Embed Size (px)
Citation preview
1
Vaccination coverage and reasons for non-vaccination after a measles mass vaccination
campaign in rural DRC, 2015.
Theocharopoulos GeorgiosESCAIDE 2016
2
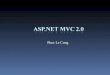
DRC/ Katanga / Haute Lomami region
3
Floating islands
4
Floating islands
5
Floating islands
6
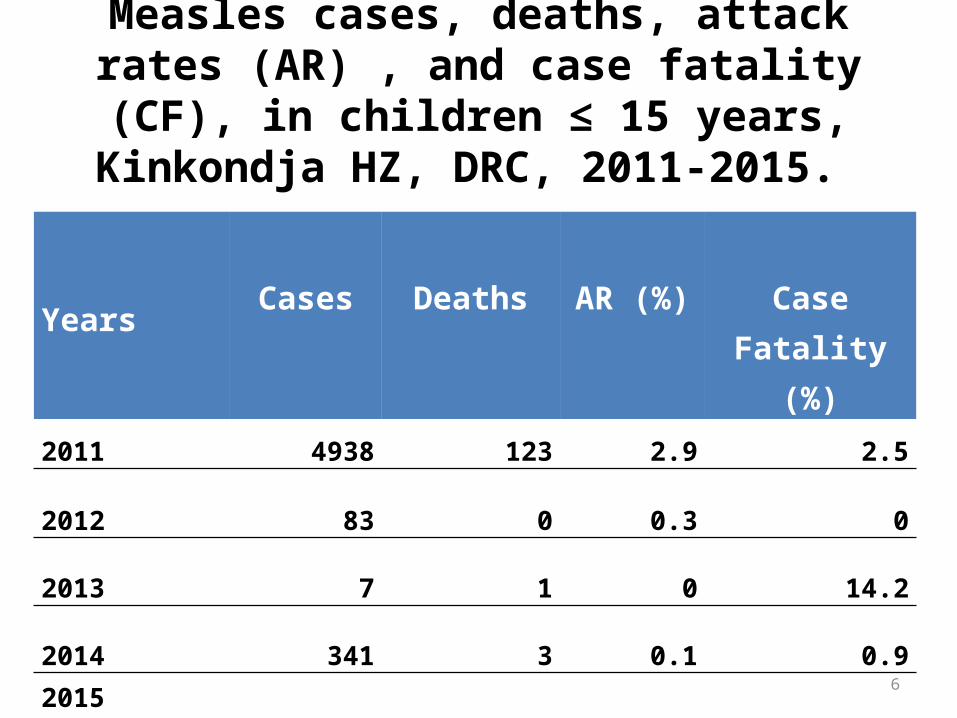
Measles cases, deaths, attack rates (AR) , and case fatality (CF), in children ≤ 15 years,
Kinkondja HZ, DRC, 2011-2015.
Years Cases Deaths AR (%) Case Fatality (%)
2011 4938 123 2.9 2.5
2012 83 0 0.3 0
2013 7 1 0 14.2
2014 341 3 0.1 0.9
2015 (week33) 3049 88 5.3 2.9
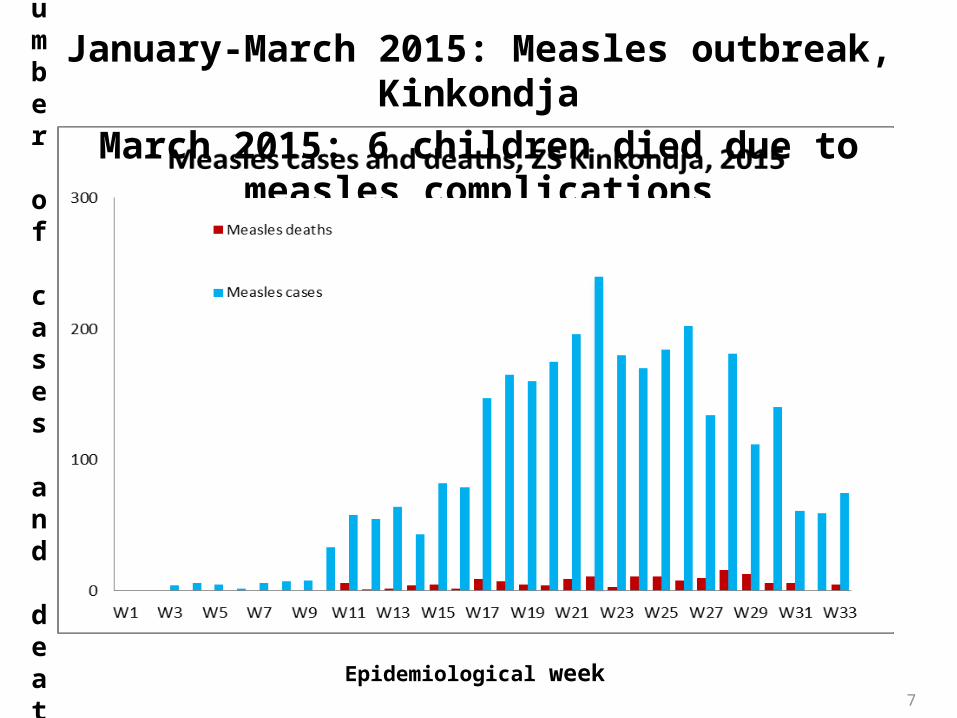
January-March 2015: Measles outbreak, KinkondjaMarch 2015: 6 children died due to measles complications
Number of cases and
deaths
Epidemiological week7
8
Survey objectives
• To estimate the vaccination coverage by gender and age groups
• To identify reasons for non vaccination & factors associated with low coverage
9
