Embed Size (px)
Citation preview

Symptomatic treatments
Celia Oreja-Guevara & Gavin Giovannoni

• The numerous symptoms and co-morbidities associated with MS can
negatively impact patient quality of life (QoL), and places a burden on
carers, family, friends and other support networks
• Many MS-related symptoms are frequently ignored in assessments of
disease status and often thought not to be associated with the disease
• Research into how MS-related symptoms can be diagnosed and
treated within the MS population is lacking
de Sá JCC, et al. Ther Adv Neurol Disord 2011; 4:139–168.
The importance of considering MS-related
symptoms

Co-morbidities and MS-related symptoms

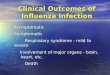
Prevalence of co-morbidities and associated
symptoms in patients with MS
a 32% of ataxia will be severe enough to decrease functional abilities. b Mortality ratio for suicide in MS of 2.3 compared with general population. Note: where a range is given in the reference, upper limit of range is plotted. de Sá JCC, et al. Ther Adv Neurol Disord 2011; 4:139–168.
90 90 90 85
80 80 75 75
68 65
50
32
25 20
5.4
0
10
20
30
40
50
60
70
80
90
100
Pati
en
ts (
%)

Epstein Bar Virus
Genetics
Vitamin D
Smoking
Risks
Adverse
events
Differential
Diagnosis
MRI
Evoked
Potentials Lumbar
puncture
Blood
Tests
Diagnostic
Criteria
Cognition
Depression
Fatigue
Bladder
Bowel
Sexual
dysfunction Tremor
Pain Swallowing
Spasticity Falls
Balance
problems Insomnia
Restless
legs Fertility
Clinical trials
Gait
Pressure
sores
Oscillopsia
Emotional
lability
Seizures
Gastrostomy
Rehab
Suprapubic
catheter
Intrathecal
baclofern
Physio-
therapy
Speech
therapy
Occupational
Therapy
Functional
neurosurgery
Colostomy
Tendonotomy
Studying
Employment Relationships
Travel
Vaccination
Anxiety
Driving
Nurse
specialists
Counselling
Family
counselling
Relapses
1st line
2nd line
Maintenance Escalation Induction
Monitoring
Disease-free
Disease
progression
DMTs
Side Effects
Advanced
Directive
Exercise
Diet
Alternative
Medicine
Pregnancy Breast
Feeding
Research
Insurance
Vision
Palliative Care
Assisted
suicide
Social
services
Legal aid Family
counselling
Prevention
Diagnosis
DMT
Symptomatic
Therapist
Terminal
Counselling

0
25
50
75
100
Physical Psychological
Mild (n=35) Moderate (n=52) Severe (n=46)
• The subgroup with mild symptoms had the
highest QoL, whereas the subgroup with severe
symptoms had the lowest QoL
MSIS-29, Multiple Sclerosis Impact Scale-29; lower MSIS-29 scores indicates higher QoL.
Motl RW et al. J Pain Symptom Manage 2010; 39:1025–1032.
Effects of MS-related symptoms on QoL
Single-factor model tested using confirmatory
factor analysis for establishing the symptom cluster
Measures of physical and psychological domains of QoL
based on mild, moderate or severe clusters of symptoms
MSIS-29 subs scale
Me
an
± s
tan
da
rd e
rro
r
Fatigue Depressio
n Pain
Perceived
cognitive
complaints
Symptom
cluster
FSS CES-D MPQ PDQ
.55 .63 .61 .71

• Gender (female), caregiver co-morbidities, age of the caregiver and EDSS score were
the main predictors of caregiver HRQoL
Rivera-Navarro J, et al. Mult Scler 2009; 15:1347–1355.
Burden of MS-related symptoms on caregivers
Scores of SF-36 dimensions of caregivers
59.3 62.3
65.5 65.6 70.7
77.5 80.2 81.9
0
20
40
60
80
100
GeneralHealth
MentalHealth
Bodily Pain Role-emotionalFunctioning
SocialFunctioning
Vitality Role-physicalFunctioning
PhysicalFunctioning
Mean

