Embed Size (px)
Citation preview

© 2006 Thomson-Wadsworth
Chapter 10
Mothers and Infants: Nutrition Assessment, Services and
Programs

© 2006 Thomson-Wadsworth
Learning Objectives
• List the recommendations for maternal weight gain during pregnancy.
• Explain the relationship of maternal weight gain to infant birthweight.
• Identify nutritional factors and lifestyle practices that increase health risk during pregnancy.
• Describe the benefits of breastfeeding.

© 2006 Thomson-Wadsworth
Learning Objectives
• Describe the purpose, eligibility requirements, and benefits of the federal nutrition programs available to assist low-income women and their children.
• Identify the common nutrition-related problems of infancy.
• Describe current recommendations for feeding during infancy.

© 2006 Thomson-Wadsworth
Introduction
• The effects of nutrition extend from one generation to the next and this is especially evident during pregnancy.
• If a mother’s nutrition stores are inadequate early in pregnancy when the placenta is developing, the fetus will develop poorly.

© 2006 Thomson-Wadsworth
Introduction
• Infants born of malnourished mothers are more likely than healthy women’s infants to become ill, to have birth defects, and to suffer retarded mental or physical development.
• It is critical to provide the best nutrition possible at the early stages of life.

© 2006 Thomson-Wadsworth
Trends in Maternal and Infant Health
• The United States spends more money on health care than most other countries, but its infant mortality rate (IMR) of 7.0 is considerably higher than several industrialized countries.
• Disparities in IMRs persist between ethnic groups and between poor and non-poor infants.

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth
IMRs by Race and Ethnicity,2002

© 2006 Thomson-Wadsworth
Trends in Maternal and Infant Health
• Failure to improve the IMR in the U.S. has been attributed to the number of infants born with low birthweights.
• Birthweight and length of gestation are the primary indicators of an infant’s future health status.

© 2006 Thomson-Wadsworth
Trends in Maternal and Infant Health
• Several factors must be addressed to reduce incidence of low birthweight:– Poverty– Minority status– Lack of access to health care– Inability to pay for health care– Poor nutrition– Low level of educational achievement– Unsanitary living conditions– Unhealthful habits such as smoking, drinking,
and drug use

© 2006 Thomson-Wadsworth
% of Low-Birthweight and Very-Low-Birthweight Infants

© 2006 Thomson-Wadsworth
National Goals for Maternal and Infant Health
• To further reduce infant mortality, the U.S. must focus on changing protective and risky behaviors that affect pregnancy outcomes.
• These factors should be addressed in preconception screening and counseling.

© 2006 Thomson-Wadsworth
National Goals for Maternal and Infant Health
• The use of timely prenatal care can also help mitigate risks by identifying women who are at high risk of high blood pressure and other maternal complications.

© 2006 Thomson-Wadsworth
National Goals for Maternal and Infant Health
• Healthy People 2010 Progress Review– Progress toward the Healthy People
2010 maternal and infant objectives is uneven.

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth
National Goals for Maternal and Infant Health
• Healthy People 2010 Progress Review (continued)– Improvement is seen in:
• The decline in infant mortality rates for Hispanics, Whites, and American Indians
• A decreased incidence of spina bifida• An increase in breastfeeding by women in
all race and ethnic groups• A continued decline in cigarette smoking
during pregnancy

© 2006 Thomson-Wadsworth
National Goals for Maternal and Infant Health
• Healthy People 2010 Progress Review (continued)– No progress or movement in the
wrong direction occurred in the areas of: • Maternal death for African American
women• Iron deficiency in women aged 12 to 49
years• Fetal alcohol syndrome• Low birthweight

© 2006 Thomson-Wadsworth
Healthy Mothers

© 2006 Thomson-Wadsworth
Healthy Mothers
• Maternal Weight Gain– Normal weight gain and adequate nutrition
support the health of the mother and the development of the fetus.
– A woman who begins pregnancy at a healthful weight should gain between 25 and 35 pounds.
– Low weight gain in pregnancy is associated with increased risk of delivering a low-birthweight infant.

