Embed Size (px)
Citation preview

Israel Surgical Israel Surgical
Association Association
Dead Sea Dead Sea 66//20122012
Ahmed Eid, MDAhmed Eid, MD
HeadHead, , Department Of Department Of Surgery, HadassahSurgery, Hadassah
Mount Scopus CampusMount Scopus Campus
JerusalemJerusalem
Mesenteric Ischemia

Mesenteric IschemiaMesenteric Ischemia

HistoryHistory 1951,Klass AA: Embolectomy in acute mesenteric occlusion.
Ann Surg 134:913-917
Mortality rate 70-90% up to 1970
1970,Boley and Clark: Angiography, Vasodilators
Mortality rate 60-80%
2000, introduction of MD –CTA in the diagnosis of AMI
No improvement in mortality rate for
the last four decades
Delay in diagnosis(8hours) and initiation of revascularization(2.5 hours)

Mesenteric blood flowMesenteric blood flow
CACA
SMASMA
IMAIMA
MCAMCA
Arc of Buhler Marginal artery of Drummond and the arc
of Riolan ( meandering mesenteric artery)
Auto regulatory ability

שאלה ראשונהשאלה ראשונה
??מה נכון לגבי הספקת דם מזנטריאליתמה נכון לגבי הספקת דם מזנטריאלית
מתפוקת הלב ורובה מכוון למוקוזהמתפוקת הלב ורובה מכוון למוקוזה 20%20% --מהווה כמהווה כ. . 11
מתפוקת הלב ורובה מכוון למוקוזהמתפוקת הלב ורובה מכוון למוקוזה 40%40%מהווה מהווה . . 22
לאחר ארוחהלאחר ארוחה 30%30% --מתפוקת הלב ועולה למתפוקת הלב ועולה ל 10%10% --מהווה רק כמהווה רק כ. . 33
מתפוקת הלב ורובה מכוון לשריריתמתפוקת הלב ורובה מכוון לשרירית 20%20% --מהווה כמהווה כ. . 44
Mesenteric blood flowMesenteric blood flow

Mesenteric blood flowMesenteric blood flow
2020--25%25% of CO (of CO (25 25 ml/KG BW/min)ml/KG BW/min) ( intensively perfused organ at rest)( intensively perfused organ at rest)
Increase to Increase to 3030% postprandial % postprandial
7070% is directed to mucosa/submucosa% is directed to mucosa/submucosa

Mesenteric Ischemia
Definition
Inadequate blood flow (Oxygen Delivery) to
visceral tissues which leads initially to
mucosal ischemia but eventually may lead
to necrosis of the entire bowel wall

Acute Mesenteric IschemiaAcute Mesenteric Ischemia
PathophysiologyPathophysiology
Inflammatory cell response, mediator surge and
breakdown of the epithelial barrier function with bacterial
translocation, and development of a systemic inflammatory
response.

Warm Ischemia Time (WIT)Warm Ischemia Time (WIT)
שאלה שניהשאלה שניה ::זמן האיסכמיה החמה של המעי הדק הוא זמן האיסכמיה החמה של המעי הדק הוא
עד שעהעד שעה. . 11
שעותשעות 66עד עד . . 22
שעותשעות 1212עד עד . . 33
שעותשעות 2424עד עד . . 44

Acute Mesenteric IschemiaAcute Mesenteric Ischemia PerspectivePerspective
WIT- 6 hours
Abdominal (Vascular ) Emergency

שאלה שלישיתשאלה שלישית
איסכמיה מזנטריאלית חריפה כוללת את המצבים איסכמיה מזנטריאלית חריפה כוללת את המצבים
::הבאים מלבדהבאים מלבד
חסימה אמבולית של עורק מזנטריאלית עליוןחסימה אמבולית של עורק מזנטריאלית עליון. . 11
חסימה טרומבוטית של עורק מזנטריאלית עליוןחסימה טרומבוטית של עורק מזנטריאלית עליון. . 22
קוליטיס איסכמית קוליטיס איסכמית . . 33
44 . .Mesenteric Vein ThrombosisMesenteric Vein Thrombosis
Classification of Intestinal Classification of Intestinal
IschemiaIschemia

