Embed Size (px)
Citation preview

April 2012
ΝΕΟΤΕΡΑ ΑΝΤΙΠΗΚΤΙΚΑ. Από τις μελέτες στην καθημερινή κλινική
πράξη. Η παγκόσμια εμπειρία.
Κωνσταντίνος Π. Λέτσας, MD, FESC
Β΄ Καρδιολογική ΚλινικήΕργαστήριο Επεμβατικής Ηλεκτροφυσιολογίας
Γ.Ν.Α. “ΕΥΑΓΓΕΛΙΣΜΟΣ”
2Ο ΑΡΡΥΘΜΙΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟΑΘΗΝΑ 2016

April 2012Eur Heart J 2016
Latest 2016 ESC guidelines recommend NOACs over VKAs

April 2012
R
RE-LY® provides robust data for both doses of dabigatran due to randomization into two treatment arms
*Dose selection based on individual assessment of thromboembolic and bleeding risk in patients aged 75–79 yrs or with moderate renal impairment, gastritis, oesophagitis, GERD, or other riskfactors for bleeding. RE-LY® followed a PROBE (prospective, randomized, open-label with blinded
endpoint evaluation) design. INR, international normalized ratio; R, randomization; TTR, time intherapeutic range. 1. Connolly SJ et al. N Engl J Med 2009; 2. Pradaxa®: EU SPC, 2015.
AF with ≥1 risk factor for stroke; absence of contraindications; 18 113 patients across 951 centres in 44 countries1
Dabigatran 110 mg BID
N=6015
Warfarin (INR 2.0–3.0)
N=6022INR control: mean TTR=64%
Dabigatran 150 mg BID
N=6076
Primary endpoint: stroke/systemic embolism
Both dabigatran arms were adequately powered to support efficacy and safety conclusions
OpenBlind dosing
The EU label recommends 150 mg BID as the standard dose of dabigatran
and 110 mg BID for patients aged ≥80 years, or on concomitant verapamil*2

April 2012
Both doses of dabigatran provide safety and efficacy benefits vs warfarin in the overall RE-LY® population
1. Connolly SJ et al. N Engl J Med 2010;
2. Connolly SJ et al. N Engl J Med 2014.
Click here to see forest plot of the key outcomes in RE-LY®
150 mg BID
Major bleeding
similar
ICH
59%
110 mg BID
ICH
70%
Major bleeding
20%
Stroke/SE
35%
CV mortality
15%
Haemorrhagic
stroke
74%
Ischaemic
stroke
24%
Stroke/SE
similar
CV mortality
similar
Haemorrhagic
stroke
69%
Ischaemic
stroke
similar

April 2012
In RE-LY®, dabigatran 150 mg BID showed both superior safety and efficacy vs warfarin in patients aged <75 years
Superior safety for dabigatran 150 mg BID vs warfarin refers to major bleeding events including ICH; *Pre-specified analysis of patients aged <75 years;6 †RRRs should be interpreted with caution for stroke/SE,
ICH and CV mortality; age–treatment interactions seen for major bleeding
1. Connolly SJ et al. N Engl J Med 2014; 2. Connolly SJ et al. N Engl J Med 2010; 3. Eikelboom JW et al. Circulation 2011; 4. Clemens A et al. Am J Cardiol 2014; 5. BI, Data on file; 6. RE-LY® trial protocol.
Stroke/SEICHMajor
bleeding
CV
mortality
Dabigatran 150 mg
vs warfarin
(<75 yrs)3–5*†
57% 37%30% 26%
Please see the MSL ‘Patients aged <75 years’ slide set for further information on this analysis
35%59%Dabigatran 150 mg
vs warfarin
(all age groups)1,215%
70%Dabigatran 110 mg
vs warfarin
(all age groups)1,220%

April 2012
Dabigatran provides superior efficacy and safety vs warfarin when used according to the EU label*

April 2012
Real-world evidence
RCTs: tightly controlled patient population
Approval
Post-approval use includes morevaried medical settings and more diverse patient populations
Differing:•Age•Race•Co-morbidities•Co-medications•Adherence
RWE clarifies whether the results observed under the tightly controlled conditions of an RCT are also observed in everyday clinical practice
1. Nallamothu BK et al. Circulation 2008

April 2012
Growing body of real-world experience from >250 000 patients confirms safety and efficacy profile of dabigatran
RE-LY®
(n>18 000)
Clinical practice (n>250000 patients)
FDA Medicare study (n>134 000)1
2 US insurance databases(n>38 000)3
US Dept of Defense database (n>25 000)2
Danish observational studies(n>21 000)4,5
1. Graham DJ et al. Circulation 2015; 2. Villines TC et al. Circulation 2014; 3. Seeger J et al. Circulation 2014; 4. Larsen TB et al. Am J Med 2014a; 5. Larsen TB et al. Am J Med 2014b; 6. Lauffenburger JC et al. J Am Heart Assoc 2015
US insurance database(n>64 000)6

