Embed Size (px)
Citation preview

Somatic Symptom Disorder and Illness Anxiety Disorder
Somatic Symptom Disorders Work Group Table of Contents for Summit Review
9-24-2012
1. Proposed DSM-5 Criteria and DSM-IV Criteria - SSD – Current proposed DSM-5 criteria for Somatic Symptom Disorder revised by APA staff and Dr. Michael First
2. Proposed DSM-5 Criteria and DSM-IV Criteria - IAD – Current proposed DSM-5 criteria for
Illness Anxiety Disorder as revised by APA staff and Dr. Michael First
3. SRC Review Summary – SRC score and summary of review
4. CPHC Review Summary – CPHC score and summary of review
5. CPHC Proposal Cover Letter from WG – Cover note provided by WG for CPHC review
6. SRC Cover Letter – Cover note provided by WG for SRC Review
7. SRC Proposal from WG– Proposal submitted by the WG for SRC review
8. Appendix 1: Creed – Key article
9. Appendix 2: Field Trial Results– Key article
DRAFT - CONFID
ENTIAL

Somatic Symptom Disorder Somatic Symptom and Related Disorders
7
Proposed Criteria for DSM-5 DSM-IV Criteria
Somatic Symptom Disorder
A. One or more somatic symptoms that are distressing or result in significant disruption of daily life.
B. Excessive thoughts, feelings, or behaviors related to the somatic symptoms or associated health concerns as manifested by at least one of the following: .
1. Disproportionate and persistent thoughts about the seriousness of one’s symptoms
2. Persistently high level of anxiety about health or symptoms
3. Excessive time and energy devoted to these symptoms or health concerns
C. Although any one somatic symptom may not be continuously present, the state of being symptomatic is persistent (typically more than 6 months).
Specify if:
With predominant pain (previously pain disorder): This specifier is for individuals whose somatic symptoms predominantly involve pain.
Specify severity: Mild: Only one of the B Criteria are fulfilled Moderate: Two or more B Criteria are fulfilled Severe: Two or more B Criteria are fulfilled plus multiple somatic complaints (or one very severe somatic symptom)
This disorder is not listed in DSM-IV; therefore DSM-IV criteria for this disorder do not exist. It is proposed that somatoform disorders be restructured. CSSD will subsume what previously was described as Somatization Disorder, as well as some presentations of Undifferentiated Somatoform Disorder, Somatoform Disorder NOS, and Pain Disorder. CSSD also includes the vast majority of patients previously diagnosed with Hypochondriasis; the rationale for the split in Hypochondriasis can be found in the report on Illness Anxiety Disorder.
Somatization Disorder
A. A history of many physical complaints beginning before age 30 years that occur over a period of several years and result in treatment being sought or significant impairment in social, occupational, or other important areas of functioning.
B. Each of the following criteria must have been met, with individual symptoms occurring at any time during the course of the disturbance:
(1) four pain symptoms: a history of pain related to at least four different sites or functions (e.g., head, abdomen, back, joints, extremities, chest, rectum, during menstruation, during sexual intercourse, or during urination)
(2) two gastrointestinal symptoms: a history of at least two gastrointestinal symptoms other than pain (e.g., nausea, bloating, vomiting other than during pregnancy, diarrhea, or intolerance of several different foods)
(3) one sexual symptom: a history of at least one sexual or reproductive symptom other than pain (e.g., sexual indifference, erectile or ejaculatory dysfunction, irregular menses, excessive menstrual bleeding, vomiting throughout
DRAFT - CONFID
ENTIAL

Somatic Symptom Disorder Somatic Symptom and Related Disorders
8
pregnancy)
(4) one pseudoneurological symptom: a history of at least one symptom or deficit suggesting a neurological condition not limited to pain (conversion symptoms such as impaired coordination or balance, paralysis or localized weakness, difficulty swallowing or lump in throat, aphonia, urinary retention, hallucinations, loss of touch or pain sensation, double vision, blindness, deafness, seizures; dissociative symptoms such as amnesia; or loss of consciousness other than fainting)
C. Either (1) or (2):
(1) after appropriate investigation, each of the symptoms in Criterion B cannot be fully explained by a known general medical condition or the direct effects of a substance (e.g., a drug of abuse, a medication)
(2) when there is a related general medical condition, the physical complaints or resulting social or occupational impairment are in excess of what would be expected from the history, physical examination, or laboratory findings
D. The symptoms are not intentionally produced or feigned (as in Factitious Disorder or Malingering). Undifferentiated Somatoform Disorder
A. One or more physical complaints (e.g., fatigue, loss of appetite, gastrointestinal or urinary complaints).
B. Either (1) or (2):
(1) after appropriate investigation, the symptoms cannot be fully explained by a known general medical condition or the direct effects of a substance (e.g., a drug of abuse, a medication)
DRAFT - CONFID
ENTIAL

Somatic Symptom Disorder Somatic Symptom and Related Disorders
9
(2) when there is a related general medical condition, the physical complaints or resulting social or occupational impairment is in excess of what would be expected from the history, physical examination, or laboratory findings
C. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
D. The duration of the disturbance is at least 6 months.
E. The disturbance is not better accounted for by another mental disorder (e.g., another Somatoform Disorder, Sexual Dysfunction, Mood Disorder, Anxiety Disorder, Sleep Disorder, or Psychotic Disorder).
F. The symptom is not intentionally produced or feigned (as in Factitious Disorder or Malingering). Somatoform Disorder Not Otherwise Specified This category includes disorders with somatoform symptoms that do not meet the criteria for any specific Somatoform Disorder.
Examples include
1. Pseudocyesis: a false belief of being pregnant that is associated with objective signs of pregnancy, which may include abdominal enlargement (although the umbilicus does not become everted), reduced menstrual flow, amenorrhea, subjective sensation of fetal movement, nausea, breast engorgement and secretions, and labor pains at the expected date of delivery. Endocrine changes may be present, but the syndrome cannot be explained by a general medical condition that causes endocrine changes (e.g., a hormone-secreting tumor)
2. A disorder involving nonpsychotic hypochondriacal
DRAFT - CONFID
ENTIAL

Somatic Symptom Disorder Somatic Symptom and Related Disorders
10
symptoms of less than 6 months’ duration
3. A disorder involving unexplained physical complaints (e.g., fatigue or body weakness) of less than 6 months’ duration that are not due to another mental disorder Pain Disorder
A. Pain in one or more anatomical sites is the predominant focus of the clinical presentation and is of sufficient severity to warrant clinical attention.
B. The pain causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
C. Psychological factors are judged to have an important role in the onset, severity, exacerbation, or maintenance of the pain.
D. The symptom or deficit is not intentionally produced or feigned (as in Factitious Disorder or Malingering).
E. The pain is not better accounted for by a Mood, Anxiety, or Psychotic Disorder and does not meet criteria for Dyspareunia.
Code as follows:
307.80 Pain Disorder Associated With Psychological Factors: psychological factors are judged to have the major role in the onset, severity, exacerbation, or maintenance of the pain. (If a general medical condition is present, it does not have a major role in the onset, severity, exacerbation, or maintenance of the pain.) This type of Pain Disorder is not diagnosed if criteria are also met for Somatization Disorder.
Specify if:
DRAFT - CONFID
ENTIAL

Somatic Symptom Disorder Somatic Symptom and Related Disorders
11
Acute: duration of less than 6 months
Chronic: duration of 6 months or longer
307.89 Pain Disorder Associated With Both Psychological Factors and a General Medical Condition: both psychological factors and a general medical condition are judged to have important roles in the onset, severity, exacerbation, or maintenance of the pain. The associated general medical condition or anatomical site of the pain (see below) is coded on Axis III.
Specify if:
Acute: duration of less than 6 months
Chronic: duration of 6 months or longer
Note: The following is not considered to be a mental disorder and is included here to facilitate differential diagnosis.
Pain Disorder Associated With a General Medical Condition: a general medical condition has a major role in the onset, severity, exacerbation, or maintenance of the pain. (If psychological factors are present, they are not judged to have a major role in the onset, severity, exacerbation, or maintenance of the pain.) The diagnostic code for the pain is selected based on the associated general medical condition if one has been established (see Appendix G) or on the anatomical location of the pain if the underlying general medical condition is not yet clearly established— for example, low back (724.2), sciatic (724.3), pelvic (625.9), headache (784.0), facial (784.0), chest (786.50), joint (719.40), bone (733.90), abdominal (789.0), breast (611.71), renal (788.0), ear (388.70), eye (379.91), throat (784.1), tooth (525.9), and urinary (788.0).
DRAFT - CONFID
ENTIAL

Somatic Symptom Disorder Somatic Symptom and Related Disorders
12
DRAFT - CONFID
ENTIAL

Illness Anxiety Disorder Somatic Symptom and Related Disorders
15
Proposed Criteria for DSM-5 DSM-IV Criteria Illness Anxiety Disorder
A. Preoccupation with having or acquiring a serious illness. B. Somatic symptoms are not present or, if present, are only mild in intensity. If another medical condition is present or there is a high risk for developing a medical condition (e.g., strong family history) is present, the preoccupation is clearly excessive or disproportionate. C. There is a high level of anxiety about health and the individual is easily alarmed about personal health status. D. The individual performs excessive health-related behaviors (e.g., repeatedly checking one's body for signs of illness) or exhibits maladaptive avoidance (e.g., avoiding doctors' appointments and hospitals). E. Illness preoccupation has been present for at least 6 months, but the specific illness that is feared may change over that period of time. F. The illness-related preoccupation is not better explained by another mental disorder, such as somatic symptom disorder, panic disorder, generalized anxiety disorder, body dysmorphic disorder, or obsessive-compulsive disorder. Specify whether: Care-seeking: medical care, including physician visits or undergoing tests and procedures, is frequently used. Care-avoidant: medical care is rarely used.
Because of the considerations discussed, Hypochondriasis is now recognized as 2 disorders. Approximately 80% of patients previously diagnosed with Hypochondriasis would now be included within the CSSD diagnosis. The remaining patients would be diagnosed with Illness Anxiety Disorder.
Hypochondriasis
A. Preoccupation with fears of having, or the idea that one has, a serious disease based on the person's misinterpretation of bodily symptoms.
B. The preoccupation persists despite appropriate medical evaluation and reassurance.
C. The belief in Criterion A is not of delusional intensity (as in Delusional Disorder, Somatic Type) and is not restricted to a circumscribed concern about appearance (as in Body Dysmorphic Disorder).
D. The preoccupation causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
E. The duration of the disturbance is at least 6 months.
F. The preoccupation is not better accounted for by Generalized Anxiety Disorder, Obsessive-Compulsive Disorder, Panic Disorder, a Major Depressive Episode, Separation Anxiety, or another Somatoform Disorder.
Specify if:
With Poor Insight: if, for most of the time during the current episode, the person does not recognize that the concern about having a serious illness is excessive or unreasonable
DRAFT - CONFID
ENTIAL

43
SRC Review Summary
Review Date: March 9, 2012
Score: 2.85 (modest support)
Scoring Summary: 1=strong support 2=moderate support (acceptable) 3=modest support (questionable) 4= limited support (probably not justified) 5= poor support (do not include) 6= insufficient data
36-38R=Somatic Disorders: This revised proposal received overall modest support with a diversity of opinions. Two members voted a “2” for approval. One member voted a “4” clearly against approval. Four members voted a “3” for modest and potentially questionable support. Favorable features that were noted were that the criteria were substantially simplified and the reliability data from the field trials was impressive. The greatest concern was the absence of good validating data, especially given the major conceptual shift that this proposal represented. The SRC felt that in light of the wide range of opinions about this proposal on the SRC, a consultation with the CPH committee would be indicted. Our “referral note” follows:
While the kappa from the field trials is of value, there is not an overall set of validator criteria and more importantly an important question on whether medically unexplained vs. medically explained criteria do actually describe different groups. Since this is a major reconceptualization of a disorder with the potential risk of pathologizing patients with multiple well defined medical illnesses and high levels of worry about them, we think a review by the CPH committee might be warranted.
Additional Comment 1:
The workgroup has done an admirable job in simplifying the existing DSMIV criteria, as well in this revision. Critical new evidence is high reliability in the field trials and validation through the Creed epidemiological study that the criteria do not result in over diagnosis. Finally, the reexamination of the Kisley study does show that medical explanations for symptoms do not reduce the intensity of symptoms from CSSD.
Additional Comment 2:
This is a complex and multipart proposal seeking to delete existing diagnostic categories of long standing but about which the workgroup has raised substantive issues regarding utility, capture
DRAFT - CONFID
ENTIAL

44
of affected populations in primary care as opposed to specialty populations, and stability of diagnosis over time.
There workgroup provides a wealth of data relevant to many validators and other considerations in relation to both the deletion and the rationale for the new diagnostic categories. With some caveats (see below) they do a better job of denoting the difficulties with the current schema especially as it affects recognition within the general medical sector. However as they note there have been no studies of the cssd-sssd-iad contruct and as such there are no validators specific to these.
Several general points:
The comorbidity with anxiety and depression is as high as the comorbidity between somatization and hypochondriasis. There is some data to suggest that response to treatment of somatiziing conditions does not covary with treatment of depression.
Concerns about the criteria for medically unexplained symptoms are well described, however in one of the papers provided by the workgroup (Kisely, Goldberg and Simon, Psychological Medicine 1997) a multi center international study found significant differences in the pattern and cut point of psychiatric co morbidity between 3 groups – those with medically explained symptoms, those with medically unexplained symptoms and those in a combined group. The latter two groups were “Patients who had five or more non-medically explained symptoms were significantly younger, had greater psychiatric morbidity, were at greater risk of harmful use of alcohol and reported greater social disability than those with a medical explanation for their somatic symptoms. Patients who had an excess of somatic symptoms in both categories had especially high rates of social and psychiatric morbidity” While the kappa from the field trials is of value, there is not an overall set of validator criteria and more importantly an important question on whether medically unexplained vs medically explained criteria do actually describe different groups. Since this is a major reconceptualization of a disorder with the potential risk of pathologizing patients with multiple well defined medical illnesses and high levels of worry about them, I do think a review by the CPH committee might be warranted
DRAFT - CONFID
ENTIAL

