Embed Size (px)
Citation preview
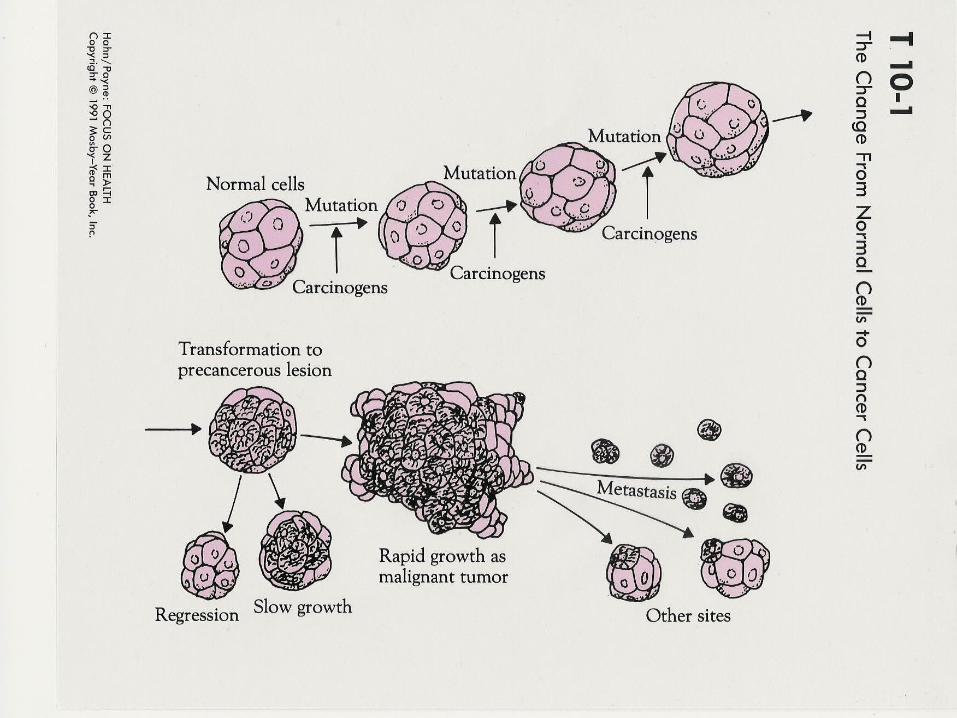
WHAT IS CANCER
Group of diseases characterized by abnormal cell growth and replication.
Precancerous cells often are destroyed by the immune system.
If not destroyed, they may form tumors.
© 2008 McGraw-Hill Higer Education. All rights reserved.
http://acs.healthology.com/hybrid/hybrid-autodetect.aspx?content_id=3790&focus_handle=lung-cancer&brand_name=acs
CANCER CONTINUED
Tumors may be benign (don’t spread) or malignant (metastasize) – both can be dangerous but malignant cancer can move to other sites in the body (metastasize).
Malignant tumors: invade surrounding tissues, spread through metastasis, grow uncontrollably, are not capsulated, are usually fatal if untreated.
CANCER: Group of diseases characterized by uncontrolled growth and spread of abnormal cells• CAUSES: External, Internal
• TREATMENT: Surgery, Radiation, Chemotherapy
• STAGES: I (Early or in situ); II (Local); III (Regional); IV (Distant or advanced)
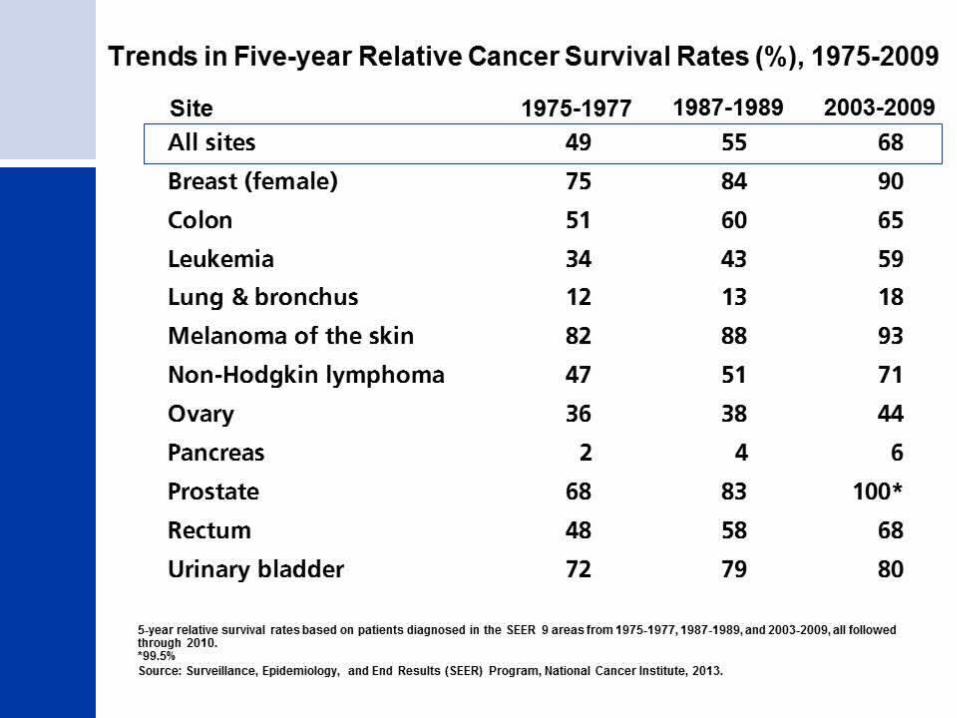