April 2012
Independent FDA study of Medicare patients provides single largest body of RWE for dabigatran
>134 000 OAC-naïve dabigatran
or VKA users aged ≥65 years
>37 500patient-years’
follow-up
Propensity score-matched
16% of patients were aged ≥85 years; 16% of patients were taking dabigatran 75 mg BIDGraham DJ et al. Circulation 2015;131:157–64

April 2012
RE-LY®1–4
N>18 000WarfarinD150 BID
MEDICARE*5
N>134 000WarfarinD150 & D75 BID combined
MORTALITYISCHAEMIC
STROKEICH
MAJORBLEEDING
GIBLEEDING
MI
HR: 0.76P=0.04
HR: 0.80P=0.02
RR: 0.41P<0.001
HR: 0.34P<0.001
RR: 0.94P=0.41
HR: 0.97P=0.50
RR: 1.48P=0.001
HR: 1.28P<0.001
RR: 1.27P=0.12
HR: 0.92P=0.29
RR: 0.88P=0.051
HR: 0.86P=0.006
RCT
Real-world data
EV
EN
T R
AT
E (
% P
ER
YE
AR)
5
4
3
2
1
0
INCI
DEN
CE P
ER 1
00PE
RSO
N-
YE
AR
S
0
1
2
3
4
5
Ischaemic stroke:what does this mean for your patients?
1. Connolly SJ et al. N Engl J Med 2009;361:1139–512. Connolly SJ et al. N Engl J Med 2010;363:1875–63. Pradaxa®: EU SPC, January 20154. Connolly SJ et al. N Engl J Med 2014;371:1464–55. Graham DJ et al. Circulation 2015;131:157–64

April 2012
RE-LY®1–4
N>18 000WarfarinD150 BID
MEDICARE*5
N>134 000WarfarinD150 & D75 BID combined
MORTALITYISCHAEMIC
STROKEICH
MAJORBLEEDING
GIBLEEDING
MI
HR: 0.76P=0.04
HR: 0.80P=0.02
RR: 0.41P<0.001
HR: 0.34P<0.001
RR: 0.94P=0.41
HR: 0.97P=0.50
RR: 1.48P=0.001
HR: 1.28P<0.001
RR: 1.27P=0.12
HR: 0.92P=0.29
RR: 0.88P=0.051
HR: 0.86P=0.006
RCT
Real-world data
EVEN
T RA
TE (%
PER
YEA
R)
5
4
3
2
1
0
INCI
DEN
CE P
ER 1
00PE
RSO
N-
YEA
RS
0
1
2
3
4
5
Intracranial haemorrhage: what does this mean for your patients?
1. Connolly SJ et al. N Engl J Med 2009;361:1139–512. Connolly SJ et al. N Engl J Med 2010;363:1875–63. Pradaxa®: EU SPC, January 20154. Connolly SJ et al. N Engl J Med 2014;371:1464–55. Graham DJ et al. Circulation 2015;131:157–64

April 2012
RE-LY®1–4
N>18 000WarfarinD150 BID
MEDICARE*5
N>134 000WarfarinD150 & D75 BID combined
MORTALITYISCHAEMIC
STROKEICH
MAJORBLEEDING
GIBLEEDING
MI
HR: 0.76P=0.04
HR: 0.80P=0.02
RR: 0.41P<0.001
HR: 0.34P<0.001
RR: 0.94P=0.41
HR: 0.97P=0.50
RR: 1.48P=0.001
HR: 1.28P<0.001
RR: 1.27P=0.12
HR: 0.92P=0.29
RR: 0.88P=0.051
HR: 0.86P=0.006
RCT
Real-world data
EVEN
T RA
TE (%
PER
YEA
R)
5
4
3
2
1
0
INCI
DEN
CE P
ER 1
00PE
RSO
N-
YEA
RS
0
1
2
3
4
5
Major and GI bleeding: what does this mean for your patients?
1. Connolly SJ et al. N Engl J Med 2009; 361:1139–512. Connolly SJ et al. N Engl J Med 2010;363:1875–63. Pradaxa®: EU SPC, January 20154. Connolly SJ et al. N Engl J Med 2014; 371:1464–55. Graham DJ et al. Circulation 2015;131:157–64