CPHC Memo: Somatic Symptom Disorder and Illness Anxiety Disorder
From: Drs. McIntyre and Yager on behalf of the DSM-5 Clinical and Public Health
Committee (CPHC)
To: Dilip Jeste, M.D. President APA
DATE: September 13, 2012
Enclosed please find the CPHC report on Somatic Symptom Disorder and Illness Anxiety Disorder, reviewed at our meeting on September 11, 2012.
The SRC scored this proposal scored 2.85. The five CPHC reviewers’ average score was 2.2.
CPHC decided to split our scoring into the two parts: SSD and IAD.
Based on our external reviews and discussions in the CPHC,
We rate SSD as: 2.5 (Good to Fair) and IAD as 1.86 (Good to Excellent)
1 = Excellent
2 = Good
3 = Fair
4 = Poor
We offer the following additional comments:
Our reviewers and our Committee unanimously agreed that the DSM IV diagnoses are significantly flawed. Although there is not substantial evidence supporting the new proposal it does appear to be a significant improvement. The high kappa of >.6 in the field trials suggests that there is good reliability for the proposed diagnosis.
DRAFT - CONFID
ENTIAL

** 5/31/2012 This document was included in the Work Group’s initial submission to the SRC. Please note that CSSD and SSSD have since been consolidated. We are providing this because of the succinct summary of problems with the status quo.
4
TO: Scientific Review Committee
FROM: Somatic Symptom Disorder Workgroup
DATE: October 7, 2011
RE:
• Complex Somatic Symptom Disorder (CSSD) • Simple Somatic Symptom Disorder (SSSD) • Illness Anxiety Disorder (IAD)
Attached please find pdfs of key references as well as 4 WORD documents. Three of the WORD documents correspond to the above disorders, and the 4th provides a side by side comparison of criteria for these disorders vs existing DSM IV TR criteria. The workgroup recognizes that analyzing these 3 disorders together represents a formidable challenge but felt that considering them as one package would actually facilitate review.
This cover memo provides an “executive summary” of the rationale for the 3 proposals. The accompanying documents follow, as closely as they can, the guidelines suggested by the SRC for new disorders. As will be evident, there are substantial limitations to the current research literature, which make it difficult to respond point-by-point to the enumerated validation topic areas. Secondly, the changes proposed are admittedly so radical that empirical data are still limited. Nonetheless, there are considerable data in support of these propositions. Accordingly, we are providing key pdf’s for each disorder that provide key data.
Problems with the status quo1:
1. The DSM IV clinical domain covered by these proposed diagnoses includes 6 existing disorders: Somatization Disorder, Undifferentiated Somatoform Disorder, Hypochondriasis, Pain Disorder Associated with Psychological Factors, Pain Disorder Associated with both Psychological Factors and a General Medical Condition, and Somatoform Disorder NOS. In fact, there is so much overlap amongst these disorders, that they can be collapsed into a simpler arrangement of the 3 proposed disorders.
2. There are enormous problems with specificity and sensitivity of the current disorders. On the one hand, Somatization Disorder is diagnosed so rarely that careful delineation of validators is next to impossible. On the other hand, Undifferentiated Somatoform Disorder and Somatoform Disorder NOS are so broadly defined that one could make such diagnoses in up to 50% of the population. The criteria for the proposed disorders are designed to improve the problems with over-specificity and over-sensitivity.
1 References for these points are provided in the accompanying documents.
DRAFT - CONFID
ENTIAL

** 5/31/2012 This document was included in the Work Group’s initial submission to the SRC. Please note that CSSD and SSSD have since been consolidated. We are providing this because of the succinct summary of problems with the status quo.
5
3. While these disorders are commonly encountered, particularly in primary care, doctors do not use the existing codes. A recent study of 1,203,927 insured patients found somatoform diagnoses in only 569 patients. What is evident however is that there is an enormous amount of patient suffering associated with these disorders, and that partially because of the diagnostic confusion itself, these disorders are more often than not neither recognized nor treated.
4. The group of disorders in DSM-IV-TR emphasizes Medically Unexplained Symptoms (MUS) as the common organizing theme. In fact, grounding a diagnosis on the absence of an explanation is intensely problematic; the reliability of MUS is limited; and the use of such labeling reinforces mind body dualism.
5. Finally, patients loathe these diagnoses. No one wants to have a diagnosis of a dreadful illness, but patients regard these diagnoses as intensely pejorative and demeaning.
Rationale for the new proposals: The proposed classification deemphasizes the central role of medically unexplained symptoms. Instead, it defines disorders on the basis of positive symptoms (distressing somatic symptoms + abnormal thoughts, feelings, and behaviors in response to these symptoms).
The proposals allow for the complexity of the interface between psychiatry and medicine. Patients with somatic symptoms plus abnormal thoughts, feelings, and behaviors may or may not have a diagnosed medical condition; indeed, frequently, they do2.
Complex Somatic Symptom Disorder (CSSD) includes the patients with the most severe symptomatology in terms of the number of abnormal thoughts, feelings, and behaviors, as well as the duration of symptoms.
Simple Somatic Symptom Disorder (SSSD) is the “ghost” of Undifferentiated Somatoform Disorder and Somatoform Disorder NOS, but is more specific than the previous disorders.
Considerable data suggest that hypochondriasis is in fact heterogeneous. Approximately 75% of hypochondriacs would be subsumed under the new diagnosis of CSSD. However, ~25% of hypochondriacs have abnormal thoughts, feelings, and behaviors in the absence of somatic symptoms; furthermore, many such patients would not qualify for an anxiety disorder diagnosis. The new diagnosis of Illness Anxiety Disorder (IAD) is proposed for this latter group of patients.
2 Shakespeare, “When sorrows come, they come not as single spies but as whole battalions.”
DRAFT - CONFID
ENTIAL

1
TO: CPHC From: Somatic Symptom and Related Disorders Workgroup Date: 7/17/12 RE: Somatic Symptom Disorder (SSD) and Illness Anxiety Disorder (IAD) This cover memo summarizes the proposals for SSD and IAD in the context of the CPHC evaluation form. Proposal: The workgroup proposes recasting the entire somatoform disorders chapter by:
1. deemphasizing the centrality of medically unexplained symptoms and instead emphasizing the disproportionate thoughts, feelings, and behaviors that accompany such symptoms
2. decreasing the number of diagnoses in recognition of their substantial overlap
3. recognizing a difference between SSD and IAD (in patients with IAD the somatic symptoms themselves are less prominent, and the patient is instead preoccupied that he will get a somatic disorder).
Magnitude of the change: We would regard this as a major change, although in actuality the amount of research on the existing DSM IVTR somatoform disorders is limited. Evidence for the change: Numerous publications have pointed out the logical problems with basing a diagnosis on negative criteria (medically unexplained symptoms). Numerous publications have pointed out the considerable overlap amongst the existing DSM IVTR somatoform disorders. Numerous publications have pointed out that the current disorders are stigmatizing. Reasons for and consequences of the proposed change Clinical utility: The diagnosis of somatization disorder has been repeatedly demonstrated as too restrictive. The diagnosis of undifferentiated somatoform disorder and somatoform disorder NOS have been repeatedly demonstrated as too diffuse and over-inclusive. By reorganizing the conceptual basis of these disorders, it is hoped that they will be more readily recognized and treated.
DRAFT - CONFID
ENTIAL

2
By eliminating the over-emphasis on medically unexplained symptoms and terms such as hypochondriasis, it is hoped that the disorders will be less stigmatizing. Public health concerns By recognizing that medically explained and medically unexplained commonly coexist, the new disorders increase the detection of previously unrecognized clinically significant problems. The new criteria are clearer and likely to reduce the over-diagnosis of undifferentiated somatoform disorder. Logical Consistency This grouping and simplification of the classification is likely to simplify and make a more rational placement of the diagnoses. The somatic symptoms workgroup and the anxiety disorders workgroup empanelled an international group of experts to advise regarding IAD. That group worked on defining criteria as well as the logic for the placement of IAD within the DSM. The consensus was that IAD could be logically placed either within the anxiety disorders section or the somatic symptom and related disorders section. The majority of the experts recommended that IAD’s primary location should be within the somatic symptom and related disorders section and that secondary listing should be provided within the anxiety disorders section. It was thought that the primary location within the Somatic Symptom and Related Disorders chapter would prove more useful, particularly for primary care clinicians. Estimation of caseness Psychiatric epidemiology has generally ignored studying this group of disorders. Thus, existing data on DSM IVTR caseness are limited. Data on caseness using the proposed criteria for SSD are even more difficult to come by. However, an international group recently conducted a secondary analysis of existing data, using items that could reasonably be expected to reflect SSD criteria (for details, see page 4 of our memo to SRC, dated 2/18/12). The group had access to data from 3 groups of subjects—healthy controls, patients with “functional disorders” (irritable bowel syndrome, etc.) and patients with major medical illnesses (e.g. cancer). All diagnoses were confirmed by review of medical records. The study found that up to 1% of healthy controls and up to 13% of patients with diagnosed major medical illnesses would be diagnosed with SSD. For patients with “functional disorders,” the comparable figure is ~17%. In comparison, using DSM IVTR criteria, >40% of the population would be diagnosed with Undifferentiated Somatoform Disorder. Caseness will certainly be affected by measures used to recognize Criteria B of SSD (disproportionate thoughts, feelings, and behaviors). It should be noted that the Field Trials assessed SSD; these studies demonstrated excellent reliability of diagnosis between clinicians and excellent agreement between clinicians and patients in terms of the severity of symptoms.
DRAFT - CONFID
ENTIAL

3
Possible negative consequences We have received and incorporated suggestions from forensic reviewers regarding clarification of criteria. Some patient groups, particularly those representing British chronic fatigue patients, feel that these criteria will erroneously categorize such patients as having a psychiatric disorder. In fact, chronic fatigue is a very heterogeneous syndrome and it is likely that some patients would and some would not qualify for a diagnosis of SSD. In contrast, under the DSM IVTR guidelines, arguably all chronic fatigue patients would be diagnosed with Undifferentiated Somatoform Disorder. Some have worried that all patients with major medical disorders will be inappropriately diagnosed with SSD. There is a wide range of responses to major illness. The diagnosis of SSD is made when patients have persistent multiple somatic complaints that are associated with disproportionate thoughts, feelings, and behaviors related to such complaints. As mentioned in the Estimation of Caseness section, we have found that only ~13% of patients with major medical illnesses would fulfill caseness.
DRAFT - CONFID
ENTIAL

6
TO: SRC
FROM: Somatic Symptom Disorders Workgroup
DATE: February 18, 2012
RE: your memo of 12/6/11
We were pleased to receive your memo of December 6, 2011. Your memo posed three questions.
1. Are these disorders included in the current Field Trials?
Somatic Symptom Disorder (SSD) was included in field trials and the criteria performed well. The intraclass kappa was .600 (95% CI: .370, .779), indicating good agreement 1 amongst raters. It is interesting to note that this new diagnosis, using very different criteria from those employed in DSM IV, actually performed better than disorders such as Major Depressive Disorder and Generalized Anxiety Disorder.
The field trial data also facilitated a number of analyses of severity. From patient self-reports on a modified version of the PHQ-15 (PHQ-SSS), the ICC was .749 (95% CI: .677, .807), which indicates good reliability1. The field trials also asked clinicians to qualitatively rate the severity of each of the B-type criteria (disproportionate beliefs, etc.) on a scale of 0 to 4, with 0=Not at all and 4 = Very much. This clinician rated measure was also found to have good test-retest reliability1 as demonstrated by an ICC of .680 (95% CI: .571, .766). The clinician’s global rating of the severity of the complex somatic symptoms (none, mild, moderate, severe, or extreme/profound) showed acceptable reliability1 with an ICC of .483 (95% CI: .361, .588).
There was excellent agreement between clinician rated severity and patient reported severity. Patient reported severity was obtained from the PHQ-SSS and clinician rated severity was rated globally and also specifically for disproportionate beliefs etc. For the former, the correlation was 0.533 and for the latter the correlation was 0.952.
These are striking and encouraging data, particularly inasmuch as SSD is a new diagnosis. 1 (Kraemer HC, Kupfer DJ, Clarke DE, Narrow WE, Regier DA. DSM5: How Reliable is Reliable Enough? American Journal of Psychiatry. 2012; 169:13-15)
DRAFT - CONFID
ENTIAL

7
Simple Somatic Symptom Disorder was not a focus in field trials; however as discussed in responses #2 and #3 below, we are no longer proposing this diagnosis, since it can be incorporated into the SSD diagnosis but scored as “mild” on severity criteria.
2. We had some confusion as to whether the criteria for CSSD and SSSD are closer to the undifferentiated somatoform or abridged somatization criteria. It would be helpful if the workgroup could prepare a grid (similar to that already provided), which would specifically compare DSM IV criteria for somatization disorder, undifferentiated somatoform disorder, the abridged criteria for somatization disorder and the proposed criteria for CSSD and SSSD. The views of the workgroup on this question would be helpful as well.
Since our original submission to the SRC, the workgroup has decided that further consolidation of diagnoses was desirable. We have eliminated Simple Somatic Symptom Disorder (SSSD) and instead recognized it as a less severe form of SSD. As a result, your question regarding CSSD and SSSD would appear to be moot.
We are not entirely sure we understand your request for preparing a new grid. It is graphically challenging to compare SSD side-by-side with all of the previous non-consolidated DSM IV diagnoses. The SSD proposal for DSM V is roughly 15% the length of the status quo in DSM IV (188 vs 1248 words). SSD emphasizes both symptoms as well as disproportionate thoughts, feelings, and behaviors (the “B” criteria). Undifferentiated somatoform and abridged somatization emphasize somatic symptoms alone. SSD is more specific than the prior criteria for undifferentiated somatoform disorder.
The data presented below in response to query 3 demonstrate that requiring both symptoms and cognitions leads to a lower estimate of the prevalence of the disorder than merely counting symptoms.
3. Are there available estimates of changes in the newly proposed disorders prevalence compared with abridged somatization disorder associated with the elimination of the requirement for medically unexplained symptoms? The Kisely et al study which you kindly provided suggested significant differences between the patients with medically unexplained symptoms, medically explained symptoms and a combined group. Please comment on how distinctive you think these subgroups are.
DRAFT - CONFID
ENTIAL

