Embed Size (px)
Citation preview

SEMMELWEIS 200
2018. JÚNIUS NŐGYÓGYÁSZATI ÉS SZÜLÉSZETI TOVÁBBKÉPZŐ SZEMLE 103
SEMMELWEIS 200
Clinical chorioamnionitis at term: New insights into the etiology, microbiology, and the fetal, maternal and amniotic cavity inflammatory responses
Roberto Romero1-4, Nardhy Gomez-Lopez1,5,6, Juan Pedro Kusanovic1,7, Percy Pacora1,5,
Bogdan Panaitescu1,5, Offer Erez1,5, Bo H. Yoon1,8
1 Perinatology Research Branch, Division of Obstetrics and Maternal-Fetal Medicine, Division of Intramural Research, Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health, U S Department of Health and Human Services, Bethesda, Maryland, and Detroit, Michigan, USA
2 Department of Obstetrics and Gynecology, University of Michigan, Ann Arbor, Michigan, USA3 Department of Epidemiology and Biostatistics, Michigan State University, East Lansing, Michigan, USA4 Center for Molecular Medicine and Genetics, Wayne State University, Detroit, Michigan, USA5 Department of Obstetrics and Gynecology, Wayne State University School of Medicine, Detroit, Michigan, USA6 Department of Immunology, Microbiology and Biochemistry, Wayne State University School of Medicine, Detroit, Michigan, USA7 Division of Obstetrics and Gynecology, Faculty of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile8 Department of Obstetrics and Gynecology, Seoul National University College of Medicine, Seoul, Republic of Korea
Roberto Romero, M.D., D.Med.Sci.

SEMMELWEIS 200
104 NŐGYÓGYÁSZATI ÉS SZÜLÉSZETI TOVÁBBKÉPZŐ SZEMLE 2018. JÚNIUS
Abstract
Clinical chorioamnionitis is the most common infection related diagnosis made in labor and delivery units worldwide. It is traditionally believed to be due to microbial invasion of the amniotic cavity, which elicits a maternal inflammatory response characterized by maternal fever, uterine tenderness, maternal tachycardia and leukocytosis. The condition is often as-sociated with fetal tachycardia and a foul smelling amniotic fluid. Recent studies in which amniocentesis has been used to characterize the microbiologic state of the amniotic cavity and the inflammatory response show that only 60% of patients with the diagnosis of clinical chorioamnionitis have proven infection using culture or molecular microbiologic techniques. The remainder of the patients have intra-amniotic inflammation without demonstrable microorganisms or a maternal systemic inflammatory response (fever) in the absence of in-tra-amniotic inflammation. The latter cases often represent a systemic inflammatory response after epidural anesthesia/analgesia has been administered. The most common microorganisms are Ureaplasma species and Gardnerella vaginalis. In the presence of ruptured membranes, the frequency of infection is 70%, which is substantially higher than patients who have intact membranes (25%). The amniotic fluid inflammatory response is characterized by an infiltra-tion of neutrophils and monocytes. Both cell types are activated in the presence of infection and can produce inflammatory cytokines. The white blood cells in the amniotic fluid can be of fetal or maternal origin. The maternal inflammatory response is characterized by an elevation in the concentration of pyrogenic cytokines. The cytokine plasma concentrations in the fetal circulation are elevated even if there is no evidence of an intra-amniotic inflam-matory response suggesting that maternal plasma cytokines may cross the placental barrier and induce a mild fetal inflammatory response. Placental pathology is of limited value in the diagnosis of proven intra-amniotic infection. The clinical criteria traditionally used in clinical medicine have accuracy around 50% and therefore, they cannot distinguish between patients with a proven intra-amniotic infection and those with intra-amniotic inflammation alone. Analysis of amniotic fluid with a bedside test for MMP-8 can allow the rapid identification of the patient at risk for infection and may decrease the need for antibiotic administration to neonates. An important consideration is whether antibiotics effective against Ureaplasma species should be administered to patients with clinical chorioamnionitis, given that these genital mycoplasmas are the most common organisms found in the amniotic fluid. The emer-gent picture is that clinical chorioamnionitis is a heterogeneous syndrome, which requires further study to optimize maternal and neonatal outcomes.
Keywords
Intra-amniotic infection, maternal fever, fetal tachycardia, amniotic fluid, cytokines, neutrophils, monocytes, MMP-8, biomarkers, rapid diagnosis, treatment, antibiotics,
maternal morbidity, neonatal morbidity

SEMMELWEIS 200
2018. JÚNIUS NŐGYÓGYÁSZATI ÉS SZÜLÉSZETI TOVÁBBKÉPZŐ SZEMLE 105
IntroductionClinical chorioamnionitis is the most common infection-re-lated diagnosis made in labor and delivery units worldwide [1-4]. The standard clinical definition refers to the presence of maternal fever associated with clinical signs (i.e. foul smelling discharge, uterine tenderness, maternal and fetal tachycardia) as well as laboratory abnormalities (i.e. leukocytosis) [5, 6]. These signs are thought to be manifestations of both local and systemic maternal-fetal inflammatory processes initiat-ed in response to microbial invasion of the amniotic cavity (MIAC) [7-13].
Clinical chorioamnionitis at term is associated with a 2- to 4-fold increase in endometritis [14], wound infection [14], septic pelvic thrombophlebitis [3, 14], pelvic abscess [3, 14], maternal admission to the intensive care unit [3, 15], and postpartum hemorrhage [3, 16]. Importantly, neonates born to mothers with clinical signs of chorioamnionitis have a high risk of neonatal mortality [1], short- and long-term complications such as neonatal sepsis [17-19], meconium aspiration syndrome [20, 21], stillbirth [22, 23], and neurodevelopmental disorders including cerebral palsy [24-35].
Although this condition is common, affecting thousands of women daily and has been known for centuries as a precursor of puerperal (or childbed) fever [36, 37], new information has emerged which has characterized, for the first time, the mi-crobiology and inflammatory responses in the mother, fetus, and amniotic cavity. This article will review new insight gained from studies published in the last three years.
The syndrome of clinical chorioamnionitis: evidence for microbiologic and inflammatory heterogeneityAmong patients with clinical chorioamnionitis, we have iden ti-fied three distinct groups [38]: 1) patients who have intra-amni-otic infection, defined by the presence of an elevated concentra-tion of interleukin (IL)-6 [a marker of inflammation [39]] and the presence of microorganisms; 2) patients who have sterile intra-amniotic inflammation, in which no organisms can be detected using standard cultivation techniques or 16S RNA broad assays, although they have an elevated amniotic fluid IL-6; and 3) patients who have neither intra-amniotic inflammation or microorganisms in the amniotic cavity. The frequency with which these conditions are present varies according to whether the membranes are ruptured at the time of amniocentesis to assess the microbial state of the amniotic cavity [38]. When the membranes are intact, the frequency of intra-amniotic infection
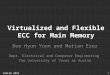
is 25%, while it is 70% when the membranes are ruptured [38]. The relative contribution of the different entities presenting as clinical chorioamnionitis are illustrated in Figure 1. A small group of patients has microbial invasion of the amniotic cavity without inflammation.
The mechanism responsible for sterile intra-amniotic inflam-mation have not been defined [38, 40-42] and could represent inflammation induced by danger signals (or alarmins) [43-47], or alternatively, infections which have escaped detection with current cultivation and molecular microbiologic techniques [48-54]. For example, it is possible that deep DNA and RNA sequencing may identify organisms which are present below the level of detection of culture and 16S PCR; however, this question remains to be addressed.