• SURVIVAL: Five (5) year relative survival rate means patients who were diagnosed and treated at least five years ago.
• SCREENINGS: One half of all diagnosed cancers can be detected by screenings
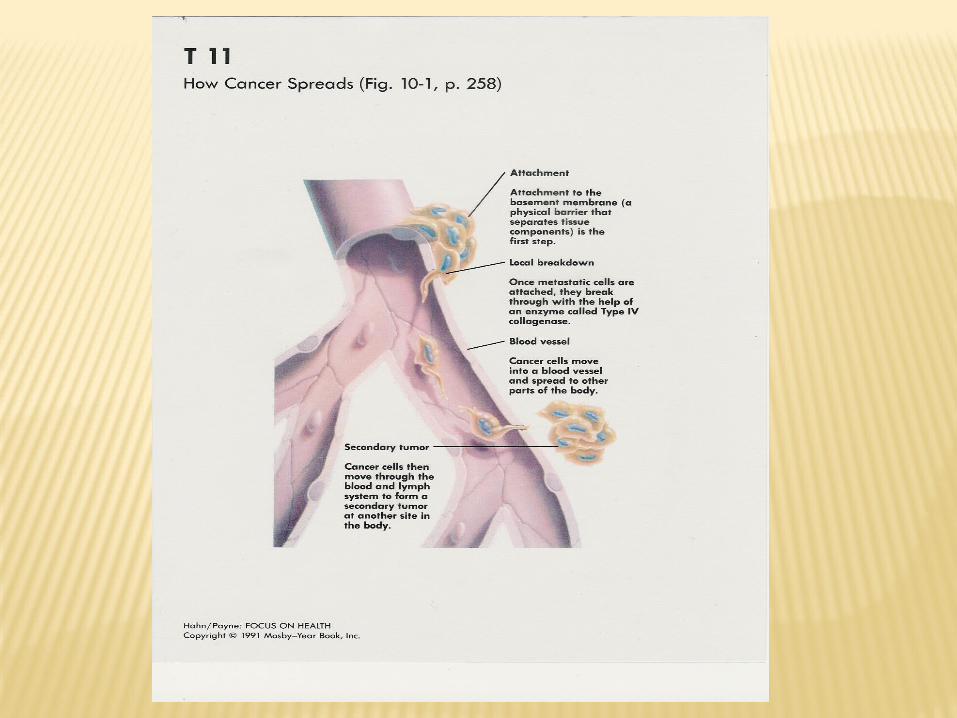
• METASTASIS: Cancer cells break away from primary tumor and migrate to other tissues through lymph or blood system
http://www.cancer.org/Cancer/BreastCancer/MoreInformation/breast-cancer-videos
CANCER: Group of diseases characterized by uncontrolled growth and spread of abnormal cells• CAUSES:
• TREATMENT:
• STAGES: I (Early or in situ); II (Local); III (Regional); IV (Distant or advanced)
• SURVIVAL:
• SCREENINGS:
• METASTASIS:
• carcinomas
• Sarcomas
• lymphomas
• leukemias
• angiogenesis
• oncology
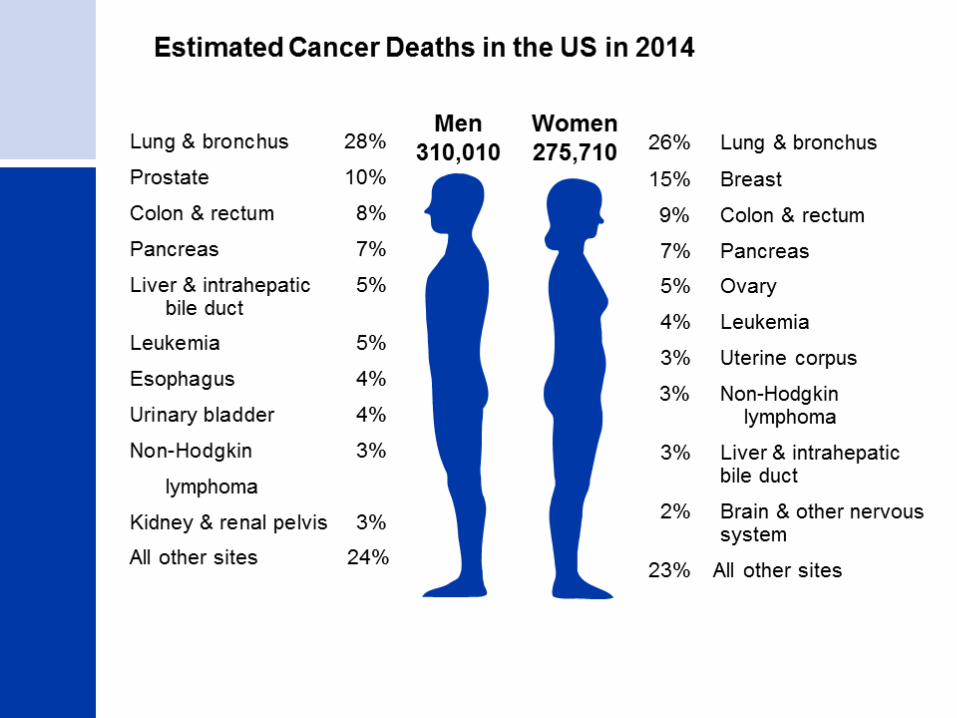
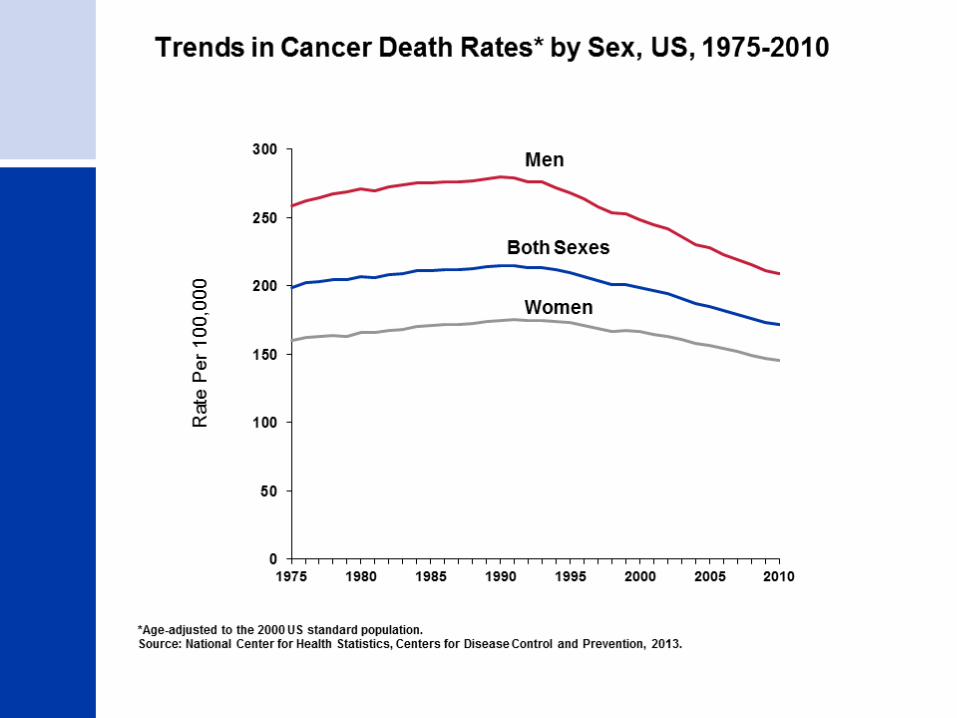
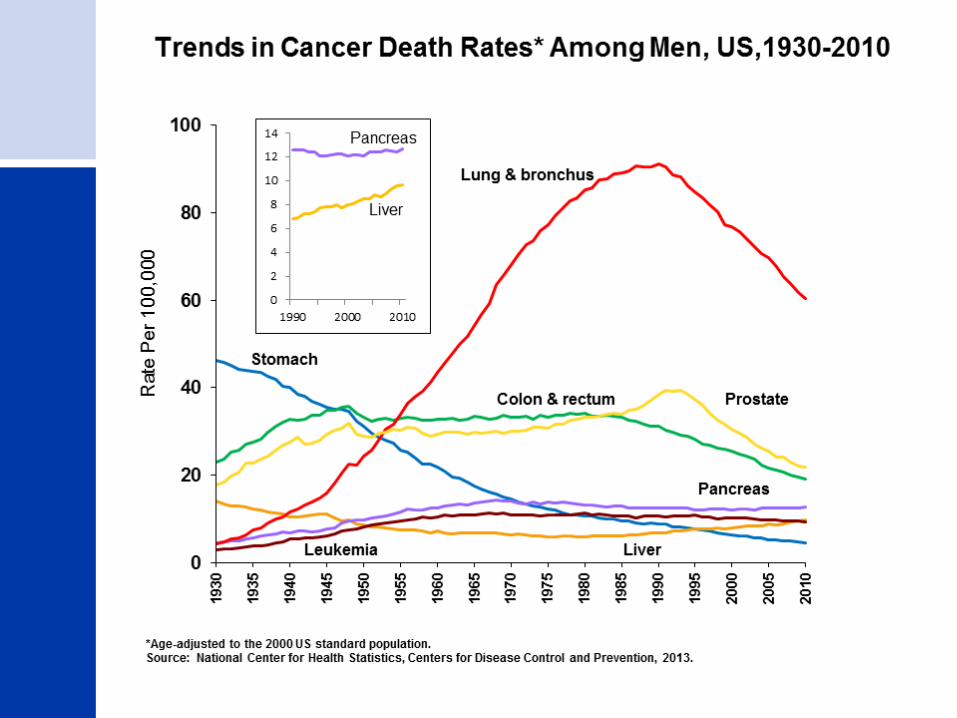
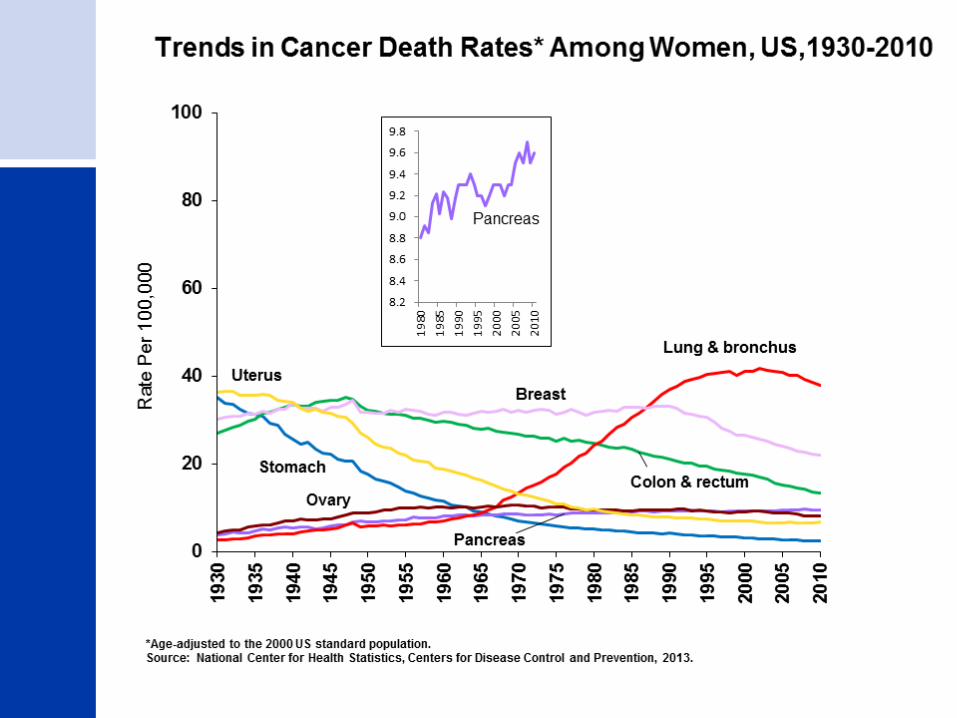
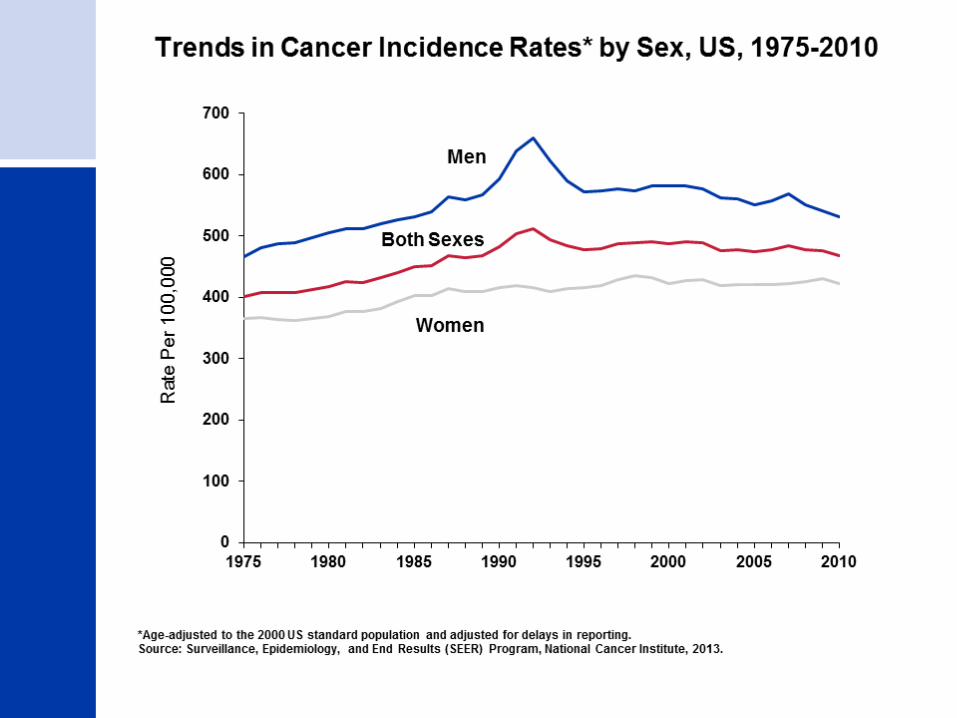
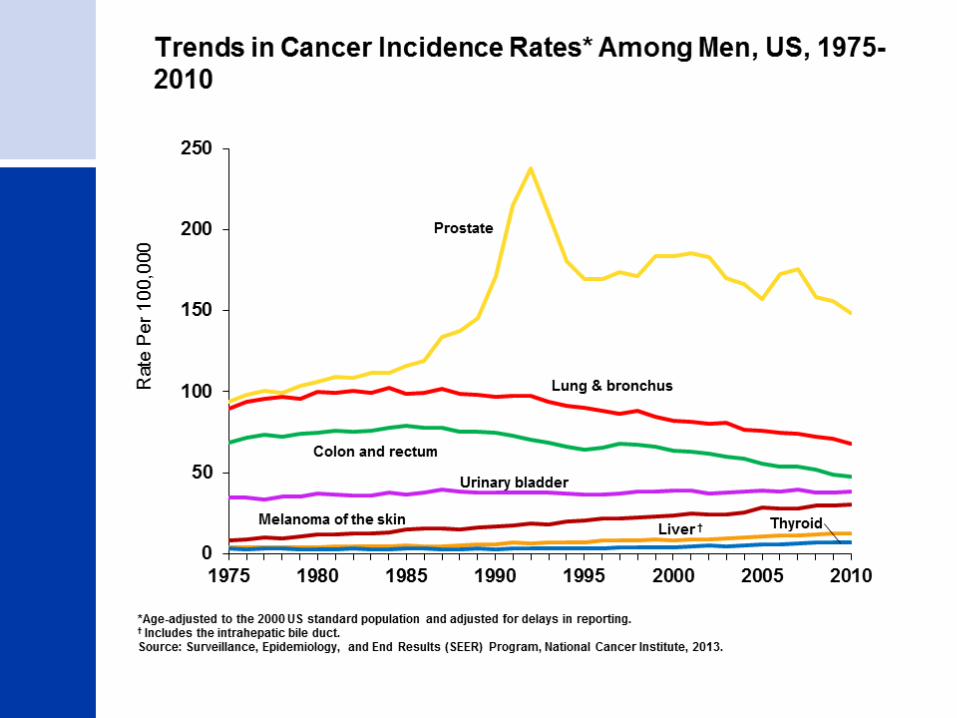
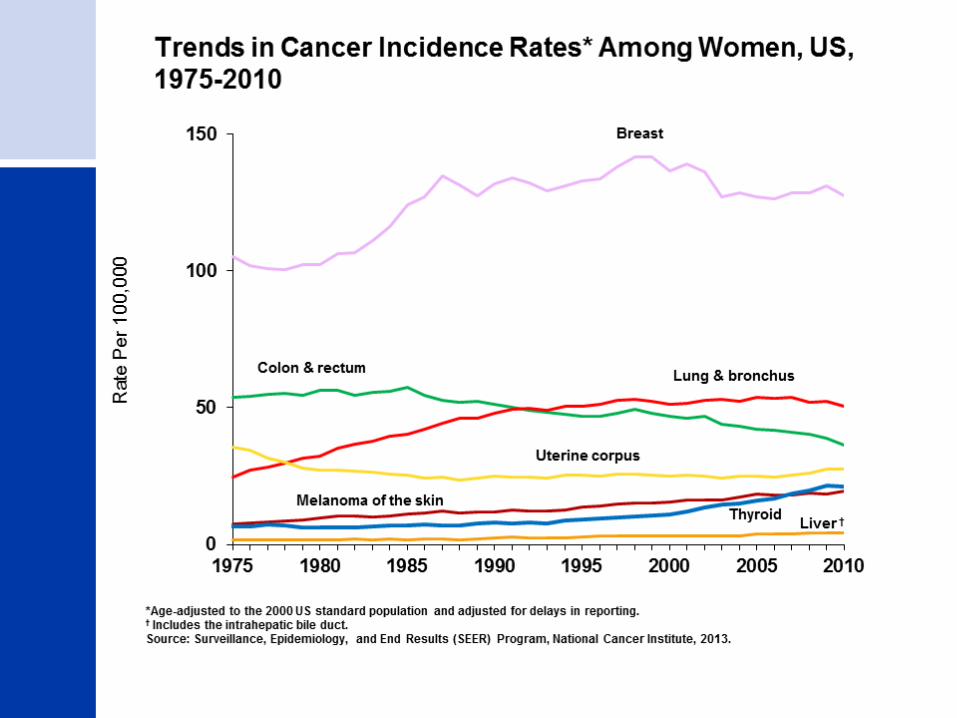