8
There are considerable data demonstrating that criteria like those proposed for SSD (i.e. eliminating the requirement for medically unexplained symptoms) result in reasonable prevalence estimates (Creed et al, J Psychosom Res, in press). In a sub-analysis of this data set, Creed surveyed 952 individuals using the Somatic Symptom Index as a count of somatic symptoms (criterion A of SSD) as well as 3 items from the Whiteley Index (proxy measures for disproportionate concerns, etc., for criterion B).
Using criterion A alone (symptom count), 197 (i.e. 20.6%) people reported multiple somatic symptoms and thus could meet criteria for abridged somatization (i.e. 6 somatic symptoms that bothered the respondent quite a bit or worse).
For criterion B, 3 Whiteley Index items were examined. When people answered “quite a bit” or “a great deal” to these items, they were considered to fulfill a B-type criterion.
• “do you think there is something seriously wrong with your body” (5.3% of the sample)
• “do you worry a lot about your health?” (9.8% of the sample) • “is it hard for you to forget about yourself and think about all sorts of
other things?” (5.1% of the sample)
Requiring both A-type and B-type criteria reduces estimates of SSD prevalence. For instance, among the high symptom respondents, 133 lacked any B criteria and would thus not be diagnosed with SSD. Thirty-six had only one B criterion and could thus be considered to have mild SSD (according to the new revised severity measures) and 28 had two or more B criteria, implying moderate to severe SSD.
The original sample was randomly selected and population-based (n=952). Not all patients allowed their medical records to be verified. However, when it was possible to verify the patient reported data, the prevalence of SSD criteria was also determined for patients with medical illness (e.g. heart disease, arthritis, n=339); patients with functional syndromes (e.g. irritable bowel syndrome, chronic widespread pain or chronic fatigue: n=107); and healthy comparison group (without medical illness or functional syndromes, n=337). The table below summarizes prevalence in each of these samples. The numbers in the groups vary as “functional disorder” could only be assessed in the group of respondents who allowed access to their medical records (necessary to exclude medical causes for pain or fatigue).
DRAFT - CONFID
ENTIAL

9
Sample high symptom count
symptoms + one B criterion
symptoms + >1 B criterion
Population based total sample (n=952)
197/952 (20.6%)
36/952 (3.8%) 28/952 (2.9%)
Healthy subgroup (n= 337)
24/337 (7.1%) 2/337 (0.6%) 1/337 (0.3%)
Medical illness subgroup (n= 339)
108/339 (31.8%)
20/339 (5.8%) 25/339 (7.3%)
Functional disorder subgroup (n=107 )
49/107 (45.7%)
4/107 (3.7%) 14/107 (13.1%)
The reviewers asked us to comment on the Kisely article. We suspect that the comment arose because the article suggested that there were different numbers of somatic symptoms associated with the threshold for psychiatric disorder. This would be relevant if SSD were diagnosed only according to number of somatic symptoms like Somatization Disorder was. The diagnosis of SSD is not based on a specified number of somatic symptoms; so this concern should not arise.
Amongst their many findings, Kisley et al observed that, irrespective of etiology, increased numbers of somatic symptoms were associated with increased psychiatric morbidity and that, frequently, medically explained and unexplained symptoms co-occurred. As such, these findings support many of our workgroup’s proposals. They also observed some differences in terms of gender and age distribution in the medically explained vs unexplained groups. While we find these latter observations interesting, we feel that the distinction between medically explained and medically unexplained is in fact an unreliable one and that it is the combination of somatic symptoms and disproportionate thoughts, feelings, and behaviors related to these symptoms that form the crucial core of SSD.
DRAFT - CONFID
ENTIAL

1F.H. Creed et al. / Journal of Psychosomatic Research xxx (2012) xxx–xxx
PSR-08408; No of Pages 6
Contents lists available at SciVerse ScienceDirect
Journal of Psychosomatic Research
The epidemiology of multiple somatic symptoms
Francis H. Creed a,⁎, Ian Davies b, Judy Jackson a, Alison Littlewood b, Carolyn Chew-Graham a,Barbara Tomenson a, Gary Macfarlane c, Arthur Barsky d, Wayne Katon e, John McBeth b
a School of Community Based Medicine, The University of Manchester, Manchester, UKb Arthritis Research UK Epidemiology Unit, The University of Manchester, Manchester, UKc Aberdeen Pain Research Collaboration (Epidemiology Group), University of Aberdeen, UKd Department of Psychiatry, Brigham and Women's Hospital and Harvard Medical School, Boston, MA, USAe Department of Psychiatry & Behavioural Sciences, University of Washington School of Medicine, Seattle, WA, USA
⁎ Corresponding author at: School of Community BMcFarlane Building, University Place, Oxford Road, Ma161 276 5331; fax: +44 161 306 7945.
E-mail address: [email protected] (F.H
0022-3999/$ – see front matter © 2012 Elsevier Inc. Alldoi:10.1016/j.jpsychores.2012.01.009
Please cite this article as: Creed FH, et aj.jpsychores.2012.01.009
a b s t r a c t IAL
a r t i c l e i n f o
Article history:
Received 18 October 2011Received in revised form 12 January 2012Accepted 12 January 2012Available online xxxxKeywords:Somatoform disordersSomatisationEpidemiologyHealth-related quality of life
Background: The risk factors for a high total somatic symptom count are unclear; and it is not known whethertotal somatic symptoms count is a predictor of impaired health status.Method: A prospective population-based cohort study in North West England. Randomly sampled residents(1443 participants; 58% response) completed questionnaires to determine number of somatic symptoms(SSI), health status and a wide range of risk factors; 741 completed questionnaires 1 year later. We usedlogistic regression to identify risk factors for high SSI at follow-up and for persistently high SSI. We usedANCOVAR and multiple regression to assess whether baseline SSI predicted health status at follow-up.Results: Twenty-one percent of participants scored over 25 on the Somatic Symptom Inventory (SSI) at base-line and 14% at both baseline and follow-up. Risk factors for a persistent high SSI were: fewer than 12 years ofeducation, separated, widowed or divorced status, reported psychological abuse during childhood, co-existing
FIDENT
medical illnesses, anxiety and depression. In multivariate analysis baseline SSI predicted health status (SF12physical component score and health-related quality of life (EuroQol)) 12 months later. Persistent high SSIwas a clinically meaningful predictor of these outcomes.Conclusions: Our data support a biopsychosocial approach to somatic symptoms rather than the dualisticapproach of identifying “medically unexplained” symptoms. The risk factors for total somatic symptomcount were those associated with psychiatric disorders including physical illness. A persistent high somaticsymptom count provides a readily measured dimension of importance in epidemiology as a predictor ofhealth status.T - C
ON
© 2012 Elsevier Inc. All rights reserved.
F A IntroductionThe concept of somatisation disorder concerns persistent multiple“medically unexplained” symptoms which impair health status [1,2].This is regarded as a psychiatric disorder and included in DSM andICD classifications as one of the somatoform disorders but the evi-dence base supporting this as an independent psychiatric disorder islimited [3]. The concept of “medically unexplained” symptoms hasbeen criticised as it is dualistic in concept, its measurement is timeconsuming, but unreliable, and it is not clear whether the relationshipbetween medically unexplained symptoms and outcome is explainedby anxiety and depression [4–10]. As a result of these difficulties,somatoform disorders have been omitted from many recentpopulation-based studies of psychiatric disorders [5,6,11–13].
DR
ased Medicine, 3rd floor, Jeannchester, M13 9PL. Tel.: +44
. Creed).
rights reserved.
l, The epidemiology of mu
Meanwhile, patients presenting with multiple somatic symptoms re-main a challenge to clinicians and this phenomenon is not well un-derstood [14–16]. It has been suggested that a biopsychosocialapproach, which encompasses the interaction of physiological, psy-chological and social factors could help explain the presentation ofbothersome somatic symptoms [17,18]. The current review of theDSM-IV somatoform disorders in preparation for DSM-V is adoptingsuch an approach by highlighting the importance of psychologicaland physical factors in the development of bothersome somaticsymptoms [9].
There is now evidence that a high total somatic symptom count,i.e. including medically explained and unexplained symptoms, is cor-related with impaired health status in cross-sectional clinical studies[13,18–21] and may predict increased health care use after adjust-ment for relevant confounders [22]. Somatic symptoms have beenshown to have some independence from anxiety and depression ingenetic and related studies [23–27], but it is unclear whether theypredict outcome independent of anxiety and depression. Somaticsymptoms predict a poor response to treatment for depression and
ltiple somatic symptoms, J Psychosom Res (2012), doi:10.1016/

Journal of Psychosomatic Research xxx (2012) xxx–xxx
anxiety [28] and can respond to specific psychological treatmentwithout reduction of concurrent anxiety or depression [29–31]. Inspite of the importance of bothersome somatic symptoms that persistover time our knowledge of their aetiology is incomplete [32–36].
If a high total somatic symptom count is to be considered an inde-pendent dimension of psychopathology it is necessary to demon-strate in prospective population-based studies the risk factors for apersistent high total somatic symptom count and its value as a predic-tor of impaired health status. In this paper we first assessed the riskfactors for a high total somatic symptom count. Secondly, we assessedwhether a high total somatic symptom count predicts impairedhealth status after adjustment for anxiety, depression and physical ill-ness [6].
To identify the risk factors for total somatic symptom count weused prospective analyses. We identified the risk factors for 1) ahigh total somatic symptom score 1 year after baseline and 2) for apersistently high score, as this is associated with poor outcomes andis used for diagnostic purposes [5,37]. We included a range of risk fac-tors including demographic characteristics, physical and psychiatricdisorders, childhood experiences, personality measures and recentthreatening life events as these are associated with somatoformdisorders [6,38–40]. The second aim of the study used a prospectivedesign to assess whether a high baseline total somatic symptomcount predicted poor health status one year later after adjustmentfor confounders.
Method
We used a cross-sectional population-based design followed by aprospective cohort study.
Sample
Wemailed 2985 baseline questionnaires to people aged 25–65 yearsregistered at two general practices in North West England, one in anaffluent rural area and one in an inner city area. Potential participantswere selected from complete population lists (i.e. GP registers) usingsimple random sampling assuming that the sampled sub-group was C
O
EN
Identifiprac
Returned questionnaireN=1999 (80.3%)
CompleteN=1443(58.0%)
Agreed to complete 1 yearfollow up questionnaire?
NoN=455(31.5%)
Returned follow up questionnaireN=741 (75.0%)
Blank/unusableN=553(22.2%)
YesN=988(68.5%)
Fig. 1. Flow of stud
Please cite this article as: Creed FH, et al, The epidemiology of muj.jpsychores.2012.01.009
DRAFT -
representative of the population from which they were drawn.Questionnaires were returned by 1999 out of 2490 eligible participants(return rate 80.3%), of which 553 (22.2%) were blank or did not containusable information and three (0.1%)were completed by thewrong per-son (see Fig. 1). A total of 1443 (58.0%) participants returned a completequestionnaire and participated in the study. Non-responders were sig-nificantly more likely to be male (53.1% vs 42.3%), and younger(mean=43.9 vs 47.0 years) than the rest of the eligible participants;participation rates between centres were similar (56.3% and 59.3%).
We requested consent from the 1443 respondents to a follow-upquestionnaire 1 year later; 988 (68%) agreed, of whom 741 (75%)completed the follow-up questionnaires.
The study received ethical approval from the North ManchesterLocal Research Ethics Committee (REC reference number: 06/Q1406/14).
Measures
The following questionnaires were administered:
Potential risk factors or correlates
We collected demographic details including age, sex, marital status,socio-economic status, current work status (including disability sta-tus) and years of education. Respondents were asked about any co-existing medical illnesses by asking them to tick relevant ones on alist of common disorders and/or adding the name of any additionalillness(es). These were analysed as none, one, two or more generalmedical illnesses.
The Childhood Physical and Sexual Abuse questionnaire consists of8 questions concerning abuse [41]. Respondents were rated as havingexperienced childhood abuse if, before the age of 16 years, theyreported that an older person touched them or they were made totouch someone else in a sexual way, or intercourse was attemptedor completed (sexual abuse); that they were hit, kicked or beatenoften and/or their life was seriously threatened (physical abuse);they were often insulted, humiliated or made to feel guilty (psycho-logical abuse).
NFIDENTIA
L
ligible=2490
ed on general tice registerN=2985
Non-responderN=491 (19.7%)
WastedN=3
(0.1%)
IneligibleN=495 (16.6%)
(494 wrong address, 1 died)
y participants.
ltiple somatic symptoms, J Psychosom Res (2012), doi:10.1016/

