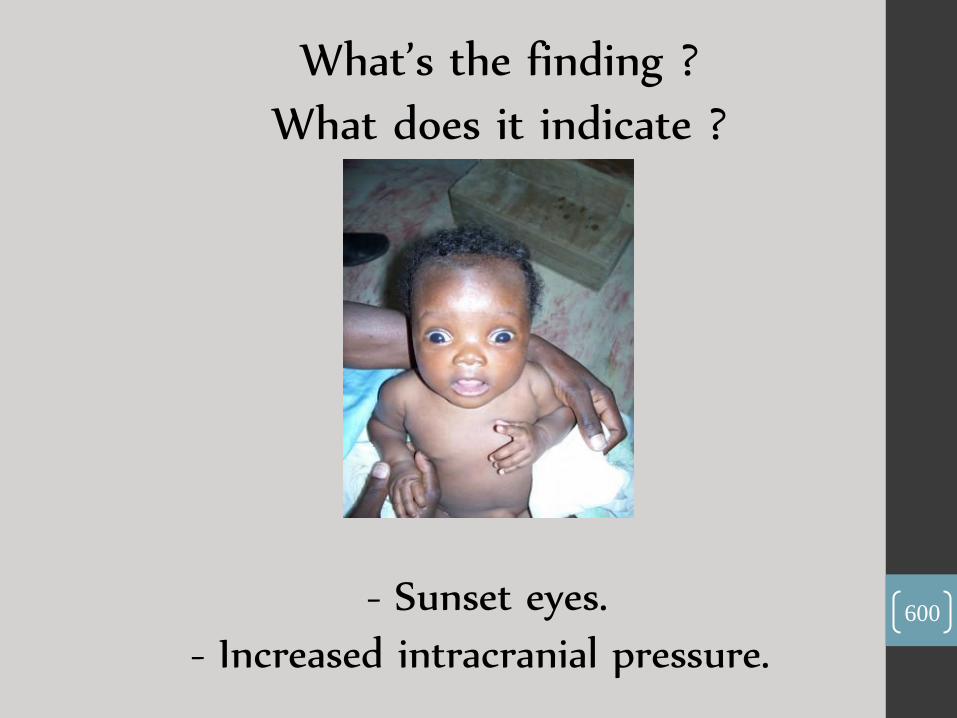
What’s the finding ?
What does it indicate ?
- Sunset eyes.
- Increased intracranial pressure. 600


تتقدم لجنة إلطب إلبشري من جميع إلزملاء
وإلزميلات من إلدفع إلسابقة بأ سمى معاني إلشكر
وإلا متنان لجهودهم في جمع هذه الاس ئلة فلاولاهم
.يرى إلنور لهذإ إلعمل أ ن لم يكن
...فشكرإ جزيلا لهم

إلعالمينوأ خر دعوإنا أ ن إلحمد لله رب