Methods: Two-stage cluster samplingFirst stage: • Random selection of 40 villages/islands (clusters) from a list
of 149 villages/islands
Second stage: • 19 households per cluster• In villages: “spin the pen” method and random number table
to select 1st households; adjacent households after• In islands: GPS spatial sampling to select houses
10
Target population & data collection
• Target population: children 6 months to 15 years living in Kinkonja health zone since April 2015
• Interviews of guardians-questionnaire on: – Socio-demographic data for children and their families – Child vaccination status based on oral feedback or on vaccination card– Knowledge about vaccination event and measles
11
Data analysis
• Proportions and 95% confidence intervals (95%CI) allowing for clustering
• Crude & Adjusted prevalence ratio using Poisson regression
12
Results: Vaccine coverage survey
• 2,980 children included from: 709 households in 40 clusters• 50% female• 64% (95%CI: 63-66) children vaccinated for measles
based on vaccination card • 85% (95%CI: 84-86) children vaccinated for measles
estimated by vaccination card & oral feedback• Data collection lasted 10 days (3 - 12 August).
13
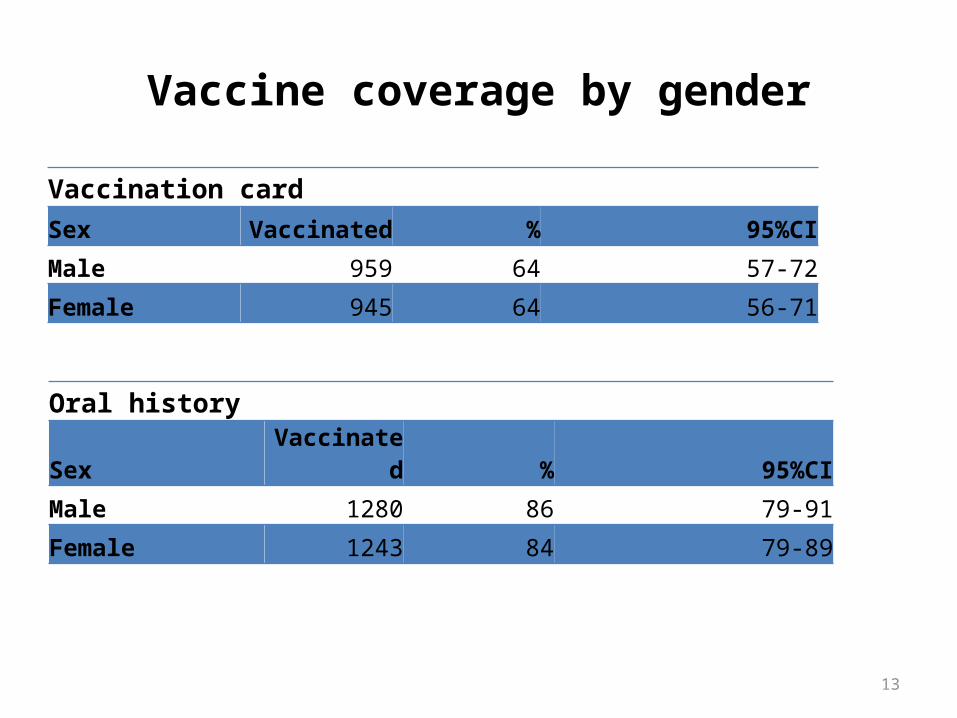
Vaccine coverage by gender
Vaccination cardSex Vaccinated % 95%CI
Male 959 64 57-72
Female 945 64 56-71
Oral historySex Vaccinated % 95%CI
Male 1280 86 79-91
Female 1243 84 79-89
14
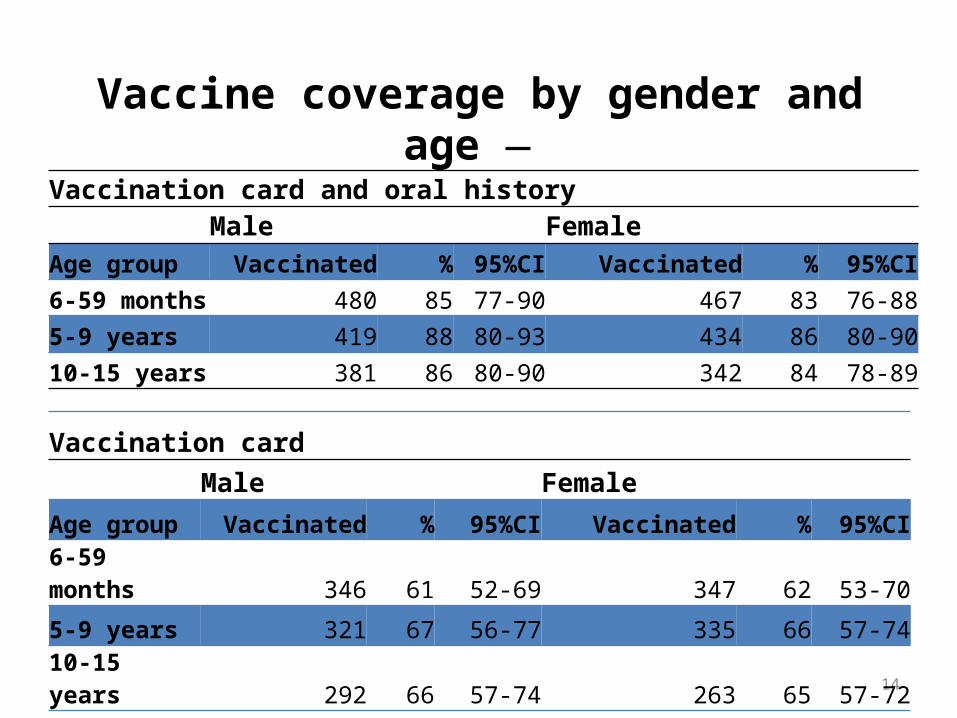
Vaccine coverage by gender and age Vaccination card and oral history
Male FemaleAge group Vaccinated % 95%CI Vaccinated % 95%CI6-59 months 480 85 77-90 467 83 76-885-9 years 419 88 80-93 434 86 80-9010-15 years 381 86 80-90 342 84 78-89
Vaccination cardMale Female
Age group Vaccinated % 95%CI Vaccinated % 95%CI
6-59 months 346 61 52-69 347 62 53-70
5-9 years 321 67 56-77 335 66 57-74
10-15 years 292 66 57-74 263 65 57-72
15
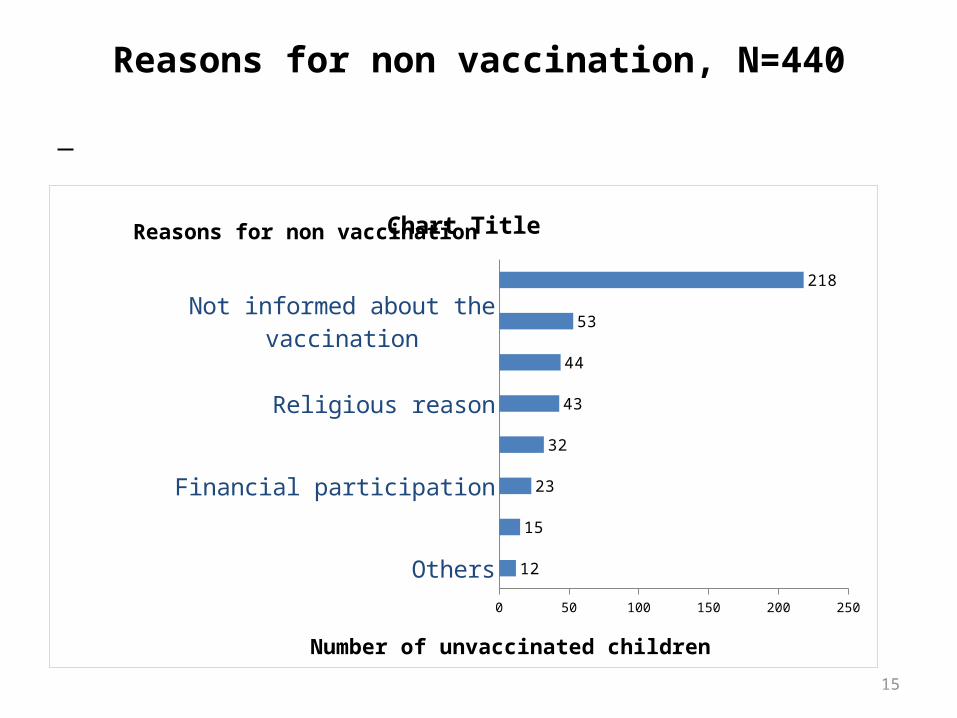
Reasons for non vaccination, N=440
Others
Lack of incentives
Financial participation
Lack of knowledge
Religious reason
Refused to answer
Not informed about the vaccination
Absent during the vaccination
