Embed Size (px)
Citation preview
Publications of the University of Eastern Finland
Dissertations in Health Sciences
isbn 978-952-61-1254-1
Publications of the University of Eastern FinlandDissertations in Health Sciencesd
issertation
s | 195 | Ville V
ar
mav
uo
| Plerixafor in A
utologous S
tem C
ell Tran
splantation
Ville VarmavuoPlerixafor in Autologous
Stem Cell Transplantation
Ville Varmavuo
Plerixafor in Autologous Stem Cell Transplantation
Autologous stem cell transplantation
(ASCT) has an established role as a
treatment modality for hematological
malignancies. Stem cells for ASCT
are almost invariably collected from
peripheral blood after mobilization
therapy. Plerixafor, a CXCR4
antagonist, is the latest addition to
stem cell mobilization and may be
used in patients who mobilize poorly
otherwise. This series of studies
provides additional information to
support the use of plerixafor.

VILLE VARMAVUO
Plerixafor in Autologous Stem Cell Transplantation
To be presented by permission of the Faculty of Health Sciences, University of Eastern Finland for public examination in Medistudia Auditorium, Kuopio, on Friday, November 1st 2013, at 12 noon
Publications of the University of Eastern Finland Dissertations in Health Sciences
Number 195
Departments of Medicine and Clinical Chemistry, Institute of Clinical Medicine School of Medicine, Faculty of Health Sciences
Laboratory of Eastern Finland University of Eastern Finland
Kuopio 2013

Kopijyvä Oy Kuopio, 2013
Series Editors:
Professor Veli-Matti Kosma, M.D., Ph.D. Institute of Clinical Medicine, Pathology
Faculty of Health Sciences
Professor Hannele Turunen, Ph.D. Department of Nursing Science
Faculty of Health Sciences
Professor Olli Gröhn, Ph.D. A.I. Virtanen Institute for Molecular Sciences
Faculty of Health Sciences
Professor Kai Kaarniranta, M.D., Ph.D. Institute of Clinical Medicine, Ophthalmology
Faculty of Health Sciences
Lecturer Veli-Pekka Ranta, Ph.D. (pharmacy) School of Pharmacy
Faculty of Health Sciences
Distributor: University of Eastern Finland
Kuopio Campus Library P.O.Box 1627
FI-70211 Kuopio, Finland http://www.uef.fi/kirjasto
ISBN (print): 978-952-61-1254-1 ISBN (pdf): 978-952-61-1255-8
ISSN (print): 1798-5706 ISSN (pdf): 1798-5714
ISSN-L: 1798-5706

III
Author’s address: Department of Medicine Kuopio University Hospital KUOPIO FINLAND
Supervisors: Professor Esa Jantunen, M.D., Ph.D. Clinical Medicine, University of Eastern Finland and Department of Medicine Kuopio University Hospital KUOPIO FINLAND Clinical Consultant Pentti Mäntymaa, M.D., Ph.D. Laboratory of Eastern Finland KUOPIO FINLAND
Reviewers: Docent Riitta Alitalo, M.D., Ph.D. HUSLAB, Helsinki University Central Hospital HELSINKI FINLAND
Docent Maija Itälä-Remes, M.D., Ph.D. Department of Clinical Haematology, Stem Cell Collection and Transplantation Center, Turku University Hospital TURKU FINLAND
Opponent: Professor Kari Remes, M.D., Ph.D.
Department of Clinical Haematology, Turku University Hospital University of Turku TURKU FINLAND

IV

V
Varmavuo, Ville Plerixafor in Autologous Stem Cell Transplantation University of Eastern Finland, Faculty of Health Sciences Publications of the University of Eastern Finland. Dissertations in Health Sciences Number 195. 2013. 91 p. ISBN (print): 978-952-61-1254-1 ISBN (pdf): 978-952-61-1255-8 ISSN (print): 1798-5706 ISSN (pdf): 1798-5714 ISSN-L: 1798-5706 ABSTRACT Autologous stem cell transplantation (ASCT) has an established role as a treatment modality for hematological malignancies. Factors influencing cellular composition of the stem cell grafts are poorly understood. In some previous studies, stem cell graft composition has been linked with immune recovery and long-term outcome after ASCT. Traditionally, a combination of chemotherapy and growth factor or growth factor alone has been used for autologous stem cell mobilization. Plerixafor is the latest addition for stem cell mobilization, where it has been studied mainly in combination with granulocyte-colony-stimulating factor (G-CSF).
The prevalence of poor stem cell mobilization in various diseases was studied in the retrospective study. Decision algorithms to guide pre-emptive plerixafor use based on blood leukocyte and CD34+ cell kinetics were created. Based on the mobilization kinetics observed, it was found that if the white blood cell count is on the rise (>5 x 109/L) and blood CD34+ cell count is �10 x 106/L after stem cell mobilization with the combination of chemotherapy and G-CSF, the use of plerixafor should be considered. Usefulness of this algorithm needs to be validated in a prospective study.
Next, the effects of plerixafor injection in blood cell composition in chemomobilized patients with non-Hodgkin's lymphoma (NHL) were studied. Plerixafor injection given in the evening was found to increase CD34+ cell mobilization by five-fold in the following morning measurements. Furthermore, also other cell populations such as neutrophils, lymphocytes and monocytes were mobilized by plerixafor.
The effects of plerixafor on stem cell graft cellular composition in NHL patients mobilized with chemotherapy and G-CSF was also evaluated. The control group included patients mobilized with chemotherapy plus G-CSF. Blood grafts collected after plerixafor injection were found to contain more primitive stem cells (CD34+CD133+CD38-) as well as more T lymphocytes and NK cells than grafts collected in the control group. The effects of plerixafor injection appeared to be similar in myeloma patients.
The possible effects of plerixafor on hematopoietic recovery and long-term outcomes after ASCT were studied in patients with NHL. Patients receiving plerixafor-mobilized grafts had similar hematopoietic recovery during the first year following ASCT compared to control group patients. Also progression-free and overall survival was equal.
This series of studies provides additional information to support the use of plerixafor in patients who mobilize poorly. The importance of graft cell composition in recovery of hematopoietic and immune system and long-term prognosis needs to be evaluated in prospective studies with larger patient numbers. National Library of Medical Classification: QV 180, WH 540, WH 525, WH 380 Medical Subject Headings: Hematopoietic Stem Cell Transplantation; Transplantation, Autologous; Hematopoietic Stem Cell Mobilization/methods; Multiple Myeloma; Lymphoma, Non-Hodgkin; Receptors, CXCR4/antagonists & inhibitors; Heterocyclic Compounds/administration and dosage; Hematologic Agents; Granulocyte Colony-Stimulating Factor; Antineoplastic Combined Chemotherapy Protocols; Lymphocyte Subsets; Antigens, CD34; Graft Survival

VI

VII
Varmavuo, Ville Pleriksafori autologisten kantasolujen siirroissa Itä-Suomen yliopisto, terveystieteiden tiedekunta Publications of the University of Eastern Finland. Dissertations in Health Sciences Numero 195. 2013. 91 s. ISBN (print): 978-952-61-1254-1 ISBN (pdf): 978-952-61-1255-8 ISSN (print): 1798-5706 ISSN (pdf): 1798-5714 ISSN-L: 1798-5706 TIIVISTELMÄ Potilaan omilla kantasoluilla tehtävät autologiset kantasolujensiirrot ovat vakiinnuttaneet asemansa hematologisten syöpätautien hoidossa. Kantasolusiirteen solukoostumukseen vaikuttavat tekijät tunnetaan puutteellisesti. Aiemmissa tutkimuksissa siirteen solukoostumus on yhdistetty intensiivihoidosta toipumiseen ja pitkäaikaisennusteeseen. Perinteisesti kantasolujen mobilisaatiossa on käytetty solunsalpaajan ja kasvutekijän yhdistelmää tai kasvutekijää yksin. Pleriksafori on uusin tulokas kantasolujen mobilisaatiossa, jossa sitä on tutkittu pääosin yhdessä kasvutekijän kanssa.
Retrospektiivisessa tutkimuksessa selvitettiin huonon kantasolumobilisaation yleisyyttä eri sairauksissa ja rakennettiin huonosti mobilisoivien potilaiden veren valkosolujen ja CD34+ solujen kinetiikan perusteella algoritmeja pre-emptiivisen pleriksaforin käytön kriteereiksi. Mobilisaatiokinetiikan perusteella todettiin, että mikäli solunsalpaajalla ja kasvutekijällä toteutetun mobilisaation jälkeen veren valkosolumäärän ollessa nousussa (>5 x 109/L) ja veren CD34+ solujen määrä ollessa �10 x 106/L, olisi syytä harkita pleriksaforin käyttöä. Tämän mallin toimivuus on syytä varmistaa etenevässä tutkimuksessa.
Seuraavaksi tutkittiin pleriksaforin vaikutuksia veren solukoostumukseen kemomobilisaation saaneilla non-Hodgkin –lymfoomaa (NHL) sairastavilla. Illalla annetun pleriksafori-injektion todettiin lisäävän kantasolujen mobilisaatiota noin viisinkertaisesti seuraavan aamun mittauksissa. Lisäksi pleriksafori mobilisoi luuytimestä myös muita solupopulaatioita kuten neutrofiileja, lymfosyyttejä ja monosyyttejä.
Kahdessa osatyössä tutkittiin pleriksaforin vaikutuksia kantasolusolusiirteen solukoostumukseen solunsalpaajahoidolla ja kasvutekijällä mobilisoiduilla NHL-potilailla. Vertailuryhmänä olivat solunsalpaajaa ja kasvutekijää saaneet potilaat. Pleriksafori-injektion jälkeen kerätyssä siirteessä todettiin enemmän sekä primitiivisiä kantasoluja (CD34+CD133+CD38-) että enemmän T-lymfosyyttejä ja NK-soluja kuin kontrolliryhmässä. Pleriksafori-injektion vaikutukset näyttivät olevan samansuuntaisia myeloomaa sairastavilta potilailta kerätyissä siirteissä.
Pleriksaforin mahdollisia vaikutuksia kantasolujensiirron jälkeiseen toipumiseen ja pitkäaikaisennusteeseen selvitettiin NHL-potilailla. Pleriksaforilla mobilisoituja siirteitä saaneilla todettiin kontrolliryhmän kanssa verrannollinen hematopoieesin toipuminen ensimmäisen vuoden aikana kantasolujensiirron jälkeen. Myös tautivapaa- ja kokonaiselinaika olivat kontrolliryhmää vastaavat.
Tutkimussarja antaa lisätietoa pleriksaforin käytön tueksi huonosti mobilisoivilla potilailla. Siirteen solukoostumuksen merkitys sekä hematopoieettisen että immuunijärjestelmän toipumisen ja pitkäaikaisennusteen kannalta vaatii kuitenkin eteneviä tutkimuksia suuremmilla potilasmäärillä. Luokitus: QV 180, WH 540, WH 525, WH 380 Yleinen Suomalainen asiasanasto: pleriksafori, myelooma, non-Hodgkinin-lymfoomat, kantasoluhoito, kantasolujen siirto, kantasolut, siirrännäiset

VIII

IX
To patients with hematological malignancies

X

XI
Acknowledgements
This thesis was carried out at the Department of Medicine, Kuopio University Hospital and at the Laboratory of Eastern Finland (ISLAB) during the years 2010-2013.
I wish to thank Academy Professor Markku Laakso, M.D., PhD., Professor Kari Pulkki, M.D., Ph.D, Professor Juhani Nuutinen, M.D., Ph.D, Director of the Doctoral Programme of Clinical Research at the University of Eastern Finland, Docent Seppo Lehto, M.D., Ph.D., Chief Physician at the Department of Medicine, and Docent Kari Punnonen, M.D., Ph.D., Administrative Chief Physician at the Laboratory of Eastern Finland, for their positive attitude towards research work and arranging the facilities to perform this study.
I owe my deepest gratitude to my supervisors, Professor Esa Jantunen, M.D., Ph.D., and Pentti Mäntymaa, M.D., Ph.D., Clinical Consultant at the Laboratory of Eastern Finland, for all the support, guidance, trust, and patience during these past years. You have introduced me to scientific thinking and to the fascinating world of stem cell transplantations. I cannot thank you enough for what you have done for me.
I also wish to express my gratitude to Docent Tapio Nousiainen, M.D., Ph.D., Chief in Hematology at the Department of Medicine, for the support and possibility to perform this study.
I wish to warmly thank all my co-authors Docent Auni Juutilainen, M.D., Ph.D., Docent Taru Kuittinen, M.D., Ph.D., Docent Outi Kuittinen, M.D., Ph.D., Hanne Kuitunen, M.D., Anu Kutila, M.D., Päivi Lehtonen, M.D., Eija Mahlamäki, M.D., Maija Mikkola, M.D., Anne Nihtinen, M.D., Ph.D., Johanna Rimpiläinen, M.D., Raija Silvennoinen, M.D., Piia Valonen, Ph.D., and Kaija Vasala, M.D., Ph.D. Especially I wish to thank Riikka Juola, Laboratory Technician at the Laboratory of Eastern Finland, for skillful assistance in flow cytometric analyses.
I also warmly thank the official reviewers of the thesis manuscript, Docent Riitta Alitalo, M.D., Ph.D., and Docent Maija Itälä-Remes, M.D., Ph.D., for their constructive criticism and feedback. Based on their suggestions and comments, this thesis has improved.
I wish to thank Docent David Laaksonen, M.D., Ph.D., M.P.H., for careful and skillful revision of the language of this thesis.
I also owe my gratitude to Anu Räsänen, M.D., and Jonna Salonen, M.D., for guiding me during the early years of my clinical career and teaching me in the field of clinical hematology. I also would like to thank all my colleagues at the Department of Medicine in Kuopio University Hospital.
Finally, I am grateful to my friends (especially to the members of ’Sikaosasto’), relatives and family. I wish to express my thanks to my parents Anna-Maija and Jarmo. I also would like to thank my siblings Marika and Juha. Ultimately, my deepest thanks go to my wife Tiia for the encouragement and support.
This study was financially supported by grants from the Research Foundation of Blood Disease and the Finnish Society of Hematology and the EVO grant from North Savo Hospital District. All this support is gratefully acknowledged. Kuopio, September 2013 Ville Varmavuo

XII
List of the original publications
This dissertation is based on the following original publications:
I Jantunen E, Varmavuo V, Juutilainen A, Kuittinen T, Mahlamäki E, Mäntymaa P, Nousiainen T. Kinetics of blood CD34(+) cells after chemotherapy plus G-CSF in poor mobilizers: implications for pre-emptive plerixafor use. Ann Hematol 91:1073-9, 2012.
II Varmavuo V, Mäntymaa P, Kuittinen T, Nousiainen T, Jantunen E. Pre-emptive plerixafor injection increases blood neutrophil, lymphocyte and monocyte counts in addition to CD34(+) counts in patients with non-Hodgkin lymphoma mobilizing poorly with chemotherapy plus G-CSF: potential implications for apheresis and graft composition. Transfus Apher Sci 46:257-62, 2012.
III Varmavuo V, Mäntymaa P, Kuittinen T, Nousiainen T, Jantunen E. Blood graft lymphocyte subsets after plerixafor injection in non-Hodgkin's lymphoma patients mobilizing poorly with chemotherapy plus granulocyte-colony-stimulating factor. Transfusion 52:1785-91, 2012.
IV Varmavuo V, Mäntymaa P, Nousiainen T, Valonen P, Kuittinen T, Jantunen E.
Blood graft composition after plerixafor injection in NHL patients. Eur J Haematol 89:128-35, 2012.
V Varmavuo V, Mäntymaa P, Silvennoinen R, Nousiainen T, Kuittinen T, Jantunen
E. CD34+ cell subclasses and lymphocyte subsets in blood grafts collected after various mobilization methods in myeloma patients. Transfusion 53:1024-32, 2013.
VI Varmavuo V, Rimpiläinen J, Kuitunen H, Nihtinen A, Vasala K, Mikkola M, Kutila A, Lehtonen P, Kuittinen T, Mäntymaa P, Nousiainen T, Kuittinen O, Jantunen E. Engraftment and outcome after autologous stem cell transplantation in plerixafor-mobilized non-Hodgkin’s lymphoma patients. Transfusion 2013. Published online.
The publications were adapted with the permission of the copyright owners.

XIII

XIV
Contents
1 INTRODUCTION .............................................................................. 1 2 REVIEW OF THE LITERATURE ..................................................... 3
2.1. Autologous stem cell transplantation (ASCT) in clinical practice ................................................................................................... 3
2.1.1. Non-Hodgkin lymphomas (NHL) ..................................... 3 2.1.2. Hodgkin lymphoma (HL) ................................................... 4 2.1.3. Multiple myeloma (MM) ..................................................... 4
2.2. Mobilization of blood stem cells for autologous stem cell transplantation...................................................................................... 5
2.2.1. Mechanisms of stem cell homing and mobilization ........ 5 2.2.2. Mobilization with cytokine(s) ............................................. 6 2.2.3. Mobilization with chemotherapy plus granulocyte colony-stimulating factor (G-CSF) ............................................... 6 2.2.4. Hard-to-mobilize patients ................................................... 7 2.2.5. Novel strategies .................................................................... 7
2.3. Collection, enumeration and processing of stem cell grafts ... 8 2.3.1. Practical aspects of blood stem cell collection .................. 8 2.3.2. CD34 cell surface antigen .................................................... 8 2.3.3. Enumeration of blood CD34+ cells and assessment of graft CD34+ cell content ............................................................. 9 2.3.4. Cell viability and cultures ................................................... 10 2.3.5. Laboratory processing of the grafts ................................... 11
2.4. Plerixafor as a mobilizing agent .................................................. 11 2.4.1. Pharmacology and pharmacokinetics ............................... 11 2.4.2. Pharmacodynamics and mechanism of stem cell mobilization..................................................................................... 12 2.4.3. Development of plerixafor and preclinical studies ......... 13 2.4.4. Clinical studies (Phase I) ..................................................... 13 2.4.5. Clinical studies (Phase II) .................................................... 14 2.4.6. Clinical studies (Phase III) ................................................... 15 2.4.7. Use of plerixafor in patients mobilizing poorly ............... 16 2.4.8. Pre-emptive use of plerixafor ............................................. 17 2.4.9. Potential concerns regarding plerixafor use ..................... 20
2.5. Cellular composition of grafts in autologous stem cell transplantation...................................................................................... 20
2.5.1. Factors influencing graft cellular composition ................ 20 2.5.2. CD34+ stem cells and subclasses ......................................... 21 2.5.3. Lymphocytes ......................................................................... 22 2.5.3.1. T lymphocytes .................................................................... 23 2.5.3.2. Natural killer (NK) cells ................................................... 23 2.5.3.3. B lymphocytes .................................................................... 23
XV
2.5.4. Dendritic cells (DC) .............................................................. 23 2.5.5. Granulocytes.......................................................................... 23 2.5.6. Tumor cells ............................................................................ 24
3 AIMS OF THE STUDY ...................................................................... 25 4 PATIENTS AND METHODS ........................................................... 26
4.1. Patients ............................................................................................ 26 4.1.1. Kinetics of CD34+ cell mobilization and implications for pre-emptive plerixafor use (study I) ...................................... 26 4.1.2. Characteristics of NHL patients (studies II-IV, VI).......... 26 4.1.2.1. Effects of plerixafor injection on blood white blood cell (WBC) composition and CD34+ cell mobilization (study II) ................................................................... 26 4.1.2.2. Effects of plerixafor injection on the collected blood graft CD34+ cell subclasses, lymphocyte subsets and lymphocyte viability (studies III - IV).......................................... 26 4.1.2.3. Engraftment and outcome after ASCT (Study VI) ........ 27 4.1.3. Characteristics of MM patients (study V) ......................... 28
4.2. Methods .......................................................................................... 29 4.2.1. Clinical methods ................................................................... 29 4.2.1.1. Mobilization of stem cells ................................................. 29 4.2.1.2. Collection of stem cells ..................................................... 29 4.2.1.3. High-dose therapy ............................................................. 30 4.2.2. Laboratory methods ............................................................. 30 4.2.2.1. White blood cell differential counts ................................ 30 4.2.2.2. Enumeration of CD34+ cells in the blood and leukapheresis product .................................................................... 30 4.2.2.3. Laboratory processing and cryopreservation of the grafts ................................................................................................. 32 4.2.2.4. Flow cytometry of frozen grafts (studies III-V) ............. 33 4.2.2.5. Colony forming unit-granulocyte/macrophage (CFU-GM) assay (studies III-V) .................................................... 34 4.2.3. Quality assurance ................................................................. 34 4.2.4. Data collection ....................................................................... 34 4.2.5. Statistical methods ................................................................ 34
4.3. Approvals ....................................................................................... 35 5 RESULTS .............................................................................................. 36
5.1. Mobilization kinetics of CD34+ cells and implications for pre-emptive plerixafor use (study I)............................................ 36 5.2. Effects of plerixafor injection on blood CD34+ cell mobilization and WBC composition (studies II, VI) ....................... 38 5.3. Effects of plerixafor injection on the collected blood graft lymphocyte subsets and lymphocyte viability (studies III - V) ...................................................................................... 40

XVI
5.4. Effects of plerixafor injection on the collected blood graft CD34+ cell subclasses and viability (studies IV, V) ................ 42 5.5. Effects of plerixafor mobilized grafts on engraftment after high-dose therapy (studies III - VI) .......................................... 44 5.6. Outcome after ASCT in NHL patients (study VI) .................... 46
6 DISCUSSION ...................................................................................... 49
6.1. Patients and methods ................................................................... 49 6.1.1. Patients ................................................................................... 49 6.1.2. Clinical methods ................................................................... 49 6.1.3. Laboratory methods ............................................................. 50 6.1.4. Study methods ...................................................................... 50
6.2. Kinetics of CD34+ cell mobilization and implications for pre-emptive plerixafor use ........................................................... 51 6.3. CD34+ cell mobilization and peripheral blood WBC composition after plerixafor injection ............................................... 52 6.4. Lymphocyte subsets of the frozen grafts ................................... 52 6.5. CD34+ subclasses of the frozen grafts ......................................... 53 6.6. Viability of graft cells .................................................................... 54 6.7. Engraftment and outcome after ASCT ....................................... 54
7 CONCLUSIONS ................................................................................. 56 8 FUTURE PERSPECTIVES ................................................................. 57 9 REFERENCES ...................................................................................... 58 APPENDIX: ORIGINAL PUBLICATIONS I-VI

XVII
XVIII
Abbreviations 7-AAD 7-aminoactinomycin D
Ab antibody
ALC absolute lymphocyte count
APC allophycocyanin
ASCT autologous stem cell
transplantation
B blood
BEAC carmustine (BCNU),
etoposide, cytarabine,
cyclophosphamide
BEAM carmustine (BCNU),
etoposide, cytarabine,
melphalan
BFU-E erythroid burst forming unit
CCR C-C chemokine receptor
CFU-GEMM colony-forming unit-
granulocyte, erythrocyte,
macrophage, megakaryocyte
CFU-GM colony-forming unit-
granulocyte, macrophage
CG cathepsin G
CHOEP cyclophosphamide,
doxorubicin, etoposide,
vincristine, prednisone
CHOP cyclophosphamide,
doxorubicin, vincristine and
prednisone
CLL chronic lymphocytic leukemia
CLP common lymphoid
progenitors
CR complete remission
CUP compassionate use program
CXCL C-X-C ligand
CXCR C-X-C chemokine receptor
CY cyclophosphamide
d day
DC dendritic cell
DHAP dexamethasone, cytarabine,
cisplatin
DLBCL diffuse large B-cell lymphoma
DMSO dimethyl sulfoxide
DPPIV dipeptidyl-peptidase 4
EBMT European Group for Blood
and Marrow Transplantation
EFS event-free survival
Fimea Finnish Medicines Agency
FITC fluorescein isothiocyanate
FL follicular lymphoma
FSC forward scatter
G-CSF granulocyte colony-
stimulating factor
GM-CSF granulocyte macrophage-
colony stimulating factor
GOA Graft and Outcome in
Autologous stem cell
transplantation (prospective
study)

XIX
HD-AraC high-dose cytarabine
HDT high-dose therapy
HIV human immunodeficiency
virus
HL Hodgkin lymphoma
ICE ifosfamide, carboplatin,
etoposide
ISCT International Society for
Cellular Therapy
IVAC ifosfamide, etoposide, high-
dose cytarabine
IVE ifosfamide, epirubicin,
etoposide
MCL mantle cell lymphoma
MINE mesna, ifosfamide,
mitoxantrone, etoposide
MM multiple myeloma
MMP-9 metalloproteinase-9
MNC mononuclear cell
NHL non-Hodgkin lymphoma
OS overall survival
PCD plasma cell disorders
PCNSL primary central nervous
system lymphoma
pDC precursor dendritic cell
PE phycoerythrin
PerCP peridinin-chlorophyll-protein
PFS progression-free survival
PMN polymorphonuclear
PR partial remission
PTCL peripheral T-cell lymphoma
SC subcutaneous
SDF-1 stromal cell-derived factor-1
SSC side scatter
TRM treatment-related mortality
UK NEQAS United Kingdom National
External Quality Assessment
Service
WBC white blood cell
VCAM-1 vascular cell adhesion
molecule 1
VLA-4 very late antigen 4
WM Waldenstrom's
macroglobulinemia
Z-BEAC ibritumomab-tiuxetan plus
BEAC

XX

1 Introduction
Chemotherapy has been used in the treatment of lymphoid malignancies for decades. In some patients and disease types, chemotherapy can be curative. However, the efficacy of chemotherapy against tumor cells is dose-dependent (Frei and Canellos 1980). Higher doses are harmful for healthy tissues (e.g. bone marrow) and side-effects limit the doses used in clinical practice. To partially overcome these problems, high-dose therapy (HDT) supported by autologous stem cell transplantation (ASCT) is used in some clinical settings. The term ASCT is often used to comprise the whole treatment modality. HDT is the treatment, however, and ASCT constitutes rescue to ameliorate the consequences of the treatment.
In 2011, altogether 18,605 first ASCTs were reported to the European Group for Blood and Marrow Transplantation (EBMT). The two main indications were plasma cell disorders (PCD) [(8586 transplants, 46%; mostly multiple myeloma (MM)] and non-Hodgkin lymphomas (NHL) (5646 transplants, 30%; Passweg et al. 2013). In almost all transplants (99%), stem cell grafts collected from the peripheral blood were used. A successful stem cell mobilization and collection of blood stem cells are thus a prerequisite for ASCT. Depending on definition and study population, 5 – 30% of patients are hard to mobilize using traditional approaches (Pusic et al. 2008, Jantunen and Kvalheim 2010, Wuchter et al. 2010).
The only accepted quality parameters for autologous stem cell grafts have been the amount of CD34-positive (CD34+) stem cells collected and infused and post-transplant engraftment. Higher CD34+ cell doses have been linked to faster engraftment (Tricot et al. 1995, Weaver et al. 1995, Allan et al. 2002, Stiff et al. 2011) and in some studies also superior outcome post-transplant in terms of better progression-free survival (PFS) and overall survival (OS) (Blystad et al. 2004, O’Shea et al. 2006, Bolwell et al. 2007). Also other cells than CD34+ cells, e.g. various lymphocyte subsets, may have an important role in the recovery process after HDT and even for long-term survival (Porrata et al. 2004a, Porrata et al. 2004b. Katipamula et al. 2006, Schmidmaier et al. 2008, Atta et al. 2009, Jantunen and Fruehauf 2011). In addition, immaturity of stem cells may also have some impact on time of engraftment after ASCT (Hénon et al. 1998a, Zubair et al. 2006). Methods used to mobilize stem cells have an impact on the graft cell composition (Fruehauf and Tricot 2010, Jantunen and Fruehauf 2011) in addition to several patient- and disease-related factors.
Plerixafor, the latest approach in the armamentarium for stem cell mobilization, has been in clinical use only for a few years. Earlier studies have shown that it effectively mobilizes CD34+ stem cells from the bone marrow into the circulation (Liles et al. 2003, Broxmeier et al. 2005). It can be safely combined with growth factors, primarily with granulocyte colony-stimulating factor (G-CSF) (Flomenberg et al. 2005) or chemotherapy plus G-CSF (Dugan et al. 2010). In addition to use in patients who fail to mobilize stem cells, it can be used pre-emptively in patients who mobilize poorly (Jantunen et al. 2011, D'Addio et al. 2011, Jantunen and Lemoli 2012). In previous studies, mainly safety and efficacy in terms of mobilizing CD34+ cells with plerixafor have been investigated. These studies have shown that plerixafor not only mobilizes CD34+ cells but may also have impact on other cell populations (Fruehauf et al. 2010, Jantunen and Fruehauf 2011). Limited data are available on the pre-emptive use of plerixafor in chemomobilized patients in regard to graft composition, engraftment and outcome after HDT.
This study was performed in order to investigate the effects of plerixafor as a part of stem cell mobilization for ASCT. The main focuses were stem cell mobilization efficacy and cellular composition of the collected grafts. Studies were initiated by analyzing the incidence of poor mobilization in different disease entities. In the same study, an algorithm based on mobilization kinetics in chemomobilized patients was developed to guide the use of plerixafor. Subsequently, the effects of a single plerixafor injection on the white blood cell types and CD34+ cell counts were evaluated. Furthermore, blood graft samples collected from poorly mobilizing

2
patients with NHL or MM who were treated with plerixafor combined with chemomobilization or G-CSF mobilization were analyzed. Both CD34+ subclasses and lymphocyte subsets were investigated by flow cytometry of the cryopreserved grafts. Follow-up data with early and late engraftment and survival after HDT were also obtained in NHL patients mobilized with plerixafor in two university hospitals.

3
2 Review of the Literature
2.1. AUTOLOGOUS STEM CELL TRANSPLANTATION (ASCT) IN CLINICAL PRACTICE
2.1.1. Non-Hodgkin lymphomas (NHL) Diffuse large B-cell lymphoma (DLBCL) is the most common histological subtype of NHL, accounting for approximately 30% of all new lymphoma cases (Gunnellini et al. 2012). DLBCL is usually aggressive by its nature, and is currently treated with immunochemotherapy. The majority of the patients can be cured with modern therapy. Most randomized studies from the pre-rituximab era have not been able to confirm the superiority of HDT+ASCT consolidation after shortened or full-length induction therapy over conventional dose chemotherapy in the first-line treatment (Greb et al. 2008), although some controversial results have been published (Gianni et al. 1997, Haioun et al. 2000, Milpied et al. 2004). DLBCL is, however, currently the most common indication for ASCT among lymphomas (Baldomero et al. 2011), because ASCT has been shown to be superior in terms of PFS and OS as salvage therapy in patients with relapsed DLBCL (Philip et al. 1995). In spite of a lack of strong evidence, ASCT is also an option in patients with poor risk initial features and in those who do not obtain complete remission after first-line immunochemotherapy (Ljungman et al. 2010, Jantunen and Sureda 2012).
Follicular lymphomas (FL) have an indolent course of the disease. The role of ASCT in FL has been evaluated in several randomized studies after first-line therapy (Lenz et al. 2004, Deconinck et al. 2005, Sebban et al. 2006, Ladetto et al. 2008, Gyan et al. 2009). ASCT has been shown to give better PFS, but not OS benefit. The randomized CUP trial showed that ASCT provides a survival advantage over conventional chemotherapy in patients with relapsed FL (Schouten et al. 2003). Also several nonrandomized studies have shown promising outcome after ASCT in patients with relapsed FL (Brice et al. 2000, Rohatiner et al. 2007, Le Gouill et al. 2011). In addition, ASCT is useful in patients with FL transformed into DLBCL (Foran et al. 1998, Williams et al. 2001, Montoto et al. 2007, Hamadani et al. 2008, Villa et al. 2013).
Many peripheral T-cell lymphomas (PTCL) are clinically aggressive, and outcome with traditional chemotherapies is generally poor (Jantunen and Sureda 2012). Due to the rarity and heterogenenity of PTCL, the number of clinical studies investigating the role of ASCT in PTCL has been limited, and most data consists of from small retrospective series (Rodriguez et al. 2001, Blystad et al. 2001, Jantunen et al. 2004) or from two phase II prospective studies (Reimer et al. 2009, d'Amore et al. 2012). However, it is likely that some PTCL patients may benefit from ASCT as a part of first-line therapy (Reimer et al. 2009, d'Amore et al. 2012, Jantunen et al. 2013a). No randomized studies are currently available to assess the role of ASCT in PTCL.
Mantle cell lymphoma (MCL) has traditionally had a poor long-term outcome. ASCT was initially investigated as a treatment for relapse (Vose 2012). In this setting, long-term event-free survival (EFS) was a rare event (Vose et al. 2000). Intensive chemotherapy and front-line ASCT has been shown to improve long-term outcome and should be considered for eligible patients (Dreyling et al. 2005, Geisler et al. 2008, Geisler et al. 2012, Jantunen and Sureda 2012, Jantunen et al. 2012).
Most ASCT studies in B-cell lymphoproliferative diseases have been performed in the pre-rituximab era. Therefore results of these studies should be assessed with care, and there is an urgent need for new prospective studies (Appelbaum 2008, Jantunen and Sureda 2012).

4
2.1.2. Hodgkin lymphoma (HL) The prognosis of Hodgkin lymphoma is usually good, and up to 80 – 90% of the cases can be cured with initial chemotherapy with or without radiotherapy without ASCT (von Tresckow and Engert 2011). For relapsed disease, the prognosis is not as good. ASCT should be considered as standard therapy for these patients (Schmitz et al. 1993, Josting et al. 1998, Schmitz et al. 2002, Ansell 2012). In those few patients responding poorly to first-line chemotherapy, ASCT may also be considered after second-line salvage chemotherapy (Linch et al. 1993, Yuen et al. 1997, Lazarus et al. 1999, Moskowitz et al. 2001, Viviani et al. 2010, Rancea et al. 2013).
2.1.3. Multiple myeloma (MM) Multiple myeloma (MM) is a B-cell disorder characterized by proliferation of neoplastic cells of the plasma cell phenotype. Two decades ago, treatment of MM consisted of melphalan combined with prednisone (Gregory et al. 1992). Recently, new molecules have been developed and are now in wide clinical use. Currently, MM represents the most frequent indication for ASCT (Passweg et al. 2013), and ASCT has become part of standard therapy in symptomatic younger myeloma patients (Bird et al. 2011).
In some studies ASCT has been shown to improve EFS (Attal et al. 1996, Child et al. 2003, Fermand et al. 2005, Sonneveld et al. 2007) and OS (Attal et al. 1996, Child et al. 2003) when compared with standard therapy. However, not all studies have been able to confirm these observations (Segeren et al. 2003, Barlogie et al. 2006). Two recent meta-analyses showed that patients who were treated with a single ASCT had a significant PFS benefit, but not a survival advantage over standard chemotherapies (Koreth et al. 2007, Faussner and Dempke 2012). Prospective randomized studies are currently ongoing to evaluate the importance of HDT relative to the non-transplant approach in MM patients.

