Embed Size (px)
Citation preview

.
.
A CASE PRESENTATION
ON
CARCINOMA STOMACH
PRESENTED BY : Sabina Akter , Moriom Mamtaz , Mahmuda Naznin (GROUP C-2)
PARTICULARS OF THE PATIENT
NAME: Mrs. Feroza Begum AGE : 65 years SEX : FEMALE Marital status :Married HUSBAND’S NAME: Late Mr Kamal Uddin OCCUPATION: HOUSEWIFE RELIGION: ISLAM ADDRESS: Vill : Nurdakhali Thana: Mirsharai ,Ctg. DATE OF ADMISSION & TIME: 5.11.13 at 2.45PM through emergency DATE OF EXAMINATION & TIME: 5.11.13 at 7.00PM BED NO : 33 WARD NO: 24 Under Prof. Dr Omar Faruque Yusuf.

CHIEF COMPLIANTS
1.Pain in mid upper abdomen for last 3 months.
2.Vomiting for last 1.5 months 3.Weight loss for same duration

HISTORY OF PRESENT ILLNESS
• According to patient’s statement she was relatively well 3 moths back. Then she developed pain in mid upper abdomen which was gradual in onset, deep seated, continuous dull aching in nature , radiate to whole upper abdomen, aggravated by taking food and does not relieved by medication but relieved after vomiting. Vomiting was projectile in nature, sour in taste and contained undigested food particles . She complained of loss of appetite, weakness and weight loss by 25% for same duration. She had no history of fever, jaundice , haematemesis , malena , bone pain cough ,chest pain or haemoptysis.
• Her bowel and bladder habit is normal
• PAST HISTORY: Patient had history of peptic ulcer disease for last 7 years and history of HTN for last7 years , no history of diabetes , bronchial asthma and any other co morbid disease
• SOCIO-ECONOMIC HISTORY: She belongs to middle class family.• PERSONAL HISTORY : Patient is non smoker , non alcoholic . She gives
history of taking betel leaf for last 20 years.• FAMILY HOSTORY: No member of her 1st degree relatives suffered
from such kind of disease. No heridiatary disease is transmitting through her family.
• • DRUG HISTORY: Patient had been taking anti ulcerant for last 7 years.• • IMMUNIZATION HISTORY: Not Immunized to any specific disease• MENTRUATION HISTORY: She is a menopausal women for last 10 years• Transfusion History : None• ALLERGIC HISTORY : Not known

GENERAL EXAMINATION• Appearance : Anxious • Body built : Average
• Co-operation: Co-operation• Decubitus: On lying• Nutrition: Average• Anaemia : Present[+]• Jaundice : Absent• Cyanosis: Absent• Dehydration : Present[+]• Edema : Present• Pulse : 72 beats|min• Blood pressure : 130|80 mmHg• Temperature : 99*F• Respiratory rate:18 breaths\min• Neck vein: Not engorged• Thyroid gland: Not enlarged• Peripheral lymph node: Not palpable• Hernial orifices : Intact• Others : I\V cannula in situ in the left hand with 5% DA infusion.

LOCAL EXMINATION
• Inspection:• .Abdomen: Flat & flank full • Umbilicus: Centrally placed, inverted.• There is no visible pulsation, no visible • peristalsis, no visible swelling & no surgical scar• mark.
• Respiratory movement is normal & symmetrical.
• Palpation : • Superficial :
• Abdomen is soft
• Temperature is normal • Tenderness: Present on epigastric region.
On deep palpation An ill defined mass present in epigastric region, approx 3”x 2” in size, firm in consistency, move with respiration, not fixed with overlying skin and underlying structure. Murphy’s sign: Negative Liver : not enlarged Spleen : not palpable Succussion splash : not present Fluid thrill: Absent.

• Percussion : • Percussion note : Tympanic.• Shifting dullness: Absent.• Upper border of liver dullness- • In right 5th intercostal space.• Auscultation:• Bowel sound- Present and normal .• Abnormal bruit- Absent.•
Digital rectal examination: Normal peri-anal region with normal anal tone. No skin tag. Rectal mucosa free. Finger is stained with stool , not blood tinged. OTHER SYSTEMIC EXAMINATION : Reveals no abnormality.
PROVISIONAL DIAGNOSIS
• GASTRIC OUTLET OBSTRUCTION DUE TO CARCINOMA OF STOMACH .
DIFFERENTIAL DIAGNOSIS
1. Pyloric stenosis secondary to peptic ulcer disease
2.Carcinoma head of the pancreas
3.Ca of transverse colon