April 2012
RE-LY®1–4
N>18 000
Warfarin
D150 BID
MEDICARE*5
N>134 000
Warfarin
D150 & D75 BID
combined
MORTALITYISCHAEMIC
STROKEICH
MAJOR
BLEEDING
GI
BLEEDINGMI
HR: 0.76P=0.04
HR: 0.80P=0.02
RR: 0.41P<0.001
HR: 0.34P<0.001
RR: 0.94P=0.41
HR: 0.97P=0.50
RR: 1.48P=0.001
HR: 1.28P<0.001
RR: 1.27P=0.12
HR: 0.92P=0.29
RR: 0.88P=0.051
HR: 0.86P=0.006
RCT
Real-world
data
EV
EN
T R
AT
E (
% P
ER
YE
AR
)
5
4
3
2
1
0
INC
IDE
NC
E P
ER
1
00
PE
RS
ON
-YE
AR
S
0
1
2
3
4
5
Myocardial infarction and mortality:what does this mean for your patients?
1. Connolly SJ et al. N Engl J Med 2009; 361:1139–512. Connolly SJ et al. N Engl J Med 2010;363:1875–63. Pradaxa®: EU SPC, January 20154. Connolly SJ et al. N Engl J Med 2014; 371:1464–55. Graham DJ et al. Circulation 2015;131:157–64

April 2012
US DoD database showed clear consistency in outcomes with data from RE-LY®
MORTALITY
N>18 000WarfarinD150 BID
DoD*5,6
N>25 000WarfarinD150 & D75 BID combined
EVEN
T RA
TE (%
PER
YEA
R)IN
CID
ENCE
PER
100
PERS
ON
-YE
ARS
STROKEISCHAEMIC
STROKEICH
MAJORBLEEDING
MI
HR: 0.64P<0.001
HR: 0.73P=0.03
HR: 0.76P=0.04
HR: 0.84P=0.25
RR: 0.41P<0.001
HR: 0.49P=0.004
RR: 0.94P=0.41
HR: 0.87P=0.09
RR: 1.27P=0.12
HR: 0.65P=0.02
RR: 0.88P=0.051
HR: 0.64P<0.0001
RE-LY®1–4
RCT
Real-world data
0
1
2
3
4
5
5
4
3
2
1
0
In the USA, the licensed doses for Pradaxa® are: 150 mg BID and 75 mg BID for the prevention of stroke and systemic embolism in adult patients with NVAF*Primary findings for dabigatran are based on analysis of both 75 mg &150 mg together without stratification by dose
1. Connolly SJ et al. N Engl J Med 2009; 2. Connolly SJ et al. N Engl J Med 2010; 3. Pradaxa®: EU SPC, January 2015; 4. Connolly SJ et al. N Engl J Med 2014; 5. Villines TC et al. Presented at AHA 2014; 6. Villines TC et al. Thromb Haemost 2015

April 2012
US Health Insurance data are consistent with RE-LY® and additional real-world data
RE-LY®1–4
N>18 000WarfarinD150 BID
US Health Insurance data*5
N>44 000WarfarinD150 & 75 BID combined
EVEN
T RA
TE (%
PER
YEA
R)IN
CID
ENCE
RA
TE P
ER 1
00PE
RSO
N-
YEA
RS
STROKEISCHAEMIC
STROKEICH
MAJORBLEEDING
MI
HR: 0.64P<0.001
HR: 0.72(0.52–1.00)
HR: 0.76P=0.04
HR: 0.82(0.57–1.18)
RR: 0.41P<0.001
HR: 0.32(0.19–0.54)
RR: 0.94P=0.41
RR: 1.27P=0.12
HR: 0.85(0.58–1.27)
HR: 0.74(0.64–0.84)
1. Connolly SJ et al. N Engl J Med 2009; 2. Connolly SJ et al. N Engl J Med 2010; 3. Pradaxa®: EU SPC, January 20154. Connolly SJ et al. N Engl J Med 2014; 5. Seeger J et al. Poster presented at AHA 2015
GIBLEEDING
HR: 0.95(0.79–1.14)
RR: 1.48P=0.001
RCT
Real-world data
5
4
3
2
1
0
0
1
2
3
4
5
In the USA, the licensed doses for Pradaxa® are: 150 mg BID and 75 mg BID for the prevention of stroke and systemic embolism in adult patients with NVAF*Primary findings for dabigatran are based on analysis of both 75 mg &150 mg together without stratification by dose