3F.H. Creed et al. / Journal of Psychosomatic Research xxx (2012) xxx–xxx
N
The Parental Bonding Instrument includes 7 questions concerningperceived maternal care and 1 item concerning maternal control[42,43]. Social Support was assessed with a question determiningwhether the respondent had a close confidant with whom they candiscuss all concerns.
The Revised NEO Personality Inventory (NEO-PI-R) measures thepersonality trait of Neuroticism [44], a well recognised correlate ofsomatisation [45].
Recent stress and mental state
The List of threatening experiences (LTE-Q) measures the experi-ence of 12 threatening personal situations or events in the last6 months [46] The total score of positive responses represents recentexposure to threatening experiences. We analysed the responses to 4illness-related items (illness affecting respondent or close others)separately from the total of the remaining 8 items.
The Hospital Anxiety and Depression Scale (HADS) assesses anxietyand depression but without asking about physical symptoms (e.g.weight loss, pain) that might be caused by physical illness [47]. It con-tains 7 items each for anxiety and depression and is valid and reliablein general population; a total HADS score (anxiety+depression) of 17or more indicates probable depressive disorder [48].
Outcome variables: somatic symptoms and health status
The Somatic Symptom Inventory (SSI) asks respondents to rateeach of 13 somatic symptoms on a 5-point Likert scale as to “howmuch it has bothered you over the past 6 months?” Answers rangefrom 1 = “Not at all” to 5 = “A great deal” [49] . The total score over-all is calculated (range 13 to 65). The list of common symptoms in SSIoverlaps considerably with the PHQ-15 [19] but, unlike the latter,does not include any gender specific symptoms, such as menstrualcramps. We analysed the data using the top two deciles of the SSI(scores of 26–30 and SSI≥31 respectively) as previous work hasused such cut-offs to define clinically significant somatic symptoms[19–21].
We measured health status using two generic measures. For thewidely used Short Form 12 (SF12) Questionnaire [50] we used thescoring algorithm to weight indicator variables, which generates thePhysical (PCS-12) andMental Health (MCS-12) Component SummaryScores. Each of these summary scores is transformed into norm basedscoring. The Euroqol (EQ5D) [51] asks respondents to rate, on a 3point scale, problems they experience in mobility, self care, usual ac-tivities, pain/discomfort and anxiety/depression. It also asks respon-dents to rate, on a vertical “thermometer”, their own health todayon a scale from 0 (worst imaginable health state) to 100 (bestimaginable).
Statistical analysis
Density plots show the distribution of Somatic Symptoms Index(SSI) for a) all participants b) stratified by HADS total score (anxietyand depression 17 or more vs 16 or less), c) by number of medical ill-nesses (0, 1, 2 or more) and d) by 2 or more medical illnesses and/orHADS total score 17 or more.
Univariate analysis compared the baseline data of respondents inthe top two deciles of the SSI at follow-up (scores of 26–30 andSSI≥31 respectively) with the remainder using chi square or oneway ANOVA with test for linear trend across the 3 groups. To adjustfor gender, anxiety, depression and recent illness or injury we usedlogistic regression (Table 1); odds ratios and 95% confidence intervalsare shown for an SSI score of 31 or more (top 8.9% of sample). Weused ANCOVAR for continuous variables (Table 2).
In order to identify risk factors of a persistent high SSI we used lo-gistic regression with high SSI score (over 25) at both baseline and
DRAFT - CO
Please cite this article as: Creed FH, et al, The epidemiology of muj.jpsychores.2012.01.009
follow up as the dependent variable; the independent variableswere all of those in Table 1 (except the marked employment statusones) and all those with an asterisk in Table 2.
To establish whether SSI is a predictor of health status at follow-up, we performed a series of ANCOVARs with follow-up SF12 physicaland mental component summary scores and EuroQol (EQ5D) as de-pendent variables. We compared participants with and without ahigh SSI (>25), adjusting for age, gender, HADS anxiety and depres-sion, number of illnesses and relevant baseline value of the health sta-tus measure. We then performed 3 multiple regression analyses withfollow-up SF-12 physical and mental component scores and Euroqolthermometer as the dependent variables. In each analysis we includ-ed baseline SSI as an independent variable in addition to those vari-ables marked in Tables 1 and 2a. These three multiple regressionanalyses were repeated using persistent high SSI (i.e. SSI>25 at bothbaseline and follow-up) instead of baseline SSI.
In all the logistic and regression analyses, the stata imputation com-mand was used to impute values for missing data on the independentvariables, using the remaining variables in the samemodel. In all the re-gression analyses, inverse probability sampling weights were used toadjust for the non completion of questionnaires. For non completionof baseline questionnaires (1443 returned out of 2487 eligible), theprobability of completion was calculated using logistic regression withindependent variables centre, age and gender. For non completion offollow-up questionnaires (741 returned out of the 1443 at baseline),the probability of completion was calculated using logistic regressionwith all the baseline variables as independent variables. Analyseswere carried out using SPSS versions 15 and 16, and Stata version 11.2.
The power calculation for the study was determined by the num-ber of new onsets of functional somatic syndromes anticipated over a1 year period. This required 2100 participants at baseline. In the eventwe had complete data on 1433 at baseline and 741 at follow-up. Forthe purposes of the present analysis the comparison of 104 partici-pants with persistent high SSI scores (top 20%: >25 at both baselineand follow-up) and the remaining 637 participants, a 2-sided 5% sig-nificance test would have 80% power to detect even an effect size of0.3. The multiple regression analyses with follow up data as depen-dent variables were based on a sample of 741 participants; thesehave 80% power to detect a multiple correlation coefficient of 0.031(r=0.18) with up to 26 covariates.
Results
The flow of participants to the study is shown in Fig. 1.
Baseline Somatic Symptom Index (SSI)
The density plot of baseline Somatic Symptom Index (SSI) shows a positivelyskewed continuous distribution (Fig. 2a). The lowest score, 13, indicates no symptoms.The curve peaks at 18 suggesting that many people report a few mildly bothersomesymptoms. Three hundred and four participants (21.1%) scored over 25 and 129(8.9%) scored over 30 The curve is shifted to the right for participants with a totalHADS (anxiety plus depression) score of 17, for those with 1 or more general medicalillnesses, and, most extremely, in those with both of these factors (Fig. 2).
Risk factors for follow-up and persistent SSI
Complete data were available for 741 participants at 1 year follow-up. Of these,104 (14%) participants had an SSI over 25 at both baseline and 1 year later; 39 (5.3%)had an SSI over 30 at both times.
Those who completed the follow-up were significantly older than the non-responders (mean 49 vs 45 years). They were more likely to be married or cohabiting(77% vs 71%) but did not differ on any other socio-demographic variable or SSI (21.3(sd=6.6) vs 21.2 (sd=6.7)).
Tables 1 and 2 demonstrate the risk factors for a high SSI at follow-up after adjust-ment for sex, HADS anxiety and depression, and recent serious illness. The risk factorswere: separated, widowed or divorced status, fewer than 12 years of education, ab-sence of a close confidant, off work due to ill health, a recent serious illness or injury,older age, neuroticism, anxiety, depression, impaired health status indicated by lowSF-12 physical component score and EUROQOL. All of these were associated withfollow-up SSI in the expected direction in a dose–response fashion.
FIDENTIA
L
ltiple somatic symptoms, J Psychosom Res (2012), doi:10.1016/

Table 2Scored measures at baseline and follow up according to SSI grouping at follow up(n=741)
Baseline scores SSI b26n=588mean (sd) a
SSI 26 to 30n=83mean (sd) a
SSI≥31n=70mean (sd) a
Pvalue a
Pvalue b
Agec 48.4 (11.1) 49.1 (10.8) 49.8 (11.1) .28 .048Maternal care scorec 16.6 (4.9) 15.9 (5.6) 16.4 (4.4) .41 .015Maternal controlscorec
0.89 (1.02) 0.98 (1.09) 0.92 (1.11) .61 .23
Neuroticism score 15.3 (8.6) 21.4 (9.3) 26.9 (8.4) b.001 .031HADS anxietyc 5.2 (3.4) 8.0 (3.6) 9.9 (3.9) b.001 b.001HADS depressionc 2.3 (2.4) 4.4 (3.4) 7.6 (4.4) b.001 b.001Threateningexperiences scorec
(excluding illness,injury and death)
0.32 (0.66) 0.57 (0.89) 0.81 (1.13) b.001 .67
SF-12 physical score 52.1 (7.8) 44.6 (9.7) 40.0 (12.0) b.001 b.001SF-12 mental score 49.9 (9.4) 45.5 (10.6) 36.3 (11.8) b.001 .41EUROQOLthermometer
82.9 (13.1) 73.7 (16.1) 60.2 (21.9) b.001 b.001
Outcome measures at 1 yearHADS anxiety 4.9 (3.5) 8.0 (4.0) 9.9 (3.9) b.001 b.001HADS depression 2.2 (2.5) 4.4 (3.5) 8.3 (4.8) b.001 b.001SF12 physical score 51.9 (7.5) 44.1 (10.8) 38.7 (12.8) b.001 b.001SF12 mental score 50.9 (9.2) 44.5 (11.7) 35.4 (12.1) b.001 b.001EUROQOLthermometer
83.2 (13.4) 71.1 (17.2) 55.7 (22.4) b.001 b.001
a Unadjusted means and standard deviations, and unadjusted p-value for trendacross 3 groups.
b p-value for trend across 3 groups adjusted for gender, HADS anxiety and depres-sion, and recent serious illness (HADS anxiety and depression adjusted for genderand recent serious illness only).
c Included in multiple regression analysis (see text).
Table 1Baseline categorical measures according to SSI grouping at follow up (n=741).
Baseline measures SSI b26n=588no (%)
SSI 26 to 30n=83no (%)
SSI≥31n=70no (%)
P value for trendacross 3 groups
Oddsratio a
95% confidenceinterval a
Oddsratio b
95% confidenceinterval b
Female 337 (57.3) 51 (61.4) 44 (62.9) .29 1.23 0.74 to 2.05 – –
Single 70 (11.9) 14 (17.1) 9 (12.9) 1.03 0.49 to 2.15 0.52 0.20 to 1.35Married (reference category) 476 (81.1) 56 (68.3) 40 (57.1) .001 1.0 – – –
Separated/widowed/divorced 41 (7.0) 12 (14.6) 21 (30.0) 4.98 2.78 to 8.92 2.84 1.37 to 5.88
Less than 12 years of education 138 (24.0) 33 (39.8) 36 (52.9) b.001 3.21 1.93 to 5.33 3.34 1.82 to 6.12
No confidant 24 (4.1) 4 (4.8) 17 (24.6) b.001 7.50 3.85 to 14.6 2.56 1.11 to 5.94
Working (reference category) d 467 (80.4) 60 (72.3) 45 (66.2) 1.0 – – –
Unemployed (seeking work) d 9 (1.5) 2 (2.4) 2 (2.9) .053 1.80 0.40 to 8.29 1.27 0.23 to 7.15Not working (ill health) d 4 (0.7) 5 (6.0) 11 (16.2) 14.0 5.59 to 35.3 3.20 0.94 to 10.9Student, retired, etc. d 101 (17.4) 16 (19.3) 10 (14.7) 0.81 0.40 to 1.62 1.08 0.48 to 2.43
Off work due to ill health in the past month 44 (7.7) 10 (12.8) 28 (42.4) b.001 8.15 4.64 to 14.3 4.43 2.20 to 8.89
Current illness 2 or more (out of 484) 36 (9.4) 10 (19.6) 13 (26.5) b.001 3.05 1.51 to 6.17 1.95 c 0.81 to 4.71 c
Childhood factors
Sexual abuse 58 (9.9) 13 (15.9) 7 (10.1) .48 0.95 0.42 to 2.15 0.46 0.16 to 1.30
Psychological abuse 17 (2.9) 10 (12.0) 7 (10.1) b.001 2.68 1.12 to 6.40 0.72 0.23 to 2.32
Physical abuse 15 (2.6) 6 (7.2) 3 (4.3) .11 1.40 0.41 to 4.83 0.13 0.02 to 0.83
Recent stress
Recent serious illness or injury (participant) 18 (3.1) 12 (14.5) 16 (22.9) b.001 6.32 3.24 to 12.3 2.40 c 1.04 to 5.56 c
Recent serious illness or injury (close relative) 136 (23.2) 22 (26.5) 16 (22.9) .83 0.96 0.54 to 1.73 0.44 0.21 to 0.92
Death of close relative 23 (3.9) 5 (6.0) 4 (5.7) .34 1.39 0.47 to 4.08 0.44 0.10 to 1.98
Death of close friend 83 (14.2) 14 (16.9) 18 (25.7) .014 2.04 1.15 to 3.64 1.28 0.62 to 2.63
a Odds ratio and 95% confidence interval for variable by SSI≥31 (unadjusted).b Odds ratio and 95% confidence interval for variable by SSI≥31 adjusted for gender, HADS anxiety and depression, and recent serious illness.c Odds ratio and 95% confidence interval for variable by SSI≥31 adjusted for gender, and HADS anxiety and depression.d These variables were omitted from regression analysis.
4 F.H. Creed et al. / Journal of Psychosomatic Research xxx (2012) xxx–xxx
Please cite this article as: Creed FH, et al, The epidemiology of muj.jpsychores.2012.01.009
DRAFT - CONFID
ENTIAL
The followingbaseline variableswere associatedwith a high SSI at follow-upbutwereno longer significant after adjustment for gender, HADS anxiety and depression, and re-cent serious illness: 2 or more general medical illnesses, reported psychological abuse,death of a close friend and threatening life events (excluding illness-related events).
The logistic regression analysis to predict a persistent high SSI identified the followingpredictors: psychological abuse, b12 years of education, separated/divorced/widowedstatus, two or more general medical illnesses, anxiety, and depression (Table 3).
SSI as a predictor of health status
Baseline SSI was significantly associated with follow-up scores of SF-12 physicaland mental components and with EUROQOL thermometer after adjustment for gender,HADS anxiety and depression scores and number of physical illnesses, (all pb.001).
Persistent SSI predicted all but one of the health status scores, after adjustment forage, gender, anxiety, depression and number of physical illness (Table 4).
In multiple regression analyses, which adjusted for all the covariates mentionedabove, baseline SSI was associated with follow-up physical component score(pb.001), Euroqol thermometer (p=.001), but not mental component score (p=.11).A persistent high SSI score was associated with follow-up physical component score(unstandardised regression coefficient, b=−5.7, 95% confidence interval −8.1 to−3.4, pb.001), mental component score (b=−5.3, 95% CI −7.9 to −2.6, pb0.001),and Euroqol thermometer score (b=−7.9, 95% CI −12.0 to −3.7, p;.001).
Discussion
There are two new findings from this study. First we have shownthat the risk factors for a persistent high total somatic symptom countinclude childhood psychological abuse, fewer than 12 years of educa-tion and separated/divorced/widowed status, aswell as generalmedicalillness, anxiety and depression. These are well-recognised risk factorsfor psychiatric disorders, which were all associated with total somaticsymptom count in a dose–response fashion. They are similar to therisk factors for persistent medically unexplained symptoms observed
ltiple somatic symptoms, J Psychosom Res (2012), doi:10.1016/

