Embed Size (px)
Citation preview
Precancerous
Lesions & Conditions
Contents
• Introduction
• Classification of precancerous lesions & conditions
• Leukoplakia
• Erythroplakia
• Carcinoma in Situ
• Oral lichen planus
• Oral submucous fibrosis
Introduction
• Precancerous lesion
• “Morphologically altered tissue in which cancer is more
likely to occur, than in its apparently normal
counterpart”
• Precancerous condition
• “Generalized state of the body, which is associated with a
significantly increased risk of cancer”
PREMALIGNANT LESIONS
• Leukoplakia
• Erythroplakia
• Carcinoma in situ
• Bowens disease
• Actinic keratosis & chelitis
• Dyskeratosis follicularis
PREMALIGNANT CONDITIONS
• Oral submucous fibrosis
• Oral lichen planus
• Syphilitic glossitis
• Sideropenic dysphagia
• Dyskeratosis congenita
Leukoplakia
• The term LEUKOPLAKIA was first coined by a Hungarian
Dermatologist SCHWIMMER in 1877
• Originates from Greek words – “leucos” - white and “plakia” -
patch
• WHO 1978
• “A white patch or plaque in the oral cavity which cannot be
scrapped off or stripped off easily & more over, which cannot be
characterized clinically or pathologically as any other disease”
Epidemiology
1. Prevalence
• Represents 85% of all oral precancers
2. Incidence
3 – 4 % of adult population
3. Age
Usually in the 4th – 6th decades of life
4. Sex
Males have the highest incidence, with the trend changing gradually
Classification of leukoplakia(Axell & Pindborg et al 1983)
• Based on CLINICAL TYPE:
Homogenous
Non homogenous
• Based on ETIOLOGY:
Tobacco associated
Idiopathic
• Based on EXTENT:
Localized
Diffuse
• Based on risk of MALIGNANT TRANSFORMATION
High risk sites
Floor of mouth
Lateral/ventral surface of tongue
Soft palate
Low risk sites
Dorsum of tongue
Hard palate
• Based on HISTOLOGY:
Dysplastic
Non dysplastic
Sharp’s staging of leukoplakia