April 2012
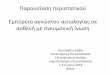
Independent Danish non-interventional study assessed bleeding and MI events with dabigatran vs warfarin
Registry 1: median age 82 years (dabigatran 110 mg BID), 67 years (dabigatran 150 mg BID), 73 years (warfarin);Registry 2: median age 82 years (dabigatran 110 mg BID), 68 years (dabigatran 150 mg BID), 72 years (warfarin)1. Larsen TB et al. Am J Med 2014;127:650–6;
2. Larsen TB et al. Am J Med 2014;127:329–36.e4
>21000 OAC-naïve
dabigatran or VKA users
Mean 13.2 months’
follow-up
Matched to warfarin
users in a 2:1 ratio
>12 000 OAC-naïve
dabigatran or VKA users
Mean 16 months’ follow-up
No statistical matching
Bleeding events analysis1
MI events analysis2

April 2012
D110 vs W HR* (95% CI)
Any 0.72 (0.59–0.88)
Major 0.93 (0.74–1.16)
Fatal 0.52 (0.28–0.95)
GI 0.50 (0.27–0.94)
ICH 0.30 (0.17–0.54)
D150 vs W
Any 0.68 (0.55–0.84)
Major 0.67 (0.53–0.85)
Fatal 0.70 (0.33–1.52)
GI 1.45 (0.84–2.50)
ICH 0.33 (0.17–0.66)
Reduced risk of any bleeding and ICH with both doses of dabigatran vs warfarin
Larsen TB et al. Am J Med 2014;127:650–6
VKA-naïve stratum
0.10 5.00
Favours dabigatran Favours warfarin
0.50 1.00 2.00

April 2012
Similar incidence of MI events with both doses of dabigatran vs warfarin (VKA-naïve stratum)
D110 vs W HR* (95% CI)
Myocardial infarction 0.71 (0.47–1.07)
D150 vs W
Myocardial infarction 0.93 (0.62–1.41)
VKA-naïve stratum
0.10 5.00
Favours dabigatran Favours warfarin
0.50 1.00 2.00
Larsen TB et al. Am J Med 2014;127:329–36.e4

April 2012
Hong Kong hospital study evaluated the risk of stroke and ICH with dabigatran vs warfarin in patients with NVAF
8754 Chinese patients with
NVAF
Mean follow-up of
3.0±3.2 years
No statistical matching of
cohorts
Mean age 79.5±9.2 years; ICH, intracranial haemorrhage; NVAF, nonvalvular atrial fibrillation
Ho et al. Stroke 2015

April 2012Ho et al. Stroke 2015
Dabigatran was associated with the lowest incidence of ischaemic stroke, compared with ASA, warfarin and no therapy
Warfarin (quartiles of TTR)
HR (95% CI)
ASA 0.73 (0.67–0.81)
Q1 0.71 (0.58–0.87)
Q2 0.56 (0.45–0.69)
Q3 0.42 (0.33–0.53)
Q4 0.31 (0.23–0.40)
Dabigatran 0.20 (0.12–0.34)
0.1 1
Decreased risk of stroke Increased risk of stroke
Warfarin
(quartiles of TTR)
1.1

April 2012Ho et al. Stroke 2015
Dabigatran was associated with the lowest mortality rate compared with ASA, warfarin and no therapy

April 2012
The favourable safety profile of dabigatran has been consistently confirmed vs different comparators
Dabigatran shows similar or lower rates of major
bleeding1–5,14
Dabigatran is associated with lower rates of bleeding*
and mortality13,14
A growing number of real-world studies confirm the
favourable safety profile of dabigatran, with safety comparable to apixaban6–12,14
Results for selected analyses. *ICH, major bleeding, and major GI bleeding. References are provided in slide notes.
Dabigatran vs warfarin
Dabigatran vs apixaban
Dabigatran vs rivaroxaban
vs
vs
vs

April 2012
Patients
• New users of dabigatran, apixaban, rivaroxaban, or warfarin• N=61 678 (12 701 dabigatran, 6349 apixaban, 7192 rivaroxaban,
35 436 warfarin); only patients on standard NOAC doses were included
Safety outcomes
• Major bleeding, any bleeding (intracranial, major GI bleeding, traumatic intracranial), and all-cause mortality
Methods
• Prospective analysis of 3 Danish health registries (Aug 2011–Nov 2015)• Follow up until outcome of interest, emigration, death, or end of study
• Cox regression and inverse probability-of-treatment weighted analysis
Funding
• Obel Family Foundation
Limitations
• Only ITT analysis presented• Limited variables for adjustment
• Follow-up duration limited
for some patients• Patients included prior to
availability of apixaban
!
Comparative effectiveness and safety of non-vitamin K antagonist oral anticoagulants and warfarin in patients with atrial fibrillation: propensity weighted nationwide cohort study. Larsen et al. BMJ 2016;353:i3189