b)
0.0
2.0
4.0
6.0
8.1
10 20 30 40 50 60somatic symptom inventory total score
< 17 >= 17
c)
0.0
2.0
4.0
6.0
8.1
10 20 30 40 50 60Somatic Symptom Inventory total score
No illnesses One illnessTwo or more illness
d)
0.0
2.0
4.0
6.0
8.1
10 20 30 40 50 60Somatic Symptom Inventory total score
Neither HADS total >= 17 only2 or more illness only Both
0.0
2.0
4.0
6.0
8
10 20 30 40 50 60somatic symptom inventory total score
a)
Fig. 2. Figure shows the distribution of SSI scores at baseline for: — a) the whole sample b) stratified by HADS total score 17 or more c) stratified by number of general medicalillnesses d) stratified by both two or more illnesses and/or HADS total score 17 or more.
5F.H. Creed et al. / Journal of Psychosomatic Research xxx (2012) xxx–xxx
NFIDENTIA
L
in the few relevant prospective studies [4,5,35–38,52–54]. This proba-bly reflects the fact that themajority of all somatic symptoms are usual-ly categorised as “medically unexplained” [55–59].
Our second new finding was that a persistent high total somaticsymptom countwas an independent predictor of subsequent health sta-tus. For both SF-12 and EUROQOL the adjusted regression coefficientsshow that a persistent high total somatic symptom count predicted clin-ically meaningful impairment [60–63]. Whereas other studies haveshown the correlation between total somatic symptoms count and thediagnosis of “somatoform disorder” [55], our study has focussed onthe fact that total somatic symptom count predicts subsequent healthstatus (SF-12) and health-related quality of life (EUROQOL).
Our findings in a population-based sample complement the most-ly cross-sectional clinical studies showing an association betweenhigh total somatic symptom count, a limited range of risk factors
DRAFT - CO
Table 3Results of logistic regression analyses with dependent variable persistent SSI score of26 or more at both assessments (n=104) vs 637 remaining participants. Samplingweights have been used to adjust for non completion of baseline and follow upquestionnaires
Odds ratio 95% CI Sig
Centre 0.48 0.28 to 0.82 0.007Psychological abuse 3.57 1.04 to 12.2 0.042Less than 12 years of education 2.67 1.46 to 4.88 0.001Separated, widowed or divorced 2.33 1.01 to 5.36 0.047Serious illness/injury to a closerelative in past 6 months
0.30 0.13 to 0.73 0.008
2 or more current illnesses 2.92 1.44 to 5.92 0.003HADS anxiety score 1.19 1.08 to 1.32 0.001HADS depression score 1.23 1.10 to 1.37 b0.001
All other variables described in text were entered also but were non-significant.
Please cite this article as: Creed FH, et al, The epidemiology of muj.jpsychores.2012.01.009
and impaired health status [19,21,64–66]. We did not find thatfollow-up or persistent SSI scores were significantly higher inwomen, which differs from some other studies of persistent medical-ly unexplained symptoms [32,37,53]. In a systematic reviewwe foundthat only half of population-based studies of somatic symptoms founda female preponderance and, in multivariate analysis, the prospectiveWHO primary care study found that female sex was not a predictor ofpersistent high number of somatic symptoms [4,38].
Two- thirds of our participants with a high total somatic symptomcount still reported numerous symptoms 1 year later suggesting con-siderable stability comparable to that reported for somatoform disor-ders [5,67]. We found, for the first time in a prospective, population-based study, that such a persistent high total somatic symptom countis an independent predictor of health status, after adjustment for a
Table 4Mean EQ5D scores (Standard error of mean) at follow-up for participants with persis-tent high (>25) SSI and the remainder
EUROQOL dimension Persistent SSI >25n=104
Remaining participantsn=637
P valuea
Mobility 1.26 (0.03) 1.09 (0.01) b.001Self care 1.04 (0.01) 1.02 (0.01) .086Usual activities 1.36 (0.04) 1.13 (0.01) b.001Pain/discomfort 1.55 (0.05) 1.35 (0.02) b.001Anxiety/depression 1.41 (0.04) 1.22 (0.02) b.001Thermometerb 73.3 (1.4) 80.3 (0.5) b.001SF-12 scoresPCS 46.8 (0.8) 50.3 (0.3) b.001MCS 45.2 (0.9) 49.3 (0.3) b.001
a Adjusted for age, gender, HADS anxiety and depression, number of illnesses andrelevant baseline value.
b Maximum=100.
ltiple somatic symptoms, J Psychosom Res (2012), doi:10.1016/

6 F.H. Creed et al. / Journal of Psychosomatic Research xxx (2012) xxx–xxx
broad range of confounders. This result held for two measures of heathstatus (SF-12 and EUROQOL) and provides some evidence that a persis-tent high SSI might be important diagnostically [5].
Strengths and limitations
The principal strengths of the study lie in its population-based,prospective design, the use of well-recognised measures and the in-clusion of a wider range of risk factors than previous studies, whichallowed us to adjust for a large number of potential confounders.The main limitation is the response rate, which is slightly lowerthan some studies, probably as a result of our further request to re-spondents to complete a follow-up questionnaire. Our sample wasolder and included more females than the population from which itwas drawn but it is not clear that this would have distorted the rela-tionships between the variables we have studied. Furthermore ourfollow-up sample had a similar SSI to the non-responders and we ad-justed for non-response in our analyses. Our numbers were too smallto perform logistic regression analyses on the participants with ahigher cut-off score (>30) at both assessments. Univariate analysisindicated, however, that both risk factors and outcomes were morepronounced in this group with the highest SSI. We did not use a stan-dardised psychiatric interview to ascertain the presence of psychiatricdisorders so we could not compare our results with those derivedfrom using such diagnoses.
As this study was not intended to assess mechanisms we did notmeasure intervening psychological mechanisms such as selective at-tention or health anxiety. Previous work has shown, however, that,in addition to depression and anxiety, heightened awareness of phys-ical symptoms occurs in the presence of chronic medical disease (es-pecially if there is more than one), with a high neuroticism score andwith exposure to parental ill health or abuse during childhood;[35,65,68–70].
Implications
The present findings, with those from three previous prospectiveprimary care studies, suggest that total somatic symptom count isan independent predictor of health status [22,71–73]. As it overcomesthe numerous difficulties of trying to determine whether symptomsare “medically unexplained”, total somatic symptom count shouldbe useful as a readily measured dimension of importance in epidemi-ological studies concerned with predictors of the outcomes of healthstatus and healthcare use. Furthermore it should have clinical utilityin identifying patients who may need specific help with their trouble-some somatic symptoms [30].
We have shown also that the risk factors for a persistent hightotal somatic symptom count are similar to those associated withother psychiatric disorders, such as anxiety and depression, so ourfindings help to strengthen the case for regarding multiple somaticsymptoms as a dimension of psychopathology which is a predictorof health status in people with or without chronic physical illness[9]. As such this is an application of the biopsychosocial model. It islikely that total number of somatic symptoms reflects a dimensionof somatic distress that is distinct from anxiety and depression[23–25,27]. It is not possible to define a disorder, however, simplyby using a “cut-off” score on the continuous variable; we used cut-off scores that approximate to the highest 10% and 20% as thesehave been used in previous clinical studies and appear to have clin-ical validity [19–21,74]. Further work is needed to establish thecut-off that might be used in epidemiological studies to define a“case” but it may be preferable to use a dimensional approach tothe diagnosis of “somatisation” [75].
Finally, it is clear from our data that a high somatic symptom scoreis best seen as a phenomenon of multifactorial aetiology with inter-acting psychological, social and biological factors. Reviewing all of
DRAFT - CO
Please cite this article as: Creed FH, et al, The epidemiology of muj.jpsychores.2012.01.009
the risk factors for a high total somatic symptom count with individ-ual patients should enable treatment to be focussed on the relevantfactors with a view to making it more effective [30,76].
Author contributions
Chew-Graham, Creed, Macfarlane, McBeth: Study development, de-sign, data collection, data analysis, manuscript preparation and revision.
Davies, Jackson, Littlewood: Data collection, manuscript prepara-tion and revision.
Tomenson B: Data analysis, manuscript preparation and revision.Barsky, Katon study development, design, manuscript revision
Conflict of interest
All authors declare no conflicts of interest in relation to the sub-mitted manuscript.
Acknowledgments
We are grateful to the participants in the project and to the GeneralPractitioners who facilitated it.
All authors had full access to all the data in the study, have beeninvolved in drafting and/or revising the article critically and givenfinal approval of the version to be published. The corresponding au-thor takes responsibility for the integrity of the data and the accuracyof the data analysis.
The study was funded by the UK Medical Research Council grantNo G0500272. The UK MRC had no role in study design and conductof the study; collection, management, analysis, and interpretation ofthe data; and preparation, review, or approval of the manuscript.
References
[1] Swartz M, Blazer D, George L, Landerman R. Somatization disorder in a communi-ty population. Am J Psychiatry November 1986;143:1403–8.
[2] American Psychiatric Association. Diagnostic and Statistical Manual of MentalDIsorders — DSM-IV. 4th ed. Washington D.C: American Psychiatric Association;1994.
[3] Mayou R, Kirmayer LJ, Simon G, Kroenke K, Sharpe M. Somatoform disorders: timefor a new approach in DSM-V. [see comment]. [Review] [50 refs]. Am J Psychiatry2005 May;162(5):847–55.
[4] Creed FH, Barsky A. A systematic review of somatisation and hypochondriasis.[Review] [96 refs]J Psychosom Res 2004;56:391–408.
[5] Rief W, Rojas G, Rief W, Rojas G. Stability of somatoform symptoms— implicationsfor classification. [Review] [43 refs]Psychosom Med December 2007;69:864–9.
[6] Lieb R, Meinlschmidt G, Araya R, Lieb R, Meinlschmidt G, Araya R. Epidemiology ofthe association between somatoform disorders and anxiety and depressive disor-ders: an update. [Review] [31 refs]Psychosom Med December 2007;69:860–3.
[7] Creed F, Guthrie E, Fink P, Henningsen P, Rief W, Sharpe M, et al. Is there a betterterm than "medically unexplained symptoms"? J Psychosom Res 2010;68:5–8.
[8] Simon GE, Gureje O. Stability of somatization disorder and somatization symp-toms among primary care patients. Arch Gen Psychiatry January 1999;56:90–5.
[9] Dimsdale J, Creed FH. DSM-V Workgroup on Somatic Symptom Disorders. Theproposed diagnosis of somatic symptom disorders in DSM-V to replace somato-form disorders in DSM-IV—a preliminary report. J Psychosom Res 2009;66:473–6 Ref Type: Generic.
[10] Leiknes KA, Finset A, Moum T, Sandanger I, Leiknes KA, Finset A, et al. Methodo-logical issues concerning lifetime medically unexplained and medically explainedsymptoms of the Composite International Diagnostic Interview: a prospective 11-year follow-up study. J Psychosom Res 2006 August;61(2):169–79.
[11] Creed FH. Should general psychiatry ignore somatization and hypochondriasis?World Psychiatry 2006;5:146–50.
[12] Wittchen HU. The size and burden of mental disorders in Europe — an ECNP taskforce report. Eur Neuropsychopharmacol 2005;15:S313.
[13] Baumeister H, Harter M. Prevalence of mental disorders based on general popula-tion surveys. Soc Psychiatry Psychiatr Epidemiol 2007;42:537–46.
[14] Salmon P. Conflict, collusion or collaboration in consultations about medicallyunexplained symptoms: the need for a curriculum of medical explanation. PatientEduc Couns 2007;67:246–54.
[15] van der Mast RC. Unexplained physical symptoms: a widespread problem but stilllow-profile in training programs and guidelines. Ned Tijdschr Geneeskd2006;150:686–92.
[16] Czachowski S, Piszczek E, Sowinska A, olde Hartman TC. GPs' challenges in themanagement of patients with medically unexplained symptoms in Poland: afocus group-based study. Fam Pract Sep. 1 2011 [Epub ahead of print].
NFIDENTIA
L
ltiple somatic symptoms, J Psychosom Res (2012), doi:10.1016/