• Stage I- Earliest lesion-non palpable, faintly translucent,
white discoloration
• Stage II- Localized or diffuse, slightly elevated plaque of
irregular outline. It is opaque white & may have a fine
granular texture
• Stage III- Thickened white lesion showing induration and
fissuring
Etiopathogenesis
• Tobacco – most imp offending agent
• Alcohol
• Chronic irritation
• Syphilis
• Nutritional deficiency
• Actinic radiation
• Galvanism
• Most studies have reported mortality ratios for smokers
versus never smokers of about 5:1, with several reporting
ratios in excess of 10:1. Furthermore, the risk for death
from oral cancer is consumption related
• Male cigarette smokers had a relative risk for oral cancer
27.7 times greater than that of a male never smoker
• These studies have found that after 3 to 5 years of smoking
abstinence, oral cancer risk decreased by about 50%
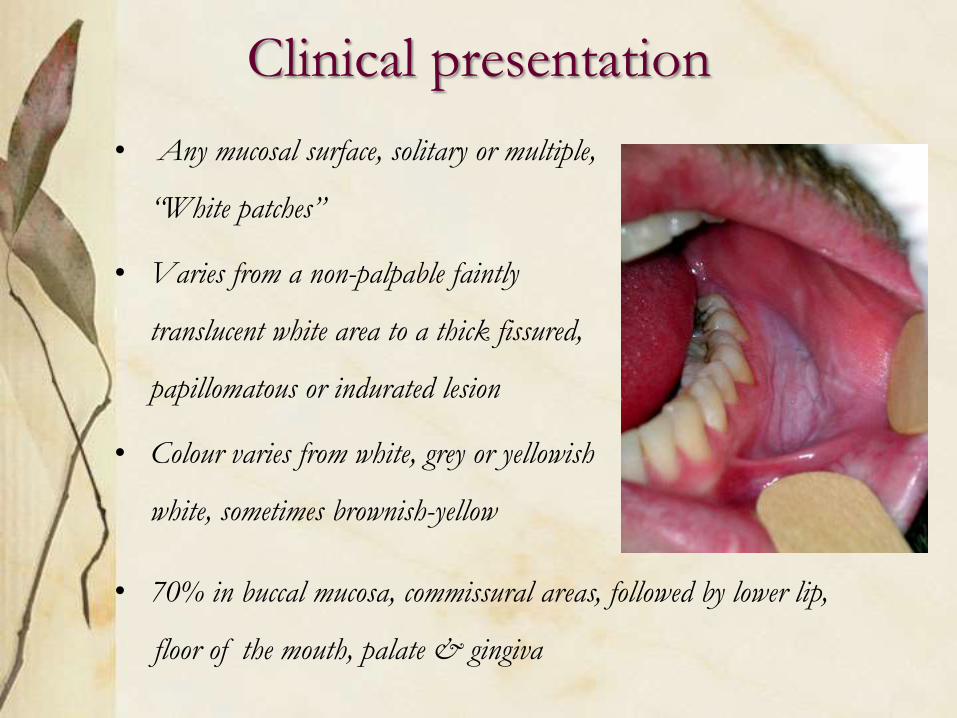
Clinical presentation
• Any mucosal surface, solitary or multiple,
“White patches”
• Varies from a non-palpable faintly
translucent white area to a thick fissured,
papillomatous or indurated lesion
• Colour varies from white, grey or yellowish
white, sometimes brownish-yellow
• 70% in buccal mucosa, commissural areas, followed by lower lip,
floor of the mouth, palate & gingiva
SYMPTOMS
• Patients may report with a feeling of increased thickness of
mucosa
• Those with ulcerated or nodular type may complain of
burning sensation
• Enlarged cervical lymph nodes may signal occurrence of
metastasis
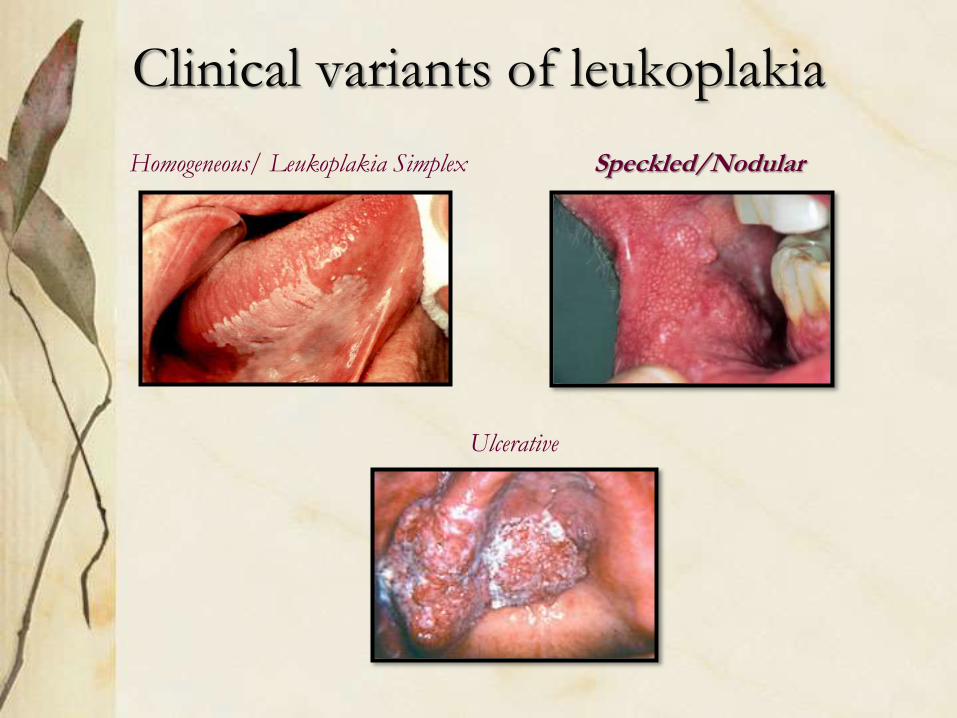
Clinical variants of leukoplakia
Homogeneous/ Leukoplakia Simplex Speckled/Nodular
Ulcerative
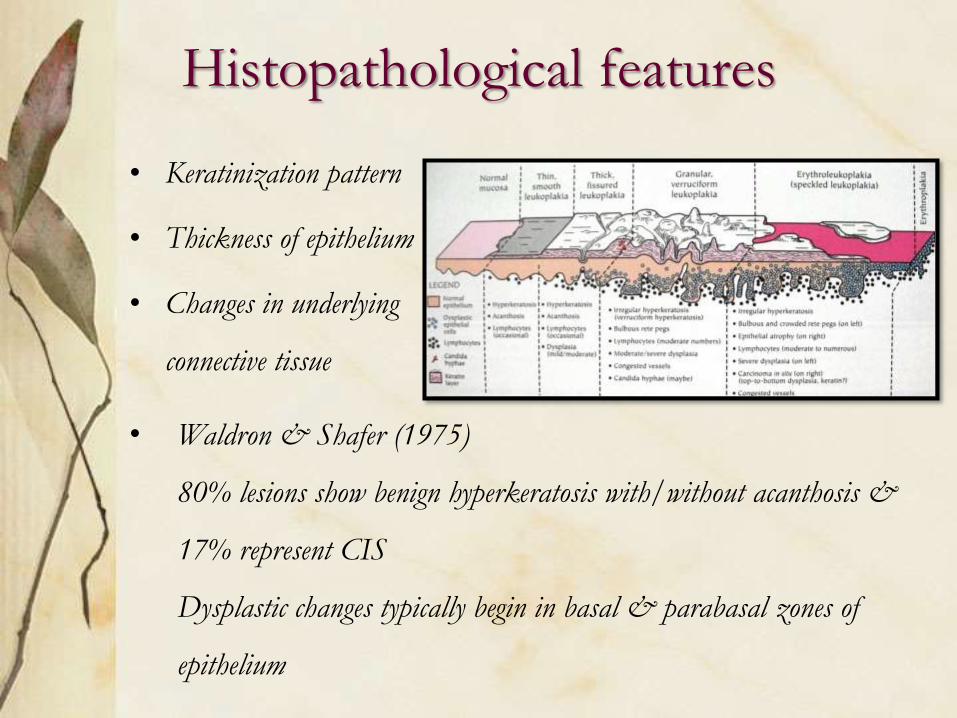
Histopathological features
• Keratinization pattern
• Thickness of epithelium
• Changes in underlying
connective tissue