0 50 100 150 200 250
12
15
23
32
43
44
53
218
Chart Title
Number of unvaccinated children
Reasons for non vaccination
16
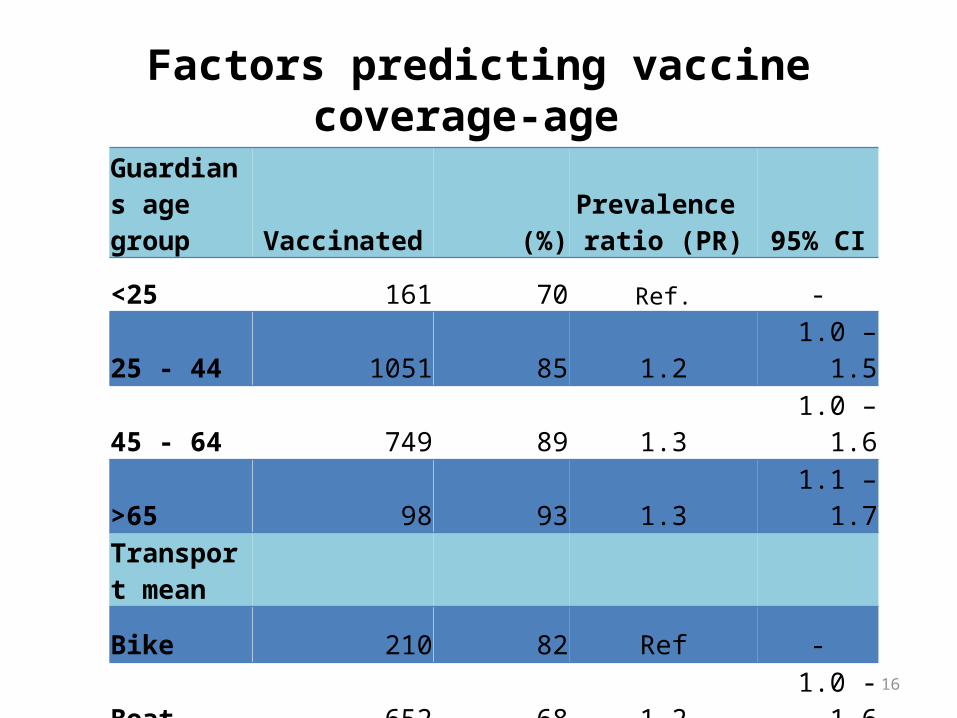
Factors predicting vaccine coverage-age
Guardians age group Vaccinated (%)
Prevalence ratio (PR) 95% CI
<25 161 70 Ref. -
25 - 44 1051 85 1.2 1.0 – 1.5
45 - 64 749 89 1.3 1.0 – 1.6
>65 98 93 1.3 1.1 – 1.7Transport mean
Bike 210 82 Ref -
Boat 652 68 1.2 1.0 - 1.6
Car 1660 89 1.3 1.0 - 1.7
17
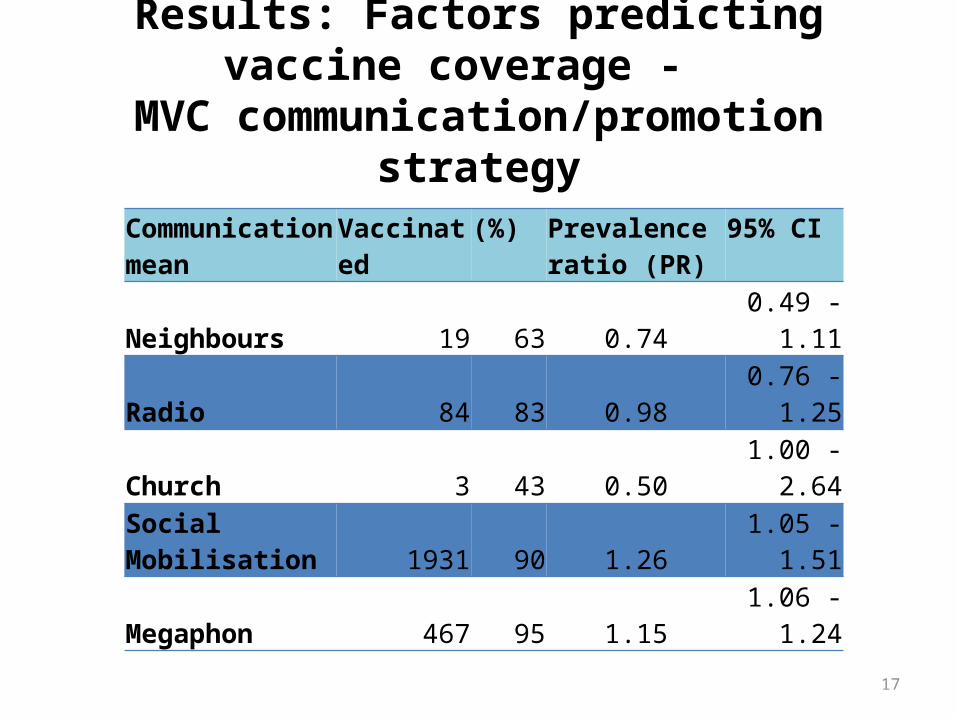
Results: Factors predicting vaccine coverage - MVC communication/promotion strategy
Communication mean
Vaccinated (%) Prevalence ratio (PR)
95% CI
Neighbours 19 63 0.74 0.49 - 1.11
Radio 84 83 0.98 0.76 - 1.25
Church 3 43 0.50 1.00 -2.64
Social Mobilisation 1931 90 1.26 1.05 - 1.51
Megaphon 467 95 1.15 1.06 - 1.24
18
Factors associated with higher vaccination coverage:Multivariate analysis
• children’s guardians over 25 years aPR: 1.2 95% CI 1.0 –1.4• communities accessible by car or boat aPR: 1.2 95% CI 1.0–1.4• social mobilisers promoting the MVC aPR: 1.3 95%CI 1.1–1.5
19
Conclusions
• Limitation: Data quality (oral history/vaccination card)
• MVC did not achieve global standard of 95% coverage in Kinkondja in 2015.
• Population mobility is an important reason for non vaccination
20
Recommendations
• MVC should take into account the seasonal displacement of the population and organise supplementary vaccination at return time
• In mass vaccination campaigns implement extensive social mobilization
21
Acknowledgements
• All survey participants/interviewees
• MSF teams, (medical, logistic, administration
• Interviewers
• Local counterparts of MSF in the Bureau Central de la Zone in Kinkondja
• EPIET coordinators and supervisors in Santé Publique France, Paris.
22
Co-authors and affiliations
Annick Lenglet, Médecins Sans Frontières (OCA), Amsterdam, The Netherlands
Junie N. Mwenge, Médecins Sans Frontières (OCA), Lubumbashi, Democratic
Republic of Congo
Claude I. Yumba, Bureau Centrale de Zone (BCZ) , Democratic Republic of Congo

23

24

25

26