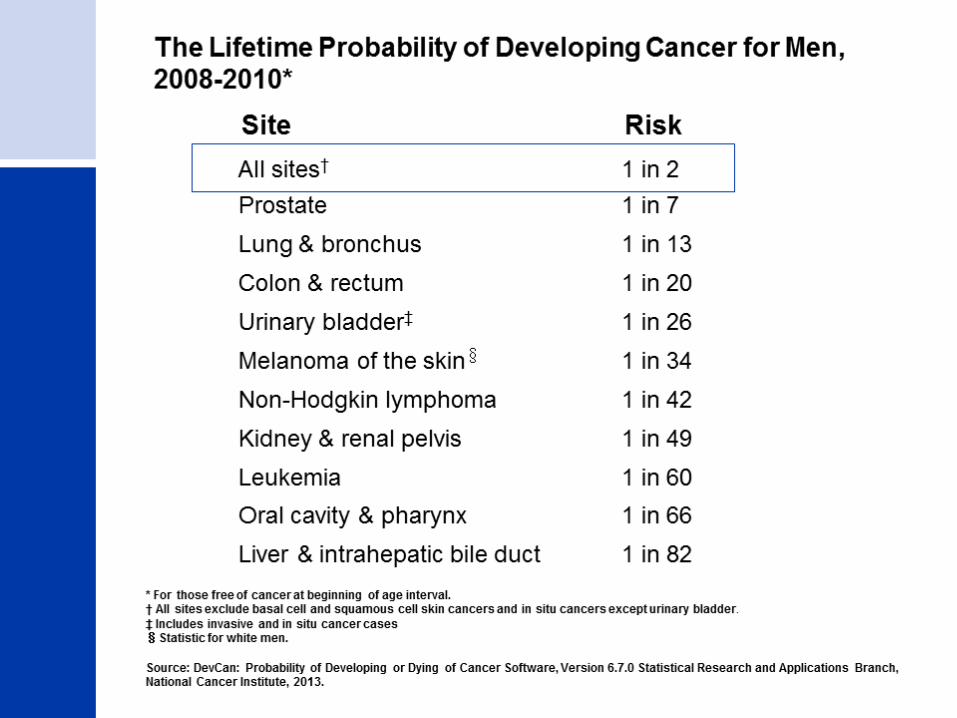
Cancer Statistics 2014
A Presentation from theAmerican Cancer Society
©2014, American Cancer Society, Inc.
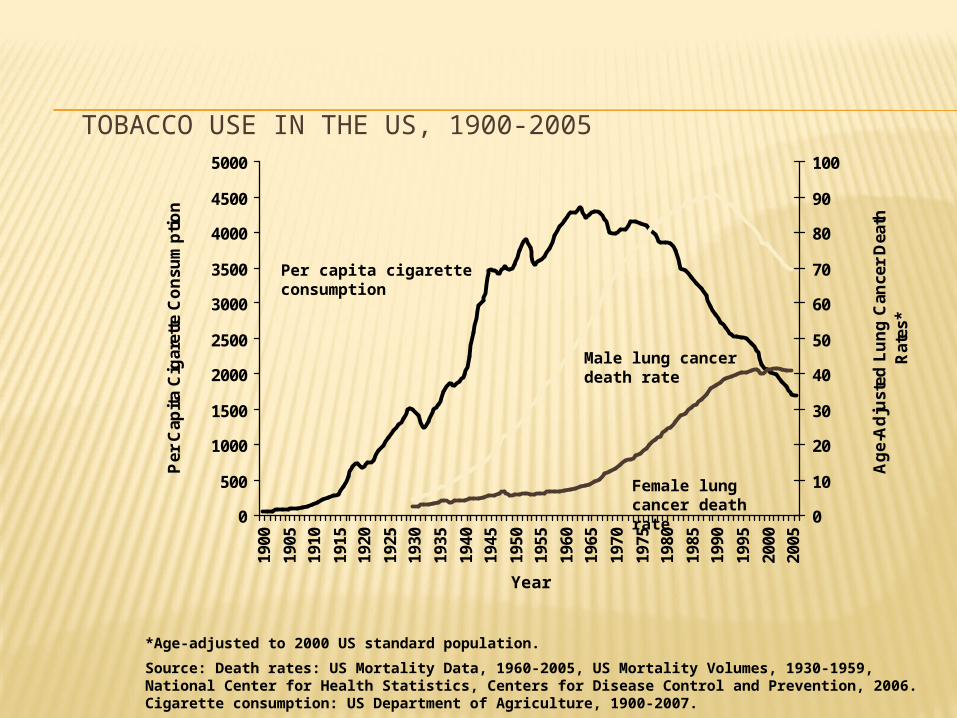
TOBACCO USE IN THE US, 1900-2005
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
1900
1905
1910
1915
1920
1925
1930
1935
1940
1945
1950
1955
1960
1965
1970
1975
1980
1985
1990
1995
2000
2005
Year
Per
Cap
ita
Cig
aret
te C
on
sum
pti
on
0
10
20
30
40
50
60
70
80
90
100
Ag
e-A
dju
sted
Lu
ng
Can
cer
Dea
th
Rat
es*
*Age-adjusted to 2000 US standard population.
Source: Death rates: US Mortality Data, 1960-2005, US Mortality Volumes, 1930-1959, National Center for Health Statistics, Centers for Disease Control and Prevention, 2006. Cigarette consumption: US Department of Agriculture, 1900-2007.
Per capita cigarette consumption
Male lung cancer death rate
Female lung cancer death rate

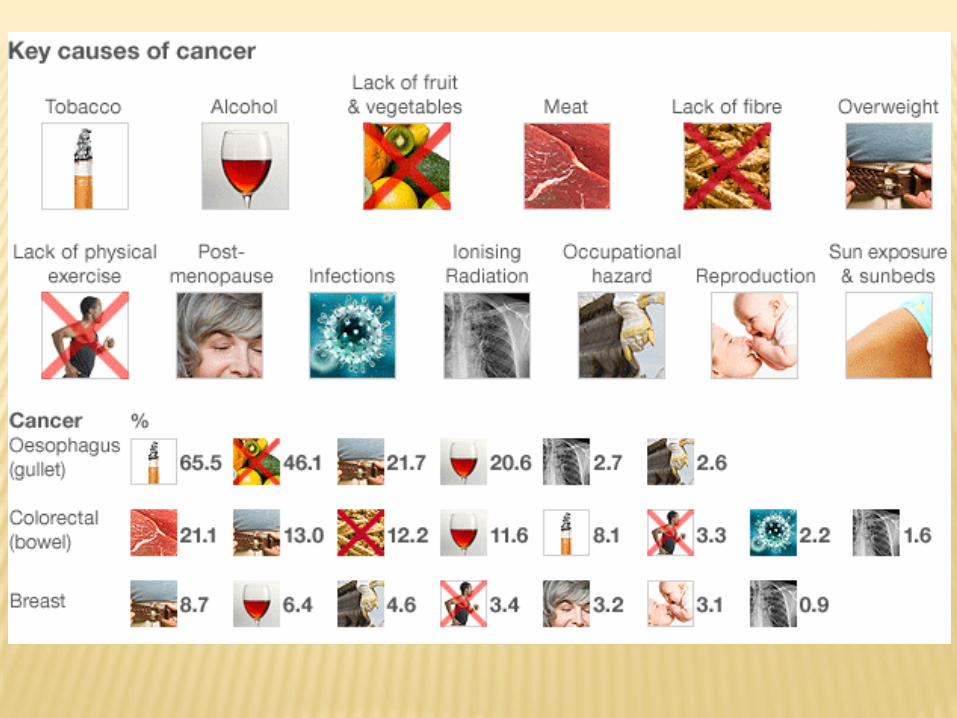

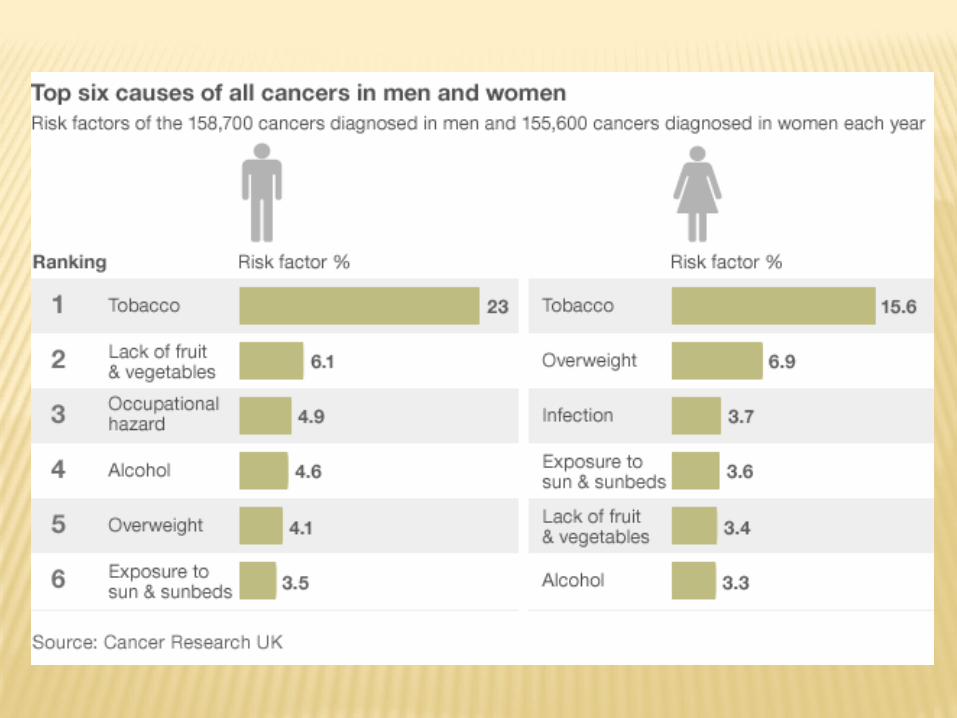
RISK FACTORS
Primary Risk Factors: tobacco, sun exposure, diet, inactivity, obesity.
