Embed Size (px)
Citation preview

ORAL MEDICINE SEMINAR
R A W A N A B E D A L - S A L A M A B U A R R AA R A B A M E R I C A N U N I V E R S I T Y J E N I N
FA C T U A L LY O F D E N T I S T R Y2 0 1 5 - 2 0 1 6

CASE HISTORYAli is 25 years of age. He attends your surgery complaining that he has pain and welling at the
back of his mouth on the lower right side, a bad taste, bad breath and that he can’t open
his mouth properly. He has lymphadenopathy of the right submandibular and cervical node. You
know from a previous visit that he has a partially erupted lower third molar.

IDEAS 1. Differential Diagnosis .2. What is pericoronitis?3. What causes pericoronitis ?4. What are pericoronitis symptoms and signs ?5. How is pericoronitis diagnosed?6. What is the treatment for pericoronitis ?7. Are home remedies effective for pericoronitis ?8. What is the prognosis for pericoronitis?9. Is it possible to prevent pericoronitis?

DIFFERENTIAL DIAGNOSIS (PERICORONITIS)i. Trismus .ii. Tonsilitis .iii.Dentigerous cyst .iv.Odontogenic cysyt.v. Periodontitis.

WHAT IS PERICORONITIS?Pericoronitis is an inflammation or infection (depending on the
causes of it) of the soft tissue (gingiva) around the crowm of partially impacted tooth especially mandibular third molar , and is usually caused by normal oral flora . It is either Acute , sub acute or chronic pericoronitis.
Age incidence :- 17-25 years History of pericoronitis :-1844:- Gunnel termed it “ Painful Affecting” End of 19th century:- changed to “Folliculitis”, as the erupted
teeth breaches the follicle.20th century:- terms “Pericoronitis”
What Is the differences between pericoronitis and
Supracoronitis ?

WHAT CAUSES OF PERICORONITIS ?1.Impaction of food and plaque accumulation under the
operculum.2.Caused by normal oral flora , if host defense are
compromised (e.g, during minor illness such as influenza or an upper respiratory infection or because immune-compromised drugs),infection can occur .
3.Can also arise following minor trauma from maxillary third molar.

WHAT ARE PERICORONITIS SYMPTOMS AND SIGNS ?Signs and symptoms of pericoronitis can range from mild to
severe and include:- pain, swelling of the gums, tenderness, redness of gum tissue, bad breath, bad taste from pus, difficulty opening the jaw, difficulty swallowing, swollen lymph nodes, fever, loss of appetite, and feeling unwell.

HOW IS PERICORONITIS DIAGNOSED?
Pericoronitis is diagnosed based on symptoms and appearance during a clinical evaluation with a health-care professional such as a dentist or oral surgeon.
A dental X-ray is used to assess the area and rule out other possible causes for pain, such as dental decay.
And here we will take about ** Causative organisms **Pathophysiological features .**Histological appearance.

CAUSATIVE ORGANISMS
1. Streptococci 2. Anaerobic
Bacteria ,such as peptococci, peptostreptococci, bacteroides and fusobacteria, and also spirochaetes
3. Most of oral flora, shuch as Spirochetes and fusi-form bacilli

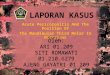
PATHOPHYSIOLOGIC FEATURES
Is the explanation of the procedure in
which pericoronitis
starts and complications
caused due to it. This is flow chart which depicts the
predisposing factors, clinical
features and the complications caused due to pericoronitis

LUDWIG’S ANGINA (RELATED TO LOWER THIRD MOLARS)
Conditon exhibiting firm, acute, toxic cellulitis and bilateral swelling of the :-
1.sub mental spaces . 2.sub lingual spaces . 3.sub mandibular spaces.

LUDWIG’S ANGINA (RELATED TO LOWER THIRD MOLARS)
Etiology :- 1. Periapical, pericoronal
or periodontal infection of the lower third molar.
2. Traumatic injuries and infected lesions.
3. Infective conditions such as osteomyelitis manifests as Ludwig’s angina.
4. Cysts or tumors in third molar region.

