Embed Size (px)
Citation preview

Electrophysiological measures of low-level vision revealspatial processing deficits and hemispheric asymmetry inautism spectrum disorder
Francesca Pei # $
Department of Psychology, Stanford University,Stanford, CA, USA
Stanford Autism Center at Packard Children’s Hospital,Department of Psychiatric, School of Medicine, Stanford
University, Stanford, CA, USA
Stefano Baldassi # $
Department of Psychology, Stanford University,Stanford, CA, USA
Department of Neuroscience, Psychology, Pharmacology,and Child Health, University of Florence, Florence, Italy
Anthony M. Norcia # $Department of Psychology, Stanford University,
Stanford, CA, USA
There is accumulating evidence from electrophysiologicalstudies that low-level visual processing is atypical inindividuals with autism spectrum disorders (ASDs).Abnormalities in early stages of sensory processing are ofinterest because they could lead to downstreamfunctional deficits in social or cognitive domains. Usingsteady-state visual evoked potentials (SSVEPs), we studiedhow well spatial information is transmitted over a widerange of spatial frequencies (2–30 cycles/deg), includingthose at the limit of visibility (visual acuity). SSVEPs wererecorded over 128 channels in 16 ASD participantsbetween 5 and 17 years old and 17 age-matched,neurotypical (NT) participants. We observed a selectivereduction of the amplitude of the SSVEP second harmonicpattern reversal response between 5 and 17 cycles/deg.Responses measured at the fourth harmonic were normalat all spatial frequencies tested, as were responses at thelowest and highest spatial frequencies at the secondharmonic. The reduction of second harmonic responsesoccurred preferentially over right occipital electrodes.Because response abnormalities are restricted to aspecific response harmonic and to specific ranges ofspatial frequency, we can rule out nonspecific differencesbetween the ASD participants and the NT controls. Thisparticular pattern of loss, combined with the observedexaggeration of the loss over the right hemisphere,suggests that a highly specific neural substrate early in thevisual pathway is compromised in ASD.
Introduction
Autism spectrum disorder (ASD) is a neurodevel-opmental disorder characterized by impairment ofcommunication skills and social interaction and byrepetitive patterns of stereotyped behaviors. In additionto these core deficits, a variety of sensory abnormalitieshave been described in ASD patients since thediscovery of the disorder. Early reports noted that theresponse to sensory stimuli in ASD was similar to thatin deaf–blind children (Kanner, 1943; Wing, 1969).Later studies reported a high rate of sensory abnor-malities, mostly on the basis of questionnaires admin-istered to the parents (Baranek, David, Poe, Stone, &Watson, 2006; Klintwall et al., 2011). Such abnormal-ities have been described across all sensory domains(Marco, Hinkley, Hill, & Nagarajan, 2011). One study(Leekam, Nieto, Libby, Wing, & Gould, 2007) reportedthat up to 90% of individuals with ASD show tactile,auditory, or visual hypersensitivity or hyposensitivity.Because sensory symptoms and abnormal reactions tosensory stimuli are so common, they are now part ofthe diagnostic criteria for ASD in the fifth edition ofDiagnostic and Statistical Manual of Mental Disorders(American Psychiatric Association, 2000a).
Citation: Pei, F., Baldassi, S., & Norcia, A. M. (2014). Electrophysiological measures of low-level vision reveal spatial processingdeficits and hemispheric asymmetry in autism spectrum disorder. Journal of Vision, 14(11):3, 1–12, http://www.journalofvision.org/content/14/11/3, doi:10.1167/14.11.3.
Journal of Vision (2014) 14(11):3, 1–12 1http://www.journalofvision.org/content/14/11/3
doi: 10 .1167 /14 .11 .3 ISSN 1534-7362 � 2014 ARVOReceived November 3, 2013; published September 5, 2014

The high prevalence of sensory disturbances in ASDshas led to the suggestion that at least some of the high-level deficits in social interaction and communication inASDs could be explained in terms of downstreamconsequences of lower-level sensory and perceptualabnormalities (Behrmann et al., 2006; Caron, Mottron,Berthiaume, & Dawson, 2006). Abnormal visualperception in ASDs on performance-based assessmentwas first demonstrated as a local versus global feature-integration bias (Happe, 1996; Mottron & Belleville,1993; Pei et al., 2009; Plaisted, O’Riordan, & Baron-Cohen, 1998; Plaisted, Swettenham, & Rees, 1999).People with ASD showed a strong bias for details andlocal characteristics of the task in tests such as theembedded figure test (Jolliffe & Baron-Cohen, 1997;Shah & Frith, 1983) or the block design subtest of theWechsler intelligence quotient (IQ) battery (Shah &Frith, 1983; Venter, Lord, & Schopler, 1992). Thesereports of superior visual performance in ASDcontributed to the development of the weak centralcoherence hypothesis (Frith, 1989) and the enhancedperceptual functioning hypothesis (Mottron et al.,2006) of ASD. The local bias effect led researchers tofocus on visual search, a task that ASD observers seemto perform with less or no influence of the number ofdistractors (O’Riordan & Passetti, 2006; O’Riordan,Plaisted, Driver, & Baron-Cohen, 2001), possibly dueto diminished peripheral visual crowding (Baldassi etal., 2009) that in turn fits with the difficulties ASDobservers experience in visual integration tasks. How-ever, it has been argued that the deficit of global formprocessing in autism is far from understood because ofa lack of studies using stimuli that control for thepresence of low spatial frequency structure in the testmaterial (Dakin & Frith, 2005).
Subsequent research (Milne et al., 2002, 2006;Pellicano, Gibson, Maybery, Durkin, & Badcock, 2005;Spencer et al., 2000) found elevated thresholds in ASDon coherent motion tasks in which sensitivity to motionis determined on the basis of the fraction of coherentlymoving dots needed by the observer to discriminate thedirection of motion. Because motion direction cannotbe estimated on the basis of small regions of a coherentmotion display, this task is believed to tap globalprocessing mechanisms in the extrastriate cortex(Newsome & Pare, 1988; Williams & Sekuler, 1984).Bertone, Mottron, Jelenic, and Faubert (2003) de-scribed deficits in second-order motion that wereinterpreted as a deficit in the perception of complexstimuli rather than as a deficit in the early detectoralong the magnocellular stream. However, directiondiscrimination thresholds are elevated for movinggratings in ASD participants and their siblings,suggesting that lower-level motion processing is, in factabnormal and may be a genetically mediated risk factorfor ASD (Koh, Milne, & Dobkins, 2010a).