What are the microorganisms found in the amniotic cavity in clinical chorioamnionitis at term?The original study describing the microbiology of clinical chorioamnionitis at term was performed using cultivation techniques of amniotic fluid obtained with transcervical catheters placed in the amniotic cavity [5]. This approach may not have provided an accurate description of the microbiology of clinical chorioamnionitis, since the placement of a transcervical catheter is frequently associated with contamination of the vaginal ecosystem. Conventional cultivation techniques cannot identify the entire microbial diversity of an ecological niche, because the conditions required for the growth of microorganisms in vitro are not known, and some organisms are, therefore, considered to be non-culturable [55]. By using both cultivation and molecular biology techniques (broad-range polymerase chain reaction coupled with electrospray ionization mass spectrometry or PCR/ESI-MS), it is possible to gain a more complete understanding of the microbiology of the amniotic cavity [56].
In a study of 46 women with clinical chorioamnionitis at term, amniotic fluid was obtained by transabdominal amniocen-tesis or at the time of Cesarean delivery under sterile conditions [38]. We found that conventional culture identified bacteria in the amniotic fluid from 46% (21/46) of the participants, while PCR/ESI-MS was positive for microorganisms in 59% (27/46) of the patients. The combination of these two approaches re-sulted in the detection of amniotic fluid microorganisms in 61% (28/46) of women with clinical chorioamnionitis at term [38]. Molecular microbiologic techniques identified more mi-croorganisms than cultivation; yet, some bacterial taxa were preferentially identified by each technique [38].

SEMMELWEIS 200
106 NŐGYÓGYÁSZATI ÉS SZÜLÉSZETI TOVÁBBKÉPZŐ SZEMLE 2018. JÚNIUS
Ureaplasma spp. and Gardnerella vaginalis are the most commonly identified microorganisms by cultivation and PCR/ESI-MS, respectively [38]. This has clinical implications, because the antibiotics used to treat patients with clinical chorioam-nionitis or puerperal endometritis do not include agents that eradicate infections due to Ureaplasma spp.
The cellular intra-amniotic inflammatory response: neu-trophils and monocytes in the amniotic fluidAn inflammatory response is characterized by cellular and soluble components. The typical changes in the soluble me-ditators are those that occur in the inflammatory cytokine network. However, cellular mediators are prominent, and mainly involve the innate immune response.
Using flow cytometry, we found that neutrophils are the most common leukocyte subset in the amniotic fluid, followed by monocytes; other white blood cells (such as lymphocytes and natural killer cells) are scarce in the amniotic fluid [57] (Figure 2). The absolute counts of neutrophils and monocytes
are significantly higher in patients with microorganisms found in the amniotic fluid than in those without detectable micro-organisms [57]. In addition, the profile of cytokine expression differs between monocytes and neutrophils; while neutrophils predominantly produce tumor necrosis factor (TNF)-α and macrophage inflammatory protein (MIP)-1β, monocytes ex-press higher levels of IL-1β and IL-1α [57]. These cytokines are implicated in both the process of parturition and host response against intra-amniotic infection [58-75].
Figure 2
Histological examination of amniotic fluid neutrophils and monocytes in women with clinical chorioamnionitis. A) Hematoxylin & Eosin staining shows the typical morphology of neutrophils (N, green arrow) and mono-cytes (M, red arrow) in the amniotic fluid of women with clinical chorio-amnionitis. Magnification 400X. Scale bars: 50μm. B) Immunofluores-cence of neutrophils and monocytes in the amniotic fluid of women with clinical chorioamnionitis. Neutrophils (CD15+ cells) are green, mono cytes (CD14+ cells) are red, and nuclei are blue (DAPI). Magnification 400X.
31.3%
6.7%
6.2%
6.6%
25,0% 70.0%
37.5%
16.7%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Intact membranes(n=16)
Rupture of membranes(n=30)
Sterile intra-amniotic inflammation
Intra-amniotic infection
No inflammation/infection
Microbial invasion of the amniotic cavity (without inflammation)
Figure 1
Prevalence of microbial-associated intra-amniotic inflammation and intra-amniotic inflammation without detectable microorganisms in patients with clinical signs of chorioamnionitis at term according to the status of the membranes at the time of amniocentesis (intact vs. ruptured). Microbial-associated intra-amniotic inflammation was diag-nosed in 70% (21/30) of the cases with rupture of membranes, and in 25% (4/16) of patients with intact membranes.

SEMMELWEIS 200
2018. JÚNIUS NŐGYÓGYÁSZATI ÉS SZÜLÉSZETI TOVÁBBKÉPZŐ SZEMLE 107
Amniotic fluid white blood cells can be of fetal or maternal origin Although traditionally considered to be of fetal origin [76, 77], neut rophils in amniotic fluid in cases of infection can be of maternal, fetal, or mixed (both) origin, as demonstrated by studies using DNA fingerprinting [78]. In general, we found that patients with intra-amniotic infection and preterm gestations had neutrophils of fetal origin, while those with intra-amniotic infection/inflammation at term had predominantly maternal neutrophils or a cellular infiltrate of mixed origin (maternal and fetal) [78]. Figure 3 shows the DNA fingerprinting of amniotic fluid neutrophils of fetal, maternal, or mixed (maternal and fetal) origin.
The soluble amniotic fluid inflammatory response: changes in the cytokine inflammatory network and lipidomeThe amniotic fluid concentrations of inflammatory cytokines [such as interferon gamma (IFN-γ), TNFα, IL-4, MIP-1β, and IL-8] are higher in patients with clinical chorioamnionitis at term than in women with spontaneous labor at term without intra-amniotic inflammation [75]. Of interest is that once a patient had intra-amniotic inflammation, the changes in the amniotic fluid cytokine network are similar in those with proven infection vs. those with intra-amniotic inflammation without demonstrable microorganisms [75].
16 7 831 31.2 17 18 8
16
16 7 8 31 31.217 18 8
16
167 9
27 31.2
17 18
13 1615
12 11 1410107
139 1210 9
12 11 1410107
139 1210 9
11 11 141010
1312 107 9
16 18 14 11X24
19
16 18 14 11X24
19
17 18 14X11
246
Amniotic Fluid
Neutrophil DNA
Fetal DNA
Maternal DNA
14
7 829 30
16 17 8 1217
167 9
28 2916 17
817
14
7 829 30
16 17 8 1217
11 10 119 12 11
8 913
10 911 9
1210
8 1113 8 11
11 10 119 12 11
8 913
X19 15
8 1118.2
24
18
X 1915
8 1020 24
16
X 1915
8 1118.2 24
18
Amniotic Fluid
Neutrophil DNA
Fetal DNA
Maternal DNA
16
6
7
8 28 15 16 811
3129 18 14
16 7 8 2816 8
2918 14
16 6 7
15 11312918 14
111213
11 810
13 2.2
10129 7 8 1012
1113
11 8 10 13 2.29 8 1012
1112
11 8 13
2.2 1012 7 10
X
X
Y
1116
1910 13
14 8
1021
22 29
X Y 1119 13 14
8 21 29
X 1116 10 14
8 1021 22
Amniotic Fluid
Neutrophil DNA
Fetal DNA
Maternal DNA
Feta
l Orig
inM
ater
nal
Orig
inFe
tal a
nd M
ater
nal O
rigin
A
B
C
Figure 3 DNA fingerprinting of amniotic fluid neutrophils
DNA fingerprinting of purified amniotic fluid neutrophils of fetal (A), maternal (B) or mixed (C) origin, the fetus (umbilical cord), and the mother (buffy coat from peripheral blood) is shown in electropherograms. Each electropherogram contains 16 genetic sites: D3S1358, TH01, D21S11, D18S51, Penta_E, D5S818, D13S317, D7S820, D16S539, CSF1PO, Penta_D, X- and Y-specific amalogenin genes, vWA, D8S1179, TPOX, and FGA. Each electropherogram was separated into three sections: blue, green, and black. Each color indicates the dye used for the PCR multiplex: blue represents the genes amplified using fluorescein (FL dye), green represents the genes amplified using 6-carboxy-4',5'-dichloro-2',7'-dimethoxyflu-orescein (JOE dye), and black represents the genes amplified using tetramethylrhodamine (TMR dye). Each genetic site has STR alleles, which is represented by peaks. The number next to/above each STR allele (peak) is the number of repeats for each STR allele.