7F.H. Creed et al. / Journal of Psychosomatic Research xxx (2012) xxx–xxx
N
[17] Hauser W, Schmutzer G, Brahler E, Glaesmer H. A cluster within the continuum ofbiopsychosocial distress can be labeled “fibromyalgia syndrome” — evidence froma representative German population survey. J Rheumatol 2009;36:2806–12.
[18] Tanaka Y, Kanazawa M, Fukudo S, Drossman DA. Biopsychosocial model of irritablebowel syndrome. J Neurogastroenterol Motil 2011;17:131–9.
[19] Kroenke K, Spitzer RL, Williams JB. The PHQ-15: validity of a new measure forevaluating the severity of somatic symptoms. Psychosom Med March 2002;64:258–66.
[20] Barsky AJ, Orav EJ, Bates DW. Somatization increases medical utilization and costsindependent of psychiatric and medical comorbidity. Arch Gen Psychiatry August2005;62:903–10.
[21] Lowe B, Spitzer RL, Williams JB, Mussell M, Schellberg D, Kroenke K. Depression,anxiety and somatization in primary care: syndrome overlap and functional im-pairment. Gen Hosp Psychiatry 2008 May;30(3):191–9.
[22] Barsky AJ, Ettner SL, Horsky J, Bates DW. Resource utilization of patients with hy-pochondriacal health anxiety and somatization. Med Care July 2001;39:705–15.
[23] Gillespie NA, Zhu G, Heath AC, Hickie IB, Martin NG. The genetic aetiology of so-matic distress. Psychol Med September 2000;30:1051–61.
[24] Kendler KS, Aggen SH, Knudsen GP, Roysamb E, Neale MC, Reichborn-KjennerudT. The structure of genetic and environmental risk factors for syndromal and sub-syndromal common DSM-IV Axis I and all Axis II disorders. Am J Psychiatry2011;168:29–39.
[25] Kotov R, Ruggero CJ, Krueger RF, Watson D, Yuan Q, Zimmerman M. New dimen-sions in the quantitative classification of mental illness. Arch Gen Psychiatry2011;68:1003–11.
[26] Kato K, Sullivan PF, Evengard B, Pedersen NL. A population-based twin study offunctional somatic syndromes. Psychol Med 2009;39:497–505.
[27] Ball HA, Siribaddana SH, Sumathipala A, Kovas Y, Glozier N, Rijsdijk F, et al.Genetic and environmental contributions to the overlap between psychological,fatigue and somatic symptoms: a twin study in Sri Lanka. Twin Res Hum Genet2011;14:53–63.
[28] Huijbregts KML, van Marwijk HWJ, de Jong FJ, Schreuders B, Beekman ATF, vander Feltz-Cornelis CM. Adverse effects of multiple physical symptoms on thecourse of depressive and anxiety symptoms in primary care. Psychother Psycho-som 2010;79:389–91.
[29] O'Malley PG, Jackson JL, Santoro J, Tomkins G, Balden E, Kroenke K. Antidepres-sant therapy for unexplained symptoms and symptom syndromes. [see com-ment]. [Review] [115 refs]J Fam Pract December 1999;48:980–90.
[30] Creed FH, Kroenke K, Henningsen P, Gudi A, White P. Evidence-based treatment.In: Creed FH, Henningsen P, Fink P, editors. Medically unexplained symptoms,somatisation and bodily distress: developing better clinical services. Cambridge:Cambridge University Press; 2011.
[31] Kroenke K, Swindle R. Cognitive–behavioral therapy for somatization and symp-tom syndromes: a critical review of controlled clinical trials. [Review] [57 refs]Psychother Psychosom July 2000;69:205–15.
[32] Leiknes KA, Finset A, Moum T, Sandanger I, Leiknes KA, Finset A, et al. Course andpredictors of medically unexplained pain symptoms in the general population. JPsychosom Res 2007 February;62(2):119–28.
[33] Henningsen P, Creed F. The genetic, physiological and psychologicalmechanisms un-derlying disabling medically unexplained symptoms and somatisation. J PsychosomRes 2010;68:395–7.
[34] Creed FH, Barsky A, Leiknes KA. Epidemiology: prevalence, causes and conse-quences. In: Creed FH, Henningsen P, Fink P, editors. Medically unexplainedsymptoms, somatisation and bodily distress: developing better clinical services.Cambridge: Cambridge University Press; 2011.
[35] Hotopf M, Mayou R, Wadsworth M, Wessely S, Hotopf M, Mayou R, et al. Child-hood risk factors for adults with medically unexplained symptoms: results froma national birth cohort study. Am J Psychiatry 1999 November;156(11):1796–800.
[36] Hotopf M, Wilson-Jones C, Mayou R, Wadsworth M, Wessely S. Childhood predic-tors of adult medically unexplained hospitalisations. Results from a national birthcohort study. Br J Psychiatry March 2000;176:273–80.
[37] Verhaak PF, Meijer SA, Visser AP, Wolters G. Persistent presentation of medicallyunexplained symptoms in general practice. Fam Pract August 2006;23:414–20.
[38] Gureje O, Simon GE. The natural history of somatization in primary care. PsycholMed May 1999;29:669–76.
[39] Barsky AJ, Peekna HM, Borus JF. Somatic symptom reporting in women and men.[Review] [146 refs]J Gen Intern Med April 2001;16:266–75.
[40] Katon W, Sullivan M, Walker E. Medical symptoms without identified pathology:relationship to psychiatric disorders, childhood and adult trauma, and personalitytraits. Ann Intern Med May 1 2001;134:917–25.
[41] Mullen PE, Martin JL, Anderson JC, Romans SE, Herbison GP. Childhood sexualabuse and mental health in adult life. [see comment]Br J Psychiatry December1993;163:721–32.
[42] Parker G. The parental bonding instrument: psychometric properties reviewed.Psychiatr Dev 1989;7:317–35.
[43] Wilhelm K, Niven H, Parker G, Hadzi-Pavlovic D. The stability of the parentalbonding instrument over a 20-year period. Psychol Med 2005;35:387–93.
[44] Costa PT, McCrae RR. The revised NEO Personality Inventory: professional manual.Psychological Assessment Resources; 1992.
[45] Rosmalen JG, Neeleman J, Gans RO, de Jonge P. The association between neuroti-cism and self-reported common somatic symptoms in a population cohort. J Psy-chosom Res 2007 March;62(3):305–11.
[46] Brugha T, Bebbington P, Tennant C, Hurry J. The list of threatening experiences: asubset of 12 life event categories with considerable long-term contextual threat.Psychol Med February 1985;15:189–94.
DRAFT - CO
Please cite this article as: Creed FH, et al, The epidemiology of muj.jpsychores.2012.01.009
[47] Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta PsychiatrScand 1983;67:361–70.
[48] Spinhoven P, Ormel J, Sloekers PP, Kempen GI, Speckens AE, Van Hemert AM. Avalidation study of the Hospital Anxiety and Depression Scale (HADS) in differentgroups of Dutch subjects. Psychol Med 1997 March;27(2):363–70.
[49] Derogatis LR, Lipman RS, Covi L. The Hopkins Symptom Checklist (HSCL): a self-report symptom inventory. Behav Sci 1974;19:1–15.
[50] Gandek B, Ware JE, Aaranson NK, Apolone G, Bjorner JB, Brazier JE, et al. Cross-validation of item selection and scoring for the SF-12 Health Survey in nine coun-tries: results from the IQOLA Project. International Quality of Life Assessment.J Clin Epidemiol 1998;51:1171–8.
[51] Williams A. Euroqol — a new facility for the measurement of health-relatedquality-of-life. Health Policy 1990;16(3):199–208.
[52] Kooiman CG, Bolk JH, Rooijmans HG, Trijsburg RW. Alexithymia does not predictthe persistence of medically unexplained physical symptoms. Psychosom MedMarch 2004;66:224–32.
[53] Lieb R, Zimmermann P, Friis RH, Hofler M, Tholen S, Wittchen HU. The naturalcourse of DSM-IV somatoform disorders and syndromes among adolescents andyoung adults: a prospective-longitudinal community study. Eur Psychiatry October2002;17:321–31.
[54] Essau CA. Course and outcome of somatoform disorders in non-referred adoles-cents. Psychosomatics November 2007;48:502–9.
[55] Koerber S, Frieser D, Steinbrecher N, Hiller W. Classification characteristics of thePatient Health Questionnaire-15 for screening somatoform disorders in a primarycare setting. J Psychosom Res 2011;71:142–7.
[56] Kisely S, Simon G, Kisely S, Simon G. An international study comparing the effectof medically explained and unexplained somatic symptoms on psychosocial out-come. J Psychosom Res February 2006;60:125–30.
[57] Rief W, Mewes R, Martin A, Glaesmer H, Brähler E. Evaluating new proposals forthe psychiatric classification of patients with multiple somatic symptoms. Psycho-som Med 2011;73:760–8.
[58] Kisely S, Goldberg D, Simon G. A comparison between somatic symptoms withand without clear organic cause: results of an international study. Psychol MedSeptember 1997;27:1011–9.
[59] Aiarzaguena JM, Grandes G, Salazar A, Gaminde I, Sanchez A. The diagnostic chal-lenges presented by patients with medically unexplained symptoms in generalpractice. Scand J Prim Health Care 2008 June;26(2):99–105.
[60] KosinskiM, Zhao SZ, Dedhiya S, Osterhaus JT,Ware JE. Determiningminimally impor-tant changes in generic and disease-specific health-related quality of life question-naires in clinical trials of rheumatoid arthritis. Arthritis Rheum 2000;43:1478–87.
[61] Whynes DK, Tombola G. Responsiveness of the EQ-5D to HADS-identified anxietyand depression. J Eval Clin Pract 2009;15:820–5.
[62] Coteur G, Feagan B, Keininger DL, Kosinski M. Evaluation of the meaningfulnessof health-related quality of life improvements as assessed by the SF-36 and theEQ-5D VAS in patients with active Crohn's disease. Aliment Pharmacol Ther2009;29:1032–41.
[63] Ware JE, Kosinski M. SF-36® Physical and Mental Health Summary Scales: a man-ual for users of version 1. 2nd Edition. Lincoln, RI: QualityMetric, Inc.; 2001. RefType: Serial (Book,Monograph).
[64] Harris AM, Orav EJ, Bates DW, Barsky AJ. Somatization increases disability inde-pendent of comorbidity. J Gen Intern Med 2009;24:155–61.
[65] Katon W, Lin EHB, Kroenke K. The association of depression and anxiety withmedical symptom burden in patients with chronic medical illness. Gen Hosp Psy-chiatry 2007;29:147–55.
[66] Jackson J, Fiddler M, Kapur N, Wells A, Tomenson B, Creed F, et al. Number of bodilysymptoms predicts outcome more accurately than health anxiety in patients at-tending neurology, cardiology, and gastroenterology clinics. J Psychosom Res 2006April;60(4):357–63.
[67] olde Hartman TC, Borghuis MS, Lucassen PL, van de Laar FA, Speckens A, van WeelC. Medically unexplained symptoms, somatisation disorder and hypochondriasis:course and prognosis. A systematic review. J Psychosom Res 2009;66:363–77.
[68] Guthrie E, Barlow J, Fernandes L, Ratcliffe J, Read N, Thompson DG, et al. Changesin tolerance to rectal distension correlate with changes in psychological state inpatients with severe irritable bowel syndrome. Psychosom Med 2004 July;66(4):578–82.
[69] Deary V, Chalder T, Sharpe M, Deary V, Chalder T, Sharpe M. The cognitive beha-vioural model of medically unexplained symptoms: a theoretical and empiricalreview. [Review] [130 refs]Clin Psychol Rev 2007 October;27:781–97.
[70] Kolk AM, Hanewald GJFP, Schagen S, van Wijk CMTG. A symptom perceptionapproach to common physical symptoms. Soc Sci Med 2003;57:2343–54.
[71] Kapur N, Hunt I. Psychosocial and illness related predictors of consultation ratesin primary care — a cohort study. Psychol Med May 2004;34:719–28.
[72] Frostholm L, Fink P, Christensen KS, Toft T, Oernboel E, Olesen F, et al. The pa-tients' illness perceptions and the use of primary health care. Psychosom Med2005;67(6):997–1005.
[73] Frostholm L, Oernboel E, Christensen KS, Toft T, Olesen F, Weinman J, et al. Do ill-ness perceptions predict health outcomes in primary care patients? A 2-year fol-low-up study. J Psychosom Res 2007 February;62(2):129–38.
[74] Hanel G, Henningsen P, HerzogW, Sauer N, Schaefert R, Szecenyi J, et al. Depression,anxiety, and somatoformdisorders: vague or distinct categories in primary care? Re-sults from a large cross-sectional study. J Psychosom Res 2009;67:189–97.
[75] Helzer JE, Kraemer HC, Krueger RF. The feasibility and need for dimensional psy-chiatric diagnoses. Psychol Med 2006;36:1671–80.
[76] Kroenke K. Efficacy of treatment for somatoform disorders: a review of random-ized controlled trials. [Review] [64 refs]Psychosom Med December 2007;69:881–8.
FIDENTIA
L
ltiple somatic symptoms, J Psychosom Res (2012), doi:10.1016/

DSM‐5 Field Trials Results for the
Somatic Symptom Disorders Work Group
This report contains the test‐retest reliability of the following DSM‐5 Diagnostic Criteria relevant to the Somatic Symptom Disorders Work Group:
Complex Somatic Symptom Disorder
Adult Test Sites included in this Report DSM‐5 Diagnostic Criteria Tested Mayo
Bipolar I Disorder
Mild Neurocognitive Disorder
Complex Somatic Symptom Disorder Major Neurocognitive Disorder
Bipolar II Disorder
DRAFT - CONFID
ENTIAL

Table of Content
Section I: Summary Tables of the Test‐Retest Reliability of the Categorical DSM‐5 and Associated
Dimensional Ratings Relevant to the Somatic Symptom Disorders Work Group. Table A.DSM‐5 Diagnostic Criteria Relevant to the Somatic Symptom Disorders WG……………………Section I: 1 Table B. Associated Dimensional Ratings Relevant to the Somatic Symptom Disorders WG….….….Section I: 2
Section II: Site‐Specific Results from the DSM‐5 Field Trial sites that tested DSM‐5 Diagnostic
Criteria Relevant to the Somatic Symptom Disorders WG – Mayo Clinic …………………………………………………………………………………………………………………………Section II: A1‐12
Section III: Forest plot of the Intraclass Kappas and associated 95% ConfidenceIntervals for the
DSM‐5 Diagnostic criteria tested in: Adult samples……………………………………………………………………….……………………………….………..……Section III: 1
i
DRAFT - CONFID
ENTIAL

Section I: Summary Tables
A. Summary Table of theTest‐Retest Reliability of DSM‐5 Diagnostic Criteria relevant to the Somatic Symptom Disorders Work Group (categorical diagnoses) – Intraclass Kappas and 95% confidence intervals for a stratified sample.
B. Summary Table of the Test‐Retest Reliability of Dimensional Ratings relevant to the Somatic Symptom Disorders Work Group – Intraclass Correlation Coefficient (and Spearman rank correlation non‐parametric equivalent) and 95% confidence intervals for a stratified sample.
ii
DRAFT - CONFID
ENTIAL

Section I: 1
Table A. Test-Retest Reliability of DSM-5 Diagnostic Criteria relevant to the Somatic Symptom Disorders Work Group – Intraclass Kappas and 95% confidence intervals for a stratified sample.
DSM-5 Diagnostic Criteria Site Tested N Sample weight
DSM-5 Prevalence
Intraclass Kappa
95% Confidence Interval Interpretation
Complex Somatic Symptom Disorder Mayo 36 0.100 0.057 0.476 0.206, 0.695 Moderate
Revised (02/18/12) - Somatic Symptom Disorder (combination of CSSD and SSSD as recommended by WG and SRC)
Mayo 36 0.100 0.081 0.600 0.370, 0.779 Good
DRAFT - CONFID
ENTIAL

Section I: 2
Table B.Test‐Retest Reliability of Dimensional Ratings relevant to the Somatic Symptom Disorders Work Group– Intraclass Correlation Coefficient (and Spearman rank correlation non‐parametric equivalent) and 95% confidence intervals for a stratified sample.
Dimensional Rating Site Tested N
Intraclass CorrelationCoefficient
(Spearman Rank) 95% Confidence
Interval Interpretation Clinician‐Rated:
Somatic Symptom – Global Mayo 181 0.483 (0.657) 0.361, 0.588 Acceptable Somatic Symptom Cognition Score Mayo 122 0.680 (0.806) 0.571, 0.766 Good
Patient‐Rated:
PHQ‐Somatic Symptom Scale Mayo 181 0.749 (0.775) 0.677, 0.807 Good
DRAFT - CONFID
ENTIAL

iii
Section II:
Site‐Specific Results from the Mayo Clinic DSM‐5 Field Trial sites –
Mayo Clinic (Mayo) …….………………………………………………………………….…………………………………Section II: A1‐11
DRAFT - CONFID
ENTIAL