The integrity of low-level spatial mechanisms thatfeed higher-order visual processes has been less wellstudied. The spatial frequency hypothesis in ASDproposes that the detail-oriented bias in ASD reflectsenhanced sensitivity to high spatial frequencies or areduced sensitivity to low spatial frequencies (Behr-mann et al., 2006; Kemner & van Engeland, 2006;Milne et al., 2002). The studies performed based on thishypothesis have used widely differing techniques tomeasure visual acuity and contrast sensitivity, and theresults have been at least partially inconsistent (for areview see Koh et al., 2010a, b). For example, a recentstudy measured visual acuity, triggering a debate aboutthe possibility of a supernormal acuity—within therange of predator birds—in ASD (Ashwin, Ashwin,Rhydderch, Howells, & Baron-Cohen, 2009). However,the methodology used in that study has been ques-tioned and has led to several follow-up studies that didnot replicate the effect (Bach & Dakin, 2009; Bolte etal., 2012; Crewther & Sutherland, 2009).
Visual acuity is just one aspect of spatial contrastsensitivity. Several behavioral studies have measuredcontrast sensitivity thresholds at different spatialfrequencies and have found no significant differencebetween ASD and neurotypical (NT) age-matchedcontrols (Behrmann et al., 2006; Bertone & Faubert,2003; Bertone, Mottron, Jelenic, & Faubert, 2005; Koh,Milne, & Dobkins, 2010b; Pellicano et al., 2005). Incontrast to these results, lower thresholds have beenfound in a high-risk population of 6-month-old siblingsof children with ASD (McCleery, Allman, Carver, &Dobkins, 2007). Behavioral spatial acuity and contrastsensitivity measures appear to be largely unaffected inASD, but tasks involving more integrative processingare adversely affected.
Electrophysiological recordings are particularly use-ful in neurodevelopmental disorders as measures ofsensory processing because they do not require any taskperformance or language/comprehension abilities.Event-related potential (ERP) data show specific neuralabnormalities in ASD that are related to low-levelvisual processing. ERP responses for Navon stimuliand motion stimuli have been compared by Sutherlandand Crewther (2010) in people with high scores on theautism spectrum quotient (AQ), a scale that measuresthe prevalence of behaviors associated with ASD(Baron-Cohen, Wheelwright, Skinner, Martin, &Clubley, 2001; Brugha et al., 2012). The AQ iscorrelated with scores on the Autism DiagnosticObservation Schedule (ADOS), the current researchstandard for the diagnosis of ASD, but it is only weaklypredictive of criterion scores for ASD. Participantswith high AQ scores showed weaker initial corticalresponses to low-contrast stimuli and diminishedidentification of the global components in the Navontask. This was interpreted as a delay in primary visual/
Journal of Vision (2014) 14(11):3, 1–12 Pei, Baldassi, & Norcia 2

prestriate cortical processing of magnocellular input(Sutherland & Crewther, 2010). A follow-up study in asimilar participant group also found deficits in theearliest recordable response components and larger-than-normal responses when measured over a range ofcontrasts (Jackson et al., 2013). The ERP in an objectboundary detection paradigm was found to be abnor-mal in ASD, with differences emerging as early as 120ms after stimulus presentation (Vandenbroucke,Scholte, van Engeland, Lamme, & Kemner, 2008),implying a deficit in early to midlevel cortical process-ing stages. Using Gabor patches of different spatialfrequencies, Milne, Scope, Pascalis, Buckley, andMakeig (2009) found a general reduction in latency forthe ASD group but also a more specific increase in lowa-band power in the components located in or near theleft cingulate gyrus in the participants with ASD,suggesting that different low-level strategies were usedduring the task by ASD versus typical participants.
ERP abnormalities have been found in the process-ing of suprathreshold spatial frequency gratings. ERPalterations at 6 cycles/deg (cpd) were found in the N80component, while atypical processing of both high- andlow-frequency gratings occurred later in the P100response (Boeschoten, Kenemans, van Engeland, &Kemner, 2007). Jemel, Mimeault, Saint-Amour, Ho-sein, and Mottron (2010) recorded visual evokedpotentials (VEPs) from vertical sinusoidal achromaticgratings at different spatial frequencies. The N80component elicited by grating from 2.8 to 8 cpd wassmaller at low contrast levels in ASD versus controlgroups. Taken together, the ERP results suggest thatsuprathreshold processing at very early stages of thevisual pathway may be disrupted in ASD.
To further quantify the extent to which very low-level visual deficits may be present in ASD, wemeasured steady-state visual evoked potentials(SSVEPs) in response to a wide range of spatialfrequencies using the sweep technique (Norcia & Tyler,1985). This method has several advantages for use inpopulations with neurodevelopmental disorders. It canbe used to estimate sensory thresholds (e.g., the limitsof neuronal performance) as well as responsiveness atsuprathreshold levels and, importantly, it does notrequire observers to engage in behavioral tasks,potentially increasing its application over a greaterrange of severities in clinical populations. The use ofgrating stimuli reduces the complexity of visualprocessing to the minimum level, and an analysis of theSSVEP scalp topography from high-density electroen-cephalography (EEG) recordings allows us to make arough assessment as to whether the underlyinggenerators of the response lie in the early visual cortex.
ASD participants show reductions in the VEPresponse recorded over the early visual cortex to aspecific range of spatial frequencies (approximately 5–
17 cpd), and these reductions are restricted to a specifictemporal component of the VEP recording, the secondharmonic. We also find a relative reduction of signalamplitude over the right hemisphere. These differencesin the way spatial frequency information is processed inthe autistic brain suggest that early cortical mechanismsare altered in ASD. Taken together, the patterns ofdeficit we observe may constitute a biomarker for ASD.
Methods and materials
Participants
Sixteen children with ASD (5–17 years old; mean age¼ 9.2 years) participated in the study. They wererecruited through the Lucile Packard Children’sHospital at Stanford, the Interactive Autism Networkat Autism Speaks, and local parents’ associations. Thediagnosis of ASD was made on the basis of the fourthedition of Diagnostic and Statistical Manual of MentalDisorders (American Psychiatric Association, 2000b)since at the time of the assessment the fifth edition ofDiagnostic and Statistical Manual of Mental Disordershad not been published. Each diagnosis was confirmedby an experienced clinician using the ADOS instrument(Lord et al., 1989). Subjects with mental retardationdue to genetic and neurological pathology of otherkinds were excluded from the study. Control partici-pants were typically developing, age-matched children(n¼17; mean age¼8.6 years) with no history of seriousmedical, psychiatric, or neurological conditions whowere recruited through local schools. Because SSVEPtesting involves no instructions or tasks, is relativelyunaffected by attention, and is not affected by IQ (as isa measure used in infants), we did not match theparticipants on cognitive level. Because SSVEP gratingacuity is adult-like at age 5 (Norcia & Manny, 2003;Norcia & Tyler, 1985), we pooled the results across allages. All participants had normal or correct-to-normalvision, as also confirmed by the results of the study.Informed consent was obtained from a parent orguardian of the child, and an assent was signed by theparticipant whenever possible. The Institutional Re-view Board at Stanford University approved theexperimental protocol.