• Discuss your experiences of diagnosing co-morbidities and
MS-related symptoms
Open discussion

Therapies and unmet needs in
symptomatic management

MS-related symptom treatment
1. de Sá JCC, et al. Ther Adv Neurol Disord 2011; 4:139–168 (the medications listed here have only been investigated for the treatment of MS-related symptoms in experimental settings and sometimes not even in patients with MS. Their inclusion in this table and the broader manuscript should not be taken to imply that the authors are in any way recommending they be used in the clinical setting); 2. Cruccu G, et al. Eur J Neurol 2008; 15:1013–1028.
Symptom Recommended/licensed
Spasticity1
Baclofen
Tizanidine
Intrathecal baclofen (for EDSS > 7)
THC-CBD (Sativex)
Pain
trigeminal neuralgia2
Carbamazepine (stronger evidence)
Oxcarbazepine (better tolerability)
Walking impairment Slow release 4-aminopyridine (fampridine)

Pharmacological agents used in treating
MS-related symptoms with limited efficacy
a without sleepiness, b fatigue with sleepiness, c erectile dysfunction, d vaginal dryness, e low libido, f used for urinary storage, g used in emptying dysfunction, h used in combined dysfunction de Sá JCC, et al. Ther Adv Neurol Disord 2011; 4:139–168 (the medications listed here have only been investigated for the treatment of MS-related symptoms in experimental settings and sometimes not even in patients with MS. Their inclusion in this table and the broader manuscript should not be taken to imply that the authors are in any way recommending they be used in the clinical setting).
Symptom Pharmacological agents with limited evidence of efficacy
Spasticity Dantrolene, tolperisone, benzodiazepines, gabapentin, tetrahydrocannabinol, botulinum
toxin
Pain (trigeminal neuralgia) Misoprostol, baclofen, oxcarbazepine
Fatigue 4-aminopyridine or other K channel blockers, SSRIs, amantadinea, modafinilb
Depression SSRIs, serotonin and noradrenaline reuptake inhibitors
Pain – general Related to suspected cause(s) of the symptom; similar approach as taken with non-MS pts
Cognitive impairment Donepezil, rivastigmine
Sexual problems Phosphodiesterase 5 inhibitorsc, topical lubricantsd, androgen therapye
Dysphagia Anticholinesterases
Dysarthria Therapies treating tremor (in rare cases)
Seizures Standard antiepileptic therapies
Vertigo and dizziness Vestibular blocking agents
Sleep disorders Dopaminergic agonists for restless legs syndrome; modafinil for excessive daytime sleepiness
Urinary Storage/emptying
dysfunction/combined
Antimuscarinic compoundsf,g, alpha blocking agentsg, antispasticity agentsg, Neurotoxin, botulinum
toxin Ah, cannabinoidsh
Bowel dysfunction Laxatives
Tremor and ataxia Isoniazid, carbamazepine, topiramate
Oculomotor Memantine, gabapentin

Alternative therapies used in treating
MS-related symptoms
a Urine storage, b emptying dysfunction, c combined dysfunction 1. de Sá JCC, et al. Ther Adv Neurol Disord 2011; 4:139–168; 2. Apel A, et al. J Neurol 2006; 253:1331–1336; 3. Sastre-Garriga J, et al. Mult Scler 2003; 9:320–322. The medications listed here have only been investigated for the treatment of MS-related symptoms in experimental settings and sometimes not even in patients with MS. Their inclusion in this table and the broader manuscript should not be taken to imply that the authors are in any way recommending they be used in the clinical setting).
Symptom Other interventions
Spasticity Physiotherapy, cooling therapy and hydrotherapy
Pain (trigeminal neuralgia) Thermocoagulation, glycerol instillation, gamma knife radiosurgery, neuroablative
procedures, microvascular decompression
Fatigue Physiotherapy, yoga, cooling therapy, aerobic exercise, energy conservation, coping
strategies
Depression Cognitive behavioural therapy
Psychosocial problems Psychotherapy, stress management, relaxation techniques
Tremor and ataxia Exercise and rehabilitation, forearm cooling, deep brain stimulation, thalamotomy
Pain – general Related to suspected causes(s) of the symptom; similar approach as taken with non-MS patients
Cognitive impairment Cognitive training techniques
Dysphagia Thickening agents in liquids, ‘chin tucking’
Dysarthria Speech therapy, spelling boards, computer-assisted programs
Vertigo and dizziness Physiotherapy, vestibular rehabilitation therapy, repositioning manoeuvres
Urinary Storage/Emptying
dysfunction/combined
Incontinence padsa,b, clean intermittent self-catheterizationb, ileovesicostomyb, permanent
catheterisationb, Sacral nerve stimulationc, hyperbaric oxygen treatmentc
Bowel dysfunction High-fibre diet, increased fluid intake, enemas
• 67.3% of MS patients in Germany reported that they were currently using one or more complementary
of alternative medicines2
• 41% of patients in Spain used unconventional therapies during the previous year3