Secondary Risk Factors: excessive alcohol intake, some viral infections, radiation, certain chemicals.
Approximately 80% of all cancers may be related to lifestyle choices.
http://www.webmd.com/video/foods-after-cancer
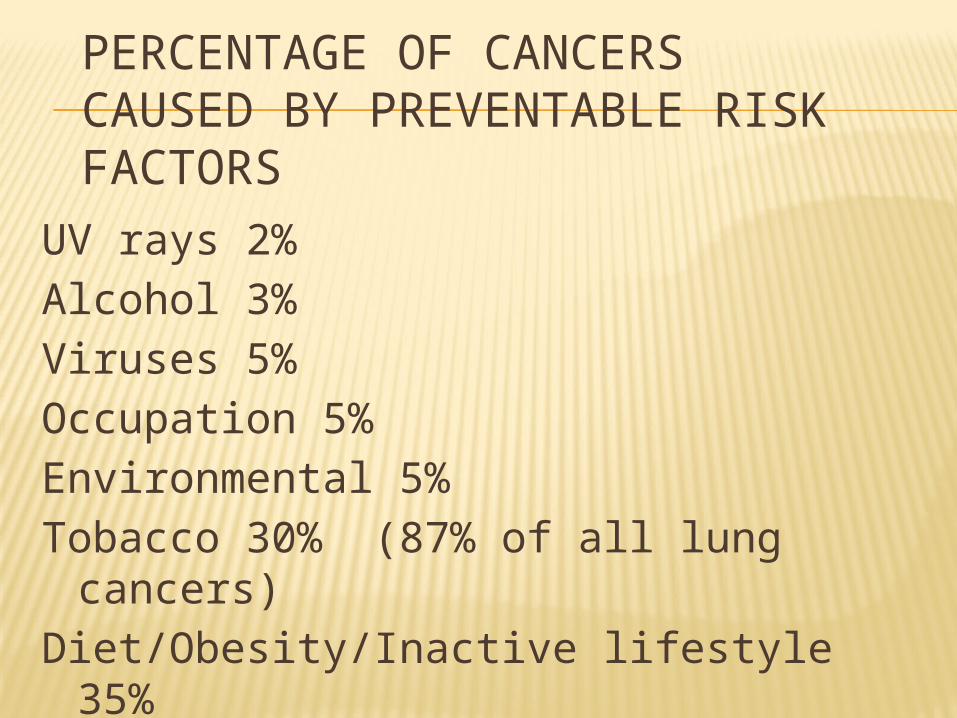
PERCENTAGE OF CANCERS CAUSED BY PREVENTABLE RISK FACTORS
UV rays 2%Alcohol 3%Viruses 5%Occupation 5%Environmental 5%Tobacco 30% (87% of all lung cancers)Diet/Obesity/Inactive lifestyle 35%
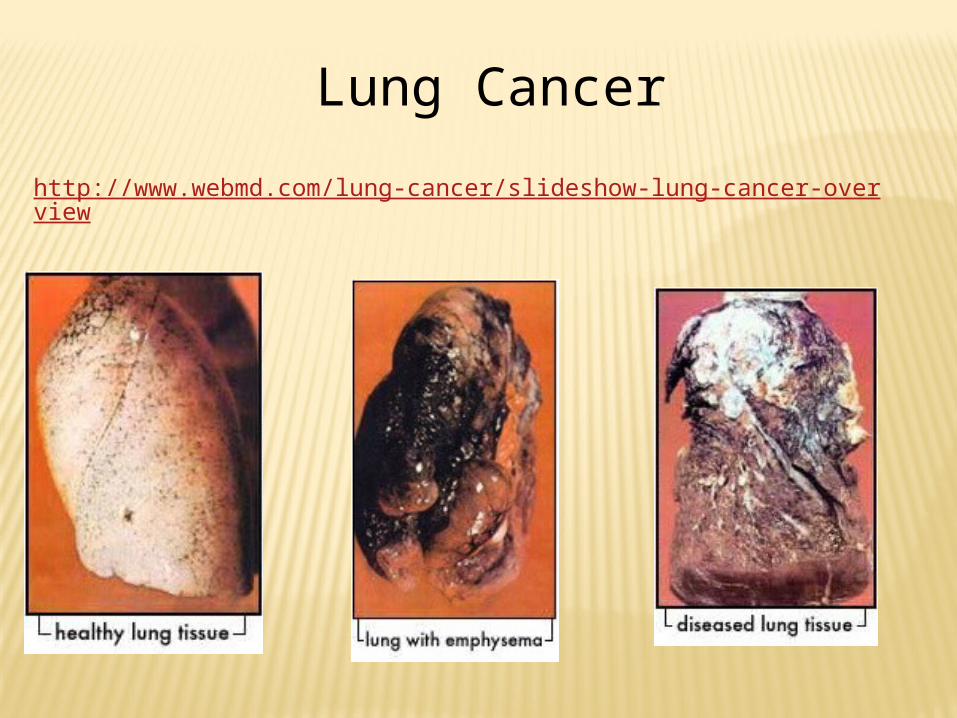
Lung Cancer
http://www.webmd.com/lung-cancer/slideshow-lung-cancer-overview
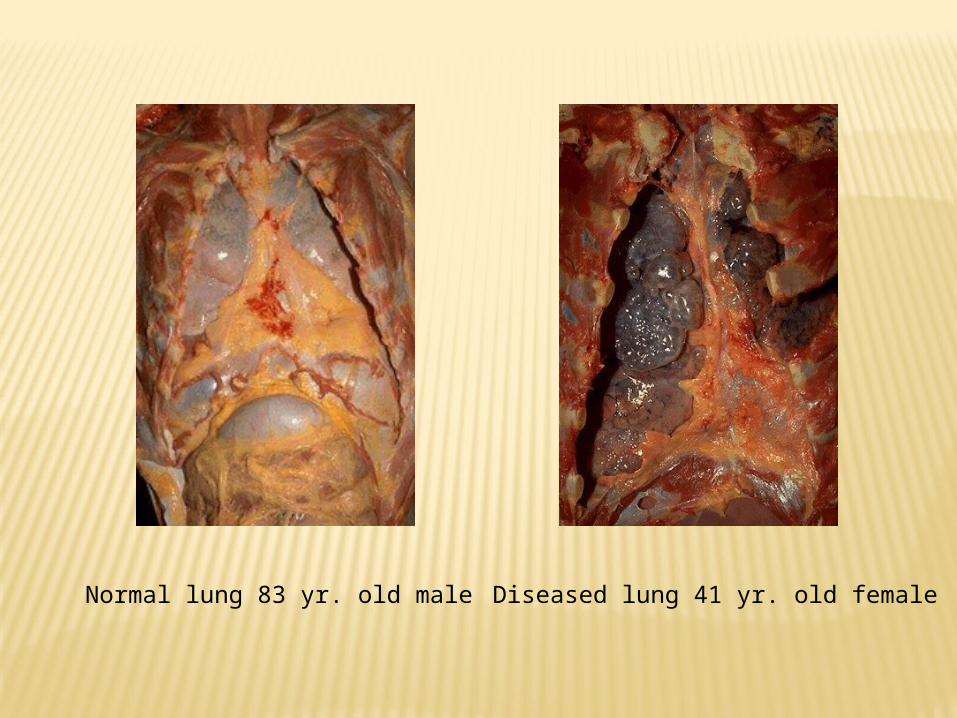
Normal lung 83 yr. old male Diseased lung 41 yr. old female
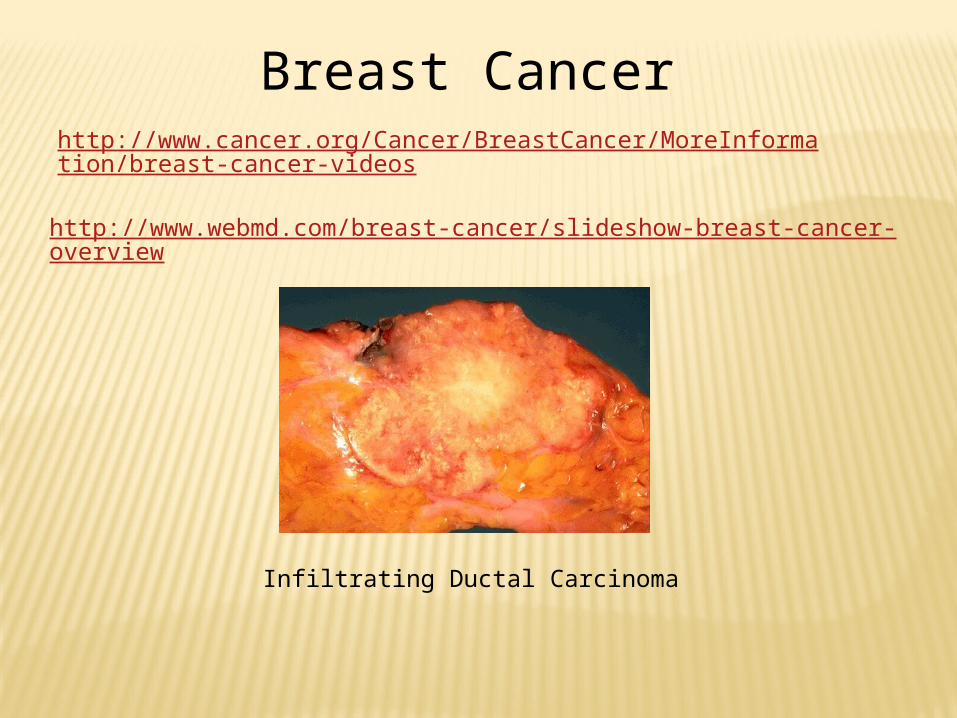
Infiltrating Ductal Carcinoma
Breast Cancer
http://www.webmd.com/breast-cancer/slideshow-breast-cancer-overview
http://www.cancer.org/Cancer/BreastCancer/MoreInformation/breast-cancer-videos

SCREENING GUIDELINES FOR THE EARLY DETECTION OF BREAST CANCER, AMERICAN CANCER SOCIETY
Yearly mammograms are recommended starting at age 40. A clinical breast exam should be part of a periodic health
examination, about every 3 years for women in their 20s and 30s. Asymptomatic women aged 40 and older should continue to undergo a clinical breast exam, preferably annually*.
