Embed Size (px)
Citation preview
Cells divide twice First step is essentially mitosis but then they
divide again First time there is replication so you end up with
a normal number of chromosomes after division – you have 46 pairs which is reduced to 23 pairs
From the second division there are now half the number of chromosomes -23 left
Things can go wrong with either step – termed meiosis I and II
The important bit of meiosis
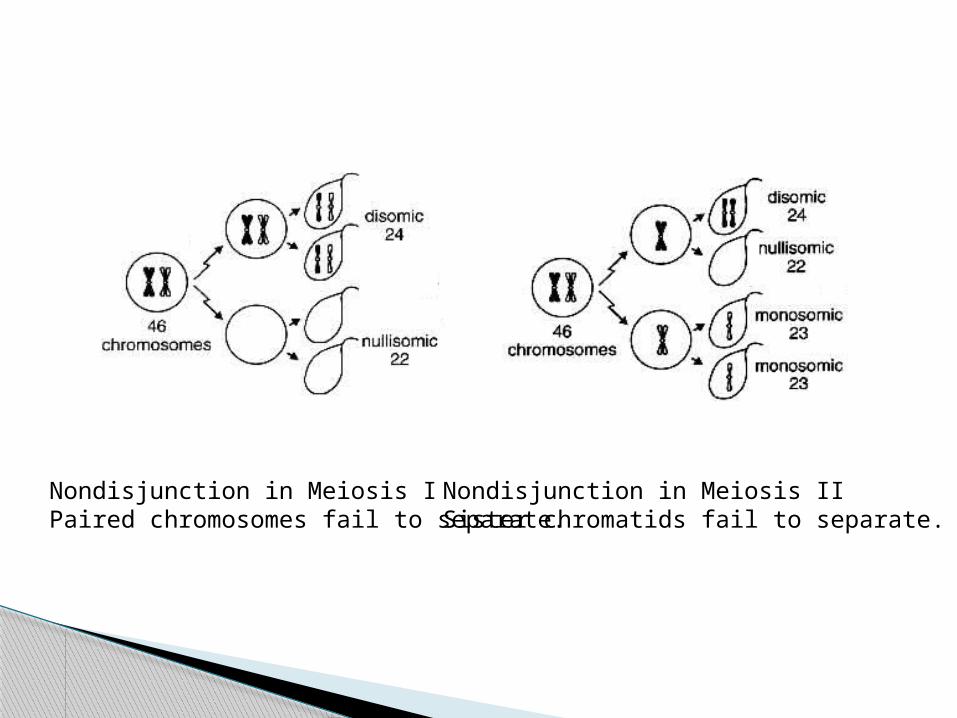
Nondisjunction in Meiosis IPaired chromosomes fail to separate.
Nondisjunction in Meiosis IISister chromatids fail to separate.
Monosomy?◦ Turner’s (XO)
Autosomal Trisomy?◦ Down’s (Trisomy 21)◦ Chromosome 21 has a small amount of info on it
thus this is compatible with life (also 13,18)
Sex chromosome trisomy Klinefelters (XXY)
Other genetic abnormalities?
◦ Translocation (Chronic Myeloid Leukemia) Chromosomes mingle when the meet which can
cause errors◦ Triplet repeats (Huntington’s)
Excess repeats create too much protein e.g. glutamine
◦ Substitution (Sickle cell) AT subsitution results in abnormal cells
◦ Insertion (Muscular Dystrophy)
What are the 5 pedigrees?◦ Autosomal Dominant◦ Autosomal Recessive◦ X-linked Dominant◦ X-linked Recessive◦ Y-linked
Look if both sexes equally effected◦ If no… look if it skips a generation
If it skips a generation, it’s X linked recessive If not, it’s X linked dominant (affected males don’t
have affected sons)
If yes… its autosomal◦ Look at chances of getting the disease from a
diseased parent◦ ½ = dominant◦ ¼ = recessive
Deciphering pedigrees
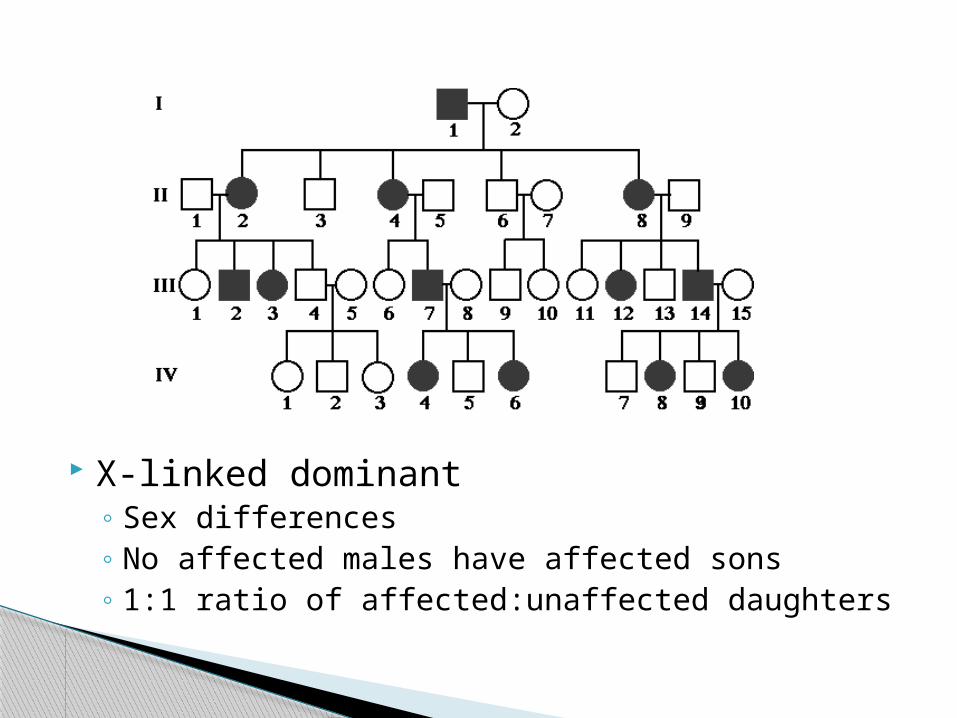
X-linked dominant◦ Sex differences◦ No affected males have affected sons◦ 1:1 ratio of affected:unaffected daughters
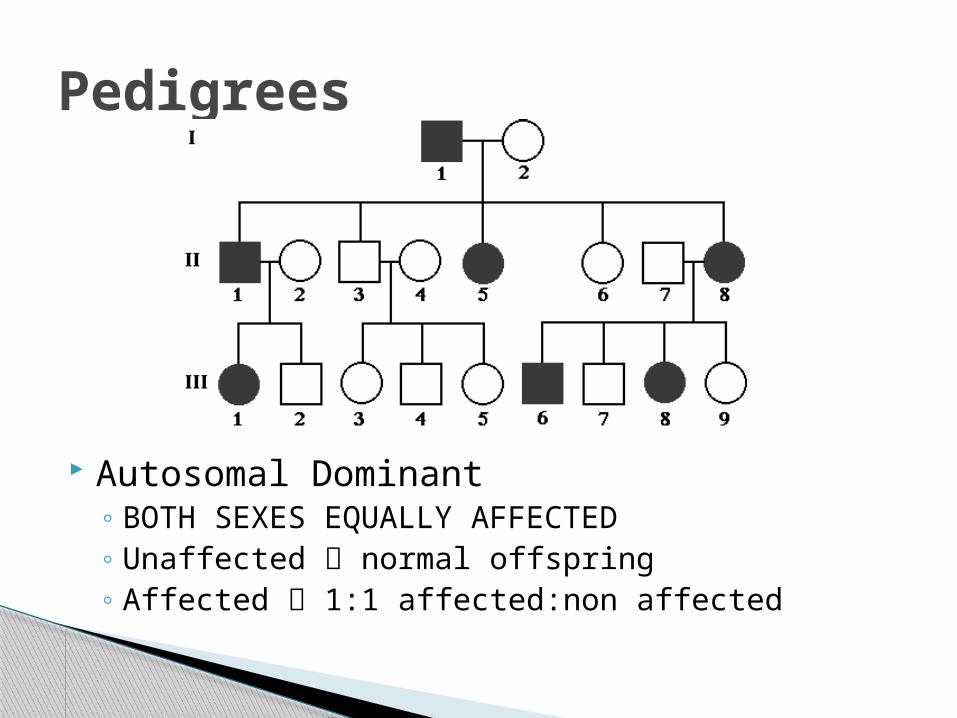