5
2.2. MOBILIZATION OF BLOOD STEM CELLS FOR AUTOLOGOUS STEM CELL TRANSPLANTATION
Figure 1. Hematopoietic stem cell niche and adhesion molecules. SDF-1, stromal cell-derived factor-1; CXCR4, C-X-C chemokine receptor type 4; CD26/DPPIV, dipeptidyl-peptidase 4; VLA-4, very late antigen 4; VCAM-1, vascular cell adhesion molecule 1.
2.2.1. Mechanisms of stem cell homing and mobilization Hematopoietic stem cells have two main specific characteristics that differentiate these cells from mature hematopoietic cells: they have the ability to self-renew and the ability to differentiate into all cell lineages of the blood and the immune system (Lymperi et al. 2010). In the steady state, the majority of hematopoietic stem cells reside in the bone marrow and their activity of proliferation, differentiation and release into the circulation is low (Lapidot and Kollet 2010).
The microenvironment where stem cells are located in the bone marrow is called a “niche” (Lymperi et al. 2010). The hematopoietic stem cell niche is a complex combination of different cell types and a three-dimensional matrix. Cell populations needed for the formation and regulation of the niche include osteoblasts (Mansour et al. 2012), sinusoidal endothelial cells (Sugiyama et al. 2006), reticular cells (Nagasawa et al. 2011), adipocytes (Naveiras et al. 2009) and mesenchymal stem cells (Méndez-Ferrer et al. 2010). In the niche, stem cells adhere to stromal cells with various ligands and receptors (Lymperi et al. 2010). Stromal cell-derived

6
factor (SDF-1 or SDF-�����-X-C ligand 12 (CXCL12) is regarded as the primary factor responsible for the retention of stem cells in the bone marrow (Lapidot and Petit 2002, Lapidot and Kollet 2010). Other adhesion molecules include C-X-C chemokine receptor type 4 (CXCR4), CXCR2 (Pelus et al. 2006), CD26 (Christopherson et al. 2004), CD44 (Zöller 2011), CD62L, very late antigen 4 (VLA-4), lymphocyte function-associated antigen-1, CD117 (c-Kit) (Cheng et al. 2010, Kimura et al. 2011) and Robo4 (Smith-Berdan et al. 2011, Rettig et al. 2012, Goto-Koshino et al. 2012). By influencing these adhesion molecules and the microenvironment, stem cells can be mobilized from the bone marrow to the circulation. The structure of the stem cell niche is illustrated in Fig 1.
Many adhesion molecules are also essential for the homing of stem cells. Homing is thought to be a rapid multistep process. Although many different cell types may home to the bone marrow, only stem cells homing into the hematopoietic niches can initiate a permanent repopulation (Lapidot et al. 2005). Stem cells may proceed from the circulation to the bone marrow by interaction with endothelial CXCR4 and SDF-1 (Lapidot et al. 2010). In addition, successful homing requires an activation of dynamic and regulated adhesion machinery (Lapidot et al. 2010).
2.2.2. Mobilization with cytokine(s) The most commonly used cytokine for stem cell mobilization is granulocyte colony-stimulating factor (G-CSF). The first growth factor for stem cell mobilization came into the clinics in 1990 (Jansen et al. 2002). Administration of G-CSF creates a proteolytic environment in the bone marrow by releasing many different proteases that interact with the adhesion molecules and the microenvironment and are therefore capable of mobilizing hematopoietic stem cells to the circulation (Motabi and DiPersio 2012). These proteases include e.g. SDF-1/CXCL12, metalloproteinase-9 (MMP-9), and cathepsin G (CG) (Heissig et al. 2002, Thomas et al. 2002, Lévesque et al. 2003).
Over the years, G-CSF has become the gold standard for the mobilization regimen because of its safety and efficacy (Thomas et al. 2002, Mohty and Ho 2011). The most widely used non-glycosylated G-CSF is filgrastim (Gertz 2010). Typically filgrastim is used over four consecutive days (usually 10 μg/kg/d) and apheresis is started on day 5. G-CSF is continued daily until an adequate graft has been collected. Alternatively, either glycosylated G-CSF (e.g. lenograstim) or GM-CSF (e.g. molgramostim) can be used for mobilization purposes (Kopf et al. 2006, Bensinger et al. 2009, Gertz 2010).
Pegfilgrastim is a pegylated form of filgrastim and it may also be used. Studies have shown that a single dose (usually 6 – 12 mg subcutaneous (SC)) of pegfilgrastim may be as effective as daily filgrastim injections in terms of stem cell mobilization (Russell et al. 2008, Kobbe et al. 2009, Putkonen et al. 2009, Simona et al. 2010). The most common side effects of pegfilgrastim are tenderness at the injection site and bone pain. These side effects are usually mild and similar to filgrastim.
In recent years, biosimilars to filgrastim have been introduced. Preliminary observations indicate that these can also be used for stem cell mobilization (Lefrère et al. 2011, Andreola et al. 2012). These biosimilar molecules are less costly than the original filgrastim or pegfilgrastim (Lefrère et al. 2011).
2.2.3. Mobilization with chemotherapy plus granulocyte colony-stimulating factor (G-CSF) The mobilization of stem cells from the bone marrow to the circulation and the so-called ‘rebound effect’ after chemotherapy was originally observed in middle 1970’s by Richmann et al (Richmann et al. 1976). The first studies of stem cell mobilization and collection after high-dose chemotherapy were published in late 1980’s (To et al. 1990). Cyclophosphamide as a single agent (from 1.5 g/m2 to up 7 g/m2) or a disease-specific combination of different drugs combined with G-CSF can be used as a mobilization regimen. The term “chemomobilization” refers to the use of chemotherapy plus G-CSF.

7
Chemomobilization has both advantages and disadvantages when compared to mobilization with G-CSF alone. The main advantage provided by chemomobilization is that it usually mobilizes more stem cells and thus fewer apheresis procedures are needed. It may also be considered as a treatment course for the underlying malignancy as it can provide tumor cytoreduction and in vivo purging (Desikan et al. 1998, Gertz 2010). On the other hand, chemomobilization is more toxic than G-CSF alone. Patients may have infections, leading to the hospitalization, and blood product transfusions are often needed (Koç et al. 2000, Gertz 2010). In addition, mobilization takes a longer time and the optimal time to start apheresis is more difficult to predict than mobilization with G-CSF alone (Hicks ML et al. 2007). The toxicity of chemotherapy depends on the dose of the drugs. This has been verified e.g. in the studies comparing low and intermediate doses of cyclophosphamide in myeloma patients (Jantunen et al. 2003a, Petrucci et al. 2003).
2.2.4. Hard-to-mobilize patients Depending on patient and disease characteristics as well as the definitions used, 5-30% of patients considered for autologous stem cell collection and transplantation are hard to mobilize. These patients are at high risk for a collection failure. A minimum blood graft for the single transplantation is commonly determined to include at least 2.0 x 106 CD34+ cells/recipient weight (kg). Many risk factors for poor mobilization are known (e.g. age, previous treatments and disease), but these do not effectively identify all these patients before mobilization (Jantunen et al. 2003b, Kuittinen et al. 2004, Jantunen and Kvalheim 2010, Olivieri et al. 2012).
If a patient is predicted to be hard to mobilize or even if the patient has failed to mobilize enough stem cells, there are some potential options. Different mobilization regimens have different potential to mobilize stem cells. Currently, the most effective combination for mobilizing stem cells is probably chemomobilization combined to plerixafor. Plerixafor can be used in a combination with chemomobilization or with G-CSF alone, and it can be used also in a pre-emptive manner (Awan et al. 2012, Jantunen and Lemoli 2012). If mobilization failure is imminent then remobilization may be considered. Some patients who fail to mobilize with G-CSF alone can be remobilized successfully. In these cases, chemomobilization or plerixafor plus G-CSF can enhance mobilization further (Pusic et al. 2008, Calandra et al. 2008, Jantunen 2011, Jantunen and Lemoli 2012).
Even if further mobilization attempts fail, bone marrow harvest may be used to collect a graft. However, it requires hospitalization, is associated with additional costs, discomfort to the patient and it is not available in every transplant center (Jantunen and Kvalheim 2010). In addition, use of harvested graft frequently results in delayed engraftment in poor mobilizers (Watts et al. 1998). The use of G-CSF-stimulated bone marrow grafts have been shown to be associated with faster engraftment (Lemoli et al. 2003, Gawronski et al. 2011). In some cases bone marrow graft and peripheral blood graft may be combined to achieve a satisfactory engraftment after ASCT (Sinitsyn et al. 2009). Theoretically, allogeneic bone marrow transplantation could also be a treatment option in patients who fail to mobilize stem cells for ASCT, but not all patients meet the other requirements for the procedure.
2.2.5. Novel strategies In addition to plerixafor, other recently evaluated CXCR4 antagonists are POL6326 (De Nigris et al. 2012), AMD3465 (Bodart V et al. 2009, De Clercq 2010), and T-140 (Abraham et al. 2007).
The next molecule to be evaluated in clinical trials ��� ����������������a ligand for receptor CXCR2. ���� -induced mobilization seems to be dependent also upon CXCR4 signaling (Christopher et al. 2009). In a murine model, ����has been shown to mobilize stem cells from the bone marrow to the circulation (Pelus et al. 2006, Fukuda et al. 2007). Also molecules interacting with VLA-4 have been studied for mobilization purposes (Ramirez et al. 2009, Rettig et al. 2012).

8
2.3. COLLECTION, ENUMERATION AND PROCESSING OF STEM CELL GRAFTS
2.3.1. Practical aspects of blood stem cell collection An adequate stem cell collection is a necessity for successful ASCT. In the beginning of the ASCT era, stem cells were collected by harvesting bone marrow. During the years, bone marrow harvesting has been replaced by peripheral blood apheresis and today almost all (99%) collections are performed by blood apheresis (Passweg et al. 2013).
The first continuous-flow apheresis device were developed in the early 1960s (Freireich et al. 1965, Körbling and Freireich 2011). Stem cell yield collected with these first-generation cell separators was low. In addition, patients did not receive any mobilization therapy and the amount of stem cells in peripheral blood is known to be low at a steady state. The first successful aphereses were performed in the 1970s (McCredie et al. 1971). However, an autologous bone marrow harvesting was the primary source of stem cells until mid-1990s when it was replaced by blood stem cell apheresis (Körbling and Freireich 2011). Currently, there are many different commercial apheresis systems available. These differ from each other in terms of technical solutions. Stem cell collection efficacy may vary between apheresis systems, and may be altered by the collection program and its settings (Wilke et al. 1999, Heuft et al. 2000, Sorensen et al. 2011, Wu et al. 2012). In addition, the best blood apheresis volume is still debatable (Abrahamsen et al. 2005, Gašová et al. 2010, Bojanic et al. 2011). In many institutions the apheresis volume is 2.5 – 3 times that of the estimated blood volume of the patient per session. Larger volume apheresis has also been used (Moog 2008, Zubair et al. 2009, Gertz 2010). Large-volume apheresis takes more time, and anticoagulant citrate dextrose has to be replaced by heparin. Apheresis-related factors may have an effect on the stem cell graft composition as different cell populations may be collected in different proportions (Lin et al. 1995, Katipamula et al. 2006, Ikeda et al. 2007).
Differences between bone marrow harvesting and blood apheresis have been evaluated in numerous studies. The apheresis procedure with a prior chemomobilization has been reported to cause less anxiety and pain for the patient when compared to marrow harvesting (Auquier et al. 1995). Platelet and neutrophil engraftment after ASCT is faster if a blood graft is used instead of a marrow graft (Geisler et al. 1998, Vellenga et al. 2001). The collection method used has been shown to have an impact on cell composition of the graft in healthy adults (Hassan et al. 1996). Engraftment with bone marrow grafts might be more rapid if G-CSF is used for priming before marrow collection (Lemoli et al. 2003, Gawronski et al. 2011). Stem cell source does not seem to have impact on survival after ASCT (Beyer et al. 1995, Schmitz et al. 1996). Total expenses of stem cell collection have been reported to be lower or at least similar when blood apheresis is used (Anderlini et al. 1996, Smith et al. 1997, Bredeson et al. 1997, Vellenga et al. 2001). Patients who fail to mobilize stem cells or fail to collect adequate peripheral blood stem cell grafts should be evaluated for re-mobilization or bone marrow harvest (Rick et al. 2000, Goterris et al. 2005).
2.3.2. CD34 cell surface antigen The CD34 cell surface antigen is a glycoprotein expressed by vascular endothelial cells and hematopoietic stem cells (Fina et al. 1990, Krause et al. 1996). The CD34 antigen belongs to the CD34 family of cell-surface transmembrane proteins that also include podocalyxin and endoglycan (Kerjaschki et al. 1984, Sassetti et al. 2000, Nielsen and McNagny 2008). The function of the CD34 antigen is not thoroughly known. It has been proposed to enhance the proliferation, block the differentiation of progenitor cells, and enhance the migration and trafficking of hematopoietic cells (Krause et al. 1996, Cheng et al. 1996, Hu et al. 1998, Nielsen and McNagny 2008).
In the steady state, the number of CD34+ cells is less than 0.1 % of all white blood cells (WBC) in the peripheral blood. Yet, CD34+ stem cells comprise 1 – 3 % of the bone marrow cells. In the clinical laboratory context, the CD34 antigen is most commonly used for the enumeration of

9
blood hematopoietic stem cells. As only stem cells homing into the bone marrow can initiate a permanent repopulation, the CD34+ cells have been linked to engraftment and also outcome after ASCT (Lapidot et al. 2005, Jantunen and Fruehauf 2011). CD34 may also be used as a part of flow cytometric diagnosis and subclassification in patients with acute leukemia (Krause et al. 1996, Buzzai and Licht 2008).
2.3.3. Enumeration of blood CD34+ cells and assessment of graft CD34+ cell content Precise enumeration of blood stem cells is useful in guiding stem cell apheresis and transplantation. The amount of CD34+ stem cells in the graft is routinely measured after the collection process. Measurements from patient blood are used to ensure adequate mobilization and to optimize the timing of apheresis (Yu et al. 1999, Lefrère et al. 2007). Blood CD34+ (B-CD34+) counts at the time of apheresis have been shown to correlate well with the CD34+ cell content in the apheresis product (Remes et al. 1997, Armitage et al. 1997, Hollingsworth et al. 1999, Villa et al. 2012). Aphereses are usually started when B-CD34+ is over 20 x 106/l. In some patients, aphereses are started with lower B-CD34+ levels. However, in these cases, additional collections may be required to achieve a sufficient total collection yield (Jantunen and Kuittinen 2008).
Figure 2. A basic principle of the flow cytometry.

10
Flow cytometric analysis of CD34+ stem cells was first introduced in early 1990s and during the years it has established its role as the gold standard (Siena et al. 1991, Keeney et al. 2004). The basic principle of flow cytometry is to induce interactions between cells and a laser beam. Cells cause the laser beam to scatter and this scattering can be measured. Forward scatter (FSC) is proportional to the size of the cell and side scatter (SSC) is proportional to the complexity of the cell (Virgo and Gibbs 2012). Additionally, fluorochromes are used to separate various cell populations. Fluorochromes are coupled with monoclonal antibodies, and therefore they are used when information about antigen structures on the cell surface is needed. Fluorochromes are molecules that can be excited to a higher energy level with a laser beam. This excitation discharges as a photon, which can be detected and measured. Commonly used fluorescent molecules are e.g. fluorescein isothiocyanate (FITC), phycoerythrin (PE), peridinin-chlorophyll-protein (PerCP) and allophycocyanin (APC) (Virgo and Gibbs 2012). In clinical practice, different fluorochromes are often used as panels. The main features of a flow cytometry device are presented Fig 2.
Guidelines for CD34+ enumeration were first published by the International Society of Hematotherapy and Graft Engineering (ISHAGE) in 1996 (Sutherland et al. 1996). In these guidelines, determination of CD34+ stem cells is based on the use of light scatter properties and two-color immunofluorescence by using CD45 FITC/CD34 PE fluorochromes. CD34 PE fluorochrome is recommended because of its brightness in the argon laser-based flow cytometer and because it makes possible a quantitative enumeration of CD34+ cells. Furthermore, the antibody clone used for CD34 detection should be either from class II or class III (e.g. 8G12 or 581). A minimum of one hundred CD34+ events and 75000 CD45+ events should be counted (Sutherland et al. 1996).
The original guidelines were based on a two-platform method, where an automated hematology analyser is used to measure the total amount of collected leukocytes and the proportion of CD34+ stem cells from all leukocytes is determined by flow cytometry. Later on a single-platform method was introduced (Keeney et al. 1998). This method is based on either volumetric measurements or the use of a known concentration of counting beads in the sample (Gratama et al. 1998). In a single-platform ISHAGE method, fluorescent microbeads are used at a known concentration. With the observed ratio between the number of flow cytometrically counted beads and CD34+ cells, the absolute CD34+ cell count can be calculated (Gratama et al. 1998). Both two- and single-platform methods have been shown to give equivalent results (Chapple et al. 2000, Gajkowska et al. 2006). However, the single-platform method is recommended due to a lower variability (Keeney et al. 1998).
Since flow cytometric analysis is more time-consuming and more expensive than routine blood cell analysis, also automated hematology analysers have been investigated for CD34+ enumeration. The preliminary results have been promising, but clinical applications have been restricted to screening of stem cell mobilization (Letestu et al. 2007, Lefrère et al. 2007, Yang et al. 2010).
2.3.4. Cell viability and cultures The viability of the collected stem cells is usually assessed by cell stainings and cultures. 7-
aminoactinomycin D (7-AAD) is a fluorescent derivative of actinomycin D. It can be used to exclude dead cells in flow cytometry (Schmid et al. 1994). In addition, 7-AAD can be used to distinguish apoptotic cells from dead cells (Zembruski et al. 2012). Also other stainings and markers for apoptotic and dead cells have been investigated. These include e.g. trypan blue, annexin V and SytoR16 (Schuurhuis et al. 2001, Abrahamsen et al. 2002a).
CFU-GM assay is often used to ensure the viability and differentiation potential of stem cells. This is very important as post-thaw parameters (such as CFU-GM) may be the most relevant for evaluating the graft quality (Decot et al. 2012). However, CFU-GM assay methods vary between transplant centers. Standardization of the culturing procedure and plating a fixed number of CD34+ cells have been proposed in order to improve the reliability and reproducibility

11
(Sheikhzadeh et al. 2001. Dobo et al. 2003, Decot et al. 2012). In addition to the traditional CFU-GM assay, other culturing methods have also been evaluated for clinical use (Motorin et al. 2003).
2.3.5. Laboratory processing of the grafts In the autologous setting, the collected grafts must be frozen in order to maintain the stem cells viable. As the freezing process may harm the stem cells, a cryoprotectant is routinely used. The most commonly used cryoprotectant for stem cell storage is dimethylsulfoxide (DMSO) (Windrum et al. 2005). DMSO prevents the formation of ice crystals and disruption of the cell membranes (Szmant 1975). DMSO is rather non-toxic to stem cells and also to the patient (Branch et al. 1994). However, it has been reported to cause many different adverse effects during re-infusion of grafts. The most common side effects include nausea, vomiting and abdominal cramps that may be caused by the intravenous infusion of a cold liquid (Zambelli et al. 1998). In addition, cardiovascular and respiratory problems and neurological toxicity have been reported (Zambelli et al. 1998, Ferrucci et al. 2000, Windrum et al. 2005). Some adverse effects in this setting may be due to other factors than DMSO itself (Bojanic et al. 2008). The most commonly used concentration of DMSO is 10%, but also other concentrations have been studied (Abrahamsen et al. 2002b, Liseth et al. 2005, Windrum et al. 2005, Abbruzzese et al. 2013). The concentration of DMSO may have an impact on the cellular composition of the graft and on the post-thaw viability and the clonogenic potential of stem cells (Akkök et al. 2009, Smagur et al. 2012). The amount of DMSO can be reduced by combining alternative cryoprotectants (Clarke et al. 2009).
During the time from collection to re-infusion, stem cell grafts are maintained in the freezer. Before freezing, grafts can be diluted to a lower cell concentration. In the most institutions, the final cell concentration during the cryopreservation is 1 x 108 to 2 x 108 nucleated cells per milliliter (Alencar et al. 2010). Nonetheless, the higher cell concentrations have also been reported to be safe (Rowley et al. 1994). Grafts are usually freezed by using an automated and controlled rate freezing program (Berz et al. 2007). The freezing program used and the duration of the cryopreservation may have an impact on the post-thaw viability of stem cells (Tijssen et al. 2008, Liseth et al. 2009, Fernyhough et al. 2013). Stem cell grafts are stored in either the liquid or vapor phase of nitrogen (most common) or at –80°C in mechanical freezers (Pamphilon et al. 2007). To avoid infectious contaminations, storage in the vapor phase has been recommended (Tedder et al. 1995).
The standard method for thawing is to warm grafts in a water bath at 37°C (Katayama et al. 1997). Use of a dry warming device designed for thawing has resulted in similar results (Röllig et al. 2002).
After cryopreservation and thawing, some transplantation centers wash the stem cell grafts before re-infusion in order to reduce the amount of DMSO (Windrum et al. 2005). It has been reported that washing reduces the incidence of adverse effects in the autologous setting (Syme et al. 2004, Sánchez-Salinas et al. 2012). However, the washing procedure may result in a loss of CD34+ cells and requires additional laboratory resources.
2.4. PLERIXAFOR AS A MOBILIZING AGENT
2.4.1. Pharmacology and pharmacokinetics Plerixafor is a bicyclam molecule with the structure 1,1�-[1,4-phenylenebis(methylene)]-bis-1,4,8,11-tetraazacyclotetradecane (De Clercq E et al. 1994). The initial synthesization process has been described in detail by Bridger and colleagues (Bridger et al. 1995). The chemical formula of plerixafor is depicted in Fig 3.

12
Figure 3. Chemical structure of plerixafor (previously AMD3100).
The pharmacokinetics of plerixafor have been extensively studied both in healthy adults (Hendrix et al. 2000, Lack et al. 2005) and in patients with non-Hodgkin lymphoma (NHL) (Stewart et al. 2009), Hodgkin lymphoma (HL) (Cashen et al. 2008) or multiple myeloma (MM) (Stewart et al. 2009). The pharmacokinetics was described using a two-compartment model with first-order absorption (Lack et al. 2005). Plerixafor exhibits linear kinetics in the 40 - 240 μg/kg dose range (Genzyme, summary of product characteristics). The pharmacokinetics of plerixafor was similar across clinical studies in healthy subjects who received plerixafor alone and in NHL or MM patients who received plerixafor in combination with granulocyte colony-stimulating factor (G-CSF) (Genzyme, summary of product characteristics). Some of the first clinical trials with plerixafor in humans were performed with intravenous administration (Hendrix et al. 2004). Currently, the recommended dose of plerixafor is 240 μg/kg body weight by SC injection in patients with normal renal function.
Plerixafor is mainly excreted by the kidneys. In the study of Hendrix et al., the clearance and estimated half-life (mean 8.6 hours, range: 8.1 – 11.1 hours) of plerixafor were similar across all given doses implying dose independency (Hendrix et al. 2004). However, in the case of renal ���������� ����������� ��������� �!" �#������ the dosage should be reduced (Genzyme, summary of product characteristics). Co-administration of plerixafor with drugs that reduce renal function or compete for active tubular secretion may increase serum concentrations of plerixafor or the co-administered drug. In clinical trials, age or gender have not had any effect on plerixafor pharmacokinetics (Genzyme, summary of product characteristics).
2.4.2. Pharmacodynamics and mechanism of stem cell mobilization Many hematopoietic and non-hematopoietic cells express CXCR4 on their surfaces (Nagasawa et al. 1998). Plerixafor selectively antagonizes CXCR4 by binding to three acidic residues in the main ligand-binding pocket of CXCR4 (Asp171 in transmembrane domain [TM]-IV, Asp262 in TM-VI and Glu288 in TM-VII) (Wong et al. 2008). By antagonizing CXCR4, plerixafor inhibits binding of stromal cell-derived factor SDF-1/CXCL12 (Fricker et al. 2006). This disruption results in a rapid mobilization of stem cells from the bone marrow to the circulation (Broxmeyer et al. 2005, Martin et al. 2006). Other stem cell mobilizing agents (e.g. G-CSF) have been reported to have same kind of effect (Lévesque et al. 2003).
Plerixafor is highly selective for CXCR4 and it has only a minor interaction with some other similar receptors (e.g. CXCR1-3 or CCR1-9) (Fricker et al. 2006). Binding to CXCR4 is both concentration and time dependent and is slowly reversible (Fricker et al. 2006). Some studies have suggested that plerixafor is a weak partial agonist (Zhang et al. 2002) while others have found no agonist activity on CXCR4 (Fricker et al. 2006).

13
Mobilization of WBC and CD34+ is a dose-dependent phenomenom (Liles et al. 2003, Hübel et al. 2004) and occurs typically 6 - 9 hours after SC administration of plerixafor (Liles et al. 2003, Hübel et al. 2004, Devine et al. 2004). When plerixafor is given with G-CSF (usually given in the morning), elevation in the peripheral blood CD34+ count is observed from 4 to 18 hours after plerixafor administration with a peak CD34+ count measured between 10 and 14 hours.
2.4.3. Development of plerixafor and preclinical studies In 1992, Erik de Clercq and colleagues reported a newly discovered class of potent and selective human immunodeficiency virus (HIV) inhibitors (De Clercq et al. 1992). In their studies, one of the tested preparations was found to be quite effective against both HIV-1 and HIV-2. That drug was characterized by a bicyclam structure in which two cyclam rings were tethered by a direct carbon-carbon linkage. Later on, it was noticed that if the aliphatic bridge was replaced by an aromatic bridge, the potency was increased up to 100-fold (De Clercq 2009).
One of the tested bicyclam compounds with the aromatic bridge was JM2987. It showed inhibitory activity against the replication of HIV-1 and HIV-2, but was not toxic to the host cells. Actually, JM2987 is almost the same compound as JM3100: JM2987 is octahydrobromide dehydrate (a bromide salt) and JM3100 is octahydrochloride dehydrate (a chloride salt) (De Clercq et al. 1994). As the two salts were equipotent, all further experiments were performed with JM3100 (De Clercq 2009). For further development JM3100 was subsequently transferred from Johnson Matthey to AnorMED and the “JM” prefix was replaced by “AMD” (De Clercq 2009). AMD3100 is now generally known as plerixafor.
In the beginning, it was thought that plerixafor mediated its anti-HIV activity via viral glycoprotein (gp120) (De Vreese K et al. 1997). However, later studies showed that plerixafor interacted with CXCR4, which was the actual mechanism of action (Schols et al. 1997a, Schols et al. 1997b, Donzella et al. 1998, Esté et al. 1999, Egberink et al. 1999).
2.4.4. Clinical studies (Phase I) The potential of plerixafor to mobilize stem cells from bone marrow was found in a phase I clinical trial. In that trial, forty HIV-infected patients with an HIV ribonucleic acid (RNA) level >5000 copies/mL and on stable antiretroviral regimens or off therapy were studied. Plerixafor showed no or only minimal antiviral activity, as only one patient had a significant HIV RNA reduction and the average change in the viral load in all patients was +0.03 log10 HIV RNA. Unexpectedly, a rapid leukocytosis (an estimated maximum effect of 3.4 times compared to the baseline) was observed in all patients after infusion of plerixafor (Hendrix et al. 2004).
This anecdotal finding of leukocytosis was soon assessed more thoroughly (Liles et al. 2003). Administration of a single dose of plerixafor caused a dose-dependent leukocytosis in healthy subjects. The differential white blood counts showed that the number of neutrophils, lymphocytes, monocytes, eosinophils, and basophils all increased (Hübel et al. 2004, Broxmeyer et al. 2005). Of note, the amount of CD34+ stem cells increased in the peripheral blood after plerixafor injection and a large proportion of mobilized CD34+ cells were c-kit positive (Broxmeyer et al. 2005). In addition, there was a significant increase in colony forming unit-granulocyte/macrophage (CFU-GM), erythroid burst forming units (BFU-E) and colony-forming unit-granulocyte, erythrocyte, macrophage, megakaryocyte (CFU-GEMM) in the grafts collected after plerixafor (Broxmeyer et al. 2005). These observations finally concluded that plerixafor mobilizes pluripotent hematopoietic stem cells from the bone marrow to the circulation.
Later, Liles and colleagues studied the effects of plerixafor (160 μg/kg x 1 on day 5) in combination with G-CSF (10 μg/kg/day) on mobilization and collection of CD34+ cells from healthy subjects (Liles et al. 2005). They showed that plerixafor could be used in combination with G-CSF. The combination of these two drugs resulted in higher CD34+ stem cell yields than G-CSF alone (Liles et al. 2005). They also observed that when plerixafor was used the

14
leukapheresis products contained significantly higher numbers of T and B lymphocytes than G-CSF-mobilized leukapheresis products (Liles et al. 2005).
In an additional phase Ib study plerixafor was evaluated with G-CSF in patients with hematological malignancies (Devine et al. 2004). That study included thirteen patients with NHL or MM. The results were quite similar to those observed on healthy subjects (Liles et al. 2005): plerixafor caused a rapid and statistically significant increase in the total WBC and CD34+ counts following a single injection (Devine et al. 2004).
The safety and possible adverse effects of SC injection of plerixafor were studied in both phase I studies mentioned before. Plerixafor had only mild and transient adverse effects when used alone or in combination with G-CSF (Liles et al. 2005). The most common side effects observed were skin erythema at the injection site, abdominal discomfort and flatulence (Devine et al. 2004).
2.4.5. Clinical studies (Phase II) The first phase II study was carried out by Flomenberg et al. (Flomenberg et al. 2005). The primary objective of that study was to determine whether patients with MM or NHL mobilized more progenitor cells per unit blood volume of apheresis after treatment with plerixafor combined with G-CSF compared to G-CSF alone. The secondary objectives included the number of apheresis procedures needed and engraftment after HDT (Flomenberg et al. 2005). All twenty-five patients were mobilized twice: once with G-CSF only and once with a combination of plerixafor and G-CSF, thus allowing each patient to serve as his or her own control. The patients had a two week wash-out period between these two mobilization rounds. G-CSF mobilization consisted of daily SC morning administration of G-CSF 10 μg/kg of actual body weight. Apheresis was initially begun on d 4 of G-CSF administration. Apheresis and G-CSF were continued daily for up to 4 consecutive daily collections until at least 5 x 106 CD34+ cells/kg had been collected, whichever occurred first. The dose of plerixafor was 160 μg/kg for the first eight patients and 240 μg/kg for the rest of the patients. The first dose of plerixafor was given on d 4 and was administered SC followed 6 hours later by apheresis. Plerixafor, G-CSF, and apheresis were continued daily thereafter through day 8 similar to the G-CSF treated patients. In every case, more hematopoietic stem cells were collected per day of apheresis after plerixafor + G-CSF mobilization than after G-CSF alone, irrespective of which regimen was used first. In addition, nine patients failed (36%) to ach��$� ��� �����*� <��=� ? @ \ �"6 CD34+ cells/kg when mobilized with G-CSF alone, but in each of these patients, plerixafor + G-CSF was successful in obtaining a sufficient graft. It was concluded that by combining plerixafor with G-CSF it was possible to avoid a mobilization failure in the case of poor mobilization with G-CSF alone. Other potential benefits from the use of plerixafor were a lower number of apheresis procedures and a higher number of collected CD34+ stem cells. Neutrophil engraftment after ASCT was similar between the groups (Flomenberg et al. 2005).
In 2007, a study involving eleven refractory or relapsed patients with NHL who were mobilized with plerixafor combined to G-CSF was published (Gazitt et al. 2007). In that study, adequate collection of the target dose of CD34+ stem cells was achieved in all but one patient with two days of collection. The dose of G-CSF was 16 μg/kg/d for four days. In addition, all patients were treated with plerixafor (240 μg/kg/d). Both drugs were continued until the collection target dose of > 2 x 106 CD34+ cells/kg was achieved. All transplanted patients engrafted with a mean of ten and twelve days for neutrophils and platelets, respectively. This study also contained a comprehensive flow cytometric analysis performed after plerixafor injection. It was shown that plerixafor induced mobilization of certain dendritic cell populations (Gazitt et al. 2007). Mobilization of tumor cells was also evaluated but was not observed (Gazitt et al. 2007).
The third phase II study was published by Stiff and colleagues in 2009 (Stiff et al. 2009). Their study had some similarities to Flomenberg’s earlier study (e.g. inclusion criteria). Altogether 49 patients (23 with NHL and 26 with MM) were enrolled. The plerixafor dose was 240 μg/kg/d

15
and it was combined with G-CSF (10 μg/kg/d). Twenty-eight patients (57%) were considered as heavily pretreated. Adequate stem cell grafts were collected from 47 of 49 patients (96%) with a median stem cell yield of 5.9 x 106 CD34+ cells/kg. After ASCT, the median days to neutrophil and platelet engraftment were eleven days and 14.5 days, respectively (Stiff et al. 2009).
The efficacy of plerixafor and G-CSF in poorly mobilizing patients was further investigated in patients with MM by Tricot and colleagues (Tricot et al. 2010). They mobilized twenty patients (ten proven poor mobilizers and ten predicted poor mobilizers) with a combination of plerixafor and G-CSF. In fifteen patients (75%) at least 2 x 106 CD34+ cells/kg were collected. Only one patient (5%) did not achieve a sufficient stem cell graft for transplantation. Among the proven poor mobilizers, there was no evidence of tumor cell mobilization. Seventeen patients proceeded to transplantation. Pooled cells from other collections were used in eight patients (47%). Platelet engraftment occurred at a median of sixteen days and nineteen days for proven and predicted poor mobilizers, respectively (Tricot et al. 2010).
One phase II study investigated the potential of plerixafor in patients with HL (Cashen et al. 2008). That study included 22 patients with relapsed or refractory HL. These patients were treated with G-CSF (10 μg/kg/d) and plerixafor (240 μg/kg) and they were compared to historical controls mobilized with G-CSF only. In fifteen patients (68%) at least 5 x 106 CD34+ cells/kg were collected and twenty-one patients (95%) achieved the minimum collection target of at least 2 x 106 CD34+ cells/kg. The collection yields in days 1-2 of apheresis were significantly improved over historical controls. Pharmacokinetics of plerixafor was also assessed and it was similar to that previously seen in healthy volunteers (Cashen et al. 2008).
Results from the US expanded access program have been published by Shaughnessy et al. (Shaughnessy et al. 2013). The total number of plerixafor-treated patients was 104 (54 patients with MM, 43 with NHL, and 7 with HD). In ninety-seven (93%) patients, 2 x 106 CD34+ cells/kg were collected in 1–3 days of apheresis. A total of 92 patients (87%) proceeded to ASCT. All these patients had a successful engraftment after ASCT (Shaughnessy et al. 2013).
The vast majority of phase II studies investigated plerixafor in a combination with G-CSF. However, one phase II study investigating the efficacy and the safety of plerixafor in a chemomobilization setting was also performed. For the study of Dugan and colleagues forty patients were enrolled (14 with NHL, 26 with MM) (Dugan et al. 2010). All patients were treated with SC plerixafor 240 μg/kg/d for up to five days after chemotherapy (regimen selection was based on disease) plus G-CSF. The addition of plerixafor to a chemomobilization resulted in an increase in the peripheral blood CD34+ cells and was well tolerated. After ASCT, the median times to neutrophil and platelet engraftment were eleven days and 13 days, respectively. Thirty-five patients completed 12 months post-transplant follow-up and they all had durable engraftment (Dugan et al. 2010).
2.4.6. Clinical studies (Phase III) Subsequently, two phase III studies were performed in the United States and Europe, which eventually led to the approval of the drug for clinical use for stem cell mobilization in the autologous setting. The first study involved patients with NHL (DiPersio et al. 2009a) and the second study patients with MM (DiPersio et al. 2009b). Both studies were multicenter, randomized (1:1), double-blind and placebo-controlled, and the study designs were quite similar.
In the first study, patients with NHL (DiPersio et al. 2009a) requiring an autologous hematopoietic stem cell transplantation who were in their first or second complete remission (CR) or partial remission (PR) were eligible for enrollment. All patients received G-CSF (10 μg/kg) SC daily for up to 8 days. Beginning on the evening of d 4 and continuing daily for up to 4 days, the patients received either plerixafor (240 μg/kg) or placebo SC. Aphereses were started on d 5, ��^^���������������� ����*�^ = �*� � _^�� �*���� ?!`�"6 CD34+ cells/kg were collected. The primary end point was the percentage of patients who collected

16
? ! ` �"6 CD34+ �����{< �� � _ ������� ^��| }�� �����*� �*���� = �~�_� ���� = �transplantation was 2 × 106 cells/kg.
Altogether 298 patients were enrolled in the study. A significantly greater proportion of ������� ����������\�= �<� *��!�|��������$�^������������^� ��� =� �������<?!`�"6 CD34+ �����{<���_�������^������� �����^ with the placebo group (19.6%). Also ?@`106 CD34+ �����{< ���_�������^������*���=*���� ������^ in a greater proportion of patients in the plerixafor group (86.7%) compared with the placebo group (47.3%). For all patients who underwent apheresis, the median number of CD34+ cells collected was 5.69 × 106 cells/kg for plerixafor-treated patients and 1.98 × 106 cells/kg for placebo-treated patients. Sufficient stem cell yield was not achieved in ten plerixafor-treated (6.8%) and 52 placebo-treated (36.6%) patients, respectively. These patients entered the rescue protocol.
Altogether 135 of 150 (90.0%) plerixafor-treated patients underwent ASCT after initial mobilization versus 82 of 148 (55.4%) in the control group. Among transplanted patients, plerixafor-treated patients received a median of 5.41 × 106 CD34+ cells/kg and placebo-treated patients received 3.85 × 106 CD34+ cells/kg. All patients who received transplantation in had successful neutrophil engraftment and 98% had successful platelet engraftment. The median time to engraftment was 10 days for neutrophils and 20 days for platelets in both groups. For patients who had undergone transplantation after an initial mobilization (135 in plerixafor group and 82 in placebo group), survival at 12 months follow-up visit was similar (88.1% in the plerixafor group and 86.6% in the placebo group).
In the study of patients with MM (DiPersio et al. 2009b), 302 patients were enrolled. A significantly greater proportion of patients in the plerixafor group yielded ? 6 × 106 CD34+ cells/kg with �2 apheresis than in the placebo group (71.6% vs. 34.4%). The median number of apheresis days required to collect that amount of stem cells was one day in the plerixafor group compared with four days in the placebo group. The engraftment after ASCT was similar between the groups.
In both studies, the most commonly observed adverse effects of plerixafor were injection site erythema and gastrointestinal disorders. Most of the adverse events were mild or moderate and only a few adverse events leading to discontinuation were seen (DiPersio et al. 2009a, DiPersio et al. 2009b).
Both studies included a rescue protocol for patients mobilizing poorly. The results of this patient population in the NHL study were published by Micallef et al. (Micallef et al. 2009). Altogether 62 patients were enrolled and in 37 of them (59.7%) at least 2.0 × 106 CD34+ cells/kg were collected after mobilization with G-CSF plus plerixafor. Fifty-two patients (83.8%) were subsequently transplanted. After ASCT, all patients had neutrophil engraftment and in addition, all but two patients had also sustained platelet engraftment.
Furthermore, a subset analysis of the Phase III trial with MM patients showed that plerixafor caused mobilization of stem cells that was not dependent on a prior B-CD34+ cell count, and the total yield of CD34+ cells from apheresis was significantly higher in the plerixafor group than in the placebo group (Nademanee et al. 2012).
2.4.7. Use of plerixafor in patients mobilizing poorly The first larger study with plerixafor in patients who were proven to mobilize poorly was performed by Calandra et al. (Calandra et al. 2008). Altogether 115 patients with NHL, MM or HL who had failed to mobilize a minimum graft were enrolled in that study. Patients were mobilized with G-CSF followed by plerixafor. Plerixafor was started on day 4 and was continued daily as well as G-CSF until an adequate graft was obtained. More than 2.0 x 106 CD34+ cells/kg were collected in 77 patients (66%). When combined with previous collections, altogether 87 patients (76%) were eligible to proceed to transplantation. The engratment data was available for 36 patients (41%). Thirty-four of these patients (94%) had a durable engraftment and were alive at least up to 12 months (Calandra et al. 2008).

