Embed Size (px)
Citation preview

ALMC
ARUSHA LUTHERAN
MEDICAL CENTRE
ANNUAL REPORT 2016

ALMC Annual Report 2016 Page 2
TABLE OF CONTENTS
EXECUTIVE SUMMARY ........................................................................................................ 3
INTRODUCTION ..................................................................................................................... 6
VISION AND MISSION OF ALMC ........................................................................................ 6
MANAGEMENT ....................................................................................................................... 7
STAFFING ............................................................................................................................... ..7
FINANCES ................................................................................................................................ 9
CLINICAL SERVICES ........................................................................................................... 11
OUTPATIENT SERVICES ........................................................................................... 11
1. OUTPATIENT DEPARTMENT ............................................................... 12
2. DENTAL SERVICES ................................................................................ 14
INPATIENT SERVICES ............................................................................................... 16
1. SURGICAL DEPARTMENT .................................................................... 17
2. NEONATAL INTENSIVE CARE ............................................................ 18
3. OBSTETRICS AND GYNECOLOGY DEPARTMENT ......................... 22
4. PEDIATRIC DEPARTMENT ................................................................... 24
PROGRAMS OF ALMC ......................................................................................................... 26
1. AIDS CONTROL PROJECT ..................................................................... 26
2. PLASTER HOUSE AND REHABILITATIVE SURGERY ..................... 28
3. HOSPICE AND PALLIATIVE CARE ..................................................... 32
CHAPLAINCY AND SPIRITUAL CARE ............................................................................. 34
MEDICAL EDUCATION ....................................................................................................... 34
CHALLENGES ....................................................................................................................... 39
PLANNING FOR THE FUTURE ........................................................................................... 41
THANKSGIVING ................................................................................................................... 42
CONCLUSION ........................................................................................................................ 43
APPENDIX 1. TOP DIAGNOSES .......................................................................................... 45

ALMC Annual Report 2016 Page 3
ARUSHA LUTHERAN MEDICAL CENTRE
ANNUAL REPORT 2016
EXECUTIVE SUMMARY
2016 has been an excellent year of service for Arusha Lutheran Medical Centre. ALMC has
experienced continued growth in many areas which has led to greater stability in the areas of
staff retention, higher quality services, and in improved financial wellbeing. The best way to
describe 2016 is as a year of continued growth and greater stability.
HIGHLIGHTS:
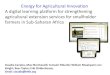
1. Dramatic 20% increase in patient visits: The year 2016 produced incredible growth in
the number of patients served. The total grew from 123,000 in 2015 to 148,000 in 2016.
This is the largest increase ever in the history of the hospital.
56,296
81,619 94,885
105,405 116,693 118,930 122,740
147,528
-
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
2009 2010 2011 2012 2013 2014 2015 2016
TOTAL VISITS PER YEAR

ALMC Annual Report 2016 Page 4
2. Improved staff retention and improved nursing to patient ratios: The year 2016
produced significant improvement in staffing for nurses. The consultants and doctors
continue to be fully staffed. Nursing has improved with the hiring of the first graduates of
the ALMC School of Nursing.
3. Financial growth and improved financial stability: The financial status of ALMC
improved significantly in 2016 as total revenues increased by 32% to 10.1 Billion
Tanzanian Shillings (TSh). This was largely a result of the increase number of patients and
the introduction of the new dialysis service to the hospital. Throughout the year, statutory
payment arrears were reduced and the servicing off the original construction loan was
complied with fully.
4. Educational highlights: Educational highlights are among the most exciting for the year.
Most notable are the School of Nursing graduating ts first two classes of certificate level
nurses and the Surgical Residency producing the first ever successful candidate for the
prestigious College of Surgeons of Eastern, Southern, and Central Africa Member exam.
The hospital is also proud and delighted by the continued progress of five or our doctors
who continue in their specialty training at institutions throughout East Africa.
5. Strengthening of Intensive Care, Newborn Intensive Care, and Hemodialysis:
Improvement in the standards of care in the ICU and NICU were emphasized through
providing new equipment for ventilating patients and with multiple intensive in service
training of staff. The introduction of the Hemodialysis Unit has provided an entirely new
service for the Arusha community.
6. Quality Assurance: In 2016 the hospital voluntarily undertook to engage in an
international accreditation exercise sponsored by SafeCare and the Government of
Tanzania. This provides ALMC with an initial sense of our level of care and a roadmap to
even greater improvement going forward.
CHALLENGES:
1. Financial Stability: True financial stability remains elusive. Great strides were
accomplished this year with breaking even on day to day running costs. Considerable
progress was made in reducing further the outstanding debts to income tax and pension
funds. However, significant challenges remain.
1. NHIF Insurance: The National Health Insurance Fund is the largest of our insurance
partners and provides 60% of hospital revenues. So when NHIF is late in paying patient
reimbursements to the hospital, it produces major cash flow problems, delays payment

ALMC Annual Report 2016 Page 5
of staff salaries, and interferes with the hospital’s ability to comply with commitments
for reduction in statutory payment arrears.
2. CRDB Bank Loan: In January 2016, the CRDB Bank offered the hospital a process
for reducing the interest rate of the loan if the hospital could make a substantially
principal payment to reduce the principal. The hospital and the diocese committed to
this but by the time such a large amount of funding was procured, the bank had to
withdraw the offer due to internal challenges at the bank. This results in a lost
opportunity to reduce the total payback over the lifetime of the loan.
3. Tanzania Revenue Authority retroactive tax assessment: At the end of 2016, the
TRA presented the hospital with a retroactive tax assessment based on five years of
non- payment of income tax on overtime and extra duties. This had not previously been
taxed to be consistent with the legal situation in government hospitals. The new
assessment reversed that position and states that nongovernment hospitals must pay tax
even though government hospitals do not. This inequitable taxation is now the basis
for a heated negotiation as the assessment is for $300,000.

ALMC Annual Report 2016 Page 6
ARUSHA LUTHERAN MEDICAL CENTRE
ANNUAL REPORT 2016
1. INTRODUCTION
The Arusha Lutheran Medical Centre is a ministry of the Evangelical Lutheran Church in
Tanzania – North Central Diocese. ALMC was founded to be model of faith-based healthcare
and to be a center of excellence and an example of the level of quality of care which the church
community could provide to the larger Arusha community. The development of this new
model was prompted by both the growing needs of a rapidly growing population in the city of
Arusha and by the economic challenge of providing sustainable holistic health care in a rapidly
changing health care environment in Tanzania.
The construction of ALMC began in June 2005 and the hospital opened its doors for service in
December 2008. The year 2016 was the eighth year of ALMC services. This year is best
characterized as a year of continued movement toward stability – in quality of care, in research
and training, and in the hospital’s financial status. The many challenges faced in the first years
have gradually begun to bear fruit with an increase in reputation, patient load, and community
recognition.
2. VISION AND MISSION OF ALMC
VISION
The vision of ALMC is that the people of Arusha might
have access to affordable and excellent consultant care.
MISSION
The mission of ALMC is to serve, treat, and minister to
the whole person; in body, mind, and spirit with the love
and compassion of Jesus Christ.

ALMC Annual Report 2016 Page 7
ALMC strives to reach this vision and mission by providing competent and compassionate
medical care, by promoting health development in the community, and by proclaiming the
gospel of the love and compassion of Jesus Christ.
ALMC seeks to be a new model of health care in Tanzania. The hospital is committed to
providing true patient centered care. It desires to provide a model of quality and compassion
for each one served. ALMC seeks to truly accomplish something new in health care in
Tanzania for the glory of God.
3. MANAGEMENT
Management of the hospital is through the Board of Directors, the Management Committee,
and a variety of committees and interest groups in the hospital.
Board of Directors: The Board of Directors is appointed by the Diocese and is required to
meet at least twice per year. In 2016, the Board of ALMC concluded its term and is awaiting
appointment of a new Board.
Management Committee: ALMC is managed by the Hospital Management Committee which
consists of the membership as prescribed by the Health Policy of the ELCT. This is essentially
the departmental leadership. The Management Committee meets twice monthly.
Executive Committee: The Executive Committee meets weekly to attend to the day to day
running of the hospital. The Executive Committee meets weekly to plan the regular running
of the hospital and consists of the following members:
• Executive Director - Prof. Mark L. Jacobson
• Director of Finance - Mr. Aminieli Mungure
• Director of Clinical Services - Dr. Paul Kisanga
• Director of Nursing - Mrs. Christine Lugakingira
• Hospital Administrator - Ms. Janeth Itemba
• Coordinator of Ancillary Services – Mr. Sizar Simba
• Chaplain - Rev. Gabriel Kimirei
Clinical Management Team Meeting: The hospital has another opportunity for various
department heads to come together in the Clinical Management Committee. Once per month,
there is a cross departmental meeting consisting of the leadership of the medical and surgical
services, nursing, and the leaders of laboratory, the imaging, security, finance, and outpatient
departments. The goal of this meeting is to consider and advise management on issues which
cut across all areas of hospital services.