Autosomal Dominant◦ BOTH SEXES EQUALLY AFFECTED◦ Unaffected normal offspring◦ Affected 1:1 affected:non affected
Pedigrees
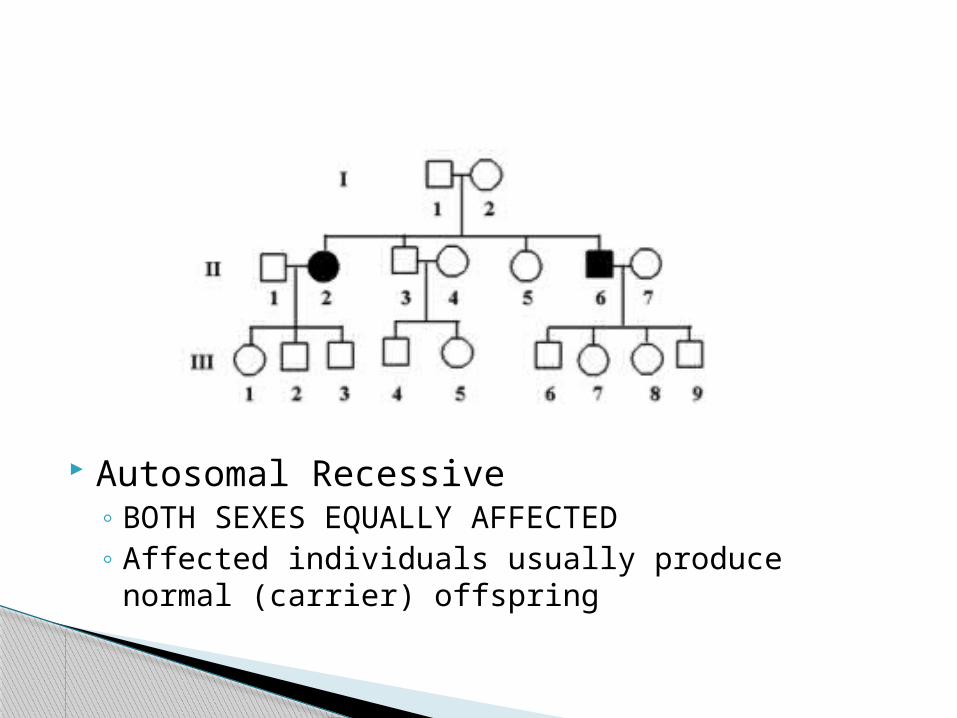
Autosomal Recessive◦ BOTH SEXES EQUALLY AFFECTED◦ Affected individuals usually produce normal
(carrier) offspring
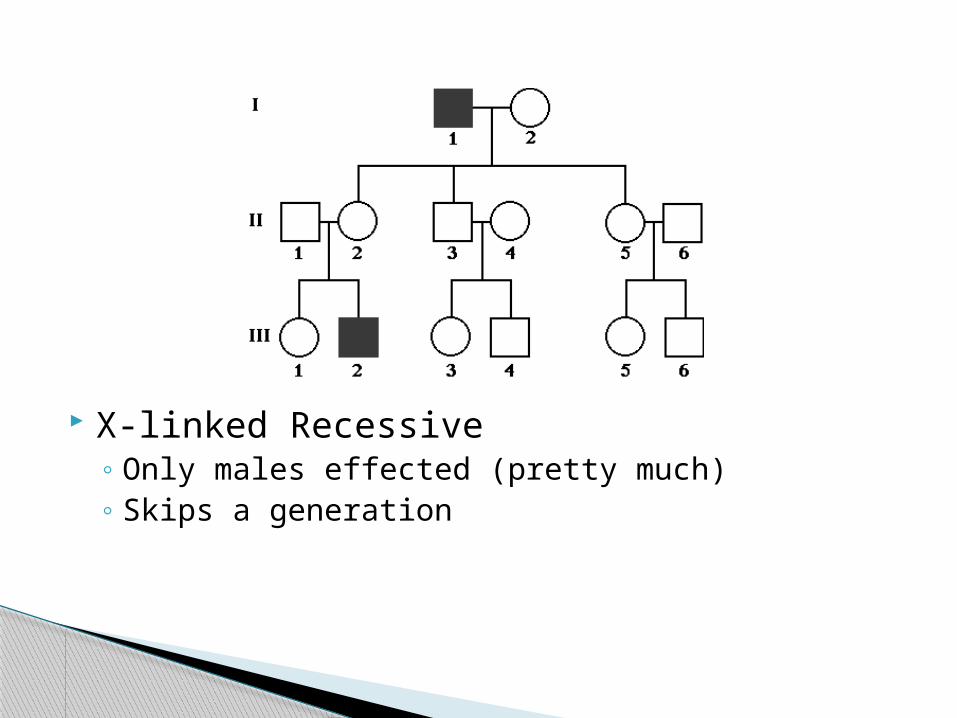
X-linked Recessive◦ Only males effected (pretty much)◦ Skips a generation
Y-linked
Exclusively affects males Effected males ALWAYS produce effected
males
(Should probably know two)◦ Mosaicism◦ Late onset◦ Incomplete penetrance◦ Mitochondrial inheritance
Complications
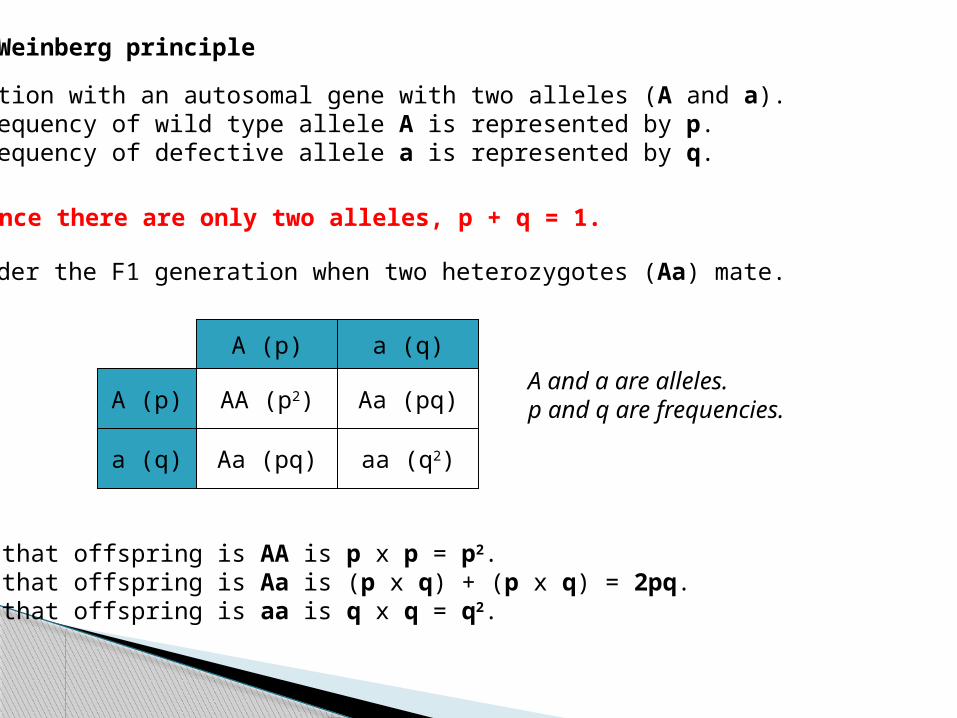
Hardy-Weinberg principle
Population with an autosomal gene with two alleles (A and a). Frequency of wild type allele A is represented by p. Frequency of defective allele a is represented by q.
AA (p2)A (p)
a (q) Aa (pq)
A (p) a (q)
Aa (pq)
aa (q2)
A and a are alleles.p and q are frequencies.
Chance that offspring is AA is p x p = p2.Chance that offspring is Aa is (p x q) + (p x q) = 2pq.Chance that offspring is aa is q x q = q2.
Consider the F1 generation when two heterozygotes (Aa) mate.
Since there are only two alleles, p + q = 1.
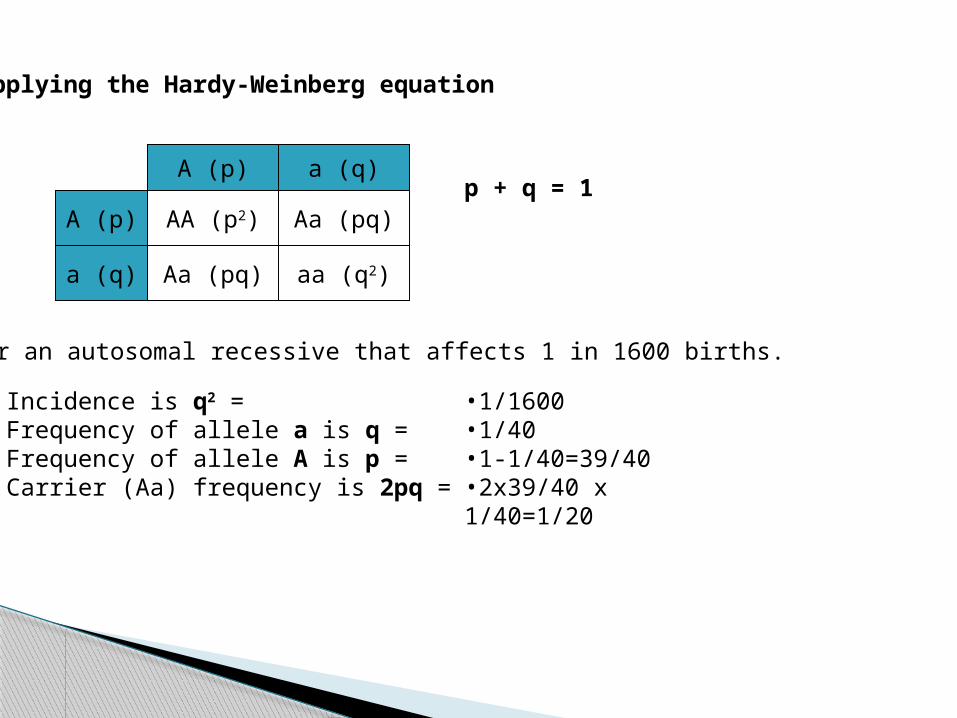
Applying the Hardy-Weinberg equation
AA (p2)A (p)
a (q) Aa (pq)
A (p) a (q)
Aa (pq)
aa (q2)
p + q = 1
Consider an autosomal recessive that affects 1 in 1600 births.
Incidence is q2 = Frequency of allele a is q = Frequency of allele A is p = Carrier (Aa) frequency is 2pq =
•1/1600•1/40•1-1/40=39/40•2x39/40 x 1/40=1/20
Factors required for Hardy-Weinberg equilibrium (know four)
•Population is large.•No migration into or out of the population.•Random mating.•Mutation rate remains constant.•No selection of alleles (neither negative not positive).