SALIENT FETURE• Mrs. Feroza Begum, 65years old lady hailed from Mirsharai , got admitted into CMCH with the
complaints of• Pain in epigastric region for last 3 months • Vomiting for last 1.5 months• According to patient statement she was relatively well about 3 months back. Then she developed
pain in epigastric region which was gradual in onset , deep seated , continuous dull aching in nature, radiated to whole abdomen , aggravated by taking food and relieved after vomiting. Vomiting was spontaneous , projectile, sour in taste, contained undigested food particles. She complained of anorexia, weakness and significant weight loss[25%] for same duration. She had no history of fever, jaundice, haematemesis, melena, bone pain or cough or chest pain . Patient had history of peptic ulcer disease for last 7 years. Patient is anxious , cooperative , avarege body build , &nutrition . Patient is anaemic , not icteric , dehyadrated and edema was present in lower leg . Pulse was 72 beat\min , blood pressure 130\80 mmHg , temperature 99 *F and respiratory rate 18 breaths\min . On examination , abdomen was flat, umbillicus centrally placed, no visible scar mark , no visible peristalsis. An ill defined mass was present in epigastric region, approx 3”x 2” in size, firm in consistency, move with respiration, not fixed to overlying skin, or underlying structure. Liver and spleen are not palpable & no other organomegaly . Succussion splash was absent . Digital rectal examination shows no abnormality . Other systemic examination reveals no abnormality .

INVESTIGATION For diagnosis: Endoscopy of upper GIT with possible biopsy For metastasis: USG of whole abdomen Chest X-RAY P\A VIEW Liver function test For anaesthetic fitness: CBC RBS Serum urea serum creatinine ECG serum albumin serum electrolyte.
. ON INVESTIGATION , our findings, On-endoscopic finding , Stomach Large ulcer involving antrum & part of the body with narrowing of pylorous.
On histo-pathological finding,
Fragments of gastric mucosa howing ulcer & inflammatory exudate on the surface & mixed with atypical epithelial cells & glands compatible with poorly differentiated adenocarcinoma.
On biochemical finding,
Na+ : 132 ml mol\L K+ : 3.2 mlmol\L Cl- : 93 mlmol\L HCO3- : 23 mlmol\L ON ROUTINE EXAMINATIPON:
Hb% : 7.5 mg\dL
ON USG examination: Few small lymph node [ Avg o.4 cm ] are seen in the para- aortic region
CONFIRMATORY DIAGNOSIS
• GASTRIC OUTLET OBSTRUCTION due to CARCINOMA OF STOMACH

Management
COUNSELLING PREOPERATIVE PREPARTION OPERATION
PATIENT PREPARATION
Anaemia correction
Electrolyte correction
Nutrition correction

STOMACH PREPARATION
3 days preparationNothing by mouthI\V fluid: Inf. DA , Inf. DNS , Inf. Normal saline with 2amp K+NG tube for suction & lavage 200ml every 2hrly until clear fluid come out.Prophylactic antibiotics
OPERATION
Due to presence of distant metastasis go for PALLIATIVE GASTRO-JEJUNOSTOMY.

CARCINOMA OF STOMACH
.
Introduction
• Ca of stomach is a major cause of cancer mortality worldwide.
• It is actually an eminently curable disease provided that is detected at an appropriate stage & treated adequately.
• Early diagnosis is therefore the key to success with this disease.