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth
• B-C = normal weight women• A-B = underweight women• D = overweight women

© 2006 Thomson-Wadsworth
Healthy Mothers – Maternal Weight Gain
• Excessive weight gain increases the risk of complications during delivery, as well as postpartum obesity.
• The suggested rate of weight gain is 2-4 pounds for the first trimester, followed by a steady gain of about one pound per week thereafter.

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth
Healthy Mothers
• Adolescent Pregnancy– Adolescent pregnancy is associated
with higher rates of pregnancy-related hypertension, iron-deficiency anemia, premature birth, low-birthweight infants, and prolonged labor.

© 2006 Thomson-Wadsworth
Healthy Mothers
• Nutrition Assessment in Pregnancy– Dietary measures including foods habits and
use of vitamin and mineral supplements.– Clinical measures including outcome of
previous pregnancies and obstetric history.– Anthropometric measures such as weight
for height and weight.– Laboratory values including screening for
anemia.

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth
Healthy Babies
• A baby grows faster during the first year of life than ever again.
• A baby’s birthweight doubles during the first 4 to 6 months and triples by the end of the first year.
• Adequate nutrition is critical to support this rapid growth and development.

© 2006 Thomson-Wadsworth
Nutrient Needs and Growth Status in Infancy
• Infants need smaller total amounts of the nutrients than adults do...
• ...but, based on body weight, infants need over twice as much of many of the nutrients.

© 2006 Thomson-Wadsworth
Nutrient Needs and Growth Status in Infancy
• Anthropometric Measures in Infancy– Length should be measured in the
recumbent position on a measuring board.
– Head circumference confirms that growth is proceeding normally and can also detect protein-energy malnutrition.

© 2006 Thomson-Wadsworth
Nutrient Needs and Growth Status in Infancy
• Anthropometric Measures (continued)– Length-for-age less than the 5th percentile
reflects chronic undernutrition.– Weight-for-length less than the 5th
percentile may reflect acute malnutrition.– Excessive weight-for-length (above the 95th
percentile) indicates overweight.

© 2006 Thomson-Wadsworth
% of Mothers Breastfeeding

© 2006 Thomson-Wadsworth
Breastfeeding Recommendations
• Breastfeeding offers both emotional and physical health benefits.
• During the first 2-3 days, the breasts produce colostrum that contains antibodies and white cells from the mother’s blood, which favors the growth of friendly bacteria.
• Breast milk also contains a powerful antibacterial agent, lactoferrin.

© 2006 Thomson-Wadsworth
Breastfeeding Recommendations
• Breast milk is tailor made to meet the nutrient needs of the young infant and breastfed infants usually require no supplements except for vitamin D and fluoride.
• At 4 to 6 months, infants may require an iron supplement.
• Breastfeeding protects against allergy development and favors normal tooth and jaw alignment.

© 2006 Thomson-Wadsworth
Breastfeeding Recommendations
• Breastfeeding Promotion– One of the Healthy People goals is to
increase the incidence of breastfeeding although there are a number of barriers to achieving this objective.
– One example of a successful approach to increasing breastfeeding rates in low-income, urban populations is the peer counseling method promoted by the La Leche League International.

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth
Using Peer Counselors to Change Culturally Based Behaviors
• Best Beginnings of Forsyth County - demonstrates motivational potential of peer counselors

© 2006 Thomson-Wadsworth
Using Peer Counselors to Change Culturally Based Behaviors
• Goals and Objectives– Goals
• Increase the number of women who breastfeed their newborn infants
• Increase the number of women who continue to breastfeed past the first few weeks of their baby’s life
– Objectives • Develop the curriculum for the didactic and
experiential components of the training • Add group discussions and breastfeeding classes