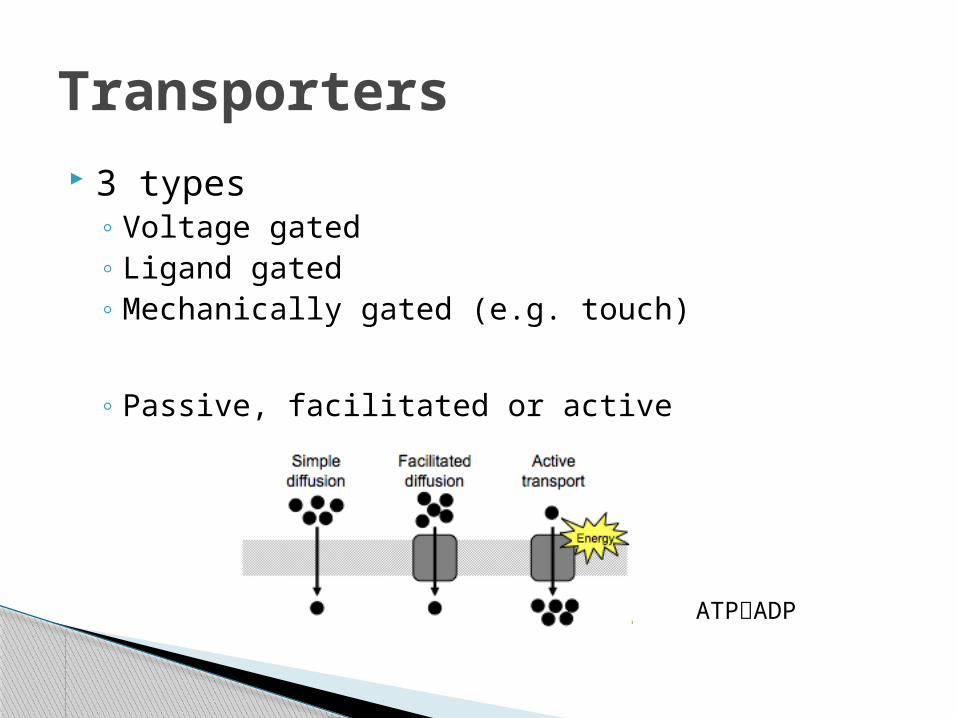
3 types◦ Voltage gated◦ Ligand gated◦ Mechanically gated (e.g. touch)
◦ Passive, facilitated or active
Transporters
ATPADP
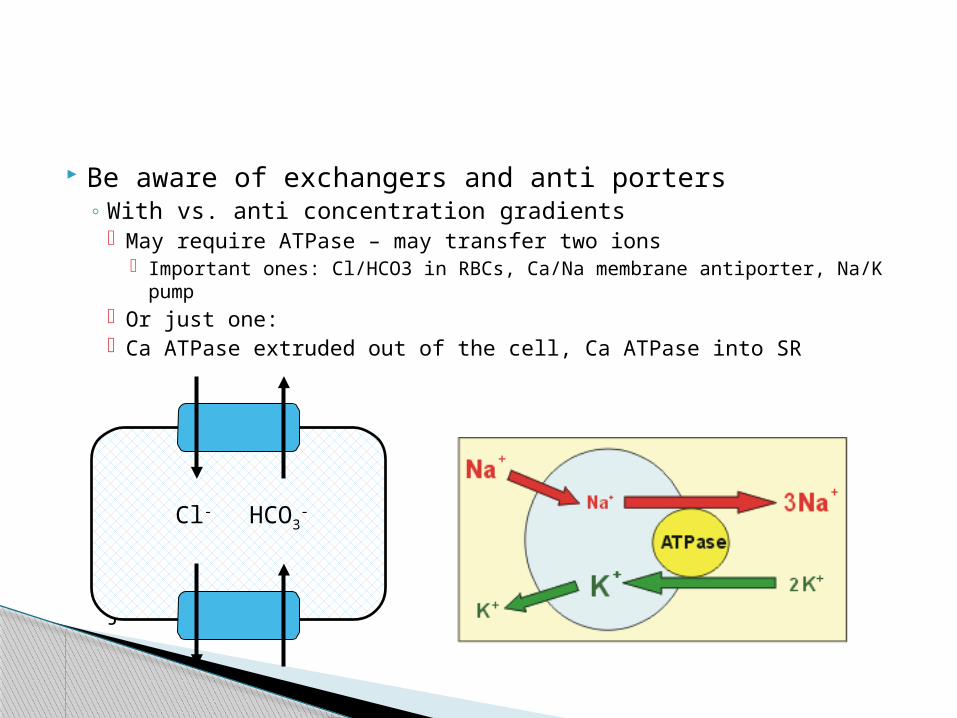
Be aware of exchangers and anti porters◦ With vs. anti concentration gradients
May require ATPase – may transfer two ions Important ones: Cl/HCO3 in RBCs, Ca/Na membrane antiporter,
Na/K pump Or just one: Ca ATPase extruded out of the cell, Ca ATPase into SR
j
Cl- HCO3-
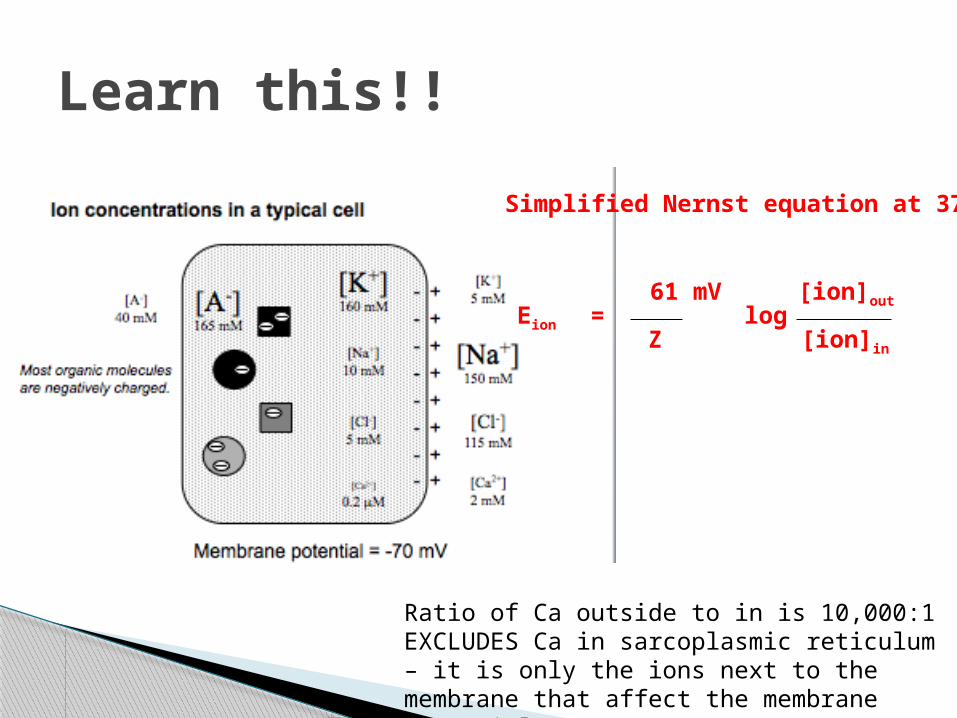
Learn this!!
Simplified Nernst equation at 37°C
Eion
61 mV
Zlog
[ion]out
[ion]in
=
Ratio of Ca outside to in is 10,000:1EXCLUDES Ca in sarcoplasmic reticulum – it is only the ions next to the membrane that affect the membrane potential
C
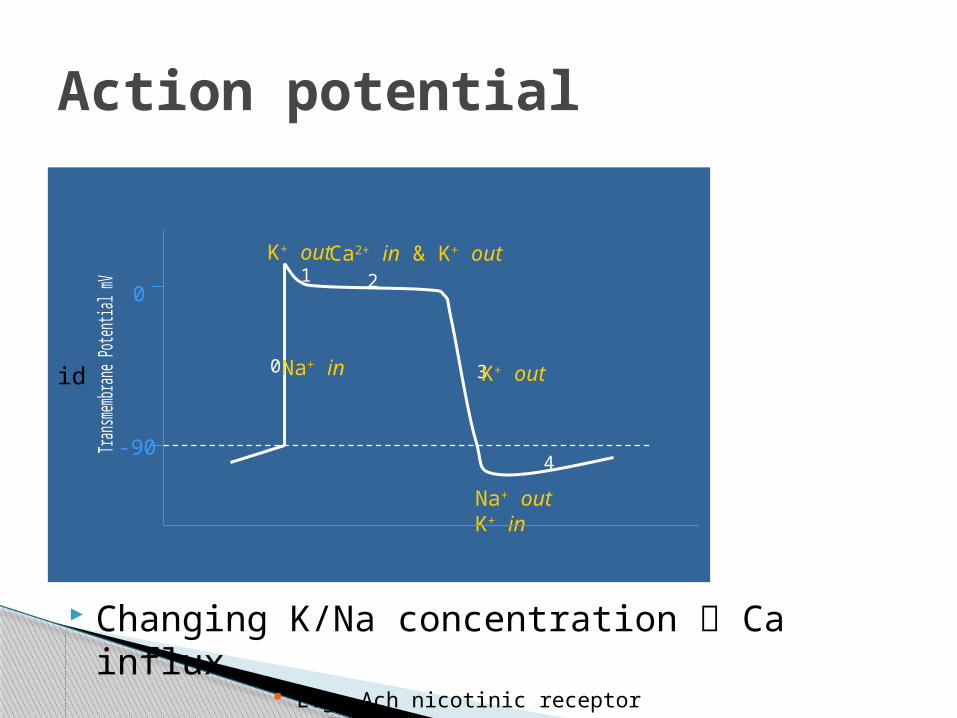
Changing K/Na concentration Ca influx E.g. Ach nicotinic receptor
Action potential
id
4
3
21
0Na+ in K+ out
Na+ outK+ in
0
-90
K+ outCa2+ in & K+ out
Paracrine Endocrine Autocrine Direct contact
With three effects:◦ Change ion balance cascade of effects (e.g.Ca)◦ Alter gene transcription◦ Alter existing enzymes via phosphorylation
Signal types
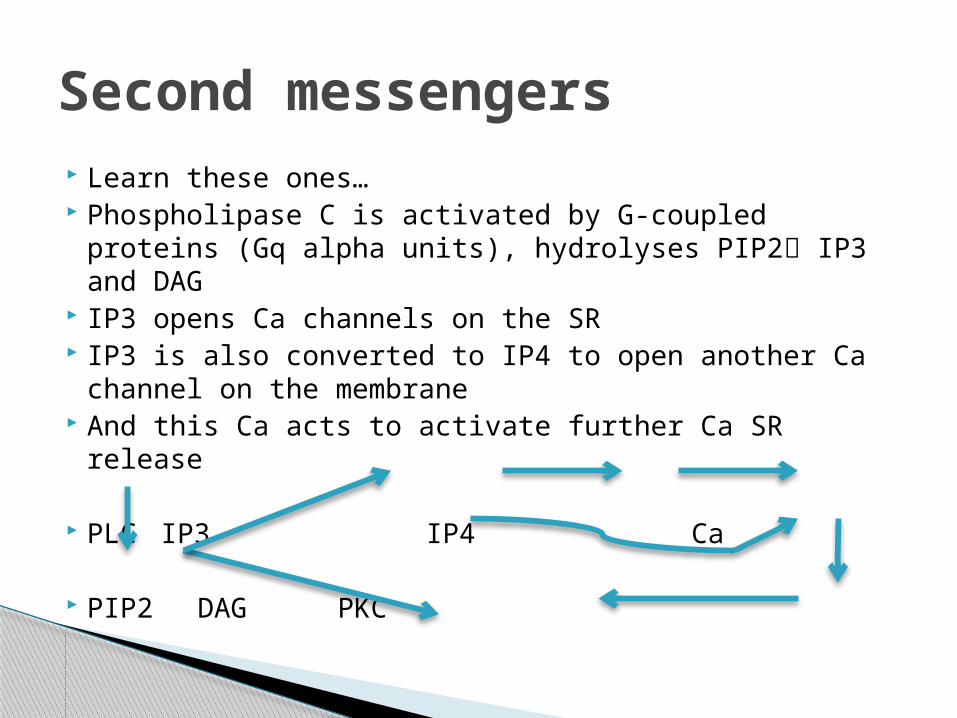
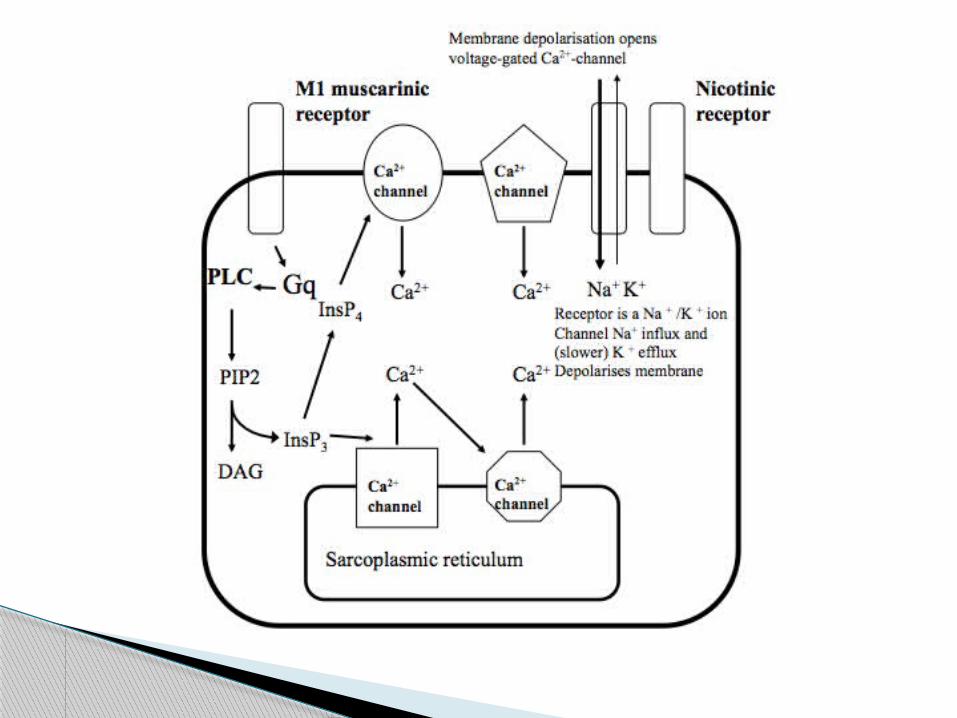
Learn these ones… Phospholipase C is activated by G-coupled proteins
(Gq alpha units), hydrolyses PIP2 IP3 and DAG IP3 opens Ca channels on the SR IP3 is also converted to IP4 to open another Ca