LUDWIG’S ANGINA (RELATED TO LOWER THIRD MOLARS)
Pericoronitis Submandibular spaceThrough submand.S.G above mylohaiod muscle
Sublingual space
Across genioglossus M.
Sublingual space in Other side
Cross mylohyiod M. to reach opposite side of
Submandibular spaceVia lymphatics
Submental space
Along sublingual artery in betw. Genioglossus & geniohyoid Ms.
spread posteriorly to tongue
Laryngeal edema
Pass along deep cervical fascia (anter.to neckClavicle & mediastinum
start

Clinical features :- **systemic
features1. Pyrexia.2. Dehydration.3. dysphagia.4. Dyspnea.5. Hoarseness of
voice.6. Stridor.
LUDWIG’S ANGINA (RELATED TO LOWER THIRD MOLARS)
Clinical features :- **extra-oral features1. Hard to firm
brawny indurated swelling skin.
2. Stretched swelling is tender with local rise in temperature.
3. Difficulty in closing the mouth + drooling of saliva .
4. Respiratory distress.
Clinical features :- **intra-oral
features1. Trismus. 2. Floor of the
mouth is raised.
3. Tongue raised upward.
4. Increased salivation

LUDWIG’S ANGINA (RELATED TO LOWER THIRD MOLARS)

HISTOLOGICAL APPEARANCE Epithelium of the opreculum includes :- • Increases vascularity • Hyperplasia • Intracellular edema • Leukocytic infiltration • Diffused infiltration of plasma cells• Diffused infiltration of lymphocytes

WHAT IS THE TREATMENT FOR PERICORONITIS ?
There are three methods for treatment of pericoronitis depending on the severity of the condition:-
1.Management of pain and resolving the infection2.Minor surgery to remove the overlapping gum tissue
(operculectomy)3.Removal of the toothTo manage the pain, over-the-counter medications such
as acetaminophen or ibuprofen are used. If it is localized to the tooth and there has been no spread of the infection, the area is thoroughly cleaned out under local anesthesia by a dentist. If there is swelling or fever, oral antibiotics such as amoxicillin or erythromycin will be prescribed.

When the tooth can be useful and there is a desire to keep the tooth, minor surgery can be performed to remove the operculum. This will allow better access to properly clean the area and prevent the accumulation of bacteria and food debris. In some unfortunate instances, the gum tissue may grow back and create the same problem.
Removal (extraction) of the tooth is the most common treatment method since wisdom teeth oftentimes are poorly positioned and do not erupt completely. This method eliminates any future occurrences of pericoronitis.
In rare instances, the symptoms become so severe that an individual needs to go the hospital emergency room to seek care due to the rapid spread of infection.
WHAT IS THE TREATMENT FOR PERICORONITIS ?


ARE HOME REMEDIES EFFECTIVE FOR PERICORONITIS ?
Sometimes, mild symptoms of pericoronitis can be treated at home without antibiotics. Thorough and gentle brushing of the area with a small-headed toothbrush may help to break up the plaque or food that is trapped. Oral water irrigators can be effective in clearing out the debris trapped under the operculum as well. Rinsing with warm saltwater can help to soothe the area. Additionally, diluted hydrogen peroxide can be used as a rinse or irrigating solution to help reduce the bacteria in the area.
For severe pericoronitis where swelling and fever are present, home treatments are not advised and proper care should be sought with the appropriate health-care professional.

WHAT IS THE PROGNOSIS FOR PERICORONITIS?
The prognosis for pericoronitis is usually very good. With timely care and treatment, pericoronitis can properly be managed or eliminated. The condition should resolve in approximately one week. If the initial cause of the infection is not treated, the condition will likely return

IS IT POSSIBLE TO PREVENT PERICORONITIS?
Pericoronitis may be prevented with regular dental visits and preemptive care. The dentist can aid in keeping these potential problem areas clean and determine the need for removal of the operculum. Alternatively, the dentist can also monitor the eruption of the third molars and determine the need for early extraction of these teeth. Removal of the wisdom teeth prior to eruption can prevent pericoronitis

REFERENCES
Contemporary oral & maxillifacial surgery “page 144” Newman.Carranza's.Clinical.Periodonyology.11th.Ed-”page103”
+page”440” Cawson’s essential of Oral pathology and oral medicine 8th – ED
“page 92+106”Angulation of mandibular third molars as a predictive factor for
pericoronitis." The Journal of Contemporary Dental Practice 10.3 (2009): 51-58.

THANK YOU