SEMMELWEIS 200
108 NŐGYÓGYÁSZATI ÉS SZÜLÉSZETI TOVÁBBKÉPZŐ SZEMLE 2018. JÚNIUS
Given that lipids are important mediators of the inflamma-tory response, we have examined the behavior of bioactive lipids using discovery techniques (i.e. lipidomics) [79]. An elevated leukotriene B4 (LTB4) was associated with the presence of microorganisms in the amniotic cavity [80]. Therefore, lipid mediators can be assessed with mass spectrometry techniques could have value as biomarkers [80].
How well do clinical criteria perform in the identification of proven intra-amniotic infection? Only 54% of patients with the diagnosis of clinical chorio-amnionitis at term have intra-amniotic inflammation and detectable bacteria [38]. These findings indicate that only half of the women with clinical chorioamnionitis at term may benefit from antibiotic administration. Therefore, we evaluated the diagnostic performance and accuracy of clinical signs for the diagnosis of clinical chorioamnionitis using the “gold standard” [a combination of cultivation and molecular biology techniques [56]] for the identification of intra-amniotic infection [81].
We reported that clinical signs of chorioamnionitis do not accurately identify patients with intra-amniotic infection [81]. Maternal and fetal tachycardia, as well as maternal leukocytosis, have low specificity (5%–30%), whereas foul-smelling amniotic fluid and uterine tenderness have poor sensitivity (<15%) for the diagnosis of intra-amniotic infection [81]. These findings call for the development of novel approaches to facilitate the rapid identification of bacteria in the amniotic fluid and reevaluation of the management of clinical chorioamnionitis at term.
The maternal plasma cytokine profileMost of the signs of clinical chorioamnionitis (except for fetal tachycardia and foul-smelling amniotic fluid) are thought to reflect a maternal inflammatory response to microbial invasion of the amniotic cavity [4, 82]. Maternal plasma concentrations of pyrogenic cytokines (IL-1β, IL-2, IL-6, IFN-γ, and TNF-α) are higher in patients with clinical chorioamnionitis at term than in those with spontaneous labor at term without clinical chorioamnionitis [83]. However, the maternal plasma concentrations of cytokines are not significantly different among the 3 major subgroups of patients with clinical chorioamnionitis at term [83]. In addition, women with clinical chorioamnionitis at term without intra-amniotic inflammation have greater maternal plasma concentrations of pyrogenic cytokines than those with spontaneous labor
at term without this clinical condition [83]. These findings indicate that the absolute concentration of cytokines in the maternal plasma cannot be used to identify women who have bacteria in the amniotic fluid and that the assessment of the amniotic fluid is required to identify intra-amniotic inflammation and/or infection.
Umbilical cord plasma cytokine profile in the context of a systemic maternal inflammatory responseNeonates born to mothers with clinical chorioamnionitis are at risk for sepsis [3, 17-19, 32, 84-89], meconium aspiration syndrome [17, 90-94], neonatal encephalopathy [31, 34, 95-97], and long-term neurodevelopmental disabilities including cognitive impairment [98-101] and cerebral palsy [27, 28, 30, 34, 35, 86, 102-104], as well as neonatal death [1, 22, 24, 88, 105]. Such adverse neonatal outcomes may be attributed to the effects of a maternal systemic inflammatory response on the fetus [83] and/or the local inflammatory response in the amniotic cavity [38, 75].
Neonates born to mothers with clinical chorioamnionitis at term have higher umbilical cord plasma concentrations of several inflammatory cytokines (IL-6, IL-12p70, IL-16, IL-13, IL-4, IL-10 and IL-8) compared to those born to mothers with spontaneous labor at term without this clinical condition [106]. Interestingly, neonates born to mothers with clinical chorioamnionitis at term without intra-amniotic inflam-mation also have higher concentrations of inflammatory cytokines (IL-6, IL-12p70, IL-13, IL-4, IL-5, and IL-8) than neonates not exposed to clinical chorioamnionitis, suggesting that maternal fever in the absence of intra-amniotic inflam-mation leads to a change in the fetal cytokine network [106]. In addition, there are significant and positive correlations between maternal and umbilical cord plasma IL-6 and IL-8 concentrations consistent with placental transfer of cytokines [106]. All neonates born to mothers with proven intra-am-niotic infection were diagnosed with fetal inflammatory response syndrome (FIRS) [106].
Can placental pathology identify the patient with intra-amniotic infection?Examination of the placenta, the largest human biopsy, can provide information about fetal exposure to intra-amniotic inflammation or infection [10, 11, 13, 24, 26, 33, 107-124]. Indeed, inflammation of the umbilical cord or chorionic vessels represents a fetal response and is indicative that

SEMMELWEIS 200
2018. JÚNIUS NŐGYÓGYÁSZATI ÉS SZÜLÉSZETI TOVÁBBKÉPZŐ SZEMLE 109
the fetus was exposed to inflammatory stimuli before birth [113]. Therefore, we examined the diagnostic performance of placental histologic features of acute inflammation in the identification of intra-amniotic infection and FIRS in patients with clinical chorioamnionitis at term [125]. Acute histologic chorioamnionitis and funisitis are indeed associated with the presence of intra-amniotic infection and FIRS [125]. However, current placental histopathologic methods have limitations in identifying whether the fetus was exposed to microorganisms in the amniotic cavity [125]. The available data suggest that placental examination is neither sensitive nor specific for the identification of intra-amniotic infection, because acute histologic chorioamnionitis and funisitis can be observed when there is intra-amniotic inflammation in the absence of demonstrable microorganisms.
A rapid MMP-8 test for the identification of intra-amniotic inflammationA rapid test which utilizes neutrophil collagenase or MMP-8 has been made available for the diagnosis of intra-amniotic inflammation [126-133]. This test in patients with intra-amniotic inflammation and clinical chorioamnionitis has the following diagnostic indices, predictive values, and likelihood ratios: sensitivity of 82.4% (28/34), specificity of 90% (9/10), positive predictive value of 96.6% (28/29), negative predictive value of 60% (9/15), positive likelihood ratio 8.2 (95% CI 1.3–53.2), and negative likelihood ratio 0.2 (95% CI 0.1–0.4) [134].
In patients with intra-amniotic infection and clinical cho-rioamnionitis, the rapid MMP-8 test has a sensitivity of 91.7% (22/24), specificity of 65% (13/20), positive predictive value of 75.9% (22/29), negative predictive value of 86.7% (13/15), positive likelihood ratio of 2.6 (95% CI 1.4–4.8), and negative likelihood ratio of 0.1 (95% CI 0.03–0.5) [134].