channel on the membrane And this Ca acts to activate further Ca SR release
PLC IP3 IP4 Ca
PIP2 DAG PKC
Second messengers
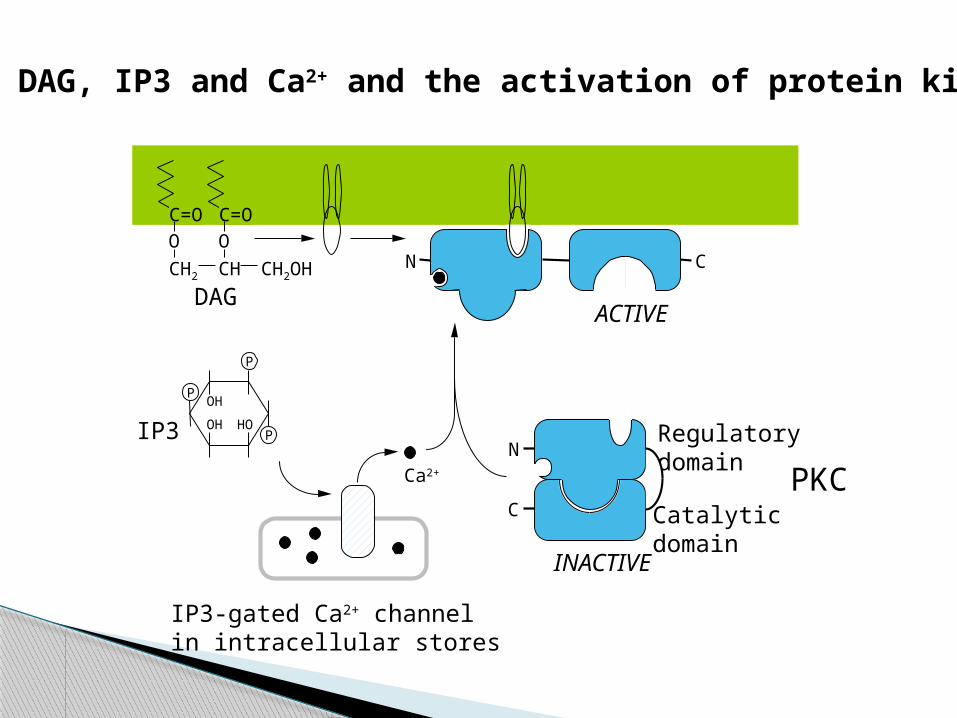
DAG, IP3 and Ca2+ and the activation of protein kinase C
CN
ACTIVEDAG
CHCH2 CH2OH
O
C=O
O
C=O
IP3
POH
OH HOP
P
IP3-gated Ca2+ channelin intracellular stores
Ca2+
N
C
Regulatorydomain
Catalyticdomain
INACTIVE
PKC
Adenylate cyclase converts ATPcAMP Guanylate cyclase converts GTPcGMP cAMP acts on protein kinase A (amongst others) cGMP acts on protein kinase G (amongst others) cGMP and cAMP are common second
messengers
The reverse (e.g. cAMPATP) is done by phosphodiesterase
Drugs can impact by inhibiting this process
cNMP’S
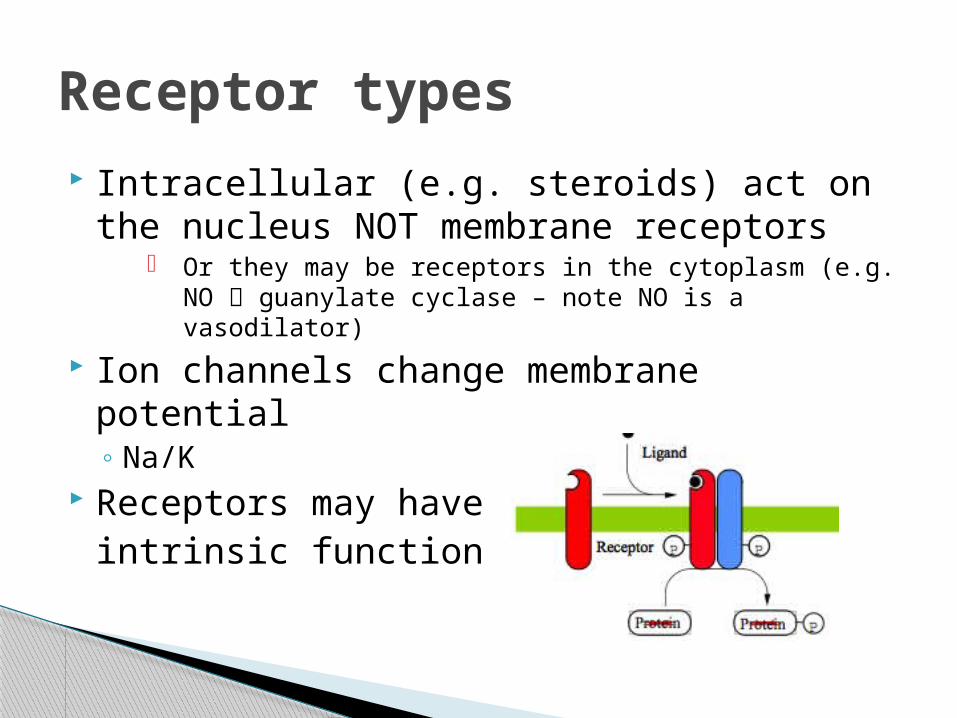
Intracellular (e.g. steroids) act on the nucleus NOT membrane receptors
Or they may be receptors in the cytoplasm (e.g. NO guanylate cyclase – note NO is a vasodilator)
Ion channels change membrane potential◦ Na/K
Receptors may haveintrinsic function
Receptor types
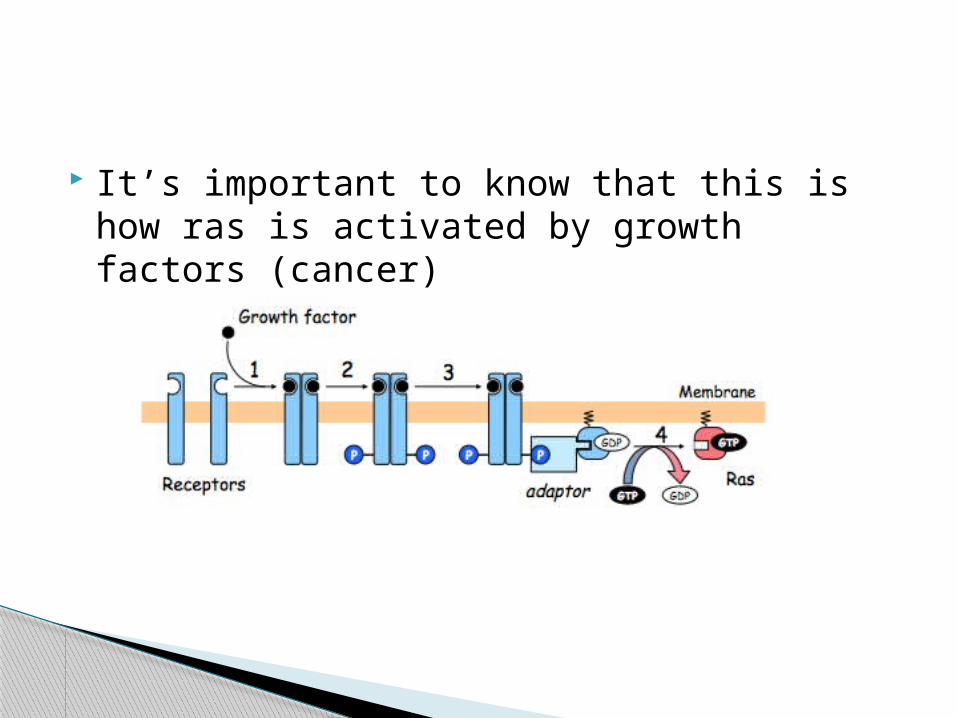
It’s important to know that this is how ras is activated by growth factors (cancer)
Ligand binds and stimulates the alpha subunit (all you really need to know)
The alpha subunit has a set function based on its classification
Gs stimulates adenylate cyclase.
Gi inhibits adenylate cyclase.
Gt stimulates cGMP phosphodiesterase.
Gq stimulates phospholipase C.