ALMC Annual Report 2016 Page 8
Doctors Meetings: The medical staff of ALMC meets every second month to discuss in
greater detail the clinical coordination and common challenges across disciplines. The doctors
work through five hospital wide committees:
• Continuing Education Committee
• Formulary Committee
• Quality Assurance
• Infection Prevention and Control Committee
• Theatre Utilization Committee
Departmental Meetings: Each department meets monthly to discuss the department specific
issues and planning.
4. STAFFING
Staffing: The total staff establishment has grown from 250 the first year of operation in 2009
to 389 currently employed at the end of 2016.
Consultants: Staffing with consultant physicians remains strong with 15 specialists who work
closely with a team of 16 Medical Officers and 6 Assistant Medical Officers plus 6 doctors
who are training as surgeons in the PAACS Surgical Residency Program.
ALMC STAFF 2009 2010 2011 2012 2013 2014 2015 2016
SPECIALIST & DOCTORS 17 20 24 31 28 27 27 36
SURGICAL RESIDENTS 2 4 6
NURSING STAFF 87 94 134 149 136 150 143 152
LAB, PHARM & X-RAY 15 13 18 20 20 20 19 26
ADMIN & FINANCE 12 16 19 22 19 17 18 25
SUPPORT STAFF 75 98 89 89 115 115 98 100
NURSING SCHOOL,
HOSPICE, & SURG REHAB 20 26 26 26 26 34 34 44
TOTAL 250 267 310 337 344 345 343 389

ALMC Annual Report 2016 Page 9
Staffing Stability: The year 2016 has seen relative improvements in retaining staff and
reducing turnover. Turnover of staff dropped substantially in 2016. This was in large part due
to our recruitment of nurses from the recent graduates of the ALMC School of Nursing. The
new graduates also contributed to the growth in total staff. Secondly, we have greatly expanded
the number of doctors working in Urgent Care to handle the dramatic increase in patient visits
the past year. The increase in staff also increased in part due to the hospital needing to absorb
staff previously recorded as employees of our AIDS Control Program, Hospice and Palliative
Care Program, and the Rehabilitative Surgery Program. Overall, the general stability in staff
numbers and limited turnover is excellent in Tanzania where the government reports a 40%
shortfall in the total number of nurses required for the needs of the nation.
5. FINANCES
2016 continued to be a year of slow but steady progress in moving toward full financial
sustainability. ALMC has reached the point where monthly revenues are sufficient to meet
daily operating costs and nearly sufficient to service the various loans and debts accrued during
the first three years of hospital operation. While the hospital has yet to reach a true breakeven
point, its progress in meeting daily costs, servicing the construction loan, and paying arrears in
taxation and pension plan is a significant accomplishment. Some of the key points for
consideration include:
Financial Status: Revenues were increased significantly from 7.6 Billion TSH (USD $3.6
Million) in 2015 to 10.1 Billion (USD $4.6 Million) in 2016. This was matched by a similar
increase in expenditures from 8.5 Billion TSH (USD $3.7 Million) in 2015 to 10.1 Billion TSH
(USD $4.6 Million) in 2016. Essentially the hospital reached a breakeven point through
carrying a large debt.
NHIF Fees53%
Patient Fees30%
Donations12%
Government0%
Other5%
ALMC REVENUE 2016

ALMC Annual Report 2016 Page 10
Moving toward sustainability: The challenges to attaining financial stability and long term
sustainability are multifactorial and require a multifactorial response.
1. In 2016, a major effort continued to reduce statutory arrears for pension and income
tax.
2. The National Health Insurance Fund is the hospitals single largest revenue source.
Internal management issues within the NHIF itself have led to late payments to the
hospital as well as to more than two year’s delay in negotiating the reimbursement
rates for services provided by the hospital.
3. At ALMC, the salaries of hospital staff have been linked to the official government
salary scales for government health employees. This leads to an unpredictable
mandatory raise each year.
Responses to the Challenge: During 2016, several longer term interventions have been
implemented to reduce and eliminate the deficit.
1. Arrears and Statutory Debts: All arrears for employee income tax have been paid and
all are up to date. This reduces the overall burden of the arrears but a significant
amount remains toward pension funds.
2. NHIF: The hospital has employed a fulltime doctor to manage the NHIF patient files
and paperwork. This has reduced the number of rejected claims and helped to file the
claims in a more timely manner.
3. New Sources of Income: ALMC is actively seeking new sources of income. In 2016,
ALMC was successful in initiating hemodialysis treatments in the hospital. This is on
a partnership basis with Tanzania Renal Limited and is expected to generate
significant new revenues for the hospital.
Salary57%
Arrears & Loan13%
MedLab/Xray13%
Util/Sec/Food
6%
Maint/Office1%
CT/Dialysis Rent6%
Other4%
ALMC EXPENDITURES 2016

ALMC Annual Report 2016 Page 11
Capital Investments: The hospital invested in several large capital expenditures this year.
1. Purchase of a Coaster Bus for the School of Nursing with assistance from Operation
Bootstrap Africa.
2. Purchase of an Ambulance with assistance from First Lutheran Church, Stoughton,
Wisconsin, USA.
3. Purchase of 2 ventilators and infusion pumps for the ICU with assistance from the
Japanese Embassy to Tanzania.
4. Purchased 2 industrial air compressors – one for replacing a broken one in the oxygen
manufacturing plant and the other to introduce medical air for using ventilators in the
ICU and NICU.
6. CLINICAL SERVICES
ALMC is a full-service hospital and serves as a “consultant” hospital. It provides a full range
of services including both primary care and sophisticated specialist care as follows:
A. OUTPATIENT SERVICES:
In the Outpatient Department ALMC provides:
• Urgent Care: General Outpatient and Emergency Care on a walk in basis
• Specialist Clinics by appointment
• Care & Treatment Services for HIV/AIDS
• Dental Care
• Mental Health Counseling
• Ophthalmology Clinic
• Ear, Nose, and Throat Clinic
• Prenatal and Post Delivery Care Clinic
• Hemodialysis
Outpatient visits grew dramatically in 2016 from 112,665 to 136.386. This is a 21% increase!
This huge increase of nearly 2,000 more patients per month is largely due shifts in insurance
companies and their policies on where their clients may be treated. Particularly, the National
Health Insurance Fund decreased the number of approved health facilities in Arusha and so
many of their clients came to ALMC. The dialysis unit also has provided a new and steady
flow of patient visits.

ALMC Annual Report 2016 Page 12
1. OUTPATIENT AND URGENT CARE DEPARTMENTS: Dr. Derrick Matthews
1. Introduction
The Outpatient Department and Urgent Care, could arguably be considered the face of the
hospital. It is the entry point for the majority of patients at ALMC, with over half of the patients
passing through Urgent Care on a given day. First impressions last long, thus Outpatient
continues to work under the glare of close scrutiny by patients, relatives, doctors,
administration, government, insurance companies and others.
2. Narrative
Again, the Outpatient Department (OPD) exceeded its previous numbers in terms of patient
visits per month and per year. New records were set in daily visits, average daily visits, and
total weekend visits. Saturdays have become similar to weekdays in urgent care. A major
component of the increase in volume has been the NHIF patients. AICC is no longer accredited
to see NHIF patients, so many are coming to ALMC for care. Staffing has increased to try to
accommodate the increase in traffic. There has been a significant decrease in complaints about
long wait times. The quality of care given has increased, reflecting improvement in training in
the doctors recruited, many from ALMC itself. Administration has responded to the need for
additional personnel by supplying additional doctors in urgent care as well greater numbers of
nursing and support services.
-
2,000
4,000
6,000
8,000
10,000
12,000
JAN15
MAR15
MAY15
JUL15
SEP15
NOV15
JAN16
MAR16
MAY16
JUL16
SEP16
NOV16
OPD VISITS 2015 -2016

ALMC Annual Report 2016 Page 13
3. Highlights:
1. In July, there was a training seminar on Emergency Paediatric Care presented by the
Emergency Medicine Department of Muhimbili. This seminar had been developed by
the Emergency Medicine Association of Tanzania (EMAT). It was attended by 2
doctors from Urgent Care, who received certificates at the end of the sessions. One of
the doctors has subsequently been teaching highlights from the session to the rest of
the staff every 1-2 weeks during the weekly in-service for Urgent Care.
2. The piles of files on the floor in the medical records have new shelving in a new
storage room, freeing up workspace and making the area safer and the files more
secure.
3. Ideas are being developed for decreasing the reliance on paper records, thereby
freeing up space and improving availability of records throughout the hospital. A
plan had already been developed for purchasing a scanner, developing an interface
with Care2X and training personnel to use it. Towards the end of the year, though,
ALMC also received an offer from a commercial scanning business to manage the
scanning program completely. We are still awaiting an onsite evaluation by this
business.
4. On the consultant side, clinic/appointment time has been further expanded for Internal
Medicine, Dental and Otolaryngology, thus making it easier for patients to see
consultants in these areas.
5. A triage nurse has been hired and a job description written. This had been reviewed
by Matron, but she requested revisions. They have been made, but not seen by her
yet.
6. 24 hour presence of CRDB personnel to set up patient pay cards had been achieved at
the end of the year.
7. A protocol book has been started and placed in the Urgent Care area. The doctors
have been made aware of it. It is rudimentary, but hopefully over the next year of
teaching a number of protocols will be added to it for reference.
8. Paediatrics has improved its availability to Urgent Care, improving care to the
youngest and most needy patients.
4. Challenges:
1. Patient waiting time as well total time spent in urgent care, and to a lesser extent on
the consultant side, remains a continuing, but improving problem requiring multiple
approaches to solutions. The issue has been impacted on by the increase in patient
visits again in 2016. Sometimes NHIF connections are not functioning causing delays
in approval. There have also been complaints from the cash patients who do not like
going into 2 lines, 1 for CRDB and the other for the cashier. Despite the fact that any
bankcard can be used for payment, patients are rarely, if ever, told that they can use
their personal bankcard.
2. Consistency and quality of support personnel also remains a problem, but also
improving. There still are personnel who do not look at the service as a ministry to
the sick and needy. There is variability among staff in terms of consistent and
competent care and attitude towards patients and toward their positions of service.