• Waldron & Shafer (1975)
80% lesions show benign hyperkeratosis with/without acanthosis &
17% represent CIS
Dysplastic changes typically begin in basal & parabasal zones of
epithelium
• Five clinical criteria for high risk of malignant change
– The nodular type
– Erosion or ulceration within lesion
– Presence of a nodule indicates malignant potential
– A lesion that is hard in its periphery
– Lesion of anterior floor of mouth & undersurface of tongue
• In all cases, relative risk of malignant potential is determined
by presence of epithelial dysplasia upon histological
examination
Diferential diagnosis
• Leukoedema
• Lichen planus
• Chemical burn
• Morsicatio buccarum
• Lupus erythematosus
• White sponge nevus
Conservative management
• Elimination of etiological factor
• Restraining from smoking or chewing tobacco
• To remove sharp broken down teeth
• Correction & replacement of overhanging or faulty metal
restorations with a metal bridge
CHEMOPREVENTION
1) Isotrenitoin / 13- cis- retinoic acid –
2) Beta carotene -30mg TID
3) Topical Bleomycin – 0.5-1% solution/2wks
4) 5-Fluorouracil & Cisplatin
• Surgical Excision: entire lesion excised if it is >1cm in size,
following modalities used:
a) Scalpel – surgical stripping
b) Cryosurgery – with liquid nitrogen
c) Electrocautery
d) Laser ablation
Erythroplakia
WHO DEFINITION:
“Any lesion of the oral mucosa that presents as a
bright red velvety patch or plaque, which cannot be
characterized clinically or pathologically as any other
recognizable condition”
Reported by Querat in 1911
CLASSIFICATION
• Clinical variants
1. Homogenous erythroplakia
2. Erythroplakia interspersed with patches of leukoplakia
3. Granular or Speckled erythroplakia
• Etiology : Same as oral leukoplakia
• Age : Mainly middle age, peak 65-74 years
• Gender : Predilection for men
• Location/size