Experimental paradigm
Vertical, sine-wave luminance gratings were pre-sented as gray-scale images on a contrast-linearizedcathode ray tube (CRT) (Apple Inc., Cupertino, CA)1600 · 1200 pixels and a vertical refresh rate of 72 Hzover a field size of 378 by 288 at a mean luminance of
Journal of Vision (2014) 14(11):3, 1–12 Pei, Baldassi, & Norcia 3

50 cd/m2. The gratings were presented at 80% contrastand were contrast reversed with a square-wavetemporal profile at 7.5 Hz. The contrast reversal wasprecisely synchronized to the vertical refresh rate of themonitor (60 Hz). The participants sat at a viewingdistance of 1.5 m and were asked to look at the centerof the screen for the duration of individual trials thatlasted 12.8 s. When necessary, a researcher stoodbehind the screen while holding a control device to stoprecording when the subject was not fixating in thecenter of the screen. The fixation was monitored byobserving the centration of the corneal reflection of thedisplay monitor in the participants’ pupils. Thismeasure is accurate to approximately 48, a smallfraction of the grating display area (Allen, Tyler, &Norcia, 1996).
We used a steady-state sweep VEP technique thathas been used many times before to measure spatialfrequency response functions both in NT infants,children, and adults and in clinical populations(Almoqbel, Leat, & Irving, 2008; Norcia & Manny,2003). Following typical practice, the spatial frequencyof the grating was swept in equal linear increments (10)over trials lasting 12 s. The spatial frequency range (2–30 cpd) was chosen based on previous studies usingadults and older children as one that would span thefull range between very visible and invisible, includingthe acuity range (Norcia & Manny, 2003; Skoczenski &Norcia, 1999). The trial began with 1 s of anunrecorded flickering 2-cpd grating in order to avoidartifacts from the transient stimulus onset. Ten trialswere recorded for each subject, and all 10 trials in bothgroups were used for the final analysis.
VEP recording and analysis
The EEG data were collected using a 128-channelHydroCell Geodesic Sensor Net (Electrical GeodesicsInc., Eugene, OR), bandpass filtered from 0.1 to 50 Hzand digitized at a rate of 432 Hz (Net Amps 300 TM,Electrical Geodesics). Individual electrodes were ad-justed until impedances were below 60 kX beforestarting the recording.
Artifact rejection was performed off-line accordingto a sample-by-sample threshold procedure to removenoisy electrodes and replace them with the average ofthe six nearest neighboring electrodes. The EEG wasthen rereferenced to the common average of all theremaining electrodes. Epochs with more than 20% ofthe data samples exceeding 100 lV were excluded on asensor-by-sensor basis; this is the criterion used fornormal adults. Typically, these epochs included eyemovements or blinks.
The 7.5-Hz pattern reversal response is an SSVEPand is traditionally analyzed in the frequency domain
via Fourier analysis. The SSVEP amplitude in each 1-sepoch corresponding to the spatial frequency steps inthe stimulus sweep was determined by a discreteFourier transform (Norcia & Tyler, 1985). Within asubject, the amplitude and phase values were averagedcoherently (i.e., the average considered both phase andamplitude values) over the 10 trials recorded in eachparticipant. Thresholds in the sweep VEP method wereestimated subject by subject by extrapolating amplitudeversus spatial frequency function to zero amplitude.
Group-average spatial frequency response functionsfor the ASD and NT participants were formed byincoherently averaging (using amplitudes only) theindividual subject amplitudes recorded at the second(15 Hz) and fourth (30 Hz) harmonics of the stimulustemporal frequency.
Acuity estimation
Grating acuity was estimated from the spatialfrequency response functions by regressing the VEPamplitude versus spatial frequency function to zeroamplitude using criteria described in detail in previouspublications (Norcia, Clarke, & Tyler, 1985; Norcia &Tyler, 1985). Briefly, an automatic scoring algorithmsearched the VEP record, starting from the highestspatial frequency bin, for sections of the record thatexceeded a statistical criterion for the presence of anevoked response that was monotonically increasingwith decreasing spatial frequency and whose phase waseither constant or decreasing in delay. Using this searchcriterion, an approximately linear portion of thesuprathreshold response function was selected for theregression to zero amplitude.
Results
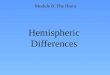
As is typical of steady-state pattern-reversal re-sponses (Regan, 1989), the recorded SSVEPs weredominated by even harmonic response components.Here reliable responses were consistently present atboth the second (15 Hz) and fourth (30 Hz) harmonics.As can be seen in Figure 1, each harmonic componentwas distributed over electrodes centered on theoccipital pole. SSVEP amplitudes were maximal at theOz electrode in both the NT and ASD groups.
Because the focus of activity at Oz in both groupswas maximal, we quantified the differences betweengroups as a function of spatial frequency and responseharmonics at three electrodes—occipital channels O1,Oz, and O2—that are centered on the maximum.Figure 2 shows the group-average spatial frequencytuning functions at each of these channels for the
Journal of Vision (2014) 14(11):3, 1–12 Pei, Baldassi, & Norcia 4

Figure 1. Topographic maps of the vector-average spectral amplitude collapsed across all spatial frequencies at the second and fourth
harmonics for both NT and ASD participants.
Figure 2. Amplitude of the sweep VEPs for the second harmonic (top) and the fourth harmonic (bottom) for three locations on the
scalp: O1 (left), Oz (Baca et al., 2009), and O2 (right). Electrodes are placed according to the 10-10 channels system map. Each graph
shows spatial frequency tuning functions for NT (filled circles) and ASD (open squares) observers. Error bars report the standard error
of the mean.
Journal of Vision (2014) 14(11):3, 1–12 Pei, Baldassi, & Norcia 5

second and fourth harmonics in the top and bottompanels, respectively. The open squares plot data fromthe ASD group, and the filled circles plot data from theNT observers.