In addition, the rapid MMP-8 test has a significantly higher specificity than the ELISA IL-6 test in the identification of intra-amniotic inflammation [66.7% (14/21) vs. 42.9% (9/21); p=0.03] [134]. Importantly, the rapid MMP-8 test has 100% sensitivity and 100% negative predictive value in the identifi-cation of neonates affected with FIRS [134].
This study showed that a rapid MMP-8 point-of-care test can be used for the diagnosis of intra-amniotic inflammation and to identify the mother at risk of delivering a neonate with systemic inflammation among patients with clinical chorio-amnionitis at term [134].
ConclusionsA series of systematic studies in patients with clinical chorio-amnionitis at term have revealed the following:
• Clinical chorioamnionitis at term is a heterogeneous condition, and only a fraction of these patients have proven intra-amniotic infection
• The frequency of infection is higher when the chorioamni-otic membranes are ruptured, rather than intact (70% vs 25%)
• The most common organisms are Ureaplasma spp. and Gardnerella vaginalis – this is important because most treat-ment approaches in clinical obstetrics and neonatology do not provide appropriate coverage for genital mycoplasmas
• The cellular intra-amniotic inflammatory response is characterized by an influx of neutrophils and monocytes
• The soluble intra-amniotic inflammatory response is char-acterized by elevated concentrations of the major inflammatory cytokines
• The maternal plasma cytokines are elevated in patients with clinical chorioamnionitis at term; however, the con-centrations of these proteins cannot distinguish between patients who have proven intra-amniotic infection and those with intra-amniotic inflammation without demonstrable microorganisms
• The fetal concentrations of inflammatory cytokines are elevated in neonates born to mothers with clinical chorio-amnionitis compared to those without clinical chorioamni-onitis at term. There is indirect evidence that elevations in neonatal inflammatory concentrations may reflect a systemic inflammatory response in the mother, even in the absence of intra-amniotic inflammation (this may occur in cases of epidural-induced fever)
• Placental pathologic examination to detect acute histologic chorioamnionitis, funisitis, or chorionic vasculitis is neither specific nor sensitive for the identification of patients with proven intra-amniotic infection
• Analysis of amniotic fluid is the only definitive way to make a diagnosis of intra-amniotic infection in patients with clinical chorioamnionitis at term
• Potential biomarkers for intra-amniotic inflammation, which can be implemented at the bedside, is an MMP-8 rapid test which detects neutrophil collagenase
• Future studies are required to determine if noninvasive collection of amniotic fluid with a special device in patients who have ruptured membranes can be of clinical value to diagnose intra-amniotic infection/inflammation

SEMMELWEIS 200
110 NŐGYÓGYÁSZATI ÉS SZÜLÉSZETI TOVÁBBKÉPZŐ SZEMLE 2018. JÚNIUS
REFERENCES
1. Malloy MH. Chorioamnionitis: epidemiology of newborn management and outcome
United States 2008. J Perinatol. 2014;34(8):611-5.
2. Tita AT, Andrews WW. Diagnosis and management of clinical chorioamnionitis. Clin
Perinatol. 2010;37(2):339-54.
3. Rouse DJ, Landon M, Leveno KJ, Leindecker S, Varner MW, Caritis SN, et al. The
Maternal-Fetal Medicine Units cesarean registry: chorioamnionitis at term and its dura-
tion-relationship to outcomes. Am J Obstet Gynecol. 2004;191(1):211-6.
4. Newton ER. Chorioamnionitis and intraamniotic infection. Clin Obstet Gynecol.
1993;36(4):795-808.
5. Gibbs RS, Blanco JD, St Clair PJ, Castaneda YS. Quantitative bacteriology of amniotic
fluid from women with clinical intraamniotic infection at term. J Infect Dis. 1982;145(1):1-8.
6. Gibbs RS, Dinsmoor MJ, Newton ER, Ramamurthy RS. A randomized trial of intra-
partum versus immediate postpartum treatment of women with intra-amniotic infection.
Obstet Gynecol. 1988;72(6):823-8.
7. Gilstrap LC, 3rd, Cox SM. Acute chorioamnionitis. Obstet Gynecol Clin North Am.
1989;16(2):373-9.
8. Gibbs RS, Duff P. Progress in pathogenesis and management of clinical intraamniotic
infection. Am J Obstet Gynecol. 1991;164(5 Pt 1):1317-26.
9. Willi MJ, Winkler M, Fischer DC, Reineke T, Maul H, Rath W. Chorioamnionitis:
elevated interleukin-6 and interleukin-8 concentrations in the lower uterine segment. J
Perinat Med. 2002;30(4):292-6.
10. Lee SE, Romero R, Kim CJ, Shim SS, Yoon BH. Funisitis in term pregnancy is as-
sociated with microbial invasion of the amniotic cavity and intra-amniotic inflammation.
J Matern Fetal Neonatal Med. 2006;19(11):693-7.
11. Lee SE, Romero R, Jung H, Park CW, Park JS, Yoon BH. The intensity of the fetal
inflammatory response in intraamniotic inflammation with and without microbial invasion
of the amniotic cavity. Am J Obstet Gynecol. 2007;197(3):294 e1-6.
12. Gotsch F, Romero R, Kusanovic JP, Mazaki-Tovi S, Pineles BL, Erez O, et al. The
fetal inflammatory response syndrome. Clin Obstet Gynecol. 2007;50(3):652-83.
13. Redline RW. Inflammatory response in acute chorioamnionitis. Semin Fetal Neonatal
Med. 2012;17(1):20-5.
14. Hauth JC, Gilstrap LC, 3rd, Hankins GD, Connor KD. Term maternal and neonatal
complications of acute chorioamnionitis. Obstet Gynecol. 1985;66(1):59-62.
15. Rojas-Suarez J, Paternina-Caicedo AJ, Miranda J, Mendoza R, Duenas-Castel C,
Bourjeily G. Comparison of severity-of-illness scores in critically ill obstetric patients:
a 6-year retrospective cohort. Crit Care Med. 2014;42(5):1047-54.
16. Mark SP, Croughan-Minihane MS, Kilpatrick SJ. Chorioamnionitis and uterine
function. Obstet Gynecol. 2000;95(6 Pt 1):909-12.
17. Yoder PR, Gibbs RS, Blanco JD, Castaneda YS, St Clair PJ. A prospective, con-
trolled study of maternal and perinatal outcome after intra-amniotic infection at term.
Am J Obstet Gynecol. 1983;145(6):695-701.
18. Yancey MK, Duff P, Kubilis P, Clark P, Frentzen BH. Risk factors for neonatal sepsis.
Obstet Gynecol. 1996;87(2):188-94.
19. Ladfors L, Tessin I, Mattsson LA, Eriksson M, Seeberg S, Fall O. Risk factors for
neonatal sepsis in offspring of women with prelabor rupture of the membranes at 34-42
weeks. J Perinat Med. 1998;26(2):94-101.
20. Rao S, Pavlova Z, Incerpi MH, Ramanathan R. Meconium-stained amniotic fluid and
neonatal morbidity in near-term and term deliveries with acute histologic chorioamnionitis
and/or funisitis. J Perinatol. 2001;21(8):537-40.