ALMC Annual Report 2016 Page 14
3. There are still a number of patients who leave without paying for lab and xray
although this has been decreasing.
4. Despite increasing availability on the consultant side with commensurate decrease in
waiting for appointments there still are some consultants with a long delay in
appointment time to new or follow-up appointments. This is particularly a problem
with Internal Medicine and Obstetrics-Gynecology and to a lesser extent in
Paediatrics.
5. There is still a significant problem of lost/misplaced files.
6. There are also errors in scheduling, including double-scheduling, scheduling at wrong
times and scheduling on holidays. This has been discussed several times with the
heads of medical records/reception.
5. Plans for the coming year
1. The issue of scanning of medical records should be resolved by the first quarter of the
year after receiving and reviewing the expected proposal by the outside scanning
business.
2. Further analysis of utilization of voice recognition dictation on our computers (Dr.
Matthews) will also be taken up.
3. It is hoped that a way to curb patients from walking out of the hospital without paying
can be found through existing avenues within the hospital protocols (Finance, IT).
4. Greater attention to OPD training will continue to be undertaken and enhanced at all
levels, from CME through morning report to the very exam rooms themselves.
Attempts to place whiteboards in exam rooms to enhance teaching will be taken up
again.
5. With continuing education and input the procedure/protocol manual will be expanded
and enlarged.
2. DENTAL SERVICES: Dr. Alex Minja
1. Introduction:
The Dental Clinic of the Arusha Lutheran Medical Centre started offering basic dental services
from the “Arusha Town Clinic” building in the year 2000 and has grown into a busy, three-
chair clinic with two dentists.
2. Present status:
1. Two working dental chair at Dental surgeon room and one at Hygienist room
2. One renovated dental chair at Oral-Maxillofacial/Surgery room in a workable
condition
3. Four old and three brand new high speed hand pieces
4. Two slow speed hand pieces
5. Five periodontal Scaler (some of them are tired that alarming for replacement)

ALMC Annual Report 2016 Page 15
6. Two periapical X-ray machine, One installed at Dental procedure room and the
other one which is movable, stationed at X-ray room
7. One working OPG X-ray machine and one that Is not working, Both of them
installed in the X-ray room
8. One Automatic Periapical X-ray developing machine at dental procedure room
9. One refurbished Automatic OPG X-ray developing machine stationed in the x-ray
room
2. Patient flow rate and income generation:
There was a slight constant flow of patients in the dental department with an Impressive
increase in monthly income generated in 2016 (see appendix 1). For example, the average
income generated per month was increased from 16,786,140 TSh in the first half of 2016 to
31,005,883 TSh on the second half of the year that means it was doubled.
3. Efforts for increasing income included:
1. Emphasizing restorative procedures which pay more as compare to extractions.
2. Motivating patients by raising their awareness on oral and health issues in general
3. Improvements on our services that attracts more patients from the city and nearby
districts by based on
4. Good customer care
5. Improved patients-Health worker relationship
6. Friendly handling of patients appointments,
7. Proper and Gentle management of patients
8. Effort for reducing patients appointment collapse
9. On the other hand, raising in NHIF service cost/price list also boost-up our income as
most of our patients are NHIF members
4. Challenges:
1. Between June and September 2016, four hand pieces broken down
2. The use of manual x-ray developing processes impaired quality of Dental image
produced
3. One of the dental chair did not work properly due to the problem of leaking water while
operating
4. There has been on-and-off shortage of sterilization pouch
5. Maintenance and serving of dental equipment
5. Developments:
Despite of the financial challenges that the Hospital has gone through especial in the 2nd half
of 2016, we really extend our appreciation to Administration and Financial Department for
their great consideration and trust that they had on us;

ALMC Annual Report 2016 Page 16
1. We managed to repair two of the broken handpieces by replacing the cartridge including
purchasing one extra cartridge for future use.
2. Two of the damaged handpiece could not get the required spare parts from market
instead; one brand new handpiece was bought in-place of the two unrepeatable
handpieces.
3. On the same effort to ensure smooth running of the clinics, we bought another two new
handpieces from Dentmed-Kenya to make a total of three brand new handpieces and
two repaired (cartridge replaced) handpiece.
6. Future Plans:
1. In order to improve services in the dental Department, we requesting for the regular
availability of consumables and supplies (including sterilization pouch)Between June
and September 2016, four hand pieces broken down
2. To increase effort of introducing more specialized procedures as they cost high and
improve our income generation but also is a way of growing as a referral and specialized
unit.
3. We have already started doing some minor surgical procedure (Cystectomy).
4. To plan for purchasing intra-osseous plate for open reduction and fixation of jaw/facial
bone fractures.
5. Orthodontics is among the highly paying specialty in dentistry that attracts most of
middle and high class families of which most of the treatment are based on cosmetics.
There is a need to focus on investing in that field by planning for purchasing or asking
for donation of instruments and equipment from our Partners in Health (Global Health
Ministries). It doesn’t need recruiting new specialist rather the available personnel in
the department can undergo a short course on it.
6. To revive our plans of establishing Dental laboratory for dental prosthesis. Possibilities
of introducing Dental implant once Dental Laboratory is in place.
7. To introduce oral health information/tips to be displayed on the screen at waiting
room/OPD for patients who attend ALMC that will help in raising their awareness on
oral and health in genera and in return will increase number of patients who demand
for dental treatment/check-up.
B. INPATIENT SERVICES:
The Inpatient Services include:
• General Surgery & Laparoscopic Surgery
• Pediatric Surgery
• Orthopedic Surgery with total knee and hip replacements
• Endoscopic Services
• Intensive Care Unit
• Maternity and Delivery Ward

ALMC Annual Report 2016 Page 17
• Neonatal Intensive Care Unit
• Medicine Ward
• Pediatric Ward
• Physical & Occupational Therapy
The Inpatient Department (IPD) continued well in 2016. Patient admissions were essentially
the same as in 2014. The management is trying to understand the lack of growth in the inpatient
departments. Surgery, it has been noted, had a considerable drop off in admissions. Efforts
have been made to ease the entry into the surgical system through smoother running of clinics,
appointments, and outreach to the referring physicians.
Total Patients throughout the hospital did increase a dramatic 21% to a total of 147,528!
1. SURGICAL DEPARTMENT – Dr. Frank Madinda
The surgical department at ALMC is responsible for all activities related to surgical patients.
One of its major roles is to offer treatment through surgical operations.
1. Functions:
Briefly the department performs the following functions:
1. Seeing patients at the surgery clinics in the outpatient department to initiate
investigations and treatment plans.
2. Surgical Operations: Two major types of techniques are normally used for General
Surgery - Open and Laparoscopic. The Orthopaedic section attends to all patients with
skeletal problems both traumatic and non-traumatic. The third part of the Surgical
Department is Paediatric Surgery and is responsible for dealing with all surgical
problems of children.
56,296
81,619 94,885
105,405 116,693 118,930 122,740
147,528
-
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
2009 2010 2011 2012 2013 2014 2015 2016
TOTAL VISITS PER YEAR

ALMC Annual Report 2016 Page 18
3. Teaching: All consultants are responsible to teach junior staff that are in the department
including residents.
2. Statistics
The department has 4 working theatres, three wards and runs outpatient clinics on daily basis.
Each section is the source of income for the Hospital.
Daily surgical turnover from theatre range from 15-20 operated patients per day resulting in
an overall an average of 250-300 patients per month.
3. Achievements
1. Residency training: The programme is ongoing well and now we have a total of 6
residents.
2. Successful operations with visiting surgeons in Plastic and Orthopedic Surgery.
3. A steady increase in endoscopy cases is maintained.
4. Introduction of Endoscopic Third Ventriculostomy: this is a Pediatric Neurosurgery
technique for potential cure of hydrocephalus in young pediatric patients.
4. Challenges
1. A consistent supply of working materials especially for the theatre.
2. Shortages of drapes and theatre clothes in part due to slow turnover in Laundry.
3. Central Surgical Sterilization Department delays in supplying morning operating sets
leads to late starts to the operating day.
4. Plans:
To improve Surgical Services at ALMC, the Surgical Department seeks to achieve the
following in the future:
1. Creation of a gastroenterology unit within the department.
2. Start urology services.
3. Achieve operational day surgery theatre.
4. Get another orthopaedic surgeon.
5. Improve on the numbers of laparoscopic cases.
2. NICU – Dr. Stephen Swanson
1. Introduction:

ALMC Annual Report 2016 Page 19
Newborn Intensive Care is provided for children who
need more assistance immediately after birth through
the first month of life. Charity cases as well as regular
clients are cared for in the unit which includes:
1. Admission and exam by a Junior Doctor, a
nurse, and consultant specialist.
2. Around the clock monitoring by NICU staff
who are present 24 hours a day.
3. ALMC provides a full range of laboratory,
imaging, and technological support.
4. The NICU provides a full range of technological support including overhead warmers,
incubators, and phototherapy lights for treating jaundice, Bubble CPAP - for respiratory
care, umbilical catheters, and cardiorespiratory monitors.
5. Each mother is provided with a bed in the hospital for round the clock availability.
2. Highlights:
2016 remained a busy year in our Neonatal Intensive Care Unit (NICU), with ongoing
improvements in our capacity to provide the highest level of neonatal available in Tanzania.
1. An increasing proportion of babies surviving that were born premature with birth
weights less than 1.5 kg
2. Seven extremely low birth weight (ELBW) babies surviving in 2016, with an average
birth weight of 845 grams (1 pound-14 ounces).
3. Our smallest survivor ever, baby Swaumu, weighing only 760 grams (1 pound – 11
ounces) on arrival. This beautiful little girl received every aspect of our care in the
NICU (advanced medications, respiratory and fluid support, antibiotics, and blood
transfusions), and was eventually discharged home after nearly 2 months as a healthy,
thriving infant.
4. A continued reduction in our NICU mortality rate across all weight categories, as our
capacity to care for the smallest, sickest neonates continues to improve.
5. The introduction of pulmonary surfactant to our NICU, a complex liquid that is placed
into the lungs of a premature baby to help keep their lungs from collapsing and to
facilitate gas exchange. We are the only hospital in Tanzania using pulmonary
surfactant, an established medication known to improve survival rates in extremely
premature neonates.
6. The development and implementation of additional NICU protocols and medication
guidelines, that standardize and support evidence-based clinical decisions.
7. The arrival of a Canadian NICU nurse, Lisa Giesbrecht, RN. Lisa worked in our
NICU for 1 year, bringing her experience and expertise to improving our NICU
protocols and training our nurses. Her NICU legacy is being carried forward by
another visiting pediatric nurse, Nicole Schank, from Minnesota.
Phototherapy for neonatal jaundice