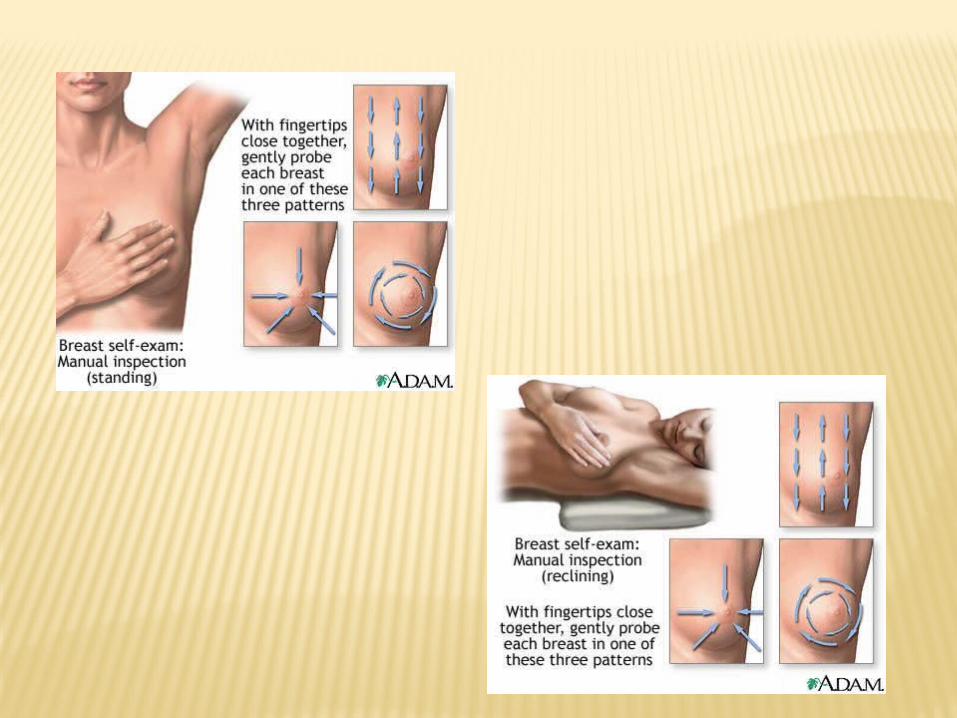
Beginning in their early 20s, women should be told about the benefits and limitations of breast-self examination. Women should know how their breasts normally feel and report any breast changes promptly to their health care providers.
__________* Beginning at age 40 years, annual CBE should be performed prior to mammography
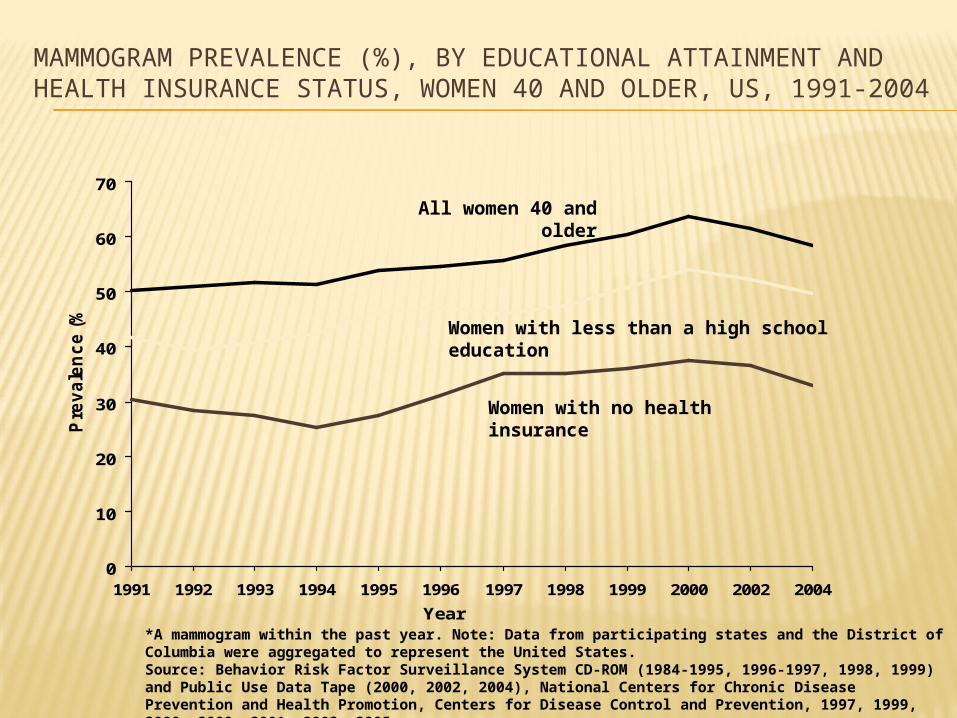
MAMMOGRAM PREVALENCE (%), BY EDUCATIONAL ATTAINMENT AND HEALTH INSURANCE STATUS, WOMEN 40 AND OLDER, US, 1991-2004
0
10
20
30
40
50
60
70
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2002 2004
Year
Pre
va
len
ce
(%
)
*A mammogram within the past year. Note: Data from participating states and the District of Columbia were aggregated to represent the United States.Source: Behavior Risk Factor Surveillance System CD-ROM (1984-1995, 1996-1997, 1998, 1999) and Public Use Data Tape (2000, 2002, 2004), National Centers for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, 1997, 1999, 2000, 2000, 2001, 2003, 2005.
Women with less than a high school education
Women with no health insurance
All women 40 and older
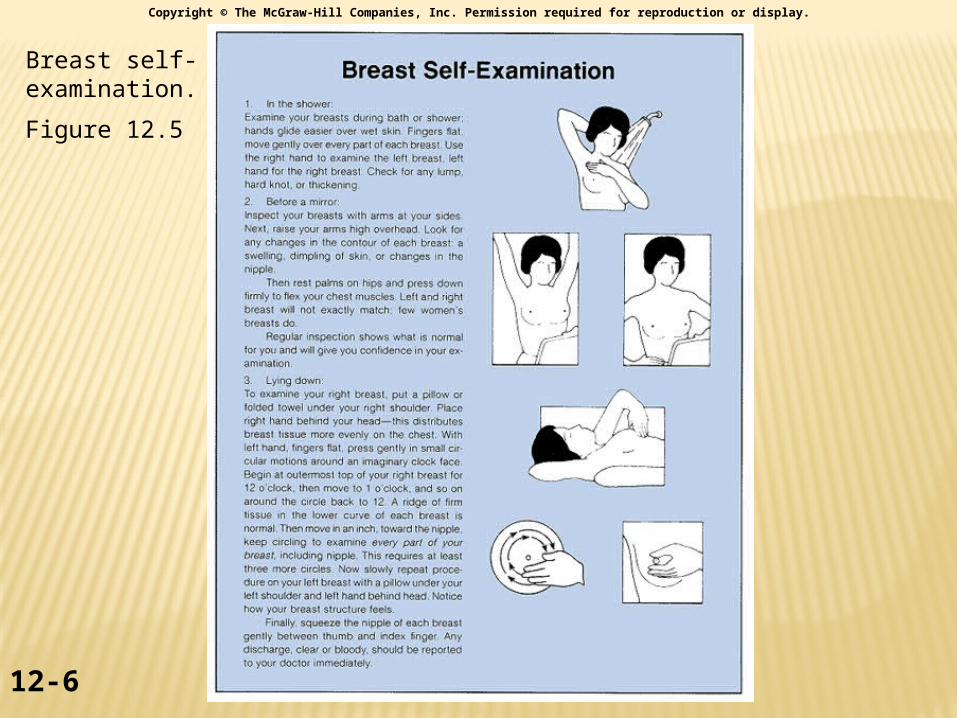
Breast self-examination.
Figure 12.5
12-6
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.