Intestinal IschemiaIntestinal Ischemia
Acute Mesenteric IschemiaAcute Mesenteric Ischemia SMA Embolic OcclusionSMA Embolic Occlusion
SMA Thrombotic occlusionSMA Thrombotic occlusion
Non Non ––Occlusive Mesenteric Ischemia (NOMI)Occlusive Mesenteric Ischemia (NOMI)
Mesenteric Vein Thrombosis (MVTMesenteric Vein Thrombosis (MVT))
Chronic Mesenteric IschemiaChronic Mesenteric Ischemia
Ischemic colitisIschemic colitis
American Gastroenterological Association American Gastroenterological Association
20002000

Acute Mesenteric IschemiaAcute Mesenteric Ischemia
EpidemiologyEpidemiology
שאלה ארבעשאלה ארבע
::הסיבה השכיחה ביותר כיום לאיסכמיה מזנטריאלית חריפההסיבה השכיחה ביותר כיום לאיסכמיה מזנטריאלית חריפה
חסימה של עורק מזנטריאלי עליוןחסימה של עורק מזנטריאלי עליון. . 11
Mesenteric Vein Thrombosis .Mesenteric Vein Thrombosis .22
NOMINOMI-- Non Occlusive Mesenteric Ischemia .Non Occlusive Mesenteric Ischemia .33
44 . .Ischemic colitisIschemic colitis

Acute Mesenteric IschemiaAcute Mesenteric Ischemia
6767..22%%
1515..77%%
1515..44%%
Epidemiology of Mesenteric Vascular Disease: Clinical Implications
Stefan Acosta
Semin Vasc Surg 23:4-8 , 2010

Incidence Of AMIIncidence Of AMI
Dr Dr EitanEitan
How common AMI is relative to other How common AMI is relative to other
abdominal emergenciesabdominal emergencies
Age influenceAge influence

IncidenceIncidence 1212..99//100100,,000 000 personperson--yearyear
11//1000 1000 Hospital AdmissionsHospital Admissions
11//100 100 Acute abdomenAcute abdomen
Toney RJ, Cunningham CG. Acute mesenteric ischemia. Surgery 1993;114(3):489–90.
Schneider TA, Longo WE, Ure T, et al. Mesenteric ischemia. Acute arterial syndromes
. Dis Colon Rectum 1994;37(11):1163–74.
Schoots IG, Levi MM, Reekers JA, et al. Thrombolytic therapy for acute superior mesenteric
artery occlusion. J Vasc Interv Radiol 2005;16(3):317–29.

1% of all patients with acute abdomen have AMI
10% of patients aged over 70

Major IssuesMajor Issues
DiagnosisDiagnosis
Risk profilingRisk profiling
Targeted diagnosis (CT/ANGIO)Targeted diagnosis (CT/ANGIO)
Initial treatment Initial treatment EGDR EGDR
Fluid resuscitation, Antibiotic, Fluid resuscitation, Antibiotic,
HeparinHeparin
Surgery/Surgery/Endovascular/Combined Endovascular/Combined logistic, sequence, teamlogistic, sequence, team
Extent of resectionExtent of resection
Need for revascularizationNeed for revascularization
Second look policySecond look policy
Chronic anticoagulation policyChronic anticoagulation policy

Diagnosis
Nonspecific clinical presentationNonspecific clinical presentation
High index of suspicionHigh index of suspicion
Acute mesenteric Ischemia is a rather common
cause of acute abdominal pain
Only one third of patients who had acute mesenteric Only one third of patients who had acute mesenteric
ischemia were correctly diagnosed before surgical ischemia were correctly diagnosed before surgical
exploration or deathexploration or death
Mamode N, Pickford I, Leiberman P. Failure to improve outcome in acute mesentericMamode N, Pickford I, Leiberman P. Failure to improve outcome in acute mesenteric
ischaemia: sevenischaemia: seven--year review. Eur J Surg year review. Eur J Surg 19991999;;165165((33):):203203––88..

Diagnosis
Major symptom Abdominal Pain
Associated Symptoms: Bloating, Vomiting, Diarrhea
Embolic Thrombosis MVT NOMI
Clin sudden, rapid progression Subacute acute, subcaute vaiable
RISK F AF,LVaneurysm Abd. Angina ,sitophobia Hypercog State CHF,Dialysis
Recent MI,valvular dis Fem,HT,DM,Smoking Thrombophylia post heart surg
Cardiomyo,other emboli sec sepsis
LAB Hemoconcentration ,WBC>15000,Anion gap acidosis
Amylase,LDH
D-dimer, αα--GST, GST, D-lactate, I-FABP
Diagnostic MD-CT A MD-CTA MD-CT A ANGIO