G protein coupled receptors
Acetylcholine – parasymathetic ns There are five muscarinic acetylcholine receptor
subtypes. M1, M3 and M5 couple through Gq to stimulate
phospholipase C. M2 couples through Gi to open a K+-channel. M4 couples through Gi to inhibit adenylate
cyclase. PLUS the nicotinic acetylcholine receptor (Na+/K+
channel)
Ca in…◦ Voltage gated Ca channels (membrane)◦ IP4 gated Ca channels (membrane)◦ Ca gated Ca channels (sarcoplasmic reticulum)◦ IP3 gated Ca channels (sarcoplasmic reticulum)
Ca out…◦ Plasma membrane ATPase◦ Sarcoplasmic reticulum ATPase◦ Ca/Na exchanger
Calcium channels
Haemaglobin is a quaternary struture 4 globins and a haem 2 alpha/2 beta structure Only two things bind to the haem…
◦ O2◦ CO (NOT CO2 – this binds to the globin)
Proteins
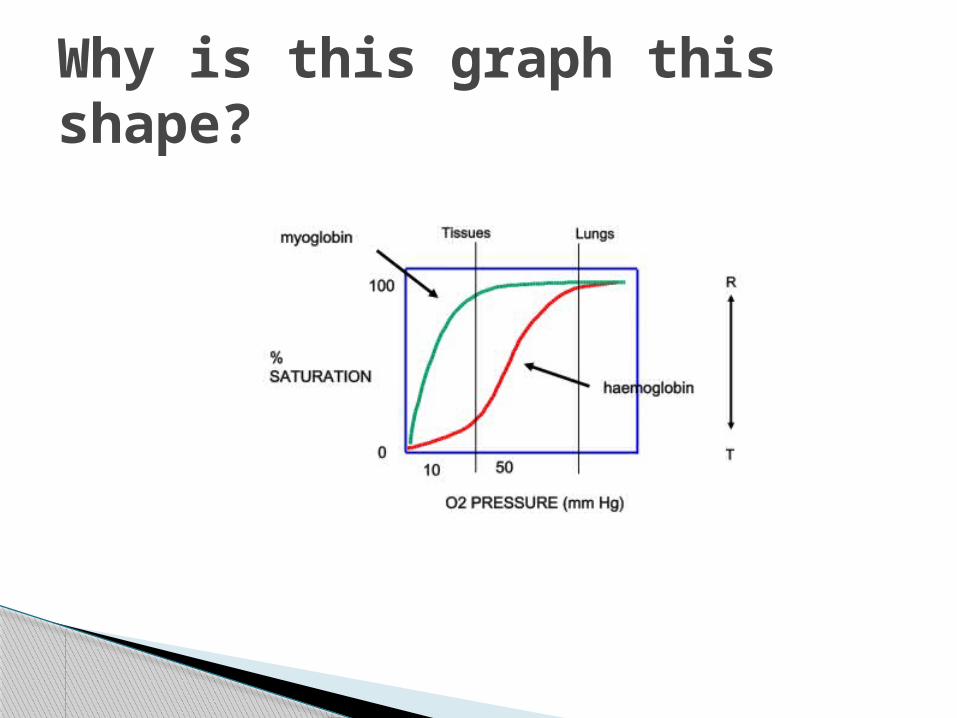
Why is this graph this shape?
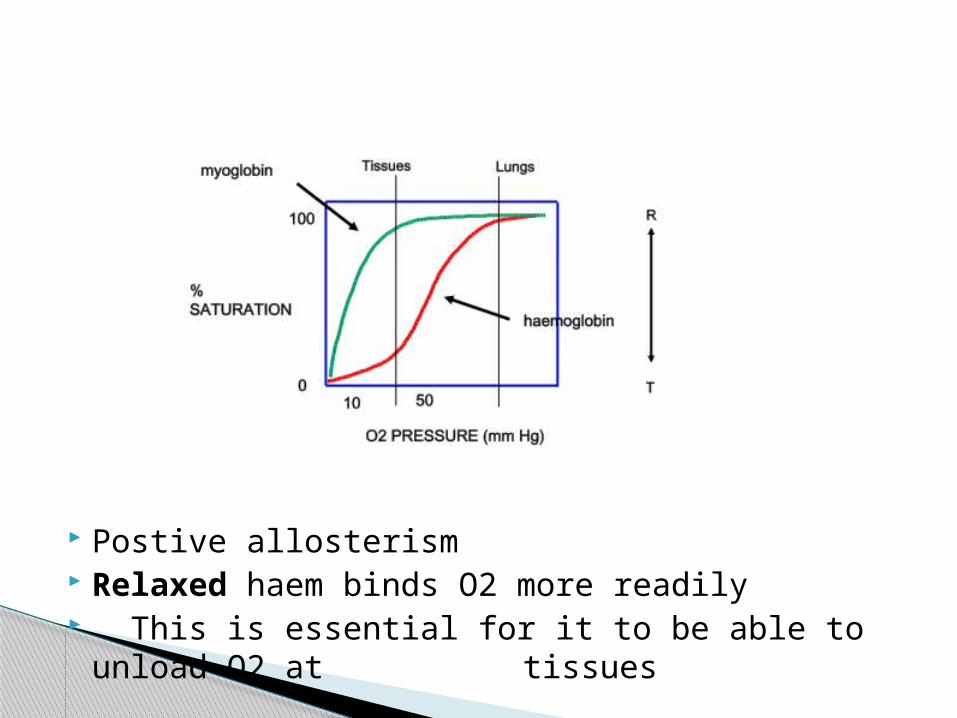
Postive allosterism Relaxed haem binds O2 more readily This is essential for it to be able to unload O2
at tissues
What lowers the affinity of haem for O2? (note this shifts the curve to the RIGHT)◦ 2,3, BPG
Stabilises deoxygenated Hb
◦ H or CO2 – effect on pH? Increases acidity – the Boer effect H binds to Hb and stabilizes dexoygenated Hb CO2 is converted to HCO3 and binds to Hb
(‘carbamation’) - stabalises deoxygenated Hb
CO2+H2O H2CO3 HCO3- + H+
Ventilation (breathing) excretes CO2◦ Hence hyperventilation respiratory alkalosis◦ And hypo ventilation respiratory acidosis
You also get metabolic imbalance◦ Increased acid (e.g. ketones in diabetes) metabolic
acidosis◦ Increase HCO3 metabolic alkalosis◦ Either way, it comes back to this…
CO2+H2O H2CO3 HCO3- + H+
Lungs Kidney
Acid-base balance
Triple helix (Left handed) Glycine: Proline/hydroproline
◦ Or glycine:lysine/hydrolysine Major part of the extra cellular matrix Need to know steps of post-translational
modification and diseases related to them
Collagen
1: Synthesise alpha chains of pre-pro collagen (Pre and pro are both precursors)
2: Hydroxylate proline to hydroxyproline (requires vitamin C so problem = scurvy)
3: Hydroxylate lysine residues to hydroxylysine 4: Glycosylate some hydroxlysine These steps are done to enable cross linking
and glycosylation gives a more open structure
Post translational steps
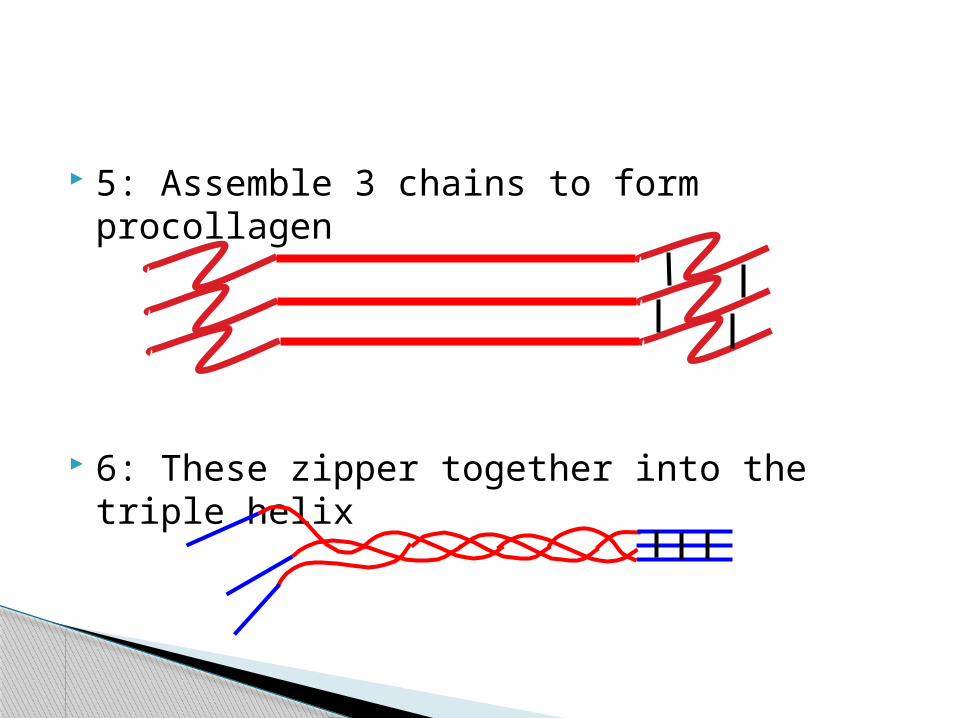
5: Assemble 3 chains to form procollagen
6: These zipper together into the triple helix
7: Remove the globular ends by procollagen peptidase, so that fibrils can be formed
(lack of this ethlers danlos (hyper mobile joints, stretchy skin)
8: Cross link fibrils (lysines and hydroxlysines) to form collagen.
Requires lysyl oxidase: defect lathyrism (curved spine, aortic aneurysm, dislocations)
Osteogenesis Imperfecta◦ Glycinebulky amino acid, so type 1 collagen
(bone) can’t fold correctly and is unstable◦ Fractures◦ NOT a post translational disease (primary
structure)
Haematocrit is just the red blood cell cell content (usually 40-45%)
Blood
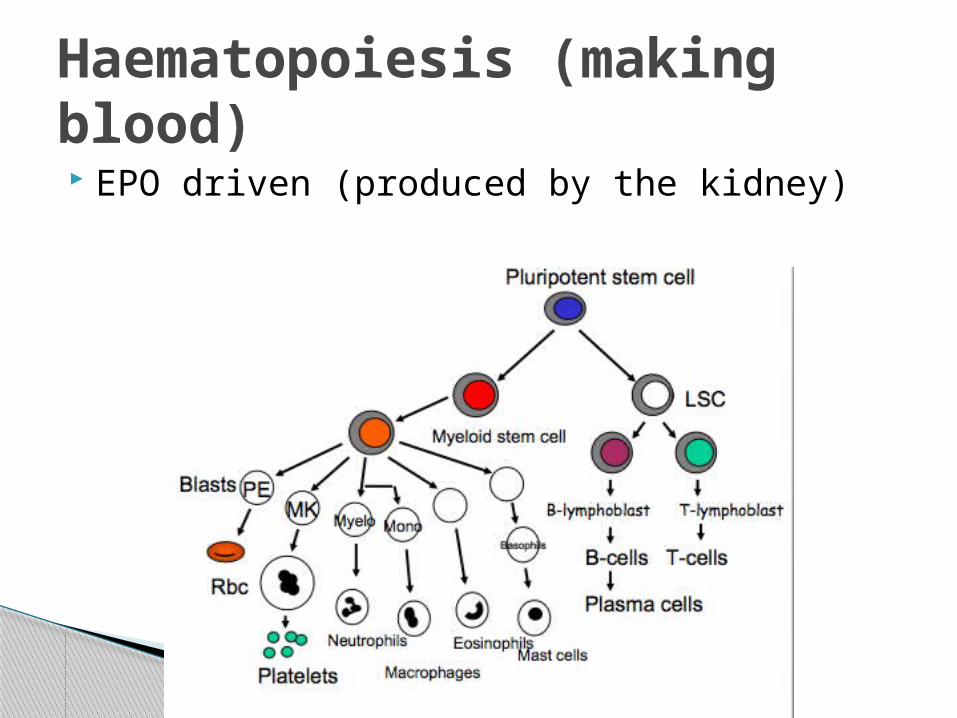
EPO driven (produced by the kidney)
Haematopoiesis (making blood)
Lots of causes Can be a symptom of bleeding anywhere in
the body (ulcers, malignancy) Symptoms:
◦ Pallor (sign?)◦ Tiredness◦ Fainting◦ Light headedness◦ Dyspnoea
Anemia
2,3 BPG Redistribute blood to important places Produce reticulocytes (immature RBCs,
limited use – note LARGER)
How does the body respond?