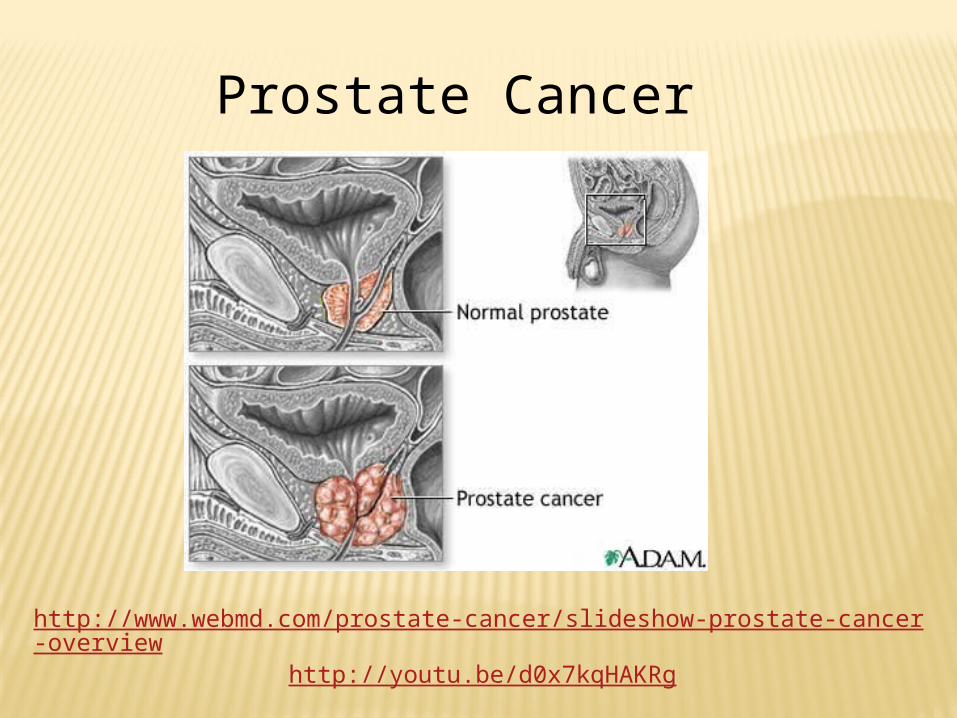
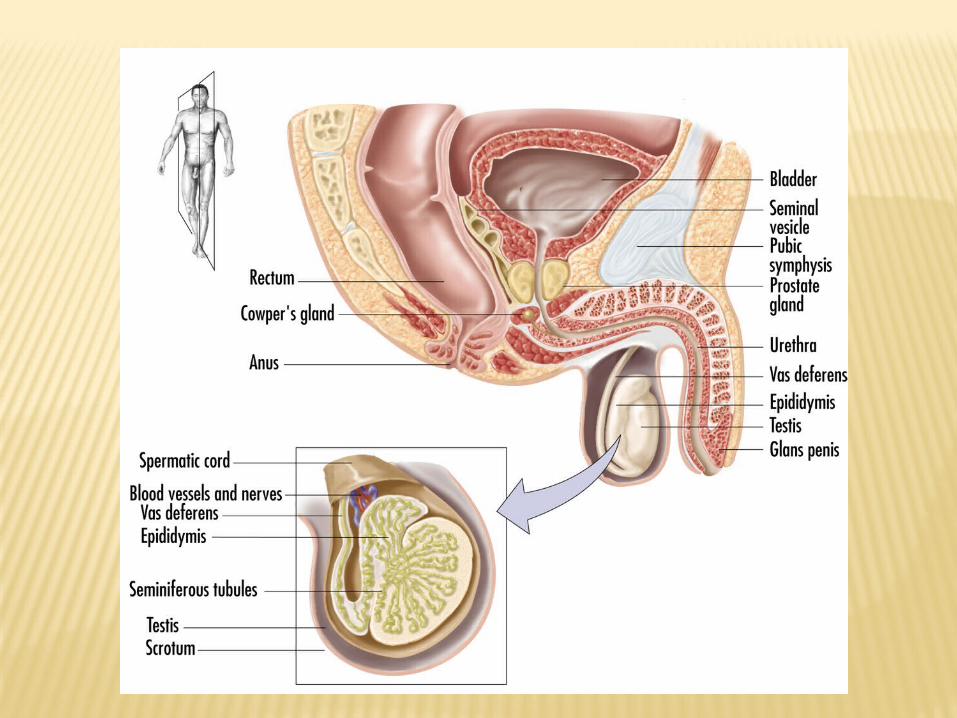
Prostate Cancer
http://www.webmd.com/prostate-cancer/slideshow-prostate-cancer-overview
http://youtu.be/d0x7kqHAKRg
•Risk increases with age•Only 25% of diagnoses are in men under the age of 65•African-Americans have a prostate cancer incidence double that of Caucasians•Men with a family history of prostate cancer have 2-3 times the risk•A diet high in saturated animal fat can double your risk.
SCREENING GUIDELINES FOR THE EARLY DETECTION OF PROSTATE CANCER, AMERICAN CANCER SOCIETY
Beginning at age 50, to men who have a life expectancy of at least 10 years, health care providers should discuss the potential benefits and limitations of prostate cancer early detection testing with men and offer the PSA blood test and the digital rectal examination.*
___________* Information should be provided to men regarding the benefits
and limitations of testing so that an informed decision concerning testing can be made with the clinician’s assistance.
57
44
29
53
42
26
50
37
22
0
10
20
30
40
50
60
Total Less than a high schooleducation
No health insurance
Pre
va
len
ce
(%
)
2001 2002 2004
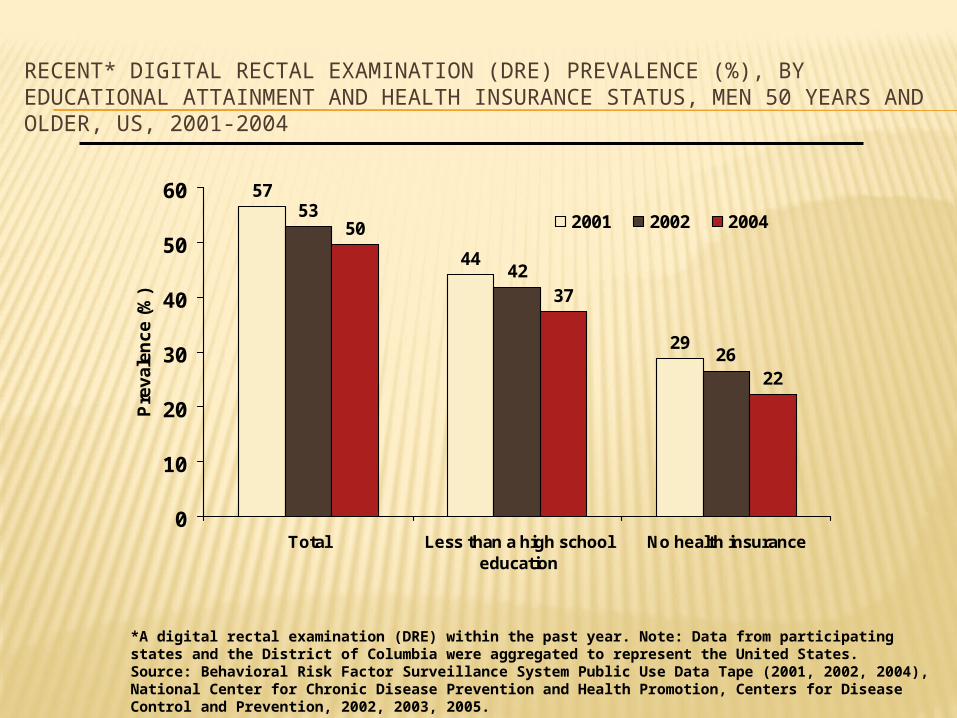
RECENT* DIGITAL RECTAL EXAMINATION (DRE) PREVALENCE (%), BY EDUCATIONAL ATTAINMENT AND HEALTH INSURANCE STATUS, MEN 50 YEARS AND OLDER, US, 2001-2004
*A digital rectal examination (DRE) within the past year. Note: Data from participating states and the District of Columbia were aggregated to represent the United States. Source: Behavioral Risk Factor Surveillance System Public Use Data Tape (2001, 2002, 2004), National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, 2002, 2003, 2005.
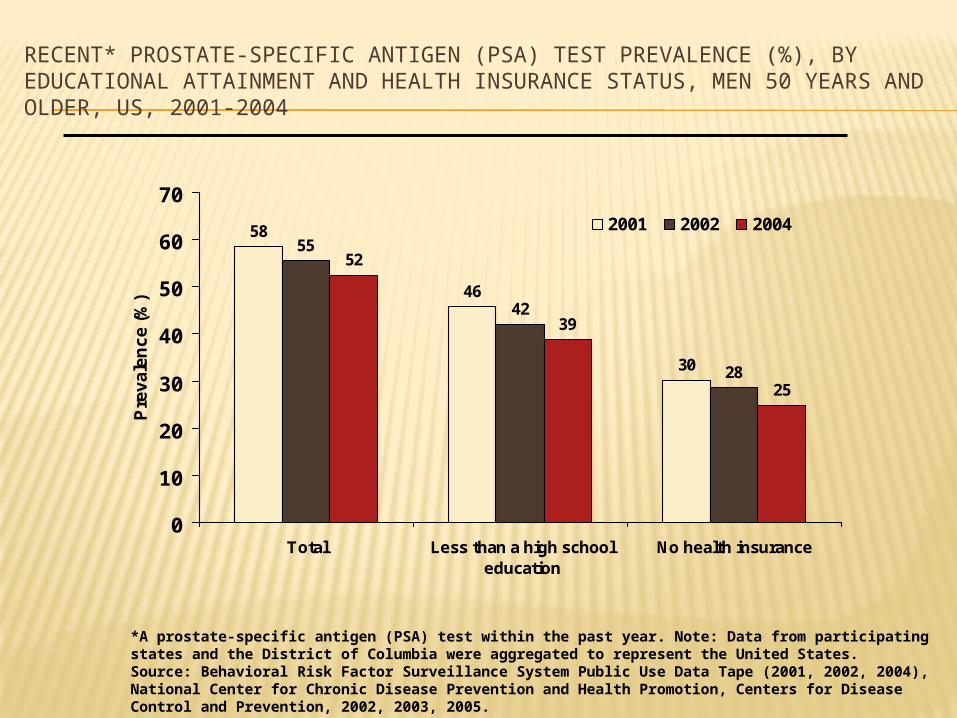
58
46
30
42
28
52
39
25
55
0
10
20
30
40
50
60
70
Total Less than a high schooleducation
No health insurance
Pre
va
len
ce
(%
)
2001 2002 2004
RECENT* PROSTATE-SPECIFIC ANTIGEN (PSA) TEST PREVALENCE (%), BY EDUCATIONAL ATTAINMENT AND HEALTH INSURANCE STATUS, MEN 50 YEARS AND OLDER, US, 2001-2004
*A prostate-specific antigen (PSA) test within the past year. Note: Data from participating states and the District of Columbia were aggregated to represent the United States. Source: Behavioral Risk Factor Surveillance System Public Use Data Tape (2001, 2002, 2004), National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, 2002, 2003, 2005.