ALMC Annual Report 2016 Page 20
3.Narrative:
During the year 2016, 209 babies were admitted to the NICU (Table 1), representing an 11%
decline in overall admissions compared to year 2015. Year 2016 represents the first year-over-
year decline in NICU admissions since our NICU first opened its doors in 2010. This reduction
in admissions does not reflect a decline in demand for admissions to our NICU. Rather, our
improving capacity to care for smaller and sicker neonates has resulted in longer
hospitalizations, with fewer beds available to accept new admissions to our NICU because of
improving survival rates. As our NICU mortality rate
declines through advances in nursing skills, improved
clinician education, new protocols and better medications,
we often experience our NICU being at full capacity.
Extremely premature or small babies, especially those with
birth weights under 1500 grams (approximately 3 pounds),
require lengthier hospitalizations. As our survival rate has
improved, our NICU is often at full capacity and unable to
accept new admissions from outside hospitals. Undoubtedly,
there remains a strong need for additional NICU beds in
Arusha. However, future admission growth in the face of
improving survival rates remains dependent on training and
retaining additional qualified nurses and increased levels
of outside funding.
Among the 209 neonatal admissions, 104 (50%) were preterm babies. Forty-five percent of all
NICU admissions were from outside ALMC (“transfers into ALMC”), reflecting a growing
recognition of ALMC’s NICU as offering the highest level of care for critically ill preterm and
term infants in northern Tanzania. Of the 95 neonates referred in to the NICU, most arrived
from Selian Lutheran Hospital in Ngaramatoni. The hospital expenses for these 95 neonates
was fully paid for by the NICU fund (Table 2).
Full term babies represented 50% of all admissions, and included newborns requiring
management of conditions such perinatal/birth asphyxia, neonatal seizures, respiratory distress,
meconium aspiration syndrome, neonatal sepsis, jaundice, and requiring care following surgery
for congenital conditions.
Despite the NICU’s many successes in 2016, 36 of 209 (17%) admitted babies died. The most
common causes of neonatal death in the NICU were extreme prematurity with respiratory
failure, severe birth asphyxia/hypoxic ischemic encephalopathy, sepsis (infection), and
irreparable severe congenital anomalies. Among the 36 neonates who did not survive, 58%
(21/36) had a birth weight of less than 1500 grams.
Mama Vicky with her 790-gram baby
girl.

ALMC Annual Report 2016 Page 21
Year 2016 represented a milestone for us in many respects. We had 7 extremely low birth
weight (ELBW) newborns survive and “graduate” from our NICU, with an average birth
weight of 845 grams (1 pound- 14 ounces). Our smallest survivor ever left our NICU after
nearly 8 weeks of hospitalization, having been born 13 weeks premature with a birth weights
of 760 grams. Another 25 babies with birth weights between 1000 – 1499 grams also were
successfully treated and discharged home to grateful parents. Our increasing capacity to care
for babies with very low birth weights has meant that our NICU remains busier, with more
beds occupied due to preterm neonates. This has also resulted in many mothers, who having
lost multiple prior pregnancies due to preterm labor, now being able to gratefully bring a baby
home that otherwise would likely have not survived.
NICU Admission and Outcome Data - 2013-16
Year Total
Admissions
Premature
Neonates*
(%)
Birthweight
<1500 gm
(% of total)
Transfers
into ALMC
(%)
Deaths
(%)
Surgical
2016 209 104 (50%) 53 (25%) 95 ( 45%) 36 (17%) 4
2015 236 74 (31%) 29 (12%) 119 (50%) 48 (20%) 20
2014 222 75 (34%) 36 (16%) 111 (50%) 53 (24%) 18
2013 117 49 (42%) 17 (15%) 25 (21%) 22 (19%) 11
The NICU Fund was started in response to families who are unable to pay for the cost of
hospitalization of their babies. The NICU fund covers all costs of NICU hospitalization and
mother’s hospital meals, and is fully supported by outside donations and fund-raising efforts.
The NICU’s overhead warmers, incubators, and phototherapy lights were in continuous use
throughout the year (Table 2). In 2016, the NICU received a donation of additional
phototherapy fiber optic pads (“Biliblankets”) from Global Health Ministries. The use of
pulmonary surfactant for babies with severe respiratory distress syndrome due to prematurity,
and meconium aspiration syndrome, was made possible through financial donations from
Church of the Cross (Hopkins, MN) and Christ Lutheran Church (Visalia, CA), as well as
through the equipment and training generously offered by Dr. Kari Roberts (Neonatologist,
University of Minnesota).
The NICU at ALMC faces many challenges in the coming year. We continue to experience
ongoing personnel needs in nurses and physicians with experience in taking care of critically
ill and extremely preterm neonates.
Finding and training Tanzanian nurses to care for the increasing complexity and census of our
NICU babies remains a significant challenge. NICU nursing care demands a level of skill,

ALMC Annual Report 2016 Page 22
dedication, and training that is widely recognized and appreciated throughout ALMC. It is the
only unit in the hospital that employs the routine use of central lines (umbilical venous
catheters), intravenous pumps, continuous positive airway pressure, and is likely the only
NICU in all of Tanzania with this level of advanced newborn care. The demands on the NICU
nurses are great, and finding enough skilled, motivated nurses remains an ongoing challenge.
Our NICU remains constrained in its growth in no small part due to a lack of qualified nursing
staff—the unfortunate reality is that we are often unable to accept requests for an admission of
a critically ill neonate from outside hospital simply due to shortages in nursing staffing.
An additional NICU challenge faced is raising adequate funds to support our increasing number
of charity cases. In 2016, 35% of all newborns admitted to our NICU received partial or full
financial support to cover their hospitalization expenses. Many of these neonates had NICU
hospitalization length of stays of 1 month or greater. Last year, our NICU provided $70,000
in free medical care to hospitalized neonates. As such, these expenses were paid for through
individual donations and outside grants to our ALMC NICU fund. Future growth in our NICU
depends on continued donations to support the costs of caring for these critically-ill neonates.
It is worth noting that our annual NICU budget is less than the cost of a single NICU
hospitalization in the United States, but allowed us to care for 209 neonates in 2016!
In 2017, we look forward to continuing to provide
the most advanced newborn care in northern
Tanzania. Additional manikin simulation preterm
dolls have been obtained through Laerdal
Medical, that will allow our nursing and
physician staff to practice further essential
lifesaving resuscitation skills, such as bag-mask
ventilation, intubation, cannulation, medication
delivery, and clinical decision making. We
continue to recruit overseas nurses and doctors to
join us in efforts to improve our care of neonates.
We hope to hire more NICU nurses,
expanding our daily census capacity. 2017
looks to be another productive year in a busy
neonatal intensive care unit, caring for the smallest of all possible patients.
4. OBSTETRICS AND GYNECOLOGY: Dr. Charles Sweke
1. INTRODUCTION:
Encouraging mothers with their NICU babies.

ALMC Annual Report 2016 Page 23
The OBS/GYN Department consists of 2 consultants, 1 registrar, one or two interns at a time,
plus one or two medical students. Nursing consists of: 8 Registered Nurses, 3 Enrolled Nurses,
3 Nurse Attendants, and 1 ward.
The department works 24 hours a day. It has 8 wards, of which 4 are two-bed-rooms and 4 are
three bed –rooms; labor ward plus one family-room.
The consultants are full time available during day time except in the night, weekends and on
public-holidays when one consultant is on call. The registrar and interns are full time in the
department, Nurses work on shift: morning, evening, and night shifts
The department has two consultant’s clinics in a week, Tuesday and Fridays; has got 4 days of
elective surgeries and full time daily for emergency surgeries.
2. ACHIEVEMENTS:
2016 has been a busy year in our department, so busy that our wards have been fully occupied
most of the time. Often, to the extent that some of our patients had to be admitted in different
departments of the hospital. Many patients who had been attending at other medical centers
had been coming to our hospital precisely to our department showing their trust in the services
we offered.
Another achievement we had in order to improve our capacity for providing good services, is
4 of our nurses underwent training seminars in Post abortion care. These nurses have already
started actively implementing the skills they learnt. MVA services have been started in the
department instead of being done in the theatre as it used to be before.
3. CHALLENGES:
Shortages of supplies, certain pharmaceuticals, and delivery sets with appropriate instruments
have been a challenge at certain times during the year. Ward space is another challenge, as
mentioned above. The wards we have do not meet the demand, as often our patients have been
admitted to different departments which gives inconveniences not only to patients but even to
service providers. Staff is another challenge, we request to have more qualified nurses
particularly midwives and at least one more registrar (MD).
4. HOPES FOR 2017:
It’s our goal to give best and highly quality services to our patients attending to our hospital.
In order to achieve this, we hope to get support from the administration by having us the
following:
1. Delivery sets with appropriate instruments
2. More qualified nurses (midwives)
3. One more registrar (MD)

ALMC Annual Report 2016 Page 24
4. If possible to have Gynecological Wards at least 2 wards, so that the current wards
remain Obstetric wards
5. Drugs problem be solved
5. PAEDIATRICS DEPARTMENT: Dr. Derrick Matthews
The Department of Paediatrics went through a number of changes over the past year, changes
in personnel, location and services.
1. Personnel
Dr. Steve Swanson and Dr. Derrick Matthews, both board-certified pediatricians, continue to
serve the department. Dr. Elena Mantz returned to Australia in March after a 6 month shortened
stay.
There has been turnover in the registrars. Dr. Christina Hongella was accepted to a paediatric
residency in Uganda and started there in August. Dr. Amon Jackson continues to work with
us. Dr. Vidda Mbaruku left in mid-December for a job in Dar Es Salaam. Dr. Theresia
Ndakidemi transferred from Urgent Care service to start as a registrar in Paediatrics at the
beginning of December. In addition, Dr. Maria Dillmann, a resident in paediatrics from
Germany will be with us for 6 months until March 2017. She started in November of this year.
All these doctors will work closely in the overall paediatric program at both ALMC and Selian
Lutheran Hospital together with Dr. Theresia Laizer and Dr. Victor Urio, who continue to work
as registrars out at Selian Hospital in Ngaramtoni.
2. Achievements:
1. International Postgraduate Paediatric Certificate: The IPPC program was started
by Dr. Mantz shortly before her departure. The program is a more formal course of
training in paediatric medicine via internet and DVD lectures as well as local tutorials.
The goals are to improve the care given by them in the hospitals as well as improve
their ability to enter into a good paediatric residency program. Dr. Matthews is
currently the main tutor in the program. There are 4 participants—2 of the registrars
at ALMC (Dr. Hongella and Dr. Mbaruku), 1 from Selian (Dr. Laizer) and 1 intern
finishing up her year at ALMC (Dr. Farida Abdallah). They have all completed and
passed 2 written health reports. 3 out of the 4 have passed their oral exams. They are
awaiting the results of their written exam now. Dr. Hongella has deferred her exams
because of her commitment to the paediatric residency in Uganda this year.
2. NICU: Full term babies continue to be >50% of admissions. Transfers are coming
several different hospitals in the area, including our first from Shree Hindu Union.
Two children have successfully received surfactant, a treatment for immature lungs in
premature infants. 2 exchange transfusion treatments for severe jaundice were also
done this year. 8 babies with birth weights under 1kg ‘graduated’ this year, including