April 2012
24
Only standard doses of NOACs were compared in this study. *Inverse probability of treatment weighted and expressedas population average treatment rates per 100 years. Adjusted HR (95% CI), bold values indicate statistical significance.Limitations: ITT analysis; limited variables for adjustment; limited follow-up; patients included prior to availability of
apixaban.
Major bleeding All-cause mortality
HR 0.58 (0.47–0.71)
Dabigatran and apixaban were associated with a statistically significantly lower risk of any bleeding, major bleeding, and death compared with rivaroxaban or warfarin
HR 0.61 (0.49–0.75)
HR 1.06 (0.91–1.23)
HR 0.63 (0.48–0.82)
HR 0.65 (0.56–0.75)
HR 0.92 (0.82–1.03)
ApixabanDabigatran Rivaroxaban Warfarin ApixabanDabigatran Rivaroxaban Warfarin
Adjusted HR (95% CI) vs warfarin Adjusted HR (95% CI) vs warfarin
Comparative effectiveness and safety of non-vitamin K antagonist oral anticoagulants and warfarin in patients with atrial fibrillation: propensity weighted nationwide cohort study. Larsen et al. BMJ 2016;353:i3189

April 2012
Patients
• New users of dabigatran, rivaroxaban, or warfarin• N=22 358 (3588 dabigatran 110 mg, 5320 dabigatran 150 mg,
776 rivaroxaban 15 mg, 1629 rivaroxaban 20 mg, 11 045 warfarin)
Safety outcomes
• Any bleeding (intracranial, GI, and major bleeding), and all-cause mortality
Rivaroxaban versus warfarin and dabigatran in atrial fibrillation: comparative effectiveness and safety in Danish routine care.Gorst-Rasmussen et al. Pharmacoepidemiol Drug Saf 2016; doi:10.1002/pds.4034
Methods
• Prospective analysis of three Danish health registries (1 Feb 2012– 30 Jul 2014)• Follow up until outcome of interest, emigration, death, or end of study
• Propensity-adjusted Cox regression
Funding
• Obel Family Foundation
Limitations
• Small to moderate sample size• Treatment switches and discontinuations were not taken into account
• Follow-up duration can be limited
!

April 2012
* Intracranial, bleeding, GI bleeding, and major bleeding events. D150, dabigatran 150 mg BID; D110, dabigatran 110 mg BID; R20, rivaroxaban 20 mg OD; R15, rivaroxaban 15 mg OD. Adjusted HR (95% CI), bold values indicate statistical significance. Limitations: small to moderate sample size; treatment switches and discontinuations were not
taken into account; follow-up duration can be limited.
Dabigatran showed lower bleeding and mortality than rivaroxaban
HR 1.28 (0.82–2.01)
HR 1.43 (1.13–1.81)HR 1.81 (1.25–2.62)
HR 1.52 (1.06–2.19)
Any bleeding* All-cause mortalityAdjusted HR (95% CI) Adjusted HR (95% CI)
Rivaroxaban versus warfarin and dabigatran in atrial fibrillation: comparative effectiveness and safety in Danish routine care.Gorst-Rasmussen et al. Pharmacoepidemiol Drug Saf 2016; doi:10.1002/pds.4034

April 2012
Dabigatran 150 mg was associated with a significantly lower rate of any bleedingand all-cause mortality vs rivaroxaban 20 mg; dabigatran 110 mg was associated
with a similar rate of bleeding and lower mortality vs rivaroxaban 15 mg
Any bleeding and all-cause death during follow-up
HR, hazard ratio. Limitations: small to moderate sample size; treatment switches and discontinuations were not taken into account; follow-up duration can be limited.
0 0,5 1 1,5 2 2,5 3
Rivaroxaban 15 mg vs dabigatran 110 mg
Rivaroxaban 20 mg vs dabigatran 150 mg
1.28 (0.82–2.01)
1.81 (1.25–2.62)
Adjusted HR (95% CI)
Any bleeding
All-cause mortality
1.43 (1.13–1.81)
1.52 (1.06–2.19)
Any bleeding
All-cause mortality
Favours rivaroxaban Favours dabigatran
HR
Rivaroxaban versus warfarin and dabigatran in atrial fibrillation: comparative effectiveness and safety in Danish routine care.Gorst-Rasmussen et al. Pharmacoepidemiol Drug Saf 2016; doi:10.1002/pds.4034

April 2012
Funding
• Bristol-Myers Squibb and Pfizer
Patients
• New NOAC users or switchers from warfarin to a NOAC• N=60 277 (20 963 dabigatran, 30 529 rivaroxaban, 8785 apixaban)
Safety outcomes
• Major and CRNM bleeding
Real-world comparison of bleeding risks among non-valvular atrial fibrillation patients on apixaban, dabigatran, rivaroxaban: cohorts comprising new initiators and/or switchers from warfarin. Tepper et al. Presented at ESC 2015; Abstract 1975
CRNM, clinically relevant non-major.
Methods
• Retrospective analysis of US MarketScan Earlyview database (Jan 2013–Oct 2014)
• Follow up for 6 months until bleeding, discontinuation or switch, or end of study
• Adjusted for baseline characteristics but no propensity-score methods used
Limitations
• Abstract only• Limited variables for adjustment
• The three NOACs were launched
at different times and treatment patterns may change over time
!