The second harmonic spatial frequency tuningfunction had a peak at ;8 cpd in the NT group and asecond limb above ;15 cpd, consistent with previousresults with similar stimuli (Parry, Murray, & Hadjize-nonos, 1999; Strasburger, Murray, & Remky, 1993). Ateach electrode, second harmonic amplitudes were lowerin the ASD group between 5 and 17 cpd. ASD and NTamplitudes were similar outside of this range of spatialfrequencies and at all spatial frequencies at the fourthharmonic. Second harmonic response amplitude at thespatial frequency of the largest response in the NT groupwas 30% to 40% larger than it was in the ASD group atOz (p¼ 0.087) and was more than a factor of two largerat O2 (p¼ 0.01). Responses at O1 were not significantlydifferent (p¼ 0.35). The peak spatial frequency of thefourth harmonic function was slightly lower (5 cpd) inboth groups, but there was no difference in amplitude atany of the electrodes. The locations of the peaks and theresults of two-tailed t-tests for each harmonic andelectrode are indicated in Figure 2 by the arrows withcorresponding p-values. The top-center panel also plotsthe average grating acuity thresholds (the two isolatedpoints with error along the x-axis) calculated fromindividual-participant vector-averaged functions, alongwith the standard error of the mean. Grating acuities didnot differ between the ASD and NT groups (25.8 6 1.47cpd in the NT group and 24.6 6 1.99 cpd in the ASDgroup, p¼ 0.11, ns).
To confirm that the reported significant differencesbetween groups were not due to a small number ofindividual participants in either group or unequalvariance between groups and to show the power of thestatistical effects, we compared the group differences on10,000 bootstrap samples of the two groups. Thisallowed us to create a distribution-free, empiricalsampling distribution that we used to confirm thedifference we report from conventional t-tests.
Table 1 summarizes the statistical analysis per-formed. For each electrode and harmonic (first and
second columns from left, respectively), we report theoutput of our two-tailed t-tests. The third column fromleft reports the degrees of freedom (df), which is always31 except for the second harmonic at O2. In this specificcondition the data do not fulfill the assumption ofhomoscedasticity and the results are corrected accord-ing to Levene’s test for equality of variances. Thecentral column (t) reports the value of t, while thecolumn labeled p reports the p-values returned com-paring the empirical data. We also performed the samecomparisons on log-transformed data because thistransformation equalized the variances betweengroups. Each of these comparisons showed p-valuesequal to or smaller than those reported in Table 1.
The two rightmost columns in Figure 2 report thepower, measured as the proportion of significant t-testcomparisons, and the median p-value. In particular, thepower column clearly indicates that the differencegrows steadily only in the second harmonic by movingthe recording site from left to right, and the t-test isvery powerful for electrode O2. At the fourth harmonicthe channel showing the largest trend was significant inonly about 12% of the bootstrap samples, implying nodifference between groups at this harmonic.
Discussion
SSVEP responses show that ASD has a highlyspecific effect on the processing of spatial informationin the early visual cortex. The effect we observe isrestricted to a subset of the full range of spatialfrequencies tested and to the second harmonic. Thereare no group-level differences at any spatial frequencyat the fourth harmonic. Our results are particularlyclear on the specifically visual and neural nature of thedifference because the selectivity of the deficits rules outnonspecific group-level differences in quality of fixa-tion, accommodation, or motion artifacts. Each ofthese possible sources of group differences should affectboth the second and fourth harmonics because theyaffect either the quality of the input or the quality of
Electrode Harmonic df t p Power Median p
O1 (left) Second 31 �0.944 0.353 0.167 0.303
Fourth 31 0.986 0.332 0.125 0.302
Oz (central) Second 31 �1.767 0.087 0.409 0.079
Fourth 31 0.698 0.491 0.088 0.389
O2 (right) Second 24.34 �2.759 0.011 0.782 0.009
Fourth 31 �0.391 0.699 0.072 0.461
Table 1. Results of the three 2-tailed t-test comparisons of peak amplitudes between groups for each of the three channels and foreach of the two harmonics considered (second column). Levene’s test of homoscedasticity was significant only at O2 for the secondharmonic component (degrees of freedom corrected accordingly). The two rightmost columns report the power measured as theproportion of significant t-test comparison.
Journal of Vision (2014) 14(11):3, 1–12 Pei, Baldassi, & Norcia 6

the evoked potential recording equivalently. Similarly,variations in attention between the groups would beunlikely to explain differences between the twoharmonics because they are measured simultaneouslyfrom the same data record.
Two previous behavioral studies (Behrmann et al.,2006; Koh et al., 2010b) made detailed measurementsof contrast sensitivity over the range of spatialfrequencies where we found second harmonic deficits(5–17 cpd). These studies found no differences inthreshold sensitivity between ASD and NT controls. Itis possible that the effects we observe are restricted tohigh levels of sensory input and may thus reflect afailure of the regulation of contrast gain rather thanchanges in absolute sensitivity.
What might underlie the specific loss seen at thesecond harmonic? A previous SSVEP spatial frequencytuning study suggested that the second harmonic of theSSVEP pattern reversal response is generated byseparate channels operating at lower versus higherspatial frequencies (Strasburger et al., 1993). Ourresults are consistent with separate spatial processingmechanisms because the response at 2 cpd is normalbut the response over the range of 8.2 to 14.4 cpd is not.However, this cannot be the whole story. First, we findanother range of spatial frequencies above the limit ofStrasburger et al.’s (1993) higher spatial frequencymechanism where responses are normal. This suggeststhe presence of a third spatial channel. Second, ourchannel properties are not strictly determined by theirspatial frequency tuning: The fourth harmonic responsecomponent shows no effect over the entire range. Giventhe mass nature of the SSVEP, it is likely that multipleunderlying generators contribute to the recorded signal.Our results indicate that a subset of these multiplegenerators is specifically affected by ASD. It will beimportant in future research to determine the underly-ing neural substrates that contribute to the second andfourth harmonics in order to pinpoint the neural basisof the ASD deficit we have observed.
Visual acuity
By recording SSVEPs over a wide range of spatialfrequencies, we were also able to objectively estimatethe visual acuity threshold without the task demands ofpsychophysical experiments. We found no difference ingrating acuity in the ASD and control groups,consistent with the results of more recent behavioralstudies (Bach & Dakin, 2009; Tavassoli, Latham, Bach,Dakin, & Baron-Cohen, 2011). These results furtherreinforce that the two groups were equally able tocomply with the task demands for fixation andaccommodation despite the absence of a requirementfor performance of a specific behavioral task.
Hemispheric asymmetry
Another important result of the present study is theselective reduction of the SSVEP response over theright hemisphere. Right-hemisphere deficits in VEPresponses have been reported in a previous study. Theevoked response to photic stimulation over the rightoccipital cortex was depressed when measured at 11fixed temporal frequencies (3–24 Hz) in a group ofchildren aged 6 to 14 years with the diagnosis of autismwithout significant mental retardation (Lazarev, Pon-tes, & deAzevedo, 2009). Our findings confirm andextend this previous report of right-hemisphere alter-ations of the visual response in ASD. Additionalevidence for right-hemisphere sensory deficits comesfrom a magnetoencephalography study on auditoryprocessing (Orekhova et al., 2012). Orekhova et al.(2012) found a relationship between the severity of thesensory modulation abnormalities and the lack ofnormal rightward lateralization of P100 in ASDchildren. The right hemisphere in autistic people alsofails to respond to auditory temporal novelty (Ore-khova et al., 2009). Finally, broadband EEG power hasan abnormal distribution suggestive of a loss in theright hemisphere when measured in boys with autismbetween 3 and 8 years old (Stroganova et al., 2007).