ALMC Annual Report 2016 Page 25
1 with a birth weight of 660g. More details about the NICU are in the report put
together by Dr. Swanson.
3. Paediatric Ward Service: The paediatric ward service is becoming more of a
referral service with more complex/less mundane conditions. Part of this is because of
the reputation of the paediatricians. We are getting referrals from all over northern
Tanzania. In addition, because of better training in the urgent care doctors, they are
able to handle or properly refer children rather than admit them “to see the
paediatrician.” There has been increased paediatric medical surveillance of the
surgical cases, but there is still room for improvement and greater consistency. In
addition, there was some cooperative work with hospitals in Kenya, both Tenwek and
Kijabe for patients who could not get the care they needed at ALMC. Both cases had
successful outcomes.
4. Serving with Selian Lutheran Hospital: Paediatrics continues to support the
services out at Selian Lutheran Hospital in Ngaramtoni. Drs. Swanson alternates
weeks doing rounds out there. There is also support from University of Minnesota
chief residents in Med-Peds to both paediatrics and adult medicine. Drs. Swanson
and the chief residents give support to visiting residents from the Minnesota pediatrics
and Med-Peds residency programs.
5. Paediatric HIV/AIDS: Dr. Matthews continues to see paediatric HIV/AIDS patients
in 2 clinics a week in Arusha Town Clinic. The program has been decimated by the
pull out of USAID from funding the program. The program at Selian in Ngaramtoni
is growing because it is government based. Because ALMC is private it receives no
funds from the government, only medication and tests (another challenge). Patients
are slowly trickling back as parents are seeking insurance for coverage. Otherwise
patients are coming for medication only without any surveillance.
6. Care at Plaster House: Because of lack of paediatrician personnel Plaster House
clinics have been decreased. Plaster House patients continue to be challenging
because of a mixture of sometimes
complex conditions. It is hoped that the
clinics can continue in the future with an
increase in personnel.
7. Teaching: Teaching continues to be at the
centre of the paediatric program.
Consultants teach registrars and interns.
Registrars teach interns and students. The
students are nurses and visiting students
from the United States and other countries.
3. Challenges
1. Challenges remain for the paediatric department, particularly in the area of personnel.
Retaining registrars for a committed time of service is sometimes difficult and
unpredictable, as has been demonstrated in the past year. Nursing turnover in the
NICU, like many other parts of the hospital has become critical and crippling at times.
Very few of the current nursing staff were in the NICU even as short as a year ago.

ALMC Annual Report 2016 Page 26
Turnover can have an increased impact on a service like the NICU, which requires
specialized training obtainable in very few, if any institutions in Tanzania.
2. Consultant services are also an area of concern. From the start of the hospital in 2008,
there has yet to be a Tanzanian paediatrician on service. The absolute number of
consultants dropped back to 2 after Dr. Mantz left in March of this year. This has had
an impact in several areas, including teaching responsibilities (registrars, residents,
nurses and students), consistent consultant coverage of paediatrics at Selian Lutheran
Hospital, coverage of Plaster House and consultant surveillance of the HIV clinic at
Selian.
3. The NICU continues to be a financial challenge, with many admissions, including
patients born at ALCM, finding it difficult, if not impossible, to pay for services.
While funds have been raised to support these patients, some are not officially eligible
for the funding. In addition, the funds generally run out early in the year because of
the high cost of service. Tied into this is the reimbursement rate received from NHIF,
which under supports the service.
4. General availability of paediatric medications in child friendly formulations has
improved, but remains a challenge. Stockouts of routine medications (e.g., as of this
writing there is no paediatric zinc) are all too common and results in time spent
writing prescriptions for patients to find their medications outside of the hospital.
This also represents potential revenue loss to the hospital.
7. PROGRAMS AT ALMC
A. AIDS CONTROL PROGRAM (ACP) – Prof. Mark Jacobson – Director ACP
1. ACP Contract with USAID Ended:
2016 was a dramatic year for the Selian AIDS Control Program (ACP) as its 10 year
partnership working with the United States Agency for International Development
(USAID) ended on 30 September 2016. The USAID, for ten years has been the sole funder
of the ACP and at a significant level of funding. Although there was anticipation and a
period of preparation for this change, it still produced major challenges, downsizing of
staff, and a great decrease in services.
The ACP is a Diocese-wide response to HIV and AIDS. It provides a full range of
integrated services including:
1. Prevention and Education
2. Prevention of Mother to Child Transmission of HIV
3. Voluntary Counseling and Testing
4. Care and Treatment with Antiretroviral Therapy
5. Care for Orphans and Vulnerable Children
6. Hospice and Palliative Care

ALMC Annual Report 2016 Page 27
Already in 2015, the Voluntary Counseling and Testing and the care of Orphans and
Vulnerable Children components had already been eliminated from funding but continued
as a smaller part of the ACP.
2016 was largely focused on managing this huge change. Throughout the year, the ACP
was led to believe that there would be a successor partner to USAID who would need to
take on the SACP as a subcontractor. But delays in the process of selecting new project
carriers meant that from October onward, there was no external funding available for the
ACP.
This of course resulted in a major reorganization of the ACP reduction in services. By far
the greatest impact is felt in the following areas:
1. Orphans and Vulnerable Children program suspended.
2. Hospice and Palliative Care Program:
a. Discontinued working with over 250 volunteers.
b. Reduction in patients under active care and visitation from 4,000 to 1,000.
c. Reduced staff by one third.
d. Reorganized into two loosely linked teams at Selian and at ALMC.
3. The Care and Treatment Centers at ALMC, Selian, and Kiruruma have had to
downsize and are considering which will be able to remain open and providing
services.
4. Overall, the staffing was reduced in the program by 70%.
Throughout this year of upheaval, the Selian AIDS Control Program did indeed continue
to serve and intends to continue serving into the future. For much of the year the program
still provided a full range of comprehensive, integrated, high quality care and support,
together with preventive education. Care is provided through “one stop” services provided
at three centers based at Selian, ALMC, and Mto wa Mbu. The program provided various
services to 45,000 people in four government districts and 42 wards! The statistics for the
year are quite impressive for a program which was dramatically downsizing.
1. Prevention of Mother to Child Transmission: 2.341 women were screened.
2. Hospice and Home Based Care: 2,720 patients were cared for in their homes by
300 volunteer providers.
3. Care and Treatment: There are currently
3,496 patients receiving services in
2016. Of these, 3,247 are on therapy.
Pediatric cases of HIV have been a focus
of care again this year with 242 on ART
therapy (an increase of 48%).
4. PICT: The “Provider Initiated
Counseling and Testing” model
recruited 15,233 hospital attendees for
HIV screening.

ALMC Annual Report 2016 Page 28
The summary estimates of the numbers served during the past ten years is outstanding:
1. Education: > 500,000
2. VCT: > 240,000
3. PMTCT: > 16,000
4. ART > 7,000
5. OVC > 6,000
6. HBC/PC Current > 4,700
2. The Way Forward:
The Selian AIDS Control Program is a program that is a diocese wide program and the
diocese leadership, the health department leadership, the leadership of the hospitals, and
the ACP leadership are all committed to seeing it continue. However, it will continue on a
smaller scale and will need to seek alternative funding sources.
Strategies Include:
1. Joining with another USAID funded partner. This has already been determined to
be the Elizabeth Glazer Pediatric AIDS Foundation (EGPAF). Preliminary
discussions have begun and it is anticipated that there will be some support for Care
and Treatment Centers together with TB care and Family Planning.
2. The Care and Treatment Center at ALMC will need to be assessed as to its longer
term financial viability and may need to be much reduced in scope.
3. The management of the ACP will remain at Selian with ALMC and Kiruruma
collaborating with the central management based at Selian.
4. Hospice and Palliative Care:
a. Will be separate from the ACP. They will have a team at ALMC and one
at Selian with the leadership and offices still in Ilboru at the Hospice and
Palliative Care office.
b. Will shift their focus to end of life care and will continue with a core of
volunteers whose numbers will be determined by the success of obtaining
donor funding.

ALMC Annual Report 2016 Page 29
B. PLASTER HOUSE – Ms. Sarah Rejman - Director
1. Introduction:
The Plaster House provides high love, low cost,
efficient and ethical surgical health care that
significantly changes the lives of many disabled
Tanzanian children. It is said, “build and they
will come”, this is certainly the case with The
Plaster House, 2016 was another exceptionally
busy year; we increased by close to 50%, the
number of cases we treated through the
subsidized surgery programme.
Our strong staff of 21 managed the daily challenges of looking after so many children with
disabilities, with calm love and presence. It is a credit to them, that The Plaster House remains
a hopeful haven for children with disabilities and their parents.
2. Achievements of 2016:
1. Treatment: Patients continued to pour in through our gates at The Plaster House.
Following our own adage, that ‘we never turn a child away’, we assessed and treated
over 700 cases of children, with varying disabilities,
who required surgical intervention and
rehabilitation.
2. Clubfoot Training Centre: The work of Jaclyn
Lekule, Occupational Therapist, in clubfoot
treatment with Ponsetti method has continued to
grow. The Plaster House’s clubfoot clinic has been
acknowledged and identified by the Tanzanian Club
Foot Association to be a future training site for
therapists from around the country.
3. Visitors: We have loved having visitors spend time
with us, understand our programme and take our
story around the world. We enjoyed a visit from
John Feakes, the Australian High Commissioner
based in Nairobi, and a team from Watsi and Tencent who are great friends of our
children and programme. Young filmmakers, Tom Attwater and Lane Brown, visited
and produced an inspiring short film on The Plaster House story.
4. Fundraising: We have had awesome fundraising energy and support from our
friends in Arusha and abroad. Locally, we had a fundraising evening at The Arusha
Coffee Lodge, we walked the 5km fun run at the Kilimanjaro marathon, we had great
exposure at the Movember fundraising event, and the Arusha Community Fair. For
the first time we took The Plaster House story on tour through the USA. We were
generously hosted in 6 cities, and we made lots of friends and raised money for the
expansion along the way.