© 2006 Thomson-Wadsworth
Using Peer Counselors to Change Culturally Based Behaviors
• Target Audience– Pregnant women who applied for WIC
in Forsyth County– 1/3 were Hispanic
• Rationale for the Intervention– 10% of mothers in the target
audience initiated breastfeeding– Almost none of these women
continued past six weeks
© 2006 Thomson-Wadsworth
Using Peer Counselors to Change Culturally Based Behaviors
• Methodology– Received grant in 1992– Peer counselor training
• 20 hours of didactic instruction on lactation and counseling
• Written test• Course information - advantages, myths,
physiology, mechanics, common problems, high-risk situations
• Competency exam• 6-week internship

© 2006 Thomson-Wadsworth
Using Peer Counselors to Change Culturally Based Behaviors
• Methodology (continued)– Peer counselors:
• Encouraged breastfeeding among WIC participants
• Increased public awareness of breastfeeding

© 2006 Thomson-Wadsworth
Using Peer Counselors to Change Culturally Based Behaviors
• Results– Within 6 months after start, the
breastfeeding initiation rate had increased from 10% to 26%
– In fiscal year 1997–1998, almost 50% of Forsyth Co. women in WIC had initiated breastfeeding
– In 1996-1997, over 27% of participants continued breastfeeding for more than 6 weeks

© 2006 Thomson-Wadsworth
Using Peer Counselors to Change Culturally Based Behaviors
• Lessons Learned– Enthusiasm of the peer counselors
was important to program success– Peer counselor programs can have a
positive influence on the peer counselors themselves

© 2006 Thomson-Wadsworth
Using Focus Group Findings
• Best Start breastfeeding promotion project guidelines were derived from focus groups
• Campaign tone - emotional • Message design
– Educational messages - succinct and easily understood
– Promotional messages - emphasize confidence and the pride breastfeeding mothers gain

© 2006 Thomson-Wadsworth
Using Focus Group Findings
• Spokespersons– Celebrities, wealthy women not
credible– Women featured should be of the
same economic, ethnic, and age groups as those targeted
– Print/broadcast materials should communicate modernity and confidence
© 2006 Thomson-Wadsworth
Using Focus Group Findings
• Educational approaches - need to be redesigned to refute perceptions of breastfeeding as difficult– Avoid emphasis on being healthy,
relaxed; special dietary guidelines – Reassurance that most women
produce sufficient quantities/quality of breast milk

© 2006 Thomson-Wadsworth
Using Focus Group Findings
• Professional training - – Materials should counter belief that
economically disadvantaged clients are not interested/do not value health professionals’ advice
– Counseling strategies should address special needs of low-income women
• Program activities/components - variety of mutually reinforcing activities

© 2006 Thomson-Wadsworth
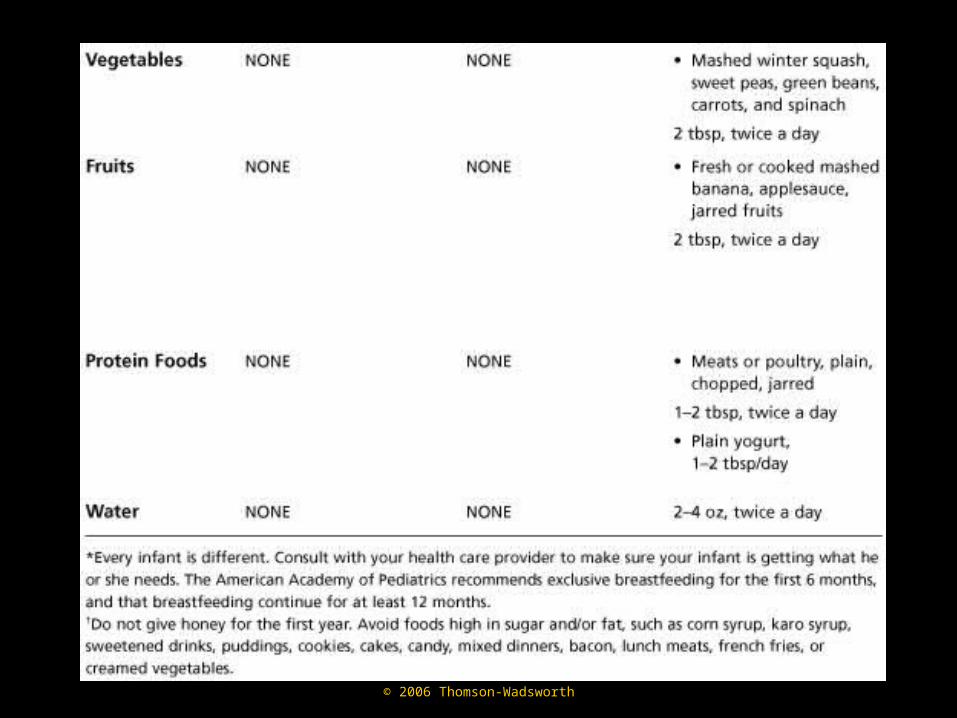
Other Recommendations on Feeding Infants
• Whole cow’s milk is not recommended during the first year of life but iron-fortified formulas can be used to support normal development in the baby’s first months of life.
• Solid foods should not be introduced too early because infants are more likely to develop allergies to them in the early months.