Case PresentationCase Presentation
Dr. Chapchay KatherineDr. Chapchay Katherine

CaseCase
66 66 y.oy.o. male. male
Pacemaker Pacemaker 20082008
AtrialAtrial fibrillationfibrillation
HyperlipidemiaHyperlipidemia
AnkylosingAnkylosing spondilitisspondilitis
ObesityObesity
Meds: Meds: propafenonpropafenon, , coumadincoumadin, , simvastatinsimvastatin

Major ComplainMajor Complain
Diffuse abdominal pain for Diffuse abdominal pain for 6 6 hours hours
bloody diarrhea and vomitingbloody diarrhea and vomiting

Physical examinationPhysical examination
Fully conscious, Fully conscious, 170170//103103, pulse , pulse 6060, , 3636..44, ,
sat sat 9898%%
Heart, lungs normalHeart, lungs normal
Abdomen: soft, not tenderAbdomen: soft, not tender
Periphery: normal pulses, no signs of DVTPeriphery: normal pulses, no signs of DVT
PR : normal color of feces, with some PR : normal color of feces, with some
bloodblood

LabsLabs

PlanPlan
Working diagnosis Working diagnosis –– GE / lower GI GE / lower GI
bleedingbleeding
Admitted to surgical ward for observation Admitted to surgical ward for observation
and treatmentand treatment..

DrDr AsafAsaf
Assessment of the presented case Assessment of the presented case
((Risk Profiling for AMIRisk Profiling for AMI))
Evaluation ANGIO/CTEvaluation ANGIO/CT
Logistic of ORLogistic of OR

MD-CTA

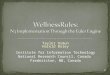
SMA Embolic OcclusionSMA Embolic Occlusion MDMD--CTA Sagittal ViewCTA Sagittal View

SMA Embolic OcclusionSMA Embolic Occlusion
Multiple emboli Mural Thickening ,Intramural gas
Absence of mural enhancement

SMA Thrombotic OcclusionSMA Thrombotic Occlusion

MD-CTA Acute Mesenteric Ischemia
Mural thickening ( symmetric and circumferential, usually does not exceed 1.5cm in thickness) .
Lack of mural enhancement
Intramural gas
Other CT findings:
Increased attenuation in the mesentery ( from mesenteric vascular
engorgement or mesenteric fluid)
Small intestinal dilatation
Ascites

Case PresentationCase Presentation
ContinuedContinued
During the first During the first 2 2 days of hospitalization days of hospitalization
the patient was intermittently painful, but the patient was intermittently painful, but
stable, soft abdomen , normal labsstable, soft abdomen , normal labs
On the third day after admission the On the third day after admission the
patient developed increasing pain and patient developed increasing pain and
peritonitisperitonitis

labslabs


MD-CTA

MD-CTA

Case PresentationCase Presentation
ContinuedContinued
Exploratory laparotomyExploratory laparotomy
Large amount of free turbid fluidLarge amount of free turbid fluid
Severe Ischemia from duodenum until Severe Ischemia from duodenum until
20 20 cm from ileocm from ileo--cecal valvececal valve

Case Presentation
Continued

Dr Dr OvnatOvnat
Heparin Y/N ,WhenHeparin Y/N ,When
Extent of resectionExtent of resection
Second LookSecond Look

ProceduresProcedures
Heparin Heparin
SMA EmbolectomySMA Embolectomy
Resection of distal Resection of distal 2 2 meters of small bowelmeters of small bowel
Bogota’s bag closureBogota’s bag closure
Case Presentation
Continued

Second lookSecond look
( ( 24 24 hours after hours after 11stst operationoperation))
Necrosis of the small bowel Necrosis of the small bowel beginning from distal duodenum up beginning from distal duodenum up to the terminal ileum.to the terminal ileum.
Procedure: total small bowel Procedure: total small bowel resection and primary anastomosis resection and primary anastomosis of duodenum to terminal ileum (of duodenum to terminal ileum (10 10 cm from ileocm from ileo--cecal valve).cecal valve).