ALMC Annual Report 2016 Page 30
5. Volunteers: Our programme is developed, strengthened and expanded by long-term
professional volunteers. In 2016, we had input from occupational therapists, Carmen
Messachalk, Mary Rourke and Keira Dispirito, and nurse Ingela Skarpe. Hannah
Kelly joined the team as our first ‘Australian Volunteers International volunteer,
working with the nursing team and helping to strengthen our outward communication.
Gail Gettler shows unending energy with supporting our fundraising effort in the US
for the expansion fund.
6. Outward communication: We established a regular newsletter for our friends and
supporters, and have increased our presence on social media. This has improved our
visibility and has shown results with increased donations and patient referrals.
7. Outreach: We continued to provide
education and support to people
living with disabilities through our
established outreach programme.
The Rehab Surgery Programme is
known in over 200 communities
around central and northern
Tanzania. Our outreach programme
continues to be a very strong
recruitment tool for our subsidized
surgery programme.
8. Community Awareness: In 2016,
we took our children ‘to town’ to educate the greater community (especially children)
about people with disabilities; we played football at the International School of Moshi
– Arusha Campus (ISMAC), went to Little Oliver’s Camp in Tarangire with Asilia
and ISMAC, and we have had two of our big boys in work experience in the
workshop at Edutours in Arusha. We have groups of students from ISMAC visiting,
working with and learning from our children in the surgery programme on a weekly
basis.
3. Challenges
1. Overcrowding: We were challenged
again this year with consistently dealing
with more patients than we expect in our
programme. Our rule to ‘never turn a
patient away’, meant that again we have
had safari tents borrowed from our
friends at Tanzanian Game Trackers
Safaris on our grass courtyard.
2. Staff absence: We were challenged by
the unexpected and extended sick leave
of an integral member of the
administrative team that began in September. African Mission Healthcare Foundation
provided great support to us during this very challenging time.
3. Communication and Collaboration: We continue to seek to establish best
communication and collaboration with all of the ALMC staff. We have enjoyed the

ALMC Annual Report 2016 Page 31
support of ALMC leadership as we have worked to improve in all areas of
communication to provide the bast care for our patients.
4. Extra Special Children: We were challenged into reflecting on the care
requirements of children in our programme with very complex needs and care
requirements, who often fall outside the parameters of the funded surgery programme.
These children require longer and more care than we often have funding to provide –
and yet we cannot turn them away, as we
are usually the only chance they have at a
better life.
5. Administrative Reporting: We were
challenged by a lack of internal systems in
the Rehabilitative Surgery Programme,
making all administrative reporting and
statistic rising challenging – especially with
a programme that continues to grow with
each month.
4. Plans for 2017
1. Staffing: Increase staffing to adequately cover our peaks in patient numbers and in
anticipation of programme expansion following the construction with:
2. Administration: Programme Co-ordinator and Programme Administrator
3. House mothers: 5 housemothers to join our team of 5 already employed
4. Ancillary: Housekeeper, Guard and Gardener
5. Medical: Therapist and Nurse
6. Medical and Administrative policies and procedures: Reflect, review and
formalize the systems for the day-to-day management of The Rehab Surgery
programme and The Plaster House. Develop and launch an Integrated Care Pathway
to standardize the care of children under the subsidized surgery programme.
7. Construction: Stage II of The Plaster House: volunteer accommodation, bunkrooms
for patients, and increased clinic and administrative space.
8. Community Presence: Streamlining outward facing communication and solidifying
the Plaster House brand to enable us to be easily identified, thereby increasing global
awareness, and enabling us to grow our programme.
9. Launching the International
Advisory Board: The members of the
International Advisory Board have
been identified and have agreed to sit
as experienced advisors to the
programme. This year will have the
parameters of the Advisory Board
established and the Board launched.

ALMC Annual Report 2016 Page 32
C. HOSPICE AND PALLIATIVE CARE – Ms. Elizabeth Makule - Director
1. SUMMARY
Selian Hospice and Palliative Care (SHPC) works under Arusha Lutheran Medical Centre
(ALMC) which is a Faith Based Health institution. mission “Selian Hospice and Palliative
Care Program is committed to provision of holistic, care to people with life threatening illnesses
through competent and passionate palliative care and enhancement of community services in a
manner that proclaims the Gospel”. The program started 1999. The program aims at
maximizing the quality of life, restoring hope and relieving the suffering of patients with life
limiting incurable diseases and support to their families.
The year 2016 was dramatically impacted by the conclusion of the 10 year long association
with the United States Agency for International Development (USAID). The majority of the
SHPC funding had been provided by USAID through the AIDS Control Program. With its
conclusion, the SHPC Program has needed to downsize dramatically and reduce services. This
came into effect from October and so, there is still a significant amount of service to report on
for 2016.
Selian Hospice and Palliative Care Program continued to
provide Hospice and Palliative Care in two (2) Districts of
Arusha region Namely Arusha City and Arusha DC the other
two districts Monduli in Arusha and Simanjiro in Manyara
regions were left due to limited funds.
Throughout 2016, the Program was providing services to 5,153
clients, majority being HIV and Cancer patients.
Since October 2016 the programme provide hospice and palliative care to only 2,418 clients,
focusing end to life care patients and this is due to cut off funds from USAID who were major
funder of the programme for the past ten (10) years.
The programme comprise of Professional team of nurses, clinicians, social worker and spiritual
leader who are responsible for service provision, capacity building to other staff and
communities. The team also conduct supervision to home based care volunteers in the
catchment area who are purely volunteering without payment. Strengthening the linkages
within and outside the health care system has been very effective in ensuring continuum of care
for clients suffering from chronic illness.
The services provided through Day care and Home visits included Psychological care, Pain
Management and symptoms control as well as prevention through education and counseling.
Several referrals were made to those who needed further managements.

ALMC Annual Report 2016 Page 33
Palliative care introductory training course were done to 20 people among them Male were 9
and female 11others were from Government and Non Government. health facilities with the
collaboration of Tanzania Palliative Care Association and the Evangelical Lutheran Church of
Tanzania Palliative Care Department.
Sensitization meetings were conducted in several Wards in Arusha District. The main
objectives of the meetings were to discuss about Sustainability and Ownership of Hospice and
Palliative Care Activities to the Local Government leaders and Religion leaders.
2. ACHIEVEMENTS:
1. The programme managed to provide services to 2,418 were clients, Male were 1,053
and 1,365 were Female.
2. 48 Day care occasions were conducted in this reporting period.
3. 120 clients supported with Nutritional food -a contribution by the community members.
4. The total number of 209 new clients were identified and registered.
5. Volunteers and supervisors monthly meetings conducted, reports collected and
compiled by the supervisors up to closure USAID Project funds in September 30th 2016.
6. Monitoring and supervision done monthly.
7. Income Generating Activities through VICOBA training was conducted to 3 groups of
30 clients each, the groups were from Moivo, Olorien and Kimnyaki.
8. Sensitization meetings were conducted to 14 wards in Arusha DC.
9. Palliative care introductory training course conducted to 20 Health professionals from
Government and Nongovernmental health facilities with the collaboration of TPCA and
ELCT Palliative care programs.
3. CHALLENGES:
1. The end of USAID funding for the project which requires a reconfiguration and
dramatic decrease in services and clients served in 2017.
2. This in the face of increased demand of Hospice and Palliative care services.
3. With no USAID funds, the limited resources from other donors are insufficient to meet
t the demands.
4. Poverty is still a problem to most of the families in the program areas.
5. Stigma is still a problem in many areas despite the sensitization and education provided.
6. With reduction in funding there now remain insufficient numbers of staff and
particularly volunteers to follow up clients.
4. HOPES FOR 2017:
1. Write proposals to solicit funds for more sustainability.

ALMC Annual Report 2016 Page 34
2. Continuing providing holistic and quality Palliative care and Hospice services focusing
to end of life care.
3. Provide medical treatment and referral to the needy patients.
4. Community sensitization and mobilization for the programme sustainability and stigma
reduction.
5. Quarterly meetings with other NGOS, CBOS providing the same service.
6. Continue providing Introductory Palliative care training course to Health Professionals
annually (self-sponsor).
7. Monthly supervision, monitoring and evaluation of the Program implementations.
D. FISTULA AND BIRTH INJURIES
Care for women with birth injuries and the terrible tragedy of incontinence due to fistula
formation during difficult deliveries has grown again in 2016. Under the direction of Dr.
Andrew Browning, the cases served in 2016 grew to over 200. The Program is primarily based
at ALMC’s partner hospital, Selian Lutheran Designated Council Hospital. It has successfully
introduced significant improvements not only in fistula care but in midwife development and
training. Through this Program, Dr. Browning continues to provide surgical care for women
with this problem throughout Africa with regular surgical visits to Kenya, Ethiopia, Malawi,
and other parts of Tanzania.
8. CHAPLAINCY AND SPIRITUAL CARE
ALMC seeks to serve all patients holistically – in body, mind, and spirit. Hence ALMC
includes a strong chaplaincy programme in its care of patients. ALMC begins the workday
in chapel for a time of prayer and reflection on God’s call to serve others with love and
compassion. Chaplain Gabriel Kimirei and his team do daily rounds for time of prayer and
support with every ALMC patient and family. The chaplaincy team is constantly available for
crisis counseling, spiritual support, and comfort in bereavement.
9. MEDICAL EDUCATION
ALMC continued making great strides in promoting its education ministries in 2015. ALMC’s
mission statement commits to striving for excellence in providing care, research, and education
for the health needs of the Arusha community. Education is a critical priority. The School of
Nursing is about to graduate its first class of nurses. The Surgical Residency is expanding each
year. Other continuing education efforts are going forward well!