- Soft palate, floor of the mouth & buccal mucosa & tongue
- Typical lesion < 1.5 cm in diameter but >4cm also
observed
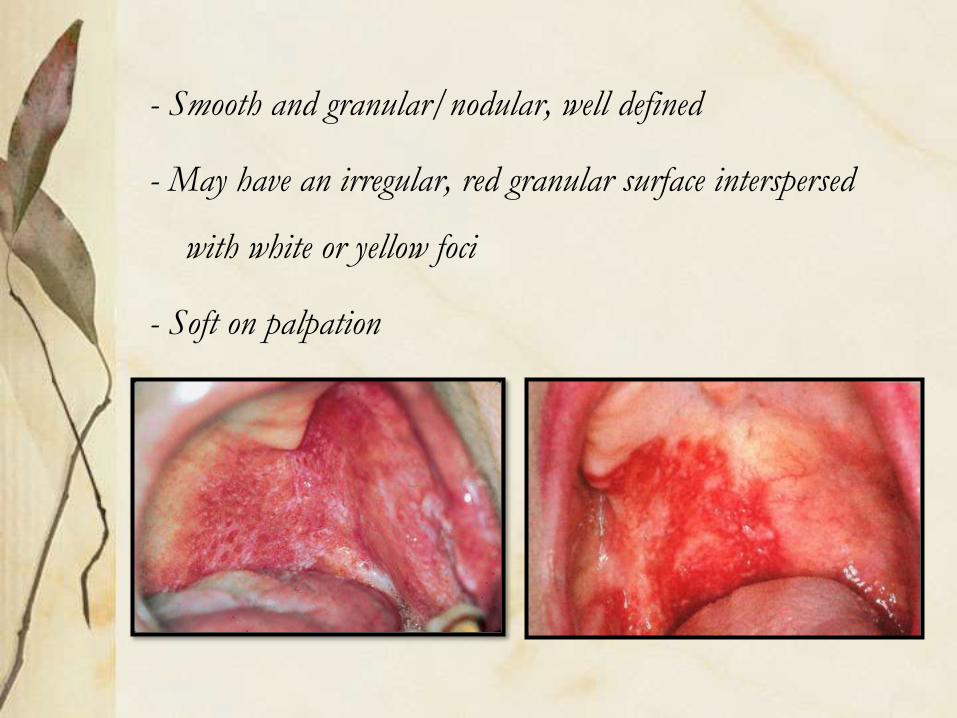
- Smooth and granular/nodular, well defined
- May have an irregular, red granular surface interspersed
with white or yellow foci
- Soft on palpation
• Highest risk for malignant transformation - 14-50%
• Based on the fact that on histology 80-90% of cases
present as-
- Carcinoma In Situ
- Severe epithelial dysplasia
- Microinvasive carcinoma
Management
• Biopsy should be performed
• Treatment guided by histopathologic diagnosis
• Recurrence , multifocality common
• Careful long term follow up
Intraepthelial carcinoma (Ca in Situ)
• Arises frequently on the skin, but also on mucous membranes,
including oral cavity
• Most severe stage of epithelial dysplasia
• Striking feature – dysplastic epithelial cells donot invade into
connective tissue
• Common among elderly, with a male prdiliction
• Present as white plaques or ulcerated, & reddened areas
• Site – floor of the mouth, tongue, lips
• Has combined features of leuko & erythroplakia
• Histopathology
• Keratin may or may not be present on the surface, but if present it
is usually parakeratin
• Individual cell keratinization or keratin pearl formation are rare
• Consistent finding – loss of orientation & normal polarity of cells
• Treatment
• No accepted treatment
• Surgical excision, irradiation & cauterization
Precancerous conditions
Oral lichen planus
• Named by E Wilson ( British physician) 1896
Lichen – latin for primitive plants (symbiotic algae & fungi)
Planus – latin for flat
• Definition
• “A common chronic immunologic inflammatory mucocutaneous
disorder that varies in appearance from keratotic (reticular or plaque
like) to erythematous and ulcerative, affecting the stratified squamous
epithelium”