At the behavioral level, abnormal brain lateralizationhas also been implicated in an eye tracking studyperformed in a group at high risk for ASD (infantsiblings of children with an ASD diagnosis). High-riskinfants did not show a left visual field fixation bias likethe one displayed by low-risk infants (Dundas, Gastgeb,& Strauss, 2012). Typically developing children prefer-entially fixate the left part of the face. Information fromthe left visual field is projected to the right hemisphere,which is known to be associated with face processingabilities, with notable lateralization in the right fusiformgyrus (Haxby, Hoffman, & Gobbini, 2000).
Vulnerability of one hemisphere versus anothermay bedue to the two cerebral hemispheres having differentdevelopmental trajectories in normal development: Theright hemisphere develops more quickly during typicalfetal development (Geschwind & Galaburda, 1985;Hellige, 1993). Differential developmental sequences mayexpose the two hemispheres differentially to environ-mental influences or may indicate that separate geneticprograms control the development of the two hemi-spheres. The ASD phenotype we observe could resultfrom either of these two factors or a combination of both.
Relationship of the present findings to higher-level visual cognition
Studying the early visual system can provideinformation on brain circuitry as well as on the extent
Journal of Vision (2014) 14(11):3, 1–12 Pei, Baldassi, & Norcia 7

to which low-level visual anomalies may influencehigher-level vision and cognition. The visual worldcontains a wide range of spatial scales that constantlychange while we are moving closer to or farther awayfrom objects. The difficulty of processing visual targetscan be predicted in typically developed subjects byusing the results of spatial contrast sensitivity tests(Owsley & Sloane, 1987). This relationship may,however, break down in autism, especially at high levelsof input. The method used here to identify spatialprocessing deficits may be useful in determiningwhether certain spatial frequency bands contribute todeficits on other tasks, such as ones involving local andglobal dimensions (Blakemore & Campbell, 1969;Brady & Oliva, 2012). Several studies in this area havesuggested that the processing of local and more globalaspects of both hierarchical and face stimuli is relatedto the processing of specific spatial frequencies (Bad-cock, Whitworth, Badcock, & Lovegrove, 1990;Boeschoten, Kemner, Kenemans, & van Engeland,2005; Goffaux, Gauthier, & Rossion, 2003; Goffaux,Hault, Michel, Vuong, & Rossion, 2005; Han, Yund, &Woods, 2003; Jemel, Mottron, & Dawson, 2006;LaGasse, 1993; Ruiz-Soler & Beltran, 2006). It wouldbe informative to compare neural measures of spatialprocessing such as the ones performed here withbehavioral ones to determine whether one is predictiveof the other, as would be the case if the local processingbias of subjects with ASD for these and other visualstimuli is related to a pervasive abnormality in spatialfrequency analysis (Deruelle, Rondan, Gepner, &Tardif, 2004; Plaisted, Dobler, Bell, & Davis, 2006).
A challenge for future research is relating thesuprathreshold processing deficits we have observed tobehavioral responses. The SSVEP deficit we haveobserved is not simply a deficit at certain spatialfrequencies. Some of the evoked response, that portioncontained in the fourth harmonic, is not affected in ASD.Exactly what aspect of behavior would be associated withthe fourth rather than the second harmonic is notcompletely clear at this point. What is needed is a betterunderstanding of the nonlinear mechanisms that give riseto the SSVEP and further exploration of the full range ofspatial and temporal frequencies that form the limits ofspatial and temporal contrast sensitivity. Further inves-tigation of this topic is needed in order to betterunderstand at which point of the neural pathway thedeficits we observe are generated. It will also be importantto determine whether the highly selective pattern ofresponse alterations we have observed here is specific toASD or whether it occurs in other forms of intellectualdisability. This is particularly important to establish if onewishes to use quantitative neural measurements such asthose presented here to guide treatment, intervention, andoptimization of the stimulation used, especially given the
proliferation of electronic device-based applicationsdedicated to a wide population of autistic users.
Conclusions
Our results add to the accumulating body ofevidence suggesting that deficits at the earliest stages ofsensory processing are associated with autism. Since thevisual system is organized hierarchically, abnormalitiesin higher-level functions may be at least partially due todownstream effects of abnormalities occurring atearlier stages. Quantitative and efficient SSVEP mea-surements of low-level visual processing mechanismsmay ultimately help us understand the overall abilitiesof people with ASD to interpret and make full sense ofthe visual world. Conversely, the specificity of thedeficits we find is difficult to explain on the basis ofdeficits in higher-level cognitive functions such aslanguage, task comprehension or performance issues,or IQ. Rather, our results point to what could be a veryspecific biological substrate that is altered in ASD.Key points:
� Sensory processing abnormalities are common inASD.
� The visual system can be used as an entry point tostudy brain activity and system regulation.
� We can use task-absent VEP tests to study very low-level visual functions that can potentially providenew biomarkers for the diagnosis of the disorderearly in life.
� The spatial processing abnormalities and the brainhemispheric asymmetry that we have found mayundermine high-level cognitive functions and inter-fere with the child’s interaction with the visualworld.
Keywords: autism, vision, visual evoked potential,spatial frequency, visual perception
Acknowledgments
This work was supported by the Simons Foundationfor Autism Research Initiative (SFARI) and by theBass Society for Pediatric Scholars. We thank all thefamilies and children who dedicated their time to helpus with our research project.
Commercial relationships: none.Corresponding author: Francesca Pei.Email: [email protected]: Department of Psychology, Stanford Uni-versity, Stanford, CA, USA.
Journal of Vision (2014) 14(11):3, 1–12 Pei, Baldassi, & Norcia 8

References
Allen, D., Tyler, C. W., & Norcia, A. M. (1996).Development of grating acuity and contrast sensi-tivity in the central and peripheral visual field of thehuman infant. Vision Research, 36(13), 1945–1953.
Almoqbel, F., Leat, S. J., & Irving, E. (2008). Thetechnique, validity and clinical use of the sweepVEP. Ophthalmic and Physiological Optics, 28(5),393–403, doi:10.1111/j.1475-1313.2008.00591.x.
American Psychiatric Association. (2000a). Diagnosticcriteria from DSM-IV-TR. Washington, DC:American Psychiatric Association.