21. Greenwell EA, Wyshak G, Ringer SA, Johnson LC, Rivkin MJ, Lieberman E. In-
trapartum temperature elevation, epidural use, and adverse outcome in term infants.
Pediatrics. 2012;129(2):e447-54.
22. Moyo SR, Hagerstrand I, Nystrom L, Tswana SA, Blomberg J, Bergstrom S, et
al. Stillbirths and intrauterine infection, histologic chorioamnionitis and microbiological
findings. Int J Gynaecol Obstet. 1996;54(2):115-23.
23. Han YW, Fardini Y, Chen C, Iacampo KG, Peraino VA, Shamonki JM, et al. Term still-
birth caused by oral Fusobacterium nucleatum. Obstet Gynecol. 2010;115(2 Pt 2):442-5.
24. Hillier SL, Krohn MA, Kiviat NB, Watts DH, Eschenbach DA. Microbiologic causes
and neonatal outcomes associated with chorioamnion infection. Am J Obstet Gynecol.
1991;165(4 Pt 1):955-61.
25. McGregor JA. Maternal and fetal infection. Curr Opin Obstet Gynecol. 1991;3(1):15-23.
26. van Hoeven KH, Anyaegbunam A, Hochster H, Whitty JE, Distant J, Crawford
C, et al. Clinical significance of increasing histologic severity of acute inflammation in
the fetal membranes and umbilical cord. Pediatr Pathol Lab Med. 1996;16(5):731-44.
27. Grether JK, Nelson KB. Maternal infection and cerebral palsy in infants of normal
birth weight. JAMA. 1997;278(3):207-11.
28. Wu YW, Colford JM, Jr. Chorioamnionitis as a risk factor for cerebral palsy: A me-
ta-analysis. JAMA. 2000;284(11):1417-24.
29. Impey L, Greenwood C, MacQuillan K, Reynolds M, Sheil O. Fever in labour and
neonatal encephalopathy: a prospective cohort study. BJOG. 2001;108(6):594-7.
30. Wu YW, Escobar GJ, Grether JK, Croen LA, Greene JD, Newman TB. Chorioamni-
onitis and cerebral palsy in term and near-term infants. JAMA. 2003;290(20):2677-84.
31. Blume HK, Li CI, Loch CM, Koepsell TD. Intrapartum fever and chorioamnionitis
as risks for encephalopathy in term newborns: a case-control study. Dev Med Child
Neurol. 2008;50(1):19-24.
32. Soraisham AS, Singhal N, McMillan DD, Sauve RS, Lee SK, Canadian Neonatal N.
A multicenter study on the clinical outcome of chorioamnionitis in preterm infants. Am
J Obstet Gynecol. 2009;200(4):372 e1-6.
33. Lee SM, Park JW, Kim BJ, Park CW, Park JS, Jun JK, et al. Acute histologic cho-
rioamnionitis is a risk factor for adverse neonatal outcome in late preterm birth after
preterm premature rupture of membranes. PLoS One. 2013;8(12):e79941.
34. Hagberg H, Wennerholm UB, Savman K. Sequelae of chorioamnionitis. Curr Opin
Infect Dis. 2002;15(3):301-6.
35. Nelson KB. The epidemiology of cerebral palsy in term infants. Ment Retard Dev
Disabil Res Rev. 2002;8(3):146-50.
36. Kirkland T. A Treatise on Child-bed Fevers: And on the Methods of Preventing Them.
Being a Supplement to the Books Lately Written on the Subject. To which are Prefixed
Two Dissertations, The One on the Brain and Nerves; the Other on the Sympathy of
the Nerves, and on Different Kinds of Irritability. By Thomas Kirkland, MD: R. Baldwin,
No. 47, and W. Dawson, No. 7, Pater-Noster-Row; 1774.
37. DeLacy M. Puerperal fever in eighteenth-century Britain. Bulletin of the History of
Medicine. 1989;63(4):521.
38. Romero R, Miranda J, Kusanovic JP, Chaiworapongsa T, Chaemsaithong P, Martinez
A, et al. Clinical chorioamnionitis at term I: microbiology of the amniotic cavity using
cultivation and molecular techniques. J Perinat Med. 2015;43(1):19-36.
39. Yoon BH, Romero R, Moon JB, Shim SS, Kim M, Kim G, et al. Clinical significance
of intra-amniotic inflammation in patients with preterm labor and intact membranes. Am
J Obstet Gynecol. 2001;185(5):1130-6.
40. Romero R, Miranda J, Chaiworapongsa T, Korzeniewski SJ, Chaemsaithong P,
Gotsch F, et al. Prevalence and clinical significance of sterile intra-amniotic inflam-
mation in patients with preterm labor and intact membranes. Am J Reprod Immunol.
2014;72(5):458-74.
41. Romero R, Miranda J, Chaiworapongsa T, Chaemsaithong P, Gotsch F, Dong Z, et
al. Sterile intra-amniotic inflammation in asymptomatic patients with a sonographic short
cervix: prevalence and clinical significance. J Matern Fetal Neonatal Med. 2014:1-17.
42. Romero R, Miranda J, Chaemsaithong P, Chaiworapongsa T, Kusanovic JP, Dong
Z, et al. Sterile and microbial-associated intra-amniotic inflammation in preterm prelabor
rupture of membranes. J Matern Fetal Neonatal Med. 2015;28(12):1394-409.
43. Chaiworapongsa T, Erez O, Kusanovic JP, Vaisbuch E, Mazaki-Tovi S, Gotsch F, et
al. Amniotic fluid heat shock protein 70 concentration in histologic chorioamnionitis, term
and preterm parturition. J Matern Fetal Neonatal Med. 2008;21(7):449-61.
44. Romero R, Chaiworapongsa T, Alpay Savasan Z, Xu Y, Hussein Y, Dong Z, et al.
Damage-associated molecular patterns (DAMPs) in preterm labor with intact mem-
branes and preterm PROM: a study of the alarmin HMGB1. J Matern Fetal Neonatal
Med. 2011;24(12):1444-55.
45. Romero R, Chaiworapongsa T, Savasan ZA, Hussein Y, Dong Z, Kusanovic JP,
et al. Clinical chorioamnionitis is characterized by changes in the expression of the
alarmin HMGB1 and one of its receptors, sRAGE. J Matern Fetal Neonatal Med.
2012;25(6):558-67.
46. Gomez-Lopez N, Romero R, Plazyo O, Panaitescu B, Furcron AE, Miller D, et al.
Intra-Amniotic Administration of HMGB1 Induces Spontaneous Preterm Labor and Birth.
Am J Reprod Immunol. 2016;75(1):3-7.

SEMMELWEIS 200
2018. JÚNIUS NŐGYÓGYÁSZATI ÉS SZÜLÉSZETI TOVÁBBKÉPZŐ SZEMLE 111
47. Plazyo O, Romero R, Unkel R, Balancio A, Mial TN, Xu Y, et al. HMGB1 Induces an
Inflammatory Response in the Chorioamniotic Membranes That Is Partially Mediated
by the Inflammasome. Biol Reprod. 2016;95(6):130.
48. Baschat AA, Towbin J, Bowles NE, Harman CR, Weiner CP. Prevalence of viral
DNA in amniotic fluid of low-risk pregnancies in the second trimester. J Matern Fetal
Neonatal Med. 2003;13(6):381-4.
49. Baschat AA, Towbin J, Bowles NE, Harman CR, Weiner CP. Is adenovirus a fetal
pathogen? Am J Obstet Gynecol. 2003;189(3):758-63.