April 2012
Real-world comparison of bleeding risks among non-valvular atrial fibrillation patients on apixaban, dabigatran, rivaroxaban: cohorts comprising new initiators and/or switchers from warfarin. Tepper et al. Presented at ESC 2015; Abstract 1975

April 2012
Funding
• Bristol-Myers Squibb and Pfizer
Patients• New users of dabigatran, rivaroxaban, apixaban, or warfarin (may include switchers from
other OACs)• N=35 757 (2440 dabigatran, 6407 rivaroxaban, 2038 apixaban, 24 872 warfarin)
Safety outcomes
• Major and CRNM bleeding
CRNM, clinically relevant non-major.
Methods
• Retrospective analysis of US Humedica EHR database (Jan 2013–Jun 2014)• Follow up until OAC switch, bleeding event, last visit, or 180 days
• Adjusted for baseline characteristics but no propensity-score methods used
Limitations
• Abstract only• Limited variables for adjustment
• Moderate sample size
• Only 6 months follow-up• Treatment discontinuations not
taken into account
!
Real-world bleeding risk among non-valvular atrial fibrillation (NVAF) patients prescribed apixaban, dabigatran, rivaroxaban and warfarin: analysis of electronic health records. Lin et al. Presented at ESC 2015

April 2012
Real-world bleeding risk among non-valvular atrial fibrillation (NVAF) patients prescribed apixaban, dabigatran, rivaroxaban and warfarin: analysis of electronic health records. Lin et al. Presented at ESC 2015
*Any bleed is a combination of major and clinically relevant non-major bleeding. Limitations: abstract only; may include switchers from other OACs; limited variables for adjustment; moderate sample size; only 6 months of follow-up; treatment discontinuations not taken into account.
0 30 60 90 120 150 1800
2
4
6
8
10
12
14
16
18
20
Time after index (Days)
Cu
mu
lati
ve
pro
po
rtio
n o
f
pa
tie
nts
wit
h a
ny
ble
ed
(%
) Log rank P<0.0001Rivaroxaban
Warfarin
Apixaban
Dabigatran
Kaplan–Meier analysis of any bleed during follow-up
Patients initiating treatment with dabigatran or apixaban experienced a
significantly lower risk of bleeding than those initiating treatment with warfarin
31
Curves unadjusted for differences in baseline characteristics

April 2012
Funding
• Bristol-Myers Squibb and Pfizer
Patients
• New users of dabigatran, rivaroxaban, apixaban, or warfarin (may include switchers from other OACs)
• N=4828 apixaban-dabigatran and 6721 apixaban-rivaroxaban matched patients
Safety outcomes
• Major bleeding
Methods
• Retrospective analysis of US MarketScan and Medicare supplemental databases (Jan 2012–Sep 2014)
• Follow up until bleeding, discontinuation or switch, or end of study
• Analysis based on propensity-score matched cohorts
Limitations
• Abstract only• Moderate sample size
• Limited variables used for adjustment
!
Real world comparison of major bleeding risk among non-valvular atrial fibrillation patients newly initiated on apixaban, warfarin, dabigatran, or rivaroxaban: a 1:1 propensity-score matched analysis. Lip et al. Presented at ACC 2016; Abstract 1268-34

April 2012
Real world comparison of major bleeding risk among non-valvular atrial fibrillation patients newly initiated on apixaban, warfarin, dabigatran, or rivaroxaban: a 1:1 propensity-score matched analysis. Lip et al. Presented at ACC 2016; Abstract 1268-34
HR, hazard ratio. Bold values indicate statistical significance. Limitations: abstract only; may include switchers from otherOACs; moderate sample size; limited variables used for adjustment.
Major bleeding during follow-up
Dabigatran was associated with a similar rate of major bleeding vs apixaban
HR 2.05 (1.50–2.79)
Apixaban(n=4828)
HR 2.06 (1.50–2.84)
Dabigatran(n=4828)
Apixaban(n=6721)
Rivaroxaban(n=6721)
Apixaban(n=6441)
Warfarin(n=6441)
HR 1.25 (0.84–1.87)
Propensity-score-matched HR (95% CI)