American Psychiatric Association. (2000b). ElectronicDSM-IV-TR plus [CD-ROM].
Ashwin, E., Ashwin, C., Rhydderch, D., Howells, J., &Baron-Cohen, S. (2009). Eagle-eyed visual acuity:An experimental investigation of enhanced per-ception in autism. Biological Psychiatry, 65(1), 17–21, doi:10.1016/j.biopsych.2008.06.012.
Baca, C. B., Cheng, E. M., Spencer, S. S., Vassar, S.,Vickrey, B. G., & Multicenter Study of EpilepsySurgery. (2009). Racial differences in patientexpectations prior to resective epilepsy surgery.Epilepsy and Behavior, 15(4), 452–455, doi:10.1016/j.yebeh.2009.05.010.
Bach, M., & Dakin, S. C. (2009). Regarding ‘‘Eagle-eyed visual acuity: An experimental investigation ofenhanced perception in autism.’’ Biological Psychi-atry, 66(10), e19–e20, doi:10.1016/j.biopsych.2009.02.035.
Badcock, J. C., Whitworth, F. A., Badcock, D. R., &Lovegrove, W. J. (1990). Low-frequency filteringand the processing of local-global stimuli. Percep-tion, 19(5), 617–629.
Baldassi, S., Pei, F., Megna, N., Recupero, G.,Viespoli, M., Igliozzi, R., . . . Cioni, G. (2009).Search superiority in autism within, but not outsidethe crowding regime. Vision Research, 49(16),2151–2156, doi:10.1016/j.visres.2009.06.007.
Baranek, G. T., David, F. J., Poe, M. D., Stone, W. L.,& Watson, L. R. (2006). Sensory ExperiencesQuestionnaire: Discriminating sensory features inyoung children with autism, developmental delays,and typical development. Journal of Child Psy-chology and Psychiatry, 47(6), 591–601, doi:10.1111/j.1469-7610.2005.01546.x.
Baron-Cohen, S., Wheelwright, S., Skinner, R., Martin,J., & Clubley, E. (2001). The autism-spectrumquotient (AQ): Evidence from Asperger syndrome/high-functioning autism, males and females, scien-
tists and mathematicians. Journal of Autism andDevelopmental Disorders, 31(1), 5–17.
Behrmann, M., Avidan, G., Leonard, G. L., Kimchi,R., Luna, B., Humphreys, K., & Minshew, N.(2006). Configural processing in autism and itsrelationship to face processing. Neuropsychologia,44(1), 110–129, doi:10.1016/j.neuropsychologia.2005.04.002.
Bertone, A., & Faubert, J. (2003). How is complexsecond-order motion processed? Vision Research,43(25), 2591–2601.
Bertone, A., Mottron, L., Jelenic, P., & Faubert, J.(2003). Motion perception in autism: A ‘‘complex’’issue. Journal of Cognitive Neuroscience, 15(2), 218–225, doi:10.1162/089892903321208150.
Bertone, A., Mottron, L., Jelenic, P., & Faubert, J.(2005). Enhanced and diminished visuo-spatialinformation processing in autism depends onstimulus complexity. Brain, 128(Pt. 10), 2430–2441,doi:10.1093/brain/awh561.
Blakemore, C., & Campbell, F. W. (1969). Adaptationto spatial stimuli. Journal of Physiology, 200(1),11P–13P.
Boeschoten, M. A., Kemner, C., Kenemans, J. L., &van Engeland, H. (2005). The relationship betweenlocal and global processing and the processing ofhigh and low spatial frequencies studied by event-related potentials and source modeling. BrainResearch Cognitive Brain Research, 24(2), 228–236,doi:10.1016/j.cogbrainres.2005.01.021.
Boeschoten, M. A., Kenemans, J. L., van Engeland, H.,& Kemner, C. (2007). Abnormal spatial frequencyprocessing in high-functioning children with per-vasive developmental disorder (PDD). ClinicalNeurophysiology, 118(9), 2076–2088, doi:10.1016/j.clinph.2007.05.004.
Bolte, S., Schlitt, S., Gapp, V., Hainz, D., Schirman, S.,Poustka, F., . . . Walter, H. (2012). A close eye onthe eagle-eyed visual acuity hypothesis of autism.Journal of Autism and Developmental Disorders,42(5), 726–733, doi:10.1007/s10803-011-1300-3.
Brady, T. F., & Oliva, A. (2012). Spatial frequencyintegration during active perception: Perceptualhysteresis when an object recedes. Frontiers inPsychology, 3, 462,doi:10.3389/fpsyg.2012.00462.
Brugha, T. S., McManus, S., Smith, J., Scott, F. J.,Meltzer, H., Purdon, S., . . . Bankart, J. (2012).Validating two survey methods for identifying casesof autism spectrum disorder among adults in thecommunity. Psychological Medicine, 42(3), 647–656, doi:10.1017/S0033291711001292.
Caron, M. J., Mottron, L., Berthiaume, C., & Dawson,M. (2006). Cognitive mechanisms, specificity and
Journal of Vision (2014) 14(11):3, 1–12 Pei, Baldassi, & Norcia 9

neural underpinnings of visuospatial peaks inautism. Brain, 129(Pt. 7), 1789–1802, doi:10.1093/brain/awl072.
Crewther, D. P., & Sutherland, A. (2009). The more helooked inside, the more Piglet wasn’t there: Isautism really blessed with visual hyperacuity?Biological Psychiatry, 66(10), e21–e22, doi:10.1016/j.biopsych.2009.02.036.
Dakin, S., & Frith, U. (2005). Vagaries of visualperception in autism. Neuron, 48(3), 497–507, doi:10.1016/j.neuron.2005.10.018.
Deruelle, C., Rondan, C., Gepner, B., & Tardif, C.(2004). Spatial frequency and face processing inchildren with autism and Asperger syndrome.Journal of Autism and Developmental Disorders,34(2), 199–210.
Dundas, E., Gastgeb, H., & Strauss, M. S. (2012). Leftvisual field biases when infants process faces: Acomparison of infants at high- and low-risk forautism spectrum disorder. Journal of Autism andDevelopmental Disorders, 42(12), 2659–2668, doi:10.1007/s10803-012-1523-y.
Geschwind, N., & Galaburda, A. M. (1985). Cerebrallateralization. Biological mechanisms, associations,and pathology: III. A hypothesis and a program forresearch. Archives of Neurology, 42(7), 634–654.
Goffaux, V., Gauthier, I., & Rossion, B. (2003). Spatialscale contribution to early visual differences be-tween face and object processing. Brain ResearchCognitive Brain Research, 16(3), 416–424.