• Affects 0.5% to 1% of world's population
• Approx half patients with cutaneous LP have oral
involvement
• Mucosal involvement, sole manifestation in up to 25%
cases
• Peak incidence - middle age, F:M- 2:1
• Characteristically associated with persistent clinical
course & resistance to most conventional treatments
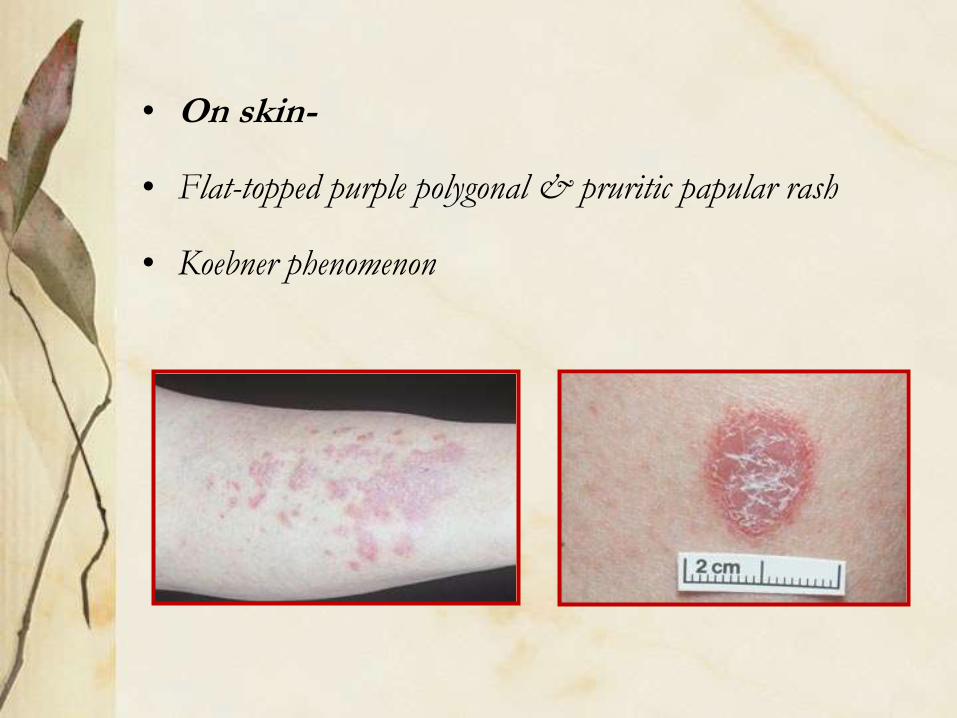
• On skin-
• Flat-topped purple polygonal & pruritic papular rash
• Koebner phenomenon
Etiology & pathogenesis
• Both antigen-specific & non-specific mechanisms may be involved
in pathogenesis of OLP
• Antigen-specific mechanisms:
– antigen presentation by basal keratinocytes and
– antigen-specific keratinocyte killing by CD8+ cytotoxic T-cells
• Non-specific mechanisms:
– mast cell degranulation and
– matrix metalloproteinase (MMP) activation
• These mechanisms may combine to cause
T-cell accumulation in superficial lamina propria
Basement membrane disruption
Intra-epithelial T-cell migration &
Keratinocyte apoptosis
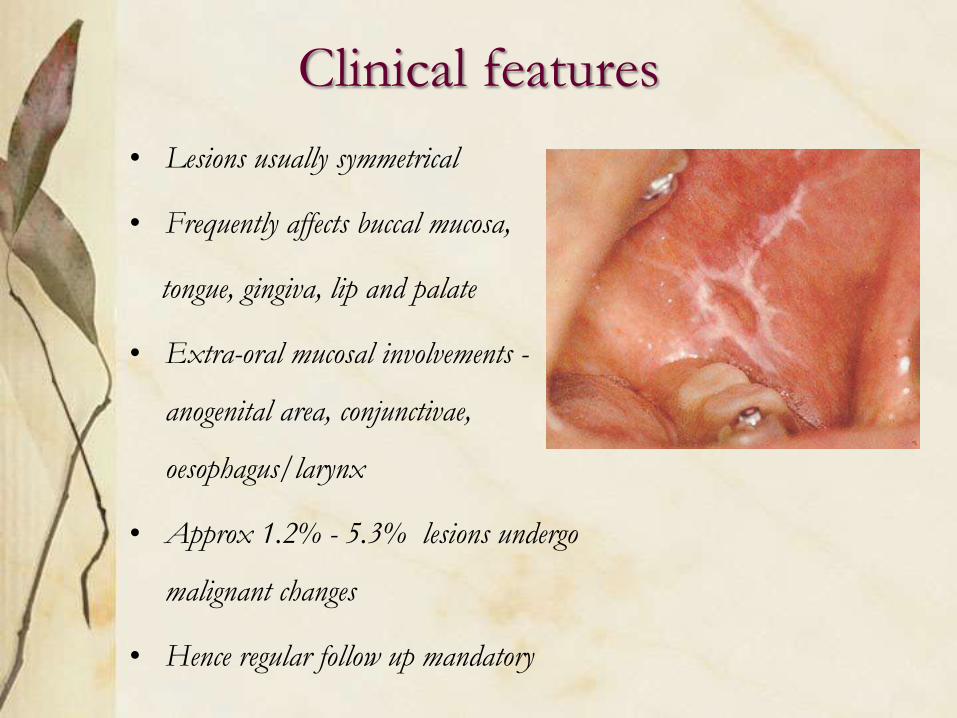
Clinical features
• Lesions usually symmetrical
• Frequently affects buccal mucosa,
tongue, gingiva, lip and palate
• Extra-oral mucosal involvements -
anogenital area, conjunctivae,
oesophagus/larynx
• Approx 1.2% - 5.3% lesions undergo
malignant changes
• Hence regular follow up mandatory
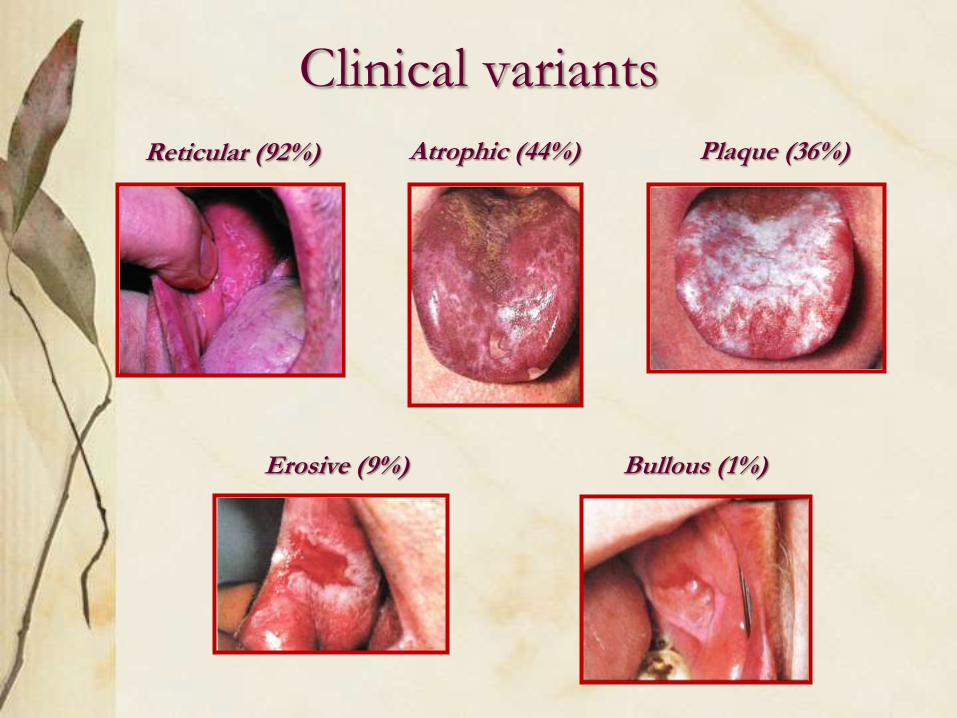
Clinical variants
Reticular (92%) Atrophic (44%) Plaque (36%)
Erosive (9%) Bullous (1%)
Clinical features
Asymptomatic
• Reticular – Wickham’s striae + discrete erythematous border
• Plaque-like – Resemble leukoplakia, common in smokers
Symptomatic
• Atrophic – Diffuse red patch, peripheral radiating white striae
• Erosive – Irregular erosion covered with a pseudomembrane
• Bullous – Small bullae / vesicles that may rupture easily
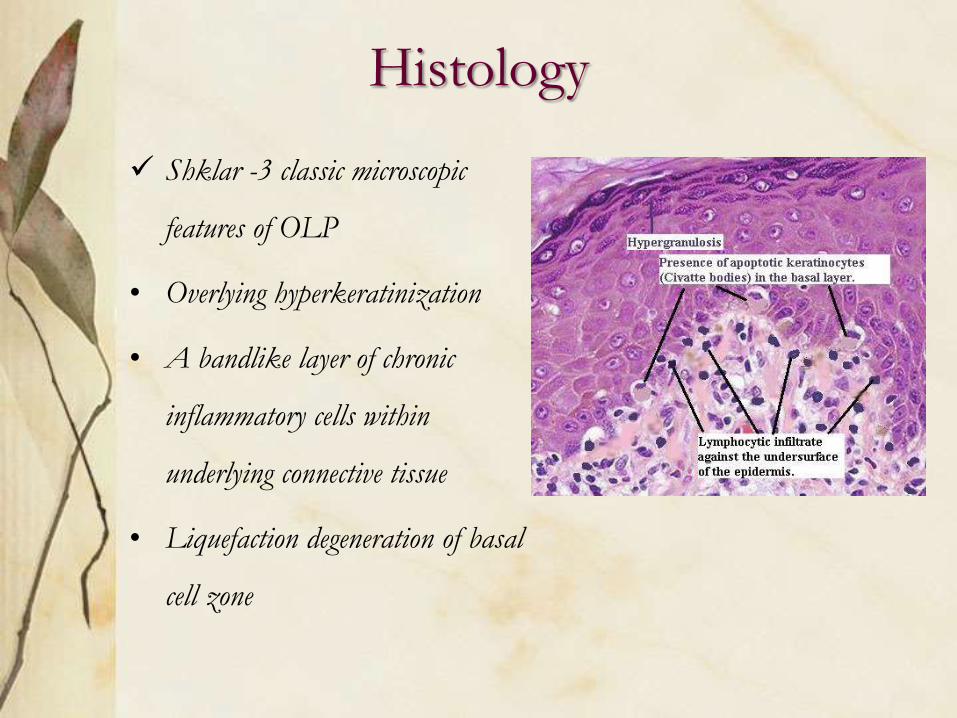
Histology
