Embed Size (px)
Citation preview
Here’s an example
comment bubble
Hello and thanks for viewing my presentation. I usually create my presentations to complement my speaking, and I’m aware they may not make as much sense to people viewing them without my discussion.
For this presentation I’ve tried to set the stage by include some explanatory comments so that when you view this it might make a little more sense to you. I did this by including yellow comment bubbles that attempt to give you some more context. See an example below.
If you have any questions about the presentation or wish to discuss any of the points, please feel free to contact me.
Thanks!Michael Ibara
http://www.linkedin.com/in/ibara
“All progress depends on the unreasonable man”
Why A Lack of Vision Will Keep Us from Using Social Media to Improve Safety
Michael A. Ibara
DISCLAIMERPfizer supports and funded ASTER and continues to
invest in the concepts and goals involved in this work.During this talk, any opinions, suggestions or crazy
statements are entirely my own.
http://www.linkedin.com/in/ibara
“All progress depends on the unreasonable man”
Why A Lack of Vision Will Keep Us from Using Social Media to Improve Safety
Michael A. Ibara
I originally presented this here
“All progress depends on the unreasonable man”
Why A Lack of Vision Will Keep Us from Using Social Media to Improve Safety
Michael A. Ibara
My first presentation used these 4 concepts.
In the webinar I dumped these concepts and
went for something else…
“The reasonable man adapts himself to the world; the unreasonable one persists in trying to adapt the world to himself. Therefore all progress depends on the unreasonable man.”
George Bernard Shaw (1856 - 1950), Man and Superman (1903) "Maxims for Revolutionists"
My current views are based on ideas I’ve been working on since 2006 which lead in 2009 to the “ASTER” study, demonstrating direct and automated capture of adverse events directly from an electronic health record.
Since then I’ve seenthe promise of new ideasin safety realized at adramatically slower ratethan ideas in healthcareat large
Enough time has passed since the first introduction of new ideas based on social media for anyone (who takes the time) to see these new concepts present fundamental challenges to our current paradigm of safety.
But social media is a symptom, not a cause, of what's wrong with safety today.
The digitization of healthcare data combined with the internet creates scenarios unimaginable 10 years ago.
And yet, we continue to try and shoehorn these new sources of data and new business models into concepts that are over 20 years old.
If we do not rise to the challenges and opportunities presented to us by this epochal change in healthcare,the currentpharma safetyIndustrywill godown in historyAs 'those other guys'.
I’m taking the long view here…
There are technology efforts, research projects, and even recent efforts in the industry that show progress, and we’re having some success in interpreting current regulations and applying themto situations created byDigitized healthcaredata and social media…
These exceptions ‘prove the rule’
BUT…
There is an immense disconnect between the business model we use to meet regulatory demands …
and the models that are fueling dramatic changes in healthcare
The concepts that make up our current business model – upon which our current regulations and practices are built – do not allow us to take advantage of the new technologies and possible working models that exist now and are evolving every day
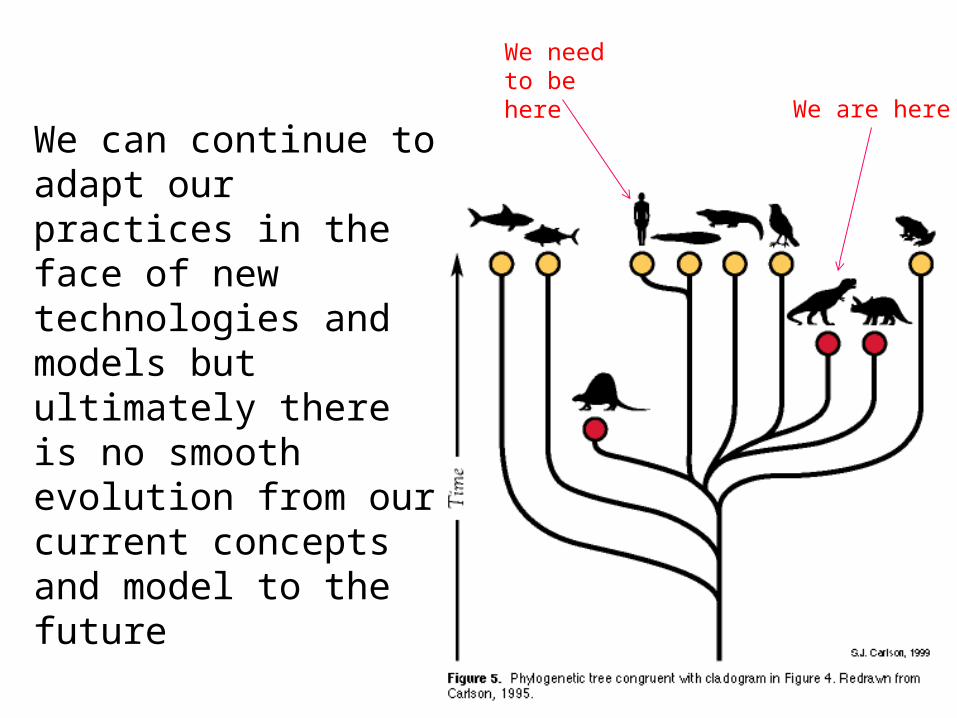
We can continue to adapt our practices in the face of new technologies and models but ultimately there is no smooth evolution from our current concepts and model to the future
We are here
We need to be here
So I’m a short-term optimist…
But I’m a long-term pessimist
Short-term we can see the promise of technologies and even some regulatory efforts…
But long-term we will not realize the potential of digital healthcare for safety unless we make radical changes to our business model, and therefore our regulations
2 examples
LDKIT (limited duration key issue team)Goal: To facilitate FDA guidance on pharmacovigilance issues in social media
Drafted a Q&A document coordination with Legal FDA Focus Group which prioritized important issues of uncertainty around pharmacovigilance for social media – created a list of questions and proposed answers.