ALMC Annual Report 2016 Page 35
A. SCHOOL OF NURSING: Lilian Shuma, Principal:
1. Introduction
The Arusha Lutheran Medical Centre School of Nursing is under the ALMC Training Center.
The School of Nursing seeks to produce high quality nurses who will assist in raising the
quality of health care and alleviate the shortage of health care workers in Tanzania.
2. Vision
The vision of the School of Nursing is to graduate nurses who meet or exceed the highest
standards of the nursing profession.
3. Mission
The mission of School of Nursing is to furnish nursing student candidates with a high quality
education that will allow them to practice as
Patient Centered nursing professionals.
4. PROGRAMME OFFERED
Arusha Lutheran Medical Centre school of
Nursing offer the following programmes:
1. Pre-service Technician certificate in
nursing program:
2. Community Health Technician: 1 year
The School has 94 students enrolled:
15 second year certificate students
44 first year certificate students
35 community health certificate students
The School of Nursing has five permanent teaching staff, six part time teaching staff, and
seventeen clinical staff.
5. Achievements
1. ALMC-SON granted full registration with NACTE
2. Second intake of Nursing sat for their final exam 1st class on March 2016 and 2nd class
on August 2016

ALMC Annual Report 2016 Page 36
3. Results of final exam for 1st Intake was good they all passed
4. 1st intake of community health Programme sat for their final exam in October 2016
5. Increased number of tutors to five
6. We received new intake of nursing
about 44 students and Community
health 35 students and welcome them
on 27 October 2016
7. Various visitors from inside and
outside the country visited ALMC-
SON and assist the school in variety
areas such as equipment, teaching and
sponsoring of students.
6. Challenges
1. Failure to win an ASHA grant for assistance in construction of our own campus has
set back the plans for construction
2. Some students fail to pay school fees
3. Lack of enough accommodation for male students
4. Lack of enough water supplies and reserve tank
for water
7. Hopes for 2017
1. To have our own school building for
sustainability of school. The current plan is to
renovate the nearby Lutheran secondary school
into our own nursing campus.
2. To apply for Full accreditation from NACTE.
3. To have Diploma nursing programme in ALMC-SON.
4. To have school projects so as to increase school income vegetable garden, school
shop or stationary.
5. To continue produce nurse graduates who will provide higher quality of nursing care.
6. To continue work hard has a team to meet institution goal.
B. SURGICAL RESIDENCY:
2016 saw the continued growth of the ALMC Pan African Academy of Christian Surgeons
(PAACS) residency in surgery. The residency is under the leadership of two ALMC surgeons,
Dr. Frank Madinda and Dr. Wendy Willmore. The training program is accredited by the

ALMC Annual Report 2016 Page 37
College of Surgeon for Eastern, Central, and Southern Africa (COSECSA) which is the
international surgical college for southern Africa. The curriculum intentionally focuses on
training highly qualified surgeon who are also Christian leaders in their hospitals and
communities.
Academics: The purpose of Arusha PAACS is to train Christian surgeons in Tanzania for
Africa. We are a partnership between Arusha Lutheran Medical Center, Pan-African Academy
of Christian Surgeons, Selian Lutheran Hospital, and the College of Surgeons of East, Central
and Southern Africa.
The training program consists of 3 facets. The most time consuming facet is the academic
curriculum. This educative facet aims to impart the knowledge of anatomy, physiology,
pathophysiology, continually changing treatment regimens, treatment environment and
research skills necessary for the mastery of a surgeons’ calling. This knowledge is tested by 2
exams – the yearly PAACS exam and the COSECSA exams sat by 2nd and 5th years. Our
residents can take pride in a job well done as they came out with very high marks. Emmanuel
Lema got the 2nd highest score on the senior exam and all the juniors passed the junior exam,
altogether giving our guys the best performance in all of PAACS! Our second year residents
went on to be tested by the Membership of the College of Surgeons Exam. All passed this
year, giving cause for great celebration.
Spiritual: The second facet of training is the spiritual curriculum. We realize that the question
is not “Will our residents be spiritual leaders in their hospitals and churches?” but “What kind
of leaders will they be?”. The spiritual curriculum aims to give them the tools to be moral
leaders with a sound understanding of the basics of theology and Christian praxis. This facet
of the program also addresses some of the needs that we all have for corporate pastoring and
reflection on our calling as Christian surgeons. We accomplish this through weekly Bible
Study, following the spiritual curriculum and prayer, as well as a short and long retreat every
year. All of the above took place in 2016, and this year we managed to complete the curriculum
for the year. We did have to discipline one of our residents for moral failure, unfortunately, but
the process was managed with grace.
Apprenticeship: The third facet of Arusha PAACS is probably the most important. This is
the traditional apprenticeship style learning that takes place in the context of looking after
surgical patients. The faculty have been mentoring and training our residents to develop better
Christ like care of the patient’s whole person, including sound clinical judgement and skillful
operative expertise during the past year. Currently our residents are evaluated at least every
three months by the faculty member to whom they are primarily attached at that time. In
addition to this, all surgical house staff are informally evaluated by their seniors at the end of
each month. In the opinion of the faculty, the residents have been progressing well. One of
the first years had to repeat his initial probation, however, placement of him with our senior
resident on call helped to correct the deficiencies that we saw.

ALMC Annual Report 2016 Page 38
C. ALMC HOSPITAL BASED CONTINUING EDUCATION:
ALMC provides regular “in house” continuing education for both medical and nursing
personnel. There are weekly training sessions for nurses and doctors. The year saw
continuation of the innovative “Morbidity and Mortality Conference” to review complications
and problems arising in the care and outcomes for patients at ALMC. Several important
surgical skill courses were provided for medical staff with the provision of Basic Surgical Skill
certification and Obstetrical Skills certification. NICU Nursing training was provided for 12
staff as ALMC seeks to fully staff its NICU and Pediatric Ward.
D. PEDIATRIC SEMINARS:
The Pediatric Department of ALMC has been holding Wednesday morning Pediatric
Residency level training for registrars, interns and residents. This represents one of the premier
training programs in Pediatrics throughout the country.
E. CONTINUING EDUCATION THROUGH UPGRADING AND SCHOLARSHIPS:
ALMC provides many opportunities for staff to go for long term upgrading courses. In 2016,
ALMC had 8 staff in training for various positions in laboratory, nursing, or medicine. Six
doctors were in specialty training: Dr. Peter Makanza has been sent to study Orthopedic
Surgery in Kampala; Dr. Immaculate Wema in Nairobi to study Radiology; Dr. Peter Mabula
is in Dar es Salaam studying Emergency Medicine; Dr. Johnstone Kayandabila at KCMC in
Internal Medicine; Dr. Arnold Itemba at Bugando in Obstetrics and Gynecology, and Christina
Hongella doing Pediatrics at Makerere University in Kampala.
F. AMO SCHOOL:
The AMO School graduated 9 candidates in August and returned them to their home bases of
work. This possibly represents the final class of AMO students under the ALMC Training
Center. Currently, there is uncertainty about the future role of this cadre of health worker in
Tanzania. The government is currently debating internally whether there will continue to be
training offered for this cadre. As a result, there are almost no applicants and the few who have
applied, were assigned to government facilities so that the small numbers could be
consolidated.
G. INTERNSHIP:
In 2016, the internship continued to grow with 18 interns shared between ALMC and Selian.
All Tanzanian doctors upon graduating are required to undertake a rotating internship for at
least one year before they are officially registered to practice medicine. ALMC and Selian
Lutheran Hospital share the residents across both hospitals. As a result, the internship is
popular as it is seen to provide a high level of training and a breadth of experiences in both a
community hospital and a referral hospital.

ALMC Annual Report 2016 Page 39
H. INTERNATIONAL ROTATIONS:
In 2016, there were 23 International Medical Students, Residents from six countries at ALMC
and Selian. These visiting scholars spend time at the original Selian Hospital and the new
ALMC. They bring a great mix into the academic atmosphere in the hospitals.
I. UNIVERSITY OF MINNESOTA RESIDENTS:
The long standing linkages to the University of Minnesota were strengthened during the year
with a formal program for mentors from the university to spend periods of time at ALMC and
Selian. In 2016, the program had a six month “chief resident” position for both halves of the
year. Ten residents participated.
10. ALMC CHALLENGES
A. FINANCIAL STABILITY:
True financial stability remains elusive. However, great strides were made this year with
breaking even on day to day running costs and the remarkable effort to pay off all outstanding
income tax debts.
1. NHIF Insurance
Delay in Payments: The National Health Insurance Fund is the largest insurer in Tanzania and
the largest single source of revenue to ALMC. This year was again marked by serious delays
in NHIF making payments for services provided to their clients. These delays contributed
heavily to the challenge of reducing and arrears and more acutely of paying salaries on time.
2. CRDB Bank Construction Loan
ALMC continues to carry the CRDB Bank construction loan in the amount of 7.6 Billion
Tanzanian Shillings (USD $3.4 Million). In 2016 ALMC regularly serviced the loan without
fail. The CRDB Bank had offered a further lowering of interest rate if the hospital could reduce
the principal by 600 Million TSh. However, even though the hospital was in a position to pay
this principal, by the end of the year, the CRDB Bank’s position had changed and they took
the offer off the table.
3. Power Outages
Increasingly regular power outages are costing the hospital dearly in terms of diesel fuel for
the backup generators. The monthly budget for generator diesel was doubled in 2016 to be 24
million per month!