© 2006 Thomson-Wadsworth
© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth
Primary Nutrition-Related Problems of Infancy
• Iron Deficiency– Iron deficiency can be prevented by:
• Breastfeeding • If not breastfeeding, using iron-fortified
formula for the first year of life • Adding appropriate foods between the
ages of 4 and 6 months

© 2006 Thomson-Wadsworth
Primary Nutrition-Related Problems of Infancy
• Food Allergies– Food allergies are much less
prevalent in breastfed babies.– New foods should be introduced
singly to facilitate prompt detection of allergies.
© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth
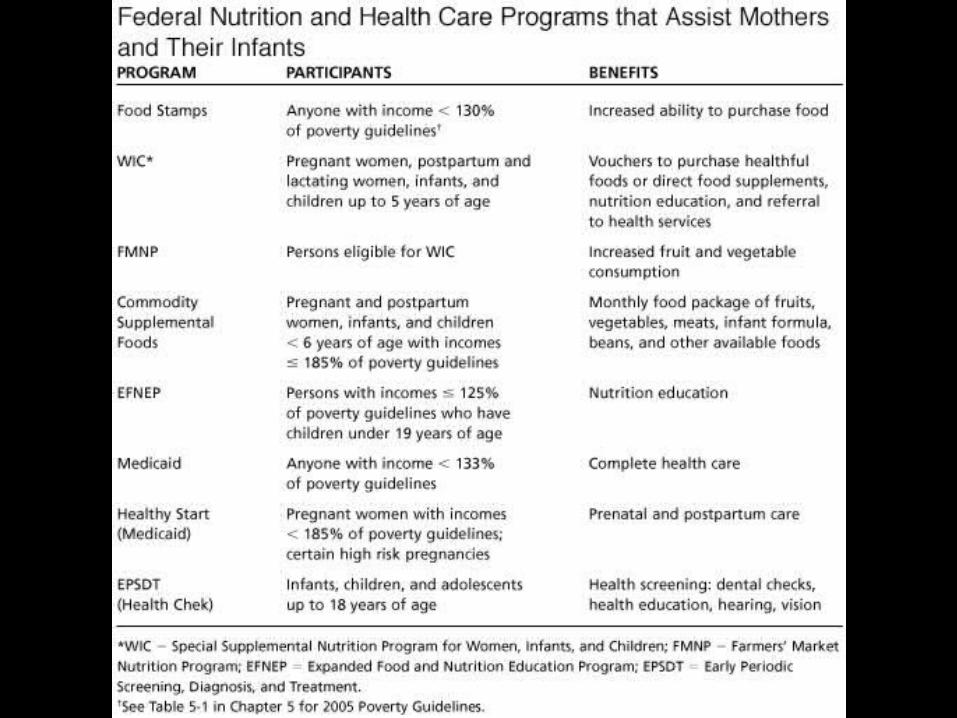
Domestic Maternal and Infant Nutrition Programs
• The WIC Program– WIC stands for Special Supplemental
Nutrition Program for Women, Infants, and Children.
– Provides supplemental foods to infants, children up to age five, and pregnant, breastfeeding, and non-breastfeeding postpartum women.