April 2012
Funding
• Bristol-Myers Squibb and Pfizer
Safety outcomes
• Bleeding-related and all-cause hospitalization
Methods
• Retrospective analysis of US Premier Hospital database (Jan 2012–March 2014) and Cerner Health Facts Hospital database (Jan 2012–Aug 2014)
• Adjusted for baseline characteristics but no propensity-score methods used
PatientsPremier Hospital database• N=74 730 (32 838 dabigatran,
37 754 rivaroxaban, 4138 apixaban)
Cerner Health Facts Hospital database
• N=14 201 (5753 dabigatran, 6635 rivaroxaban, 1813 apixaban)
Limitations
• OAC-experienced patients• Limited variables for adjustment
• Moderate sample size
• Only 1 month of follow-up• Patients included prior to
availability of apixaban
!
An early evaluation of bleeding-related hospital readmissions among hospitalized patients with nonvalvular atrial fibrillation treated with direct oral anticoagulants. Deitelzweig et al. Curr Med Res Opin 2016;32:573–82

April 2012
An early evaluation of bleeding-related hospital readmissions among hospitalized patients with nonvalvular atrial fibrillation treated with direct oral anticoagulants. Deitelzweig et al. Curr Med Res Opin 2016;32:573–82
*Frequency data not reported for the Cerner Health Facts database. OR, odds ratio. Limitations: includes OAC-experienced patients; limited variables used for adjustment; moderate sample size; 1 month of follow-up; patients included prior to availability of apixaban.
OR 1.2 (0.9–1.6); P=0.16
OR 1.1 (1.0–1.2); P=0.21
Dabigatran was associated with a similar risk of bleeding-related
or all-cause readmission compared with apixaban
ORs (95% CI) adjusted for baseline characteristics
Bleeding-related readmissions All cause readmissions
Hospital readmissions in the Premier Hospital database*
Dabigatran
Apixaban

April 2012
Funding
• Bristol-Myers Squibb and Pfizer
Safety outcomes
• All-cause and major bleeding-related hospitalization and length of stay
Methods
• Retrospective analysis of US Truven MarketScan and Medicare supplemental databases (Jan 2012–Dec 2013)
• Adjusted for baseline characteristics but no propensity-score methods used
• Follow up until admission, discontinuation or switch, or end of study
Patients
• New users of dabigatran, rivaroxaban, apixaban, or warfarin (may include switchers from another OAC)
• N=29 338 (4173 dabigatran, 10 050 rivaroxaban, 2402 apixaban, 12 713
warfarin)
Limitations
• Abstract only• Moderate sample size
!
What do real world data say about safety and resource use of oral anticoagulants? Early analysis of newly anticoagulated non-valvular atrial fibrillation patients using either apixaban, dabigatran, rivaroxaban or warfarin. Pan et al. Presented at ACC 2016; Abstract 1268-361

April 2012
What do real world data say about safety and resource use of oral anticoagulants? Early analysis of newly anticoagulated non-valvular atrial fibrillation patients using either apixaban, dabigatran, rivaroxaban or warfarin. Pan et al. Presented at ACC 2016; Abstract 1268-361
HR, hazard ratio. Bold values indicate statistical significance. Limitations: abstract only; may include switchers from otherOACs; moderate sample size.
Major bleeding-related hospitalization during follow-up
Dabigatran was associated with a similar rate of major bleeding
and hospital length of stay vs apixaban
HRs (95% CI) vs apixaban
HR 2.06 (1.19–3.57)
HR 1.18 (1.04–3.11)
HR 1.65 (0.90–3.00)

April 2012
What can we expect in the field of DOACs ?

April 2012Boehringer Ingelheim Clinical Trial Protocol, Trial No. 1160.204
RE-CIRCUIT™: robust data on the use of dabigatran in patients undergoing catheter ablation
Randomization(Month −1)
Warfarin (INR 2.0–3.0)
Dabigatran 150 mg BID
Day 0 (Ablation)
Target n=362 patients per arm (total N=724 patients)
Patients with paroxysmal or
persistent NVAFscheduled for catheter ablation, eligible for dabigatran 150 mg
BID according to local label
Pre-ablation4–8 weeks
Post-ablation60 days
Screening0–2 weeks Follow-up
Day 60(End of treatment)
Pr imaryendpoint:
ISTH majorbleeding

April 2012
Even the low dose dabigatran regimen displays an excellent profile in left atrial ablation procedures