Shklar -3 classic microscopic
features of OLP
• Overlying hyperkeratinization
• A bandlike layer of chronic
inflammatory cells within
underlying connective tissue
• Liquefaction degeneration of basal
cell zone
Diagnosis
• The characteristic clinical aspects of OLP - sufficient for
correct diagnosis
• An oral biopsy - to confirm clinical diagnosis
(exclude dysplasia & malignancy)
• Gingival LP more difficult to diagnose, direct
immunofluorescence of perilesional mucosa for diagnosis
IMMUNOFLUORESCENCE
• Direct immunofluorescence – shaggy band of fibrinogen
in the basement membrane, IgM stained cytoid bodies
are also seen in dermal papilla or peribasilar area
Management
• Reticular type is asymptomatic & treatment often
unnecessary
• Erosive type presents significant management problems
• All patients should optimize oral hygiene
• Oral candidiasis should be excluded/treated
• Cortico steroids, is the treatment of choice eg – Fluocinonide
or Clobetasol gel for 2 weeks, with 3mnths follow-up
• In symptomatic patients with apparent contact dental
factor, patch test with replacement of amalgam
• In those with no apparent contact factor, topical or
intralesional steroid - first line treatment. A short course
of systemic steroid for more rapid control
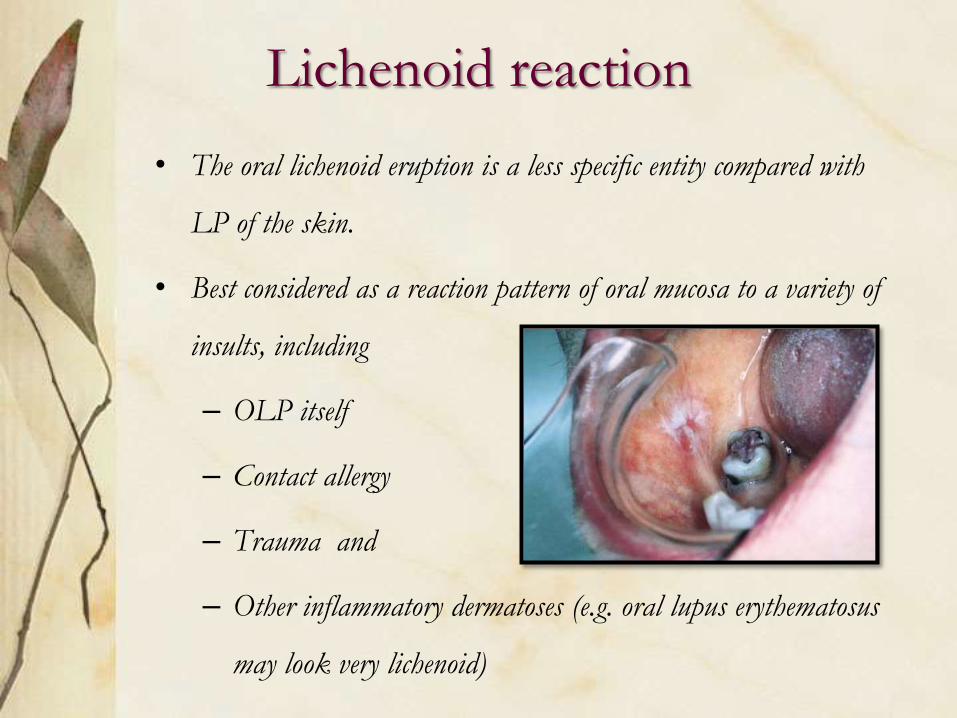
Lichenoid reaction
• The oral lichenoid eruption is a less specific entity compared with
LP of the skin.
• Best considered as a reaction pattern of oral mucosa to a variety of
insults, including
– OLP itself
– Contact allergy
– Trauma and
– Other inflammatory dermatoses (e.g. oral lupus erythematosus
may look very lichenoid)
Oral submucous fibrosis
DEFINITION -
“It is a slowly progressing chronic fibrotic disease of the
oral cavity & oropharynx, characterized by fibroelastic
change and inflammation leading to a progressive