Mayo Preliminary Analysis 1/17/2012
A. Preliminary Results of the DSM‐5 Field Trials at the Mayo Clinic site
The preliminary results presented in this document were derived from the Mayo Clinic (Mayo), where consecutive patients age 18 and older entering the Integrated Mood Clinic/Unit and the Behavioral Medicine Program for their routine clinical care between January 10, 2011 ‐ October 31, 2011, were screened for eligibility for the DSM‐5 Field Trials at the site. The final study sample of patients who were eligible, consented to the study, and who completed visit 1 was 210, ranging in age from 19‐90. The DSM‐5 Field Trial at the Mayo Clinic was overseen by Drs. Mark Frye, Jeffrey Staab, and Glenn Smith and their research team. Dr. Frye is a psychiatrist and is the Director of the Mayo Integrated Mood Clinic and Research Program. Dr. Staab is Associate Professor of Psychiatry and Director of the Behavioral Medicine Program in the Department of Psychology and Psychiatry at Mayo Clinic, Rochester, MN. Dr. Glenn Smith is a Professor of Psychology, co‐Chair of the Division of Outpatient Consultation and Director of Education Core of the Mayo Alzheimer’s Disease Research Center.
DSM‐5 diagnostic criteria tested at Mayo included:
Bipolar I Disorder Mild Neurocognitive Disorder Complex Somatic Symptom Disorder Major Neurocognitive Disorder Bipolar II Disorder
In order to assess the test‐retest reliability and obtain Intraclass Kappa statistics for a stratified sample, a comparison group of patients with “Other” DSM‐IV diagnoses other the disorders of interest at the site were sampled. Table A. Criteria Defining Each Stratum (information is based on what is known about the patient before DSM‐5 criteria is applied). Stratum Criteria Defining Each StratumBipolar I Disorder DSM‐IV diagnosis of Bipolar I Disorder?
Mild Neurocognitive Disorder
Is there evidence of Mild Cognitive Impairment, cognitive complaints, or memory complaints (but not a diagnosis of Dementia such as Dementia, Dementia NOS, Alzheimer’s Disease, Vascular Dementia, Lewy Body Dementia, Parkinson’s Dementia, etc)?
Complex Somatic Symptom Disorder
DSM‐IV diagnosis of Somatization Disorder?DSM‐IV diagnosis of Hypochondriasis? DSM‐IV diagnosis of Pain Disorder Associated With Psychological Factors? DSM‐IV diagnosis of Pain Disorder Associated With Psychological Factors and a General Medical Condition? DSM‐IV diagnosis of Undifferentiated Somatoform Disorder?
Major Neurocognitive Disorder
Is there evidence or a history of ANY dementia disorder (e.g., Dementia of Alzheimer's Disease Type, Vascular Dementia, Dementia Due to General Medical Condition, Dementia Due to Multiple Etiologies, or Dementia Not Otherwise Specified) or Amnestic Disorder?
Bipolar II Disorder DSM‐IV diagnosis of Bipolar II Disorder?
Other Diagnosis Is the patient currently symptomatic for any DSM‐IV disorder(s) not including any of the disorders/conditions listed above?
Section II: A ‐ 1
DRAFT - CONFID
ENTIAL

Mayo Preliminary Analysis 1/17/2012
To be eligible for the study, patients qualifying for each stratum had to be:
I. Currently symptomatic, and II. Able to read and communicate in English.
Patient Sampling/Sampling Frame: In the Mayo DSM‐5 field trial site, all clinicians as well as the intake worker at the clinics involved in the study were allowed to complete the Patient Recruitment and Screening Forms on patients seen during the study period. Each patient was then seen by two other participating clinicians who had never been involved in the patient’s previous assessment or care (i.e., new to the patient). Therefore, the target population refers to the population of patients seen in the general clinics by the site clinicians in their routine practice during the recruitment period of the DSM‐5 Field Trial (i.e., January 10, 2011 ‐ October 31, 2011).
Section II: A ‐ 2
DRAFT - CONFID
ENTIAL

Mayo Preliminary Analysis 1/17/2012
A. Basic Demographic Information on Screening Information (n=Number Enrolled and Completed Visit 1)
Table 1. Patient demographic characteristics in Mayo (weighted; n=210). n (%) Mean Age (SD, 25th, 50th, 75th percentile )
51.8 (7.0, 40, 51, 63)
Sex (Male) 32.9% (n=72) Ethnic Origin (i.e., Of Hispanic or Latino origin?) Of Hispanic or Latino origin* 2.0% (n=3)
Married/ Cohabiting
63.8% (n=143)
Race/ Ethnicity White/ Caucasian 95.1% (n=201) Black, African descent 0.9 % (n=2) Other
4.0% (n=7)
Level of Education Less than high school 2.2% (n=6) Completed high school 14.8% (n=31) Greater than high school 82.4% (n=172) Other 0.7% (n=1)
*Of the 3 patients who were of Hispanic or Latino origin, 1 were of Mexican origin and 2 of “another Hispanic or Latino origin”
Section II: A ‐ 3
DRAFT - CONFID
ENTIAL

Mayo Preliminary Analysis 1/17/2012
Table 2. Mayo Clinician characteristics (n=22). % (n) Discipline1
Board Certified Psychiatrist 55.0% (n=11) Psychiatrists in training (PGY2‐5) 15.0% (n=3) Lic. Dr. Level Psychologist 5.0% (n=1) Supervised practice 25.0% (n=5) Lic. Counselors (Masters‐level) ‐ Lic. Clinical Social Worker ‐ Lic. Advanced Mental Health Nurse ‐
Mean Years in Practice (SD)2 13.1 (9.1) Mean Age (SD)3 45.9 (8.8) Sex (Male) 63.6% (n=14) Race/ Ethnicity4 White/ Caucasian 84.6% (n=11) Black ‐ Other 15.4% (n=2)
1 2 missing information 2 6 missing information 3 7 missing information 4 9 missing information
Section II: A ‐ 4
DRAFT - CONFID
ENTIAL

Mayo Preliminary Analysis 1/17/2012
Section II: A - 5
B. Test-retest Reliability Table 3. The test-retest reliability of the categorical diagnosis of DSM-5 Diagnosis tested at the Mayo site (Intraclass Kappa for a stratified sample).
Target DSM-5 Diagnostic Criteria Intraclass KAPPA€
95% Confidence Interval± Interpretation†
Bipolar I Disorder 0.730 0.569, 0.849 Good Mild Neurocognitive Disorder 0.759 0.604, 0.884 Good Complex Somatic Symptom Disorder 0.476 0.206, 0.695 Moderate Revised (02/18/12) - Somatic Symptom Disorder (combination of CSSD and SSSD as recommended by WG and SRC)
0.600 0.370, 0.779 Good
Major Neurocognitive Disorder 0.750 0.593, 0.898 Good Bipolar II Disorder 0.397 0.088, 0.645 Fair Other diagnosis 0.699 0.590, 0.793 Good
€Estimated for a stratified sample ± Bootstrap CI †Strength of agreement for the kappa coefficient was interpreted as follows: <.20=poor, .20–.40=fair, .40–.60=moderate, .60–.80=good, and .80–1=almost perfect. Estimates in which the confidence interval overlap 0 is un-interpretable due to insufficient sample size. Kraemer HC, Kupfer DJ, Clarke DE, Narrow WE, Regier DA. DSM-5: How Reliable is Reliable Enough? American Journal of Psychiatry. 2012; 169:13-15. Table 3 Description: Column 1: DSM-5 Diagnostic Criteria: The “Other Diagnosis” category represents DSM-5 diagnoses other than the Target Diagnoses. Column 2: The Intraclass Kappa coefficient for a stratified sample for each of the DSM-5 categorical diagnoses targeted at this site with suggested criteria for evaluation of diagnostic reliability listed in footnote. Column 3: The 95% two-tailed confidence interval for the population Intraclass Kappa, indicating how precisely the kappa is measured with the sample selected. Note that if zero is not within this interval, the kappa is statistically significant at the 5% two-tailed level. Column 4: Interpretation of the DSM-5 Intraclass Kappa with suggested standards described in the footnote.
DRAFT - CONFID
ENTIAL
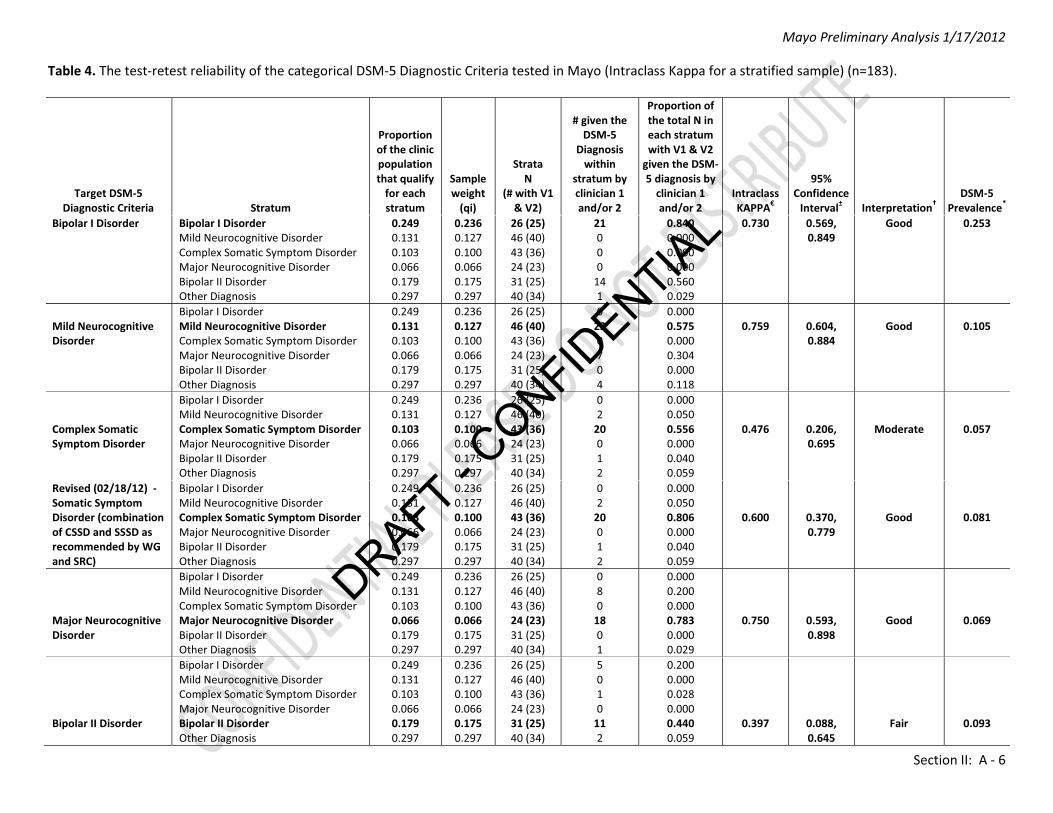
Mayo Preliminary Analysis 1/17/2012
Section II: A - 6
Table 4. The test-retest reliability of the categorical DSM-5 Diagnostic Criteria tested in Mayo (Intraclass Kappa for a stratified sample) (n=183).
Target DSM-5 Diagnostic Criteria Stratum
Proportion of the clinic population that qualify
for each stratum
Sample weight
(qi)
Strata N
(# with V1 & V2)
# given the DSM-5
Diagnosis within
stratum by clinician 1 and/or 2
Proportion of the total N in each stratum with V1 & V2
given the DSM-5 diagnosis by
clinician 1 and/or 2
Intraclass KAPPA€
95% Confidence
Interval± Interpretation† DSM-5
Prevalence* Bipolar I Disorder Bipolar I Disorder
Mild Neurocognitive Disorder Complex Somatic Symptom Disorder Major Neurocognitive Disorder Bipolar II Disorder Other Diagnosis
0.249 0.131 0.103 0.066 0.179 0.297
0.236 0.127 0.100 0.066 0.175 0.297
26 (25) 46 (40) 43 (36) 24 (23) 31 (25) 40 (34)
21 0 0 0
14 1
0.840 0.000 0.000 0.000 0.560 0.029
0.730 0.569, 0.849
Good 0.253
Mild Neurocognitive Disorder
Bipolar I Disorder Mild Neurocognitive Disorder Complex Somatic Symptom Disorder Major Neurocognitive Disorder Bipolar II Disorder Other Diagnosis
0.249 0.131 0.103 0.066 0.179 0.297
0.236 0.127 0.100 0.066 0.175 0.297
26 (25) 46 (40) 43 (36) 24 (23) 31 (25) 40 (34)
0 23 0 7 0 4
0.000 0.575 0.000 0.304 0.000 0.118
0.759
0.604, 0.884
Good
0.105
Complex Somatic Symptom Disorder
Bipolar I Disorder Mild Neurocognitive Disorder Complex Somatic Symptom Disorder Major Neurocognitive Disorder Bipolar II Disorder Other Diagnosis
0.249 0.131 0.103 0.066 0.179 0.297
0.236 0.127 0.100 0.066 0.175 0.297
26 (25) 46 (40) 43 (36) 24 (23) 31 (25) 40 (34)
0 2
20 0 1 2
0.000 0.050 0.556 0.000 0.040 0.059
0.476
0.206, 0.695
Moderate
0.057
Revised (02/18/12) - Somatic Symptom Disorder (combination of CSSD and SSSD as recommended by WG and SRC)
Bipolar I Disorder Mild Neurocognitive Disorder Complex Somatic Symptom Disorder Major Neurocognitive Disorder Bipolar II Disorder Other Diagnosis
0.249 0.131 0.103 0.066 0.179 0.297
0.236 0.127 0.100 0.066 0.175 0.297
26 (25) 46 (40) 43 (36) 24 (23) 31 (25) 40 (34)
0 2
20 0 1 2
0.000 0.050 0.806 0.000 0.040 0.059
0.600
0.370, 0.779
Good
0.081
Major Neurocognitive Disorder
Bipolar I Disorder Mild Neurocognitive Disorder Complex Somatic Symptom Disorder Major Neurocognitive Disorder Bipolar II Disorder Other Diagnosis
0.249 0.131 0.103 0.066 0.179 0.297
0.236 0.127 0.100 0.066 0.175 0.297
26 (25) 46 (40) 43 (36) 24 (23) 31 (25) 40 (34)
0 8 0
18 0 1
0.000 0.200 0.000 0.783 0.000 0.029
0.750
0.593, 0.898
Good
0.069
Bipolar II Disorder
Bipolar I Disorder Mild Neurocognitive Disorder Complex Somatic Symptom Disorder Major Neurocognitive Disorder Bipolar II Disorder Other Diagnosis
0.249 0.131 0.103 0.066 0.179 0.297
0.236 0.127 0.100 0.066 0.175 0.297
26 (25) 46 (40) 43 (36) 24 (23) 31 (25) 40 (34)
5 0 1 0
11 2
0.200 0.000 0.028 0.000 0.440 0.059
0.397
0.088, 0.645
Fair
0.093
DRAFT - CONFID
ENTIAL