Incidence
• Marked variation in worldwide per million per year
• Japan-70• Eastern Europe-40• UK-15• USA-10(Some geographical areas in China incidence is double that in Japan).
Aetiological factors1.Age-middle to elderly2.Sex-more in male3.Environmental factors- a. Diet (Excessive salt intake , smoked food, deficiency of antioxidant) b . Low socio-economic condition c . Cigarette smoking4.Host factors- Gastric polyps , gastric atrophy , chronic gastritis , achlorohydria, pernicious anaemia , duodeno gastric reflex , intestinal metaplasia.5.Infective- H. pylori infection6.Genetic factors- blood group-A Family H/O gastric cancer Hereditary Non polyposis colon cancer syndrome
Site
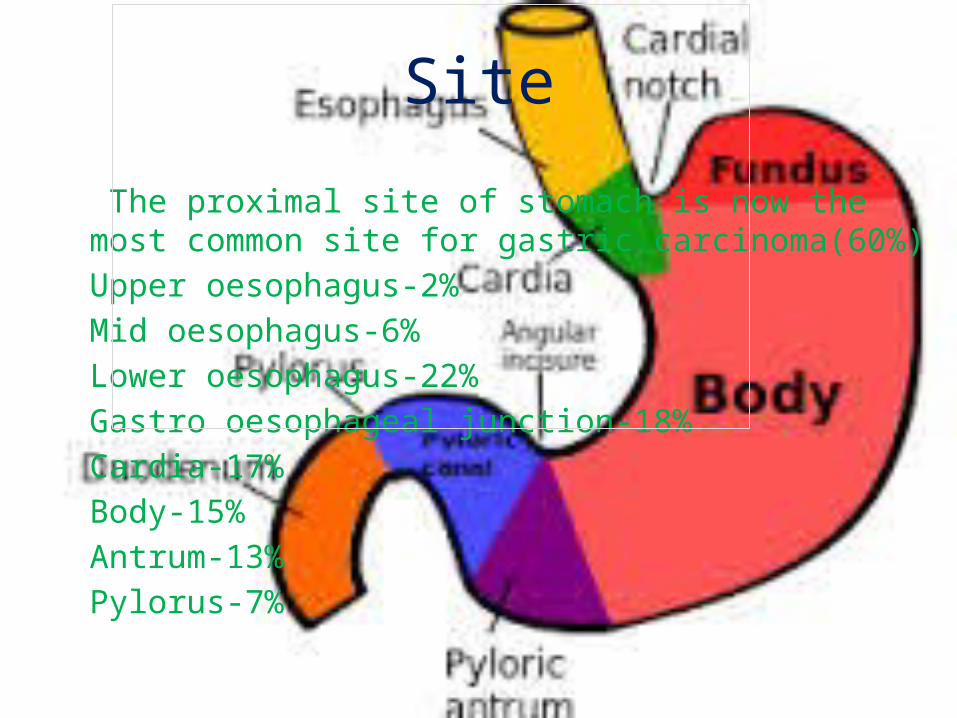
The proximal site of stomach is now the most common site for gastric carcinoma(60%)Upper oesophagus-2%Mid oesophagus-6%Lower oesophagus-22%Gastro oesophageal junction-18%Cardia-17%Body-15%Antrum-13%Pylorus-7%

Classification
Japanese classification (Early gastric cancer) 1.Protruded 2.Superficial -Depressed -Elevated -Flat 3.Excavated

,,

Borrmann Classification(Advanced gastric Ca)
• Type1:Polypoid/fungating• Type2:Ulcerated with elevated margin• Type3:Ulcerated with infiltration• Type4:Diffusely infiltrative
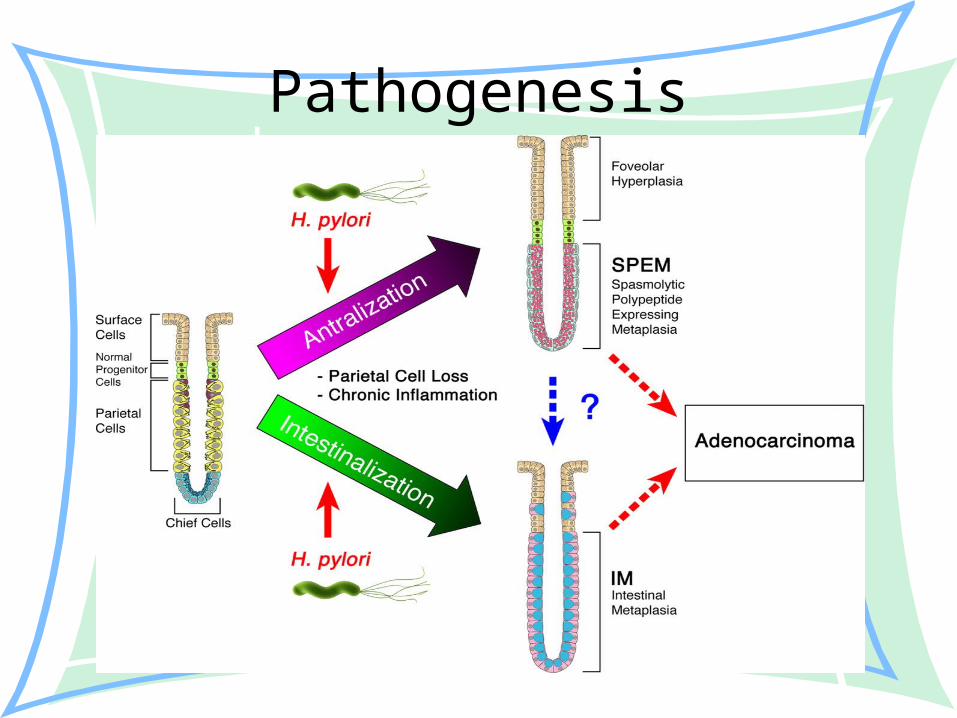
Pathogenesis
Clinical featuresSymptom
• 1.Early case-• New dyspepsia over 40 years• Vague post prandial abdominal heaviness• Anorexia• Malaise
• 2.Advanced case-• Early satiety• Bloating• Abdominal distension• Constant epigastric pain• Lump in epigastric region• Vomiting• Loss of appetite• Wt loss• Haematemesis• Malena• Features of metastasis
SIGN• General examination Anaemia , jaundice, Wasting Dehydration, Enlarged supraclavicular lymph node (Virchow’s gland) • Local examination• Abdominal distension• Visible peristalsis(if obstruction)• Epigastric lump ( Irregular, tender ,hard )• Enlarged liver(if secondary deposit)• Succussion splash-Positive (If GOO)• Sister Joseph’s nodule• Trousseaus sign