17
The compassionate use program (CUP) for plerixafor opened in July 2008 in Europe. It was allocated for patients with NHL, HL or MM who had experienced a mobilization failure and were not suitable for registration trials (Duarte et al. 2011). The first published data from the European CUP was based on a series of 56 patients (24 patients with NHL and 32 patients with myeloma) (Duarte et al. 2011). Altogether, there were 73 prior mobilization failures among these patients. In that trial, patients were mobilized with G-CSF (10 μg/kg/d) and plerixafor (240 μg/kg). The first plerixafor injection was given in the evening of the fourth day. G-CSF and plerixafor injections were continued daily until 2.0 x 106 CD34+ cells/kg were collected or mobilization failure was obvious. After mobilization therapy, 42 of 52 (75%) of patients were successfully collected with at least 2.0 x 106 CD34+ cells/kg. Thirty-five out of 56 patients (63%) had been transplanted by the time of analysis. All patients had both neutrophil and platelet engraftment after ASCT.
More extensive experience in the European CUP trial was subsequently published by Hübel and colleagues (Hübel et al. 2012). It contained altogether 580 patients (270 patients with NHL, 54 patients with HL and 256 patients with MM). The mobilization process was similar to the original CUP study. The median stem cell yield was 3.1 x 106 CD34+ cells/kg and the collection ���<�� =?@|"\�"6 CD34+ cells/kg was achieved in 428 (73.8%) patients. The CD34+ stem cell yield was significantly higher in patients with MM than in patients with NHL. No post-ASCT analysis was included. In the substudy of the German CUP, poorly mobilizing patients mobilized with chemotherapy and/or G-CSF and plerixafor were studied (Hübel et al. 2011). The series included 60 patients (28 patients with NHL, 17 patients with MM and 15 patients with other malignancies). The median total stem cell yield was 2.2 x 106 CD34+ cells/kg among patients with NHL. All transplanted patients had durable engraftment after ASCT. Additional subanalysis and reports based on the CUP trial patients have been published (Fowler et al. 2009, Selleslag et al. 2011, Basak et al. 2011). These studies have confirmed that plerixafor can be used in addition to G-CSF or also with chemotherapy and mobilizes significantly more CD34+ stem cells when compared to the traditional approaches, even in patients with a prior mobilization failure.
Only a few studies about long-term engraftment or outcome are available in this setting. Moreb et al. reported outcomes of nine lymphoma and eight MM patients that were treated with G-CSF mobilization and received plerixafor as a rescue mobilization in the CUP. In their study, long-term engraftment and hospital course were similar between poorly mobilizing patients and the control group. Due to the retrospective nature and small number of patients, no comparison between groups in outcomes was performed (Moreb et al. 2011). Engraftment after ASCT has been reported to be slightly delayed in patients who have been mobilized with G-CSF and who have received plerixafor due to inadequate mobilization when compared to standard mobilizers (Alexander et al. 2011).
2.4.8. Pre-emptive use of plerixafor The possible utility of plerixafor has been studied also in a pre-emptive setting. In this context, the term pre-emptive means that plerixafor is given only if it becomes apparent that stem cell mobilization will be inadequate with traditional methods (chemotherapy and/or G-CSF). This approach may be beneficial in terms of cost-effective use of plerixafor (Jantunen 2011). Other terms used in this setting are just-in-time, add-on, rescue and salvage use.
Pre-emptive use of plerixafor has been primarily studied in a few small studies among patients with NHL or MM (Jantunen et al. 2011, D'Addio et al. 2011, Gopal et al. 2012, Horwitz et al. 2011). The retrospective study of Jantunen et al. (Jantunen et al. 2011) included altogether 63 patients (32 patients with NHL, 29 patients with MM and 2 patients with HL). All patients were mobilized with chemotherapy plus G-CSF. In addition, plerixafor was given to 16 patients (25%) due to poor stem cell mobilization or due to insufficient stem cell yield of the prior aphereses. The median increase in blood CD34+ count was five-fold after the first plerixafor injection. Thirteen out of sixteen patients (80%) obtained at least 2.0 x 106 CD34+ cells/kg. All

18
these patients proceeded to ASCT, and all but one patient had neutrophil and platelet engraftment. The results from the study of D'Addio were similar, but the minimum collection target was achieved in all patients (D'Addio et al. 2011).
In the study by Alexander et al., altogether 96 MM and NHL patients were retrospectively analyzed. Patients were mobilized with cyclophosphamide plus G-CSF and GM-CSF or G-CSF alone. In addition, 32 patients mobilized with G-CSF received plerixafor due to inadequate mobilization. The investigators reported that neutrophil and platelet engraftment was significantly slower in the group of plerixafor-mobilized patients when compared to other groups. However, there was no significant difference in WBC count, absolute neutrophil count, or platelet count among groups at d +100. No comparisons between groups in regard to long-term engraftment or outcomes were performed (Alexander et al. 2011).
In clinical practice, it may be hard to identify in advance patients who mobilize poorly and require plerixafor. Therefore, various algorithms to help this identification have been developed (Costa et al. 2011, Chen et al. 2012, Sinha et al. 2011, Ozsan et al. 2012, Sancho et al. 2012, Abhyankar et al. 2012, Micallef et al. 2013, Milone et al. 2013, Abusin et al. 2013, Hay et al. 2013). These algorithms are usually based on predictive factors that are patient dependent, including blood CD34+ cell counts, blood WBC counts or stem cell yields. Most of the algorithms are based on G-CSF mobilization and only a few algorithms for chemomobilization have been published. None of the published algorithms have been accepted widely for clinical use. While different transplant centers have their own distinctive mobilization methods, guidelines and practices, it has been suggested that each center should determine their own trigger or cut-off levels (To et al. 2011). A summary of published algorithms to guide pre-emptive use of plerixafor is presented in Table 1.

19
Table 1. Summary of published algorithms to guide pre-emptive use of plerixafor.
Study Number of included patients
Diseases Mobilization method
Suggested trigger/cut-off level for plerixafor
Costa et al. 2011 50 lymphomas, MM
G-CSF alone Calculated individually on d4 based on B-CD34+ count and collection
target
Chen et al. 2012 49 lymphomas, MM
G-CSF alone B-CD34+ 5 – 15 x 106/L on d4
Sinha et al. 2011 1556 lymphomas, PCD
G-CSF alone B-CD34+ <6 x 106/L on d4 or B-CD34+ <10 x 106/L on d5 or first
collection yield <1.0 x 106 CD34 cells/kg
Abusin et al. 2013.
130 lymphomas, PCD
G-CSF alone B-CD34+ �������6/L on d4
Abhyankar et al. 2012.
159 lymphomas, PCD, solid
tumors
G-CSF alone B-CD34+ <10 x 106/L on d5 (target ��������6 CD34 cells/kg) or
B-CD34+ >10 x 106/L but <20 x 106/L on d5 (�� ���������6 CD34
cells/kg) or first collection yield is less than one-half of the desired
dose
Sancho et al. 2012.
397 lymphomas, MM, acute myeloid
leukemia and other
G-CSF alone (mainly) or chemotherapy +
G-CSF
A peak value of B-CD34+ ��������6/L
Micallef et al. 2013.
592 lymphomas, PCD
G-CSF alone (mainly) or chemotherapy +
G-CSF
Algorithm I: B-CD34+ <10 x 106/L on d4 or d5 or any collection yield <0.5 x 106 CD34
cells/kg
Algorithm II: B-CD34+ <10 x 106/L for single
transplantation and <20 x 106/L for multiple transplantations on d4 or
first collection yield <1.5 x 106 CD34 cells/kg or any collection yield <0.5
x 106 CD34 cells/kg
Milone et al. 2013.
233 lymphomas, MM
cyclophosphamide 4 g/m2 + G-CSF
B-CD34+ <6 x 106/L on d12 or B-CD34+ <10 x 106/L on d13
Ozsan et al. 2012.
396 MM cyclophosphamide 3 g/m2 + G-CSF
B-CD34+ <10 x 106/L on d13 or 1 d after WBC>1
Hay et al. 2013. 354 lymphomas, MM, acute myeloid
leukemia and other
chemotherapy + G-CSF
A peak value of B-CD34+ <16.5 x 106/L

20
2.4.9. Potential concerns regarding plerixafor use As discussed earlier, plerixafor is well tolerated and severe adverse effects are seen rarely. There are not much data or studies with long follow-up concerning long-term effects. In larger studies, the follow-up period has usually been up to 12 months. This is enough to assess engraftment, but not enough to assess possible effects of plerixafor regarding patient survival. Of note, a higher incidence of therapy-related myelodysplastic syndrome/acute myeloid leukemia after ASCT has been reported in patients with plerixafor mobilized stem cells (Deol et al. 2013).
One of the concerns with a mobilizing agent is the potential for tumor cell mobilization. Yet, the relevance of graft tumor cell contamination is still debatable (DiPersio et al. 2011). One study assessed tumor cell mobilization in myeloma patients, and it seemed that the combination of G-CSF plus plerixafor did not increase mobilization of clonal tumor cells compared to G-CSF only mobilization (Fruehauf et al. 2010). A similar result has been reported for NHL patients too (DiPersio et al. 2009). No data are available in this regard for plerixafor combined with chemomobilization in lymphoma patients. In addition, plerixafor not only mobilizes stem cells, but also other cell populations are mobilized from the bone marrow to the circulation (Liles et al. 2003). These mobilized cells may be collected during the apheresis procedures. This may lead to a lower ratio of CD34+ cells and result in greater storage costs (Tanhehco et al. 2010).
In September 2013, the official price of one 24 mg plerixafor dose in Finland was 7786.82 €. As some patients require multiple doses, the total costs of plerixafor alone can rise to substantial levels. Few studies in regard of costs and resource utilization have been published. The study of Shaughnessy et al. (Shaughnessy et al. 2011), compared retrospectively total costs between patients mobilized with G-CSF plus plerixafor with those mobilized with cyclophosphamide plus G-CSF. Their conclusion was that there was no difference in median total costs but mobilization was more predictable in the plerixafor plus G-CSF group. The use of plerixafor in pre-emptive settings has resulted in similar or lower total costs when compared to traditional mobilization methods (Li et al. 2011, Vishnu et al. 2012, Kymes et al. 2012, Perkins et al. 2012). However, all pharmacoeconomic studies of plerixafor are subject to a number of limitations, and this should be taken into consideration before making any final conclusions (Keating 2011). No pharmacoeconomic evaluations have been published from the European transplant centers.
2.5. CELLULAR COMPOSITION OF GRAFTS IN AUTOLOGOUS STEM CELL TRANSPLANTATION
2.5.1. Factors influencing graft cellular composition All mobilizing agents have a different and unique potential to mobilize stem cells. Due to the complexity of stem cell mobilization, the mobilization methods used may have a variable effect on the cellular composition of the graft (Talmadge et al. 1996, Webb et al. 1996, Cesana et al. 1998, Menéndez et al. 2002, Fruehauf et al. 2010, Jantunen and Fruehauf 2011). Mobilization therapy also mobilizes cell populations other than CD34+ cells and may have an impact on the maturity stage of mobilized CD34+ stem cells. The other cell populations may have importance in terms of engraftment and long-term outcome, and will be discussed in detail later. In addition to the mobilization therapy used, there may also be other factors influencing the graft cell composition (patient, disease and treatment-related factors). Effects of various mobilization methods on cellular composition of autografts are summarized in Table 2. Potential effects of graft characteristics in ASCT are presented in Table 3.

21
Table 2. Effect of mobilization regimen on autologous graft content (modified from Jantunen and Fruehauf 2011). Parameter G-CSF alone Chemotherapy
+ G-CSF Plerixafor + G-CSF
CD34+ More than G-CSF alone (Narayanasami et al. 2001)
More than G-CSF alone (DiPersio et al. 2009a, DiPersio
et al. 2009b)
CD34+ ���- More than chemotherapy + G-CSF (Möhle et al.
1994)
More than chemotherapy + G-CSF (Fruehauf et al. 2009)
Lymphocytes More than chemotherapy + G-CSF (Hiwase et al.
�����
More than G-CSF alone (Holtan et al. 2007)
CD3+, CD4+, ���+
More than G-CSF alone (Holtan et al. 2007)
Natural killer cells
More than G-CSF alone (Holtan et al. 2007)
Dendritic cells More than chemotherapy + G-CSF (Bolwell et al.
2003)
More than G-CSF alone (Gazitt et al. 2007)
2.5.2. CD34+ stem cells and subclasses The amount of CD34+ stem cells has been the most important characteristic of an autologous stem cell graft in the past, and it is still the only widely accepted indicator for graft quality in addition to engrafment after HDT (Jantunen and Fruehauf 2011). The CD34+ cell dose has been linked to engraftment and also outcome after ASCT. The CD34+ cell population can be divided into subclasses by their antigen properties. Cells of these different subclasses differ from each other in terms of their maturity stage, function and repopulating capacity (Terstappen et al. 1991, Huang et al. 1994, Waller et al. 1995, Larochelle et al. 1996, Beksac and Preffer 2012).
Higher infused CD34+ cell doses have been shown to result in faster neutrophil and platelet engraftment after HDT (Tricot et al. 1995, Weaver et al. 1995, Allan et al. 2002, Stiff et al. 2011). In addition, patients receiving higher CD34+ doses need fewer blood product transfusions and less supportive care (Ketterer et al. 1998, Schulman et al. 1999, Limat et al. 2000, Klaus et al. 2007, Stiff et al. 2011).
The relationship between CD34+ dose and outcome has been studied extensively. Most of the published studies have confirmed that larger CD34+ doses are associated with better PFS and OS after ASCT (Blystad et al. 2004, Pavone et al. 2006, O’Shea et al. 2006, Bolwell et al. 2007). However, not all studies have been able to confirm these observations (Stockerl-Goldstein et al. 2000, Wang et al. 2007). Reasons why the CD34+ dose and outcome may be linked are not known.
The minimum graft for a single autologous transplantation is usually considered to be at least 2.0 x 106 CD34+ cells/kg, which usually means CD34+ cell content measured after collection but before freezing. If a tandem (or double) transplantation is an option, then the minimum graft is usually at least 4.0 x 106 CD34+ cells/kg divided in two doses. Higher CD34+ doses (e.g. 4.0 – 8.0 x 106 CD34+ cells/kg for a single transplant and 8.0 – 10.0 x 106 CD34+ cells/kg for a tandem transplant) have also been suggested (Siena et al. 2000, Giralt et al. 2009). However, in regard to total costs of ASCT and the outcome after ASCT, the optimal CD34+ cell dose still remains to be defined.

22
Despite stem cell properties, most CD34+ cells have already been committed to a specific lineage (e.g. erythroid, lymphoid, or monomyeloid) (Andrews et al. 1989). In the study of Terstappen et al. (Terstappen et al. 1991) CD38 was the most promising marker indicating multilineage commitment of CD34+ bone marrow cells. In that study the amount of CD34+ cells lacking CD38 antigen (CD34+CD38-) was very low (only 1% of all CD34+ cells), and morphologic examination showed that these cells were a homogeneous population of primitive blasts. The ability to form colonies was inversely proportionate to CD38 antigen density. In addition, these primitive stem cells have been shown to have high self-renewal potential and to be progenitors of different cell types (i.e. lymphoid and myeloid) (Huang et al. 1994, Rusten et al. 1994, Miller et al. 1999). In ASCT recipients, the amount of infused CD34+CD38- cells has been shown to correlate with short-term engraftment but not with long-term hematopoietic reconstitution (Zubair et al. 2006). Yet, other studies have reported that some primitive CD34+ cell subtypes may also correlate with long-term engraftment (Hénon et al. 1998a, Hénon et al. 1998b, Lanza et al. 2001, Ninan et al. 2007). Primitive stem cells may also be more resistant to damage during cryopreservation (Ojeda-Uribe et al. 2004). Thrombopoietin has been shown to promote survival and stimulate growth of CD34+CD38- cells (Borge et al. 1997, Ramsfjell et al. 1997). CD110 is a receptor for thrombopoetin expressed in a subpopulation of CD34+ cells (Ramsfjell et al. 1997). The number of CD34+CD110+ cells in the graft has been linked with platelet engraftment (Sartor et al. 2007, Wallington-Beddoe et al. 2009).
Like the CD38 antigen, the CD133 antigen has also been linked with primitiveness of stem cells (Yin et al. 1997, Pasino et al. 2000, Hess et al. 2006). In a murine model, use of CD34+CD133+
cells has been shown to result in superior engraftment when compared to use of the CD34+CD133- cell population (de Wynter et al. 1998, Gordon et al. 2003). In MM patients, the higher number of transplanted CD34+CD133+ stem cells has been correlated with better neutrophil and platelet recovery after high-dose therapy (Hicks C et al. 2007, Camacho et al. 2012). Also the expression of CXCR4 on stem cells may have an impact on platelet recovery (Hicks et al. 2011).
The mobilization therapy has an effect on the amount and primitiveness of stem cells in the autologous stem cell grafts. Currently, perhaps the most efficient mobilization method in clinical use is chemotherapy + G-CSF combined with plerixafor (Dugan et al. 2010, Jantunen and Fruehauf 2011). The combination of G-CSF and plerixafor has been shown to mobilize more primitive stem cells than G-CSF alone in patients with MM or NHL (Fruehauf et al. 2009, Taubert et al. 2011). Mobilization with G-CSF alone has resulted in a higher number of more primitive stem cells (CD34+CD38-) when compared to chemotherapy + G-CSF mobilization (Möhle et al. 1994).
2.5.3. Lymphocytes All lymphocytes originate from the common lymphoid progenitors (CLP). There are at least four major types of lymphocytes: B cells, T cells, natural killer (NK) and NKT cells with features of both T cells and NK cells. Lymphocytes are a backbone of the humoral and cell-mediated immunity.
In the context of ASCT, lymphocytes in the graft have been primarily linked with engraftment and outcome. It has been shown that the amount of infused lymphocytes correlate with outcome after ASCT in NHL and MM patients (Porrata et al. 2004a, Porrata et al. 2004b, Katipamula et al. 2006). However, not all studies have been able to confirm this association (Percy et al. 2012). Lymphocyte engraftment has been faster after ASCT when more lymphocytes have been infused following HDT (Porrata et al. 2004b, Hiwase et al. 2008b). Furthermore, a faster lymphocyte recovery has been linked with superior outcome post-transplant (Yoong et al. 2005, Hiwase et al. 2008b). Relative proportions of infused lymphocyte subsets may also have an impact on the lymphocyte engraftment. Furthermore, lymphocyte subsets at the engraftment may predict early infectious complications after ASCT (Lee et al. 2012).

23
The lymphocyte count in stem cell grafts may be linked with mobilization therapy used. In the patients with NHL, the combination of plerixafor and G-CSF results in a higher amount of lymphocytes in the stem cell grafts than mobilization with G-CSF only (Holtan et al. 2007). On the other hand, mobilization with G-CSF alone has resulted in a higher amount of lymphocytes in the stem cell grafts than mobilization with chemotherapy plus G-CSF (Hiwase et al. 2008a).
2.5.3.1. T lymphocytes T cells (CD3+) are essential for the cell-mediated immunity. T cells can be divided into two main subclasses, CD4-positive helper T cells (CD3+CD4+), and CD8-positive cytotoxic T cells (CD3+CD8+). CD4- and CD8-positive T are divided further into smaller subclasses as naïve T cells, memory T cells, and regulatory T cells. Many different T cell populations are present in stem cell grafts (Condomines et al. 2006).
Higher numbers of CD4+ cells in the graft and an increased CD4/CD8 ratio have been shown to be associated with prolonged EFS after ASCT in MM patients (Schmidmaier et al. 2008). The corresponding phenomenon has been observed also with CD8+ cells (Atta et al. 2009). In addition, a lower ratio of CD4+ to CD8+ cells in the infused graft has been reported to be an independent risk-factor for severe mucositis in MM patients after HDT (Lee et al. 2012). On the other hand, a higher number of infused CD26+ T cells was associated with poorer outcome after ASCT (Hildebrandt et al. 2012). Infusing a higher number of CD4+ T cells may reduce the incidence of moderate and severe infections after ASCT (Menéndez et al. 2002).
2.5.3.2. Natural killer (NK) cells NK cells (CD3-CD16/56+) are cytotoxic lymphocytes that are a part of adaptive innate immunity. NK cells have been shown to be the first lymphocyte population that recovers after hematopoietic stem cell transplantation (Porrata and Markovic 2004). The amount of re-infused NK cells has been correlated with absolute lymphocyte count recovery after transplantation in patients with MM or NHL (Porrata et al. 2003). In addition, NHL patients with a higher amount of NK cells in the peripheral blood at day +15 after ASCT have had a better OS and PFS after transplantation in one study (Porrata et al. 2008).
2.5.3.3. B lymphocytes Johnsen et al. (Johnsen et al. 1998) have reported that potentially malignant CD19+ B-lymphocytes are mobilized during stem cell mobilization in patients with MM or NHL. In their study, more than 10% of the analyzed leukapheresis products contained at least than 5% CD19+ cells. Re-infused CD19+ may participate in immunological reconstitution after ASCT (Bomberger et al. 1998, Lee et al. 2012). Mobilization of CD19+ cells has also been confirmed in healty inviduals (Hassan et al. 1996).
2.5.4. Dendritic cells (DC) The main function of dendritic cells (DC) is to process antigens and present them to other immunologically active cells. Higher pre- and post-transplant levels of DCs have been correlated with better survival after ASCT in patients with DLBCL (Dean et al. 2005). Administration of GM-CSF combined with G-CSF may improve DC reconstitution after autologous stem cell transplantation when compared to patients treated with G-CSF alone (Eksioglu et al. 2011).
It has been reported that plerixafor may induce mobilization of precursor dendritic cells (pDC1) (type 1) and pDC2 (type 2) populations, but does not have an effect on the pDC1/pDC2 ratio (Gazitt et al. 2007).
2.5.5. Granulocytes Although the apheresis system is aimed to collect cells from the mononuclear fraction, also polymorphonuclear (PMN) cells are collected, and can be found in the leukapheresis product

24
(Menéndez et al. 2002, Pierelli et al. 2012). It is likely that most of these PMN cells with a short half-life lose their biological functions and vanish during cryopreservation (Price and Dale 1978, Reich-Slotky et al. 2008). However, some PMN cells may recover and be active after storage in the vapor or liquid phase of liquid nitrogen (Richman et al. 1983, Foïs et al. 2007). High levels of granulocytes in the stem grafts have been suspected to cause adverse events during re-infusion (Cordoba et al. 2007, Khera et al. 2012).
2.5.6. Tumor cells The role of tumor cells in stem cell grafts is controversial (DiPersio et al. 2011). Many studies have reported that the amount of tumor cells in the stem cell grafts do not have an influence on PFS or OS in patients with MM or NHL (Demirkazik et al. 2001, Blystad et al. 2004, Ho et al. 2009). However, controversial results have also been reported (López-Pérez et al. 2000, Vogel et al. 2005, Kopp et al. 2009). While it is possible that tumor cells in the stem cell graft could cause a relapse, it is more likely that relapse is due to an insufficient eradication of tumor cells in the patient (DiPersio et al. 2011). This concept is corroborated by the results from the studies investigating the impact of CD34+ cell selection from the stem cell grafts (Dreger et al. 1999, Stewart et al. 2001, Remes et al. 2003, Bourhis et al. 2007). There are no data from randomized studies suggesting that some form of positive or negative selection in order to reduce tumor cell contamination of grafts results in superior patient outcomes after HDT. Table 3. Graft characteristics of potential importance in autologous setting (modified from Jantunen and Fruehauf 2011). Parameter Reported impact
CD34+ cell dose Engraftment, outcome
CD34+ subclasses Engraftment
Lymphocyte subsets Immunological recovery, outcome
NK cells Immunological recovery, outcome
DCs Immunological recovery, outcome
Tumor cells Outcome
Other cell types Adverse effects at re-infusion

25
3 Aims of the Study
The aim of this retrospective study was to investigate the effects of the new stem cell mobilizing agent plerixafor in ASCT. The more specific study aims were:
To evaluate the kinetics of the white blood cell count and CD34+ cells after chemomobilization in poor and standard mobilizers to create an algorithm for pre-emptive use of plerixafor (I)
To explore the effects of plerixafor injection on CD34+ cell mobilization and WBC differential counts (II) To assess the effects of plerixafor injection on graft lymphocyte subsets and lymphocyte viability (III - V) To assess the effects of plerixafor injection on CD34+ cell subclasses and viability of CD34+ cells in the collected blood graft (IV, V) To investigate the effects of plerixafor on short and long-term engraftment and outcome after ASCT (III - VI)

26
4 Patients and Methods
4.1. PATIENTS
4.1.1. Kinetics of CD34+ cell mobilization and implications for pre-emptive plerixafor use (study I) A total of 390 first-time chemomobilized patients with hematological malignancies from Kuopio University Hospital mobilized between 1 January 2001 and 31 December 2010 were analyzed in the study. The main disease entities were NHL (181 patients, 46%), MM (152 patients, 39%), and HL (33 patients, 8%). Patients were grouped according to their CD34+ mobilization. Group A included patients with very poor mobilization (maximum B-CD34+ � *���!\�"6/L; n=29) and group B included patients with inadequate mobilization (maximum B-CD34+ count 6–10 x 106/L; n=14). Group C consisted of standard mobilizers (only patients who were mobilized from 1 August 2009 to 30 July 2010 and collected CD34+ ���� ? @ \ �"6/kg with a maximum of three aphereses without plerixafor were included) (n=33).
4.1.2. Characteristics of NHL patients (studies II-IV, VI)
4.1.2.1. Effects of plerixafor injection on blood white blood cell (WBC) composition and CD34+ cell mobilization (study II) In study II, 39 patients with NHL were mobilized with chemotherapy plus G-CSF between April 2009 and March 2011, and were admitted for stem cell apheresis to the hematological ward at Kuopio University Hospital (Table 4). Twenty of the patients also received plerixafor. The most common indication for plerixafor use was insufficient stem cell mobilization. All patients in the control grou� ���� *���=*��� � ������^ ��^ � ������^ �? @ \ �"6/kg CD34+ cells) by 1–2 apheresis without plerixafor. Twelve out of 20 (60%) plerixafor-treated patients were included in subsequent studies III and IV evaluating cellular composition of collected grafts.
4.1.2.2. Effects of plerixafor injection on the collected blood graft CD34+ cell subclasses, lymphocyte subsets and lymphocyte viability (studies III - IV) In study III, 24 patients with NHL were mobilized with chemotherapy plus G-CSF. Thirteen of these patients additionally received plerixafor (Table 4). The control group consisted of 11 NHL patients who received mobilization with chemotherapy plus G-CSF and in whom 2 x 106 to 6 x 106/kg CD34+ cells were collected with 1–2 apheresis procedures without plerixafor.
In study IV, 34 patients were included (Table 4). Nineteen patients (56%) received plerixafor pre-emptively after mobilization with chemotherapy plus G-CSF. The control group consisted of 15 patients with NHL who received chemomobilization and were successfully collected without plerixafor with 1–2 aphereses. All patients included in Study III were included also in the subsequent Study IV with some additional patients.

27
Table 4. Characteristics of NHL patients in studies II - IV. Study II, n=39 Study III, n=24 Study IV, n=34
Stem cell mobilization with plerixafor, n (%)
20 (51%) 13 (54%) 19 (56%)
Stem cell mobilization without plerixafor, n (%)
19 (49%) 11 (46%) 15 (44%)
Gender, n (%)
� Male ���� %) 17 (71%) 26 (76%)
� Female ���� �%) 7 (29%) ��� �%)
Age (years), median (range) ������– ��� 52 (31 – 66) 54 (29 – 66)
Histology, n (%)
� DLBCL ������� 12 (50%) 15 (44%)
� FL 9 (23%) 6 (25%) 9 (26%)
� MCL 9 (23%) 5 (21%) �������
� PTCL 6 (15%) 1 (4%) 4 (12%)
Mobilization, n (%)
� CY 6 (15%) ����� 2 (6%)
� DHAP 5 (13%) 6 (25%) 11 (32%)
� HD-AraC 24 (62%) �������� �������
� ICE ����� ����� 3 (9%)
� CHOP 1 (3%) - -
G-CSF used in mobilization, n (%)
� pegfilgrastim 25 (64%) 17 (71%) 25 (74%)
� filgrastim 14 (36%) 7 (29%) 9 (26%)
Abbreviations: DLBCL, diffuse large B-cell lymphoma; FL, follicular lymphoma; MCL, mantle cell lymphoma; PTCL, peripheral T-cell lymphoma; CY, cyclophosphamide; DHAP, dexamethasone, high-dose cytarabine, cisplatin; HD-AraC, high-dose cytarabine; ICE, ifosfamide, carboplatinum, etoposide; CHOP, cyclophosphamide, doxorubicin, vincristine, prednisolone.
4.1.2.3. Engraftment and outcome after ASCT (Study VI) Study VI included 89 consecutive NHL patients from Kuopio and Oulu University Hospitals who received ASCT between January 2009 and December 2011. All patients were initially mobilized with chemotherapy plus G-CSF. Thirty-three of these patients received also plerixafor. The rest of the patients (n=56, 63%) served as a control group. The median age of the patients was 57 years (range 26 – 71). The plerixafor group included more relapsed patients (52% vs. 32%, p=0.071) and more lymphomas with aggressive histology (DLBCL, PTCL, or Burkitt's lymphoma (BL)) (63% vs. 44%, p=0.083). The proportion of patients in CR at the time of stem cell mobilization was 58% (n=19) in the plerixafor group and 48% (n=27) in the control

28
group (p=0.393). High-dose cytarabine was the most commonly used mobilization therapy in both groups. Detailed patient and mobilization characteristics are presented in Table 5. Table �. Characteristics of NHL patients in study VI. Stem cell mobilization with
plerixafor, n=33 Stem cell mobilization
without plerixafor, n=56 Gender, n (%)
� Male 22 (67%) 43 (77%)
� Female 11 (33%) 13 (23%)
Age (years), median (range) ������– ��� 57 (26 – 71)
Histology, n (%)
� DLBCL* 15 (45%) 19 (34%)
� FL 7 (21%) �����%)
� MCL 3 (9%) 17 (30%)
� PTCL �����%) 12 (21%)
� Burkitt 2 (6%) -
Mobilization, n (%)
� CY 3 (9%) 4 (7%)
� DHAP ������� 11 (20%)
� HD-AraC 17 (52%) 26 (46%)
� ICE/IVAC/IVE/MINE �����%) 5 (10%)
� CHOP/CHOEP 1 (3%) 5 (9%)
� Bonn C 0 5 (9%)
G-CSF used in mobilization, n (%)
� pegfilgrastim ������%) 32 (57%)
� filgrastim 15 (46%) 24 (43%)
Abbreviations: DLBCL, diffuse large B-cell lymphoma; FL, follicular lymphoma; MCL, mantle cell lymphoma; PTCL, peripheral T-cell lymphoma; CY, cyclophosphamide; DHAP, dexamethasone, high-dose cytarabine, cisplatin; HD-AraC, high-dose cytarabine; ICE, ifosfamide, carboplatinum, etoposide; IVAC, ifosfamide, etoposide, high-dose cytarabine; IVE, ifosfamide, epirubicin, etoposide; MINE, mesna, ifosfamide, mitoxantrone, etoposide; CHOP, cyclophosphamide, doxorubicin, vincristine, prednisolone; CHOEP, cyclophosphamide, doxorubicin, etoposide, vincristine, prednisolone; Bonn C, high-dose cytarabine, vindesine, dexamethasone.
* including two patients with primary central nervous system lymphoma (PCNSL) in the plerixafor group and six patients in the control group
4.1.3. Characteristics of MM patients (study V) In study V, 21 MM patients were mobilized between April 2010 and March 2011 in Kuopio and Tampere University Hospitals. Seventeen patients (81%) were mobilized with CY 2 g/m2 plus

29
G-CSF. The rest of the patients (n=4, 19%) were mobilized with G-CSF. In addition, all G-CSF-mobilized patients and five chemomobilized patients (29%) received plerixafor. The control group included twelve patients who were mobilized with CY 2 g/m2 plus G-CSF, and at least 2.0 x 106 CD34+ cells/kg collected with 1–2 aphereses. Patient characteristics are presented in Table 6 and Study V, Table 1. Table 6. Characteristics of MM patients in study V. Stem cell mobilization with
plerixafor Stem cell mobilization without
plerixafor Number of patients, n 9 12
Gender, n (%)
� Male 5 (56%) 5 (42%)
� Female 4 (44%) �����%)
Age (years), median (range) 59 (53 – 67) 62 (42 – 70)
Chemomobilization, n (%) 5 (56%) 12 (100%)
Filgrastim used as G-CSF in mobilization, n (%)
4 (44%) 6 (50%)
Pegfilgrastim used as G-CSF in mobilization, n (%)
5 (56%) 6 (50%)
4.2. METHODS
4.2.1. Clinical methods
4.2.1.1. Mobilization of stem cells In NHL patients, the mobilization regimens consisted of disease-specific chemotherapy, usually high-dose cytarabine or intermediate-dose cyclophosphamide (4 g/m2). In MM patients, either low-dose cyclophosphamide (2 g/m2) or G-CSF alone was used. Either filgrastim or pegfilgrastim were used as a growth factor. In case of poor mobilization or low collection yield, the patients treated with pegfilgrastim received an extra dose of filgrastim followed by plerixafor injection. The most common plerixafor dose was 240 μg/kg. Detailed mobilization methods and growth factors used are presented in Tables 4-6.
4.2.1.2. Collection of stem cells Blood samples for measurements of blood WBC differential and CD34+ counts taken daily in the morning were started routinely when WBC count exceeded 0.5 x 109/L (1.0 x 109/L in Tampere University Hospital, study V). Measurements were continued until completion of aphereses or when the mobilization failure was observed.
Stem cell aphereses were started routinely if the morning B-CD34+ counts exceeded 20 x 106/L. However, in individual patients apheresis was started with rising B-CD34+ counts between 5-19 x 106/L, because it was anticipated that higher B-CD34+ counts were not to be expected due to stable or slowly increasing B-CD34+ counts. Collections were finished when the target yield had been reached or if collection failure was apparent. Collections were performed with a COBE Spectra AutoPBSCTM cell separator (Cobe BCT, Lakewood, CO). The blood volume

30
processed daily was 2.5 times by the patient’s estimated blood volume, and it took four to five hours.
In NHL patients, the minimum target of the CD34+ cells was 2 x 106/kg both in Oulu University Hospital and Kuopio University Hospital. In Study V (MM patients), the minimum target was 2 x 106/kg CD34+ cells for a single transplant in Kuopio University Hospital, and 4 x 106/kg �~�_����� �� � *�<��������� ����������!���� �^���� $�^��<�� ��� � = � �� transplants. In Tampere University Hospital the collection target was 4 x 106/kg CD34+ cells for a single transplant and 8-10 x 106/kg in patients with option for tandem transplants, respectively.
4.2.1.3. High-dose therapy In studies III and IV, all patients with NHL received as conditioning a BEAM regimen (carmustine 300 mg/m2 on d -6, etoposide 200 mg/m2 d -5 to d -2, cytarabine 300 mg/m2 d -5 to d -2 and melphalan 140 mg/m2 on day -2). BEAM was also the most common (n=56, 63%) high-dose regimen in study VI. Other regimens used for NHL patients in study VI included BEAC (carmustine 300 mg/m2 on d -7, etoposide 200 mg/m2 d -6 to d -3, cytarabine 400 mg/m2 d -6 to d -3, and cyclophosphamide 35 mg/kg d -6 to d -3) (n=19, 21%) or ibritumomab-tiuxetan with BEAC (Z-BEAC) (n=3, 3%). Patients with primary CNS lymphoma were treated with a combination of carmustine (400 mg/m2 on d -6) and thiotepa (10 mg/kg d -5 and d -4) (n=11, 12%). In all MM patients (study V), HDT consisted of high-dose melphalan (200 mg/m2) as a single dose. G-CSF was used after stem cell graft infusion in all NHL patients.
4.2.2. Laboratory methods
4.2.2.1. White blood cell differential counts WBC differential was measured by automated analysers, most commonly with an ADVIA 2120R hematology system (Siemens Healthcare Diagnostics, Deerfield, IL). If an automated analysis failed, differential was counted manually by using May-Grünwald-Giemsa staining and microscopic examination of the blood smears.
4.2.2.2. Enumeration of CD34+ cells in the blood and leukapheresis product The percentage of CD34+ cells, the CD34+ cell content of cryopreserved apheresis products and B-CD34+ counts were analyzed by flow cytometry. Most analyses were performed with a FACSCanto flow cytometer (Becton Dickinson, San Jose, CA), (Fig. 4), and Stem-Kit (Immunotech SAS/Beckman Coulter, Marseille, France) enumeration kit was used. In study V, samples of patients from Tampere University Hospital were analyzed with FACSCanto or FACSCalibur flow cytometers (Becton Dickinson, San Jose, CA), and a ProCount (Becton Dickinson, San Jose, CA) enumeration kit was used. In study VI, samples from patients in Oulu University Hospital were analyzed with FACSSort or FACSCalibur flow cytometers (Becton Dickinson, San Jose, CA), using a ProCount enumeration kit (Becton Dickinson, San Jose, CA). ISHAGE protocol for a single platform method was used. Gating was based on light scattering and immunophenotypic properties of the counted cells. The flow cytometer used and the gating strategy are shown in detail in Figs. 5 and 6.