© 2006 Thomson-Wadsworth
Domestic Maternal and Infant Nutrition Programs – WIC
• WIC participants must qualify financially and be considered at nutritional risk.

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth
Domestic Maternal and Infant Nutrition Programs – WIC
• WIC foods include the following:– Iron-fortified infant formula and infant
cereal.– Iron-fortified breakfast cereal.– Vitamin C-rich fruit or vegetable juice.– Eggs, milk, cheese, and peanut butter
or dried beans and peas.

© 2006 Thomson-Wadsworth
Domestic Maternal and Infant Nutrition Programs – WIC
• WIC is distinguished among federal assistance programs by the combination of: – Supplementary foods– Nutrition education– Preventive health care
© 2006 Thomson-Wadsworth
Domestic Maternal and Infant Nutrition Programs – WIC
• Program benefits of WIC include:– Improved dietary quality.– More efficient food purchasing.– Better use of health services.– Improved maternal, fetal, and child
health and development.

© 2006 Thomson-Wadsworth

© 2006 Thomson-Wadsworth
Domestic Maternal and Infant Nutrition Programs – WIC
• WIC Works– WIC has been described as one of the
most efficient programs undertaken by government...
– ...but it is not an entitlement program and can only serve as many people as its annual appropriation from Congress permits.

© 2006 Thomson-Wadsworth
Annual Growth in WIC Participation

© 2006 Thomson-Wadsworth
Domestic Maternal and Infant Nutrition Programs
• Other Nutrition Programs of the U.S. Department of Agriculture– Food Stamp Program– WIC Farmers’ Market Nutrition
Program– Commodity Supplemental Food
Program

© 2006 Thomson-Wadsworth
Domestic Maternal and Infant Nutrition Programs – Other USDA Programs
• Expanded Food and Nutrition Education Program (EFNEP)– This program is directed at low-
income families.– It is delivered by trained nutrition
aides from the local community and is administered by the USDA Extension Service.

© 2006 Thomson-Wadsworth
Domestic Maternal and Infant Nutrition Programs
• Nutrition Programs of the U.S. Department of Health and Human Services– Title V Maternal and Child Health Program
• Maternity and infant care• Intensive infant care• Family planning• Health care for children and youth• Dental care for children

© 2006 Thomson-Wadsworth
Domestic Maternal and Infant Nutrition Programs – Other DHHS Programs
• Medicaid and EPSDT– EPSDT is a mandatory Medicaid
service to improve the health status of children from low-income families by providing services not typically found under the current Medicaid program.

© 2006 Thomson-Wadsworth
Domestic Maternal and Infant Nutrition Programs – Other DHHS Programs
• Community Health Centers– Program designed to provide health
services and related training in medically underserved areas
– Focuses on comprehensive primary care services

© 2006 Thomson-Wadsworth
Domestic Maternal and Infant Nutrition Programs – Other DHHS Programs
• The Healthy Start Program– Goal is to identify and develop
community-based approaches to: • Reducing infant mortality• Improving the health of low-income
women, infants, children and their families

© 2006 Thomson-Wadsworth
Looking Ahead: Improving the Health of Mothers and Infants
• Many of the existing health care programs do not have nutrition counseling or education available within their own sites.
• The increasing numbers of working women along with the growth in worksite health promotion programs have implications for community nutritionists in providing nutrition education and related services to this population.

© 2006 Thomson-Wadsworth
Looking Ahead: Improving the Health of Mothers and Infants
• Recommendations:– Provide food supplementation and nutrition
education to all pregnant women with low incomes.
– Appropriate additional federal funds to WIC.– Include prenatal nutrition counseling as a
reimbursable service in health insurance policies for all pregnant women in the U.S.