inability to open the mouth, swallow or speak”
Clinical featuresAge
• Range wide & regional; even prevalent among teenagers in India
Ranges from 11-60 years
Sex
• From 0.2 - 2.3% in males to 1.2 - 4.5% in females in Indian
communities
Race
• South-East Asian countries, in Indian immigrants to other
countries
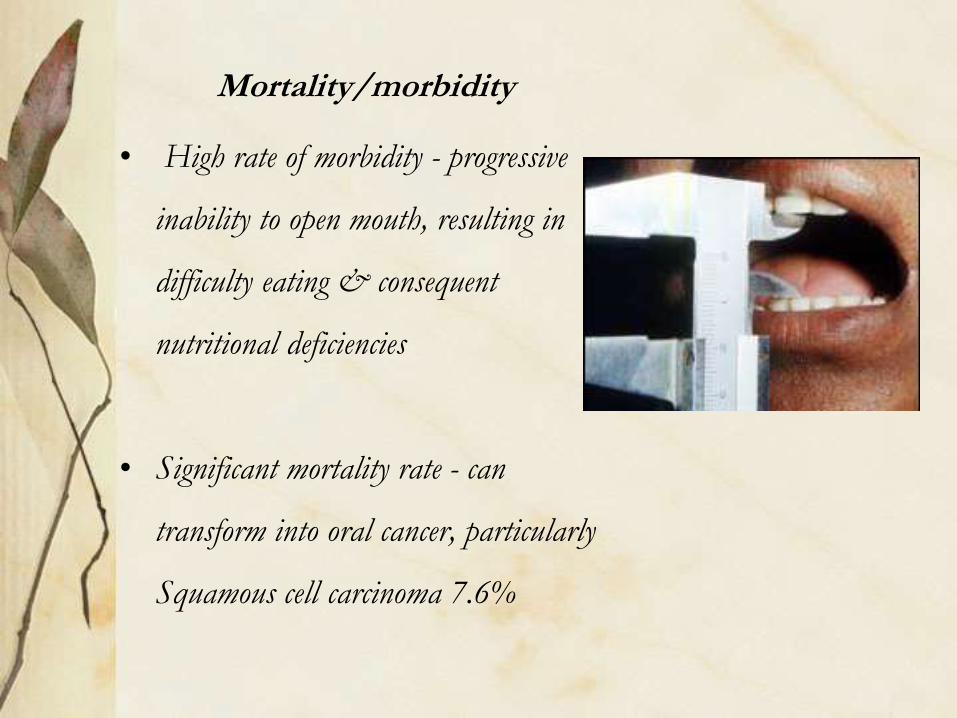
Mortality/morbidity
• High rate of morbidity - progressive
inability to open mouth, resulting in
difficulty eating & consequent
nutritional deficiencies
• Significant mortality rate - can
transform into oral cancer, particularly
Squamous cell carcinoma 7.6%
Etiology
• Initially classified as idiopathic, now
• Betel quid & it’s components (Arecoline, an active
alkaloid found in betel nuts, stimulates fibroblasts to
increase production of collagen by 150%)
• Capsaicin – Chillies (hypersensitivity reaction)
• Nutritional factors
• Immunological factors
Clinical presentation
• Common site – buccal mucosa, retromolar area, uvula,
palate, etc
• Initially, pain and a burning sensation upon
consumption of hot & spicy foods
• Vesicle & ulcers
• Excessive or reduced salivation & defective gustation
• Hearing loss
• Depapillation & atrophy of tongue and uvula
• Depigmented & loss of stippling over gingiva
• Nasal tone in the voice
• Difficulty in deglutition
• Impaired mouth movements (eg, eating, whistling,
blowing, sucking)
Clinical stages
Three stages (Pindborg, 1989) based on physical findings:
• Stage 1: Stomatitis includes erythematous mucosa, vesicles,
mucosal ulcers, melanotic mucosal pigmentation & mucosal
petechiae
• Stage 2: Fibrosis occurs in ruptured vesicles & ulcers when
they heal, hallmark of this stage
• Stage 3: Sequelae of OSF
– Leukoplakia is found in more than 25% of
individuals with OSF
– Speech and hearing deficits may occur because of
involvement of the tongue and the eustachian tubes