31
Figure �. Becton Dickinson FACSCanto™ flow cytometer.

32
Figure 6. Gating strategy for B-CD34+ enumeration.
4.2.2.3. Laboratory processing and cryopreservation of the grafts Apheresis products were processed at the stem cell laboratory (the Laboratory of Eastern Finland, Kuopio, Finland). The grafts were not manipulated (e.g. purging or washing post-thaw). DMSO was added to the products to protect cells during the cryopreservation, using a final concentration of 10%. Graft samples (0.5 ml) were taken before cryopreservation, and these samples were handled in a similar way as the other apheresis products. These samples were originally intended for quality control, but were also used for research purposes in the present studies. The products were frozen in the liquid nitrogen freezer using a controlled rate-freezing program, and maintained in the vapor phase of the liquid nitrogen refrigerator until analyses. The median graft sample preservation times from the collection to the flow cytometric analysis are presented in the original publications (Studies III-V).

33
4.2.2.4. Flow cytometry of frozen grafts (studies III-V) The samples of the cryopreserved leukapheresis products were thawed in the Laboratory of Eastern Finland (Kuopio, Finland), in a +37°C water bath immediately before the flow cytometric analysis.
In Studies IV-V, the samples of cryopreserved leukapheresis products were stained for CD34+ subtyping with antibodies (Ab) according to standard procedures and analyzed with FACSCanto flow cytometry (Becton Dickinson, San Jose, CA). 7-AAD was used to exclude dead cells from the analysis. Ab’s against the following cell-surface markers were used (clone designations are given in parenthesis): CD34 (8G12), CD38 (HB7), CD133 (AC133), and CD45 (2D1). All antibodies were obtained from Becton Dickinson (Heidelberg, Germany), except for CD133 (Miltenyi Biotec GmbH, Bergisch Gladbach, Germany). The gating strategy for CD34+ subtyping is presented in Fig. 7.
Figure 7. Gating strategy for CD34+ cell subtyping.

34
BDMultitest CD3/CD8/CD45/CD4 and CD3/CD16+ CD56/CD45/CD19 reagents (Becton
Dickinson, Heidelberg, Germany) with BD Trucount tubes (Becton Dickinson, Heidelberg, Germany) were used with FACSCanto flow cytometry to determine the absolute numbers of T, B, and NK cells as well as the CD4 and CD8 subpopulations in the graft. The viability of lymphocytes was measured using 7-AAD staining.
Frozen samples of the first graft collected after plerixafor injection, and in the control group, of the first graft collected, were thawed and evaluated by flow cytometry. The exception was in study IV where in addition to the graft collected after plerixafor injection, also the first graft collected was evaluated in five patients.
The data of the CD34 measurements were analyzed using BD FACSDiva software and the data of the lymphocyte subsets using BD FACSCanto software (Becton Dickinson, San Jose, CA). The cell content of the graft was calculated by multiplying the concentration of each cell population with the graft volume and dividing that by patient weight (kg).
4.2.2.5. Colony forming unit-granulocyte/macrophage (CFU-GM) assay (studies III-V) The in vitro growth of CFU-GM was assessed routinely from all grafts after collection. A few days after freezing, the samples from cryopreserved leukapheresis products were thawed in +37°C water bath and suspended in IMDM with l-glutamine (Gibco, Paisley, UK). The cell suspension was dispensed into methylcellulose medium containing recombinant human cytokines (MethoCult H4434 Classic, StemCell Technologies, Vancouver, British Columbia, Canada). The methylcellulose medium was aliquoted into two Petri dishes, and the dishes were incubated in a humidified 37°C incubator with 5% CO2 for a total of 14 days and studied using an inverted microscope. CFU-GMs were enumerated in both dishes and the results were used to calculate the absolute number of CFU-GMs per patient weight (kg). The total number of incubated cells was not standardized. Therefore, the CFU-GM assay used should be considered as a qualitative test instead of being quantitative.
4.2.3. Quality assurance All participating transplantation centers (Kuopio University Hospital, Oulu University Hospital, and Tampere University Hospital) were supervised by the Finnish Medicines Agency (Fimea). The Laboratory of Eastern Finland conducted external quality assessment programs for the CD34 and lymphocyte subset measurements (both 6 times a year) organized by the United Kingdom National External Quality Assessment Service (UK NEQAS) and for the hematopoietic progenitor assays (two times a year) organized by Stemcell Technologies Inc. (Vancouver, Canada).
4.2.4. Data collection Clinical patient data were collected from hospital data systems using a specifically designed information retrieval form. All forms were blinded to enhance the protection of privacy.
4.2.5. Statistical methods In Study I, Fisher’s exact test was used as a statistical significance test. In addition, sensitivity, specificity, positive and negative predictive values were calculated. In other studies, the Mann-Whitney U test, Wilcoxon signed-rank test, Pearson's chi-squared test, Kaplan-Meier and Log-Rank test were used to analyze data. A two-tailed p value of less than 0.05 was considered statistically significant. All calculations and statistical analyses except for Fisher’s exact test were conducted using SPSS Statistics (version 19.0 in studies I and II and version 20.0 in other studies) for Windows (SPSS Inc., Somers, NY). Fisher’s exact test was calculated with GraphPad Prism (GraphPad Software Inc., La Jolla, CA).

35
4.3. APPROVALS
The study protocol was approved by the Ethical Committee of the Kuopio University Hospital and the National Supervisory Authority for Welfare and Health (Valvira). Permission for analysing the graft samples and collecting the follow-up data was also authorized by the Valvira.

36
5 Results
5.1. MOBILIZATION KINETICS OF CD34+ CELLS AND IMPLICATIONS FOR PRE-EMPTIVE PLERIXAFOR USE (STUDY I)
The incidence of poor mobilization was highest among patients with Waldenstrom's macroglobulinemia. However, the number of these patients was very low in this series. The risk of poor or inadequate mobilization was substantially higher in NHL patients than in patients with MM (17% vs. 1.3%, respectively, p < 0.001). Detailed data on the incidences of very poor or inadequate mobilization are presented in Table 7. Table 7. Incidence of poor or inadequate mobilization in different diseases (Study I).
Disease Group A, very poor mobilization (maximum B-CD34+�����106/L)
(n=29)
Group B, inadequate mobilization (maximum B-CD34+ 6–10×106/L)
(n=14) NHL (n=181) 20 (11%) 11 (6%)
MM (n=152) 1 (0.7%) 1 (0.7%)
HL (n=33) 2 (6%) 1 (3%)
CLL (n=15) 3 (20%) 0 (0%)
Waldenstrom's macroglobulinemia (n=6)
3 (50%) 1 (17%)
In the group of poorly mobilizing patients (group A, maximum B-CD34+ � *���!\�"6/L), the median WBC count at the time of highest CD34+ count measured was 8.1 x 109/L (range 1.9–21.6). The mobilization kinetics of these patients are presented in Fig 7. Due to poor stem cell � �������� ��� ������������<� *������$�^�����\�= �|����������������������<��=��?2 x 106/kg CD34+ cells) was not achieved. Apheresis was attempted only in one patient in group A. Two patients in group A were later remobilized and two proceeded to marrow collection, but only four patients (14% of patients in the group A) proceeded to ASCT.
In the group of inadequate mobilizers (group B, maximum B-CD34+ count measured 6-10 x 106/L), the median WBC count at the time of maximum CD34+ count was 11.0 x 109/L (range 3.2–��|!�|The kinetics of B-CD34+ cell counts in relation to WBC counts are presented in Fig. 7. No patient in group B received plerixafor. Apheresis was started in 13 patients (93%). The median number of collections was 2 (range 1–4) with a ��^��� � ��� � ������ � ����^ = �|! \ �"6/kg CD34+ cells (range 0.4–1.9). Nine patients (64%) proceeded to ASCT in this group.
The median number of aphereses was one �����<� *� =���^��^� ��������<� *���?@\106/kg CD34+ cells with maximum of three aphereses, plerixafor-treated patients excluded). In this group, the median stem cell yield was 2.9 x 106/kg CD34+ cells (range 2.4–12.3). The mobilization kinetics in this group is presented in Fig 7.
Based on the collected data and statistical tests, four algorithms based on B-CD34 counts were constructed. A�< ������������!\�"9/L and B-CD34+ ��"\�"6/L) was found to be the most suitable for separating patients who might benefit from plerixafor injections from those who mobilize sufficiently well without plerixafor. The algorithms are presented in Tables 8 and 9.
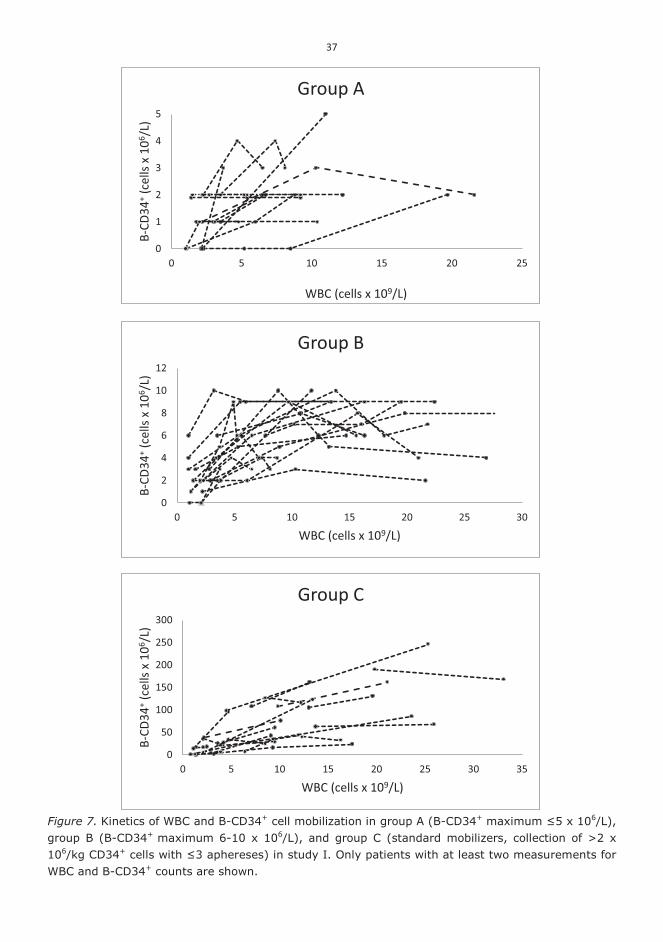
37
Figure 7. Kinetics of WBC and B-CD34+ cell mobilization in group A (B-CD34+ �������������106/L), group B (B-CD34+ maximum 6-10 x 106/L), and group C (standard mobilizers, collection of >2 x 106/kg CD34+ ��������������!��"����) in study I. Only patients with at least two measurements for WBC and B-CD34+ counts are shown.
0
1
2
3
4
5
0 5 10 15 20 25
B-CD
34+ (
cells
x 1
06 /L)
WBC (cells x 109/L)
Group A
0
2
4
6
8
10
12
0 5 10 15 20 25 30
B-CD
34+ (
cells
x 1
06 /L)
WBC (cells x 109/L)
Group B
0
50
100
150
200
250
300
0 5 10 15 20 25 30 35
B-CD
34+ (
cells
x 1
06 /L)
WBC (cells x 109/L)
Group C

38
Table 8. Summary of algorithms for pre-emptive plerixafor use.
Yes No Number of patients with
WBC counts and CD34+ counts not available
Algorithm I (WBC >5 x 109/L and B-CD34+ �������6/L)
Group A (n=29) 19 (66%) 0 (0%) 10 (34%)
Group B (n=14) 3 (21%) 11 (79%) 0 (0%)
Group C (n=33) 0 (0%) 28 (85%) 5 (15%)
Algorithm II (WBC >5 x 109/L and B-CD34+ ��������6/L)
Group A (n=29) 19 (66%) 0 (0%) 10 (34%)
Group B (n=14) 14 (100%) 0 (0%) 0 (0%)
Group C (n=33) 1 (3%) 27 (82%) 5 (15%)
Algorithm III (WBC >10 x 109/L and B-CD34+ �������6/L)
Group A (n=29) 9 (31%) 0 (0%) 20 (69%)
Group B (n=14) 0 (0%) 12 (86%) 2 (14%)
Group C (n=33) 0 (0%) 19 (58%) 14 (42%)
Algorithm IV (WBC >10 x 109/L and B-CD34+ ��������6/L)
Group A (n=29) 9 (31%) 0 (0%) 20 (69%)
Group B (n=14) 12 (86%) 0 (0%) 2 (14%)
Group C (n=33) 0 (0%) 19 (58%) 14 (42%)
Table 9. Summary statistics of algorithms for pre-emptive plerixafor use. Algorithm I Algorithm II Algorithm III Algorithm IV
Significance (Fisher’s exact test) p<0.001 p<0.001 p=0.001 p<0.001
Sensitivity 1.00 0.97 1.00 1.00
Specificity 0.72 1.00 0.61 1.00
Positive predictive value 0.67 1.00 0.43 1.00
Negative predictive value 1.00 0.96 1.00 1.00
5.2. EFFECTS OF PLERIXAFOR INJECTION ON BLOOD CD34+ CELL MOBILIZATION AND WBC COMPOSITION (STUDIES II, VI)
The first injection of plerixafor significantly increased WBC, neutrophil, lymphocyte, eosinophil, monocyte and mononuclear cell (MNC) counts when compared to the morning values preceding plerixafor injection. In study II, the median B-CD34+ count increased from 3 x 106/L (range <1 – 25) to 27 x 106/L (range <1 – 81) with a median 5-fold increase (range 1 – 17, p < 0.001). The B-CD34+ count in the morning of the first plerixafor dose (pre) and about 8 hours

39
after (post) in 20 NHL patients are shown in Fig 8. There were no significant differences in these parameters in plerixafor-treated patients who received either filgrastim or pegfilgrastim as a G-CSF. However, in study VI, the median fold-increase in the B-CD34+ count after the first plerixafor injection was 4.1 (range 1.2 – 19.0) among the filgrastim-treated patients and 7.2 (range 2.0 – 17.0) among the pegfilgrastim-treated patients (p=0.027).
In the control group, the median B-CD34+ count increased from 6 x 106/L (range 1 – 17) to 34 x 106/L (range 16 – 123) with a median 7-fold increase (range 1 – 25) from the day prior to the first apheresis to the morning value of the day of the first apheresis (p < 0.001).
Figure 8. B-CD34+ counts in the morning of the first plerixafor dose and 8 h after (study II).
WBC, neutrophil, lymphocyte, eosinophil, monocyte and MNC counts increased between the observed time points also in the control group patients. WBC counts were significantly higher in the plerixafor group than in the control group on the first collection morning, (21.5 vs. 9.1 x 109)/L, p < 0.001). In addition, the count of neutrophils (16.8 vs. 4.0 x 109/L, p < 0.001), lymphocytes (2.0 vs. 1.1 x 109/L, p=0.053), monocytes (1.3 vs. 0.6 x 109/L, p=0.001), eosinophils (0.4 vs. 0.1 x 109/L, p=0.061), and MNCs (3.2 vs. 1.8 x 109/L, p=0.01) was higher in the plerixafor group. The median B-CD34+ count was higher in the control group (34 vs. 27 x 106/L, p=0.043). Detailed data are presented in Tables 10 and 11.
0
10
20
30
40
50
60
70
80
90
pre post
B-C
D34
+ (ce
lls x
106 /L
)

40
Table 10. CD34+ and WBC counts and WBC differential in NHL patients before and after the first plerixafor dose. The data are presented as median (range). Morning prior to the first
plerixafor dose After the first plerixafor dose
(next morning) Significance
p WBC (x 109/L) 6.6 (2.1 – 35.2) 21.5 (5.2 – 73.2) <0.001
B-CD34+ (x 106/L) 3 (< 1 – 25) 27 (< 1 – 81) <0.001
Neutrophils (x 109/L) 5.3 (1.2 – 32.1) 16.8 (4.3 – 53.4) <0.001
Lymphocytes (x 109/L) 0.7 (0.1 – 2.8) 2.0 (0.5 – 5.9) <0.001
Monocytes (x 109/L) 0.5 (0.1 – 2.1) 1.3 (0.3 – 7.3) <0.001
Eosinophils (x 109/L) 0.1 (0.0 – 0.5) 0.4 (0.0 – 2.7) 0.001
MNC abs. (x 109/L) 1.5 (0.5 – 4.9) 3.2 (0.7 – 10.6) <0.001
Table 11. Comparison of CD34+ and WBC counts in NHL patients mobilized without plerixafor on the morning preceding the first apheresis and on the morning of the first apheresis. The data are presented as medians (range). Day prior to the
first apheresis In the morning of the day of
the first apheresis Significance
p WBC (x 109/L) 2.1 (0.7 – 6.4) 9.1 (1.5 – 15.8) <0.001
B-CD34+ (x 106/L) 6 (1 – 17)* 34 (16 – 123) <0.001
Neutrophils (x 109/L) 0.5 (0.0 – 2.7) 4.0 (0.5 – 13.2) <0.001
Lymphocytes (x 109/L) 0.7 (0.2 – 4.7) 1.1 (0.3 – 5.3) 0.002
Monocytes (x 109/L) 0.3 (0.0 – 1.0) 0.6 (0.1 – 1.6) 0.001
Eosinophils (x 109/L) 0.1 (0.0 – 0.6) 0.1 (0.0 – 0.6) 0.009
MNC abs. (x 109/L) 0.9 (0.4 – 5.7) 1.8 (0.7 – 6.5) <0.001
* data missing in two patients
The median yield after the first collection was 2.1 x 106/kg CD34+ cells (range 0.6 – 6.1) in the plerixafor group and 2.4 x 106/kg CD34+ cells (range 1.1 – 18.6) in the control group (p=0.123). In nine plerixafor-������^������� �_!��� ���������� � ������ � ���<�� �?@\�"6/kg CD34+ cells) was reached after the first plerixafor dose. For comparison, 74% of the control group patients reached the minimal collection target with a single apheresis. There were no significant differences in the median total stem cell yields between the groups (2.8 x 106/kg CD34+ cells vs. 3.4 x 106/kg CD34+ cells, p=0.122).
5.3. EFFECTS OF PLERIXAFOR INJECTION ON THE COLLECTED BLOOD GRAFT LYMPHOCYTE SUBSETS AND LYMPHOCYTE VIABILITY (STUDIES III - V)
The total amount of T lymphocytes (CD3+) was significantly higher in the grafts collected from NHL patients after pre-emptive plerixafor injection than in grafts from the control group patients (p=0.004 and p=0.002). In addition, the amount of helper T lymphocytes (CD3+CD4+), cytotoxic T lymphocytes (CD3+CD8+) and natural killer (NK) cells (CD3-CD16/56+) were all significantly higher after plerixafor injection (p=0.002 and p=0.001, p=0.006 and p=0.007, p=0.045

41
and p=0.019, respectively). In MM patients there were no significant differences in any of these cell populations when grafts collected from plerixafor-mobilized and control patients were compared (p=0.279 for the CY 2 g/m2 + G-CSF + plerixafor group vs. the control group; p=0.133 for the G-CSF + plerixafor group vs. the control group, and p=0.730 for the CY 2 g/m2 + G-CSF + plerixafor group vs. the G-CSF + plerixafor group). Detailed data are presented in Table 12 for NHL studies and Table 13 for the MM study.
The number of B lymphocytes (CD19+) was below the detection limit by flow cytometry in the vast of majority of grafts collected from NHL patients. Only small amounts of B lymphocytes were observed in some patients (0.03-0.1% of all lymphocytes in five plerixafor mobilized grafts and 0.03-0.08% of all lymphocytes in four grafts in the control group (p=0.971)). In MM patients, there was no significant difference in the amount of B lymphocytes in grafts from patients mobilized either with CY 2 g/m2 + G-CSF + plerixafor or CY 2 g/m2 + G-CSF (p=0.160). On the other hand, the number of B lymphocytes was significantly higher in grafts mobilized with G-CSF + plerixafor than in grafts mobilized with CY 2 g/m2 + G-CSF + plerixafor or CY 2 g/m2 + G-CSF (p=0.016 and p=0.013, respectively) (Table 13). Table 12. Summary of the lymphocyte subset analysis of freezed blood grafts in NHL patients (III - IV). The data are presented as medians (range). Study III Study IV
Chemotherapy +
G-CSF + plerixafor, n=13
Chemotherapy + G-CSF, n=13
Chemotherapy + G-CSF + plerixafor,
n=19
Chemotherapy + G-CSF,
n=15 CD3+ cell content (x 106/kg)
75.3 (14.6 – 327.3)* 21.3 (9.1 – 159.4)* 100.4 (14.6 – 327.3)* 25.0 (9.1 – 159.4)*
CD3+CD4+ cell content (x 106/kg)
32.7 (10.6 – � ��* 12.4 (6.9 – 51.5)* 50.9 (10.6 – � ��* 15.1 (7.0 – 54.9)*
CD3+���+ cell content (x 106/kg)
33.4 (4.2 – 200.5)* ���� �– 125.0)* 44.2 (4.2 – 233.0)* 10.7 (2.2 – 125.0)*
CD19+ cell content (x 106/kg)
0 (0 – 0) 0 (0 – 0) 0 (0 – 0) 0 (0 – 0)
NK (CD3-CD16/56+) cell content (x 106/kg)
5.1 (0.2 – 30.40)# 1.5 (0.3 – ���# ����� �– 30.4)# ������– 13.7)#
CD4+$���+ cell ratio �&����� – 3.04) ������ � – 5.06) 1.0 (0.3 – 3.0) 1.4 (0.3 – 5.1)
Significances (comparison made between the groups within the same study): * p=<0.01, # p=<0.05.

42
Table 13. Summary of the lymphocyte subset analysis of freezed blood grafts in MM patients (V). The data are presented as medians (range).
CY 2 g/m2 + G-CSF +
plerixafor, n=5
G-CSF + plerixafor, n=4
CY 2 g/m2 + G-CSF, n=12
CD3+ cell content (x 106/kg)
61.7 (16.9 – 197.2) � ��������– 333.9) 40.1 (6.4 – 90.7)
CD3+CD4+ cell content (x 106/kg)
51.9 (10.2 – 126.5) ������&�– 206.5) 26.6 (3.6 – ��&�
CD3+���+ cell content (x 106/kg)
10.2 (6.9 – ���� 73.0 (2.7 – 125.1) � ��� ��– 23.10)
CD19+ cell content (x 106/kg)
�������– 2.7)+ ����� ��– 56.0)* 0.5 (0.1 – 53.70)*,+
NK (CD3-CD16/56+) cell content (x 106/kg)
2.5 (1.1 – 17.6) 23.2 (2.7 – 27.6)* 3.3 (1.0 – ����*
CD4+$���+ cell ratio 2.6 (1.5 – 5.1) 1.3 (0.6 – 3.2) 2.0 (0.9 – 7.5)
Significances: * p=<0.05 (the G-CSF + plerixafor group compared to the CY 2 g/m2 + G-CSF group), + p=<0.05 (the CY 2 g/m2 + G-CSF + plerixafor group compared to the CY 2 g/m2 + G-CSF group).
The median proportion of nonviable lymphocytes was 10% (range 2 – 31%) in grafts collected from NHL patients after plerixafor injection and 14% (range 1 – 49%) in grafts collected from the control group patients (p=0.732). In MM patients, the median proportions were 19% (range 7 – 43%) after CY 2 g/m2 + G-CSF + plerixafor mobilization, 8% (range 2 – 20%) after G-CSF + plerixafor mobilization, and 17% (range 4 – 28%) after CY 2 g/m2 + G-CSF, respectively. There were no significant differences in these proportions between MM patient groups (p=0.506 for the CY 2 g/m2 + G-CSF + plerixafor group vs. the control group, p=0.262 for the G-CSF + plerixafor group vs. the control group, and p=0.190 for the CY 2 g/m2 + G-CSF + plerixafor group vs. the G-CSF + plerixafor group).
5.4. EFFECTS OF PLERIXAFOR INJECTION ON THE COLLECTED BLOOD GRAFT CD34+ CELL SUBCLASSES AND VIABILITY (STUDIES IV, V)
In NHL patients (IV), there were no significant differences in the median amounts of CD34+ cells when the control group and the plerixafor group were compared. The loss of viable CD34+ cells during cryopreservation was also equal between the groups (p=0.430). The detailed data are presented in Table 14.

43
Table 14. Summary of CD34+ amounts with different mobilization methods in NHL patients (study IV). The data are presented as medians (range). Chemotherapy + G-CSF +plerixafor,
n=19 Chemotherapy + G-CSF,
n=15 Original CD34+ cell content (x 106/kg)
2.7 (0.6 – 6.1) 2.0 (0.6 – 5.9)
CD34+ cell content after cryopreservation without 7-AAD (x 106/kg)
2.0 (0.5 – 6.0) �����6 – 5.1)
CD34+ cell content after cryopreservation with 7-AAD (x 106/kg)
1.7 (0.4 – 4.4) 1.7 (0.2 – 4.7)
Loss of viable CD34+ cells during cryopreservation (%)
22 (0 – 63) 17 (0 – ��)
In MM patients (V), the median amounts of CD34+ cells before, after cryopreservation without 7-AAD, and after cryopreservation with 7-AAD were significantly higher in the control group than in the group of patients mobilized with CY 2 g/m2 + G-CSF + plerixafor . There were no significant differences when the control group and the G-CSF + plerixafor group were compared. There were no significant differences between groups in the loss of viable CD34+ cells during cryopreservation either. The detailed data are presented in Table 15. Table ��. Summary of CD34+ amounts with different mobilization methods in MM patients (study V). The data are presented as medians (range). CY 2 g/m2 + G-CSF +
plerixafor, n=5 G-CSF + plerixafor,
n=4 CY 2 g/m2 + G-CSF,
n=12 Original CD34+ cell content (x 106/kg)
2.1 (0.3 – 2.7) 2.4 (1.2 – 5.0) 4.0 (1.2 – ���
CD34+ cell content after cryopreservation without 7-AAD (x 106/kg)
����� �– 2.1) �����&�– 4.7) 3.5 (1.0 – 7.4)
CD34+ cell content after cryopreservation with 7-AAD (x 106/kg)
1.6 (0.2 – 2.2) 1.4 (0.5 – �� &�����– 6.1)
Loss of viable CD34+ cells during cryopreservation (%)
24 (10 – 33) 43 (24 – 61) 30 (4 – 65)
In NHL patients, the median proportion of primitive stem cells (CD34+CD133+CD38-) from CD34+CD133+ cells and from all CD34+ cells were significantly higher in the group of plerixafor-treated patients (p=0.008 and p=0.009, respectively). The absolute amount of primitive stem cells was also significantly higher in the plerixafor group (p=0.003). A corresponding finding was also observed in MM patients as the median proportions of primitive stem cells from CD34+CD133+ cells and from all CD34+ cells were significantly higher in the group of plerixafor-treated patients (p=0.048 and p=0.020, p=0.048 and p=0.020, respectively). However, in MM patients, there were no significant differences between these groups in the absolute amount of primitive stem cells (p=0.574 for the CY 2 g/m2 + G-CSF + plerixafor group vs. the control group, p=0.212 for the G-CSF + plerixafor group vs. the control group, and p=0.413 for the CY 2 g/m2 + G-CSF + plerixafor group vs. the G-CSF + plerixafor group). The detailed data are presented in Table 16 and Table 17.

44
Table 16. Summary of CD34+ cell subclass analysis of cryopreserved blood grafts in NHL patients (study IV). The data are presented as medians (range).
Chemotherapy + G-CSF
+ plerixafor, n=19
Chemotherapy + G-CSF, n=15
Proportion of CD34+CD133+���- cells from CD34+CD133+ cells (%)
4.5 (1.4 – 13.4) 1.9 (0.0 – 7.7)
Proportion of CD34+CD133+���- cells from all CD34+ cells (%)
2.9 (1.0 – 11.6) 1.6 (0.0 – 5.9)
The most primitive stem cell (CD34+ CD133+���-) content in the graft (x 106/kg)
0.06 (0.01 – 0.34) 0.02 (0.00 – 0.12)
Table 17. Summary of CD34+ cell subclass analysis of cryopreserved blood grafts in MM patients (study V). The data are presented as medians (range).
CY 2 g/m2
+ G-CSF + plerixafor, n=5
G-CSF + plerixafor, n=4
CY 2 g/m2 + G-CSF, n=12
Proportion of CD34+CD133+���- cells from CD34+CD133+ cells (%)
3.6 (0.3 – 7.1) 4.7 (1.7 – ��� �������– 6.2)
Proportion of CD34+CD133+���- cells from all CD34+ cells (%)
���� �– 6.1) 3.5 (1.4 – 7.1) 0.6 (0.1 – 4.9)
The most primitive stem cell (CD34+ CD133+���-) content in the graft (x 106/kg)
0.02 (0.00 – 0.10) 0.05 (0.01 – 0.14) 0.02 (0.00 – �����
5.5. EFFECTS OF PLERIXAFOR MOBILIZED GRAFTS ON ENGRAFTMENT AFTER HIGH-DOSE THERAPY (STUDIES III - VI)
The median total collected CD34+ cell doses were compared in studies II-VI. There were no significant differences in the median amounts between the control group and the groups of plerixafor-treated patients. The detailed data are presented in Table 18. Table 18. Summary of total collected CD34+ cell dose (measured before freezing) in NHL patients who proceeded to ASCT. The data are presented as medians (range). Stem cell mobilization
with plerixafor Stem cell mobilization
without plerixafor Significance
p Study II (x 106/kg) 3.2 (2.1 – 6.5) 3.4 (2.0 – ���� ���&
Study III (x 106/kg) 3.1 (1.7 – 6.5) 3.4 (1.9 – 5.9) 0.563
Study IV (x 106/kg) 3.2 (1.7 – 6.5) 3.2 (1.9 – 5.9) 0.439
Study VI (x 106/kg) 3.5 (2.1 – �&� 4.2 (1.9 – ���� 0.076
Early engraftment after ASCT in NHL patients was assessed in studies III, IV and VI. In study III, the median time from the stem cell infusion to neutrophil engraftment (neutrophils > 0.5 x 109/L) was 10 days in both groups (range 9-17 days in the plerixafor group and 9-11 days in the control group) without any significant difference between the groups (p=0.092). In study IV,

45
the median time from graft infusion to neutrophil engraftment was also 10 days in both groups (ranges 9-17 days in the plerixafor group and 9-11 days in the control group) (p=0.773). Similar results were seen in study VI, in which the median engraftment time was also 10 days (ranges 8-81 days in the plerixafor group and 8-21 days in the control group) (p=0.899). In the study of MM patients (V), the median time for neutrophil engraftment was 12 days (range 9-13) in the plerixafor group and 10 days (range 9-13) days in the control group (p=0.291). Early neutrophil engraftment data from Study VI are presented in Fig 9.
Figure 9. Proportion of NHL patients with neutrophil engraftment (Study VI).
Platelet engraftment (unsupported platelets > 20 x 109/L) was seen on day +16 (median) in the
plerixafor group (range, 11-169 days) and on day +13 (range, 11-20 days) in the control group (p=0.211) in study III. In study IV, the time to platelet engraftment was 13 days in both groups (range 10–169 days in the plerixafor group and 11–18 days in the control group) (p=0.586), and in the study VI the median time was 14 days in both groups (range 10-165 days in the plerixafor group and 10-91 days in the control group) (p=0.083). Early platelet engraftment data from Study VI are presented in Fig 10. In MM patients (V), the time needed for platelet engraftment was 11 days in both groups (ranges 9-13 days and 10-15 days, respectively) (p=0.731).

46
Figure �. Proportion of NHL patients with platelet engraftment (Study VI).
Long-term engraftment in NHL patients was also investigated in studies III, IV and VI. In study III, lymphocyte and platelet counts were analyzed one, three and six months after ASCT. There were no significant differences between the groups in blood counts at specific time-points. In study IV, in addition to lymphocyte and platelet counts, also hemoglobin, leukocyte and neutrophil counts were analyzed, with prolonged follow-up up to twelve months after ASCT. The leukocyte count was statistically significantly higher in the plerixafor group at six months after ASCT (5.4 x 109/L vs. 4.5 x 109/L, p=0.047). There were no significant differences in other cell populations studied. Study VI had the same follow-up parameters (cell populations) as study IV. In study VI, the concentration of hemoglobin was significantly higher in the control group at three months after ASCT (121 g/L vs. 112 g/L, p=0.009). There were no significant differences in other cell populations in study VI. The proportion seemed higher in the control group three, six and twelve months after ASCT, but differences were not statistically significant. Data of blood counts at specific time points are presented in the original manuscripts (Studies III - IV).
5.6. OUTCOME AFTER ASCT IN NHL PATIENTS (STUDY VI)
Outcome after ASCT in NHL patients was evaluated in study VI. The median follow-up time was 677 days (range 5-1340 days) in the plerixafor group and 735 days (range 12-1338 days) in the control group (p=0.087).
The incidence of neutropenic fever (> 38 C, B-neutrophils < 0.5 x 109/L) was similar between the groups (76% in the plerixafor group vs. 71% in the control group, p=0.657). Bacteremia (most commonly staphylococci or enterococci) was observed in 28% of patients having

47
neutropenic fever in the plerixafor group and 23% in the control group, respectively (p=0.617). In the plerixafor group, six patients (16%) and in the control group seven patients (13%) had other infections (most commonly herpes zoster; 4 patient vs. 3 patients, respectively) during the follow-up after ASCT (p=0.464).
Ten patients (PTCL 4, DLBCL 3, FL 2, MCL 1) in the plerixafor group and thirteen patients (DLBCL 6, PTCL 3, MCL 3, and FL 1) in the control group experienced a relapse after ASCT. PFS at one year was 79% for the plerixafor group and 86 % for the control group (p=0.399). Two-year PFS was 70% and 83% (p=0.203), respectively. The median time from ASCT to a disease progression or relapse was 235 days (range 63-907 days) in the plerixafor group and 253 days (range 53-1102 days) in the control group (p=0.446). There was no significant difference between the groups in the incidence of relapse (30% vs. 23%, p=0.228).
Nineteen patients (ten patients from the plerixafor group and nine patients from the control group, p=0.114) died by the end of follow-up. OS at one year was 82% for the plerixafor group and 89% for the control group (p=0.319). Two-year OS was 71% and 85% (p=0.132) and three-year OS was 65% and 81% (p=0.114), respectively. The most common cause of death was progressive disease in both groups (seven patients from each group). In the plerixafor group, two patients died from septic shock a few days after stem cell infusion. These deaths were considered as early treatment-related mortality (TRM). One patient from the control group died from Influenza A virus (subtype H1N1) infection and acute respiratory distress syndrome. Two patients died from late non-relapse reasons (intracerebral hemorrhage and fatal abdominal bleeding after liver biopsy). Kaplan-Meier survival curves for PFS and OS are presented in are presented in Figs 11 and 12, respectively.
Figure 11. Cumulative progression-free survival of NHL patients (study VI).