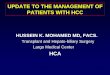
Improving outcomes in patients with MS:
unmet needs in symptomatic management
Rieckmann et al., J Neurol 2012 (Epub ahead of print).
Area for
development
More therapy options Commitment to
research
Personalized
care
Area for
development
Area for
development
Affording patients psychological and social support as part of their treatment package
Diverse therapies and strategies needed to address the complexity of MS symptoms and challenges
New approaches incorporating a wide range of pharmacological and non-pharmacological strategies need to be developed
Widen the focus of research to ensure the continuous development of better therapy options
Ensure greater access to comprehensive care regimens that include symptomatic care, rehabilitation and psychological support
Research across all domains is key for a better understanding of disease mechanisms

• Discuss case scenarios
– Spasticity
– Fatigue
– Depression
Open discussion

• 46-year-old woman with secondary progressive MS, spastic
paraparesis (3 to 4/5) and painful clonic spasms. Using bilateral
support for walking. Currently on oxybutynin (5 mg TDS) and
intermittent self-catheterisation for urinary symptoms, but no other
medications.
• How are you going to manage her spasticity?
Case scenario: spasticity

• A 28-year-old woman with early relapsing–remitting MS. Little
neurological impairment but suffering from severe fatigue. Recently
split up with long-term partner. Has had to stop work as a bank clerk
because of the fatigue.
• How are you going to manage her fatigue?
Case scenario: fatigue

• A 43-year-old man with relapsing–remitting MS complains of feeling
depressed. He is continuously tired as has no energy. Has difficulty
motivating himself to do any physical chores. He is sleeping poorly,
i.e. early morning waking, has lost his appetite and has no libido.
• How are you going to treat his depression?
Case scenario: depression

Epstein Bar Virus
Genetics
Vitamin D
Smoking
Risks
Adverse
events
Differential
Diagnosis
MRI
Evoked
Potentials Lumbar
puncture
Blood
Tests
Diagnostic
Criteria
Cognition
Depression
Fatigue
Bladder
Bowel
Sexual
dysfunction Tremor
Pain Swallowing
Spasticity Falls
Balance
problems Insomnia
Restless
legs Fertility
Clinical trials
Gait
Pressure
sores
Oscillopsia
Emotional
lability
Seizures
Gastrostomy
Rehab
Suprapubic
catheter
Intrathecal
baclofern
Physio-
therapy
Speech
therapy
Occupational
Therapy
Functional
neurosurgery
Colostomy
Tendonotomy
Studying
Employment Relationships
Travel
Vaccination
Anxiety
Driving
Nurse
specialists
Counselling
Family
counselling
Relapses
1st line
2nd line
Maintenance Escalation Induction
Monitoring
Disease-free
Disease
progression
DMTs
Side Effects
Advanced
Directive
Exercise
Diet
Alternative
Medicine
Pregnancy Breast
Feeding
Research
Insurance
Vision
Palliative Care
Assisted
suicide
Social
services
Legal aid Family
counselling
Prevention
Diagnosis
DMT
Symptomatic
Therapist
Terminal
Counselling