50. Srinivas SK, Ma Y, Sammel MD, Chou D, McGrath C, Parry S, et al. Placental
inflammation and viral infection are implicated in second trimester pregnancy loss. Am
J Obstet Gynecol. 2006;195(3):797-802.
51. DiGiulio DB, Romero R, Amogan HP, Kusanovic JP, Bik EM, Gotsch F, et al. Microbial
prevalence, diversity and abundance in amniotic fluid during preterm labor: a molecular
and culture-based investigation. PLoS One. 2008;3(8):e3056.
52. Miller JL, Harman C, Weiner C, Baschat AA. Perinatal outcomes after second
trimester detection of amniotic fluid viral genome in asymptomatic patients. J Perinat
Med. 2009;37(2):140-3.
53. Tsekoura EA, Konstantinidou A, Papadopoulou S, Athanasiou S, Spanakis N,
Kafetzis D, et al. Adenovirus genome in the placenta: association with histological
chorioamnionitis and preterm birth. J Med Virol. 2010;82(8):1379-83.
54. DiGiulio DB, Romero R, Kusanovic JP, Gomez R, Kim CJ, Seok KS, et al. Preva-
lence and diversity of microbes in the amniotic fluid, the fetal inflammatory response,
and pregnancy outcome in women with preterm pre-labor rupture of membranes. Am
J Reprod Immunol. 2010;64(1):38-57.
55. Stewart EJ. Growing unculturable bacteria. J Bacteriol. 2012;194(16):4151-60.
56. Romero R, Miranda J, Chaiworapongsa T, Chaemsaithong P, Gotsch F, Dong Z,
et al. A novel molecular microbiologic technique for the rapid diagnosis of microbial
invasion of the amniotic cavity and intra-amniotic infection in preterm labor with intact
membranes. Am J Reprod Immunol. 2014;71(4):330-58.
57. Martinez-Varea A, Romero R, Xu Y, Miller D, Ahmed AI, Chaemsaithong P, et al.
Clinical chorioamnionitis at term VII: the amniotic fluid cellular immune response. J
Perinat Med. 2017;45(5):523-38.
58. Romero R, Manogue KR, Mitchell MD, Wu YK, Oyarzun E, Hobbins JC, et al. Infec-
tion and labor. IV. Cachectin-tumor necrosis factor in the amniotic fluid of women with
intraamniotic infection and preterm labor. Am J Obstet Gynecol. 1989;161(2):336-41.
59. Romero R, Mazor M, Sepulveda W, Avila C, Copeland D, Williams J. Tumor necrosis
factor in preterm and term labor. Am J Obstet Gynecol. 1992;166(5):1576-87.
60. Fortunato SJ, Menon R. Distinct molecular events suggest different pathways
for preterm labor and premature rupture of membranes. Am J Obstet Gynecol.
2001;184(7):1399-405; discussion 405-6.
61. Fortunato SJ, Menon R, Lombardi SJ. Role of tumor necrosis factor-alpha in the
premature rupture of membranes and preterm labor pathways. Am J Obstet Gynecol.
2002;187(5):1159-62.
62. Moore RM, Mansour JM, Redline RW, Mercer BM, Moore JJ. The physiology of
fetal membrane rupture: insight gained from the determination of physical properties.
Placenta. 2006;27(11-12):1037-51.
63. Kumar D, Fung W, Moore RM, Pandey V, Fox J, Stetzer B, et al. Proinflammatory
cytokines found in amniotic fluid induce collagen remodeling, apoptosis, and biophys-
ical weakening of cultured human fetal membranes. Biol Reprod. 2006;74(1):29-34.
64. Menon R, Fortunato SJ. Infection and the role of inflammation in preterm premature
rupture of the membranes. Best Pract Res Clin Obstet Gynaecol. 2007;21(3):467-78.
65. Romero R, Brody DT, Oyarzun E, Mazor M, Wu YK, Hobbins JC, et al. Infection
and labor. III. Interleukin-1: a signal for the onset of parturition. Am J Obstet Gynecol.
1989;160(5 Pt 1):1117-23.
66. Romero R, Parvizi ST, Oyarzun E, Mazor M, Wu YK, Avila C, et al. Amniotic fluid
interleukin-1 in spontaneous labor at term. J Reprod Med. 1990;35(3):235-8.
67. Romero R, Mazor M, Brandt F, Sepulveda W, Avila C, Cotton DB, et al. Interleu-
kin-1 alpha and interleukin-1 beta in preterm and term human parturition. Am J Reprod
Immunol. 1992;27(3-4):117-23.
68. Hillier SL, Witkin SS, Krohn MA, Watts DH, Kiviat NB, Eschenbach DA. The relation-
ship of amniotic fluid cytokines and preterm delivery, amniotic fluid infection, histologic
chorioamnionitis, and chorioamnion infection. Obstet Gynecol. 1993;81(6):941-8.
69. Gomez R, Ghezzi F, Romero R, Munoz H, Tolosa JE, Rojas I. Premature labor and
intra-amniotic infection. Clinical aspects and role of the cytokines in diagnosis and
pathophysiology. Clin Perinatol. 1995;22(2):281-342.
70. Yoon BH, Romero R, Jun JK, Park KH, Park JD, Ghezzi F, et al. Amniotic fluid
cytokines (interleukin-6, tumor necrosis factor-alpha, interleukin-1 beta, and interleu-
kin-8) and the risk for the development of bronchopulmonary dysplasia. Am J Obstet
Gynecol. 1997;177(4):825-30.
71. Gonzalez-Bosquet E, Cerqueira MJ, Dominguez C, Gasser I, Bermejo B, Cabero L.
Amniotic fluid glucose and cytokines values in the early diagnosis of amniotic infection in
patients with preterm labor and intact membranes. J Matern Fetal Med. 1999;8(4):155-8.
72. Figueroa R, Garry D, Elimian A, Patel K, Sehgal PB, Tejani N. Evaluation of amniotic
fluid cytokines in preterm labor and intact membranes. J Matern Fetal Neonatal Med.
2005;18(4):241-7.
73. Sadowsky DW, Adams KM, Gravett MG, Witkin SS, Novy MJ. Preterm labor is
induced by intraamniotic infusions of interleukin-1beta and tumor necrosis factor-alpha
but not by interleukin-6 or interleukin-8 in a nonhuman primate model. Am J Obstet
Gynecol. 2006;195(6):1578-89.
74. Marconi C, de Andrade Ramos BR, Peracoli JC, Donders GG, da Silva MG. Amniotic
fluid interleukin-1 beta and interleukin-6, but not interleukin-8 correlate with microbial
invasion of the amniotic cavity in preterm labor. Am J Reprod Immunol. 2011;65(6):549-56.
75. Romero R, Chaemsaithong P, Korzeniewski SJ, Tarca AL, Bhatti G, Xu Z, et al.
Clinical chorioamnionitis at term II: the intra-amniotic inflammatory response. J Perinat
Med. 2016;44(1):5-22.
76. Sampson JE, Theve RP, Blatman RN, Shipp TD, Bianchi DW, Ward BE, et al.
Fetal origin of amniotic fluid polymorphonuclear leukocytes. Am J Obstet Gynecol.
1997;176(1 Pt 1):77-81.