RANGANATHAN K (2001)
• Group I : Only Symptoms, No mouth opening
• Group II : Mouth opening > 20mm
• Group III : Mouth opening < 20mm
• Group IV: Limited mouth opening, precancerous
& cancerous changes throughout mucosa
Histopathology
• Hyperkeratinized, atrophic epithelium with flattening
& shortening of rete pegs
• Nuclear pleomorphism & severe inter-cellular edema
• Finely fibrilar collagen & increased fibroblastic activity
in early stage showing dilated & congested blood vessels
with areas of hemorrhage
• Advanced stage shows “homogenization” and
“hyalinization” of collagen fibers (important feature)
• Degeneration of muscle fibers and chronic inflammatory
cell infiltration in the connective tissue
Management1. Behavioral therapy
- Patient counseling, stoppage of habit
2. Medicinal therapy
-Hyaluronidase: Topically, shown to improve symptoms more
quickly than steroids alone
- Mild cases – intralesional inj Dexamethasone 4 mg to reduce
symptoms & surgical splitting / excision of fibrous bands
- Recent study – intralesional inj of gamma interferon 3 times a
week, improves mouth opening significantly
References
1. Burket’s oral medicine diagnosis & treatment – 10th edition
2. Textbook of oral pathology –shafer 5th edition
3. Neville’s Oral and Maxillofacial Pathology - 2nd edition
4. Emedicine – Diseases of oral mucosa, Oral submucous fibrosis,
Jan 26, 2007
5. Oral leukoplakia related to malignant transformation, Oral
Science International 2006;45-55
Thank You












![Short Communication Low Cost Technology for Screening ......lesions of the oral cavity.[2,3] In India, a vast majority of oral cancers are preceded by precancerous lesions and conditions](https://img.pdfslide.us/doc/110x75/5ff933da099ce719ef02b8ab/short-communication-low-cost-technology-for-screening-lesions-of-the-oral.jpg)