Spread of Ca of Stomach
• Usually 4 ways -Direct spread -Lymphatic spread -Blood borne metastases -Transperitoneal spread Krukenberg’s tumours Sister Joseph’s nodule
Staging• TNM Staging T1- Involves lamina propria T2-involves muscularis mucosa T3-Involves serosa T4-Involves adjacent organs N1-Involves 1-6 regional lymph node N2-Involves 7-15 regional lymph node N3-Involves >15 nodes
M0-No distant metastasis M1-Distant metastasis

....• Clinical Staging Stage 1 : Involvement of mucosa or submucosa. Stage 2 : Involvement of muscularis layer Stage 3: Involvement of lymph node Stage 4 : Involvement of distal lymph node or adjacent organ.

Investigation
* For diagnosis Endoscopy of upper GIT with possible biopsy If required Barium meal X-ray of stomach and duodenum
*For metastasis USG of whole abdomen Chest X-ray LFT CT scan Bone scan
*For G/A fitness
• CBC
• Urine R/M/E
. Random blood glucose
• Serum creatinine
• Chest X-ray P/A view
• ECG
.
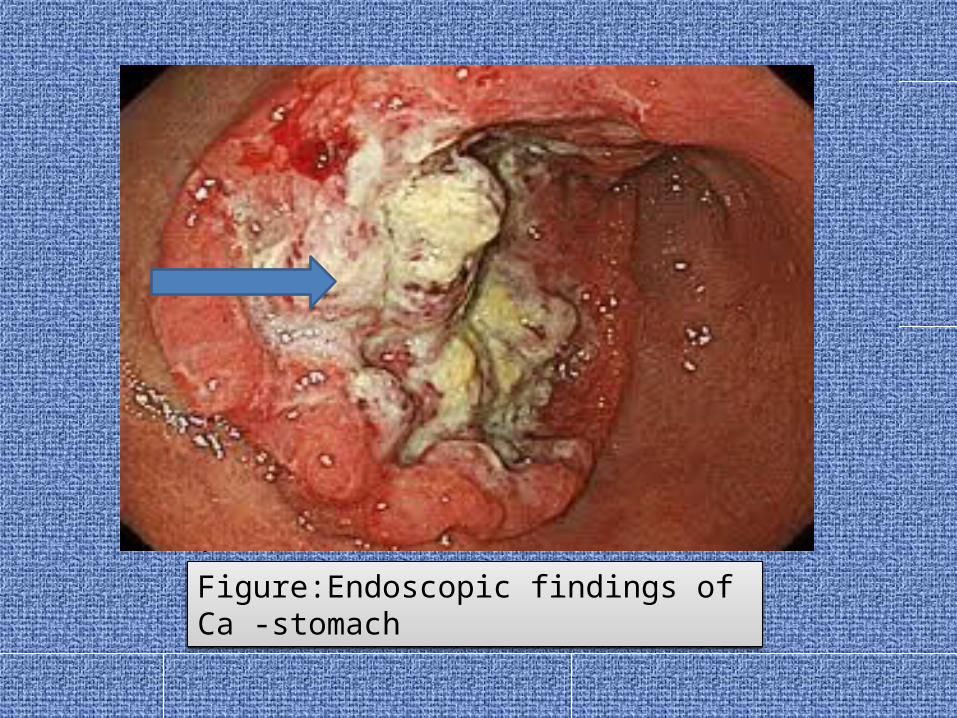
Figure:Endoscopic findings of Ca -stomach