Case PresentationCase Presentation
ContinuedContinued
Uneventful recoveryUneventful recovery
Transthoracic Echo: No thrombiTransthoracic Echo: No thrombi

TreatmentTreatment SMA Thrombotic occlusion SMA Thrombotic occlusion
Exploratory laparotomy :Confluent necrosisExploratory laparotomy :Confluent necrosis
EndarterectomyEndarterectomy
Bypass: Antegrade/Retro multivessel bypassBypass: Antegrade/Retro multivessel bypass
Hybrid Procedure : Retrograde Open Mesenteric Stent
(ROMS)
Bowel resection Bowel resection ±± Second lookSecond look
Endovascular therapy :Endovascular therapy :Thrombolysis ± PTA/ Stent
Emerging approach in selectedEmerging approach in selected

Dr Dr YofeYofe
Endovascular Vs Open Surgical TreatmentEndovascular Vs Open Surgical Treatment

Endovascular Revascularization
VS Traditional (surgical) Therapy in Acute
Mesenteric Ischemia
Successful endovascular treatment was achieved in 87%.
Mortality rate dropped from 50% to 36% mainly in thrombotic
SMA occlusion
Necrotic bowel resection decreased from 160 cm to 52 cm
69% required adjuvant laparotomy ( 31% no need for
laparotomy)
Acute renal failure decreased from 50% to 27%
Pulmonary failure decreased from 64% to 27%
A comparison of endovascular revascularization with traditional
therapy for the treatment of acute mesenteric ischemia
Zachary M,… and Daniel G. Clair, MD, Cleveland, Ohio
J Vasc Surg 2011;53:698-705

TreatmentTreatment SMA Thrombotic occlusionSMA Thrombotic occlusion

Summary
Acute mesenteric ischemia is still a challenging diagnosis to
do in the light of its relative rarity, NONSPECIFIC CLINICAL
PICTURE AND ABSENCE OF DIANOSTIC CHEMICAL TEST
High index of suspicion following risk profiling patients with
acute abdominal pain should prompt Diagnostic targeting
using MD-CTA or angiogram
Once the diagnosis of SMA occlusive mesenteric ischemia is
maid
Swift bowel revascularization should
be the aim

Summary
Heparin
OR1 setup
Recruit vascular surgeon
Vascular prep and drape
Peritonitis: Open surgery
Thrombectomy, bypass ,or ROM
Bowel resection
Schedule second look
No Peritonitis ,High risk: Endovascular
Adjuvant laparotomy

MVTMVT
Case presentation Case presentation ––Dr David HochsteinDr David Hochstein

History
63 y.o.m
Severe right upper quadrant pain of one
day duration
Vomiting

Physical examination
Full consciousness, in pain, vomiting
100, 147/87, 36.5 c, 98%
Abdomen: diffuse peritonitis

Labs
WBC 19000
CRP 4.5
Chemistry, renal function, liver
function, pro time - normal

X-Rays




Exploratory laparotomy
Necrotic small bowel loop, 60 cm from
ICV, with bloody fluid
Resection of small bowel loop and
primary anastomosis


Post operative course
Anticoagulation
Antibiotics

Pathology report
22 cm segment of small bowel
Hemorrhagic necrosis
Blood clots in mesenteric veins

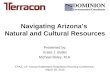
MVTMVT
Clinical PresentationClinical Presentation

MVT
Hypo attenuating
SMV thrombus Mural thickening
Mural enhancement

TreatmentTreatment MVTMVT
Nonoperative management: HeparinNonoperative management: Heparin
Exploratory laparotomy :peritonitisExploratory laparotomy :peritonitis
Only clearly nonviable or perforated Only clearly nonviable or perforated
intestine should be resentedintestine should be resented
secondsecond--look look laparotomieslaparotomies are frequently are frequently
necessary to preserve as much viable necessary to preserve as much viable
intestine as possibleintestine as possible
Thrombolysis:PTC,TIPS,SMA,IntraoperativeThrombolysis:PTC,TIPS,SMA,Intraoperative
( ( Esp. Portal vein Thrombosis)Esp. Portal vein Thrombosis)
ThrombectomyThrombectomy

NOMI
Clinical PresentationClinical Presentation

NOMI

TreatmentTreatment NOMINOMI
Systemic anticoagulationSystemic anticoagulation
CatheterCatheter--based directed arterial infusion of based directed arterial infusion of
papaverine at papaverine at 30 30 to to 60 60 mg/h or mg/h or prostaglandin E1
AfterloadAfterload--reducing agents and vasodilatorsreducing agents and vasodilators
Laparotomy: signs of peritonitis, worsening Laparotomy: signs of peritonitis, worsening
sepsis suggestive of intestinal necrosis or sepsis suggestive of intestinal necrosis or
perforationperforation

End End
QuestionsQuestions