Normocytic, normochromic ◦ Cells are the same, just less◦ So blood less – either Acute Blood Loss, or Anemia of
Chronic Disease Microcytic, hypochromic
◦ Little girly cells ◦ No iron◦ Menstruation
Macrocytic, normochromic◦ BIG cells (may be reticulocytes)◦ Vitamin B12/Folate deficiency◦ Intrinsic factor required for uptake – any question
involving terminal ilium, think anemia!
3 Classifications
1: Vascular constriction◦ Near instant contraction◦ Due to inhibited local production of NO and
prostacylcin◦ Usual, relaxed state comes back to pathways…
4 stages following vascular injury
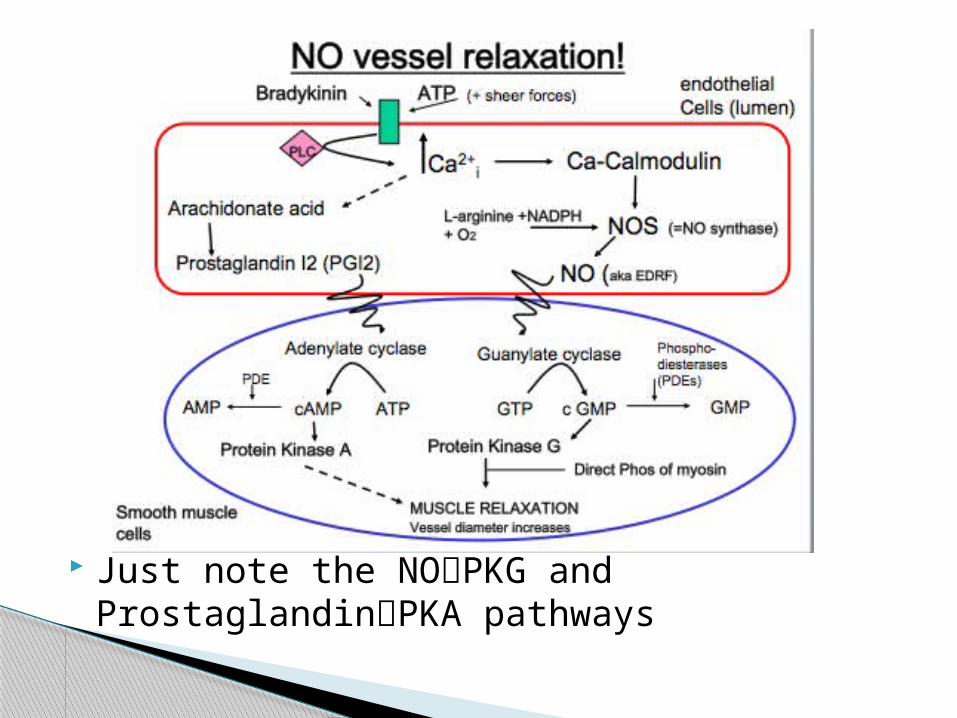
Just note the NOPKG and ProstaglandinPKA pathways
2: Platelet plug◦ Collagen and vWF exposed by damage◦ Platelets bind and activate◦ Reinforcing : binding thromboxane A2 and ADP
release (platelet activator/aggregators)◦ Again, we’ve done the pathways…
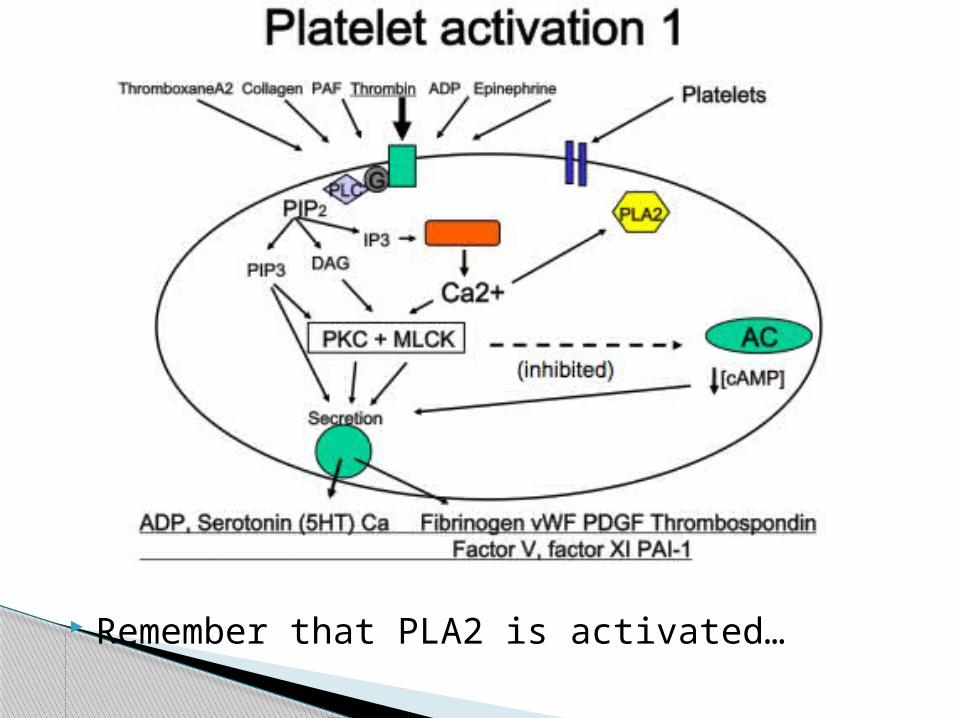
Remember that PLA2 is activated…
PLA is converted to PI – COX1 converts this to thromboxane… which does what?
Aspirin inhibits COX1 blood thinner. Why is this permanent?
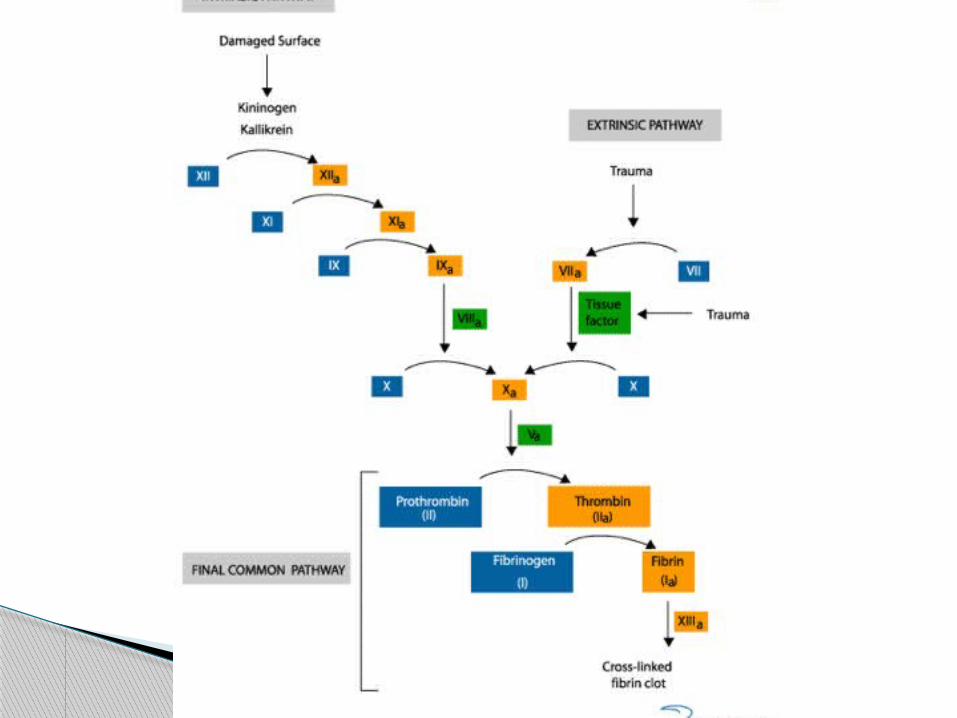
3: Clotting Collagen starts intrinsic clotting Thromboplastin/tissue damage starts
extrinsic (slower) Both of these activate factor X Which converts ProThrombinThrombin Which converts Fibrinogen Fibrin Forms the clot
4: Clot lysis (have to get rid of it) Process is ‘fibrinolysis’ (-lysis = degrade) Plasminogen is converted to plasmin which
leads to fibrinolysis Activation of plasminogen plasmin is by
agents such as tPA and streptokinase (‘clot busters’)
Fed 0-4 hours post prandial◦ Insulin release muscle/adipose uptake◦ Brain uses glucose independent of insulin◦ Stimulates protein, lipogenesis, glycogen synthesis◦ Stimulates glycolysis
Fasted 4-12 hours◦ Glucagon>insulin◦ Break down glycogen, and triglycerides into FFA◦ Muscle uses up glycogen
Starved >12◦ Proteolysis, lipolysis◦ Gluconeogenesis◦ FFA ketones
Metabolism
Remember insulin does the opposite of glucagon and insulin is released after eating
These regulate glucose uptake Hexokinase is found in the brain – where
affinity is much higher than (usual) glucose levels
Converted to G6P – inhibitive Glucokinase is found in the liver – much
lower affinity – except after eating G6P is NOT inhibited – glucose is stored (as
glycogen) and released as required
Hexokinase and Glucokinase
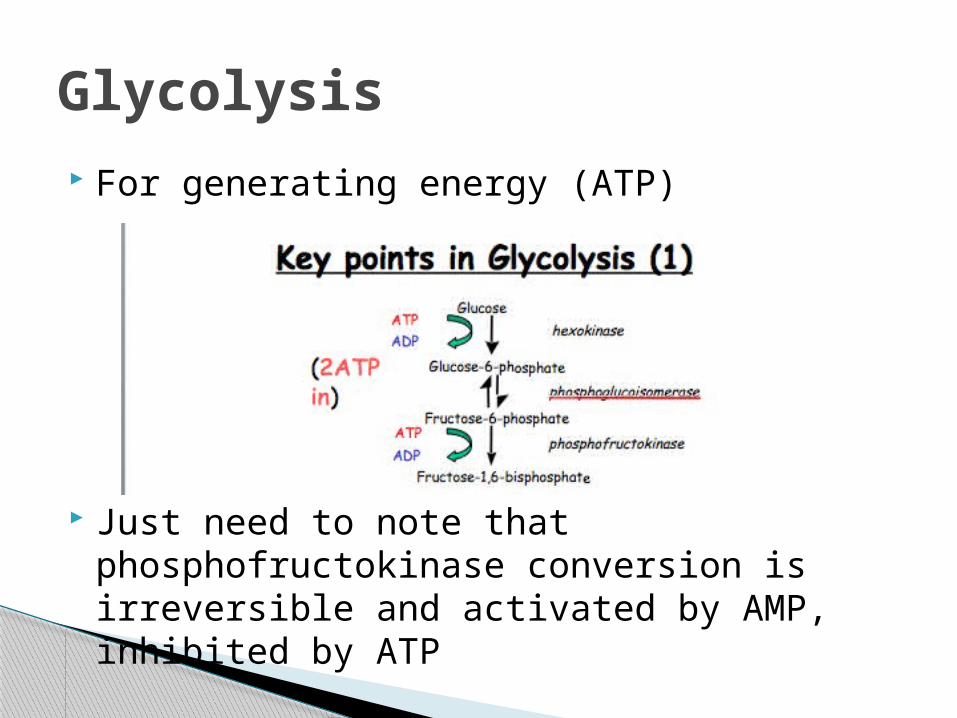
For generating energy (ATP)