Met with FDA to discuss document.
Q: Does the International Conference on Harmonization (ICH) E2D guidance still apply with respect to the adverse event screening and reporting requirements of IND sponsors and NDA/BLA applicants (referred to in this document as “companies”)?
Q: Under ICH E2D, companies “are not expected to screen external websites for ADR information. However, if [a company] becomes aware of an adverse reaction on a website that it does not control, the [company] should review the adverse reaction and determine whether it should be reported.” Does the FDA continue to support the recommendation in the ICH guidance regarding the responsibility of companies for screening external websites for potential adverse event information?
Q: Are companies expected to screen web sites and media that they control to find potential adverse event information?
Example questions…
A: Yes, consistent with the ICH standard discussed above, the FDA does not require companies to review the content and process safety information on third-party web sites that companies do not control. FDA understands that it is impossible for companies to monitor all web sites and social media.
If a company chooses to view non-company sponsored sites, the viewed pages should be monitored for adverse events for the period of viewing. For example, if a company project plan specifies that the company will view user-generated content for three days, then it is expected that the company will monitor for adverse events for the duration of the three days.” Companies should develop policies and procedures under which employees or agents who encounter potentially reportable safety information on the Internet while working for the company would report such information to company pharmacovigilance staff for analysis.
Example answer…
PV Working SubteamTo develop a globally applicable set of recommendations for standard practices and policies to optimize the value of, and minimize the risks posed by the information contained in social media
Develop white paper
Develop real-life scenarios
Meet with FDA
Study…?
Work underway now…
Survey of current regulations related to social media
Excellent suggestions, solutions
Meetings, etc. TBD

BUT…
In spite of our best efforts and the
reassuring guidance from certain
groups, we don’t know
how to take advantage
of the models that are
emerging at the interface
of social media and healthcare
A few examples
A network of oncology patients have patients who are as expert as most doctors in their particular form of cancer. These patients can provide deep insight into adverse events and are regularly sharing insightful clinical information that is far more detailed than a typical AE report, but they want to be active participants in their disease – including the AEs.
How do we make them active partners vs dumb AE reporting terminals?
A medical network in the Southeast has automated reporting of AEs from their doctors, but the reports are sent completely blinded to drug companies with no information except an email address from the medical center.
A company is receiving 50 reports a week from this email address. Are they valid? How do they validate them?
A company would like to develop a baseline of searches and tweets for their drugs so that they can monitor changes in baseline searching and tweeting. These changes in baseline could be possible AE signals.
The company declines to pursue this because they will be forced to review, follow up on and report many potential AE reports and this workload would completely overwhelm their pharmacovigilance department.
Each of these scenarios points to fundamental changes in our concepts of:
- Reports from pts vs HCPs and hard separation from patients as reporters;
- Verifying identify of a reporter and the “four elements”
- The binary distinctions of reportable vs onreportable or serious vs nonserious
“Neither a wise man nor a brave man lies down on the tracks of history to wait for the train of the future to run over him.“
Dwight D. Eisenhower
Flickr: Ruud Welton
No amount of re-interpreting the current regulations or messing around the edges of our current systems will fix this problem. We need to recognize that we are being given a chance to make history, or fight against it.
The implications are scary but clear: we need to rethink the regulations; we need to envision new ways to collect data; we need to move away from an assembly-line model and ivory tower mentality toward an interactive, transparent approach.
And we are the ones to do this - we have the accumulated knowledge of safety and the expertise and wisdom to address it.
In asking us to make these deep and jarring changes, I am clearly an unreasonable man…
But that’s not a reason to stop…
Michael Ibara’s picture
goes here

I’m (still) looking for a few unreasonable (wo)men…
Thank You!