.
FIGURE : Barium meal X-ray of stomach & duodenum

FIGURE : Barium meal X-ray of stomach & duodenum

Management
• A. General management 1.Correction of anaemia -by blood transfusion 2.Correction of dehydration& electrolyte imbalance-by I/V fluid 3.Preparation of stomach by NBM & gastric lavage
4.Correction of nutrition status by -Parenteral nutrition -Vit. supplementation

B.Surgical management
• CURATIVE SURGERY 1-Lower subtotal gastrectomy – If Ca of lower third of
stomach 2-Total gastrectomy with Roux en-y reconstruction-When
growth involve proximal1/3rd or middle1/3rd of stomach
• PALIATIVE SURGERY Gastro-jejunostomy Palliative stenting or intubation(feeding jejunostomy)

Figure: Roux-en-Y Gastric bypass

FIGURE : Subtotal gastrectomy
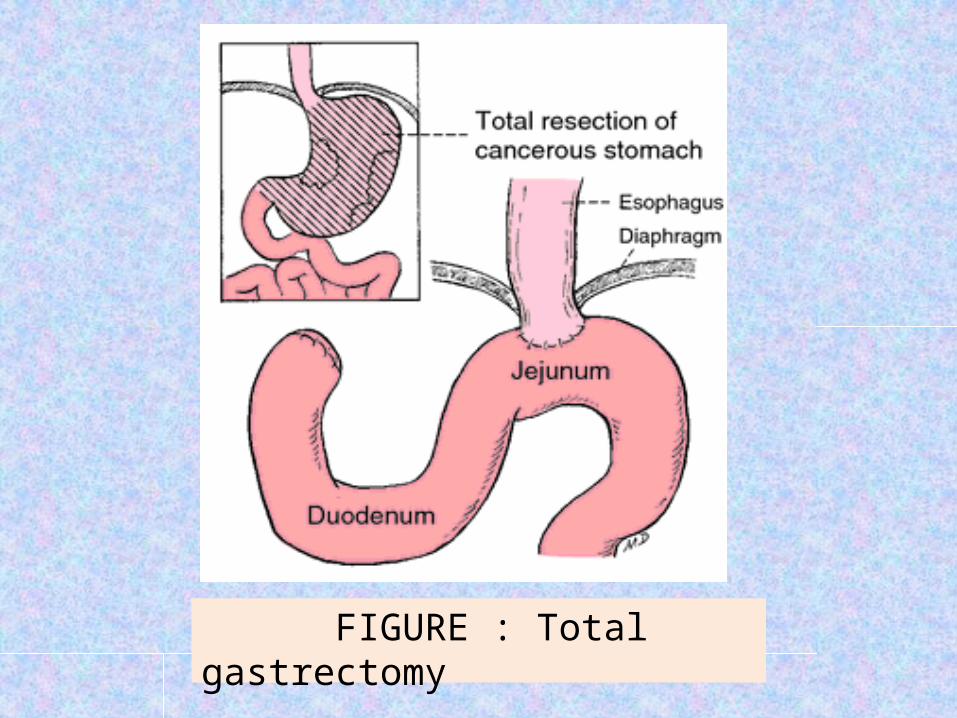
FIGURE : Total gastrectomy

OTHER MODALITIES
CHEMO THERAPY Commonly used chemotherapeutic agents are ECF ( Epirobucin , Cisplatin , 5-FU) RADIOTHERAPY : Has a role in palliative treatment of painful bony metastasis.
SIGNS OF INOPERABILITY Haematogenous metastasis or distant metastasis Fixation to pancreas or post abdominal or involvement of the mesentary especially the origin of the superior mesenteric vessel. Gross local involvement of lymph node -N4 Nodal disease or -Disease beyond N4 node Involvement of distant peritoneum with -Peritoneal seedling & -Huge ascites
Post-operative complication of Ca-stomach
• 1.Small stomach syndrome• 2.EarlyDumping• 3.Late Dumping • 4.Bile vomiting.• 5.Nutritional deficiency• 6.Anastomotic leakage• 7.Secondary Haemorrhage

Prognostic factors of Ca-stomach
• 5 years survival Early gastric cancer-90% Stage 1 -70% Stage 2 -30% Stage 3 -10% Stage 4 -0%
THANK YOU
.