Just need to note that phosphofructokinase conversion is irreversible and activated by AMP, inhibited by ATP
Glycolysis
The next step splits fructose 1,6 biphosphate into 2 x gylceraldehyde (by isomerase – reorganises it)
This is converted into pyruvate – but this is not a efficient payoff in terms of ATP
Under AEROBIC conditions, this is converted into acetyl-CoA
Under anaerobic conditions it lactate
It is this that produces ATP In mitochondria Lots of things input Driven by AMP, inhibited by what it
produces: ATP, NADH
Citric Acid Cycle
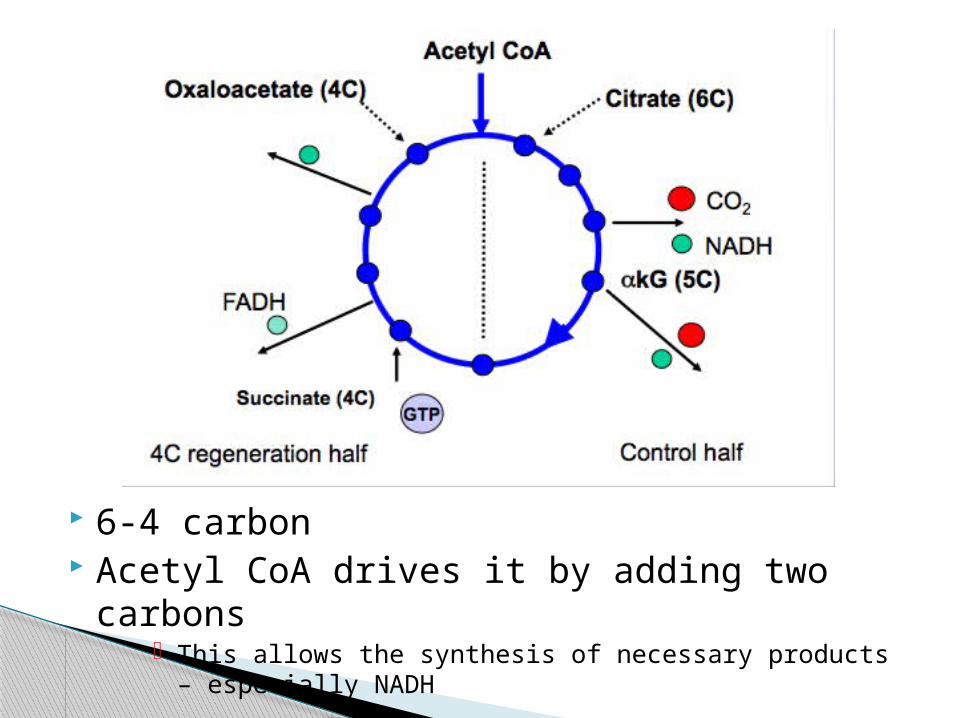
6-4 carbon Acetyl CoA drives it by adding two carbons
This allows the synthesis of necessary products – especially NADH
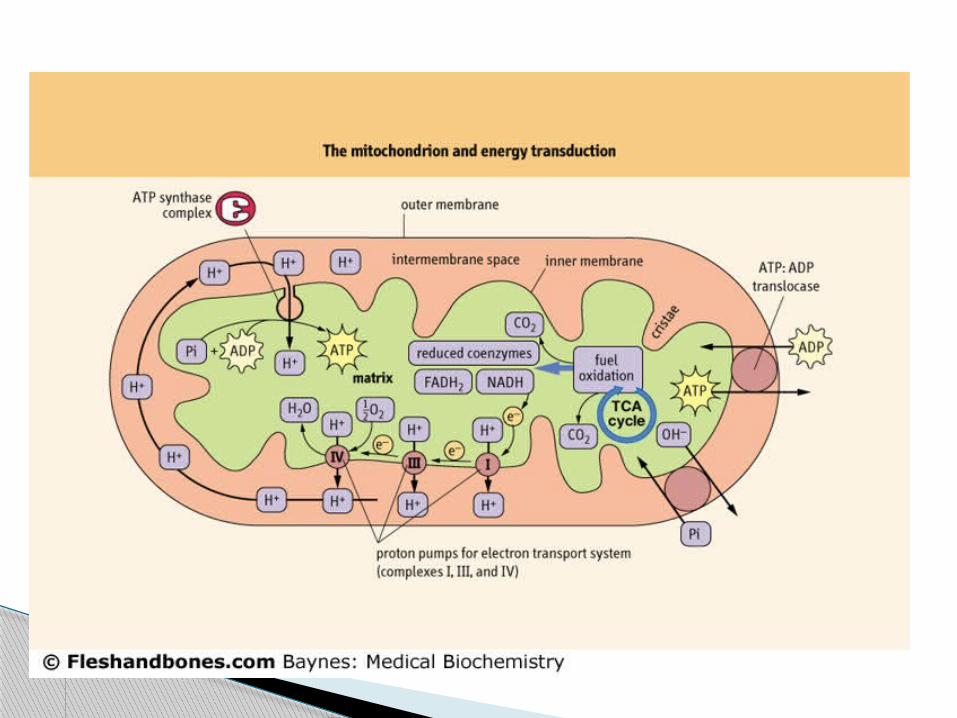
NADH donates its H (becomes NAD) The H is used to drive proton pumps Lots of H results in ADPATP by oxidative
phosphorylation
This is the real pay off stage of glycolysis – without oxidative phosphorylation (i.e. in anaerobic conditions) ATP yield is low
Lots of glucose lots of insulin lots of glycolysis lots of acetyl coa
Fatty acids are synthesised which creates more available acetyl-coa
So lots to drive the cycle This just means you can make more things
you wouldn’t usually e.g. purines, GABA
Back to the fed state…
Low acetyl-coa means the cycle isn’t driven FFA are broken down to feed in. A fatty acid is just lots of acetyl units –
which contain carbon So these are harvested for their carbon and
bound to coa so they can be fed into the cycle
Which is why you get lipolysis and FFA breakdown but this also creates ketones which are acidic… so lead to what…?
But in the starved/fasted state…
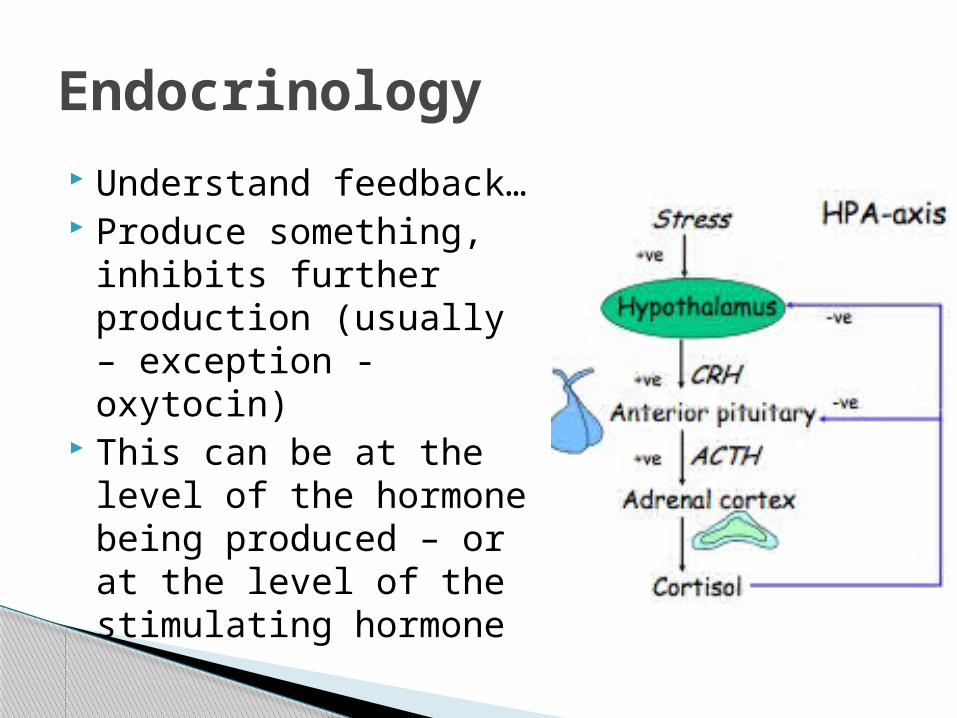
Endocrinology Understand feedback… Produce something,
inhibits further production (usually – exception - oxytocin)
This can be at the level of the hormone being produced – or at the level of the stimulating hormone
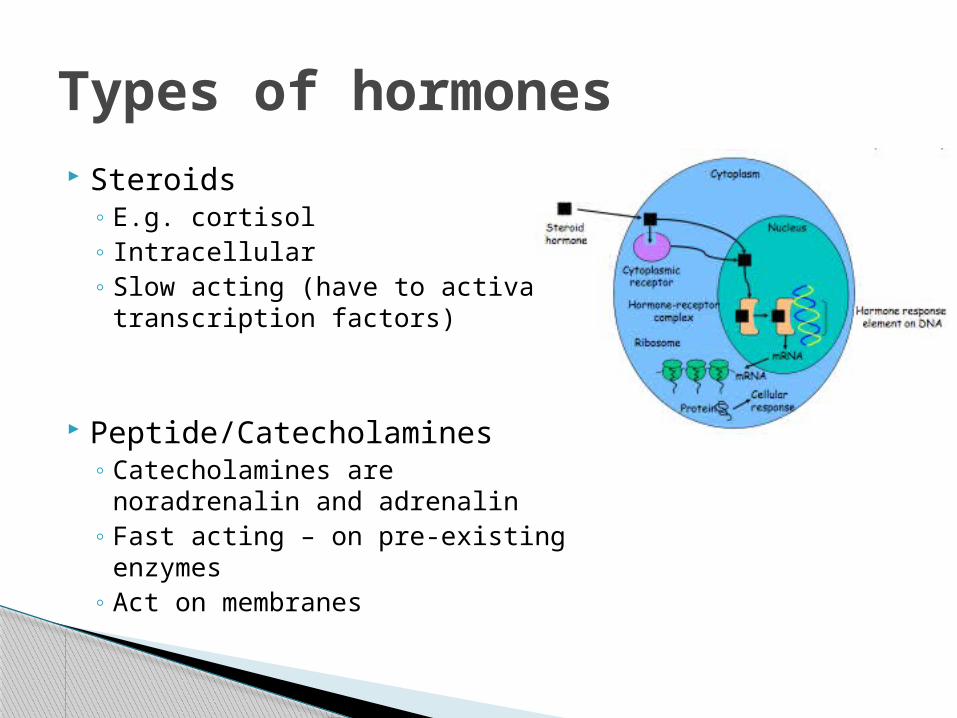
Steroids◦ E.g. cortisol◦ Intracellular◦ Slow acting (have to activate
transcription factors)
Peptide/Catecholamines◦ Catecholamines are noradrenalin
and adrenalin◦ Fast acting – on pre-existing
enzymes◦ Act on membranes
Types of hormones
Know the ones that are released by the hypothalamus and what they release from the anterior pituitary
Then need to know the diseases associated with them – there’s always a problem with too much or too little
What hormones do you need to know?