48
Figure 12. Cumulative overall survival of NHL patients (study VI).

49
6 Discussion
The aim of this thesis was to investigate the effects of plerixafor in the ASCT setting. A significant proportion of patients mobilize inadequately, and the studies were started by analyzing the incidence of poor mobilization in different disease entities. In this study, an algorithm based on the mobilization kinetics of blood CD34+ cells in relation to WBC counts in chemomobilized patients was presented in an attempt to guide the use of plerixafor. Studies were thereafter continued by analyzing the effects of plerixafor injection on blood CD34+ cell counts and WBC differential counts. Stem cell subclasses and lymphocyte subsets from cryopreserved stem cell graft were analyzed in NHL and MM patients mobilized with and without plerixafor. In the last study, both short and long-term engraftment and outcome in plerixafor-mobilized NHL patients were evaluated.
6.1. PATIENTS AND METHODS
6.1.1. Patients All studies were retrospective and included only patients eligible for ASCT. The two main groups consisted of NHL patients and MM patients. These diseases are currently the main indications for ASCT (Passweg et al. 2013). Patients were gathered from a historical cohort of mobilizations and aphereses. Some patients had to be excluded from studies due to missing essential laboratory data or graft sample for flow cytometric analysis.
With the exception of study I, the patient groups were relatively small. The amount of patients included was primarily limited by the fact that there were no more patients available at the time of the study in the adult hematology unit at Kuopio University Hospital. To overcome this issue, in two studies (V, VI), patients from two other university hospitals, Tampere and Oulu University Hospitals, were also included to achieve larger patient groups. The number of patients in these studies is quite similar to previously published studies in this field (Fruehauf et al. 2009, Moreb et al. 2011, Alexander et al. 2011, Taubert et al. 2011). In addition to the limited number of patients, the results may be affected by large inter-individual variability of the measures and heterogeneity of the patients. These caveats may partly explain why statistically significant differences were not reached for some measures despite notable differences in absolute median values.
In studies II-VI, the patients were sorted into groups according to the use of plerixafor. Furthermore, in study V, the plerixafor group was divided into two separate groups by mobilization therapy (CY + G-CSF vs. G-CSF). There were no significant differences between the groups in regard to gender or age in any of the studies.
In studies II-IV and VI with NHL patients, the histology of the disease was evaluated. In many cases, the plerixafor group had more patients with aggressive histology. This is probably due to several factors. Patients with more aggressive diseases (e.g. DLBCL) are likely to receive more intensive treatment courses than patients with indolent diseases. The number of treatment courses may have an impact on the ability to mobilize stem cells.
6.1.2. Clinical methods In the studies included in this thesis, all but four MM patients in study V received chemomobilization. In NHL patients, the most commonly used mobilization regimen was disease-specific chemotherapy or high-dose cytarabine. The distribution of different chemomobilization regimens was similar between the groups. The type of disease-specific

50
chemotherapy was quite heterogeneous in study VI. This is at least in part due to the fact that there is no gold standard for chemomobilization regimen in NHL patients. This may cause some variability between the patients. It is likely that drugs or their combinations have an impact on the graft cellular composition, but not much is known about this. On the other hand, in MM patients, cyclophosphamide-based regimens are widely used for mobilization, but also other protocols have been applied (Wood et al. 2011).
If stem cell mobilization was insufficient or collection yields were low, patients were treated with plerixafor to boost stem cell mobilization. The vast majority of patients received plerixafor specifically due to poor stem cell mobilization. However, the definition for poor mobilization varies between transplant centers, and there is no widely accepted consensus on the definition (Piccirillo et al. 2012). Many transplant centers use B-CD34+ cell count >20 x 106/L as a threshold to start collection. In some cases, plerixafor was given when adequate mobilization did not occur within the typical time schedule. It is possible that in some of these patients mobilization would have been sufficient without plerixafor injection, but with a longer observation time. Some of these patients may have been late mobilizers instead of being ‘true’ poor mobilizers. Some patients were treated with plerixafor because of low and decreasing B-CD34 cell counts before the start or completion of apheresis. These patients can be considered poor mobilizers. The same is true for patients who had failed a previous mobilization attempt.
The high-dose regimen BEAM was used in all patients in studies III-IV and BEAC/BEAM in 88% of patients in study VI. In addition, all NHL patients received G-CSF after stem cell infusion. In MM patients, standard high-dose melphalan (200 mg/m2) was used in all patients.
6.1.3. Laboratory methods All procedures were standardized and quality control was involved in blood counts and CD34+ cell measurements. Analyses were performed with calibrated and highly validated equipment used in clinical practice. International guidelines (e.g. ISHAGE) were used when possible.
Samples of freezed grafts were used for the evaluation of cellular content in studies III-V. The reason was that these measurements most likely represent the post-thaw situation in clinical practice. The length of freezing time varied substantially due to the retrospective nature of this study. It is known that prolonged freezing may alter the amount and viability of cells (Liseth et al. 2009). However, the length of freezing time was similar between plerixafor-mobilized and control grafts. All flow cytometric analyses of freezed grafts were performed by the same qualified laboratory technician. To reduce variability, two graft samples (one from the control group and one from the plerixafor group) were always analyzed at the same time.
In studies III-V, only the first graft collected after plerixafor injection or the first graft collected from a single patient (control group) were evaluated with flow cytometry after thawing the sample. Therefore, direct comparisons between graft cellular content and engraftment are not possible. In study VI, only data from CD34+ cell dose before freezing was available.
6.1.4. Study methods All studies included in this thesis were retrospective. This research method has some inherent limitations. Retrospective study designs may also result in partly incomplete follow-up data.
Furthermore, it should be noted that as patients were sorted by the use of plerixafor, it may cause imbalance between the groups. Patients who were treated with plerixafor (poor or late mobilizers) may be intrinsically different from standard mobilizers. Many patient-related factors that may have an impact in stem cell mobilization have been identified, including age, diagnosis, prior treatments (e.g. chemotherapy load, certain drugs, and radiotherapy), pre-mobilization platelet count, bone marrow involvement and even gender (Drake et al. 1997, Micallef et al. 2000, Jantunen et al. 2003b, Kuittinen et al. 2004, Mendrone et al. 2008, Sancho et al. 2012). Because there was no randomization, it is possible that plerixafor-treated patients could have some or many of these risk factors for poor mobilization. In addition, risk factors for

51
poor mobilization may be also risk factors for poor outcome, and this should be taken into account when outcome after ASCT is evaluated.
6.2. KINETICS OF CD34+ CELL MOBILIZATION AND IMPLICATIONS FOR PRE-EMPTIVE PLERIXAFOR USE
Based on prior studies, 5-30% of patients considered for ASCT are hard to mobilize (Jantunen and Kuittinen 2008, Pusic et al. 2008, Jantunen and Kvalheim 2010, Wuchter et al. 2010). In study I, only 1.5% of myeloma patients belonged to the group of very poor mobilizers or inadequate mobilizers. Among NHL patients the proportion was as high as 17%. These figures are quite similar to the figures reported by others (Pusic et al. 2008, Wuchter et al. 2010, Sancho et al. 2012). It is possible that the proportion of very poor mobilizers might have been even higher in this series as some NHL patients who seemed to mobilize poorly were treated with plerixafor pre-emptively. In retrospect, it is difficult to determine how many of these patients would have been categorized as poor or inadequate mobilizers without plerixafor use.
Because plerixafor is expensive and it may be hard to identify beforehand patients who mobilize poorly and require plerixafor, clinical decision models are needed to optimize its use. Therefore, algorithms to help this identification have been developed, but none of the published algorithms (Table 1) have been accepted widely for clinical use (Costa et al. 2011, Chen et al. 2012, Sinha et al. 2011, Ozsan et al. 2012, Sancho et al. 2012, Abhyankar et al. 2012, Micallef et al. 2013, Milone et al. 2013, Abusin et al. 2013, Hay et al. 2013). In study I, based on the mobilization kinetics of CD34+ cells and WBC observed and decision algorithms applied, algorithms II and IV were found to be the most suitable. Algorithm II (WBC > 5 x 109/L and B-CD34+ ��"\�"6/L) appears to be even better in finding the really hard to mobilize patients than algorithm IV as it was more often applicable in this retrospective study. In real life, it is very possible that algorithm IV (WBC > 10 x 109/L and B-CD34+ ��"\�"6/L) might work as well as algorithm II.
As plerixafor results in a median 4- to 5-fold increase in B-CD34+ when given pre-emptively in poor mobilizers after chemomobilization (D'Addio et al. 2011, Jantunen and Lemoli 2012), it is possible to estimate how many patients might have benefited from plerixafor. Some patients in the group of very poor mobilizers (B-CD34+ � *���!\�"6/L) would have failed to mobilize enough stem cells even with the addition of plerixafor. On the other hand, the majority if not all patients in the group of inadequate mobilization (maximum B-CD34+ count 6–10 x 106/L) might have had successful collections with plerixafor.
All of tested algorithms in study I include a potential weakness as they do not take platelet counts into account. Platelet count is an important indicator for bone marrow recovery and the phase of stem cell mobilization (Ninan et al. 2007). Waiting for a few days might abolish the need for plerixafor use especially if the platelet counts are still low. It is also possible that some of the included patients were late mobilizers. Within this patient group, follow-up of WBC and B-CD34+ counts during mobilization should continue longer than normally. Although there are several suggested or even tested algorithms for pre-emptive plerixafor use in G-CSF mobilized patients (Costa et al. 2011, Chen et al. 2012, Sinha et al. 2011, Micallef et al. 2013), only a few algorithms for chemomobilized patients have been published (Ozsan et al. 2012, Sancho et al. 2012, Milone et al. 2013, Hay et al. 2013).
Results from study I confirmed that mobilization is difficult in a significant proportion of patients intended for ASCT. Poor mobilization is especially a problem among NHL patients. In addition, the mobilization kinetics in these patients is different from standard mobilizers. Pre-emptive plerixafor use based on constructed decision algorithms may prove to be cost-effective by reducing other costs associated with mobilization and collection of stem cells. These algorithms need a prospective validation.

52
6.3. CD34+ CELL MOBILIZATION AND PERIPHERAL BLOOD WBC COMPOSITION AFTER PLERIXAFOR INJECTION
In study II, plerixafor injection increased the blood CD34+ cells counts measured the next morning by a median of five-fold. This is in line with previous observations in the same setting (D'Addio et al. 2011, Jantunen and Lemoli 2012). In most cases, the mobilization boost induced �������\�= � ������� �����<��� *<�� �������������^���^��*���<��=� �?@\�"6/kg CD34+ cells) could be collected. Furthermore, an adequate graft could be collected in 85% of patients considered poor mobilizers. This kind of pre-emptive strategy seems to be useful as re-mobilization or prolonged aphereses can be avoided in the majority of these patients.
In study II, the WBC composition of peripheral blood at the time of apheresis also was assessed before and after plerixafor injection. The number of neutrophils was higher after plerixafor injection than in the control group on the morning of the first apheresis. One conceivable reason for this is that plerixafor was used in a later phase of mobilization in poor mobilizers. Higher neutrophil counts on the morning of apheresis may result in higher neutrophil counts also in the collection bag. This may also lead to a higher volume of DMSO to be infused to the patient (Tanhehco et al. 2010). Taken together, these factors may cause adverse effects during re-infusion of stem cell grafts (discussed earlier in Chapter 2.3.4.). In the present study, the median graft volumes after apheresis and after preservation were, however, similar between the groups.
Blood lymphocyte counts after the first plerixafor dose were higher than in the first collection day in the control group. This may imply that more lymphocytes will be collected after plerixafor injection. The great majority of lymphocytes are likely to be T lymphocytes as the vast majority of patients had previously received rituximab. Detailed lymphocyte characterization was not performed in study II due its retrospective nature.
Results from study II suggests that plerixafor use is associated with an increase of many leukocyte subtypes other than just CD34+ cells. Whether this is due to more complex mechanisms of action of plerixafor or due to ongoing mobilization caused by previous chemotherapy plus G-CSF is unknown. As the number of eosinophils, lymphocytes and monocytes increased also in the control group, part of the effect is likely to be associated with chemomobilization effect as such. It is known that many other hematopoietic cells besides CD34+ stem cells express CXCR4 (Aiuti et al. 1999). Thus, it is possible that these cells are also mobilized by plerixafor.
6.4. LYMPHOCYTE SUBSETS OF THE FROZEN GRAFTS
Previous studies have reported that plerixafor alone or combined with G-CSF may increase various lymphocyte subsets in the graft (Holtan et al. 2007, Gaugler et al. 2011). In the context of ASCT, lymphocytes in the graft have been primarily linked with more rapid immune recovery and better outcome as discussed earlier in Chapter 2.5.3. Of note, there have been no previous studies on the effects of plerixafor on lymphocyte subsets in chemomobilized patients where mobilizing chemotherapy may kill lymphocytes.
In studies of NHL patients (III, IV), plerixafor added to chemomobilization seemed to result in significantly higher amounts of NK cells, total T cells, helper T cell subsets and cytotoxic T cell subsets in the grafts compared to the control grafts. In addition, plerixafor appears to increase the mobilization of T cell subsets and NK cells independently of CD34+ cell mobilization as the number of CD34+ cells was similar between the groups. CD19+ B lymphocytes were detected in very low numbers only in a few samples. An apparent reason for this observation is that the vast majority of patients had received rituximab as a part of their mobilizing chemotherapy.

53
In MM patients (study V), the number of NK cells was higher in the grafts collected after G-CSF + plerixafor than in the grafts collected from chemomobilized patients with or without plerixafor. This is in line with a study by Holtan et al. (Holtan et al. 2007), where G-CSF + plerixafor resulted in higher number of certain lymphocyte subsets (CD3+, CD4+, CD8+) in NHL patients. In addition, a higher total number of lymphocytes were collected after G-CSF plus plerixafor than after mobilization with G-CSF alone (Holtan et al. 2007). Moreover, the amount of B lymphocytes was higher in the grafts collected after G-CSF plus plerixafor in MM patients when compared to the control group (cyclophosphamide + G-CSF) and group A (cyclophosphamide + G-CSF + plerixafor). The most obvious explanation for the higher number of B lymphocytes in MM patients mobilized with G-CSF + plerixafor (study V) is that the cyclophosphamide used in the other groups for mobilization purposes destroys lymphocytes. The broad ranges observed in the amounts of various lymphoid subsets suggest that also factors other than the use of plerixafor may be important in terms of mobilization of lymphoid cell subsets.
As the amount of lymphoid cells in the cryopreserved grafts is about ten times higher than CD34+ cell counts and the majority of them are viable after thawing, they may have an impact in tempo and type of immune recovery after HDT. The higher number of these cells in the graft may be beneficial in terms of speed of immune recovery and outcome after ASCT (Porrata et al. 2003, Porrata et al. 2004a, Porrata et al. 2004b. Hiwase et al. 2008b, Atta et al. 2009). However, the amount and function of NK cells in the graft has been stated to be insignificant, because they recover quickly post-transplant (Klingemann 2000). In this retrospective series of studies, evaluation of immunorecovery after ASCT was not possible. The clinical relevance of different lymphocyte subsets in the cryopreserved grafts remains to be elucidated. This topic will be specifically evaluated in the prospective GOA (Graft and Outcome in Autologous stem cell transplantation) study, which includes assessment of the graft cellular composition and immune reconstitution post-transplant (Jantunen et al. 2013b).
This new data may have clinical relevance because a large proportion of NHL and MM patients are currently mobilized with a combination of chemotherapy plus G-CSF. However, prospective study designs with larger patient numbers and with a longer follow up are needed to evaluate whether the amount of various lymphocyte subsets in the grafts affects post-transplant outcomes like severe infections or a relapse.
6.5. CD34+ SUBCLASSES OF THE FROZEN GRAFTS
It has been reported that plerixafor combined with G-CSF may mobilize more primitive CD34+CD38- stem cells in MM patients (Fruehauf et al. 2009, Taubert et al. 2011). As discussed earlier in Chapter 2.5.2., these primitive stem cells have been shown to have a high self-renewal potential and the amount of infused CD34+CD38- cells may correlate with engraftment after ASCT.
In NHL patients (study IV), plerixafor significantly increased both the proportion and the number of the most primitive stem cells (CD34+CD133+CD38-) in the stem cell graft in poorly mobilizing NHL patients treated with chemomobilization when compared to control group patients. This result corroborates the findings from a prior study by Fruehauf et al. (Fruehauf et al. 2009) in patients mobilized without chemotherapy. In patients with MM (study V) the results were similar as the proportion of the most primitive cells was significantly higher in plerixafor-treated patients than in the control group. In MM patients, the absolute number of the most primitive cells did not differ between the groups. This was possibly due to the small number of patients, because the median proportions of primitive stem cells were significantly higher in plerixafor-treated patients. The results in study V are also in line with previously published results in MM patients mobilized without chemotherapy (Fruehauf et al. 2009, Taubert et al. 2011). Taken together, these observations suggest that plerixafor may increase mobilization of

54
more primitive CD34+ cell subclasses both in NHL and MM patients, regardless of whether it is combined with G-CSF or with chemomobilization. However, short and long-term engraftment was similar between the groups in both studies after ASCT. Furthermore, the possible relationship between graft composition and engraftment cannot be fully assessed as only the first graft was analyzed in detail even though many patients received grafts collected with two or even three aphereses.
The clinical relevance of the most primitive stem cells is at present unclear. Further studies are needed regarding the importance of more primitive stem cells in ASCT (Zubair et al. 2006).
6.6. VIABILITY OF GRAFT CELLS
7-AAD staining was used to evaluate the number of dead cells by flow cytometry. There were no significant differences in the amount of either dead CD34+ cells or lymphoid cells after freezing between the different mobilization groups among NHL or MM patients. In MM patients the proportion of dead lymphoid cells was higher in cyclophosphamide-treated patients, but perhaps due to the low numbers and high variability, no statistical significance was observed. These observations suggest that plerixafor-mobilized grafts have viability characteristics similar to G-CSF or chemomobilized grafts if freezing times range from a few months to about a year.
Taking into account the relatively wide use of plerixafor in stem cell mobilization for ASCT, more refined characterization of CD34+ cells, including gene-expression profiling (Fruehauf et al. 2006, Donahue et al. 2009) and functional assays of various lymphocyte subsets (Schwartzberg et al. 2009), are also warranted.
6.7. ENGRAFTMENT AND OUTCOME AFTER ASCT
Plerixafor added to G-CSF resulted in superior mobilization of CD34+ cells compared to G-CSF alone in randomized studies and was associated with equal engraftment and outcome at one year post-transplant (DiPersio et al. 2009a, DiPersio et al. 2009b). In poor mobilizers the effects of plerixafor on long-term outcomes are less well established, and only small patient series have been published (Moreb el al. 2011, Alexander et al. 2011). Specifically, there are no published data available about long-term outcome after ASCT in poorly mobilizing NHL patients treated with chemomobilization plus plerixafor.
The number of patients included in study VI (n=89) was larger than in any previous study investigating engraftment and long-term outcome after ASCT in NHL patients treated with chemomobilization and plerixafor. The patient groups were heterogeneous in terms of histology (patients in the plerixafor group more commonly had aggressive histology) and disease status at transplant (the plerixafor group included more relapsed patients). Therefore, it is likely that many patients in the plerixafor group had poorer long-term prognosis than patients in the control group.
In study VI, the collected CD34+ cell dose was, not unexpectedly, higher in the control group than in the study group, which consisted of poor mobilizers. Yet, hematopoietic recovery was similar between the groups during the first year after ASCT. Infectious complications post-transplant were also similar between the groups. Higher numbers of CD34+ cells in the graft have been linked with more rapid hematopoietic recovery and with better survival after ASCT in some studies as discussed earlier in Chapter 2.5.2. These observations in study VI may indicate that also factors other than solely CD34+ cell dose influence hematopoietic and immune recovery post-transplant. It is possible that these mobilization-related changes (e.g. changes in the cell composition of the graft) may explain similar outcomes between the groups. Absolute

55
lymphocyte count (ALC) on day +15, which has been found to be important for progression-free and overall survival in some retrospective studies (Porrata et al. 2001, Gordan et al. 2003), was not assessed in study VI. Taken together, these observations suggest that the quality of grafts collected with plerixafor is at least equal to the grafts collected without it, although prospective studies are needed to assess e.g. the tempo of immunorecovery after ASCT. As previously mentioned, this will be an important topic of the ongoing GOA study (Jantunen et al. 2013b).
Another interesting issue in regard to the use of plerixafor for stem cell mobilization is the question of possible tumor cell mobilization. Previous studies have not observed higher tumor cell mobilization in patients mobilized with G-CSF plus plerixafor (DiPersio et al. 2009, Fruehauf et al. 2010). When patients are treated with cytotoxic chemomobilization, tumor cell contamination has been reported to be similar when compared to G-CSF based mobilization (López-Pérez et al. 2000, Narayanasami et al. 2001). Possible contamination was not measured in any of the studies included in this thesis, but no increase in the risk of relapse was observed in plerixafor-treated patients, suggesting no excessive mobilization of tumor cells.
The main conclusion from study VI was that the use of plerixafor to enhance blood stem cell mobilization in NHL patients appears to be associated with similar early and long-term engraftment as well as equal post-transplant outcomes. However, due to the retrospective nature, these preliminary observations must be confirmed in a prospective study setting.

56
7 Conclusions
The main findings and conclusions of this series of studies were: I A significant proportion of NHL patients were found to be hard to mobilize with
chemomobilization. The mobilization kinectics of these patients differ from standard mobilizers. An algorithm to optimize plerixafor use was developed to be prospectively validated.
II Plerixafor combined to chemomobilization enhanced the yield of CD34+ cells in
poorly mobilizing NHL patients. In addition, plerixafor increased the amount of leukocytes, neutrophils, lymphocytes, eosinophils and monocytes in the peripheral blood at the time of apheresis.
III Plerixafor combined with chemomobilization in poorly mobilizing NHL patients
seems to mobilize more T cells, helper T subsets, suppressor T subsets, and NK cells than chemomobilization alone. Use of plerixafor results in similar engraftment and outcome after ASCT compared to standard mobilizers.
IV Plerixafor added to chemomobilization in poorly mobilizing NHL patients
mobilizes more primitive CD34+ cells than chemomobilization alone. V Plerixafor combined with chemomobilization or G-CSF in poorly mobilizing MM
patients increases the proportion of more primitive stem cells in the grafts. In addition, plerixafor may increase the amount of certain lymphocyte populations in stem cell grafts.
VI Plerixafor combined with chemomobilization in poorly mobilizing patients with
NHL results in rapid and long-term engraftment, and the outcome after ASCT is similar to standard mobilizers.

57
8 Future Perspectives
At the moment, the major factor limiting the use of plerixafor for stem cell mobilization in autologous transplantation is its substantially higher price. Therefore, more sophisticated methods are needed to optimize the use of plerixafor in clinical practice and, on the other hand, to recognize patients who do not benefit from it. These aspects should be assessed in prospective studies with larger patient numbers. As the most effective combination for mobilizing stem cells is probably chemomobilization combined with plerixafor and many transplant centers still mobilize patients with chemomobilization, more data and algorithms to guide plerixafor use are warranted. Future studies should also include cost-benefit analysis that covers the costs of the entire mobilization and collection process. Furthermore, uniform and internationally accepted definitions for poor and inadequate mobilization should be created and put into practice.
To evaluate the potential clinical impact of graft cellular content on patient outcomes including late post-transplant complications and risk of relapse, larger prospective studies and longer follow-up are needed. The effects of plerixafor on the cellular content of the graft should be evaluated in larger patient series and compared with traditional mobilization regimens. The possible link between graft cellular content, speed and tempo of engraftment including immune recovery post-ASCT and long-term outcome should also be studied. Some of these aspects will be studied in the ongoing GOA study in Finland (Jantunen et al. 2013b) and in the prospective phase II study of the Finnish Myeloma Group (FMG-MM02). In addition, gene expression profiling (Fruehauf et al. 2006, Donahue et al. 2009), more detailed phenotypic and functional studies of CD34+ cells as well as various functional aspects of lymphocyte activation (e.g. signaling lymphocyte activation molecules) (Schwartzberg et al. 2009) are needed. Also the possible mobilization of tumor cells and its clinical impact should be assessed.
Because there will be patients intended for ASCT who fail mobilization even with plerixafor, new mobilizing agents are needed. Some molecules (e.g. POL6326) have entered early phase clinical trials (Rettig et al. 2012). As some of them will become commercially available, different mobilization methods should be compared in regard to safety, efficacy, graft composition, and possible impact on short- and long-term outcomes post-transplant.
The first reports of chemosensitization with plerixafor in patients with acute leukemia have been published (Nervi et al. 2009, Uy et al. 2012). It remains to be seen whether this will be possible in MM or NHL patients. This would be especially interesting in patients with primarily refractory diseases or in patients with a high risk of the relapse. Promising preliminary studies in this topic have been published (Azab et al. 2009). Similar observations with solid tumors have also been reported (Domanska et al. 2012, Heckmann et al. 2013). However, more studies are urgently needed to assess the clinical utility of this treatment modality.

58
9 References
Abbruzzese L, Agostini F, Durante C, Toffola RT, Rupolo M, Rossi FM, Lleshi A, Zanolin S, Michieli M, Mazzucato M. Long term cryopreservation in 5% DMSO maintains unchanged CD34(+) cells viability and allows satisfactory hematological engraftment after peripheral blood stem cell transplantation. Vox Sang. 2013;105:77-80. Abhyankar S, DeJarnette S, Aljitawi O, Ganguly S, Merkel D, McGuirk J. A risk-based approach to optimize autologous hematopoietic stem cell (HSC) collection with the use of plerixafor. Bone Marrow Transplant. 2012;47:483-7. Abraham M, Biyder K, Begin M, Wald H, Weiss ID, Galun E, Nagler A, Peled A. Enhanced unique pattern of hematopoietic cell mobilization induced by the CXCR4 antagonist 4F-benzoyl-TN14003. Stem Cells. 2007;25:2158-66. Abrahamsen JF, Bakken AM, Bruserud Ø, Gjertsen BT. Flow cytometric measurement of apoptosis and necrosis in cryopreserved PBPC concentrates from patients with malignant diseases. Bone Marrow Transplant. 2002a;29:165-71. Abrahamsen JF, Bakken AM, Bruserud Ø. Cryopreserving human peripheral blood progenitor cells with 5-percent rather than 10-percent DMSO results in less apoptosis and necrosis in CD34+ cells. Transfusion. 2002b;42:1573-80. Abrahamsen JF, Stamnesfet S, Liseth K, Hervig T, Bruserud Ø. Large-volume leukapheresis yields more viable CD34+ cells and colony-forming units than normal-volume leukapheresis, especially in patients who mobilize low numbers of CD34+ cells. Transfusion. 2005;45:248-53. Abusin GA, Abu-Arja RF, Gingrich RD, Silverman MD, Zamba GK, Schlueter AJ. An algorithm for utilizing peripheral blood CD34 count as a predictor of the need for plerixafor in autologous stem cell mobilization-cost-effectiveness analysis. J Clin Apher. 2013;28:293-300. Aiuti A, Tavian M, Cipponi A, Ficara F, Zappone E, Hoxie J, Peault B, Bordignon C. Expression of CXCR4, the receptor for stromal cell-derived factor-1 on fetal and adult human lympho-hematopoietic progenitors. Eur J Immunol. 1999;29:1823-31. Akkök CA, Liseth K, Hervig T, Ryningen A, Bruserud Ø, Ersvaer E. Use of different DMSO concentrations for cryopreservation of autologous peripheral blood stem cell grafts does not have any major impact on levels of leukocyte- and platelet-derived soluble mediators. Cytotherapy. 2009;11:749-60. Alencar S, Garnica M, Luiz RR, Nogueira CM, Borojevic R, Maiolino A, Dutra HS. Cryopreservation of peripheral blood stem cell: the influence of cell concentration on cellular and hematopoietic recovery. Transfusion. 2010;50:2402-12.

59
Alexander ET, Towery JA, Miller AN, Kramer C, Hogan KR, Squires JE, Stuart RK, Costa LJ. Beyond CD34+ cell dose: impact of method of peripheral blood hematopoietic stem cell mobilization (granulocyte-colony-stimulating factor [G-CSF], G-CSF plus plerixafor, or cyclophosphamide G-CSF/granulocyte-macrophage [GM]-CSF) on number of colony-forming unit-GM, engraftment, and Day +100 hematopoietic graft function. Transfusion. 2011;51:1995-2000. Allan DS, Keeney M, Howson-Jan K, Popma J, Weir K, Bhatia M, Sutherland DR, Chin-Yee IH. Number of viable CD34(+) cells reinfused predicts engraftment in autologous hematopoietic stem cell transplantation. Bone Marrow Transplant. 2002;29:967-72. Anderlini P, Przepiorka D, Seong D, Miller P, Sundberg J, Lichtiger B, Norfleet F, Chan KW, Champlin R, Körbling M. Clinical toxicity and laboratory effects of granulocyte-colony-stimulating factor (filgrastim) mobilization and blood stem cell apheresis from normal donors, and analysis of charges for the procedures. Transfusion. 1996;36:590-5. Andreola G, Babic A, Rabascio C, Negri M, Martinelli G, Laszlo D. Plerixafor and filgrastim XM02 (Tevagastrim) as a first line peripheral blood stem cell mobilisation strategy in patients with multiple myeloma and lymphoma candidated to autologous bone marrow transplantation. Eur J Haematol. 2012;88:154-8. Andrews RG, Singer JW, Bernstein ID. Precursors of colony-forming cells in humans can be distinguished from colony-forming cells by expression of the CD33 and CD34 antigens and light scatter properties. J Exp Med. 1989;169:1721-31. Ansell SM. Hodgkin lymphoma: 2012 update on diagnosis, risk-stratification, and management. Am J Hematol. 2012;87:1096-103. Appelbaum FR. Hematopoietic cell transplantation for non-Hodgkin's lymphoma: yesterday, today, and tomorrow. J Clin Oncol. 2008;26:2927-9. Armitage S, Hargreaves R, Samson D, Brennan M, Kanfer E, Navarrete C. CD34 counts to predict the adequate collection of peripheral blood progenitor cells. Bone Marrow Transplant. 1997;20:587-91. Atta EH, de Azevedo AM, Maiolino A, Coelho CJ, Sarcinelli SM, de Alvarenga Máximo C, Marra VL. High CD8+ lymphocyte dose in the autograft predicts early absolute lymphocyte count recovery after peripheral hematopoietic stem cell transplantation. Am J Hematol. 2009;84:21-8. Attal M, Harousseau JL, Stoppa AM, Sotto JJ, Fuzibet JG, Rossi JF, Casassus P, Maisonneuve H, Facon T, Ifrah N, Payen C, Bataille R. A prospective randomized trial of autologous bone marrow transplantation and chemotherapy in multiple myeloma. Intergroupe Francais du Myelome. N Engl J Med. 1996;335:91-7. Auquier P, Macquart-Moulin G, Moatti JP, Blache JL, Novakovitch G, Blaise D, Faucher C, Viens P, Maraninchi D. Comparison of anxiety, pain and discomfort in two procedures of hematopoietic stem cell collection: leukacytapheresis and bone marrow harvest. Bone Marrow Transplant. 1995;16:541-7.

60
Awan FT, Kochuparambil ST, Deremer D, Cumpston A, Craig M, Jillella A, Hamadani M. Plerixafor salvage is safe and effective in hard-to-mobilize patients undergoing chemotherapy and filgrastim-based peripheral blood progenitor cell mobilization. J Oncol. 2012;2012:931071. Azab AK, Runnels JM, Pitsillides C, Moreau AS, Azab F, Leleu X, Jia X, Wright R, Ospina B, Carlson AL, Alt C, Burwick N, Roccaro AM, Ngo HT, Farag M, Melhem MR, Sacco A, Munshi NC, Hideshima T, Rollins BJ, Anderson KC, Kung AL, Lin CP, Ghobrial IM. CXCR4 inhibitor AMD3100 disrupts the interaction of multiple myeloma cells with the bone marrow microenvironment and enhances their sensitivity to therapy. Blood. 2009;113:4341-51. Baldomero H, Gratwohl M, Gratwohl A, Tichelli A, Niederwieser D, Madrigal A, Frauendorfer K; European Group for Blood and Marrow Transplantation EBMT. The EBMT activity survey 2009: trends over the past 5 years. Bone Marrow Transplant. 2011;46:485-501. Barlogie B, Kyle RA, Anderson KC, Greipp PR, Lazarus HM, Hurd DD, McCoy J, Moore DF Jr, Dakhil SR, Lanier KS, Chapman RA, Cromer JN, Salmon SE, Durie B, Crowley JC. Standard chemotherapy compared with high-dose chemoradiotherapy for multiple myeloma: final results of phase III US Intergroup Trial S9321. J Clin Oncol. 2006;24:929-36. Basak GW, Knopinska-Posluszny W, Matuszak M, Kisiel E, Hawrylecka D, Szmigielska-Kaplon A, Urbaniak-Kujda D, Dybko J, Zielinska P, Dabrowska-Iwanicka A, Werkun J, Rzepecki P, Wroblewska W, Wiktor-Jedrzejczak W. Hematopoietic stem cell mobilization with the reversible CXCR4 receptor inhibitor plerixafor (AMD3100)-Polish compassionate use experience. Ann Hematol. 2011;90:557-68. Beksac M, Preffer F. Is it time to revisit our current hematopoietic progenitor cell quantification methods in the clinic? Bone Marrow Transplant. 2012;47:1391-6. Bensinger W, DiPersio JF, McCarty JM. Improving stem cell mobilization strategies: future directions. Bone Marrow Transplant. 2009;43:181-95. Berz D, McCormack EM, Winer ES, Colvin GA, Quesenberry PJ. Cryopreservation of hematopoietic stem cells. Am J Hematol. 2007;82:463-72. Beyer J, Schwella N, Zingsem J, Strohscheer I, Schwaner I, Oettle H, Serke S, Huhn D, Stieger W. Hematopoietic rescue after high-dose chemotherapy using autologous peripheral-blood progenitor cells or bone marrow: a randomized comparison. J Clin Oncol. 1995;13:1328-35. Bird JM, Owen RG, D'Sa S, Snowden JA, Pratt G, Ashcroft J, Yong K, Cook G, Feyler S, Davies F, Morgan G, Cavenagh J, Low E, Behrens J; Haemato-oncology Task Force of British Committee for Standards in Haematology (BCSH) and UK Myeloma Forum. Guidelines for the diagnosis and management of multiple myeloma 2011. Br J Haematol. 2011;154:32-75. Blystad AK, Delabie J, Kvaløy S, Holte H, Vålerhaugen H, Ikonomou I, Kvalheim G. Infused CD34 cell dose, but not tumour cell content of peripheral blood progenitor cell grafts, predicts clinical outcome in patients with diffuse large B-cell lymphoma and follicular lymphoma grade 3 treated with high-dose therapy. Br J Haematol. 2004;125:605-12. Blystad AK, Enblad G, Kvaløy S, Berglund A, Delabie J, Holte H, Carlson K, Kvalheim G, Bengtsson M, Hagberg H. High-dose therapy with autologous stem cell transplantation in patients with peripheral T cell lymphomas. Bone Marrow Transplant. 2001;27:711-6.