ALMC Annual Report 2016 Page 40
4. Arrears
ALMC managed to pay the income tax arrears into a current status. However, the NSSF
Pension fund remains with a significant debt of 1.5 Billion TSh. The payment schedule for
this was successfully renegotiated for 2017.
5. ALMC Status as Zonal Referral Hospital
While the hospital was officially gazetted as a “Referral Hospital” in November of 2010, the
Ministry of Health and Social Work has yet to prepare guidelines to define this status and lead
the process forward. In 2013, CSSC assisted the government to create a draft of such guidelines
and they are now before the government for a decision. Unfortunately, no guidelines were
issued during 2016. So ALMC has nothing to either accept or reject in this referral status with
the Ministry of Health and Social Welfare.
2. Financial Stability: True financial stability remains elusive. Great strides were
accomplished this year with breaking even on day to day running costs. Considerable
progress was made in reducing further the outstanding debts to income tax and pension
funds. However, significant challenges remain.
4. NHIF Insurance: The National Health Insurance Fund is the largest of our insurance
partners and provides 60% of hospital revenues. So when NHIF is late in paying patient
reimbursements to the hospital, it produces major cash flow problems, delays payment
of staff salaries, and interferes with the hospital’s ability to comply with commitments
for reduction in statutory payment arrears.
5. CRDB Bank Loan: In January 2016, the CRDB Bank offered the hospital a process
for reducing the interest rate of the loan if the hospital could make a substantially
principal payment to reduce the principal. The hospital and the diocese committed to
this but by the time such a large amount of funding was procured, the bank had to
withdraw the offer due to internal challenges at the bank. This results in a lost
opportunity to reduce the total payback over the lifetime of the loan.
6. Tanzania Revenue Authority retroactive tax assessment: At the end of 2016, the
TRA presented the hospital with a retroactive tax assessment based on five years of
non- payment of income tax on overtime and extra duties. This had not previously been
taxed to be consistent with the legal situation in government hospitals. The new
assessment reversed that position and states that nongovernment hospitals must pay tax
even though government hospitals do not. This inequitable taxation is now the basis
for a heated negotiation as the assessment is for $300,000.

ALMC Annual Report 2016 Page 41
11. PLANNING FOR THE FUTURE
2016 looks to be a year of continued financial stability, expanding educational opportunities,
and focusing upon improving the quality of services.
1. Financial Stabilization: The strategy to move toward greater financial stability continues
as the highest priority. ALMC intends to move forward though the introduction of a
strategic plan for increasing revenues. This includes:
1. Undertaking the development of a long term sustainability plan.
2. Increasing the number of surgical cases per month by having more frequent and
more customer friendly surgical clinics.
3. Increasing the number of NHIF patients attending ALMC as other hospitals in
Arusha have been downgraded in their NHIF status.
4. Initiating new clinical services - specifically in spine and back clinic.
2. Improvement of Care: A higher level of care will continue to attract a growing patient
base and increase the number of clients for the hospital. A detailed set of goals is under
development and will focus on improving:
The primary effort is under the nationally recognized system of “SafeCare”. ALMC is
currently ranked at the 3 out of 5 star level but we intend to improve to at least level 4 in
2017. This will be accomplished through:
1. Laboratory services
2. Patient experiences in the Outpatient Department
3. Newborn Intensive Care Unit
4. Adult Intensive Care Unit
5. Food services
3. New Services: ALMC is planning to begin a new Spine and Back Clinic early in the year.
ALMC will begin a private midwifery service called “Birth Matters” in May of 2017.
4. Training: In 2016 ALMC plans to continue its strong emphasis on capacity building and
training. This will be accomplished through:
1. Continuing the training through the Surgical Residency, the School of Nursing, the
Assistant Officer Training School, and the Internship for newly graduated doctors.
2. Continuing the specialist training which currently is for three doctors and expanding it
by one to go for training in Obstetrics and Gynecology and another in Internal
Medicine.
3. To introduce a rotation for Pediatric Residents from other institutions to undertake a
month long training in Newborn Intensive Care.

ALMC Annual Report 2016 Page 42
12. THANKSGIVING
Many, many dear friends and supporters have helped to make the dream of Arusha Lutheran
Medical Centre a reality and continue to help it to serve the people of Tanzania.
First of all, great thanks to the leadership of the ELCT-North Central Diocese. ALMC is
particularly grateful to the Bishop, Rev. Dr. Solomon Massangwa, the General Secretary, Mrs.
Rose Makara, and the Head of the Diocese Health Department, Dr. Simon Megiroo with whom
many of the current challenges are shared.
Great thanks is extended to the ALMC Board of Directors and its Chairman, Rev. Dr. Prof.
Joseph Parsalaw for their leadership and hard work in support of ALMC.
The greatest thanks is to the many members of staff who have worked incredibly hard and long
hours above and beyond the call of duty to make the dream of ALMC become a reality.
Finally, we pause to reflect upon the great generosity of so many supporters of the hospital who
have helped its development and to strengthen its services, and who continue to generously
support the hospital financially. Many have supported ALMC for years from the planning
phase, through construction, and now continue to support ALMC into an exciting future.
The following is a sincere effort to list the faithful and generous supporters of ALMC. Yet, it
is certainly recognized that any such list includes the risk of an inadvertent omission of the
names of very dear supporters. So to each who has given something of themselves to ALMC
and ministries in Arusha we say a loud and thrilling thank you! Some of those most involved
in 2016 include:
Global Health Ministries – Minneapolis, Minnesota
Japanese Embassy in Tanzania
Sisters of Charity Leavenworth Health Systems – Denver, Colorado
Operation Bootstrap Africa – Minneapolis, Minnesota
Denver Hospice, Denver, Colorado
IMPACT UK
Evangelical Lutheran Church in America – Global Mission
Northern Illinois Synod, ELCA
Arusha Community Church
Prairie Farms, Minnesota
Maasai Health Systems, Seattle, Washington
Ray and Gerrie Butler
Njokuti, The Netherlands
International Federation for Spina Bifida and Hydrocephalus, Belgium
Pan African Academy of Christian Surgeons
Rockland Community Church
Amari Foundation – United Kingdom

ALMC Annual Report 2016 Page 43
African Mission Healthcare Foundation
WATSI
InFaith Community Fund
The Tufundishane and University of Minnesota Volunteer Faculty: Drs. Dunlop,
Rhodes, Debes, and Schnobrich
Pediatrician Dr. Elena Mantz for her two years of volunteering
The many congregations which have contributed to the ministry ALMC and for extra
special gifts this year we thank: First Lutheran Church, Stoughton USA; Rockland
Community Church, Golden USA; Augustana Lutheran Church, West St. Paul, USA;
St. Peter Lutheran Church, Colorado, USA
Ron and Debi Gustafson
The many individuals who have so generously supported ALMC
Dr. Ron Eggert for website support
Mark Gerson
Project Cure
Medtronic Laboratories
To ALMC's many visiting surgeons and physicians including Drs. William Brown,
Royal Gerow, James Lessig, Dave Thiel, Dave Palmer, Jack Cochran, Russ McGill,
Elena Mantz, Maria Dillmann, Don Rowberg, Peyton Taylor, Hannu Lintula, Vita
Stagno, Collins Kabachelor, Paula Craigo, Jose Debes, Frank Wiffels, Stephen De
Cock, Mark Wheeler, Steve Ekrick, Stephen Dunlop, Erick Bothun, Rebecca Hartwig,
Tara Rick
Volunteer nurses: Kent Thompson and Sally Thompson, Lisa Giesbrecht, Christy
Miller, Jodi Swanson, and Nicole Schenk,
Clearly, bringing the dream of ALMC into a reality has been due to the contributions of many.
The greatest thanksgiving is to God for faithfulness in leading ALMC to this wondrous vision
of health care for Tanzania.

ALMC Annual Report 2016 Page 44
13. CONCLUSION
ALMC continues to mature as a health care provider of excellence and vision. It is a wonderful
place of service, compassion, and care. In 2016, 147,000 patients were served. This brings the
total served since opening the hospital to over 850,000 patients impacted. It has successfully
expanded its educational and research capacity with training in surgery and nursing. It is indeed
by the grace of God that so much has been accomplished. Certainly, the challenges are great
and many. ALMC has only been open now for these brief eight years. Yet God has continued
to bless this effort and it is clear to all of the ALMC team that God will continue to lead ALMC
forward for God’s honor and glory.
“He who began a good work in you will be faithful to complete it!” Phil 1:6
Respectfully submitted,
Prof. Mark L. Jacobson, MD, MPH
Executive Director ALMC

ALMC Annual Report 2016 Page 45
APPENDIX 1. TOP FIFTEEN IPD AND OPD DIAGNOSES
IPD TOP FIFTEEN DIAGNOSES 2016
RANK DX # %
1 PREGNANCY RELATED 932 13%
2 SURGERY - GENERAL 875 13%
3 HYPERTENSION 419 6%
4 GASTRO INTESTINAL 318 5%
5 DIABETES 301 4%
6 SURG OBG (INCL C-SECTIONS) 270 4%
7 SURGERY ORTHO 254 4%
8 OTHER DX 2% 4%
9 TRAUMA – FRACTURE 242 4%
10 STROKE/CVA 231 3%
11 CARDIAC NON CCF 221 2%
12 TRAUMA – GENERAL 185 2%
13 CONGESTIVE HEART FAILURE 137 2%
14 DIARRHEA 137 2%
15 INFECTIONS - OTHERS 134 2%
OPD VISITS TOP FIFTEEN DIAGNOSES 2015
RANK DX # %
1 AIDS 18,525 13%
2 ALL OTHERS (NOT SPECIFIC) 14,532 10%
3 MUSCULAR SKELETAL 8,096 6%
4 SURGICAL 7,712 5%
5 HYPERTENSION 6,868 5%
6 GASTRO INTESTINAL 5,846 4%
7 PREGNANCY – NORMAL 5,713 4%
8 RESPIRATORY TRACK INFECT 5,301 4%
9 DERMATOLOGICAL 3,875 3%
10 DIABETES 3,848 3%
11 GYNECOLOGICAL 3,222 2%
12 TRAUMA 3,131 2%
13 PULMONARY – OTHER 3,051 2%
14 GENITO-URINARY 2,803 2%
15 OPHTHALMOLOGICAL 2,484 2%