Corticotrophin releasing hormone (CRH) from hypothalamus
Adrenocorticotrophin hormone from anterior pituitory
Cortisol from Adrenal gland Breaks down protein, causes lipolysis,
increases gluconeogesis/glycogen synthesis Effects:
◦ Immunosuppressive◦ Decreases bone density◦ Decreases muscle mass
CRH
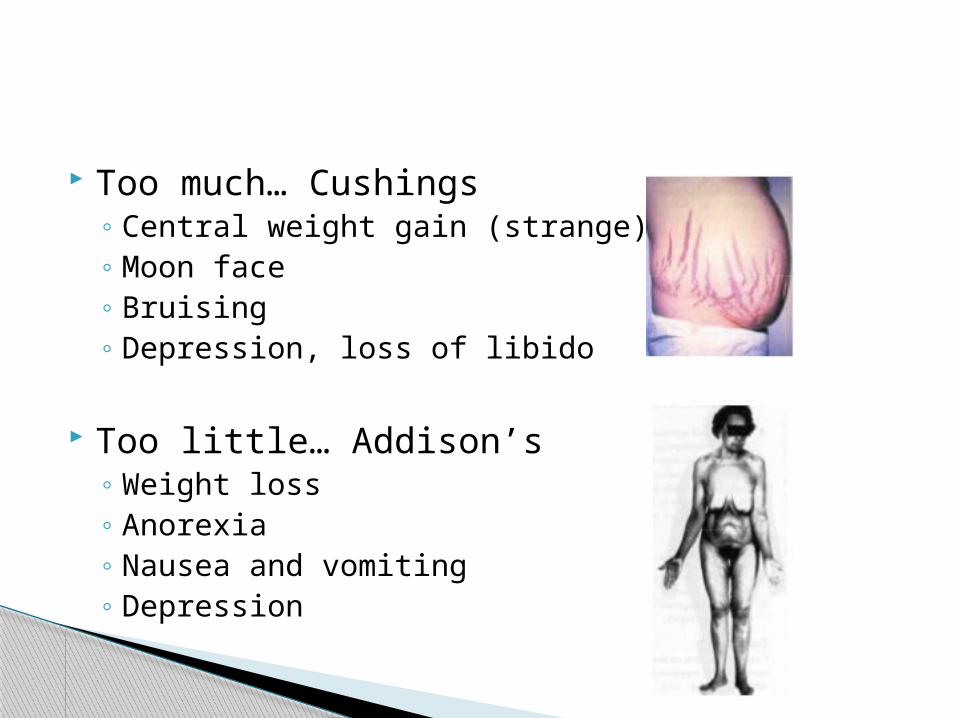
Too much… Cushings◦ Central weight gain (strange)◦ Moon face◦ Bruising◦ Depression, loss of libido
Too little… Addison’s◦ Weight loss◦ Anorexia◦ Nausea and vomiting◦ Depression
Growth hormone releasing hormone and growth hormone inhibiting hormone from hypothalamus
Anterior pituitary then releases growth hormone
Does what you would expect- builds things up e.g. protein synthesis, stimulates IGF-1 ( growth), stimulates gluconeogenesis, stimulates glycogen synthesis
What are these actions the opposite of?
GHRH and GHIH
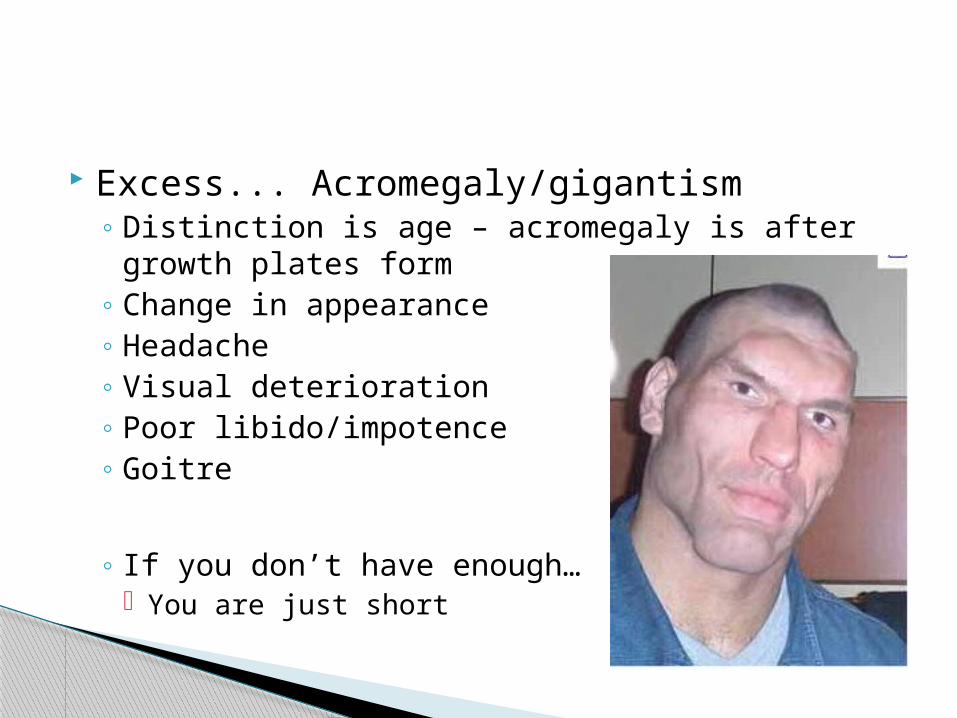
Excess... Acromegaly/gigantism◦ Distinction is age – acromegaly is after growth
plates form◦ Change in appearance◦ Headache◦ Visual deterioration◦ Poor libido/impotence◦ Goitre
◦ If you don’t have enough… You are just short
Thyrotropin Releasing Hormone from hypothalamus
Thyroid Stimulating Hormone from AP Releases T3 (Tri-idiothyronine) And T4 (Thryoxine)
◦ The major effect of these is to increase the basal metabolic rate
TRH
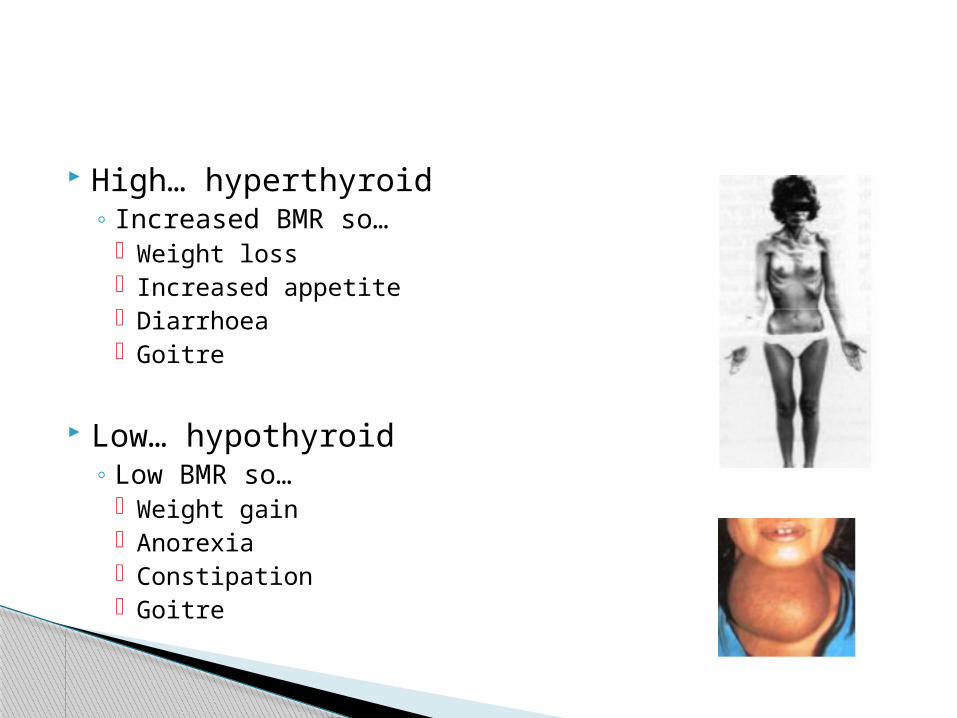
High… hyperthyroid◦ Increased BMR so…
Weight loss Increased appetite Diarrhoea Goitre
Low… hypothyroid◦ Low BMR so…
Weight gain Anorexia Constipation Goitre
Luteinizing hormone releasing =Gonadatrophin releasing hormone
From hypothalamus Stimulates AP to produce luteinizing
hormone and follicle stimulating hormone Important for when you do repro (act on
gonads to produce sex steroids – oestrogen, testosterone)
LHRH/GnRH
2 things released – ADH (vasopressin) and oxytocin
You will cover both of these in semester 2/3…
Just worth knowing hypothalamusposterior pituitary is neuroendocrine transmission unlike AP which is endocrine
This means low amounts have an effect◦ Oxytocin important in giving birth◦ ADH is anti-diuretic hormone – you retain water so it
regulates blood pressure
The posterior pituitary
Increased action:◦ Increased availability of substrate
Iodine excess in hyperthyoid◦ Immune response
Hyperthyroid caused by Graves Disease (antibodies stimulate thyroid gland)◦ Tumours
Pituitary/hypothalamas tumour – can cause excess secretion of any hormone
Decreased action:
◦ Decreased availability of substrate Iodine deficiency in hypothyroid
◦ Immune response Hypothyroid - Hashimotos – destruction of the thyroid gland
◦ Destruction of the gland Radiation, surgery (hypothyroid)
Why do things go wrong?