61
Bodart V, Anastassov V, Darkes MC, Idzan SR, Labrecque J, Lau G, Mosi RM, Neff KS, Nelson KL, Ruzek MC, Patel K, Santucci Z, Scarborough R, Wong RS, Bridger GJ, Macfarland RT, Fricker SP. Pharmacology of AMD3465: a small molecule antagonist of the chemokine receptor CXCR4. Biochem Pharmacol. 2009;78:993-1000. Bojanic I, Cepulic BG, Mazic S, Batinic D, Nemet D, Labar B. Toxicity related to autologous peripheral blood haematopoietic progenitor cell infusion is associated with number of granulocytes in graft, gender and diagnosis of multiple myeloma. Vox Sang. 2008;95:70-5. Bojanic I, Dubravcic K, Batinic D, Cepulic BG, Mazic S, Hren D, Nemet D, Labar B. Large volume leukapheresis: Efficacy and safety of processing patient's total blood volume six times. Transfus Apher Sci. 2011;44:139-47. Bolwell B, Sobecks R, Pohlman B, Andresen S, Theil K, Serafino S, Rybicki L, Kalaycio M. Etoposide (VP-16) plus G-CSF mobilizes different dendritic cell subsets than does G-CSF alone. Bone Marrow Transplant. 2003;31:95-8. Bolwell BJ, Pohlman B, Rybicki L, Sobecks R, Dean R, Curtis J, Andresen S, Koo A, Mineff V, Kalaycio M, Sweetenham JW. Patients mobilizing large numbers of CD34+ cells ('super mobilizers') have improved survival in autologous stem cell transplantation for lymphoid malignancies. Bone Marrow Transplant. 2007;40:437-41. Bomberger C, Singh-Jairam M, Rodey G, Guerriero A, Yeager AM, Fleming WH, Holland HK, Waller EK. Lymphoid reconstitution after autologous PBSC transplantation with FACS-sorted CD34+ hematopoietic progenitors. Blood. 1998;91:2588-600. Borge OJ, Ramsfjell V, Cui L, Jacobsen SE. Ability of early acting cytokines to directly promote survival and suppress apoptosis of human primitive CD34+CD38- bone marrow cells with multilineage potential at the single-cell level: key role of thrombopoietin. Blood. 1997;90:2282-92. Bourhis JH, Bouko Y, Koscielny S, Bakkus M, Greinix H, Derigs G, Salles G, Feremans W, Apperley J, Samson D, Björkstrand B, Niederwieser D, Gahrton G, Pico JL, Goldschmidt H; European Group for Blood and Marrow Transplantation. Relapse risk after autologous transplantation in patients with newly diagnosed myeloma is not related with infused tumor cell load and the outcome is not improved by CD34+ cell selection: long term follow-up of an EBMT phase III randomized study. Haematologica. 2007;92:1083-90. Branch DR, Calderwood S, Cecutti MA, Herst R, Solh H. Hematopoietic progenitor cells are resistant to dimethyl sulfoxide toxicity. Transfusion. 1994;34:887-90. Bredeson C, Malcolm J, Davis M, Bence-Bruckler I, Kearns B, Huebsch L. Cost analysis of the introduction of PBPC for autologous transplantation: effect of switching from bone marrow (BM) to peripheral blood progenitor cells (PBPC). Bone Marrow Transplant. 1997;20:889-96. Brice P, Simon D, Bouabdallah R, Bélanger C, Haïoun C, Thieblemont C, Tilly H, Harousseau JL, Doyen C, Martin C, Brousse N, Solal-Céligny PH; Groupe d'Etude des Lymphomes de l'Adulte (GELA). High-dose therapy with autologous stem-cell transplantation (ASCT) after first progression prolonged survival of follicular lymphoma patients included in the prospective GELF 86 protocol. Ann Oncol. 2000;11:1585-90.

62
Bridger GJ, Skerlj RT, Thornton D, Padmanabhan S, Martellucci SA, Henson GW, Abrams MJ, Yamamoto N, De Vreese K, Pauwels R, De Clercq E. Synthesis and structure-activity relationships of phenylenebis(methylene)-linked bis-tetraazamacrocycles that inhibit HIV replication. Effects of macrocyclic ring size and substituents on the aromatic linker. J Med Chem. 1995;38:366-78. Broxmeyer HE, Orschell CM, Clapp DW, Hangoc G, Cooper S, Plett PA, Liles WC, Li X, Graham-Evans B, Campbell TB, Calandra G, Bridger G, Dale DC, Srour EF. Rapid mobilization of murine and human hematopoietic stem and progenitor cells with AMD3100, a CXCR4 antagonist. J Exp Med. 2005;201:1307-18. Buzzai M, Licht JD. New molecular concepts and targets in acute myeloid leukemia. Curr Opin Hematol. 2008;15:82-7. Calandra G, McCarty J, McGuirk J, Tricot G, Crocker SA, Badel K, Grove B, Dye A, Bridger G. AMD3100 plus G-CSF can successfully mobilize CD34+ cells from non-Hodgkin's lymphoma, Hodgkin's disease and multiple myeloma patients previously failing mobilization with chemotherapy and/or cytokine treatment: compassionate use data. Bone Marrow Transplant. 2008;41:331-8. Camacho Villa AY, Reyes Maldonado E, Montiel Cervantes LA, Vela Ojeda J. CD133+CD34+ and CD133+CD38+ blood progenitor cells as predictors of platelet engraftment in patients undergoing autologous peripheral blood stem cell transplantation. Transfus Apher Sci. 2012;46:239-44. Cashen A, Lopez S, Gao F, Calandra G, MacFarland R, Badel K, DiPersio J. A phase II study of plerixafor (AMD3100) plus G-CSF for autologous hematopoietic progenitor cell mobilization in patients with Hodgkin lymphoma. Biol Blood Marrow Transplant. 2008;14:1253-61. Cesana C, Carlo-Stella C, Regazzi E, Garau D, Sammarelli G, Caramatti C, Tabilio A, Mangoni L, Rizzoli V. CD34+ cells mobilized by cyclophosphamide and granulocyte colony-stimulating factor (G-CSF) are functionally different from CD34+ cells mobilized by G-CSF. Bone Marrow Transplant. 1998;21:561-8. Chapple P, Prince HM, Wall D, Filshie R, Haylock D, Quinn M, Bretell M, Venter D. Comparison of three methods of CD34+ cell enumeration in peripheral blood: dual-platform ISHAGE protocol versus single-platform, versus microvolume fluorimetry. Cytotherapy. 2000;2:371-6. Chen AI, Bains T, Murray S, Knight R, Shoop K, Bubalo J, Fowler C, Slater S, Maziarz RT. Clinical experience with a simple algorithm for plerixafor utilization in autologous stem cell mobilization. Bone Marrow Transplant. 2012;47:1526-9. Cheng J, Baumhueter S, Cacalano G, Carver-Moore K, Thibodeaux H, Thomas R, Broxmeyer HE, Cooper S, Hague N, Moore M, Lasky LA. Hematopoietic defects in mice lacking the sialomucin CD34. Blood. 1996;87:479-90. Cheng M, Zhou J, Wu M, Boriboun C, Thorne T, Liu T, Xiang Z, Zeng Q, Tanaka T, Tang YL, Kishore R, Tomasson MH, Miller RJ, Losordo DW, Qin G. CXCR4-mediated bone marrow progenitor cell maintenance and mobilization are modulated by c-kit activity. Circ Res. 2010;107:1083-93.

63
Child JA, Morgan GJ, Davies FE, Owen RG, Bell SE, Hawkins K, Brown J, Drayson MT, Selby PJ; Medical Research Council Adult Leukaemia Working Party. High-dose chemotherapy with hematopoietic stem-cell rescue for multiple myeloma. N Engl J Med. 2003;348:1875-83. Christopher MJ, Liu F, Hilton MJ, Long F, Link DC. Suppression of CXCL12 production by bone marrow osteoblasts is a common and critical pathway for cytokine-induced mobilization. Blood. 2009;114:1331-9. Christopherson KW 2nd, Hangoc G, Mantel CR, Broxmeyer HE. Modulation of hematopoietic stem cell homing and engraftment by CD26. Science. 2004;305:1000-3. Clarke DM, Yadock DJ, Nicoud IB, Mathew AJ, Heimfeld S. Improved post-thaw recovery of peripheral blood stem/progenitor cells using a novel intracellular-like cryopreservation solution. Cytotherapy. 2009;11:472-9. Condomines M, Quittet P, Lu ZY, Nadal L, Latry P, Lopez E, Baudard M, Requirand G, Duperray C, Schved JF, Rossi JF, Tarte K, Klein B. Functional regulatory T cells are collected in stem cell autografts by mobilization with high-dose cyclophosphamide and granulocyte colony-stimulating factor. J Immunol. 2006;176:6631-9. Cordoba R, Arrieta R, Kerguelen A, Hernandez-Navarro F. The occurrence of adverse events during the infusion of autologous peripheral blood stem cells is related to the number of granulocytes in the leukapheresis product. Bone Marrow Transplant. 2007;40:1063-7. Costa LJ, Alexander ET, Hogan KR, Schaub C, Fouts TV, Stuart RK. Development and validation of a decision-making algorithm to guide the use of plerixafor for autologous hematopoietic stem cell mobilization. Bone Marrow Transplant. 2011;46:64-9. D'Addio A, Curti A, Worel N, Douglas K, Motta MR, Rizzi S, Dan E, Taioli S, Giudice V, Agis H, Kopetzky G, Soutar R, Casadei B, Baccarani M, Lemoli RM. The addition of plerixafor is safe and allows adequate PBSC collection in multiple myeloma and lymphoma patients poor mobilizers after chemotherapy and G-CSF. Bone Marrow Transplant. 2011;46:356-63. d'Amore F, Relander T, Lauritzsen GF, Jantunen E, Hagberg H, Anderson H, Holte H, Österborg A, Merup M, Brown P, Kuittinen O, Erlanson M, Østenstad B, Fagerli UM, Gadeberg OV, Sundström C, Delabie J, Ralfkiaer E, Vornanen M, Toldbod HE. Up-front autologous stem-cell transplantation in peripheral T-cell lymphoma: NLG-T-01. J Clin Oncol. 2012;30:3093-9. De Clercq E, Yamamoto N, Pauwels R, Baba M, Schols D, Nakashima H, Balzarini J, Debyser Z, Murrer BA, Schwartz D, Thornton D, Bridger G, Fricker S, Henson G, Abrams M, Picker D. Potent and selective inhibition of human immunodeficiency virus (HIV)-1 and HIV-2 replication by a class of bicyclams interacting with a viral uncoating event. Proc Natl Acad Sci USA. 1992;89:5286-90. De Clercq E, Yamamoto N, Pauwels R, Balzarini J, Witvrouw M, De Vreese K, Debyser Z, Rosenwirth B, Peichl P, Datema R, Thornton D, Skerlj R, Gaul F, Padmanabhan S, Bridger G, Henson G, Abrams M. Highly potent and selective inhibition of human immunodeficiency virus by the bicyclam derivative JM3100. Antimicrob Agents Chemother. 1994;38:668-74. De Clercq E. Recent advances on the use of the CXCR4 antagonist plerixafor (AMD3100, Mozobil™) and potential of other CXCR4 antagonists as stem cell mobilizers. Pharmacol Ther. 2010;128:509-18.

64
De Clercq E. The AMD3100 story: the path to the discovery of a stem cell mobilizer (Mozobil). Biochem Pharmacol. 2009;77:1655-64. De Nigris F, Schiano C, Infante T, Napoli C. CXCR4 inhibitors: tumour vasculature and therapeutic challenges. Recent Pat Anticancer Drug Discov. 2012;7:251-64. De Vreese K, Van Nerum I, Vermeire K, Anné J, De Clercq E. Sensitivity of human immunodeficiency virus to bicyclam derivatives is influenced by the three-dimensional structure of gp120. Antimicrob Agents Chemother. 1997;41:2616-20. de Wynter EA, Buck D, Hart C, Heywood R, Coutinho LH, Clayton A, Rafferty JA, Burt D, Guenechea G, Bueren JA, Gagen D, Fairbairn LJ, Lord BI, Testa NG. CD34+AC133+ cells isolated from cord blood are highly enriched in long-term culture-initiating cells, NOD/SCID-repopulating cells and dendritic cell progenitors. Stem Cells. 1998;16:387-96. Dean R, Masci P, Pohlman B, Andresen S, Serafino S, Sobecks R, Kuczkowski E, Curtis J, Maciejewski J, Rybicki L, Kalaycio M, Hsi E, Theil K, Bolwell BJ. Dendritic cells in autologous hematopoietic stem cell transplantation for diffuse large B-cell lymphoma: graft content and post transplant recovery predict survival. Bone Marrow Transplant. 2005;36:1049-52. Deconinck E, Foussard C, Milpied N, Bertrand P, Michenet P, Cornillet-LeFebvre P, Escoffre-Barbe M, Maisonneuve H, Delwail V, Gressin R, Legouffe E, Vilque JP, Desablens B, Jaubert J, Ramee JF, Jenabian A, Thyss A, Le Pourhiet-Le Mevel A, Travade P, Delepine R, Colombat P; GOELAMS. High-dose therapy followed by autologous purged stem-cell transplantation and doxorubicin-based chemotherapy in patients with advanced follicular lymphoma: a randomized multicenter study by GOELAMS. Blood. 2005;105:3817-23. Decot V, Alla F, Latger-Cannard V, Visanica S, Witz B, Stoltz JF, Bensoussan D. Thawed autologous peripheral blood stem cells require modified quantification methods for hematopoietic progenitor cell evaluation. Biomed Mater Eng. 2012;22:57-67. Demirkazik A, Kessinger A, Armitage JO, Bierman PJ, Lynch J, Vose J, Chan W, Sharp JG. Progenitor and lymphoma cells in blood stem cell harvests: impact on survival following transplantation. Bone Marrow Transplant. 2001;28:207-12. Deol A, Abrams J, Masood A, Al-Kadhimi Z, Abidi MH, Ayash L, Lum LG, Ratanatharathorn V, Uberti JP. Long-term follow up of patients proceeding to transplant using plerixafor mobilized stem cells and incidence of secondary myelodysplastic syndrome/AML. Bone Marrow Transplant. 2013;48:1112-6. Desikan KR, Barlogie B, Jagannath S, Vesole DH, Siegel D, Fassas A, Munshi N, Singhal S, Mehta J, Tindle S, Nelson J, Bracy D, Mattox S, Tricot G. Comparable engraftment kinetics following peripheral-blood stem-cell infusion mobilized with granulocyte colony-stimulating factor with or without cyclophosphamide in multiple myeloma. J Clin Oncol. 1998;16:1547-53. Devine SM, Flomenberg N, Vesole DH, Liesveld J, Weisdorf D, Badel K, Calandra G, DiPersio JF. Rapid mobilization of CD34+ cells following administration of the CXCR4 antagonist AMD3100 to patients with multiple myeloma and non-Hodgkin's lymphoma. J Clin Oncol. 2004;22:1095-102.

65
DiPersio JF, Bridger G, Calandra G. Effect of plerixafor (AMD3100) plus G-CSF on tumor cell mobilization among patients with lymphoma. Biol Blood Marrow Transplant. 2009;15:37. DiPersio JF, Ho AD, Hanrahan J, Hsu FJ, Fruehauf S. Relevance and clinical implications of tumor cell mobilization in the autologous transplant setting. Biol Blood Marrow Transplant. 2011;17:943-55. DiPersio JF, Micallef IN, Stiff PJ, Bolwell BJ, Maziarz RT, Jacobsen E, Nademanee A, McCarty J, Bridger G, Calandra G; 3101 Investigators. Phase III prospective randomized double-blind placebo-controlled trial of plerixafor plus granulocyte colony-stimulating factor compared with placebo plus granulocyte colony-stimulating factor for autologous stem-cell mobilization and transplantation for patients with non-Hodgkin's lymphoma. J Clin Oncol. 2009a;27:4767-73. DiPersio JF, Stadtmauer EA, Nademanee A, Micallef IN, Stiff PJ, Kaufman JL, Maziarz RT, Hosing C, Früehauf S, Horwitz M, Cooper D, Bridger G, Calandra G; 3102 Investigators. Plerixafor and G-CSF versus placebo and G-CSF to mobilize hematopoietic stem cells for autologous stem cell transplantation in patients with multiple myeloma. Blood. 2009b;113:5720-6. Dobo I, Pineau D, Robillard N, Geneviève F, Piard N, Zandecki M, Hermouet S. Standardization of the CFU-GM assay: Advantages of plating a fixed number of CD34+ cells in collagen gels. J Hematother Stem Cell Res. 2003;12:543-51. Domanska UM, Timmer-Bosscha H, Nagengast WB, Oude Munnink TH, Kruizinga RC, Ananias HJ, Kliphuis NM, Huls G, De Vries EG, de Jong IJ, Walenkamp AM. CXCR4 inhibition with AMD3100 sensitizes prostate cancer to docetaxel chemotherapy. Neoplasia. 2012;14:709-18. Donahue RE, Jin P, Bonifacino AC, Metzger ME, Ren J, Wang E, Stroncek DF. Plerixafor (AMD3100) and granulocyte colony-stimulating factor (G-CSF) mobilize different CD34+ cell populations based on global gene and microRNA expression signatures. Blood. 2009;114:2530-41. Donzella GA, Schols D, Lin SW, Esté JA, Nagashima KA, Maddon PJ, Allaway GP, Sakmar TP, Henson G, De Clercq E, Moore JP. AMD3100, a small molecule inhibitor of HIV-1 entry via the CXCR4 co-receptor. Nat Med. 1998;4:72-7. Drake M, Ranaghan L, Morris TC, Nolan L, Desai ZR, Irvine AE, Jordan A, Magill K, Price S. Analysis of the effect of prior therapy on progenitor cell yield: use of a chemotherapy scoring system. Br J Haematol. 1997;98:745-9. Dreger P, Viehmann K, von Neuhoff N, Glaubitz T, Petzoldt O, Glass B, Uharek L, Rautenberg P, Suttorp M, Mills B, Mitsky P, Schmitz N. Autografting of highly purified peripheral blood progenitor cells following myeloablative therapy in patients with lymphoma: a prospective study of the long-term effects on tumor eradication, reconstitution of hematopoiesis and immune recovery. Bone Marrow Transplant. 1999;24:153-61. Dreyling M, Lenz G, Hoster E, Van Hoof A, Gisselbrecht C, Schmits R, Metzner B, Truemper L, Reiser M, Steinhauer H, Boiron JM, Boogaerts MA, Aldaoud A, Silingardi V, Kluin-Nelemans HC, Hasford J, Parwaresch R, Unterhalt M, Hiddemann W. Early consolidation by myeloablative radiochemotherapy followed by autologous stem cell transplantation in first remission significantly prolongs progression-free survival in mantle-cell lymphoma: results of a prospective randomized trial of the European MCL Network. Blood. 2005;105:2677-84.

66
Duarte RF, Shaw BE, Marín P, Kottaridis P, Ortiz M, Morante C, Delgado J, Gayoso J, Goterriz R, Martínez-Chamorro C, Mateos-Mazón JJ, Ramírez C, de la Rubia J, Achtereekte H, Gandhi PJ, Douglas KW, Russell NH. Plerixafor plus granulocyte CSF can mobilize hematopoietic stem cells from multiple myeloma and lymphoma patients failing previous mobilization attempts: EU compassionate use data. Bone Marrow Transplant. 2011;46:52-8. Dugan MJ, Maziarz RT, Bensinger WI, Nademanee A, Liesveld J, Badel K, Dehner C, Gibney C, Bridger G, Calandra G. Safety and preliminary efficacy of plerixafor (Mozobil) in combination with chemotherapy and G-CSF: an open-label, multicenter, exploratory trial in patients with multiple myeloma and non-Hodgkin's lymphoma undergoing stem cell mobilization. Bone Marrow Transplant. 2010;45:39-47. Egberink HF, De Clercq E, Van Vliet AL, Balzarini J, Bridger GJ, Henson G, Horzinek MC, Schols D. Bicyclams, selective antagonists of the human chemokine receptor CXCR4, potently inhibit feline immunodeficiency virus replication. J Virol. 1999;73:6346-52. Eksioglu EA, Kielbasa J, Eisen S, Reddy V. Granulocyte-macrophage colony-stimulating factor increases the proportion of circulating dendritic cells after autologous but not after allogeneic hematopoietic stem cell transplantation. Cytotherapy. 2011;13:888-96. Esté JA, Cabrera C, De Clercq E, Struyf S, Van Damme J, Bridger G, Skerlj RT, Abrams MJ, Henson G, Gutierrez A, Clotet B, Schols D. Activity of different bicyclam derivatives against human immunodeficiency virus depends on their interaction with the CXCR4 chemokine receptor. Mol Pharmacol. 1999;55:67-73. Faussner F, Dempke WC. Multiple myeloma: myeloablative therapy with autologous stem cell support versus chemotherapy: a meta-analysis. Anticancer Res. 2012;32:2103-9. Fermand JP, Katsahian S, Divine M, Leblond V, Dreyfus F, Macro M, Arnulf B, Royer B, Mariette X, Pertuiset E, Belanger C, Janvier M, Chevret S, Brouet JC, Ravaud P; Group Myelome-Autogreffe. High-dose therapy and autologous blood stem-cell transplantation compared with conventional treatment in myeloma patients aged 55 to 65 years: long-term results of a randomized control trial from the Group Myelome-Autogreffe. J Clin Oncol. 2005;23:9227-33. Fernyhough LJ, Buchan VA, McArthur LT, Hock BD. Relative recovery of haematopoietic stem cell products after cryogenic storage of up to 19 years. Bone Marrow Transplant. 2013;48:32-5. Ferrucci PF, Martinoni A, Cocorocchio E, Civelli M, Cinieri S, Cardinale D, Peccatori FA, Lamantia G, Agazzi A, Corsini C, Tealdo F, Fiorentini C, Cipolla CM, Martinelli G. Evaluation of acute toxicities associated with autologous peripheral blood progenitor cell reinfusion in patients undergoing high-dose chemotherapy. Bone Marrow Transplant. 2000;25:173-7. Fina L, Molgaard HV, Robertson D, Bradley NJ, Monaghan P, Delia D, Sutherland DR, Baker MA, Greaves MF. Expression of the CD34 gene in vascular endothelial cells. Blood. 1990;75:2417-26. Flomenberg N, Devine SM, Dipersio JF, Liesveld JL, McCarty JM, Rowley SD, Vesole DH, Badel K, Calandra G. The use of AMD3100 plus G-CSF for autologous hematopoietic progenitor cell mobilization is superior to G-CSF alone. Blood. 2005;106:1867-74.

67
Foïs E, Desmartin M, Benhamida S, Xavier F, Vanneaux V, Rea D, Fermand JP, Arnulf B, Mounier N, Ertault M, Lotz JP, Galicier L, Raffoux E, Benbunan M, Marolleau JP, Larghero J. Recovery, viability and clinical toxicity of thawed and washed haematopoietic progenitor cells: analysis of 952 autologous peripheral blood stem cell transplantations. Bone Marrow Transplant. 2007;40:831-5. Foran JM, Apostolidis J, Papamichael D, Norton AJ, Matthews J, Amess JA, Lister TA, Rohatiner AZ. High-dose therapy with autologous haematopoietic support in patients with transformed follicular lymphoma: a study of 27 patients from a single centre. Ann Oncol. 1998;9:865-9. Fowler CJ, Dunn A, Hayes-Lattin B, Hansen K, Hansen L, Lanier K, Nelson V, Kovacsovics T, Leis J, Calandra G, Maziarz RT. Rescue from failed growth factor and/or chemotherapy HSC mobilization with G-CSF and plerixafor (AMD3100): an institutional experience. Bone Marrow Transplant. 2009;43:909-17. Frei E, Canellos GP. Dose: a critical factor in cancer chemotherapy. Am J Med. 1980;69:585-94. Freireich EJ, Judson G, Levin RH. Separation and collection of leukocytes. Cancer Res. 1965;25:1516-20. Fricker SP, Anastassov V, Cox J, Darkes MC, Grujic O, Idzan SR, Labrecque J, Lau G, Mosi RM, Nelson KL, Qin L, Santucci Z, Wong RS. Characterization of the molecular pharmacology of AMD3100: a specific antagonist of the G-protein coupled chemokine receptor, CXCR4. Biochem Pharmacol. 2006;72:588-96. Fruehauf S, Seeger T, Maier P, Li L, Weinhardt S, Laufs S, Wagner W, Eckstein V, Bridger G, Calandra G, Wenz F, Zeller WJ, Goldschmidt H, Ho AD. The CXCR4 antagonist AMD3100 releases a subset of G-CSF-primed peripheral blood progenitor cells with specific gene expression characteristics. Exp Hematol. 2006;34:1052-9. Fruehauf S, Ehninger G, Hübel K, Topaly J, Goldschmidt H, Ho AD, Müller S, Moos M, Badel K, Calandra G. Mobilization of peripheral blood stem cells for autologous transplant in non-Hodgkin's lymphoma and multiple myeloma patients by plerixafor and G-CSF and detection of tumor cell mobilization by PCR in multiple myeloma patients. Bone Marrow Transplant. 2010;45:269-75. Fruehauf S, Tricot G. Comparison of unmobilized and mobilized graft characteristics and the implications of cell subsets on autologous and allogeneic transplantation outcomes. Biol Blood Marrow Transplant. 2010;16:1629-48. Fruehauf S, Veldwijk MR, Seeger T, Schubert M, Laufs S, Topaly J, Wuchter P, Dillmann F, Eckstein V, Wenz F, Goldschmidt H, Ho AD, Calandra G. A combination of granulocyte-colony-stimulating factor (G-CSF) and plerixafor mobilizes more primitive peripheral blood progenitor cells than G-CSF alone: results of a European phase II study. Cytotherapy. 2009;11:992-1001. Fukuda S, Bian H, King AG, Pelus LM. The chemokine GRObeta mobilizes early hematopoietic stem cells characterized by enhanced homing and engraftment. Blood. 2007;110:860-9.

68
Gajkowska A, Oldak T, Jastrzewska M, Machaj EK, Walewski J, Kraszewska E, Pojda Z. Flow cytometric enumeration of CD34+ hematopoietic stem and progenitor cells in leukapheresis product and bone marrow for clinical transplantation: a comparison of three methods. Folia Histochem Cytobiol. 2006;44:53-60. Gašová Z, Bhuiyan-#*^$�{ $������� $�������� $�����{ $���� �������~�}������|PBPC collections: management, techniques and risks. Transfus Apher Sci. 2010;43:237-43. Gaugler B, Arbez J, Frikeche J, Le Gouill S, Gastinne T, Blin N, Chevallier P, Guillaume T, Delaunay J, Ayari S, Rialland F, Mahe B, Dubruille V, Clavert A, Rolland V, Saas P, Moreau P, Derenne S, Mohty M. Characterization of peripheral blood stem cell grafts mobilized by G-CSF and plerixafor in comparison to G-CSF alone. Bone Marrow Transplant 2011;46(Suppl.1):S61 (abstr. 380). Gawronski K, Rzepecki P, Oborska S, Wasko-Grabowska A. Hematologic recovery in patients who are treated with autologous stem cells transplantation taken from bone marrow after granulocyte-colony-stimulating factor stimulation. Transplant Proc. 2011;43:3114-5. Gazitt Y, Freytes CO, Akay C, Badel K, Calandra G. Improved mobilization of peripheral blood CD34+ cells and dendritic cells by AMD3100 plus granulocyte-colony-stimulating factor in non-Hodgkin's lymphoma patients. Stem Cells Dev. 2007;16:657-66. Geisler CH, Hansen MM, Andersen NS, Brown P, Christensen LD, Dickmeiss E, Ersbøll J, Myhre J, Hansen M, Juhl BR, Mortensen BT, Pedersen-Bjergaard J. BEAM+autologous stem cell transplantation in malignant lymphoma: 100 consecutive transplants in a single centre. Efficacy, toxicity and engraftment in relation to stem-cell source and previous treatment. Eur J Haematol. 1998;61:173-82. Geisler CH, Kolstad A, Laurell A, Andersen NS, Pedersen LB, Jerkeman M, Eriksson M, Nordström M, Kimby E, Boesen AM, Kuittinen O, Lauritzsen GF, Nilsson-Ehle H, Ralfkiaer E, Akerman M, Ehinger M, Sundström C, Langholm R, Delabie J, Karjalainen-Lindsberg ML, Brown P, Elonen E; Nordic Lymphoma Group. Long-term progression-free survival of mantle cell lymphoma after intensive front-line immunochemotherapy with in vivo-purged stem cell rescue: a nonrandomized phase 2 multicenter study by the Nordic Lymphoma Group. Blood. 2008;112:2687-93 Geisler CH, Kolstad A, Laurell A, Jerkeman M, Räty R, Andersen NS, Pedersen LB, Eriksson M, Nordström M, Kimby E, Bentzen H, Kuittinen O, Lauritzsen GF, Nilsson-Ehle H, Ralfkiaer E, Ehinger M, Sundström C, Delabie J, Karjalainen-Lindsberg ML, Brown P, Elonen E; Nordic Lymphoma Group. Nordic MCL2 trial update: six-year follow-up after intensive immunochemotherapy for untreated mantle cell lymphoma followed by BEAM or BEAC + autologous stem-cell support: still very long survival but late relapses do occur. Br J Haematol. 2012;158:355-62. Genzyme Corporation. Mozobil (plerixafor injection), Highlights of prescribing information and full prescribing information. [cited 14.9.2013] http://www.mozobil.com/document/Package_Insert.pdf. Gertz MA. Current status of stem cell mobilization. Br J Haematol. 2010;150:647-62.

69
Gianni AM, Siena S, Bregni M, Tarella C, Stern AC, Pileri A, Bonadonna G. Granulocyte-macrophage colony-stimulating factor to harvest circulating haemopoietic stem cells for autotransplantation. Lancet. 1989;2:580-5. Gianni AM, Bregni M, Siena S, Brambilla C, Di Nicola M, Lombardi F, Gandola L, Tarella C, Pileri A, Ravagnani F, Valagussa P, Bonadonna G. High-dose chemotherapy and autologous bone marrow transplantation compared with MACOP-B in aggressive B-cell lymphoma. N Engl J Med. 1997;336:1290-7. Giralt S, Stadtmauer EA, Harousseau JL, Palumbo A, Bensinger W, Comenzo RL, Kumar S, Munshi NC, Dispenzieri A, Kyle R, Merlini G, San Miguel J, Ludwig H, Hajek R, Jagannath S, Blade J, Lonial S, Dimopoulos MA, Einsele H, Barlogie B, Anderson KC, Gertz M, Attal M, Tosi P, Sonneveld P, Boccadoro M, Morgan G, Sezer O, Mateos MV, Cavo M, Joshua D, Turesson I, Chen W, Shimizu K, Powles R, Richardson PG, Niesvizky R, Rajkumar SV, Durie BG; IMWG. International myeloma working group (IMWG) consensus statement and guidelines regarding the current status of stem cell collection and high-dose therapy for multiple myeloma and the role of plerixafor (AMD 3100). Leukemia. 2009;23:1904-12. Gopal AK, Karami M, Mayor J, Macebeo M, Linenberger M, Bensinger WI, Holmberg L. The effective use of plerixafor as a real-time rescue strategy for patients poorly mobilizing autologous CD34(+) cells. J Clin Apher. 2012;27:81-7. Gordan LN, Sugrue MW, Lynch JW, Williams KD, Khan SA, Moreb JS. Correlation of early lymphocyte recovery and progression-free survival after autologous stem-cell transplant in patients with Hodgkin's and non-Hodgkin's Lymphoma. Bone Marrow Transplant. 2003;31:1009-13. Gordon PR, Leimig T, Babarin-Dorner A, Houston J, Holladay M, Mueller I, Geiger T, Handgretinger R. Large-scale isolation of CD133+ progenitor cells from G-CSF mobilized peripheral blood stem cells. Bone Marrow Transplant. 2003;31:17-22. Goterris R, Hernández-Boluda JC, Teruel A, Gómez C, Lis MJ, Terol MJ, Tormo M, Solano C, Arbona C. Impact of different strategies of second-line stem cell harvest on the outcome of autologous transplantation in poor peripheral blood stem cell mobilizers. Bone Marrow Transplant. 2005;36:847-53. Goto-Koshino Y, Fukuchi Y, Shibata F, Abe D, Kuroda K, Okamoto S, Kitamura T, Nakajima H. Robo4 plays a role in bone marrow homing and mobilization, but is not essential in the long-term repopulating capacity of hematopoietic stem cells. PLoS One. 2012;7:e50849. Gratama JW, Orfao A, Barnett D, Brando B, Huber A, Janossy G, Johnsen HE, Keeney M, Marti GE, Preijers F, Rothe G, Serke S, Sutherland DR, Van der Schoot CE, Schmitz G, Papa S. Flow cytometric enumeration of CD34+ hematopoietic stem and progenitor cells. European Working Group on Clinical Cell Analysis. Cytometry. 1998;34:128-42. Greb A, Bohlius J, Schiefer D, Schwarzer G, Schulz H, Engert A. High-dose chemotherapy with autologous stem cell transplantation in the first line treatment of aggressive non-Hodgkin lymphoma (NHL) in adults. Cochrane Database Syst Rev. 2008;CD004024. Gregory WM, Richards MA, Malpas JS. Combination chemotherapy versus melphalan and prednisolone in the treatment of multiple myeloma: an overview of published trials. J Clin Oncol. 1992;10:334-42.

70
Gunnellini M, Emili R, Coaccioli S, Liberati AM. The role of autologous stem cell transplantation in the treatment of diffuse large B-cell lymphoma. Adv Hematol. 2012;2012:195484. Gyan E, Foussard C, Bertrand P, Michenet P, Le Gouill S, Berthou C, Maisonneuve H, Delwail V, Gressin R, Quittet P, Vilque JP, Desablens B, Jaubert J, Ramée JF, Arakelyan N, Thyss A, Moluçon-Chabrot C, Delépine R, Milpied N, Colombat P, Deconinck E; Groupe Ouest-Est des Leucémies et des Autres Maladies du Sang (GOELAMS). High-dose therapy followed by autologous purged stem cell transplantation and doxorubicin-based chemotherapy in patients with advanced follicular lymphoma: a randomized multicenter study by the GOELAMS with final results after a median follow-up of 9 years. Blood. 2009;113:995-1001. Hay AE, Lawrie A, Robinson N, Dong B, Culligan DJ. A retrospective study of autologous stem cell mobilization to guide an immediate salvage protocol using plerixafor for patients who mobilize stem cells poorly. J Clin Apher. 2013 Mar 11 [Epub ahead of print]. Haioun C, Lepage E, Gisselbrecht C, Salles G, Coiffier B, Brice P, Bosly A, Morel P, Nouvel C, Tilly H, Lederlin P, Sebban C, Brière J, Gaulard P, Reyes F. Survival benefit of high-dose therapy in poor-risk aggressive non-Hodgkin's lymphoma: final analysis of the prospective LNH87-2 protocol-a groupe d'Etude des lymphomes de l'Adulte study. J Clin Oncol. 2000;18:3025-30. Hamadani M, Benson DM Jr, Lin TS, Porcu P, Blum KA, Devine SM. High-dose therapy and autologous stem cell transplantation for follicular lymphoma undergoing transformation to diffuse large B-cell lymphoma. Eur J Haematol. 2008;81:425-31. Hassan HT, Stockschläder M, Schleimer B, Krüger W, Zander AR. Comparison of the content and subpopulations of CD3 and CD34 positive cells in bone marrow harvests and G-CSF-mobilized peripheral blood leukapheresis products from healthy adult donors. Transpl Immunol. 1996;4:319-23. Heckmann D, Maier P, Laufs S, Wenz F, Zeller WJ, Fruehauf S, Allgayer H. CXCR4 expression and treatment with SDF-�� �plerixafor modulate proliferation and chemosensitivity of colon cancer cells. Transl Oncol. 2013;6:124-32. Heissig B, Hattori K, Dias S, Friedrich M, Ferris B, Hackett NR, Crystal RG, Besmer P, Lyden D, Moore MA, Werb Z, Rafii S. Recruitment of stem and progenitor cells from the bone marrow niche requires MMP-9 mediated release of kit-ligand. Cell. 2002;109:625-37. Hendrix CW, Collier AC, Lederman MM, Schols D, Pollard RB, Brown S, Jackson JB, Coombs RW, Glesby MJ, Flexner CW, Bridger GJ, Badel K, MacFarland RT, Henson GW, Calandra G; AMD3100 HIV Study Group. Safety, pharmacokinetics, and antiviral activity of AMD3100, a selective CXCR4 receptor inhibitor, in HIV-1 infection. J Acquir Immune Defic Syndr. 2004;37:1253-62. Hendrix CW, Flexner C, MacFarland RT, Giandomenico C, Fuchs EJ, Redpath E, Bridger G, Henson GW. Pharmacokinetics and safety of AMD-3100, a novel antagonist of the CXCR-4 chemokine receptor, in human volunteers. Antimicrob Agents Chemother. 2000;44:1667-73.
71
Hénon P, Sovalat H, Becker M, Arkam Y, Ojeda-Uribe M, Raidot JP, Husseini F, Wunder E, Bourderont D, Audhuy B. Primordial role of CD34+ 38- cells in early and late trilineage haemopoietic engraftment after autologous blood cell transplantation. Br J Haematol. 1998b;103:568-81. Hénon P, Sovalat H, Bourderont D, Ojeda-Uribe M, Arkam Y, Wunder E, Raidot JP, Husseini F, Audhuy B. Role of the CD34+ 38- cells in posttransplant hematopoietic recovery. Stem Cells. 1998a;Suppl 1:113-22. Hess DA, Wirthlin L, Craft TP, Herrbrich PE, Hohm SA, Lahey R, Eades WC, Creer MH, Nolta JA. Selection based on CD133 and high aldehyde dehydrogenase activity isolates long-term reconstituting human hematopoietic stem cells. Blood. 2006;107:2162-9. Heuft HG, Dubiel M, Kingreen D, Oertel J, De Reys S, Rick O, Serke S, Schwella N. Automated collection of peripheral blood stem cells with the COBE Spectra for autotransplantation. Vox Sang. 2000;79:94-9. Hicks C, Isaacs A, Wong R, Chong BH. CXCR4 expression on transplanted peripheral blood CD34+ cells: relationship to engraftment after autologous transplantation in a cohort of multiple myeloma patients. Ann Hematol. 2011;90:547-55. Hicks C, Wong R, Manoharan A, Kwan YL. Viable CD34+/CD133+ blood progenitor cell dose as a predictor of haematopoietic engraftment in multiple myeloma patients undergoing autologous peripheral blood stem cell transplantation. Ann Hematol. 2007;86:591-8. Hicks ML, Lonial S, Langston A, Flowers C, Roback JD, Smith KJ, Mossavi Sai S, Teagarden D, Hamilton ES, Waller EK, Kaufman J. Optimizing the timing of chemotherapy for mobilizing autologous blood hematopoietic progenitor cells. Transfusion. 2007;47:629-35. Hildebrandt M, Dijkstra D, Gollasch H, Daemen K, Stevanovic-Meyer M, Ludwig WD. Apheresis-related enrichment of CD26++ T lymphocytes: phenotypic characterization and correlation with unfavorable outcome in autologous hematopoietic progenitor cell transplantation. Transfusion. 2012;52:765-76. Hiwase DK, Hiwase S, Bailey M, Bollard G, Schwarer AP. Higher infused lymphocyte dose predicts higher lymphocyte recovery, which in turn, predicts superior overall survival following autologous hematopoietic stem cell transplantation for multiple myeloma. Biol Blood Marrow Transplant. 2008b;14:116-24. Hiwase DK, Hiwase S, Bailey M, Bollard G, Schwarer AP. The role of stem cell mobilization regimen on lymphocyte collection yield in patients with multiple myeloma. Cytotherapy. 2008a;10:507-17. Ho J, Yang L, Banihashemi B, Martin L, Halpenny M, Atkins H, Sabloff M, McDiarmid SA, Huebsch LB, Bence-Bruckler I, Giulivi A, Allan DS. Contaminating tumour cells in autologous PBSC grafts do not influence survival or relapse following transplant for multiple myeloma or B-cell non-Hodgkin's lymphoma. Bone Marrow Transplant. 2009;43:223-8. Hollingsworth KL, Zimmerman TM, Karrison T, Oliver A, Williams SF. The CD34+ cell concentration in peripheral blood predicts CD34+ cell yield in the leukapheresis product. Cytotherapy. 1999;1:141-6.