Goffaux, V., Hault, B., Michel, C., Vuong, Q. C., &Rossion, B. (2005). The respective role of low andhigh spatial frequencies in supporting configuraland featural processing of faces. Perception, 34(1),77–86.
Frith, U. (1989). Autism and ‘‘theory of mind.’’ In C.Gillberg (Ed.), Diagnosis and treatment of autism(pp. 33–52). New York: Plenum Press.
Han, S., Yund, E. W., & Woods, D. L. (2003). An ERPstudy of the global precedence effect: The role ofspatial frequency. Clinical Neurophysiology,114(10), 1850–1865.
Happe, F. G. (1996). Studying weak central coherenceat low levels: Children with autism do not succumbto visual illusions. A research note. Journal of ChildPsychology and Psychiatry, 37(7), 873–877.
Haxby, J. V., Hoffman, E. A., & Gobbini, M. I. (2000).The distributed human neural system for faceperception. Trends in Cognitive Science, 4(6), 223–233.
Hellige, J. B. (1993). Hemispheric asymmetry: What’s
right and what’s left. Cambridge, MA: HarvardUniversity Press.
Jackson, B. L., Blackwood, E. M., Blum, J., Car-ruthers, S. P., Nemorin, S., Pryor, B. A., . . .Crewther, D. P. (2013). Magno- and parvocellularcontrast responses in varying degrees of autistictrait. PLoS One, 8(6), e66797, doi:10.1371/journal.pone.0066797.
Jemel, B., Mimeault, D., Saint-Amour, D., Hosein, A.,& Mottron, L. (2010). VEP contrast sensitivityresponses reveal reduced functional segregation ofmid and high filters of visual channels in autism.Journal of Vision, 10(6):13, 1–13, http://www.journalofvision.org/content/10/6/13, doi:10.1167/10.6.13. [PubMed] [Article]
Jemel, B., Mottron, L., & Dawson, M. (2006).Impaired face processing in autism: Fact orartifact? Journal of Autism and DevelopmentalDisorders, 36(1), 91–106, doi:10.1007/s10803-005-0050-5.
Jolliffe, T., & Baron-Cohen, S. (1997). Are people withautism and Asperger syndrome faster than normalon the Embedded Figures Test? Journal of ChildPsychology and Psychiatry, 38(5), 527–534.
Kanner, L. (1943). Autistic disturbances of affectivecontact. Nervous Child, 2(3), 217–250.
Kemner, C., & van Engeland, H. (2006). ERPs and eyemovements reflect atypical visual perception inpervasive developmental disorder. Journal of Au-tism and Developmental Disorders, 36(1), 45–54.
Klintwall, L., Holm, A., Eriksson, M., Carlsson, L. H.,Olsson, M. B., Hedvall, A., . . . Fernell, E. (2011).Sensory abnormalities in autism. A brief report.Research in Developmental Disabilities, 32(2), 795–800, doi:10.1016/j.ridd.2010.10.021.
Koh, H. C., Milne, E., & Dobkins, K. (2010a).Contrast sensitivity for motion detection anddirection discrimination in adolescents with autismspectrum disorders and their siblings. Neuropsy-chologia, 48(14), 4046–4056, doi:10.1016/j.neuropsychologia.2010.10.008.
Koh, H. C., Milne, E., & Dobkins, K. (2010b). Spatialcontrast sensitivity in adolescents with autismspectrum disorders. Journal of Autism and Devel-opmental Disorders, 40(8), 978–987, doi:10.1007/s10803-010-0953-7.
LaGasse, L. L. (1993). Effects of good form and spatialfrequency on global precedence. Perception andPsychophysics, 53(1), 89–105.
Lazarev, V. V., Pontes, A., & deAzevedo, L. C. (2009).EEG photic driving: Right-hemisphere reactivitydeficit in childhood autism. A pilot study. Interna-
Journal of Vision (2014) 14(11):3, 1–12 Pei, Baldassi, & Norcia 10

tional Journal of Psychophysiology, 71(2), 177–183,doi:10.1016/j.ijpsycho.2008.08.008.
Leekam, S. R., Nieto, C., Libby, S. J., Wing, L., &Gould, J. (2007). Describing the sensory abnor-malities of children and adults with autism. Journalof Autism and Developmental Disorders, 37(5), 894–910, doi:10.1007/s10803-006-0218-7.
Lord, C., Rutter, M., Goode, S., Heemsbergen, J.,Jordan, H., Mawhood, L., & Schopler, E. (1989).Autism diagnostic observation schedule: A stan-dardized observation of communicative and socialbehavior. Journal of Autism and DevelopmentalDisorders, 19(2), 185–212.
Marco, E. J., Hinkley, L. B., Hill, S. S., & Nagarajan,S. S. (2011). Sensory processing in autism: A reviewof neurophysiologic findings. Pediatric Research,69(5 Pt. 2), 48R–54R, doi:10.1203/PDR.0b013e3182130c54.
McCleery, J. P., Allman, E., Carver, L. J., & Dobkins,K. R. (2007). Abnormal magnocellular pathwayvisual processing in infants at risk for autism.Biological Psychiatry, 62(9), 1007–1014, doi:10.1016/j.biopsych.2007.02.009.
Milne, E., Scope, A., Pascalis, O., Buckley, D., &Makeig, S. (2009). Independent component analy-sis reveals atypical electroencephalographic activityduring visual perception in individuals with autism.Biological Psychiatry, 65(1), 22–30, doi:10.1016/j.biopsych.2008.07.017.
Milne, E., Swettenham, J., Hansen, P., Campbell, R.,Jeffries, H., & Plaisted, K. (2002). High motioncoherence thresholds in children with autism.Journal of Child Psychology and Psychiatry, 43(2),255–263.
Milne, E., White, S., Campbell, R., Swettenham, J.,Hansen, P., & Ramus, F. (2006). Motion and formcoherence detection in autistic spectrum disorder:Relationship to motor control and 2:4 digit ratio.Journal of Autism and Developmental Disorders,36(2), 225–237, doi:10.1007/s10803-005-0052-3.
Mottron, L., & Belleville, S. (1993). A study ofperceptual analysis in a high-level autistic subjectwith exceptional graphic abilities. Brain and Cog-nition, 23(2), 279–309, doi:10.1006/brcg.1993.1060.
Mottron, L., Dawson, M., Soulieres, I., Hubert, B., &Burack, J. (2006). Enhanced perceptual functioningin autism: an update, and eight principles of autisticperception. Journal of Autism and DevelopmentalDisorders, 36(1), 27–43.
Newsome, W. T., & Pare, E. B. (1988). A selectiveimpairment of motion perception following lesionsof the middle temporal visual area (MT). Journal ofNeuroscience, 8(6), 2201–2211.