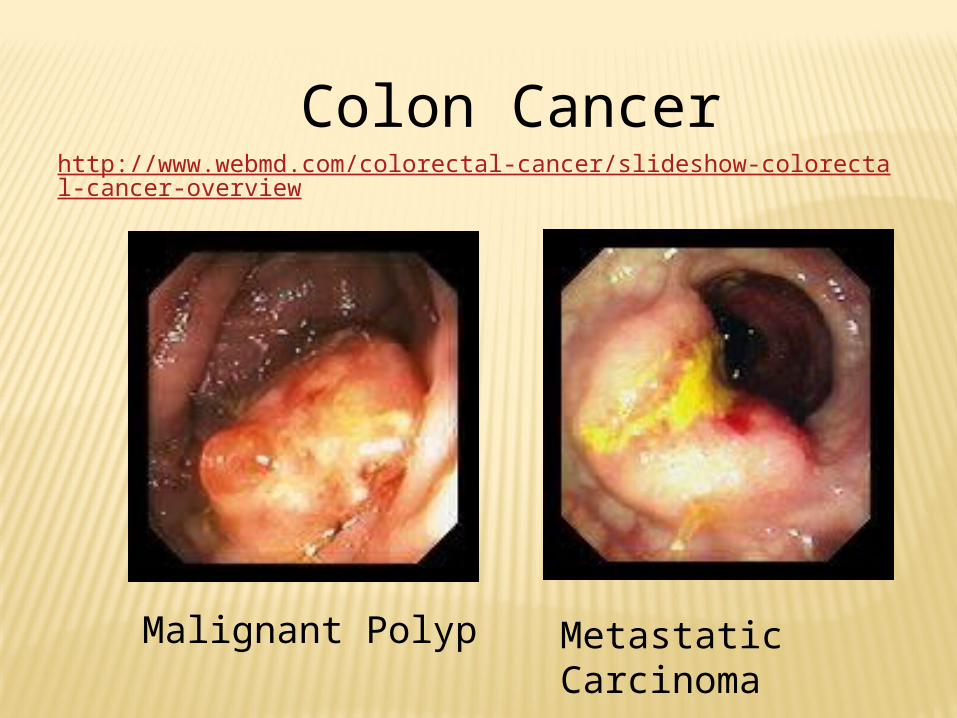
Metastatic Carcinoma
Malignant Polyp
Colon Cancerhttp://www.webmd.com/colorectal-cancer/slideshow-colorectal-cancer-overview
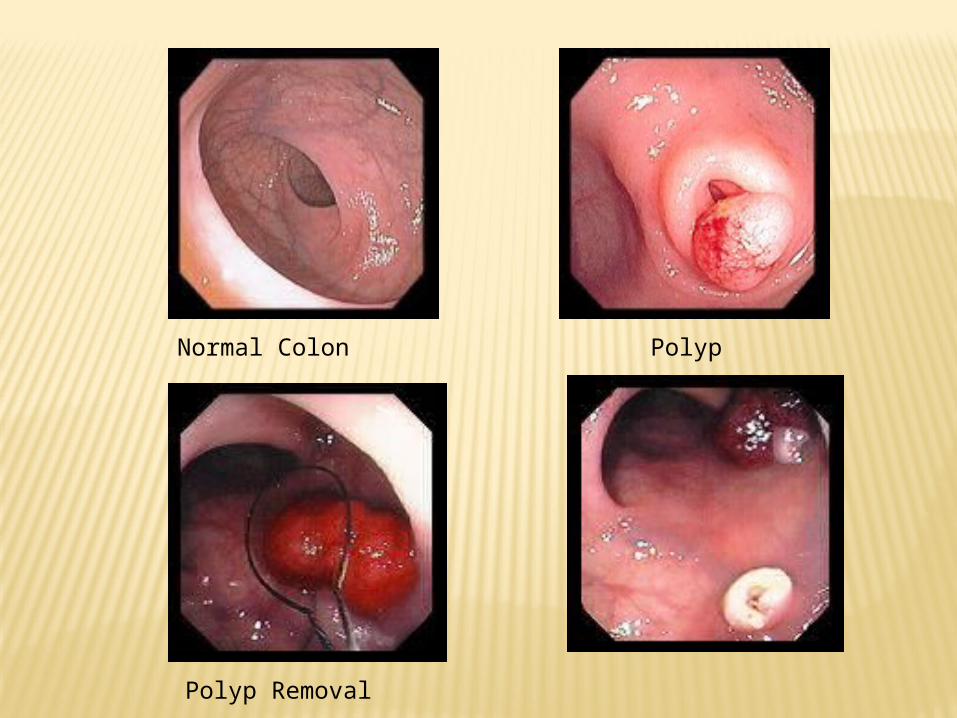
PolypNormal Colon
Polyp Removal
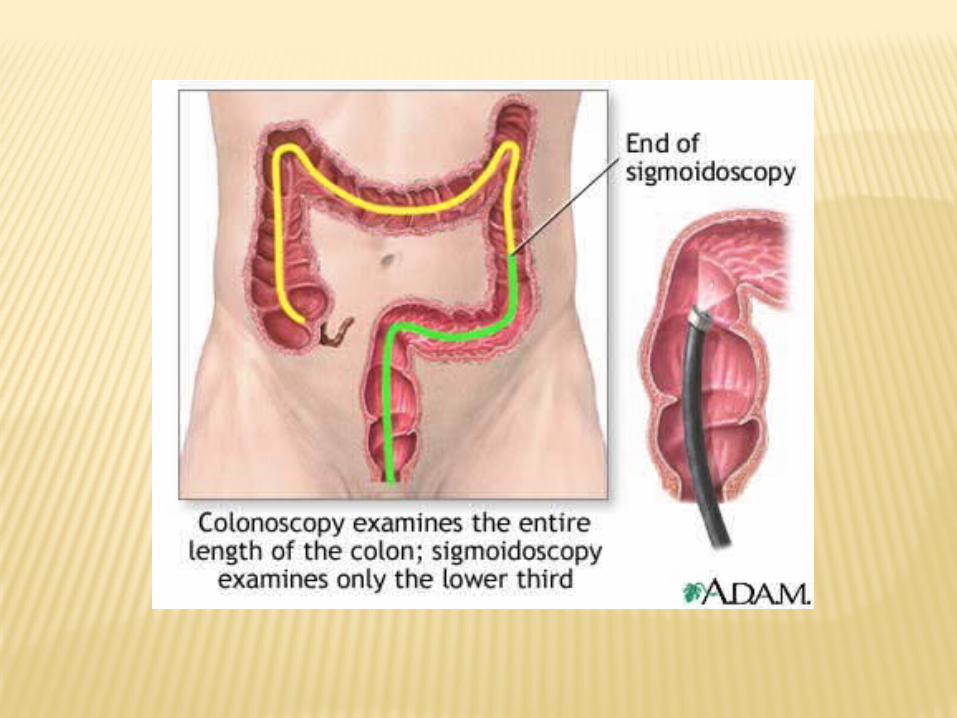
SCREENING GUIDELINES FOR THE EARLY DETECTION OF COLORECTAL CANCER AND ADENOMAS, AMERICAN CANCER SOCIETY 2008
Beginning at age 50, men and women should follow one of the following examination schedules:
A flexible sigmoidoscopy (FSIG) every five years A colonoscopy every ten years A double-contrast barium enema every five years A Computerized Tomographic (CT) colonography every five years A guaiac-based fecal occult blood test (FOBT) or a fecal
immunochemical test (FIT) every year A stool DNA test (interval uncertain)
Tests that detect adenomatous polyps and cancer Tests that primarily detect cancer
People who are at moderate or high risk for colorectal cancer should talk with a doctor about a different testing schedule
3128
16
34
29
16
39
32
17
41
33
18
45
36
19
0
5
10
15
20
25
30
35
40
45
50
Total Less than a high schooleducation
No health insurance
Pre
vale
nce
(%
)
1997 1999 2001 2002 2004
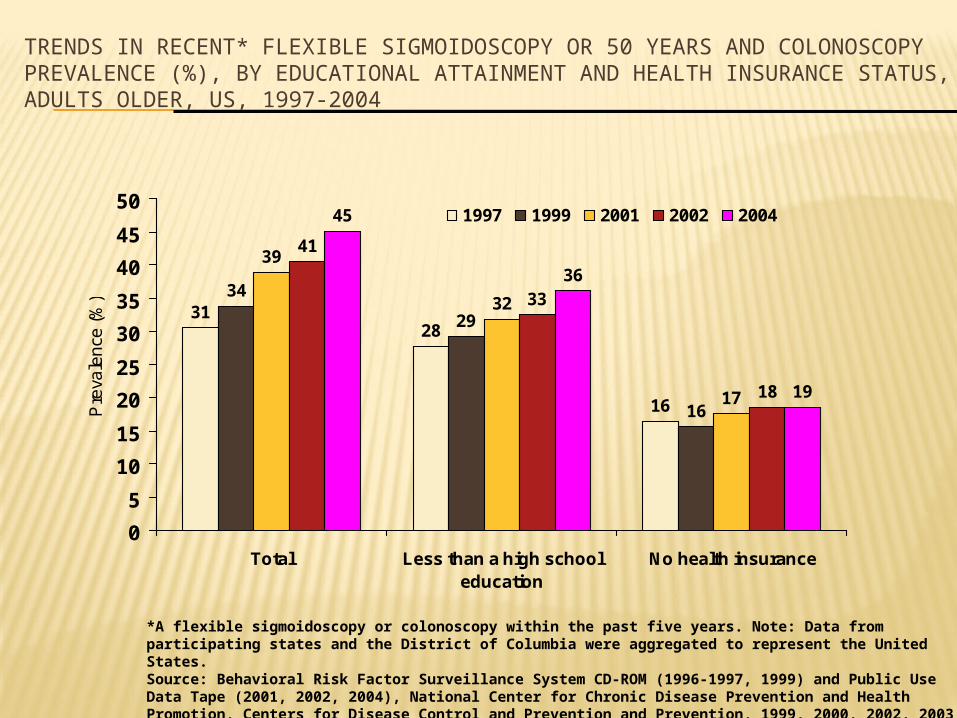
TRENDS IN RECENT* FLEXIBLE SIGMOIDOSCOPY OR 50 YEARS AND COLONOSCOPY PREVALENCE (%), BY EDUCATIONAL ATTAINMENT AND HEALTH INSURANCE STATUS, ADULTS OLDER, US, 1997-2004
*A flexible sigmoidoscopy or colonoscopy within the past five years. Note: Data from participating states and the District of Columbia were aggregated to represent the United States. Source: Behavioral Risk Factor Surveillance System CD-ROM (1996-1997, 1999) and Public Use Data Tape (2001, 2002, 2004), National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention and Prevention, 1999, 2000, 2002, 2003, 2005.
20
16
8
21
16
9
18
12
22
16
9
19
14
9
24
0
5
10
15
20
25
30
Total Less than a high schooleducation
No health insurance
Pre
va
len
ce
(%
)
1997 1999 2001 2002 2004
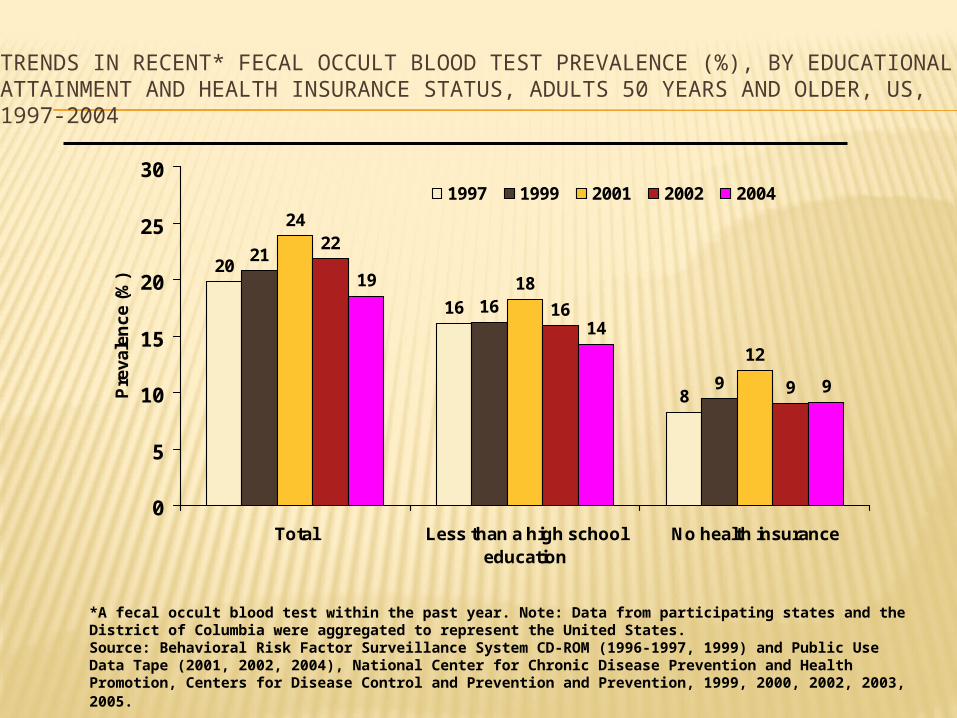
TRENDS IN RECENT* FECAL OCCULT BLOOD TEST PREVALENCE (%), BY EDUCATIONAL ATTAINMENT AND HEALTH INSURANCE STATUS, ADULTS 50 YEARS AND OLDER, US, 1997-2004
*A fecal occult blood test within the past year. Note: Data from participating states and the District of Columbia were aggregated to represent the United States. Source: Behavioral Risk Factor Surveillance System CD-ROM (1996-1997, 1999) and Public Use Data Tape (2001, 2002, 2004), National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention and Prevention, 1999, 2000, 2002, 2003, 2005.