72
Holtan SG, Porrata LF, Micallef IN, Padley DJ, Inwards DJ, Ansell SA, Johnston PB, Gastineau DA, Markovic SN. AMD3100 affects autograft lymphocyte collection and progression-free survival after autologous stem cell transplantation in non-Hodgkin lymphoma. Clin Lymphoma Myeloma. 2007;7:315-8. Horwitz ME, Chute JP, Gasparetto C, Long GD, McDonald C, Morris A, Rizzieri DA, Sullivan KM, Chao NJ. Preemptive dosing of plerixafor given to poor stem cell mobilizers on day 5 of G-CSF administration. Bone Marrow Transplant. 2012;47:1051-5. Hu MC, Chien SL. The cytoplasmic domain of stem cell antigen CD34 is essential for cytoadhesion signaling but not sufficient for proliferation signaling. Blood. 1998;91:1152-62. Huang S, Terstappen LW. Lymphoid and myeloid differentiation of single human CD34+, HLA-DR+, CD38- hematopoietic stem cells. Blood. 1994;83:1515-26. Hübel K, Fresen MM, Apperley JF, Basak GW, Douglas KW, Gabriel IH, Geraldes C, Jaksic O, Koristek Z, Kröger N, Lanza F, Lemoli RM, Mikala G, Selleslag D, Worel N, Mohty M, Duarte RF. European data on stem cell mobilization with plerixafor in non-Hodgkin's lymphoma, Hodgkin's lymphoma and multiple myeloma patients. A subgroup analysis of the European Consortium of stem cell mobilization. Bone Marrow Transplant. 2012;47:1046-50. Hübel K, Fresen MM, Salwender H, Basara N, Beier R, Theurich S, Christopeit M, Bogner C, Galm O, Hartwig R, Heits F, Lordick F, Rösler W, Wehler D, Zander AR, Albert MH, Dressler S, Ebinger M, Frickhofen N, Hertenstein B, Kiehl M, Liebler S, von Lilienfeld-Toal M, Weidmann E, Weigelt C, Lange F, Kröger N. Plerixafor with and without chemotherapy in poor mobilizers: results from the German compassionate use program. Bone Marrow Transplant. 2011;46:1045-52. Hübel K, Liles WC, Broxmeyer HE, Rodger E, Wood B, Cooper S, Hangoc G, Macfarland R, Bridger GJ, Henson GW, Calandra G, Dale DC. Leukocytosis and mobilization of CD34+ hematopoietic progenitor cells by AMD3100, a CXCR4 antagonist. Support Cancer Ther. 2004;1:165-72. Ikeda K, Ohto H, Kanno T, Ogata T, Noji H, Ogawa K, Maruyama Y. Automated programs for collection of mononuclear cells and progenitor cells by two separators for peripheral blood progenitor cell transplantation: comparison by a randomized crossover study. Transfusion. 2007;47:1234-40. Jansen J, Thompson JM, Dugan MJ, Nolan P, Wiemann MC, Birhiray R, Henslee-Downey PJ, Akard LP. Peripheral blood progenitor cell transplantation. Ther Apher. 2002;6:5-14. Jantunen E, Boumendil A, Finel H, Luan JJ, Johnson P, Rambaldi A, Haynes A, Duchosal MA, Bethge W, Biron P, Carlson K, Craddock C, Rudin C, Finke J, Salles G, Kroschinsky F, Sureda A, Dreger P. Autologous stem cell transplantation for enteropathy-associated T-cell lymphoma: a retrospective study by the EBMT. Blood. 2013a;121:2529-32. Jantunen E, Canals C, Attal M, Thomson K, Milpied N, Buzyn A, Ferrant A, Biron P, Crawley C, Schattenberg A, Luan JJ, Tilly H, Rio B, Wijermans PW, Dreger P, Sureda A; Lymphoma Working Party of the European Group for Blood and Marrow Transplantation (EBMT). Autologous stem-cell transplantation in patients with mantle cell lymphoma beyond 65 years of age: a study from the European Group for Blood and Marrow Transplantation (EBMT). Ann Oncol. 2012;23:166-71.

73
Jantunen E, Fruehauf S. Importance of blood graft characteristics in auto-SCT: implications for optimizing mobilization regimens. Bone Marrow Transplant. 2011;46:627-35. Jantunen E, Kuittinen T, Mahlamäki E, Pyörälä M, Mäntymaa P, Nousiainen T. Efficacy of pre-emptively used plerixafor in patients mobilizing poorly after chemomobilization: a single centre experience. Eur J Haematol. 2011;86:299-304. Jantunen E, Kuittinen T, Nousiainen T. Is chemotherapy scoring useful to predict progenitor cell mobilisation in patients with non-Hodgkin's lymphoma? Bone Marrow Transplant. 2003b;32:569-73. Jantunen E, Kuittinen T. Blood stem cell mobilization and collection in patients with lymphoproliferative diseases: practical issues. Eur J Haematol. 2008;80:287-95. Jantunen E, Kvalheim G. Mobilization strategies in hard-to-mobilize patients with lymphoid malignancies. Eur J Haematol. 2010;85:463-71. Jantunen E, Lemoli RM. Preemptive use of plerixafor in difficult-to-mobilize patients: an emerging concept. Transfusion. 2012;52:906-14. Jantunen E, Putkonen M, Nousiainen T, Pelliniemi TT, Mahlamäki E, Remes K. Low-dose or intermediate-dose cyclophosphamide plus granulocyte colony-stimulating factor for progenitor cell mobilisation in patients with multiple myeloma. Bone Marrow Transplant. 2003a;31:347-51. Jantunen E, Sureda A. The evolving role of stem cell transplants in lymphomas. Biol Blood Marrow Transplant. 2012;18:660-73. Jantunen E, Wiklund T, Juvonen E, Putkonen M, Lehtinen T, Kuittinen O, Franssila K, Söderström KO, Leppä S, Elonen E, Remes K, Nousiainen T. Autologous stem cell transplantation in adult patients with peripheral T-cell lymphoma: a nation-wide survey. Bone Marrow Transplant. 2004;33:405-10. Jantunen E. Novel strategies for blood stem cell mobilization: special focus on plerixafor. Expert Opin Biol Ther. 2011;11:1241-8. Jantunen E, Ropponen A, Siitonen T, Niittyvuopio R, Sankelo M, Putkonen M, Varmavuo V, Pyörälä M, Kuittinen T, Silvennoinen R, Kutila A, Nihtinen A, Vasala K, Lehtonen P, Sikiö A, Valonen P, Nousiainen P, Pelkonen J, Mäntymaa P. Graft and outcome in autologous stem cell transplantation: a prospective GOA study. Bone Marrow Transplant. (Abstracts of the Annual Meeting of the European Group for Blood and Marrow Transplantation). 2013b;Abstract R1507. Johnsen HE, Rasmussen T, Knudsen LM. CD34+ subset and tumor cell quantitation by flow cytometry-step toward quality assessment of autografts in B cell malignancies. Vox Sang. 1998;74 Suppl 2:477-82. Josting A, Kàtay I, Rueffer U, Winter S, Tesch H, Engert A, Diehl V, Wickramanayake PD. Favorable outcome of patients with relapsed or refractory Hodgkin's disease treated with high-dose chemotherapy and stem cell rescue at the time of maximal response to conventional salvage therapy (Dex-BEAM). Ann Oncol. 1998;9:289-95.

74
Katayama Y, Yano T, Bessho A, Deguchi S, Sunami K, Mahmut N, Shinagawa K, Omoto E, Makino S, Miyamoto T, Mizuno S, Fukuda T, Eto T, Fujisaki T, Ohno Y, Inaba S, Niho Y, Harada M. The effects of a simplified method for cryopreservation and thawing procedures on peripheral blood stem cells. Bone Marrow Transplant. 1997;19:283-7. Katipamula R, Porrata LF, Gastineau DA, Markovic SN, Moore SB, Greiner C, Burgstaler EA, Padley DJ, Winters JL. Apheresis instrument settings influence infused absolute lymphocyte count affecting survival following autologous peripheral hematopoietic stem cell transplantation in non-Hodgkin's lymphoma: the need to optimize instrument setting and define a lymphocyte collection target. Bone Marrow Transplant. 2006;37:811-7. Keating GM. Plerixafor: a review of its use in stem-cell mobilization in patients with lymphoma or multiple myeloma. Drugs. 2011;71:1623-47. Keeney M, Chin-Yee I, Weir K, Popma J, Nayar R, Sutherland DR. Single platform flow cytometric absolute CD34+ cell counts based on the ISHAGE guidelines. International Society of Hematotherapy and Graft Engineering. Cytometry. 1998;34:61-70. Keeney M, Gratama JW, Sutherland DR. Critical role of flow cytometry in evaluating peripheral blood hematopoietic stem cell grafts. Cytometry A. 2004;58:72-5. Kerjaschki D, Sharkey DJ, Farquhar MG. Identification and characterization of podocalyxin--the major sialoprotein of the renal glomerular epithelial cell. J Cell Biol. 1984;98:1591-6. Ketterer N, Salles G, Raba M, Espinouse D, Sonet A, Tremisi P, Dumontet C, Moullet I, Eljaafari-Corbin A, Neidhardt-Berard EM, Bouafia F, Coiffier B. High CD34(+) cell counts decrease hematologic toxicity of autologous peripheral blood progenitor cell transplantation. Blood. 1998;91:3148-55. Khera N, Jinneman J, Storer BE, Heimfeld S, O'Meara MM, Chauncey TR, Lee SJ, Linenberger M. Limiting the daily total nucleated cell dose of cryopreserved peripheral blood stem cell products for autologous transplantation improves infusion-related safety with no adverse impact on hematopoietic engraftment. Biol Blood Marrow Transplant. 2012;18:220-8. Kimura Y, Ding B, Imai N, Nolan DJ, Butler JM, Rafii S. c-Kit-mediated functional positioning of stem cells to their niches is essential for maintenance and regeneration of adult hematopoiesis. PLoS One. 2011;6:e26918. Klaus J, Herrmann D, Breitkreutz I, Hegenbart U, Mazitschek U, Egerer G, Cremer FW, Lowenthal RM, Huesing J, Fruehauf S, Moehler T, Ho AD, Goldschmidt H. Effect of CD34 cell dose on hematopoietic reconstitution and outcome in 508 patients with multiple myeloma undergoing autologous peripheral blood stem cell transplantation. Eur J Haematol. 2007;78:21-8. Klingemann HG. Relevance and potential of natural killer cells in stem cell transplantation. Biol Blood Marrow Transplant. 2000;6:90-9. Kobbe G, Bruns I, Fenk R, Czibere A, Haas R. Pegfilgrastim for PBSC mobilization and autologous haematopoietic SCT. Bone Marrow Transplant. 2009;43:669-77.

75
Koç ON, Gerson SL, Cooper BW, Laughlin M, Meyerson H, Kutteh L, Fox RM, Szekely EM, Tainer N, Lazarus HM. Randomized cross-over trial of progenitor-cell mobilization: high-dose cyclophosphamide plus granulocyte colony-stimulating factor (G-CSF) versus granulocyte-macrophage colony-stimulating factor plus G-CSF. J Clin Oncol. 2000;18:1824-30. Kopf B, De Giorgi U, Vertogen B, Monti G, Molinari A, Turci D, Dazzi C, Leoni M, Tienghi A, Cariello A, Argnani M, Frassineti L, Scarpi E, Rosti G, Marangolo M. A randomized study comparing filgrastim versus lenograstim versus molgramostim plus chemotherapy for peripheral blood progenitor cell mobilization. Bone Marrow Transplant. 2006;38:407-12. Kopp HG, Yildirim S, Weisel KC, Kanz L, Vogel W. Contamination of autologous peripheral blood progenitor cell grafts predicts overall survival after high-dose chemotherapy in multiple myeloma. J Cancer Res Clin Oncol. 2009;135:637-42. Koreth J, Cutler CS, Djulbegovic B, Behl R, Schlossman RL, Munshi NC, Richardson PG, Anderson KC, Soiffer RJ, Alyea EP 3rd. High-dose therapy with single autologous transplantation versus chemotherapy for newly diagnosed multiple myeloma: A systematic review and meta-analysis of randomized controlled trials. Biol Blood Marrow Transplant. 2007;13:183-96. Krause DS, Fackler MJ, Civin CI, May WS. CD34: structure, biology, and clinical utility. Blood. 1996;87:1-13. Kuittinen T, Nousiainen T, Halonen P, Mahlamäki E, Jantunen E. Prediction of mobilisation failure in patients with non-Hodgkin's lymphoma. Bone Marrow Transplant. 2004;33:907-12. Kymes SM, Pusic I, Lambert DL, Gregory M, Carson KR, DiPersio JF. Economic evaluation of plerixafor for stem cell mobilization. Am J Manag Care. 2012;18:33-41. Körbling M, Freireich EJ. Twenty-five years of peripheral blood stem cell transplantation. Blood. 2011;117:6411-6. Lack NA, Green B, Dale DC, Calandra GB, Lee H, MacFarland RT, Badel K, Liles WC, Bridger G. A pharmacokinetic-pharmacodynamic model for the mobilization of CD34+ hematopoietic progenitor cells by AMD3100. Clin Pharmacol Ther. 2005;77:427-36. Ladetto M, De Marco F, Benedetti F, Vitolo U, Patti C, Rambaldi A, Pulsoni A, Musso M, Liberati AM, Olivieri A, Gallamini A, Pogliani E, Rota Scalabrini D, Callea V, Di Raimondo F, Pavone V, Tucci A, Cortelazzo S, Levis A, Boccadoro M, Majolino I, Pileri A, Gianni AM, Passera R, Corradini P, Tarella C; Gruppo Italiano Trapianto di Midollo Osseo (GITMO); Intergruppo Italiano Linfomi (IIL). Prospective, multicenter randomized GITMO/IIL trial comparing intensive (R-HDS) versus conventional (CHOP-R) chemoimmunotherapy in high-risk follicular lymphoma at diagnosis: the superior disease control of R-HDS does not translate into an overall survival advantage. Blood. 2008;111:4004-13. Lanza F, Campioni D, Moretti S, Dominici M, Punturieri M, Focarile E, Pauli S, Dabusti M, Tieghi A, Bacilieri M, Scapoli C, De Angeli C, Galluccio L, Castoldi G. CD34(+) cell subsets and long-term culture colony-forming cells evaluated on both autologous and normal bone marrow stroma predict long-term hematopoietic engraftment in patients undergoing autologous peripheral blood stem cell transplantation. Exp Hematol. 2001;29:1484-93.

76
Lapidot T, Dar A, Kollet O. How do stem cells find their way home? Blood. 2005;106:1901-10. Lapidot T, Kollet O. The brain-bone-blood triad: traffic lights for stem-cell homing and mobilization. Hematology Am Soc Hematol Educ Program. 2010;1-6. Lapidot T, Petit I. Current understanding of stem cell mobilization: the roles of chemokines, proteolytic enzymes, adhesion molecules, cytokines, and stromal cells. Exp Hematol. 2002;30:973-81. Larochelle A, Vormoor J, Hanenberg H, Wang JC, Bhatia M, Lapidot T, Moritz T, Murdoch B, Xiao XL, Kato I, Williams DA, Dick JE. Identification of primitive human hematopoietic cells capable of repopulating NOD/SCID mouse bone marrow: implications for gene therapy. Nat Med. 1996;2:1329-37. Lazarus HM, Rowlings PA, Zhang MJ, Vose JM, Armitage JO, Bierman PJ, Gajewski JL, Gale RP, Keating A, Klein JP, Miller CB, Phillips GL, Reece DE, Sobocinski KA, van Besien K, Horowitz MM. Autotransplants for Hodgkin's disease in patients never achieving remission: a report from the Autologous Blood and Marrow Transplant Registry. J Clin Oncol. 1999;17:534-45. Lee SE, Yahng SA, Cho BS, Eom KS, Kim YJ, Kim HJ, Lee S, Cho SG, Kim DW, Lee JW, Min WS, Park CW, Min CK. Lymphocyte subset analysis for the assessment of treatment-related complications after autologous stem cell transplantation in multiple myeloma. Cytotherapy. 2012;14:505-12. Lefrère F, Brignier AC, Elie C, Ribeil JA, Bernimoulin M, Aoun C, Dal Cortivo L, Delarue R, Hermine O, Cavazzana-Calvo M. First experience of autologous peripheral blood stem cell mobilization with biosimilar granulocyte colony-stimulating factor. Adv Ther. 2011;28:304-10. Lefrère F, Zohar S, Beaudier S, Audat F, Ribeil JA, Ghez D, Varet B, Cavazzana-Calvo M, Dal Cortivo L, Letestu R, McIntyre E, Brouzes C. Evaluation of an algorithm based on peripheral blood hematopoietic progenitor cell and CD34+ cell concentrations to optimize peripheral blood progenitor cell collection by apheresis. Transfusion. 2007;47:1851-7. Le Gouill S, De Guibert S, Planche L, Brice P, Dupuis J, Cartron G, Van Hoof A, Casasnovas O, Gyan E, Tilly H, Fruchart C, Deconinck E, Fitoussi O, Gastaud L, Delwail V, Gabarre J, Gressin R, Blanc M, Foussard C, Salles G; GELA and GOELAMS. Impact of the use of autologous stem cell transplantation at first relapse both in naive and previously rituximab exposed follicular lymphoma patients treated in the GELA/GOELAMS FL2000 study. Haematologica. 2011;96:1128-35. Lemoli RM, de Vivo A, Damiani D, Isidori A, Tani M, Bonini A, Cellini C, Curti A, Gugliotta L, Visani G, Fanin R, Baccarani M. Autologous transplantation of granulocyte colony-stimulating factor-primed bone marrow is effective in supporting myeloablative chemotherapy in patients with hematologic malignancies and poor peripheral blood stem cell mobilization. Blood. 2003;102:1595-600.

77
Lenz G, Dreyling M, Schiegnitz E, Forstpointner R, Wandt H, Freund M, Hess G, Truemper L, Diehl V, Kropff M, Kneba M, Schmitz N, Metzner B, Pfirrmann M, Unterhalt M, Hiddemann W; German Low-Grade Lymphoma Study Group. Myeloablative radiochemotherapy followed by autologous stem cell transplantation in first remission prolongs progression-free survival in follicular lymphoma: results of a prospective, randomized trial of the German Low-Grade Lymphoma Study Group. Blood. 2004;104:2667-74. Letestu R, Marzac C, Audat F, Belhocine R, Tondeur S, Baccini V, Garçon L, Cortivo LD, Perrot JY, Lefrère F, Valensi F, Ajchenbaum-Cymbalista F. Use of hematopoietic progenitor cell count on the Sysmex XE-2100 for peripheral blood stem cell harvest monitoring. Leuk Lymphoma. 2007;48:89-96. Lévesque JP, Hendy J, Takamatsu Y, Simmons PJ, Bendall LJ. Disruption of the CXCR4/CXCL12 chemotactic interaction during hematopoietic stem cell mobilization induced by GCSF or cyclophosphamide. J Clin Invest. 2003;111:187-96. Li J, Hamilton E, Vaughn L, Graiser M, Renfroe H, Lechowicz MJ, Langston A, Prichard JM, Anderson D, Gleason C, Lonial S, Flowers CR, Kaufman JL, Waller EK. Effectiveness and cost analysis of "just-in-time" salvage plerixafor administration in autologous transplant patients with poor stem cell mobilization kinetics. Transfusion. 2011;51:2175-82. Liles WC, Broxmeyer HE, Rodger E, Wood B, Hübel K, Cooper S, Hangoc G, Bridger GJ, Henson GW, Calandra G, Dale DC. Mobilization of hematopoietic progenitor cells in healthy volunteers by AMD3100, a CXCR4 antagonist. Blood. 2003;102:2728-30. Liles WC, Rodger E, Broxmeyer HE, Dehner C, Badel K, Calandra G, Christensen J, Wood B, Price TH, Dale DC. Augmented mobilization and collection of CD34+ hematopoietic cells from normal human volunteers stimulated with granulocyte-colony-stimulating factor by single-dose administration of AMD3100, a CXCR4 antagonist. Transfusion. 2005;45:295-300. Limat S, Woronoff-Lemsi MC, Milpied N, Chartrin I, Ifrah N, Deconinck E, Gressin R, Colombat P, Cahn JY, Arveux P; Groupe Ouest Est d'étude des Leucémies et Autres Maladies du Sang (GOELAMS). Effect of cell determinant (CD)34+ cell dose on the cost and consequences of peripheral blood stem cell transplantation for non-Hodgkin's lymphoma patients in front-line therapy. Eur J Cancer. 2000;36:2360-7. Lin JS, Burgstaler EA, Pineda AA, Gertz MA. Effects of whole blood flow rates on mononuclear cell yields during peripheral blood stem cell collection using Fenwal CS 3000 Plus. J Clin Apher. 1995;10:7-11. Linch DC, Winfield D, Goldstone AH, Moir D, Hancock B, McMillan A, Chopra R, Milligan D, Hudson GV. Dose intensification with autologous bone-marrow transplantation in relapsed and resistant Hodgkin's disease: results of a BNLI randomised trial. Lancet. 1993;341:1051-4. Liseth K, Abrahamsen JF, Bjørsvik S, Grøttebø K, Bruserud Ø. The viability of cryopreserved PBPC depends on the DMSO concentration and the concentration of nucleated cells in the graft. Cytotherapy. 2005;7:328-33. Liseth K, Ersvær E, Abrahamsen JF, Nesthus I, Ryningen A, Bruserud Ø. Long-term cryopreservation of autologous stem cell grafts: a clinical and experimental study of hematopoietic and immunocompetent cells. Transfusion. 2009;49:1709-19.

78
Ljungman P, Bregni M, Brune M, Cornelissen J, de Witte T, Dini G, Einsele H, Gaspar HB, Gratwohl A, Passweg J, Peters C, Rocha V, Saccardi R, Schouten H, Sureda A, Tichelli A, Velardi A, Niederwieser D; European Group for Blood and Marrow Transplantation. Allogeneic and autologous transplantation for haematological diseases, solid tumours and immune disorders: current practice in Europe 2009. Bone Marrow Transplant. 2010;45:219-34. López-Pérez R, García-Sanz R, González D, Balanzategui A, Chillón MC, Alaejos I, Mateos MV, Caballero MD, Mateo G, Nieto MJ, González M, San Miguel JF. The detection of contaminating clonal cells in apheresis products is related to response and outcome in multiple myeloma undergoing autologous peripheral blood stem cell transplantation. Leukemia. 2000;14:1493-9. Lymperi S, Ferraro F, Scadden DT. The HSC niche concept has turned 31. Has our knowledge matured? Ann N Y Acad Sci. 2010;1192:12-8. Mansour A, Abou-Ezzi G, Sitnicka E, Jacobsen SE, Wakkach A, Blin-Wakkach C. Osteoclasts promote the formation of hematopoietic stem cell niches in the bone marrow. J Exp Med. 2012;209:537-49. Martin C, Bridger GJ, Rankin SM. Structural analogues of AMD3100 mobilise haematopoietic progenitor cells from bone marrow in vivo according to their ability to inhibit CXCL12 binding to CXCR4 in vitro. Br J Haematol. 2006;134:326-9. McCredie KB, Hersh EM, Freireich EJ. Cells capable of colony formation in the peripheral blood of man. Science. 1971;171:293-4. Méndez-Ferrer S, Michurina TV, Ferraro F, Mazloom AR, Macarthur BD, Lira SA, Scadden DT, Ma'ayan A, Enikolopov GN, Frenette PS. Mesenchymal and haematopoietic stem cells form a unique bone marrow niche. Nature. 2010;466:829-34. Mendrone A Jr, Arrais CA, Saboya R, Chamone Dde A, Dulley FL. Factors affecting hematopoietic progenitor cell mobilization: an analysis of 307 patients. Transfus Apher Sci. 2008;39:187-92. Menéndez P, Caballero MD, Prosper F, Del Cañizo MC, Pérez-Simón JA, Mateos MV, Nieto MJ, Corral M, Romero M, García-Conde J, Montalbán MA, San Miguel JF, Orfao A. The composition of leukapheresis products impacts on the hematopoietic recovery after autologous transplantation independently of the mobilization regimen. Transfusion. 2002;42:1159-72. Micallef IN, Apostolidis J, Rohatiner AZ, Wiggins C, Crawley CR, Foran JM, Leonhardt M, Bradburn M, Okukenu E, Salam A, Matthews J, Cavenagh JD, Gupta RK, Lister TA. Factors which predict unsuccessful mobilisation of peripheral blood progenitor cells following G-CSF alone in patients with non-Hodgkin's lymphoma. Hematol J. 2000;1:367-73. Micallef IN, Sinha S, Gastineau DA, Wolf R, Inwards DJ, Gertz MA, Hayman SR, Hogan WJ, Johnston PB, Lacy MQ, Ansell SM, Buadi F, Dingli D, Dispenzieri A, Litzow MR, Porrata LF, Winters JL, Kumar S. Cost-effectiveness analysis of a risk-adapted algorithm of plerixafor use for autologous peripheral blood stem cell mobilization. Biol Blood Marrow Transplant. 2013;19:87-93.

79
Micallef IN, Stiff PJ, DiPersio JF, Maziarz RT, McCarty JM, Bridger G, Calandra G. Successful stem cell remobilization using plerixafor (Mozobil) plus granulocyte colony-stimulating factor in patients with non-Hodgkin lymphoma: results from the plerixafor NHL phase 3 study rescue protocol. Biol Blood Marrow Transplant. 2009;15:1578-86. Miller JS, McCullar V, Punzel M, Lemischka IR, Moore KA. Single adult human CD34(+)/Lin-/CD38(-) progenitors give rise to natural killer cells, B-lineage cells, dendritic cells, and myeloid cells. Blood. 1999;93:96-106. Milone G, Tripepi G, Martino M, Ancora F, Bartolozzi B, Spadaro A, Nozzoli C, La Fauci A, Amico I, Leotta S, Poidomani M, Irrera G, Iacopino P, Saccardi R, Guidi S, Bosi A. Early measurement of CD34+ cells in peripheral blood after cyclophosphamide and granulocyte colony-stimulating factor treatment predicts later CD34+ mobilisation failure and is a possible criterion for guiding "on demand" use of plerixafor. Blood Transfus. 2013;11:94-101. Milpied N, Deconinck E, Gaillard F, Delwail V, Foussard C, Berthou C, Gressin R, Lucas V, Colombat P, Harousseau JL; Groupe Ouest-Est des Leucémies et des Autres Maladies du Sang. Initial treatment of aggressive lymphoma with high-dose chemotherapy and autologous stem-cell support. N Engl J Med. 2004;350:1287-95. Mohty M, Ho AD. In and out of the niche: perspectives in mobilization of hematopoietic stem cells. Exp Hematol. 2011;39:723-9. Montoto S, Canals C, Rohatiner AZ, Taghipour G, Sureda A, Schmitz N, Gisselbrecht C, Fouillard L, Milpied N, Haioun C, Slavin S, Conde E, Fruchart C, Ferrant A, Leblond V, Tilly H, Lister TA, Goldstone AH; EBMT Lymphoma Working Party. Long-term follow-up of high-dose treatment with autologous haematopoietic progenitor cell support in 693 patients with follicular lymphoma: an EBMT registry study. Leukemia. 2007;21:2324-31. Moog R. Management strategies for poor peripheral blood stem cell mobilization. Transfus Apher Sci. 2008;38:229-36. Moreb JS, Salmasinia D, Hsu J, Hou W, Cline C, Rosenau E. Long-term outcome after autologous stem cell transplantation with adequate peripheral blood stem cell mobilization using plerixafor and G-CSF in poor mobilizer lymphoma and myeloma patients. Adv Hematol. 2011;2011:517561. Moskowitz CH, Nimer SD, Zelenetz AD, Trippett T, Hedrick EE, Filippa DA, Louie D, Gonzales M, Walits J, Coady-Lyons N, Qin J, Frank R, Bertino JR, Goy A, Noy A, O'Brien JP, Straus D, Portlock CS, Yahalom J. A 2-step comprehensive high-dose chemoradiotherapy second-line program for relapsed and refractory Hodgkin disease: analysis by intent to treat and development of a prognostic model. Blood. 2001;97:616-23. Motabi IH, DiPersio JF. Advances in stem cell mobilization. Blood Rev. 2012;26:267-78. Möhle R, Pförsich M, Fruehauf S, Witt B, Krämer A, Haas R. Filgrastim post-chemotherapy mobilizes more CD34+ cells with a different antigenic profile compared with use during steady-state hematopoiesis. Bone Marrow Transplant. 1994;14:827-32. Motorin D, Bakken A, Foss Abrahamsen J, Ernst P, Bruserud Ø. Characterization of clonogenic progenitors in autologous peripheral blood stem cell grafts: evaluation of a simple in vitro assay suitable for routine clinical use. Hematology. 2003;8:313-8.

80
Nademanee AP, DiPersio JF, Maziarz RT, Stadtmauer EA, Micallef IN, Stiff PJ, Hsu FJ, Bridger G, Bolwell BJ. Plerixafor plus granulocyte colony-stimulating factor versus placebo plus granulocyte colony-stimulating factor for mobilization of CD34(+) hematopoietic stem cells in patients with multiple myeloma and low peripheral blood CD34(+) cell count: results of a subset analysis of a randomized trial. Biol Blood Marrow Transplant. 2012;18:1564-72. Nagasawa T, Omatsu Y, Sugiyama T. Control of hematopoietic stem cells by the bone marrow stromal niche: the role of reticular cells. Trends Immunol. 2011;32:315-20. Nagasawa T, Tachibana K, Kishimoto T. A novel CXC chemokine PBSF/SDF-1 and its receptor CXCR4: their functions in development, hematopoiesis and HIV infection. Semin Immunol. 1998;10:179-85. Naveiras O, Nardi V, Wenzel PL, Hauschka PV, Fahey F, Daley GQ. Bone-marrow adipocytes as negative regulators of the haematopoietic microenvironment. Nature. 2009;460:259-63. Narayanasami U, Kanteti R, Morelli J, Klekar A, Al-Olama A, Keating C, O'Connor C, Berkman E, Erban JK, Sprague KA, Miller KB, Schenkein DP. Randomized trial of filgrastim versus chemotherapy and filgrastim mobilization of hematopoietic progenitor cells for rescue in autologous transplantation. Blood. 2001;98:2059-64. Nielsen JS, McNagny KM. Novel functions of the CD34 family. J Cell Sci. 2008;121:3683-92. Ninan MJ, Flowers CR, Roback JD, Arellano ML, Waller EK. Posttransplant thrombopoiesis predicts survival in patients undergoing autologous hematopoietic progenitor cell transplantation. Biol Blood Marrow Transplant. 2007;13:895-904. Nervi B, Ramirez P, Rettig MP, Uy GL, Holt MS, Ritchey JK, Prior JL, Piwnica-Worms D, Bridger G, Ley TJ, DiPersio JF. Chemosensitization of acute myeloid leukemia (AML) following mobilization by the CXCR4 antagonist AMD3100. Blood. 2009;113:6206-14. Ojeda-Uribe M, Sovalat H, Bourderont D, Brunot A, Marr A, Lewandowski H, Chabouté V, Peter P, Henon P. Peripheral blood and BM CD34+ CD38- cells show better resistance to cryopreservation than CD34+ CD38+ cells in autologous stem cell transplantation. Cytotherapy. 2004;6:571-83. Olivieri A, Marchetti M, Lemoli R, Tarella C, Iacone A, Lanza F, Rambaldi A, Bosi A; Italian Group for Stem Cell Transplantation. Proposed definition of 'poor mobilizer' in lymphoma and multiple myeloma: an analytic hierarchy process by ad hoc working group Gruppo ItalianoTrapianto di Midollo Osseo. Bone Marrow Transplant. 2012;47:342-51. O'Shea D, Giles C, Terpos E, Perz J, Politou M, Sana V, Naresh K, Lampert I, Samson D, Narat S, Kanfer E, Olavarria E, Apperley JF, Rahemtulla A. Predictive factors for survival in myeloma patients who undergo autologous stem cell transplantation: a single-centre experience in 211 patients. Bone Marrow Transplant. 2006;37:731-7. Ozsan GH, Micallef IN, Dispenzieri A, Kumar S, Lacy MQ, Dingli D, Hayman SR, Buadi FK, Wolf RC, Gastineau DA, Hogan WJ, Gertz MA. Hematopoietic recovery kinetics predicts for poor CD34+ cell mobilization after cyclophosphamide chemotherapy in multiple myeloma. Am J Hematol. 2012;87:1-4.