77. Macias AE, Wong SW, Sadowsky DW, Luetjens CM, Axthelm MK, Gravett MG, et
al. Maternal or fetal origin of rhesus monkey (Macaca mulatta) amniotic fluid leukocytes
can be identified by polymerase chain reaction using the zinc finger Y gene. Am J
Primatol. 2001;55(3):159-70.
78. Gomez-Lopez N, Romero R, Xu Y, Leng Y, Garcia-Flores V, Miller D, et al. Are
amniotic fluid neutrophils in women with intraamniotic infection and/or inflammation of
fetal or maternal origin? Am J Obstet Gynecol. 2017;217(6):693 e1- e16.
79. Maddipati KR, Romero R, Chaiworapongsa T, Chaemsaithong P, Zhou SL, Xu Z, et al. Clinical
chorioamnionitis at term: the amniotic fluid fatty acyl lipidome. J Lipid Res. 2016;57(10):1906-16.
80. Maddipati KR, Romero R, Chaiworapongsa T, Chaemsaithong P, Zhou SL, Xu Z, et
al. Lipidomic analysis of patients with microbial invasion of the amniotic cavity reveals
up-regulation of leukotriene B4. FASEB J. 2016;30(10):3296-307.
81. Romero R, Chaemsaithong P, Korzeniewski SJ, Kusanovic JP, Docheva N, Marti-
nez-Varea A, et al. Clinical chorioamnionitis at term III: how well do clinical criteria perform
in the identification of proven intra-amniotic infection? J Perinat Med. 2016;44(1):23-32.
82. Gibbs RS. Diagnosis of intra-amniotic infection. Semin Perinatol. 1977;1(1):71-7.
83. Romero R, Chaemsaithong P, Docheva N, Korzeniewski SJ, Tarca AL, Bhatti G, et
al. Clinical chorioamnionitis at term IV: the maternal plasma cytokine profile. J Perinat
Med. 2016;44(1):77-98.
84. Benitz WE, Gould JB, Druzin ML. Risk factors for early-onset group B streptococcal
sepsis: estimation of odds ratios by critical literature review. Pediatrics. 1999;103(6):e77.
85. Volante E, Moretti S, Pisani F, Bevilacqua G. Early diagnosis of bacterial infection
in the neonate. J Matern Fetal Neonatal Med. 2004;16 Suppl 2:13-6.
86. Martinelli P, Sarno L, Maruotti GM, Paludetto R. Chorioamnionitis and prematurity:
a critical review. J Matern Fetal Neonatal Med. 2012;25 Suppl 4:29-31.
87. de Sam Lazaro S, Cheng Y, Snowden J, Pereira L, Aziz N, Caughey A. 746. Does
the neonatal impact of chorioamnionitis in the setting of PPROM vary depending on
degree of prematurity? Am J Obstet Gynecol. 2013;208(1):S314.
88. Uyemura A, Ameel B, Caughey A. 425. Outcomes of chorioamnionitis in term
pregnancies. Am J Obstet Gynecol. 2014;210(1):S215.
89. Garcia-Munoz Rodrigo F, Galan Henriquez GM, Ospina CG. Morbidity and mortality
among very-low-birth-weight infants born to mothers with clinical chorioamnionitis.
Pediatr Neonatol. 2014;55(5):381-6.
90. Romero R, Hanaoka S, Mazor M, Athanassiadis AP, Callahan R, Hsu YC, et al.
Meconium-stained amniotic fluid: a risk factor for microbial invasion of the amniotic
cavity. Am J Obstet Gynecol. 1991;164(3):859-62.

SEMMELWEIS 200
112 NŐGYÓGYÁSZATI ÉS SZÜLÉSZETI TOVÁBBKÉPZŐ SZEMLE 2018. JÚNIUS
91. Wen TS, Eriksen NL, Blanco JD, Graham JM, Oshiro BT, Prieto JA. Association
of clinical intra-amniotic infection and meconium. Am J Perinatol. 1993;10(6):438-40.
92. Cleary GM, Wiswell TE. Meconium-stained amniotic fluid and the meconium aspiration
syndrome. An update. Pediatr Clin North Am. 1998;45(3):511-29.
93. Romero R, Yoon BH, Chaemsaithong P, Cortez J, Park CW, Gonzalez R, et al.
Bacteria and endotoxin in meconium-stained amniotic fluid at term: could intra-amniotic
infection cause meconium passage? J Matern Fetal Neonatal Med. 2014;27(8):775-88.
94. Romero R, Yoon BH, Chaemsaithong P, Cortez J, Park CW, Gonzalez R, et al.
Secreted phospholipase A2 is increased in meconium-stained amniotic fluid of term
gestations: potential implications for the genesis of meconium aspiration syndrome. J
Matern Fetal Neonatal Med. 2014;27(10):975-83.
95. Adamson SJ, Alessandri LM, Badawi N, Burton PR, Pemberton PJ, Stanley F. Pre-
dictors of neonatal encephalopathy in full-term infants. BMJ. 1995;311(7005):598-602.
96. Willoughby RE, Jr., Nelson KB. Chorioamnionitis and brain injury. Clin Perinatol.
2002;29(4):603-21.
97. Cooke R. Chorioamnionitis, maternal fever, and neonatal encephalopathy. Dev Med
Child Neurol. 2008;50(1):9.
98. Versland LB, Sommerfelt K, Elgen I. Maternal signs of chorioamnionitis: persistent
cognitive impairment in low-birthweight children. Acta Paediatr. 2006;95(2):231-5.
99. Burd I, Brown A, Gonzalez JM, Chai J, Elovitz MA. A mouse model of term chorioamni-
onitis: unraveling causes of adverse neurological outcomes. Reprod Sci. 2011;18(9):900-7.
100. Korzeniewski SJ, Romero R, Cortez J, Pappas A, Schwartz AG, Kim CJ, et al.
A "multi-hit" model of neonatal white matter injury: cumulative contributions of chronic
placental inflammation, acute fetal inflammation and postnatal inflammatory events. J
Perinat Med. 2014;42(6):731-43.
101. Pappas A, Kendrick DE, Shankaran S, Stoll BJ, Bell EF, Laptook AR, et al.
Chorioamnionitis and early childhood outcomes among extremely low-gestational-age
neonates. JAMA Pediatr. 2014;168(2):137-47.
102. Eastman NJ, Deleon M. The etiology of cerebral palsy. Am J Obstet Gynecol.
1955;69(5):950-61.
103. Nelson KB, Willoughby RE. Infection, inflammation and the risk of cerebral palsy.
Curr Opin Neurol. 2000;13(2):133-9.
104. Shatrov JG, Birch SC, Lam LT, Quinlivan JA, McIntyre S, Mendz GL. Chorioamni-
onitis and cerebral palsy: a meta-analysis. Obstet Gynecol. 2010;116(2 Pt 1):387-92.
105. Mendez-Figueroa H, Abramovici A, O’Neil AE, Dahlke J, Pedroza C, Chauhan S.
647. Chorioamnionitis without and with neonatal sepsis: newborn and infant outcomes.
Am J Obstet Gynecol. 2015;212(1):S318-19.
106. Romero R, Chaemsaithong P, Docheva N, Korzeniewski SJ, Tarca AL, Bhatti G,
et al. Clinical chorioamnionitis at term V: umbilical cord plasma cytokine profile in the
context of a systemic maternal inflammatory response. J Perinat Med. 2016;44(1):53-76.
107. Benirschke K, Clifford SH. Intrauterine bacterial infection of the newborn infant:
frozen sections of the cord as an aid to early detection. J Pediatr. 1959;54(1):11-8.