SCREENING GUIDELINES FOR THE EARLY DETECTION OF CERVICAL CANCER, AMERICAN CANCER SOCIETY
Screening should begin approximately three years after a women begins having vaginal intercourse, but no later than 21 years of age.
Screening should be done every year with regular Pap tests or every two years using liquid-based tests.
At or after age 30, women who have had three normal test results in a row may get screened every 2-3 years with cervical cytology (either conventional or liquid-based Pap test) alone, or every 3 years with a human papillomavirus DNA test plus cervical cytology.
Women 70 and older who have had three or more consecutive Pap tests in the last ten years may choose to stop cervical cancer screening.
Screening after a total hysterectomy (with removal of the cervix) is not necessary unless the surgery was done as a treatment for cervical cancer.
The vaccine now in use requires a series of 3 shots over a one-year period. It has been approved by the FDA and should be covered by most insurance. The American Cancer Society recommends the vaccine for girls when they are 11 or 12, before they begin having sex. It is also recommended as a “catch up” for women aged 13 to 18, and that women age 19 to 26 talk to their doctor about whether the vaccine is right for them. It is important to realize that the vaccine doesn’t protect against all cancer-causing types of HPV, so Pap tests are still needed.
The second way to prevent cancer of the cervix is to have a Pap test. The Pap test can detect HPV infection and pre-cancers. Treatment of these problems can stop cervical cancer before it develops fully into an invasive cancer.
Cervical Cancer Prevention
SKIN CANCER Exposure to the sun is the main cause of
skin cancer. 1 in 6 Americans will have skin cancer,
making it the most common cancer. Prevention is the key:
avoid prolonged exposure plan activities during morning and evening use sunscreen avoid tanning protect children from the sun – even one
exposure could increase risk for future cancer, use screenings and prevention techniques
© 2008 McGraw-Hill Higher Education. All rights reserved.

Basel Cell Carcinoma
A Scar-Like Area →
A Pink Growth A Shiny Bump
← A Reddish Patch
An Open Sore

SQUAMOUS CELL CARCINOMA
An open sore that bleeds and crusts and persists for weeks
An elevated growth with a central depression that occasionally bleeds.
A persistent, scaly red patch with irregular borders that sometimes crusts or bleeds.
A wart-like growth that crusts and occasionally bleeds.

Melanoma
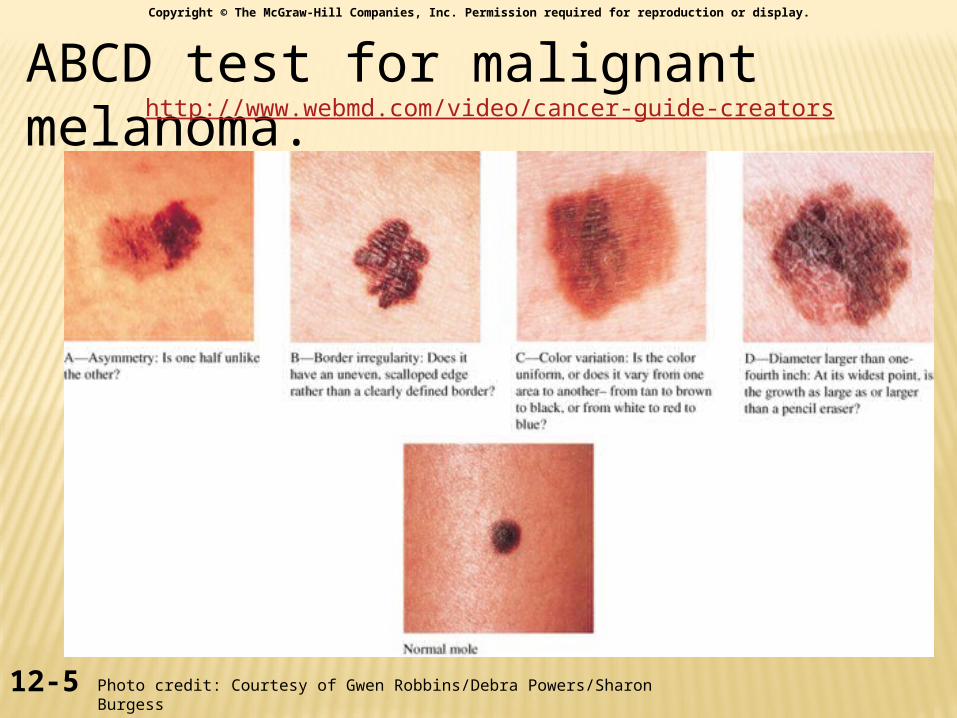
ABCD test for malignant melanoma.
12-5
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
Photo credit: Courtesy of Gwen Robbins/Debra Powers/Sharon Burgess
http://www.webmd.com/video/cancer-guide-creators
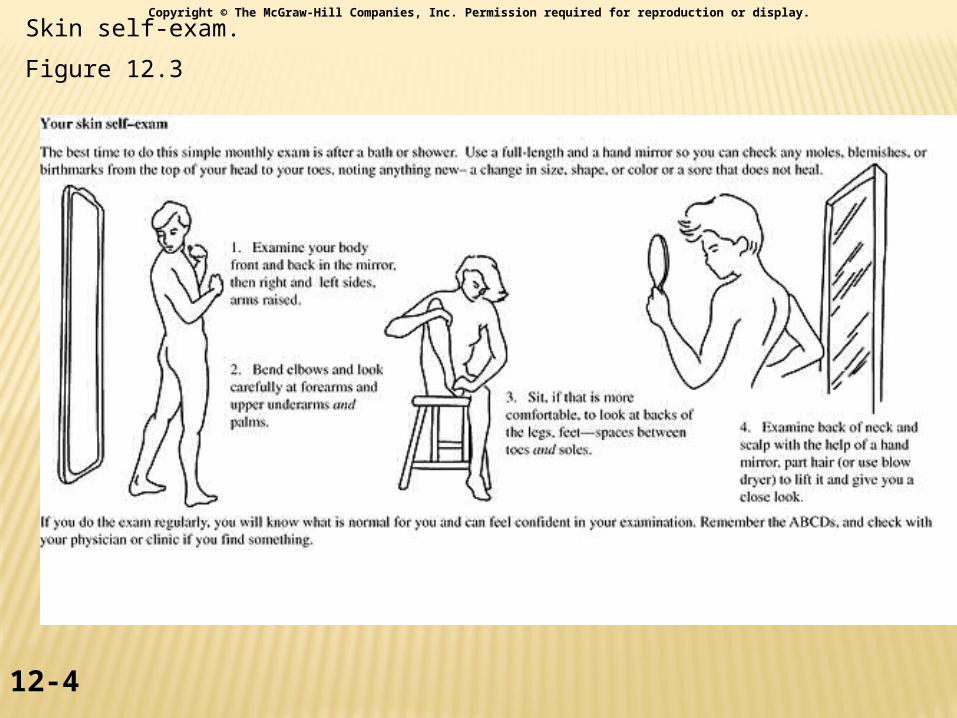
Skin self-exam.
Figure 12.3
12-4
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.

Testicular Cancer
Normal testicle
Testicular Cancer
http://www.webmd.com/video/testicular-cancer-protection
http://www.webmd.com/video/marks-testicular-self-exam
12-10
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
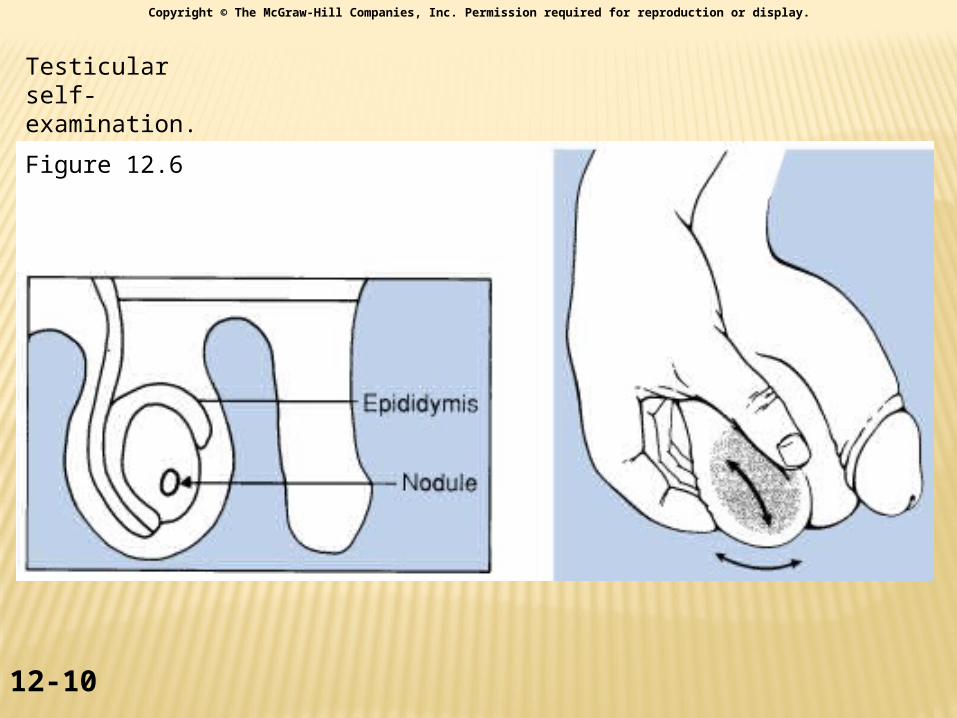
Testicular self- examination.
Figure 12.6
http://www.webmd.com/cancer/pancreatic-cancer/slideshow-pancreatic-cancer-overview