Norcia, A. M., Clarke, M., & Tyler, C. W. (1985).Digital filtering and robust regression techniquesfor estimating sensory thresholds from the evokedpotential. IEEE Engineering and Medicine inBiology, 4, 26–32.
Norcia, A. M., & Manny, R.E. (2003). Development ofvision in infants. In P. L. Kaufman & A. Alm(Eds.), Adler’s physiology of the eye (10th ed., pp.531–551). St. Louis, MO: Mosby.
Norcia, A. M., & Tyler, C. W. (1985). Spatial frequencysweep VEP: Visual acuity during the first year oflife. Vision Research, 25(10), 1399–1408.
Orekhova, E. V., Stroganova, T. A., Prokofiev, A. O.,Nygren, G., Gillberg, C., & Elam, M. (2009). Theright hemisphere fails to respond to temporalnovelty in autism: Evidence from an ERP study.Clinical Neurophysiology, 120(3), 520–529, doi:10.1016/j.clinph.2008.12.034.
Orekhova, E. V., Tsetlin, M. M., Butorina, A. V.,Novikova, S. I., Gratchev, V. V., Sokolov, P. A.,. . . Stroganova, T. A. (2012). Auditory cortexresponses to clicks and sensory modulation diffi-culties in children with autism spectrum disorders(ASD). PLoS One, 7(6), e39906, doi:10.1371/journal.pone.0039906.
O’Riordan, M., & Passetti, F. (2006). Discrimination inautism within different sensory modalities. Journalof Autism and Developmental Disorders, 36(5), 665–675, doi:10.1007/s10803-006-0106-1.
O’Riordan, M. A., Plaisted, K. C., Driver, J., & Baron-Cohen, S. (2001). Superior visual search in autism.Journal of Experimental Psychology: Human Per-ception and Performance, 27(3), 719–730.
Owsley, C., & Sloane, M. E. (1987). Contrastsensitivity, acuity, and the perception of ‘real-world’ targets. British Journal of Ophthalmology,71(10), 791–796.
Parry, N. R., Murray, I. J., & Hadjizenonos, C. (1999).Spatio-temporal tuning of VEPs: Effect of mode ofstimulation. Vision Research, 39(21), 3491–3497.
Pei, F., Baldassi, S., Procida, G., Igliozzi, R., Tancredi,R., Muratori, F., & Cioni, G. (2009). Neuralcorrelates of texture and contour integration inchildren with autism spectrum disorders. VisionResearch, 49(16), 2140–2150, doi:10.1016/j.visres.2009.06.006.
Pellicano, E., Gibson, L., Maybery, M., Durkin, K., &Badcock, D. R. (2005). Abnormal global process-ing along the dorsal visual pathway in autism: Apossible mechanism for weak visuospatial coher-ence? Neuropsychologia, 43(7), 1044–1053, doi:10.1016/j.neuropsychologia.2004.10.003.
Plaisted, K., Dobler, V., Bell, S., & Davis, G. (2006).
Journal of Vision (2014) 14(11):3, 1–12 Pei, Baldassi, & Norcia 11

The microgenesis of global perception in autism.Journal of Autism and Developmental Disorders,36(1), 107–116, doi:10.1007/s10803-005-0047-0.
Plaisted, K., O’Riordan, M., & Baron-Cohen, S.(1998). Enhanced visual search for a conjunctivetarget in autism: A research note. Journal of ChildPsychology and Psychiatry, 39(5), 777–783.
Plaisted, K., Swettenham, J., & Rees, L. (1999).Children with autism show local precedence in adivided attention task and global precedence in aselective attention task. Journal of Child Psychologyand Psychiatry, 40(5), 733–742.
Regan, D. (1989). Human brain electrophysiology:Evoked potentials and evoked magnetic fields inscience and medicine. New York: Elsevier.
Ruiz-Soler, M., & Beltran, F. S. (2006). Face percep-tion: An integrative review of the role of spatialfrequencies. Psychological Research, 70(4), 273–292, doi:10.1007/s00426-005-0215-z.
Shah, A., & Frith, U. (1983). An islet of ability inautistic children: A research note. Journal of ChildPsychology and Psychiatry, 24(4), 613–620.
Skoczenski, A. M., & Norcia, A. M. (1999). Develop-ment of VEP Vernier acuity and grating acuity inhuman infants. Investigative Ophthalmology andVisual Science, 40(10), 2411–2417, http://www.iovs.org/content/40/10/2411. [PubMed] [Article]
Spencer, J., O’Brien, J., Riggs, K., Braddick, O.,Atkinson, J., & Wattam-Bell, J. (2000). Motionprocessing in autism: Evidence for a dorsal streamdeficiency. Neuroreport, 11(12), 2765–2767.
Strasburger, H., Murray, I. J., & Remky, A. (1993).Sustained and transient mechanisms in the steady-state visual-evoked potential—Onset presentation
compared to pattern reversal. Clinical VisionSciences, 8(3), 211–234.
Stroganova, T. A., Nygren, G., Tsetlin, M. M.,Posikera, I. N., Gillberg, C., Elam, M., &Orekhova, E. V. (2007). Abnormal EEG laterali-zation in boys with autism. Clinical Neurophysiol-ogy, 118(8), 1842–1854, doi:10.1016/j.clinph.2007.05.005.
Sutherland, A., & Crewther, D. P. (2010). Magnocel-lular visual evoked potential delay with high autismspectrum quotient yields a neural mechanism foraltered perception. Brain, 133(Pt. 7), 2089–2097,doi:10.1093/brain/awq122.
Tavassoli, T., Latham, K., Bach, M., Dakin, S. C., &Baron-Cohen, S. (2011). Psychophysical measuresof visual acuity in autism spectrum conditions.Vision Research, 51(15), 1778–1780, doi:10.1016/j.visres.2011.06.004.
Vandenbroucke, M. W., Scholte, H. S., van Engeland,H., Lamme, V. A., & Kemner, C. (2008). A neuralsubstrate for atypical low-level visual processing inautism spectrum disorder. Brain, 131(Pt. 4), 1013–1024, doi:10.1093/brain/awm321.
Venter, A., Lord, C., & Schopler, E. (1992). A follow-up study of high-functioning autistic children.Journal of Child Psychology and Psychiatry, 33(3),489–507.
Williams, D. W., & Sekuler, R. (1984). Coherent globalmotion percepts from stochastic local motions.Vision Research, 24(1), 55–62.
Wing, L. (1969). Handicaps of autistic children—Acomparative study. Journal of Child Psychology andPsychiatry and Allied Disciplines, 10(1), 1–40, doi:10.1111/J.1469-7610.1969.Tb02066.X.
Journal of Vision (2014) 14(11):3, 1–12 Pei, Baldassi, & Norcia 12