108. Olding L. Value of placentitis as a sign of intrauterine infection in human subjects.
Acta Pathol Microbiol Scand A. 1970;78(3):256-64.
109. Zhang JM, Kraus FT, Aquino TI. Chorioamnionitis: a comparative histologic,
bacteriologic, and clinical study. Int J Gynecol Pathol. 1985;4(1):1-10.
110. Svensson L, Ingemarsson I, Mardh PA. Chorioamnionitis and the isolation of
microorganisms from the placenta. Obstet Gynecol. 1986;67(3):403-9.
111. Hillier SL, Martius J, Krohn M, Kiviat N, Holmes KK, Eschenbach DA. A case-control
study of chorioamnionic infection and histologic chorioamnionitis in prematurity. N Engl
J Med. 1988;319(15):972-8.
112. Smulian JC, Shen-Schwarz S, Vintzileos AM, Lake MF, Ananth CV. Clinical chorio-
amnionitis and histologic placental inflammation. Obstet Gynecol. 1999;94(6):1000-5.
113. Pacora P, Chaiworapongsa T, Maymon E, Kim YM, Gomez R, Yoon BH, et al.
Funisitis and chorionic vasculitis: the histological counterpart of the fetal inflammatory
response syndrome. J Matern Fetal Neonatal Med. 2002;11(1):18-25.
114. Rhone SA, Magee F, Remple V, Money D. The association of placental abnormal-
ities with maternal and neonatal clinical findings: a retrospective cohort study. J Obstet
Gynaecol Can. 2003;25(2):123-8.
115. Redline RW, Heller D, Keating S, Kingdom J. Placental diagnostic criteria and
clinical correlation--a workshop report. Placenta. 2005;26 Suppl A:S114-7.
116. Redline RW. Inflammatory responses in the placenta and umbilical cord. Semin
Fetal Neonatal Med. 2006;11(5):296-301.
117. Seong HS, Lee SE, Kang JH, Romero R, Yoon BH. The frequency of microbi-
al invasion of the amniotic cavity and histologic chorioamnionitis in women at term
with intact membranes in the presence or absence of labor. Am J Obstet Gynecol.
2008;199(4):375 e1-5.
118. Kim MJ, Romero R, Gervasi MT, Kim JS, Yoo W, Lee DC, et al. Widespread mi-
crobial invasion of the chorioamniotic membranes is a consequence and not a cause
of intra-amniotic infection. Lab Invest. 2009;89(8):924-36.
119. Park CW, Moon KC, Park JS, Jun JK, Romero R, Yoon BH. The involvement
of human amnion in histologic chorioamnionitis is an indicator that a fetal and an
intra-amniotic inflammatory response is more likely and severe: clinical implications.
Placenta. 2009;30(1):56-61.
120. Roberts DJ, Celi AC, Riley LE, Onderdonk AB, Boyd TK, Johnson LC, et al.
Acute histologic chorioamnionitis at term: nearly always noninfectious. PLoS One.
2012;7(3):e31819.
121. Park CW, Yoon BH, Kim SM, Park JS, Jun JK. Which is more important for the
intensity of intra-amniotic inflammation between total grade or involved anatomical
region in preterm gestations with acute histologic chorioamnionitis? Obstet Gynecol
Sci. 2013;56(4):227-33.
122. Park CW, Yoon BH, Park JS, Jun JK. A fetal and an intra-amniotic inflammatory
response is more severe in preterm labor than in preterm PROM in the context of
funisitis: unexpected observation in human gestations. PLoS One. 2013;8(5):e62521.
123. Kim SM, Romero R, Park JW, Oh KJ, Jun JK, Yoon BH. The relationship between the
intensity of intra-amniotic inflammation and the presence and severity of acute histologic
chorioamnionitis in preterm gestation. J Matern Fetal Neonatal Med. 2015;28(13):1500-9.
124. Park CW, Kim SM, Park JS, Jun JK, Yoon BH. Fetal, amniotic and maternal
inflammatory responses in early stage of ascending intrauterine infection, inflamma-
tion restricted to chorio-decidua, in preterm gestation. J Matern Fetal Neonatal Med.
2014;27(1):98-105.
125. Romero R, Chaemsaithong P, Docheva N, Korzeniewski SJ, Kusanovic JP, Yoon BH,
et al. Clinical chorioamnionitis at term VI: acute chorioamnionitis and funisitis according
to the presence or absence of microorganisms and inflammation in the amniotic cavity.
J Perinat Med. 2016;44(1):33-51.
126. Nien JK, Yoon BH, Espinoza J, Kusanovic JP, Erez O, Soto E, et al. A rapid MMP-8
bedside test for the detection of intra-amniotic inflammation identifies patients at risk for
imminent preterm delivery. Am J Obstet Gynecol. 2006;195(4):1025-30.
127. Kim KW, Romero R, Park HS, Park CW, Shim SS, Jun JK, et al. A rapid matrix metal-
loproteinase-8 bedside test for the detection of intraamniotic inflammation in women with
preterm premature rupture of membranes. Am J Obstet Gynecol. 2007;197(3):292 e1-5.
128. Park CW, Lee SM, Park JS, Jun JK, Romero R, Yoon BH. The antenatal identifi-
cation of funisitis with a rapid MMP-8 bedside test. J Perinat Med. 2008;36(6):497-502.
129. Park HS, Kim SA. Abstract No. 322: The value of the genedia MMP-8 rapid test
for diagnosing intraamniotic infection/inflammation and predicting adverse pregnancy
outcomes in women with preterm prematue rupture of membranes. Am J Obstet Gy-
necol. 2015;212(1):S174.
130. Chaemsaithong P, Romero R, Docheva N, Chaiyasit N, Kim YM, Dong Z, et al.
A rapid point-of-care test (MMP-8) for the identification of intra-amniotic inflammation
and impending preterm delivery. Abstract presented at 12th World Congress of Perinatal
Medicine, 3rd-6th November, 2015, Madrid, Spain. 2015.
131. Chaemsaithong P, Romero R, Chaiyasit N, Docheva N, Korzeniewski SJ, Kim YM,
et al. Rapid MMP-8 as a point-of-care test in the identification of intra-amniotic inflam-
mation in patients with preterm PROM. Abstract presented at 12th World Congress of
Perinatal Medicine, 3rd-6th November, 2015, Madrid, Spain. 2015.
132. Chaiyasit N, Chaemsaithong P, Romero R, Docheva N, Dong Z, Kim CJ, et al.
A rapid MMP-8 test for the identification of intra-amniotic inflammation/infection in patients
with clinical chorioamnionitis at term : a solution at last! Abstract presented at 12th
World Congress of Perinatal Medicine, 3rd-6th November, 2015, Madrid, Spain. 2015.
133. Kim SM, Romero R, Lee J, Chaemsaithong P, Lee MW, Chaiyasit N, et al. About
one-half of early spontaneous preterm deliveries can be identified by a rapid matrix
metalloproteinase-8 (MMP-8) bedside test at the time of mid-trimester genetic amnio-
centesis. J Matern Fetal Neonatal Med. 2016;29(15):2414-22.
134. Chaiyasit N, Romero R, Chaemsaithong P, Docheva N, Bhatti G, Kusanovic JP,
et al. Clinical chorioamnionitis at term VIII: a rapid MMP-8 test for the identification of
intra-amniotic inflammation. J Perinat Med. 2017;45(5):539-50.