April 2012
DAPT, dual antiplatelet therapy
1. Lip GY et al. Thromb Haemost 2010;103:13–28; 2. Schlitt A et al. Catheter Cardiovasc Interv 2013;82:E864–704; 3. Ruiz-Nodar JM et al. J Am Coll Cardiol 2008;51:818–25; 4. Nikolsky E et al. Am J Cardiol 2012;109:831–8;5. Lamberts M et al. J Am Coll Cardiol 2013;62:981–9; 6. Dewilde WJ et al. Lancet 2013;381:1107–15
RE-DUAL PCI™: There is a need for robust data on antithrombotic strategy for patients with AF undergoing PCI
PCI in patient with AF:expert consensus =
triple therapy1
Stroke prevention in
AF = OAC
Thrombosis prevention in
PCI = DAPT
~30% of AF patients at risk of stroke have coexisting CAD and
may require PCI:
BUT: how to balance benefit–risk with double vs triple
antithrombotic therapy?4–6
Additional data will help to optimize antithrombotic strategy
High risk of ischaemic CV events and bleeding1–3

April 2012
Antithrombotic therapy after an acute coronary syndrome in AF patients requiring anticoagulation
2016 ESC Guidelines for the management of atrial
fibrillation developed in collaboration with EACTS

April 2012
Antithrombotic therapy after elective percutaneous intervention in AF patients requiring anticoagulation
2016 ESC Guidelines for the management of atrial
fibrillation developed in collaboration with EACTS

April 2012
*Warfarin arm: 1 month after bare metal stent or 3 months after drug-eluting stent
Adapted from Cannon C. AHA 2013 and Boehringer Ingelheim data on file
RE-DUAL PCI™: two new approaches to improving care for patients with AF undergoing PCI
Dual primary endpoints: death, MI, stroke/SE and major bleeding
Patients with AF undergoing PCI (n=8520)
R
Dabigatran 150 mg BID + clopidogrel/ticagrelor
Screening
0–72 hours after PCI
Dabigatran 110 mg BID + clopidogrel/ticagrelor
Warfarin (INR 2.0–3.0) + clopidogrel/ticagrelor*
n=2840 patients per arm
Minimum treatment duration: 6 months

April 20121. Andersen K et al. Stroke 2009;40:2068–72; 2. Adams HP et al. Stroke 1993;24:35–41; 3. Hart RG et al. Lancet Neurol 2014;13:429–38
RE-SPECT ESUS™: There is currently limited data to guide preventative treatment after embolic strokes of undetermined source
92% of all strokes are ischaemic1,2
25% are cryptogenic2,3
If clearly specified diagnostic criteria are
fulfilled
ESUS3
A subgroup of these strokes are due to thromboembolism
~300 000 incident cases/year in North America and Europe3
Standard of care:Antiplatelets
Clinical data limited

April 2012
*All patients receive dabigatran 150 mg BID, unless ≥75 years or CrCl 30–50 mL/min. These patients receive dabigatran 110 mg BID; †0 days–6 months in patients aged >60 years with additional risk factors
Adapted from Boehringer Ingelheim press release 19 November 2013; available at: http://www.boehringer-ingelheim.com/news/news_releases/press_releases/2013/19_november_2013_dabigatranetexilate1.html ; accessed November 2014
RE-SPECT ESUS™: efficacy and safety of dabigatran for secondary stroke prevention after ESUS
Primary endpoints: stroke & SE // major bleeding
30-dayfollow-up0 days–3 months† 0.5–3 years
‘Diagnostic pathway’:
Assess with MRI/CTto rule out lacunae; vascular imagingand ≥24-hour rhythm monitoring to ruleout AF
Patients with ESUS(estimated n=6000) n=3000
n=3000
Dabigatran (150 or 110 mg BID)*
ASA (100 mg OD)
Placebo (matching dabigatran)
Placebo (matching ASA)
End of treatment
R

April 2012Huisman et al. Am Heart J 2014; Huisman et al. Am J Med 2015
GLORIA™-AF: observation registry programme with a unique study design
up to 56 000 patients Up to 2200 sites up to 50 countries
All patients
Phase IIICross-sectional and comparative analysis
Patients on dabigatran etexilate
Phase IICross-sectional, cohort, andcase-control analysis
Phase ICross-sectional analysis
Patients with newly diagnosed AF at risk of stroke (CHA2DS2-VASc score ≥1)
May 2011–Jan 2013

April 2012Huisman et al. ESC 2015
GLORIA™-AF Phase II (Europe): clear shift away from VKAs and ASA following introduction of the NOACs
Phase I(n=291)
Phase II(n=7108)
VKA 64% 38%
ASA 25% 5%
None 9% 4%
NOAC 0 52%

April 2012
Thank you very much for your attention
Bad Krozingen, 2008

April 2012
Thank you very much for your attention !!!!!!
Bad Krozingen, 2008