Mayo Preliminary Analysis 1/17/2012
Section II: A - 7
Other Diagnosis
Bipolar I Disorder Mild Neurocognitive Disorder Complex Somatic Symptom Disorder Major Neurocognitive Disorder Bipolar II Disorder Other Diagnosis
0.249 0.131 0.103 0.066 0.179 0.297
0.236 0.127 0.100 0.066 0.175 0.297
26 (25) 46 (40) 43 (36) 24 (23) 31 (25) 40 (34)
5 18 29 1
11 27
0.200 0.450 0.806 0.043 0.440 0.794
0.699
0.590, 0.793
Good
0.427 €Estimated for a stratified sample ±Bootstrap Confidence Interval †Strength of agreement for the kappa coefficient was interpreted as follows: <.20=poor, .20–.40=fair, .40–.60=moderate, .60–.80=good, and .80–1=almost perfect. Estimates with confidence intervals that overlap zero are considered un-interpretable due to insufficient sample size. Kraemer HC, Kupfer DJ, Clarke DE, Narrow WE, Regier DA. DSM-5: How Reliable is Reliable Enough? American Journal of Psychiatry. 2012; 169:13-15. *DSM-5 Prevalence = Sum of (qi*proportion of concordant pairs) across the stratum + 0.5*Sum of (qi*proportion of discordant pairs) across the stratum
Table 4 Description:
Column 1: DSM-5 Target Diagnostic Criteria: The “Other Diagnosis” category represents DSM-5 diagnoses other than the Target Diagnoses.
Column 2: Patients are enrolled into the study in strata, usually defined by DSM-IV criteria, with a high probability of having a DSM-5 diagnosis (see page 1).
Column 3: The percentage of the clinic population that qualify for each stratum. In most cases this estimates the DSM-IV prevalence of that diagnosis. The total of these percentages may exceed 100% because of comorbidity of the screening diagnoses.
Column 4: Sample weights (qi). Proportion eligible to be sampled from each stratum as defined on page 1. If a patient was found to be eligible for two or more strata, s/he was assigned to the rarest stratum.
Column 5: Number Recruited into each stratum. The numbers in parentheses represent those who completed both Visits 1 and 2 —those on whom the test-retest reliabilities are based.
Column 6: Number of those in each stratum for whom criteria were met, per clinician 1 and/or 2, for the DSM-5 diagnostic criteria being tested as indicated in Column 1.
Column 7: Proportion of those in each stratum with completed V1 and V2 who were given the DSM-5 diagnosis indicated in Column 1, as determined by clinician 1 and/or clinician 2. It would generally be expected that for each target diagnostic criteria (Column 1), the DSM-IV stratum corresponding to the target diagnostic criteria will have the highest proportion of the diagnosis based on DSM-5 diagnostic criteria (bolded values). The closer the correspondence between the DSM-IV and DSM-5 diagnoses, the greater the discrepancy between the bolded prevalence and the other prevalence estimates in that row.
Column 8: The Intraclass Kappa for a stratified sample for each of the DSM-5 categorical diagnostic criteria targeted at this site. Suggested criteria for evaluation of diagnostic reliability are listed in the footnote.
DRAFT - CONFID
ENTIAL

Mayo Preliminary Analysis 1/17/2012
Section II: A - 8
Column 9: The 95% two-tailed confidence interval for the population Intraclass Kappa, indicating how precisely the kappa is measured with the sample selected. Note that if zero is not within this interval, the kappa is statistically significant at the 5% two-tailed level.
Column 10: Interpretation of the DSM-5 kappa found by suggested standards in the footnote. Column 11: The estimated DSM-5 prevalence in the sample that might be compared with the DSM-IV prevalence Column 3. Calculated as Sum of (qi*proportion of concordant pairs) across the stratum + 0.5*Sum of (qi*proportion of discordant pairs) across the stratum.
DRAFT - CONFID
ENTIAL

Mayo Preliminary Analysis 1/17/2012
Section II: A ‐ 9
Table 5. The test‐retest reliability of clinician’s dimensional ratings (Intraclass Correlation Coefficient for a stratified sample) (n=183). Test‐Retest Reliability Summary Statistics
Clinician dimensional rating of: # pairs
responded
Intraclass Correlation Coefficient
(ICC)
95% Confidence Interval Interpretation Mean (SD) €
25th, 50th, and 75th quartiles€
Possible Range
Anxious Distress (Goldberg)* 88 ‐ ‐ ‐ 0.245 (0.273) 0.0, 0.0, 0.0 0‐4 Cognitive Problems 176 0.573 0.463, 0.665 Acceptable 0.261 (0.252) 0.0, 0.0, 0.0 0‐4 Mood 183 0.299 0.159, 0.426 Poor 0.983 (0.476) 0.0, 0.0, 2.0 0‐4 Somatic Symptom 181 0.483 0.361, 0.588 Acceptable 0.232 (0.298) 0.0, 0.0, 0.0 0‐4 Somatic Symptom Cognition Score 122 0.680 0.571, 0.766 Good 1.134 (1.078) 0.0, 0.0, 0.0 0‐12 €Estimated for a stratified sample *Reliability estimate for Anxious Distress not reported due to over 25% missing data Table 5: The n in the title is the number of test‐retest evaluations in the study. This table illustrates the test‐retest reliability of the clinician‐rated dimensional measures associated with the target DSM‐5 diagnostic criteria being tested at the study site. Diagnosticians were instructed to fill out these measures for any patient with any symptoms suggesting the presence of the disorder, regardless of whether the diagnostic criteria were met. Therefore, if a clinician did not go down a particular diagnostic path in the Research Electronic Data Capture (REDCap) system and hence did not complete the dimensional measures associated with the target DSM‐5 diagnostic criteria, the absence of a recorded measure is interpreted as 0. Column 1: Name of clinician‐rated dimensional measures associated with the DSM‐5 diagnostic criteria tested at the study site. Column 2: The number of pairs with completed data on the measures. Column 3: The Intraclass Correlation Coefficient for a stratified sample, the measure of reliability of a dimensional measure. Column 4: The 95% confidence interval for the population Intraclass Correlation Coefficient. If zero is not inside the interval, the Intraclass Correlation Coefficient is statistically significant at the two‐tailed 5% level. Column 5: Interpretation according to suggested standards of evaluation. The criteria for evaluation are higher than for the Intraclass Kappa, since it is generally expected that test‐retest reliability will be improved with the use of a dimensional measure. Kraemer et al. propose ICC of 0.6‐0.8 should be the goal for DSM‐5 dimensional measure and 0.4‐0.6 as acceptable. Kraemer HC, Kupfer DJ, Clarke DE, Narrow WE, Regier DA. DSM‐5: How Reliable is Reliable Enough? American Journal of Psychiatry. 2012; 169:13‐15. Column 6‐8: The mean, standard deviation, the 25th, 50th, and 75th percentiles and possible range.
DRAFT - CONFID
ENTIAL

Mayo Preliminary Analysis 1/17/2012
Section II: A ‐ 10
Table 6. The test‐retest reliability of patient’s dimensional ratings (Intraclass Correlation Coefficient for a stratified sample) (n=183).
Test‐Retest Reliability Summary Statistics
Patient’s Dimensional Ratings of: # pairs
responded
Intraclass Correlation Coefficient
(ICC)
95% Confidence Interval Interpretation Mean (SD) €
25th, 50th, and 75th quartiles€
Possible Range
Altman Self‐Rated Mania Scale 161 0.497 0.370, 0.606 Acceptable 1.579 (1.371) 0.0, 0.0, 1.0 0‐20 Depression (PHQ‐9) 143 0.763 0.684, 0.825 Good 6.076 (2.813) 0.0, 0.0, 11.0 0‐27 Somatic Symptoms (PHQ) 181 0.749 0.677, 0.807 Good 5.581 (2.972) 0.0, 0.0, 12.0 0‐32 €Estimated for a stratified sample Table 6: The n in the title is the number of test‐retest evaluations in the study. This table illustrates the test‐retest reliability of the patient‐rated dimensional measures associated with the target DSM‐5 diagnostic criteria being tested at the study site. Diagnosticians were instructed to either administer to the patient or have the patient complete these measures if the patient had any symptoms suggesting the presence of the disorder regardless of whether the diagnostic criteria were met. Therefore, if a clinician did not go down a particular diagnostic path in the Research Electronic Data Capture (REDCap) system and hence did not complete the dimensional measures associated with the diagnosis, the absence of a recorded measure is interpreted as 0. Column 1: Name of patient‐rated dimensional measures associated with the DSM‐5 diagnostic criteria tested at the study site. Column 2: The number of pairs with completed data on the measures. Column 3: The Intraclass Correlation Coefficient for a stratified sample, the measure of reliability of a dimensional measure. Column 4: The 95% confidence interval for the population Intraclass Correlation Coefficient. If zero is not inside the interval, the Intraclass Correlation Coefficient is statistically significant at the two‐tailed 5% level. Column 5: Interpretation according to suggested standards of evaluation. The criteria for evaluation are higher than for the Intraclass Kappa, since it is generally expected that test‐retest reliability will be improved with the use of a dimensional measure. Kraemer et al. propose ICC of 0.6‐0.8 should be the goal for DSM‐5 dimensional measure and 0.4‐0.6 as acceptable. Kraemer HC, Kupfer DJ, Clarke DE, Narrow WE, Regier DA. DSM‐5: How Reliable is Reliable Enough? American Journal of Psychiatry. 2012; 169:13‐15. Column 6‐8: The mean, standard deviation, the 25th, 50th, and 75th percentiles and possible range.
DRAFT - CONFID
ENTIAL

Mayo Preliminary Analysis 1/17/2012
Appendix. Diagnostic Boundary Matrix The Diagnostic Boundary Matrix is presented to identify common confusions between two target diagnostic criteria, when one of the two has an Intraclass Kappa of less than 0.40. The rows represent a randomly chosen one of the two clinicians’ diagnosis, and the columns represent the other’s. In each cell is the proportion of patients in which Clinician 1 chose the column diagnosis and Clinician 2 the row diagnosis. When the target diagnostic criteria set has high reliability, the highest proportion in the row and column corresponding to that diagnosis is on the diagonal. If the highest proportion is not on the diagonal, which often happens when the kappa is low, the highest proportion in that row or column indicates where the most likely confusion is, either with the other diagnosis, with absence of both or with comorbidity of the two. This might be of help in considering how to strengthen diagnoses with low Intraclass Kappas. Below for Bipolar II Disorder (BP II), the confusion is between BP I and BP II as indicated by the highest value in row 3 being in the BPI or second column (i.e., r=0.061). The Intraclass Kappa and estimated prevalence of each of the two target diagnoses is also presented. Appendix. Diagnostic Boundary Matrix for Bipolar I Disorder (BP I) and Bipolar II Disorder (BP II). Clinician 1 Neither BP I BP II Both
Clinician 2
Neither 0.612 0.009 0.019 0.000
BP I 0.033 0.202 0.000 0.000
BP II 0.023 0.061 0.042 0.000
Both 0.000 0.000 0.000 0.000
KappaBP I = 0.730 (0.569, 0.849) PrevalenceBP I= 0.253 KappaBP II = 0.397 (0.088, 0.645) PrevalenceBP II= 0.093
Section II: A ‐ 11
DRAFT - CONFID
ENTIAL

iv
Section III:
Forest Plots of Intraclass Kappas and 95% Confidence Intervals for any DSM-5 Diagnostic Criteria
Tested in Multiple Adult Sites
DRAFT - CONFID
ENTIAL

Section III: 1
Figure 1: Forest plot of the test-retest reliability coefficients (i.e., Intraclass Kappas [ICK]) for Bipolar I Disorder (BP-I), Borderline Personality Disorder (PD), Major Depressive Disorder (MDD), Mixed Anxiety Depression (MADD), Mild Traumatic Brain Injury (TBI), Major and Mild Neurocognitive Disorders (NCDs), Posttraumatic Stress Disorder (PTSD) and Schizophrenia as tested across the seven adult sites and the pooled reliability coefficient for each disorder [pooled ICK]. Note: For each diagnostic criteria, attention should be paid to the black line that indicates the pooled ICK and its 95% CI taking into account the caution in interpreting those flagged by an asterisk (
*).
*If the individual Intraclass Kappas (ICKs) for a stratified sample, for all sites testing the diagnostic criteria set, and their 95% CI do not overlap, the pooled ICK need to be interpreted with caution. †Strength of agreement for the intraclass kappa coefficient was interpreted as follows: <.20=poor, .20–.40=fair, .40–.60=moderate, .60–.80=good, and .80–1=almost perfect. Estimates with 95% CIs that overlap
zero are considered un-interpretable due to insufficient sample size. Kraemer HC, Kupfer DJ, Clarke DE, Narrow WE, Regier DA. DSM-5: How Reliable is Reliable Enough? American Journal of Psychiatry. 2012;
169:13-15.
-0.3 -0.2 -0.1 0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
Schizophrenia
PTSD
Mild NCD*
Major NCD
Mild TBI
MADD
MDD
Borderline PD*
BP-I*
LEGEND: CAMH Dallas VA Houston VA/Menninger Mayo
Penn UCLA UTSA Pooled ICK
DRAFT - CONFID
ENTIAL