81
Pamphilon D, Mijovic A. Storage of hemopoietic stem cells. Asian J Transfus Sci. 2007;1:71-6. Pasino M, Lanza T, Marotta F, Scarso L, De Biasio P, Amato S, Corcione A, Pistoia V, Mori PG. Flow cytometric and functional characterization of AC133+ cells from human umbilical cord blood. Br J Haematol. 2000;108:793-800. Passweg JR, Baldomero H, Bregni M, Cesaro S, Dreger P, Duarte RF, Falkenburg JH, Kröger N, Farge-Bancel D, Bobby Gaspar H, Marsh J, Mohty M, Peters C, Sureda A, Velardi A, Ruiz de Elvira C, Madrigal A. Hematopoietic SCT in Europe: data and trends in 2011. Bone Marrow Transplant. 2013;48:1161-7. Pavone V, Gaudio F, Console G, Vitolo U, Iacopino P, Guarini A, Liso V, Perrone T, Liso A. Poor mobilization is an independent prognostic factor in patients with malignant lymphomas treated by peripheral blood stem cell transplantation. Bone Marrow Transplant. 2006;37:719-24. Pelus LM, Fukuda S. Peripheral blood stem cell mobilization: the CXCR2 ligand GRObeta rapidly mobilizes hematopoietic stem cells with enhanced engraftment properties. Exp Hematol. 2006;34:1010-20. Percy LA, Moore SE, Qian W, Dorman J, Rabin N, Watts M, Linch DC, Yong KL. Re-infused lymphocyte dose does not influence disease control following upfront autologous stem cell transplantation for multiple myeloma. Br J Haematol. 2012;157:494-6. Perkins JB, Shapiro JF, Bookout RN, Yee GC, Anasetti C, Janssen WE, Fernandez HF. Retrospective comparison of filgrastim plus plerixafor to other regimens for remobilization after primary mobilization failure: clinical and economic outcomes. Am J Hematol. 2012;87:673-7. Petrucci MT, Avvisati G, La Verde G, De Fabritiis P, Ribersani M, Palumbo G, De Felice L, Rusignuolo A, Simone F, Meloni G, Mandelli F. Intermediate-dose cyclophosphamide and granulocyte colony-stimulating factor is a valid alternative to high-dose cyclophosphamide for mobilizing peripheral blood CD34+ cells in patients with multiple myeloma. Acta Haematol. 2003;109:184-8. Philip T, Guglielmi C, Hagenbeek A, Somers R, Van der Lelie H, Bron D, Sonneveld P, Gisselbrecht C, Cahn JY, Harousseau JL, et al. Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy-sensitive non-Hodgkin's lymphoma. N Engl J Med. 1995;333:1540-5. Piccirillo N, Vacca M, Lanti A, Ipsevich F, Maresca M, Fiorelli E, Bianchi M, Adorno G, Pierelli L, Majolino I, Leone G, Zini G. Poor mobilizer: a retrospective study on proven and predicted incidence according to GITMO criteria. Transfus Apher Sci. 2012;47:217-21. Pierelli L, Fioravanti D, Patti D, Iudicone P, Scocchera R, Pandolfi A, Nuti M. Counting of leukocytes in samples from G-CSF mobilized donors, leukapheresis products, and cord blood: the performances of an analyzer with dedicated profiles. Int J Lab Hematol. 2012;34:154-63. Porrata LF, Gertz MA, Inwards DJ, Litzow MR, Lacy MQ, Tefferi A, Gastineau DA, Dispenzieri A, Ansell SM, Micallef IN, Geyer SM, Markovic SN. Early lymphocyte recovery predicts superior survival after autologous hematopoietic stem cell transplantation in multiple myeloma or non-Hodgkin lymphoma. Blood. 2001;98:579-85.

82
Porrata LF, Gastineau DA, Padley D, Bundy K, Markovic SN. Re-infused autologous graft natural killer cells correlates with absolute lymphocyte count recovery after autologous stem cell transplantation. Leuk Lymphoma. 2003;44:997-1000. Porrata LF, Gertz MA, Geyer SM, Litzow MR, Gastineau DA, Moore SB, Pineda AA, Bundy KL, Padley DJ, Persky D, Lacy MQ, Dispenzieri A, Snow DS, Markovic SN. The dose of infused lymphocytes in the autograft directly correlates with clinical outcome after autologous peripheral blood hematopoietic stem cell transplantation in multiple myeloma. Leukemia. 2004a;18:1085-92. Porrata LF, Inwards DJ, Ansell SM, Micallef IN, Johnston PB, Gastineau DA, Litzow MR, Winters JL, Markovic SN. Early lymphocyte recovery predicts superior survival after autologous stem cell transplantation in non-Hodgkin lymphoma: a prospective study. Biol Blood Marrow Transplant. 2008;14:807-16. Porrata LF, Litzow MR, Inwards DJ, Gastineau DA, Moore SB, Pineda AA, Bundy KL, Padley DJ, Persky D, Ansell SM, Micallef IN, Markovic SN. Infused peripheral blood autograft absolute lymphocyte count correlates with day 15 absolute lymphocyte count and clinical outcome after autologous peripheral hematopoietic stem cell transplantation in non-Hodgkin's lymphoma. Bone Marrow Transplant. 2004b;33:291-8. Porrata LF, Markovic SN. Timely reconstitution of immune competence affects clinical outcome following autologous stem cell transplantation. Clin Exp Med. 2004;4:78-85. Price TH, Dale DC. Neutrophil transfusion: effect of storage and of collection method of neutrophil blood kinetics. Blood. 1978;51:789-98. Pusic I, Jiang SY, Landua S, Uy GL, Rettig MP, Cashen AF, Westervelt P, Vij R, Abboud CN, Stockerl-Goldstein KE, Sempek DS, Smith AL, DiPersio JF. Impact of mobilization and remobilization strategies on achieving sufficient stem cell yields for autologous transplantation. Biol Blood Marrow Transplant. 2008;14:1045-56. Putkonen M, Rauhala A, Pelliniemi TT, Remes K. Single-dose pegfilgrastim is comparable to daily filgrastim in mobilizing peripheral blood stem cells: a case-matched study in patients with lymphoproliferative malignancies. Ann Hematol. 2009;88:673-80. Rancea M, Monsef I, von Tresckow B, Engert A, Skoetz N. High-dose chemotherapy followed by autologous stem cell transplantation for patients with relapsed/refractory Hodgkin lymphoma. Cochrane Database Syst Rev. 2013;6:CD009411. Ramirez P, Rettig MP, Uy GL, Deych E, Holt MS, Ritchey JK, DiPersio JF. BIO5192, a small molecule inhibitor of VLA-4, mobilizes hematopoietic stem and progenitor cells. Blood. 2009;114:1340-3. Ramsfjell V, Borge OJ, Cui L, Jacobsen SE. Thrombopoietin directly and potently stimulates multilineage growth and progenitor cell expansion from primitive (CD34+ CD38-) human bone marrow progenitor cells: distinct and key interactions with the ligands for c-kit and flt3, and inhibitory effects of TGF-beta and TNF-alpha. J Immunol. 1997;158:5169-77. Reich-Slotky R, Colovai AI, Semidei-Pomales M, Patel N, Cairo M, Jhang J, Schwartz J. Determining post-thaw CD34+ cell dose of cryopreserved haematopoietic progenitor cells demonstrates high recovery and confirms their integrity. Vox Sang. 2008;94:351-7.

83
Reimer P, Rüdiger T, Geissinger E, Weissinger F, Nerl C, Schmitz N, Engert A, Einsele H, Müller-Hermelink HK, Wilhelm M. Autologous stem-cell transplantation as first-line therapy in peripheral T-cell lymphomas: results of a prospective multicenter study. J Clin Oncol. 2009;27:106-13. Remes K, Itälä M, Kauppila M, Pelliniemi TT, Rajamäki A. Autologous blood cell transplantation in multiple myeloma: impact of CD34+ cell selection with long follow-up. J Hematother Stem Cell Res. 2003;12:63-70. Remes K, Matinlauri I, Grenman S, Itälä M, Kauppila M, Pelliniemi TT, Salminen E, Vanharanta R, Rajamäki A. Daily measurements of blood CD34+ cells after stem cell mobilization predict stem cell yield and posttransplant hematopoietic recovery. J Hematother. 1997;6:13-9. Rettig MP, Ansstas G, DiPersio JF. Mobilization of hematopoietic stem and progenitor cells using inhibitors of CXCR4 and VLA-4. Leukemia. 2012;26:34-53. Richman CM, Weiner RS, Yankee RA. Increase in circulating stem cells following chemotherapy in man. Blood. 1976;47:1031-9. Richman CM. Prolonged cryopreservation of human granulocytes. Transfusion. 1983;23:508-11. Rick O, Beyer J, Kingreen D, Kühl JS, Zingsem J, Huhn D, Siegert W, Schwella N. Successful autologous bone marrow rescue in patients who failed peripheral blood stem cell mobilization. Ann Hematol. 2000;79:681-6. Rodriguez J, Munsell M, Yazji S, Hagemeister FB, Younes A, Andersson B, Giralt S, Gajewski J, de Lima M, Couriel D, Romaguera J, Cabanillas FF, Champlin RE, Khouri IF. Impact of high-dose chemotherapy on peripheral T-cell lymphomas. J Clin Oncol. 2001;19:3766-70. Rohatiner AZ, Nadler L, Davies AJ, Apostolidis J, Neuberg D, Matthews J, Gribben JG, Mauch PM, Lister TA, Freedman AS. Myeloablative therapy with autologous bone marrow transplantation for follicular lymphoma at the time of second or subsequent remission: long-term follow-up. J Clin Oncol. 2007;25:2554-9. Rowley SD, Bensinger WI, Gooley TA, Buckner CD. Effect of cell concentration on bone marrow and peripheral blood stem cell cryopreservation. Blood. 1994;83(9):2731-6. Russell N, Mesters R, Schubert J, Boogaerts M, Johnsen HE, Canizo CD, Baker N, Barker P, Skacel T, Schmitz N. A phase 2 pilot study of pegfilgrastim and filgrastim for mobilizing peripheral blood progenitor cells in patients with non-Hodgkin's lymphoma receiving chemotherapy. Haematologica. 2008;93:405-12. Rusten LS, Jacobsen SE, Kaalhus O, Veiby OP, Funderud S, Smeland EB. Functional differences between CD38- and DR- subfractions of CD34+ bone marrow cells. Blood. 1994;84:1473-81. Röllig C, Babatz J, Wagner I, Maiwald A, Schwarze V, Ehninger G, Bornhäuser M. Thawing of cryopreserved mobilized peripheral blood--comparison between waterbath and dry warming device. Cytotherapy. 2002;4:551-5.

84
Sánchez-Salinas A, Cabañas-Perianes V, Blanquer M, Majado MJ, Insausti CL, Monserrat J, Sánchez-Ibáñez MV, Menchón P, García-Hernández A, Gómez-Espuch J, Morales A, Moraleda JM. An automatic wash method for dimethyl sulfoxide removal in autologous hematopoietic stem cell transplantation decreases the adverse effects related to infusion. Transfusion. 2012;52:2382-6. Sancho JM, Morgades M, Grifols JR, Juncà J, Guardia R, Vives S, Ferrà C, Batlle M, Ester A, Gallardo D, Millà F, Feliu E, Ribera JM. Predictive factors for poor peripheral blood stem cell mobilization and peak CD34(+) cell count to guide pre-emptive or immediate rescue mobilization. Cytotherapy. 2012;14:823-9. Sartor MM, Garvin F, Antonenas V, Bradstock KF, Gottlieb DJ. Failure to achieve a threshold dose of CD34+ CD110+ progenitor cells in the graft predicts delayed platelet engraftment after autologous stem cell transplantation. Bone Marrow Transplant. 2007;40:851-7. Sassetti C, Van Zante A, Rosen SD. Identification of endoglycan, a member of the CD34/podocalyxin family of sialomucins. J Biol Chem. 2000;275:9001-10. Schmid I, Uittenbogaart CH, Giorgi JV. Sensitive method for measuring apoptosis and cell surface phenotype in human thymocytes by flow cytometry. Cytometry. 1994;15:12-20. Schmidmaier R, Oversohl N, Schnabel B, Straka C, Emmerich B. Helper T cells (CD3 + /CD4 + ) within the autologous peripheral blood stem cell graft positively correlate with event free survival of multiple myeloma patients. Exp Oncol. 2008;30:240-3. Schmitz N, Glass B, Dreger P, Haferlach T, Horst HA, Ollech-Chwoyka J, Suttorp M, Gassmann W, Löffler H. High-dose chemotherapy and hematopoietic stem cell rescue in patients with relapsed Hodgkin's disease. Ann Hematol. 1993;66:251-6. Schmitz N, Linch DC, Dreger P, Goldstone AH, Boogaerts MA, Ferrant A, Demuynck HM, Link H, Zander A, Barge A. Randomised trial of filgrastim-mobilised peripheral blood progenitor cell transplantation versus autologous bone-marrow transplantation in lymphoma patients. Lancet. 1996;347:353-7. Schmitz N, Pfistner B, Sextro M, Sieber M, Carella AM, Haenel M, Boissevain F, Zschaber R, Müller P, Kirchner H, Lohri A, Decker S, Koch B, Hasenclever D, Goldstone AH, Diehl V; German Hodgkin's Lymphoma Study Group; Lymphoma Working Party of the European Group for Blood and Marrow Transplantation. Aggressive conventional chemotherapy compared with high-dose chemotherapy with autologous haemopoietic stem-cell transplantation for relapsed chemosensitive Hodgkin's disease: a randomised trial. Lancet. 2002;359:2065-71. Schols D, Esté JA, Henson G, De Clercq E. Bicyclams, a class of potent anti-HIV agents, are targeted at the HIV coreceptor fusin/CXCR-4. Antiviral Res. 1997a;35:147-56. Schols D, Struyf S, Van Damme J, Esté JA, Henson G, De Clercq E. Inhibition of T-tropic HIV strains by selective antagonization of the chemokine receptor CXCR4. J Exp Med. 1997b;186:1383-8.

85
Schouten HC, Qian W, Kvaloy S, Porcellini A, Hagberg H, Johnsen HE, Doorduijn JK, Sydes MR, Kvalheim G. High-dose therapy improves progression-free survival and survival in relapsed follicular non-Hodgkin's lymphoma: results from the randomized European CUP trial. J Clin Oncol. 2003;21:3918-27. Schulman KA, Birch R, Zhen B, Pania N, Weaver CH. Effect of CD34(+) cell dose on resource utilization in patients after high-dose chemotherapy with peripheral-blood stem-cell support. J Clin Oncol. 1999;17:1227. Schuurhuis GJ, Muijen MM, Oberink JW, de Boer F, Ossenkoppele GJ, Broxterman HJ. Large populations of non-clonogenic early apoptotic CD34-positive cells are present in frozen-thawed peripheral blood stem cell transplants. Bone Marrow Transplant. 2001;27:487-98. Schwartzberg PL, Mueller KL, Qi H, Cannons JL. SLAM receptors and SAP influence lymphocyte interactions, development and function. Nat Rev Immunol. 2009;9:39-46. Sebban C, Mounier N, Brousse N, Belanger C, Brice P, Haioun C, Tilly H, Feugier P, Bouabdallah R, Doyen C, Salles G, Coiffier B. Standard chemotherapy with interferon compared with CHOP followed by high-dose therapy with autologous stem cell transplantation in untreated patients with advanced follicular lymphoma: the GELF-94 randomized study from the Groupe d'Etude des Lymphomes de l'Adulte (GELA). Blood. 2006;108:2540-4. Segeren CM, Sonneveld P, van der Holt B, Vellenga E, Croockewit AJ, Verhoef GE, Cornelissen JJ, Schaafsma MR, van Oers MH, Wijermans PW, Fibbe WE, Wittebol S, Schouten HC, van Marwijk Kooy M, Biesma DH, Baars JW, Slater R, Steijaert MM, Buijt I, Lokhorst HM; Dutch-Belgian Hemato-Oncology Cooperative Study Group. Overall and event-free survival are not improved by the use of myeloablative therapy following intensified chemotherapy in previously untreated patients with multiple myeloma: a prospective randomized phase 3 study. Blood. 2003;101:2144-51. Selleslag D, Dierickx D, Breems DA, Huynh P, Van De Velde A, Meers S, Brouwer E, Mertens A. Plerixafor in poor stem cell mobilizers: the Belgian Compassionate Use Program. Acta Clin Belg. 2011;66:200-4. Shaughnessy P, Islas-Ohlmayer M, Murphy J, Hougham M, MacPherson J, Winkler K, Silva M, Steinberg M, Matous J, Selvey S, Maris M, McSweeney PA. Cost and clinical analysis of autologous hematopoietic stem cell mobilization with G-CSF and plerixafor compared to G-CSF and cyclophosphamide. Biol Blood Marrow Transplant. 2011;17:729-36. Shaughnessy P, Uberti J, Devine S, Maziarz RT, Vose J, Micallef I, Jacobsen E, McCarty J, Stiff P, Artz A, Ball ED, Berryman R, Dugan M, Joyce R, Hsu FJ, Johns D, McSweeney P. Plerixafor and G-CSF for autologous stem cell mobilization in patients with NHL, Hodgkin's lymphoma and multiple myeloma: results from the expanded access program. Bone Marrow Transplant. 2013;48:777-81. Sheikhzadeh S, Hammers HJ, Hartwig D, Kirchner H, Schlenke P. Improvement of the precision in CFU-GM and BFU-E counting by flow cytometry-based standardization of short-term culture assays. J Hematother Stem Cell Res. 2001;10:881-5. Siena S, Bregni M, Brando B, Belli N, Ravagnani F, Gandola L, Stern AC, Lansdorp PM, Bonadonna G, Gianni AM. Flow cytometry for clinical estimation of circulating hematopoietic progenitors for autologous transplantation in cancer patients. Blood. 1991;77:400-9.

86
Siena S, Schiavo R, Pedrazzoli P, Carlo-Stella C. Therapeutic relevance of CD34 cell dose in blood cell transplantation for cancer therapy. J Clin Oncol. 2000;18:1360-77. Simona B, Cristina R, Luca N, Sara S, Aleksandra B, Paola B, Federica G, Pierluigi A, Laura O, Simona S, Jessica Q, Mara N, Giovanni M. A single dose of pegfilgrastim versus daily filgrastim to evaluate the mobilization and the engraftment of autologous peripheral hematopoietic progenitors in malignant lymphoma patients candidate for high-dose chemotherapy. Transfus Apher Sci. 2010;43:321-6. Sinha S, Gastineau D, Micallef I, Hogan W, Ansell S, Buadi F, Dingli D, Dispenzieri A, Gertz M, Greiner C, Hayman S, Inwards D, Johnston P, Lacy M, Litzow M, Porrata L, Winters JL, Kumar S. Predicting PBSC harvest failure using circulating CD34 levels: developing target-based cutoff points for early intervention. Bone Marrow Transplant. 2011;46:943-9. Sinitsyn Y, Malone A, Mandeli J, Grosskreutz C, Osman K, Scigliano E, Shi P, Isola L. Combined bone marrow and peripheral blood progenitor cell autografts for patients with poor mobilization. Cytotherapy. 2009;11:457-63. Smagur A, Mitrus I, Giebel S, Sadus-Wojciechowska M, Najda J, Kruzel T, Czerw T, Gliwinska J, Prokop M, Glowala-Kosinska M, Chwieduk A, Holowiecki J. Impact of different dimethyl sulphoxide concentrations on cell recovery, viability and clonogenic potential of cryopreserved peripheral blood hematopoietic stem and progenitor cells. Vox Sang. 2013;104:240-7. Smith TJ, Hillner BE, Schmitz N, Linch DC, Dreger P, Goldstone AH, Boogaerts MA, Ferrant A, Link H, Zander A, Yanovich S, Kitchin R, Erder MH. Economic analysis of a randomized clinical trial to compare filgrastim-mobilized peripheral-blood progenitor-cell transplantation and autologous bone marrow transplantation in patients with Hodgkin's and non-Hodgkin's lymphoma. J Clin Oncol. 1997;15:5-10. Smith-Berdan S, Nguyen A, Hassanein D, Zimmer M, Ugarte F, Ciriza J, Li D, García-Ojeda ME, Hinck L, Forsberg EC. Robo4 cooperates with CXCR4 to specify hematopoietic stem cell localization to bone marrow niches. Cell Stem Cell. 2011;8:72-83. Sonneveld P, van der Holt B, Segeren CM, Vellenga E, Croockewit AJ, Verhoe GE, Cornelissen JJ, Schaafsma MR, van Oers MH, Wijermans PW, Westveer PH, Lokhorst HM; Dutch-Belgian Hemato-Oncology Cooperative Group (HOVON). Intermediate-dose melphalan compared with myeloablative treatment in multiple myeloma: long-term follow-up of the Dutch Cooperative Group HOVON 24 trial. Haematologica. 2007;92:928-35. Sorensen BS, Thomsen AM, Moller BK. Collection of peripheral blood progenitor cells for autologous use: performance enhancements of COBE Spectra, auto-PBSC. J Clin Apher. 2011;26:307-14. Stewart AK, Vescio R, Schiller G, Ballester O, Noga S, Rugo H, Freytes C, Stadtmauer E, Tarantolo S, Sahebi F, Stiff P, Meharchard J, Schlossman R, Brown R, Tully H, Benyunes M, Jacobs C, Berenson R, White M, DiPersio J, Anderson KC, Berenson J. Purging of autologous peripheral-blood stem cells using CD34 selection does not improve overall or progression-free survival after high-dose chemotherapy for multiple myeloma: results of a multicenter randomized controlled trial. J Clin Oncol. 2001;19:3771-9.

87
Stewart DA, Smith C, MacFarland R, Calandra G. Pharmacokinetics and pharmacodynamics of plerixafor in patients with non-Hodgkin lymphoma and multiple myeloma. Biol Blood Marrow Transplant. 2009;15:39-46. Stiff P, Micallef I, McCarthy P, Magalhaes-Silverman M, Weisdorf D, Territo M, Badel K, Calandra G. Treatment with plerixafor in non-Hodgkin's lymphoma and multiple myeloma patients to increase the number of peripheral blood stem cells when given a mobilizing regimen of G-CSF: implications for the heavily pretreated patient. Biol Blood Marrow Transplant. 2009;15:249-56. Stiff PJ, Micallef I, Nademanee AP, Stadtmauer EA, Maziarz RT, Bolwell BJ, Bridger G, Marulkar S, Hsu FJ, DiPersio JF. Transplanted CD34(+) cell dose is associated with long-term platelet count recovery following autologous peripheral blood stem cell transplant in patients with non-Hodgkin lymphoma or multiple myeloma. Biol Blood Marrow Transplant. 2011;17:1146-53. Stockerl-Goldstein KE, Reddy SA, Horning SF, Blume KG, Chao NF, Hu WW, Johnston LF, Long GD, Strober S, Wong RM, Feiner RH, Kobler S, Negrin RS. Favorable treatment outcome in non-Hodgkin's lymphoma patients with "poor" mobilization of peripheral blood progenitor cells. Biol Blood Marrow Transplant. 2000;6:506-12. Sugiyama T, Kohara H, Noda M, Nagasawa T. Maintenance of the hematopoietic stem cell pool by CXCL12-CXCR4 chemokine signaling in bone marrow stromal cell niches. Immunity. 2006;25:977-88. Sutherland DR, Anderson L, Keeney M, Nayar R, Chin-Yee I. The ISHAGE guidelines for CD34+ cell determination by flow cytometry. International Society of Hematotherapy and Graft Engineering. J Hematother. 1996;5:213-26. Syme R, Bewick M, Stewart D, Porter K, Chadderton T, Glück S. The role of depletion of dimethyl sulfoxide before autografting: on hematologic recovery, side effects, and toxicity. Biol Blood Marrow Transplant. 2004;10:135-41. Szmant HH. Physical properties of dimethyl sulfoxide and its function in biological systems. Ann N Y Acad Sci. 1975;243:20-3. Talmadge JE, Reed EC, Kessinger A, Kuszynski CA, Perry GA, Gordy CL, Mills KC, Thomas ML, Pirruccello SJ, Letheby BA, Arneson MA, Jackson JD. Immunologic attributes of cytokine mobilized peripheral blood stem cells and recovery following transplantation. Bone Marrow Transplant. 1996;17:101-9. Tanhehco YC, Adamski J, Sell M, Cunningham K, Eisenmann C, Magee D, Stadtmauer EA, O'Doherty U. Plerixafor mobilization leads to a lower ratio of CD34+ cells to total nucleated cells which results in greater storage costs. J Clin Apher. 2010;25:202-8. Taubert I, Saffrich R, Zepeda-Moreno A, Hellwig I, Eckstein V, Bruckner T, Ho AD, Wuchter P. Characterization of hematopoietic stem cell subsets from patients with multiple myeloma after mobilization with plerixafor. Cytotherapy. 2011;13:459-66. Tedder RS, Zuckerman MA, Goldstone AH, Hawkins AE, Fielding A, Briggs EM, Irwin D, Blair S, Gorman AM, Patterson KG, Linch DC, Heptonstall J, Brink NS. Hepatitis B transmission from contaminated cryopreservation tank. Lancet. 1995;346:137–40.

88
Terstappen LW, Huang S, Safford M, Lansdorp PM, Loken MR. Sequential generations of hematopoietic colonies derived from single nonlineage-committed CD34+CD38- progenitor cells. Blood. 1991;77:1218-27. Thomas J, Liu F, Link DC. Mechanisms of mobilization of hematopoietic progenitors with granulocyte colony-stimulating factor. Curr Opin Hematol. 2002;9:183-9. Tijssen MR, Woelders H, de Vries-van Rossen A, van der Schoot CE, Voermans C, Lagerberg JW. Improved postthaw viability and in vitro functionality of peripheral blood hematopoietic progenitor cells after cryopreservation with a theoretically optimized freezing curve. Transfusion. 2008;48:893-901. To LB, Levesque JP, Herbert KE. How I treat patients who mobilize hematopoietic stem cells poorly. Blood. 2011;118:4530-40. To LB, Shepperd KM, Haylock DN, Dyson PG, Charles P, Thorp DL, Dale BM, Dart GW, Roberts MM, Sage RE, Juttner CA. Single high doses of cyclophosphamide enable the collection of high numbers of hemopoietic stem cells from the peripheral blood. Exp Hematol. 1990;18:442-7. von Tresckow B, Engert A. The role of autologous transplantation in Hodgkin lymphoma. Curr Hematol Malig Rep. 2011;6:172-9. Tricot G, Cottler-Fox MH, Calandra G. Safety and efficacy assessment of plerixafor in patients with multiple myeloma proven or predicted to be poor mobilizers, including assessment of tumor cell mobilization. Bone Marrow Transplant. 2010;45:63-8. Tricot G, Jagannath S, Vesole D, Nelson J, Tindle S, Miller L, Cheson B, Crowley J, Barlogie B. Peripheral blood stem cell transplants for multiple myeloma: identification of favorable variables for rapid engraftment in 225 patients. Blood. 1995;85:588-96. Uy GL, Rettig MP, Motabi IH, McFarland K, Trinkaus KM, Hladnik LM, Kulkarni S, Abboud CN, Cashen AF, Stockerl-Goldstein KE, Vij R, Westervelt P, DiPersio JF. A phase 1/2 study of chemosensitization with the CXCR4 antagonist plerixafor in relapsed or refractory acute myeloid leukemia. Blood. 2012;119:3917-24. Waller EK, Olweus J, Lund-Johansen F, Huang S, Nguyen M, Guo GR, Terstappen L. The "common stem cell" hypothesis reevaluated: human fetal bone marrow contains separate populations of hematopoietic and stromal progenitors. Blood. 1995;85:2422-35. Wallington-Beddoe CT, Gottlieb DJ, Garvin F, Antonenas V, Sartor MM. Failure to achieve a threshold dose of CD34+CD110+ progenitor cells in the graft predicts delayed platelet engraftment after autologous stem cell transplantation for multiple myeloma. Biol Blood Marrow Transplant. 2009;15:1386-93. Wang S, Nademanee A, Qian D, Dagis A, Park HS, Fridey J, Smith E, Snyder D, Somlo G, Stein A, Rosenthal J, Falk P, Kogut N, Palmer J, Gaal K, Kim Y, Bhatia R, Yuan S, Kay C, Weiss L, Forman S. Peripheral blood hematopoietic stem cell mobilization and collection efficacy is not an independent prognostic factor for autologous stem cell transplantation. Transfusion. 2007;47:2207-16.

89
Watts MJ, Sullivan AM, Leverett D, Peniket AJ, Perry AR, Williams CD, Devereux S, Goldstone AH, Linch DC. Back-up bone marrow is frequently ineffective in patients with poor peripheral-blood stem-cell mobilization. J Clin Oncol. 1998;16:1554-60. Weaver CH, Hazelton B, Birch R, Palmer P, Allen C, Schwartzberg L, West W. An analysis of engraftment kinetics as a function of the CD34 content of peripheral blood progenitor cell collections in 692 patients after the administration of myeloablative chemotherapy. Blood. 1995;86:3961-9. Webb IJ, Eickhoff CE, Elias AD, Ayash LJ, Wheeler CA, Schwartz GN, Demetri GD, Anderson KC. Kinetics of peripheral blood mononuclear cell mobilization with chemotherapy and/or granulocyte-colony-stimulating factor: implications for yield of hematopoietic progenitor cell collections. Transfusion. 1996;36:160-7. Vellenga E, van Agthoven M, Croockewit AJ, Verdonck LF, Wijermans PJ, van Oers MH, Volkers CP, van Imhoff GW, Kingma T, Uyl-de Groot CA, Fibbe WE. Autologous peripheral blood stem cell transplantation in patients with relapsed lymphoma results in accelerated haematopoietic reconstitution, improved quality of life and cost reduction compared with bone marrow transplantation: the Hovon 22 study. Br J Haematol. 2001;114:319-26. Wilke R, Brettell M, Prince HM, Wolf M, McKenna R, Serpell E, Molloy M, Stevens H, Quinn M, Gates P, Chapple P. Comparison of COBE Spectra software version 4.7 PBSC and version 6.0 auto PBSC program. J Clin Apher. 1999;14:26-30. Villa CH, Shore T, Van Besien K, Cushing M. Addition of plerixafor to mobilization regimens in autologous peripheral blood stem cell transplants does not affect the correlation of preharvest hematopoietic precursor cell enumeration with first-harvest CD34+ stem cell yield. Biol Blood Marrow Transplant. 2012;18:1867-75. Villa D, Crump M, Panzarella T, Savage KJ, Toze CL, Stewart DA, Macdonald DA, Buckstein R, Lee C, Alzahrani M, Rubinger M, Foley R, Xenocostas A, Sabloff M, Muccilli A, Chua N, Couture F, Larouche JF, Cohen S, Connors JM, Ambler K, Al-Tourah A, Ramadan KM, Kuruvilla J. Autologous and allogeneic stem-cell transplantation for transformed follicular lymphoma: a report of the Canadian Blood and Marrow Transplant Group. J Clin Oncol. 2013;31:1164-71. Williams CD, Harrison CN, Lister TA, Norton AJ, Blystad AK, Coiffier B, Taghipour G, Schmitz N, Goldstone AH; European Bone Marrow Transplant Lymphoma Working Party. High-dose therapy and autologous stem-cell support for chemosensitive transformed low-grade follicular non-Hodgkin's lymphoma: a case-matched study from the European Bone Marrow Transplant Registry. J Clin Oncol. 2001;19:727-35. Windrum P, Morris TC, Drake MB, Niederwieser D, Ruutu T; EBMT Chronic Leukaemia Working Party Complications Subcommittee. Variation in dimethyl sulfoxide use in stem cell transplantation: a survey of EBMT centres. Bone Marrow Transplant. 2005;36:601-3. Virgo PF, Gibbs GJ. Flow cytometry in clinical pathology. Ann Clin Biochem. 2012;49(Pt 1):17-28. Vishnu P, Roy V, Paulsen A, Zubair AC. Efficacy and cost-benefit analysis of risk-adaptive use of plerixafor for autologous hematopoietic progenitor cell mobilization. Transfusion. 2012;52:55-62.

90
Viviani S, Di Nicola M, Bonfante V, Di Stasi A, Carlo-Stella C, Matteucci P, Magni M, Devizzi L, Valagussa P, Gianni AM. Long-term results of high-dose chemotherapy with autologous bone marrow or peripheral stem cell transplant as first salvage treatment for relapsed or refractory Hodgkin lymphoma: a single institution experience. Leuk Lymphoma. 2010;51:1251-9. Vogel W, Kopp HG, Kanz L, Einsele H. Myeloma cell contamination of peripheral blood stem-cell grafts can predict the outcome in multiple myeloma patients after high-dose chemotherapy and autologous stem-cell transplantation. J Cancer Res Clin Oncol. 2005;131:214-8. Wong RS, Bodart V, Metz M, Labrecque J, Bridger G, Fricker SP. Comparison of the potential multiple binding modes of bicyclam, monocylam, and noncyclam small-molecule CXC chemokine receptor 4 inhibitors. Mol Pharmacol. 2008;74:1485-95. Vose JM, Bierman PJ, Weisenburger DD, Lynch JC, Bociek Y, Chan WC, Greiner TC, Armitage JO. Autologous hematopoietic stem cell transplantation for mantle cell lymphoma. Biol Blood Marrow Transplant. 2000;6:640-5. Vose JM. Autotransplantation for mantle cell lymphoma. Cancer J. 2012;18:427-31. Wood WA, Whitley J, Moore D, Sharf A, Irons R, Rao K, Serody J, Coghill J, Gabriel D, Shea T. Chemomobilization with etoposide is highly effective in patients with multiple myeloma and overcomes the effects of age and prior therapy. Biol Blood Marrow Transplant. 2011;17:141-6. Wu FY, Heng KK, Salleh RB, Soh TG, Lee JJ, Mah J, Linn YC, Loh Y, Hwang W, Tan LK, Law P, Goh YT. Comparing peripheral blood stem cell collection using the COBE Spectra, Haemonetics MCS+, and Baxter Amicus. Transfus Apher Sci. 2012;47:345-50. Wuchter P, Ran D, Bruckner T, Schmitt T, Witzens-Harig M, Neben K, Goldschmidt H, Ho AD. Poor mobilization of hematopoietic stem cells - definitions, incidence, risk factors, and impact on outcome of autologous transplantation. Biol Blood Marrow Transplant. 2010;16:490-9. Yang SH, Wang TF, Tsai HH, Lin TY, Wen SH, Chen SH. Preharvest hematopoietic progenitor cell counts predict CD34+ cell yields in granulocyte-colony-stimulating factor-mobilized peripheral blood stem cell harvest in healthy donors. Transfusion. 2010;50:1088-95. Yin AH, Miraglia S, Zanjani ED, Almeida-Porada G, Ogawa M, Leary AG, Olweus J, Kearney J, Buck DW. AC133, a novel marker for human hematopoietic stem and progenitor cells. Blood. 1997;90:5002-12. Yoong Y, Porrata LF, Inwards DJ, Ansell SM, Micallef IN, Litzow MR, Gertz MA, Lacy MQ, Dispenzieri A, Gastineau DA, Tefferi A, Elliott M, Snow DS, Hogan WJ, Markovic SN. The effect of absolute lymphocyte count recovery kinetics on survival after autologous stem cell transplantation for non-Hodgkin's lymphoma. Leuk Lymphoma. 2005;46:1287-94. Yu J, Leisenring W, Bensinger WI, Holmberg LA, Rowley SD. The predictive value of white cell or CD34+ cell count in the peripheral blood for timing apheresis and maximizing yield. Transfusion. 1999;39:442-50. Yuen AR, Rosenberg SA, Hoppe RT, Halpern JD, Horning SJ. Comparison between conventional salvage therapy and high-dose therapy with autografting for recurrent or refractory Hodgkin's disease. Blood. 1997;89:814-22.

91
Zambelli A, Poggi G, Da Prada G, Pedrazzoli P, Cuomo A, Miotti D, Perotti C, Preti P, Robustelli della Cuna G. Clinical toxicity of cryopreserved circulating progenitor cells infusion. Anticancer Res. 1998;18:4705-8. Zembruski NC, Stache V, Haefeli WE, Weiss J. 7-aminoactinomycin D for apoptosis staining in flow cytometry. Anal Biochem. 2012;429:79-81. Zhang WB, Navenot JM, Haribabu B, Tamamura H, Hiramatu K, Omagari A, Pei G, Manfredi JP, Fujii N, Broach JR, Peiper SC. A point mutation that confers constitutive activity to CXCR4 reveals that T140 is an inverse agonist and that AMD3100 and ALX40-4C are weak partial agonists. J Biol Chem. 2002;277:24515-21. Zubair AC, Kao G, Daley H, Schott D, Freedman A, Ritz J. CD34(+) CD38(-) and CD34(+) HLA-DR(-) cells in BM stem cell grafts correlate with short-term engraftment but have no influence on long-term hematopoietic reconstitution after autologous transplantation. Cytotherapy. 2006;8:399-407. Zubair AC, Rymer R, Young J, Keeton U, Befort R, Nolot B, Evans C, Bleach T, Torloni A. Multiple myeloma patients receiving large volume leukapheresis efficiently yield enough CD34+ cells to allow double transplants. J Clin Apher. 2009;24:6-11. Zöller M. CD44: can a cancer-initiating cell profit from an abundantly expressed molecule? Nat Rev Cancer. 2011;11:254-67.

Publications of the University of Eastern Finland
Dissertations in Health Sciences
isbn 978-952-61-1254-1
Publications of the University of Eastern FinlandDissertations in Health Sciences
dissertatio
ns | 195 | V
ille Va
rm
avu
o | P
lerixafor in Autologou
s Stem
Cell T
ransplantation
Ville VarmavuoPlerixafor in Autologous
Stem Cell Transplantation
Ville Varmavuo
Plerixafor in Autologous Stem Cell Transplantation
Autologous stem cell transplantation
(ASCT) has an established role as a
treatment modality for hematological
malignancies. Stem cells for ASCT
are almost invariably collected from
peripheral blood after mobilization
therapy. Plerixafor, a CXCR4
antagonist, is the latest addition to
stem cell mobilization and may be
used in patients who mobilize poorly
otherwise. This series of studies
provides additional information to
support the use of plerixafor.





























